Risk Adjustment: Implications for Community Health Centers
|
|
|
- Shon Cummings
- 9 years ago
- Views:
Transcription
1 Risk Adjustment: Implications for Community Health Centers Todd Gilmer, PhD Division of Health Policy Department of Family and Preventive Medicine University of California, San Diego
2 Overview Program and Policy Goals of Risk Adjustment Brief History of Risk Adjustment Mechanics of Risk Adjustment using CDPS Risk Adjustment and Primary Care Opportunities for Community Health Centers to Demonstrate Value Added
3 Program and Policy Goals of Risk Adjustment
4 What is Risk Adjustment? Health based risk assessment measuring illness burden at the individual or group level using indicators of health status such as diagnoses, pharmaceuticals, cognitive / functional limitations Health based risk adjustment comparing populations, adjusting outcomes, or adjusting health plan payments using health status
5 Why is Risk Adjustment Necessary? % of Population 1% 10% 50% % of Expenditure 30% 72% 95%
6 Goals of Risk Adjustment To make equitable comparisons among health plans that take the health status of their enrolled members into consideration To minimize the incentives for plans and providers from selectively enrolling healthier members To provide adequate financing for those who treat individuals with higher-than-average health needs
7 Reasons for Risk Variation A particular health plan s provider network may predispose it to certain risk selections (e.g., those affiliated with academic medical centers) Some geographic regions may include a sicker-thanaverage mix of enrollees Some provider groups may attract specific population subsets (e.g. diabetes, AIDS, children with disabilities)
8 Risk Adjustment Applications To adjust capitation payments for expected future expenditure based on health status To risk profile and/or identify persons for disease or high risk case management To adjust observed differences in performance measures, utilization, and/or cost based upon observed differences illness burden
9 Benefits of Risk Adjustment Allows states to foster competition based on quality and efficiency rather than on risk selection Supports health plans that attract clients with specific service needs Allows health plans to promote efficiency in care management without the accompanying expenditure risk that results from attracting a sicker population
10 History of Risk Adjustment
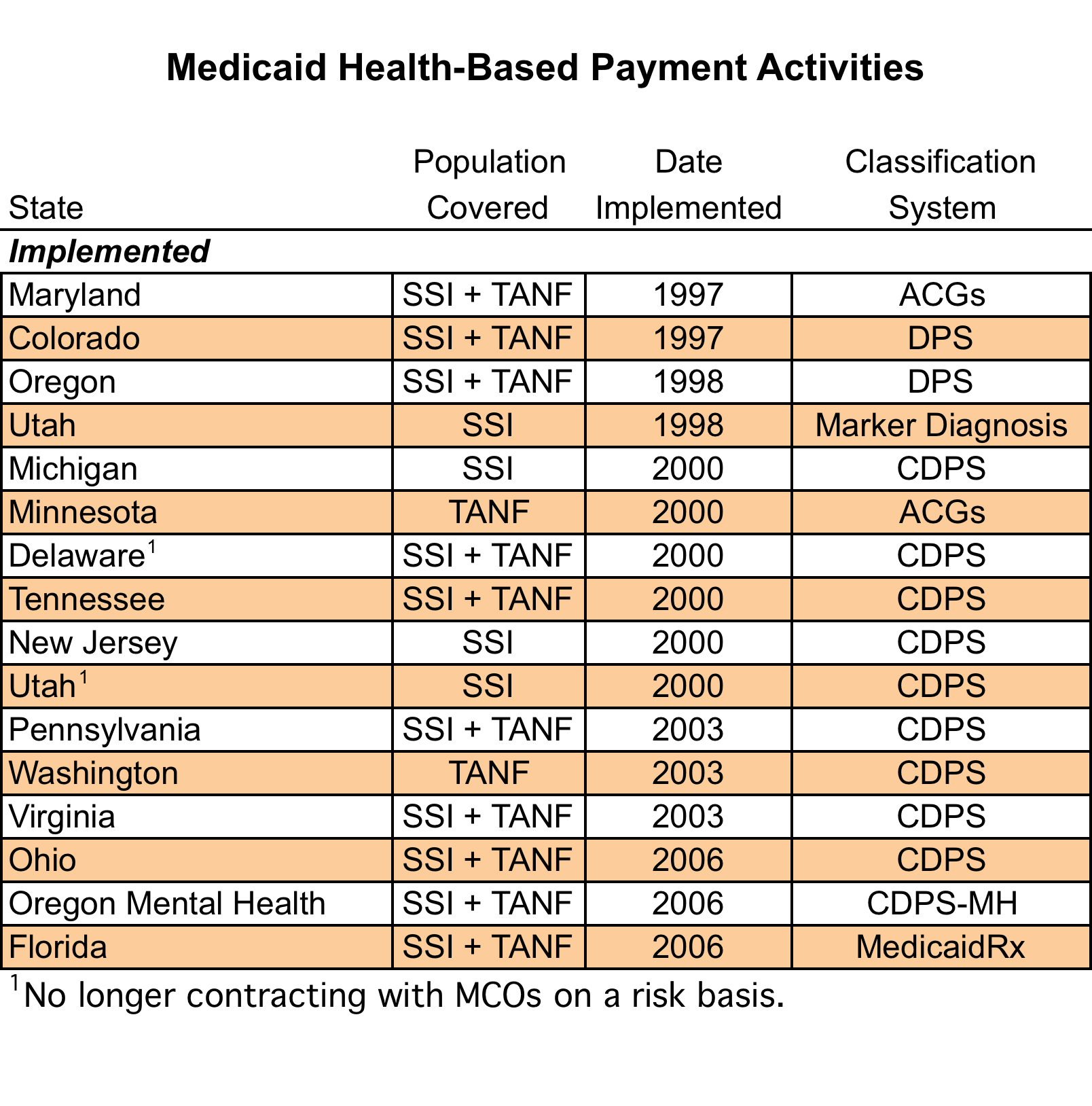
11 Risk Adjustment in Medicaid and Medicare Risk adjustment systems developed in academia in the 1990s as a method to adjust capitated payments First models targeted Medicare (DCGs, ACGs) Medicare was an early promoter but a late adaptor Medicaid risk adjustment begins in 1997 (ACGs, DPS) Medicare Part C risk adjustment in 2004 (mod-hcc) Medicare Part D risk adjustment in 2006 (mod-hcc)
12
13 Risk Adjustment in Health Care Reform State health insurance exchanges will use risk adjustment to adjust payments to health plans that are participating in the exchange Medicaid programs may use risk adjustment to adjust capitation payment to managed care plans that provide coverage for their expansion populations
14 Risk Adjustment and Long Term Care Dual eligible pilot programs are diving and interest in risk adjustment models that span Medicare and Medicaid, and home and community based and institutional long term care These models will need to include additional measures predictive of HCB and LTC services Functional and cognitive limitations, social support Additional data from clinician and self assessments WI uses web based assessment
15 Risk Adjustment and SES Substantial literature and growing interest in social determinants of health Income, education, race/ethnicity, language proficiency, epigenetics SES may affect risk is complex ways Effect of SES on health may be different than the effect of SES on risk (i.e. use of services) Latinos and Asians with LEP are more likely to access outpatient vs. inpatient or emergency MH services LEP is associated with higher medication adherence among Latinos LEP is associated with lower medication adherence among Asians
16 Mechanics of Risk Adjustment Using CDPS
17 Chronic Illness and Disability Payment System CDPS is a risk adjustment system for Medicaid that maps diagnoses to 58 CDPS categories corresponding to major body systems or chronic diseases CDPS is similar to models used for Medicare (ie HCCs), but places a greater emphasis on less common, but costly chronic conditions that are more prevalent among disabled Medicaid beneficiaries CDPS models for disabled, TANF Adults, and TANF Children
18 Major CDPS Categories Cardiovascular, Psychiatric, Skeletal, Central Nervous System, Pulmonary, Gastrointestinal, Diabetes, Skin, Renal, Substance Abuse, Cancer, Developmental Disability, Genital, Metabolic, Pregnancy, Eye, Cerebrovascular, AIDS/Infectious Disease, Hematological
19 CDPS Hierarchies CDPS categories are hierarchical within major categories For example, in the major category cardiovascular: CARVH includes 7 diagnoses, eg heart transplant CARM includes 53 diagnoses, eg heart failure CARL includes 314 diagnoses, eg AMI CAREL includes 35 diagnoses, eg hypertension
20 Hierarchies and Comorbidities Weights are additive across major categories Within major categories, only the most severe (i.e. expensive) diagnosis counts This allows an accounting of comorbidities, but reduces the incentive for upcoding of diagnoses For example, if a beneficiary has both diabetes and depression, both count towards the risk score However, if a beneficiary has heart failure and hypertension, only heart failure counts towards the CDPS risk score
21 Estimating CDPS Weights National Medicaid claims data, Linear regression is used to regress expenditures on the vector of CDPS categories Weights are resulting regression coefficients, also the marginal expenditure effects for each category For example, when expenditure = Y (mean=1.0): Y = Intercept + b1*cdps1 + b2*cdps2 + + b58*cdps58 CDPSi are indicator variables (0,1 s) and bi are the estimated coefficients
22 CDPS Weights Cardiovascular, very high Cardiovascular, medium Cardiovascular, low Cardiovascular, extra low Psychiatric, high Psychiatric, medium Psychiatric, medium low Psychiatric, low 0.206
23 Calculating CDPS Scores Multiply the CDPS category vector by the weight vector (and sum the factors) Include the intercept and age and gender factors A 50 year old female with type 2 diabetes and hypertension has a risk factor of If the same female also had bipolar disorder, her risk factor would be
24 Calculating Payments for Health Plans Average the risk scores of all plan enrollees with eligibility in the observation period Calculate weighted average of all plans; normalize to 1.0 to assure budget neutrality If FFS is included as a plan -- HBP is not budget neutral in those states Pay each plan it s normalized risk score multiplied by the base rate (eg: $800 PMPM for disabled)
25 Actuarial Adjustments Partial capitation Partial risk adjustment Risk corridors Reinsurance Carve-outs (with weight options) Behavioral health carve-outs Pregnancy / delivery carve-outs Pharmacy carve-outs
26 Medicaid RX Model Pharmaceutical based model uses National Drug Codes (NDC) to assign 45 therapeutic categories Developed as an alternative to diagnosis based models when the health plan encounter data is low quality Pharmacotherapy vs clinical diagnosis Combined CDPS + Rx model using 15 MRX categories that were considered to be the least affected by practice patterns
27 Results of Risk Adjustment In CO, for PWDs, a University and Children s Hospital has a case-mix of 1.35 In OR, a plan that uses Oregon Health Sciences University has a case-mix of 1.13 In MD and NJ, implementation errors created major problems requiring retroactive adjustments; problems have been corrected and the states are moving forward
28 Results of Risk Adjustment Risk adjustment appears to get more money to plans that serve sicker people Equitable data is key technical challenge Not much evidence yet that plans or providers respond by developing systems of care to attract sicker people Risk adjustment models are also widely used to profile illness burden and to identify beneficiaries with multiple chronic conditions for complex case management
29 Risk Adjustment and Primary Care
30 Risk Adjusted Primary Care Risk adjustment models have been primarily used to adjust premium payments Acute care (sometimes with carve-outs) Pharmacy coverage (i.e. Part D) Risk adjustment models have not been widely used to pay for primary care Primary care is more likely to be integrated (e.g. Kaiser) or paid by fee-for-service There is a growing interest in capitated payment for primary care Either fully capitated (and risk adjusted) or partial capitated with FFS component
31 Risk Adjustment and Scope of Primary Care Services It can be a challenge to identify the appropriate scope of services In Medicare, this might be part B In Medicaid, there is wide use of other providers and other services Under health care reform, the appropriate scope of services may be changing Medical health care homes, care management, electronic health records, community integration
32 Data Available to Primary Care Providers May be limited to services provided in primary care / primary care clinic Missing inpatient diagnoses, diagnoses from other providers and other services, pharmacy data Clinical profiles may be incomplete without these data Might be possible to obtain these data from the health plan.
33 Care Coordination and Cost Offsets It is often difficult to coordinate care across primary care and other providers such as hospitals and specialists Improved care coordination and health promotion activities may result in reduced costs in other sectors This might justify a rebalancing of payments to primary care and other providers
34 Diabetes Management Diabetes case management and self management training was provided to newly insurance adults Participants were compared to non-particpants Improved clinical risk factors (eg A1c, BP, lipids) Increased costs related to care coordination and pharmaceuticals Reduced costs for inpatient and emergency services Cost neutral, quality improvement
35 Opportunities for Community Health Centers to Demonstrate Value Added
36 Opportunity Frameworks Chronic Care Model Accountable Care Organizations Primary Care Medical Homes Integration of Physical and Mental Health and Substance Abuse Services Disease Care Management Complex Chronic Disease Case Management
37 Common Elements Team based care Reorientation from the physician centric model Collaboration and communication is essential Expanded workforce Care management Nurses focused on complex chronic conditions Social workers focused on mental health, care transitions, social issues Pharmacists focused on complex pharmacotherapy Peers focused on education and self management training IT needed to support the above efforts
38 Conclusions Risk adjustment does not currently impact primary care directly, although there may be indirect effects operating through the health plans Opportunities and risk in capitated primary care Multiple avenues for community health centers to demonstrate value through improved care coordination and improved quality of care Also an opportunity to expand the scope of primary care / clinic services
Medicare- Medicaid Enrollee State Profile
 Medicare- Medicaid Enrollee State Profile Montana Centers for Medicare & Medicaid Services Introduction... 1 At a Glance... 1 Eligibility... 2 Demographics... 3 Chronic Conditions... 4 Utilization... 6
Medicare- Medicaid Enrollee State Profile Montana Centers for Medicare & Medicaid Services Introduction... 1 At a Glance... 1 Eligibility... 2 Demographics... 3 Chronic Conditions... 4 Utilization... 6
Medicare- Medicaid Enrollee State Profile
 Medicare- Medicaid Enrollee State Profile Centers for Medicare & Medicaid Services Introduction... 1 At a Glance... 1 Eligibility... 2 Demographics... 3 Chronic Conditions... 4 Utilization... 6 Spending...
Medicare- Medicaid Enrollee State Profile Centers for Medicare & Medicaid Services Introduction... 1 At a Glance... 1 Eligibility... 2 Demographics... 3 Chronic Conditions... 4 Utilization... 6 Spending...
Risk Adjustment in the Medicare ACO Shared Savings Program
 Risk Adjustment in the Medicare ACO Shared Savings Program Presented by: John Kautter Presented at: AcademyHealth Conference Baltimore, MD June 23-25, 2013 RTI International is a trade name of Research
Risk Adjustment in the Medicare ACO Shared Savings Program Presented by: John Kautter Presented at: AcademyHealth Conference Baltimore, MD June 23-25, 2013 RTI International is a trade name of Research
Selection of Medicaid Beneficiaries for Chronic Care Management Programs: Overview and Uses of Predictive Modeling
 APRIL 2009 Issue Brief Selection of Medicaid Beneficiaries for Chronic Care Management Programs: Overview and Uses of Predictive Modeling Abstract Effective use of care management techniques may help Medicaid
APRIL 2009 Issue Brief Selection of Medicaid Beneficiaries for Chronic Care Management Programs: Overview and Uses of Predictive Modeling Abstract Effective use of care management techniques may help Medicaid
Introduction to Risk Adjustment Programs for Medicare Advantage and the Affordable Care Act (Commercial Health Insurance Exchange)
") Introduction to Risk Adjustment Programs for Medicare Advantage and the Affordable Care Act (Commercial Health Insurance Exchange) November, 2014 An independent licensee of the Blue Cross and Blue Shield
Introduction to Risk Adjustment Programs for Medicare Advantage and the Affordable Care Act (Commercial Health Insurance Exchange) November, 2014 An independent licensee of the Blue Cross and Blue Shield
REIMBURSEMENT, CAPITATION AND RISK ADJUSTMENT
 REIMBURSEMENT, CAPITATION AND RISK ADJUSTMENT HIV/AIDS BUREAU HEALTH RESOURCES AND SERVICES ADMINISTRATION HRSA HIV/AIDS Bureau 1 REIMBURSEMENT METHODOLOGIES Retrospective Cost Based Prospective TYPES
REIMBURSEMENT, CAPITATION AND RISK ADJUSTMENT HIV/AIDS BUREAU HEALTH RESOURCES AND SERVICES ADMINISTRATION HRSA HIV/AIDS Bureau 1 REIMBURSEMENT METHODOLOGIES Retrospective Cost Based Prospective TYPES
Physical and Mental Health Condition Prevalence and Comorbidity among Fee-for-Service Medicare- Medicaid Enrollees
 Physical and Mental Health Condition Prevalence and Comorbidity among Fee-for-Service Medicare- Medicaid Enrollees Centers for Medicare & Medicaid Services September, 2014 i Executive Summary Introduction
Physical and Mental Health Condition Prevalence and Comorbidity among Fee-for-Service Medicare- Medicaid Enrollees Centers for Medicare & Medicaid Services September, 2014 i Executive Summary Introduction
Risk Adjustment 101: Health-Based Payment Adjustment Methodology
 Risk Adjustment 101: Health-Based Payment Adjustment Methodology Presented by: Kim Browning, CHC, PMP, CHRS Executive Vice President, Cognisight, LLC Tara Swenson Attorney, Mintz, Levin, Cohn, Ferris,
Risk Adjustment 101: Health-Based Payment Adjustment Methodology Presented by: Kim Browning, CHC, PMP, CHRS Executive Vice President, Cognisight, LLC Tara Swenson Attorney, Mintz, Levin, Cohn, Ferris,
Improving risk adjustment in the Medicare program
 C h a p t e r2 Improving risk adjustment in the Medicare program C H A P T E R 2 Improving risk adjustment in the Medicare program Chapter summary In this chapter Health plans that participate in the
C h a p t e r2 Improving risk adjustment in the Medicare program C H A P T E R 2 Improving risk adjustment in the Medicare program Chapter summary In this chapter Health plans that participate in the
Medicare- Medicaid Enrollee State Profile
 Medicare- Medicaid Enrollee State Profile The National Summary Centers for Medicare & Medicaid Services Introduction... 1 Data Source and General Notes... 2 Types and Ages of Medicare-Medicaid Enrollees...
Medicare- Medicaid Enrollee State Profile The National Summary Centers for Medicare & Medicaid Services Introduction... 1 Data Source and General Notes... 2 Types and Ages of Medicare-Medicaid Enrollees...
Analysis of Care Coordination Outcomes /
 Analysis of Care Coordination Outcomes / A Comparison of the Mercy Care Plan Population to Nationwide Dual-Eligible Medicare Beneficiaries July 2012 Prepared by: Varnee Murugan Ed Drozd Kevin Dietz Aetna
Analysis of Care Coordination Outcomes / A Comparison of the Mercy Care Plan Population to Nationwide Dual-Eligible Medicare Beneficiaries July 2012 Prepared by: Varnee Murugan Ed Drozd Kevin Dietz Aetna
Economic Impact of Integrated Medical-Behavioral Healthcare
 Economic Impact of Integrated Medical-Behavioral Healthcare Implications for Psychiatry Prepared for: American Psychiatric Association Prepared by: Milliman, Inc. Stephen P. Melek, FSA, MAAA Douglas T.
Economic Impact of Integrated Medical-Behavioral Healthcare Implications for Psychiatry Prepared for: American Psychiatric Association Prepared by: Milliman, Inc. Stephen P. Melek, FSA, MAAA Douglas T.
Florida Medicaid: Mental Health and Substance Abuse Services
 Florida Medicaid: Mental Health and Substance Abuse Services Beth Kidder Assistant Deputy Secretary for Medicaid Operations Agency for Health Care Administration House Children, Families, and Seniors Subcommittee
Florida Medicaid: Mental Health and Substance Abuse Services Beth Kidder Assistant Deputy Secretary for Medicaid Operations Agency for Health Care Administration House Children, Families, and Seniors Subcommittee
8/14/2012 California Dual Demonstration DRAFT Quality Metrics
 Stakeholder feedback is requested on the following: 1) metrics 69 through 94; and 2) withhold measures for years 1, 2, and 3. Steward/ 1 Antidepressant medication management Percentage of members 18 years
Stakeholder feedback is requested on the following: 1) metrics 69 through 94; and 2) withhold measures for years 1, 2, and 3. Steward/ 1 Antidepressant medication management Percentage of members 18 years
Gateway Health Medicare Assured RubySM (HMO SNP) $6,700 out-of-pocket limit for Medicare-covered services. No No No No. Days 1-6: $0 or $225 copay per
 $6,700 out-of-pocket limit for Medicare-covered services. No No No No. Days 1-6: $0 or $225 copay per") Assured RubySM (HMO Premium $0 monthly plan $0 - $33.90 monthly plan Assured GoldSM (HMO $12.40 - $46.30 monthly plan $43.90 - $77.80 monthly plan In Network Maximum Out-of-Pocket $3,400 out-of-pocket
Assured RubySM (HMO Premium $0 monthly plan $0 - $33.90 monthly plan Assured GoldSM (HMO $12.40 - $46.30 monthly plan $43.90 - $77.80 monthly plan In Network Maximum Out-of-Pocket $3,400 out-of-pocket
MaineCare Value Based Purchasing Initiative
 MaineCare Value Based Purchasing Initiative The Accountable Communities Strategy Jim Leonard, Deputy Director, MaineCare Peter Kraut, Acting Accountable Communities Program Manager Why Value-Based Purchasing
MaineCare Value Based Purchasing Initiative The Accountable Communities Strategy Jim Leonard, Deputy Director, MaineCare Peter Kraut, Acting Accountable Communities Program Manager Why Value-Based Purchasing
Article from: Health Watch. January 2008 No. 57
 Article from: Health Watch January 2008 No. 57 Risk Adjustment in State Medicaid Programs by Ross Winkelman and Rob Damler Rob Damler is a principal and consulting Actuary at Milliman Inc in Indianapolis,
Article from: Health Watch January 2008 No. 57 Risk Adjustment in State Medicaid Programs by Ross Winkelman and Rob Damler Rob Damler is a principal and consulting Actuary at Milliman Inc in Indianapolis,
Brief Research Report: Fountain House and Use of Healthcare Resources
 ! Brief Research Report: Fountain House and Use of Healthcare Resources Zachary Grinspan, MD MS Department of Healthcare Policy and Research Weill Cornell Medical College, New York, NY June 1, 2015 Fountain
! Brief Research Report: Fountain House and Use of Healthcare Resources Zachary Grinspan, MD MS Department of Healthcare Policy and Research Weill Cornell Medical College, New York, NY June 1, 2015 Fountain
Department of Health Services. Behavioral Health Integrated Care. Health Home Certification Application
 Department of Health Services Behavioral Health Integrated Care Health Home Certification Application (Langlade, Lincoln, and Marathon Counties) December 18, 2013 1 Behavioral Health Integrated Care Health
Department of Health Services Behavioral Health Integrated Care Health Home Certification Application (Langlade, Lincoln, and Marathon Counties) December 18, 2013 1 Behavioral Health Integrated Care Health
2015 Orange County HICAP Medicare Advantage Special Needs Plans Comparison Chart
 Brand New Day Brand New Day Brand New Day Brand New Day Bridges Drug Savings Bridges Extra Care Harmony Healthy Heart Drug Savings dementia. dementia. chronic and disabling mental health conditions. chronic
Brand New Day Brand New Day Brand New Day Brand New Day Bridges Drug Savings Bridges Extra Care Harmony Healthy Heart Drug Savings dementia. dementia. chronic and disabling mental health conditions. chronic
ATTACHMENT B Care Management Organization (CMO) Quality Incentive Payment Methodology
 Quality Incentive Payment Methodology") This attachment describes the CMO program period cost reduction guarantees as follows: 1. Fees-at-Risk; 2. Reconciliation Methodology and Holdback Calculation; 3. Operational and Reconciliation Data Requirements;
This attachment describes the CMO program period cost reduction guarantees as follows: 1. Fees-at-Risk; 2. Reconciliation Methodology and Holdback Calculation; 3. Operational and Reconciliation Data Requirements;
Care needs for dual-eligible beneficiaries
 C h a p t e r6 Care needs for dual-eligible beneficiaries C H A P T E R 6 Care needs for dual-eligible beneficiaries Chapter summary In this chapter Dual-eligible beneficiaries are eligible for both Medicare
C h a p t e r6 Care needs for dual-eligible beneficiaries C H A P T E R 6 Care needs for dual-eligible beneficiaries Chapter summary In this chapter Dual-eligible beneficiaries are eligible for both Medicare
kaiser medicaid commission on and the uninsured May 2009 Community Care of North Carolina: Putting Health Reform Ideas into Practice in Medicaid
 P O L I C Y B R I E F kaiser commission on medicaid SUMMARY and the uninsured Community Care of North Carolina: Putting Health Reform Ideas into Practice in Medicaid May 2009 Why is Community Care of North
P O L I C Y B R I E F kaiser commission on medicaid SUMMARY and the uninsured Community Care of North Carolina: Putting Health Reform Ideas into Practice in Medicaid May 2009 Why is Community Care of North
Accountable Care and Value Based Payments 101: Government Programs Update
 1 Accountable Care and Value Based Payments 101: Government Programs Update June 24 th, 2014 Dave Neiman, FSA, MAAA Senior Consulting Actuary [email protected] (720) 226-9806 2 Caveats Opinions expressed
1 Accountable Care and Value Based Payments 101: Government Programs Update June 24 th, 2014 Dave Neiman, FSA, MAAA Senior Consulting Actuary [email protected] (720) 226-9806 2 Caveats Opinions expressed
Enhancing Medicaid Primary Care Case Management to Improve Care Management and Accountability
 Enhancing Medicaid Primary Care Case Management to Improve Care Management and Accountability Prepared by James M. Verdier Mathematica Policy Research, Inc. for the Fourth National Medicaid Congress Washington,
Enhancing Medicaid Primary Care Case Management to Improve Care Management and Accountability Prepared by James M. Verdier Mathematica Policy Research, Inc. for the Fourth National Medicaid Congress Washington,
INSIGHT on the Issues
 INSIGHT on the Issues AARP Public Policy Institute Medicare Beneficiaries Out-of-Pocket for Health Care Claire Noel-Miller, PhD AARP Public Policy Institute Medicare beneficiaries spent a median of $3,138
INSIGHT on the Issues AARP Public Policy Institute Medicare Beneficiaries Out-of-Pocket for Health Care Claire Noel-Miller, PhD AARP Public Policy Institute Medicare beneficiaries spent a median of $3,138
From Mental Health and Substance Abuse to Behavioral Health Services: Opportunities and Challenges with the Affordable Care Act.
 From Mental Health and Substance Abuse to Behavioral Health Services: Opportunities and Challenges with the Affordable Care Act. Ron Manderscheid, Ph.D. Exec Dir, National Association of County Behavioral
From Mental Health and Substance Abuse to Behavioral Health Services: Opportunities and Challenges with the Affordable Care Act. Ron Manderscheid, Ph.D. Exec Dir, National Association of County Behavioral
Risk Adjustment Medicare and Commercial
 Risk Adjustment Medicare and Commercial Transform your thinking about documentation and coding 900-1169-0715 Introduction In a time of continual regulatory reform and the evolution of payer/provider reimbursement
Risk Adjustment Medicare and Commercial Transform your thinking about documentation and coding 900-1169-0715 Introduction In a time of continual regulatory reform and the evolution of payer/provider reimbursement
Medicare Beneficiaries Out-of-Pocket Spending for Health Care
 Insight on the Issues OCTOBER 2015 Beneficiaries Out-of-Pocket Spending for Health Care Claire Noel-Miller, MPA, PhD AARP Public Policy Institute Half of all beneficiaries in the fee-for-service program
Insight on the Issues OCTOBER 2015 Beneficiaries Out-of-Pocket Spending for Health Care Claire Noel-Miller, MPA, PhD AARP Public Policy Institute Half of all beneficiaries in the fee-for-service program
Achieving Quality and Value in Chronic Care Management
 The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
Shaping our future: a call to action to tackle the diabetes epidemic and reduce its economic impact
 Shaping our future: a call to action to tackle the diabetes epidemic and reduce its economic impact Task Force for the National Conference on Diabetes: The Task Force is comprised of Taking Control of
Shaping our future: a call to action to tackle the diabetes epidemic and reduce its economic impact Task Force for the National Conference on Diabetes: The Task Force is comprised of Taking Control of
Maryland Medicaid Program. Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 15, 2012
 Maryland Medicaid Program Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 15, 2012 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance or MA. MA is a joint
Maryland Medicaid Program Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 15, 2012 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance or MA. MA is a joint
Overview of Health Risk Adjustment in the U.S. John Bertko, F.S.A., M.A.A.A.
 Overview of Health Risk Adjustment in the U.S. John Bertko, F.S.A., M.A.A.A. VP and Chief Actuary, Humana Inc. IAA, Cancun, Mexico March 18, 2002 Health Risk Adjustment in the U.S.: An Evolving Tool Overview
Overview of Health Risk Adjustment in the U.S. John Bertko, F.S.A., M.A.A.A. VP and Chief Actuary, Humana Inc. IAA, Cancun, Mexico March 18, 2002 Health Risk Adjustment in the U.S.: An Evolving Tool Overview
The Collaborative Models of Mental Health Care for Older Iowans. Model Administration. Collaborative Models of Mental Health Care for Older Iowans 97
 6 The Collaborative Models of Mental Health Care for Older Iowans Model Administration Collaborative Models of Mental Health Care for Older Iowans 97 Collaborative Models of Mental Health Care for Older
6 The Collaborative Models of Mental Health Care for Older Iowans Model Administration Collaborative Models of Mental Health Care for Older Iowans 97 Collaborative Models of Mental Health Care for Older
Summary of the Major Provisions in the Patient Protection and Affordable Health Care Act
 Summary of the Major Provisions in the Patient Protection and Affordable Care Act Updated 10/22/10 On March 23, 2010, President Barack Obama signed into law comprehensive health care reform legislation,
Summary of the Major Provisions in the Patient Protection and Affordable Care Act Updated 10/22/10 On March 23, 2010, President Barack Obama signed into law comprehensive health care reform legislation,
The role of t he Depart ment of Veterans Affairs (VA) as
 as") The VA Health Care System: An Unrecognized National Safety Net Veterans who use the VA health care system have a higher level of illness than the general population, and 60 percent have no private or Medigap
The VA Health Care System: An Unrecognized National Safety Net Veterans who use the VA health care system have a higher level of illness than the general population, and 60 percent have no private or Medigap
Home Care Association of Washington Conference. MaryAnne Lindeblad, State Medicaid Director Washington Health Care Authority
 Home Care Association of Washington Conference MaryAnne Lindeblad, State Medicaid Director Washington Health Care Authority April 25, 2013 Overview Overview of Health Care Authority Public Employees Benefits
Home Care Association of Washington Conference MaryAnne Lindeblad, State Medicaid Director Washington Health Care Authority April 25, 2013 Overview Overview of Health Care Authority Public Employees Benefits
How are Health Home Services Provided to the Medically Needy?
 Id: NEW YORK State: New York Health Home Services Effective Date- January 1, 2012 SPA includes both Categorically Needy and Medically Needy Beneficiaries- check box 3.1 - A: Categorically Needy View Attachment
Id: NEW YORK State: New York Health Home Services Effective Date- January 1, 2012 SPA includes both Categorically Needy and Medically Needy Beneficiaries- check box 3.1 - A: Categorically Needy View Attachment
MedStar Family Choice (MFC) Case Management Program. Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015
 Case Management Program. Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015") MedStar Family Choice (MFC) Case Management Program Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015 Case Management Program Presentation Overview CM Programs Disease Management Complex
MedStar Family Choice (MFC) Case Management Program Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015 Case Management Program Presentation Overview CM Programs Disease Management Complex
MEDICARE SUPPLEMENTAL COVERAGE. Medigap and Other Factors Are Associated with Higher Estimated Health Care Expenditures
 United States Government Accountability Office Report to the Ranking Member, Committee on Finance, U.S. Senate September 2013 MEDICARE SUPPLEMENTAL COVERAGE Medigap and Other Factors Are Associated with
United States Government Accountability Office Report to the Ranking Member, Committee on Finance, U.S. Senate September 2013 MEDICARE SUPPLEMENTAL COVERAGE Medigap and Other Factors Are Associated with
The Maryland Public Behavioral Health System
 The Maryland Public Behavioral Health System Arleen Rogan, Ph.D. Division Director, Integrated Health Services Family Services, Inc. [email protected] Behavioral Health includes: Mental health conditions
The Maryland Public Behavioral Health System Arleen Rogan, Ph.D. Division Director, Integrated Health Services Family Services, Inc. [email protected] Behavioral Health includes: Mental health conditions
Behavioral Health Policy in Illinois: Major Policy Initiatives in 2013 and Beyond
 : Major Policy Initiatives in 2013 and Beyond P R E S E N T A T I O N T O T H E M E D I C A I D A D V I S O R Y C O M M I T T E E N O V E M B E R 7, 2 0 1 3 L O R R I E R I C K M A N J O N E S, P H. D.
: Major Policy Initiatives in 2013 and Beyond P R E S E N T A T I O N T O T H E M E D I C A I D A D V I S O R Y C O M M I T T E E N O V E M B E R 7, 2 0 1 3 L O R R I E R I C K M A N J O N E S, P H. D.
Maryland Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland As of July 2003, 638,662 people were covered under Maryland's Medicaid/SCHIP programs. There were 525,080 enrolled in the Medicaid
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland As of July 2003, 638,662 people were covered under Maryland's Medicaid/SCHIP programs. There were 525,080 enrolled in the Medicaid
See page 331 of HEDIS 2013 Tech Specs Vol 2. HEDIS specs apply to plans. RARE applies to hospitals. Plan All-Cause Readmissions (PCR) *++
 *++") Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Disparities in Realized Access: Patterns of Health Services Utilization by Insurance Status among Children with Asthma in Puerto Rico
 Disparities in Realized Access: Patterns of Health Services Utilization by Insurance Status among Children with Asthma in Puerto Rico Ruth Ríos-Motta, PhD, José A. Capriles-Quirós, MD, MPH, MHSA, Mario
Disparities in Realized Access: Patterns of Health Services Utilization by Insurance Status among Children with Asthma in Puerto Rico Ruth Ríos-Motta, PhD, José A. Capriles-Quirós, MD, MPH, MHSA, Mario
Improving Service Delivery Through Administrative Data Integration and Analytics
 Improving Service Delivery Through Administrative Data Integration and Analytics Getty Images David Mancuso, PhD October 2, 2015 1 Analytics in the Social and Health Service Environment Program costs are
Improving Service Delivery Through Administrative Data Integration and Analytics Getty Images David Mancuso, PhD October 2, 2015 1 Analytics in the Social and Health Service Environment Program costs are
 Prescription drugs are a critical component of health care. Because of the role of drugs in treating conditions, it is important that Medicare ensures that its beneficiaries have access to appropriate
Prescription drugs are a critical component of health care. Because of the role of drugs in treating conditions, it is important that Medicare ensures that its beneficiaries have access to appropriate
WHAT HEALTHCARE PROVIDERS SHOULD KNOW ABOUT THE PROPOSED MEDICAID MANAGED CARE REGULATIONS RELEASED LAST WEEK
 WHAT HEALTHCARE PROVIDERS SHOULD KNOW ABOUT THE PROPOSED MEDICAID MANAGED CARE REGULATIONS RELEASED LAST WEEK By Mark E. Reagan, Felicia Y Sze, Joseph R. LaMagna, Nina Adatia Marsden and Yanyan Zhou Basics:
WHAT HEALTHCARE PROVIDERS SHOULD KNOW ABOUT THE PROPOSED MEDICAID MANAGED CARE REGULATIONS RELEASED LAST WEEK By Mark E. Reagan, Felicia Y Sze, Joseph R. LaMagna, Nina Adatia Marsden and Yanyan Zhou Basics:
Maryland Medicaid Program: An Overview. Stacey Davis Planning Administration Department of Health and Mental Hygiene May 22, 2007
 Maryland Medicaid Program: An Overview Stacey Davis Planning Administration Department of Health and Mental Hygiene May 22, 2007 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance
Maryland Medicaid Program: An Overview Stacey Davis Planning Administration Department of Health and Mental Hygiene May 22, 2007 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance
Medicare Economics. Part A (Hospital Insurance) Funding
 Funding") Medicare Economics Medicare expenditures are a substantial part of the federal budget $556 billion, or 15 percent in 2012. They also comprise 3.7 percent of the country s gross domestic product (GDP),
Medicare Economics Medicare expenditures are a substantial part of the federal budget $556 billion, or 15 percent in 2012. They also comprise 3.7 percent of the country s gross domestic product (GDP),
GAO MEDICARE ADVANTAGE. Relationship between Benefit Package Designs and Plans Average Beneficiary Health Status. Report to Congressional Requesters
 GAO United States Government Accountability Office Report to Congressional Requesters April 2010 MEDICARE ADVANTAGE Relationship between Benefit Package Designs and Plans Average Beneficiary Health Status
GAO United States Government Accountability Office Report to Congressional Requesters April 2010 MEDICARE ADVANTAGE Relationship between Benefit Package Designs and Plans Average Beneficiary Health Status
5/3/2016. Value-Based Purchasing in Minnesota Medicaid AGENDA
 Value-Based Purchasing in Minnesota Medicaid Gretchen Ulbee Manager, Special Needs Purchasing, Health Care Administration Minnesota Department of Human Services May 11, 2016 AGENDA What is Value-Based
Value-Based Purchasing in Minnesota Medicaid Gretchen Ulbee Manager, Special Needs Purchasing, Health Care Administration Minnesota Department of Human Services May 11, 2016 AGENDA What is Value-Based
Oregon Statewide Performance Improvement Project: Diabetes Monitoring for People with Diabetes and Schizophrenia or Bipolar Disorder
 Oregon Statewide Performance Improvement Project: Diabetes Monitoring for People with Diabetes and Schizophrenia or Bipolar Disorder November 14, 2013 Prepared by: Acumentra Health 1. Study Topic This
Oregon Statewide Performance Improvement Project: Diabetes Monitoring for People with Diabetes and Schizophrenia or Bipolar Disorder November 14, 2013 Prepared by: Acumentra Health 1. Study Topic This
The Centers for Medicare & Medicaid Services (CMS) strives to make information available to all. Nevertheless, portions of our files including
 strives to make information available to all. Nevertheless, portions of our files including") The Centers for Medicare & Medicaid Services (CMS) strives to make information available to all. Nevertheless, portions of our files including charts, tables, and graphics may be difficult to read using
The Centers for Medicare & Medicaid Services (CMS) strives to make information available to all. Nevertheless, portions of our files including charts, tables, and graphics may be difficult to read using
How Health Reform Will Help Children with Mental Health Needs
 How Health Reform Will Help Children with Mental Health Needs The new health care reform law, called the Affordable Care Act (or ACA), will give children who have mental health needs better access to the
How Health Reform Will Help Children with Mental Health Needs The new health care reform law, called the Affordable Care Act (or ACA), will give children who have mental health needs better access to the
Household health care spending: comparing the Consumer Expenditure Survey and the National Health Expenditure Accounts Ann C.
 Household health care spending: comparing the Consumer Expenditure Survey and the National Health Expenditure Accounts Ann C. Foster Health care spending data produced by the Federal Government include
Household health care spending: comparing the Consumer Expenditure Survey and the National Health Expenditure Accounts Ann C. Foster Health care spending data produced by the Federal Government include
HCCs and Star-Ratings: An IPA s Successful Approach to Revenue Integrity. Nancy Hirschl, CCS Victoria McKemy, MHA James Taylor, MD, CPC
 HCCs and Star-Ratings: An IPA s Successful Approach to Revenue Integrity Nancy Hirschl, CCS Victoria McKemy, MHA James Taylor, MD, CPC 1 Introduction Agenda HCCs (Hierarchical Condition Categories) Diagnosis
HCCs and Star-Ratings: An IPA s Successful Approach to Revenue Integrity Nancy Hirschl, CCS Victoria McKemy, MHA James Taylor, MD, CPC 1 Introduction Agenda HCCs (Hierarchical Condition Categories) Diagnosis
Dual RFI Response Summary
 Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Welcome to Magellan Complete Care
 Magellan Complete Care of Florida Provider Newsletter Welcome to Magellan Complete Care On behalf of Magellan Complete Care of Florida, thank you for your continued support and collaboration. As the only
Magellan Complete Care of Florida Provider Newsletter Welcome to Magellan Complete Care On behalf of Magellan Complete Care of Florida, thank you for your continued support and collaboration. As the only
 1115 Medicaid Waiver Programs Section1115 of the Social Security Act allows CMS the authority to approve state demonstration projects that improve care, increase efficiency, and reduce costs related to
1115 Medicaid Waiver Programs Section1115 of the Social Security Act allows CMS the authority to approve state demonstration projects that improve care, increase efficiency, and reduce costs related to
Part D payment system
 Part D payment system paymentbasics Revised: October 204 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 70 Washington, DC 2000 ph: 202-220-3700 fax: 202-220-3759
Part D payment system paymentbasics Revised: October 204 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 70 Washington, DC 2000 ph: 202-220-3700 fax: 202-220-3759
IMPACT: An Evidence-based Approach to Integrated Depression Care Beth Israel Medical Center New York, NY. Day One: June 8, 2011
 IMPACT: An Evidence-based Approach to Integrated Depression Care Beth Israel Medical Center New York, NY 8:00 Registration & Continental Breakfast 8:30 Welcome & Introductions Day One: June 8, 2011 8:45
IMPACT: An Evidence-based Approach to Integrated Depression Care Beth Israel Medical Center New York, NY 8:00 Registration & Continental Breakfast 8:30 Welcome & Introductions Day One: June 8, 2011 8:45
Quality Improvement and Payment Reform
 Quality Improvement and Payment Reform Mark McClellan, MD, PhD Senior Fellow and Director, Initiative on Value and Innovation in Health Care Brookings Institution Mark McClellan. All rights reserved. No
Quality Improvement and Payment Reform Mark McClellan, MD, PhD Senior Fellow and Director, Initiative on Value and Innovation in Health Care Brookings Institution Mark McClellan. All rights reserved. No
Risk Adjustment Models for Medicare Part D Capitation Payments Modeling
 Risk Adjustment Models for Medicare Part D Capitation Payments Modeling John Kautter Melvin J. Ingber Gregory C. Pope Sara Freeman RTI International AcademyHealth 2011 RTI International is a trade name
Risk Adjustment Models for Medicare Part D Capitation Payments Modeling John Kautter Melvin J. Ingber Gregory C. Pope Sara Freeman RTI International AcademyHealth 2011 RTI International is a trade name
FEHB Program Carrier Letter All FEHB Carriers
 FEHB Program Carrier Letter All FEHB Carriers U.S. Office of Personnel Management Healthcare and Insurance Letter No. 2016-03 Date: February 26, 2016 Fee-for-service [3] Experience-rated HMO [3] Community-rated
FEHB Program Carrier Letter All FEHB Carriers U.S. Office of Personnel Management Healthcare and Insurance Letter No. 2016-03 Date: February 26, 2016 Fee-for-service [3] Experience-rated HMO [3] Community-rated
c. determine the factors that will facilitate/limit physician utilization of pharmacists for medication management services.
 Consumer, Physician, and Payer Perspectives on Primary Care Medication Management Services with a Shared Resource Pharmacists Network Marie Smith, PharmD and Michlle Breland, PhD University of Connecticut,
Consumer, Physician, and Payer Perspectives on Primary Care Medication Management Services with a Shared Resource Pharmacists Network Marie Smith, PharmD and Michlle Breland, PhD University of Connecticut,
Healthy PA: Medicaid Expansion. Ann Bacharach PA Health Law Project February 20, 2014
 Healthy PA: Medicaid Expansion 1 Ann Bacharach PA Health Law Project February 20, 2014 Healthy PA Medicaid Proposal A waiver proposal to: 2 Make substantial changes PA s existing Medical Assistance program
Healthy PA: Medicaid Expansion 1 Ann Bacharach PA Health Law Project February 20, 2014 Healthy PA Medicaid Proposal A waiver proposal to: 2 Make substantial changes PA s existing Medical Assistance program
Utah Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Utah
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Utah As of July 2003, 196,600 people were covered under Utah s Medicaid/SCHIP programs. There were 157,322 enrolled in the Medicaid program,
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Utah As of July 2003, 196,600 people were covered under Utah s Medicaid/SCHIP programs. There were 157,322 enrolled in the Medicaid program,
Limiting the Duration of Medication Assisted Treatment for Opioid Addiction: Will New State Policies Help or Hurt?
 Limiting the Duration of Medication Assisted Treatment for Opioid Addiction: Will New State Policies Help or Hurt? Medicaid Evidence-Based Decisions Project June 25, 2014 Supported by National Institute
Limiting the Duration of Medication Assisted Treatment for Opioid Addiction: Will New State Policies Help or Hurt? Medicaid Evidence-Based Decisions Project June 25, 2014 Supported by National Institute
American Society of Addiction Medicine
 American Society of Addiction Medicine Public Policy Statement on Treatment for Alcohol and Other Drug Addiction 1 I. General Definitions of Addiction Treatment Addiction Treatment is the use of any planned,
American Society of Addiction Medicine Public Policy Statement on Treatment for Alcohol and Other Drug Addiction 1 I. General Definitions of Addiction Treatment Addiction Treatment is the use of any planned,
Private Fee-For-Service ----- Beneficiary Questions and Answers
 Private Fee-For-Service ----- Beneficiary Questions and Answers 1. What Is a Private Fee-For-Service Plan? A Private Fee-For-Service plan is a Medicare Advantage health plan offered by a private insurance
Private Fee-For-Service ----- Beneficiary Questions and Answers 1. What Is a Private Fee-For-Service Plan? A Private Fee-For-Service plan is a Medicare Advantage health plan offered by a private insurance
An Update on Medicare Parts C & D Performance Measures
 An Update on Medicare Parts C & D Performance Measures CMS Spring Conference April 12 & 13, 2011 Liz Goldstein, Ph.D. Director, Division of Consumer Assessment & Plan Performance Vikki Oates, M.A.S Director,
An Update on Medicare Parts C & D Performance Measures CMS Spring Conference April 12 & 13, 2011 Liz Goldstein, Ph.D. Director, Division of Consumer Assessment & Plan Performance Vikki Oates, M.A.S Director,
DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource
 E-Resource March, 2015 DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource Depression affects approximately 20% of the general population
E-Resource March, 2015 DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource Depression affects approximately 20% of the general population