Population Health: Chronic Disease Prevention and Quality Improvement
|
|
|
- Emerald Greene
- 7 years ago
- Views:
Transcription


1 Population Health: Chronic Disease Prevention and Quality Improvement September 2015 Presented by Adrienne Mims, MD MPH, FAAFP, AGSF Vice President, Chief Medical Officer 10/27/2015 1
2
3 Learning Objectives Why it is important to transform clinical practice What is population based care Why prevention and management of chronic disease is the key to success Using quality improvement tools to manage populations
4 Hierarchy of Needs in the 15-minute Visit Self- Management Support Preventive Care Chronic Disease Management THE URGENT Acute illness or injury, paperwork, psychosocial crisis, getting the meds straight
5 Current State Reactive Limited access Provider-delivered care Paper-driven Quality Assurance Siloed care Future State Proactive Expanded access Team-delivered care Data-driven Quality Improvement Coordinated & Integrated care Health plan-directed Disease Management Fee-for-service Provider/Team-directed Disease Management Global payment & shared savings

6
7 PQRS
8
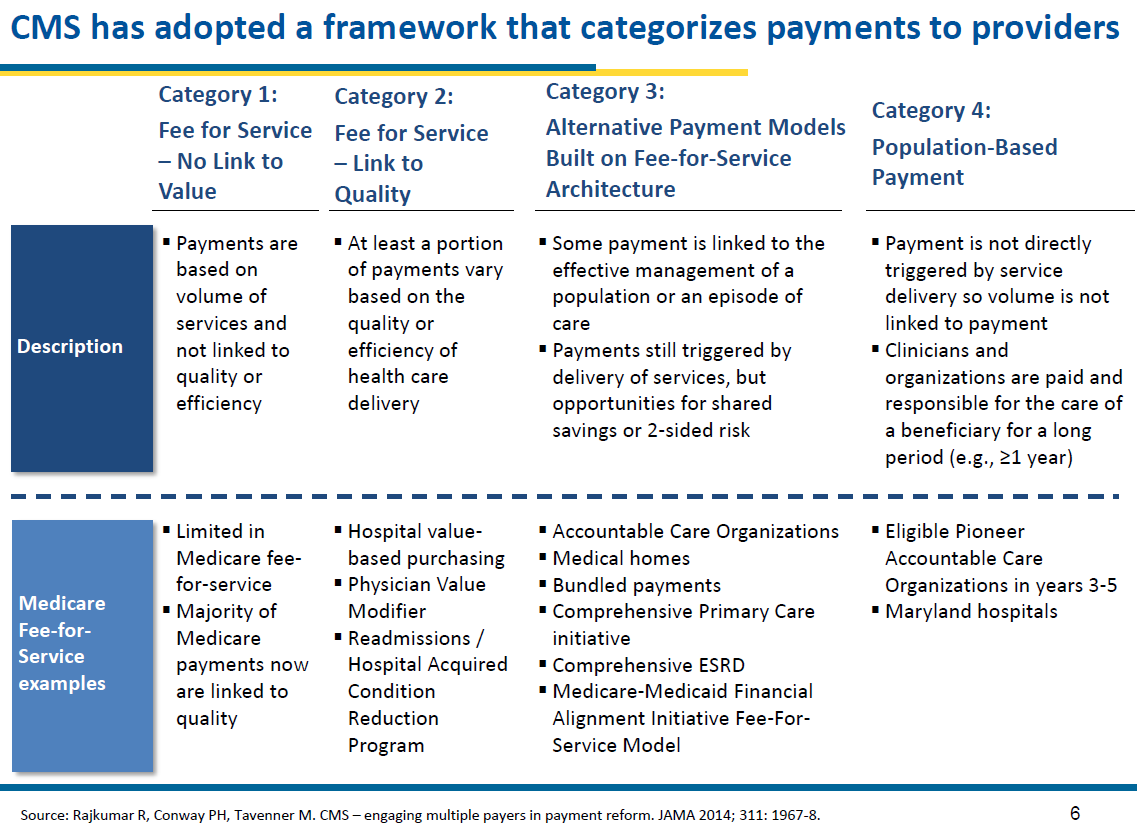
9 Accountable Care Organizations Essential Characteristics: Complete and timely information about patients and services received Technology and skills for population management and care coordination Resources for patient education and self-management Culture of teamwork Relationships with specialists and hospitals Ability to measure and report on quality Infrastructure and skills for managing risk Operational accountability and commitment to improve value Adapted from How to Create Accountable Care Organizations, Miller, HD, CHQPR.org 2009

10
11 Refinements to CCM Patient safety (in Health System); Cultural competency (in Delivery System Design) Care coordination (in Health System and Clinical Information Systems) Community policies (in Community Resources and Policies) Case management (in Delivery System Design) (accessed November 6, 2013)
12 Population-based Approach Identify patients in priority populations and then offer a variety of services to meet their needs Each population-based program has measurable goals and plans for improvement which include: Defining eligibility criteria for the identified population Defining evidence-based guidelines to guide care Defining measures to track performance Developing tools to assist practitioners in caring for these members, such as registries, panel reports, pamphlets, and other self-management tools
13 An Improvement Story : Mammography rates - The multispecialty group had: approx. 250,000 patients 125 physicians 10 offices Wanted to be known for high quality of care (HEDIS) Already adopted evidence based guidelines Group performance measured below national average Wide variation around the geographical region, within facilities, among practitioners
14 Population of Focus All plan patients Women Over 50 Population of Focus Mammogram Outcome Measure Denominator Unscreened Outcome Measure Numerator
15 Road to Improvement: Over 3 years Step 1 assembled a quality improvement team Step 2- determined baseline performance (73.8%) Step 3- ensured that all practitioners knew the evidence based guidelines (CME) Step 4 provided education to patients about the recommendations, covered benefit, location of services (posters, mailings, newsletters) Step 5 analyzed data - geo maps
16 Step 6 increased access van transportation Step 7 increased access - Saturday hours Step 8 increased access satellite facilities Step 9 patient surveys of unscreened Step 10 created a fact sheet to address reasons for not being screened * Too painful Fear of finding a lump Controversy over frequency Have a pacemaker Not interested Bad experience Breasts too small Not recommended by PCP Don t believe in them Step 10 tracked improvement rate 84.3% Step 11 Celebrated Success *The Permanente Journal/ Winter 2005/ Volume 9 No. 1

17 Ideal Distribution of Healthcare Services
18 200,000 Preventable Deaths from Heart Disease and Stroke Many of the deaths caused by heart disease and stroke are preventable Preventable deaths are those attributed to lack of preventive health care or timely and effective medical care
19 Health Disparities African-Americans develop high blood pressure more often, and at an earlier age, than whites and Hispanics do. African-Americans are nearly twice as likely as whites to die early from heart disease and stroke. American Indians and Alaska Natives die from heart diseases at younger ages than other racial and ethnic groups in the United States. 36% of those who die of heart disease die before age 65. Source: Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics 2013 update: a report from the American Heart Association. Circulation. 2013;127:e Morbidity and Mortality Weekly Report (MMWR): Vital Signs: Avoidable Deaths from Heart Disease, Stroke, and Hypertensive Disease United States, SS Oh, JB Croft, KJ Greenlund, C Ayala, ZJ Zheng, GA Mensah, WH Giles. Disparities in Premature Deaths from Heart Disease 50 States and the District of Columbia. MMWR 2004;53:
20
21 Heart Age: Is Your Heart Older Than You?
22 Screening for Hypertension The U.S. Preventive Services Task Force (USPSTF) recommends screening for high blood pressure in adults aged 18 and older. (This is a grade "A" recommendation) Screen: Every 2 years - blood pressure less than 120/80 mm Hg Yearly - systolic mm Hg or diastolic mm Hg U.S. Preventive Services Task Force. Screening for high blood pressure: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2007:
23 Screening for Hypertension (cont d) Hypertension diagnosed - 2 or more elevated readings on at least 2 visits over a period of 1 to several weeks Use code R03.0 (ICD-10) -Elevated bloodpressure reading, without diagnosis of hypertension Hypertension definition - adults with: Systolic - of 140 mmhg or higher or Diastolic - of 90 mmhg or higher U.S. Preventive Services Task Force. Screening for high blood pressure: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2007:
 Controlled SOURCE: National Health and Nutrition Examination Survey 2011-2012.")
24 Only Half of Americans with Hypertension Have It Under Control 72 MILLION ADULTS WITH HYPERTENSION (31%) 52% 48% Uncontrolled (35 M) Controlled SOURCE: National Health and Nutrition Examination Survey

25 Awareness and Treatment among Adults with Uncontrolled Hypertension 35 MILLION ADULTS WITH UNCONTROLLED HYPERTENSION 13M 17M Aware and treated 5M Aware and untreated SOURCE: National Health and Nutrition Examination Survey
26 Millions Prevalence of Uncontrolled Hypertension by Selected Characteristics % 85% 74% Yes No Usual Source of Care Yes No Health Insurance 2 1 None # Times Received Care in Past Year SOURCE: National Health and Nutrition Examination Survey
27 Million Hearts Goal: Prevent 1 million heart attacks and strokes by 2017 National initiative co-led by CDC and CMS In partnership with federal, state, and private organizations 27

28 Key Components of Million Hearts Keeping Us Healthy Changing the environment Health Disparities Excelling in the ABCS Optimizing care Aspirin when appropriate Blood pressure control Cholesterol management Smoking cessation TRANS FAT Focus on the ABCS Health information technology Innovations in care delivery

29 Million Hearts Progress to Date Engagement and activation 125 partners, 50 states, coalitions, >58K subscribers, 135 Congregations Clinical Quality Measure alignment Understand what works, where, and why Resources that help Focus on what makes a difference Champions Guides, Healthy Eating Center, CQM Dashboard, Protocols, Funding 6.3M smokers quit 10M people with hypertension achieve control 20% less sodium each day Focus on those with the greatest burden and at the greatest risk


30 Million Hearts Clinical Quality Dashboard Performance on the S Performance Targets Million Hearts Clinical Target = 70% Red = 0%-49% Yellow = 50%-69% Green = 70%+ Smoking Assessment and Treatment
31 Hypertension Control 2013 Georgia Data Source Performance Rate Goal HRSA UDS 61% 70% HEDIS Commercial 61% 70% HEDIS Medicaid 47% 70% PQRS GPRO 67% 70% PQRS ACO 60% 70%

32 Standardized HTN Treatment Protocols Evidence-based protocols examples: U.S. Department of Veterans Affairs Kaiser Permanente Institute for Clinical Systems Improvement NYC Health and Hospitals Corporation Customizable template Key protocol components Implementation guidance
33 Recommended Elements of Effective Hypertension Protocols Clarity and simplicity Lifestyle modification Treatment by stage of hypertension Time interval to titration and reassessment Use of low-cost 1st-line treatment Exclusions and suggestions for medications based on concurrent medical conditions
34 Recommended Elements (continued) Recommended lab tests Reminder of the underlying causes of nonessential or secondary hypertension Adherence-enhancing approaches such as fixed dose and/or combination drugs Indications for referral to hypertensive specialist Number needed to treat to avoid a clinical event Supporting references Congruent with current guidelines
35 Implementing a Hypertension Protocol Make hypertension control a priority Fully use the expertise and scope of practice of every member of the health care team Include the patient and family as key team members Conduct pre-visit planning care Learn about community resources and Recommend them to patients Look for opportunities to check in with patients and adjust medication dose as needed

36 Percent of patients with controlled hypertension Success Story: Kaiser Permanente Northern California 90% Promotion of single-pill combination therapy 87% 80% 70% 60% 50% 44% Hypertension control reports every 1 3 months and evidence-based hypertension control protocol Medical assistant visits for follow-up measurements 40% Jaffe, M.G., et al. (2013). Improved blood pressure control associated with a large-scale hypertension program. JAMA, 310 (7).
37 Standardized Treatment Protocols Can Help Reduce Disparate Outcomes: Kaiser Permanente Southern California To help ensure homogeneity of practice delivered, the hypertension treatment had to be standardized as well. This meant that an internal treatment guideline was needed. Sim, et al. Systemic Implementation Strategies to Improve Hypertension: The Kaiser Permanente Southern California Experience. Canadian Journal of Cardiology 30 (2014)
38 Standardized Treatment Protocols Can Help Reduce Disparate Outcomes: Kaiser Permanente Southern California Across all ages, races, and sexes, hypertension control has exceeded 80%. 85.0% BP control 86.6% BP control 87.9% BP control 81.4% BP control 85.0% BP control Shaw KM, Handler J, Wall HK, Kanter MH. Improving Blood Pressure Control in a Large Multiethnic California Population Through Changes in Health Care Delivery, Prev Chronic Dis 2014;11: DOI:
39 Protocol Implementation: How Can A Practice Get Started? Make decisions about roles, content, meds, more Workflow of BP measurement and recording What lifestyle advice will you give? By whom? When? How? Which medications will you use and at what dosages? What are your target goals and for what ages? How often to re-check and titrate? Who does this? How? How will you define and manage resistance? Track implementation weekly; share monthly control rates Celebrate your success along the way


40 Self-Measured Blood Pressure Monitoring: Action Steps for Clinicians Guidance for clinicians on SMBP Teach patients to use monitors Check home machines for accuracy Suggested protocol for home monitoring Guidance on establishing a patientclinician feedback loop Docs/MH_SMBP_Clinicians.pdf

41 /materials/blood_blood_pressure_tracker_10 SOW-GA-IHPC pdf
42 Using Quality Improvement Tools To Manage Populations
43 Defining the Population of Focus All Clinic Patients Adult Patients Diagnosis of HTN Population of Focus BP Measured Outcome Measure Denominator Blood Pressure Controlled Outcome Measure Numerator

44 Model for Improvement

45 Project Flow Over Time Define population and measures Develop Aim A P D A P D A P D Obtain baseline measures Set measureable goals S S S Re-measure Re-measure
46 Aim Statement Specific Measureable Attainable Relevant/realistic Timely
47 Aim Statement Examples A. We will increase the amount of patients with blood pressure under control among our clinic patients. (weak) B. In three months, patients who have uncontrolled blood pressure will be requested to perform self monitoring of blood pressures. (better) C. By December 2015, we will increase the number of people with hypertension who have a normal blood pressure from 50% to 55% by utilizing a nurse visit protocol (strong) 47
48 Diagnosis of Hypertension Population Segmentation YES Blood Pressure Measured NO YES Quantifiable Data Segment : used to monitory change in improvement Clinic Visit NO Blood Pressure Under Control YES NO YES Measure in 6 Months NO On Medications YES NO YES Track When Next Due

49 Root Cause Analysis Example Aim Statement BP monitored 90% of Population of Focus will have an clinic visit within the next 6 months Baseline 61% Root Cause Analysis BP monitored Short Staff Availability of equipment Lack of standing orders Provider inconsistency Not maximizing the use of pt. alerts/notifications Lack of training (MAs) Aim Statement On medication By the end of December, 2015, the 55% of patients with blood pressure under control Baseline 50% under control Root Cause Analysis On a medication Failure to keep appointments/take meds/follow diet Transportation Provider inertia Family support patient stubbornness Adherence Lack of home monitoring Lack of exercise Psychological depression, anxiety Environmental Financial limitations Patient denial Personal habits smoking/illicit drug use
 Plan")
50 PDSA Cycle for Process Improvement ACT What changes are to be made? Next cycle? STUDY Complete the analysis of the data Compare data to predictions Summarize what is learned PLAN Objective Questions and predictions Plan to carry out the cycle (who, what, where, when) Plan for data collection DO Carry out the plan Document the problems and unexpected observations Begin analysis of the data
51 Receptionist Nurse Work Flow Swim Lanes Swim Lanes Check In Vitals taken rooms patient Physician performs exam reviews labs, writes orders Lab performs UA, A1C Health Education education provided Referrals process referral Billing Desk pays bill books next appt
52 Final Advice Team is Critical Use QI tools for structure and documentation Go for Low Hanging Fruit Celebrate and Recognize Remind everyone why we are here for Patients!
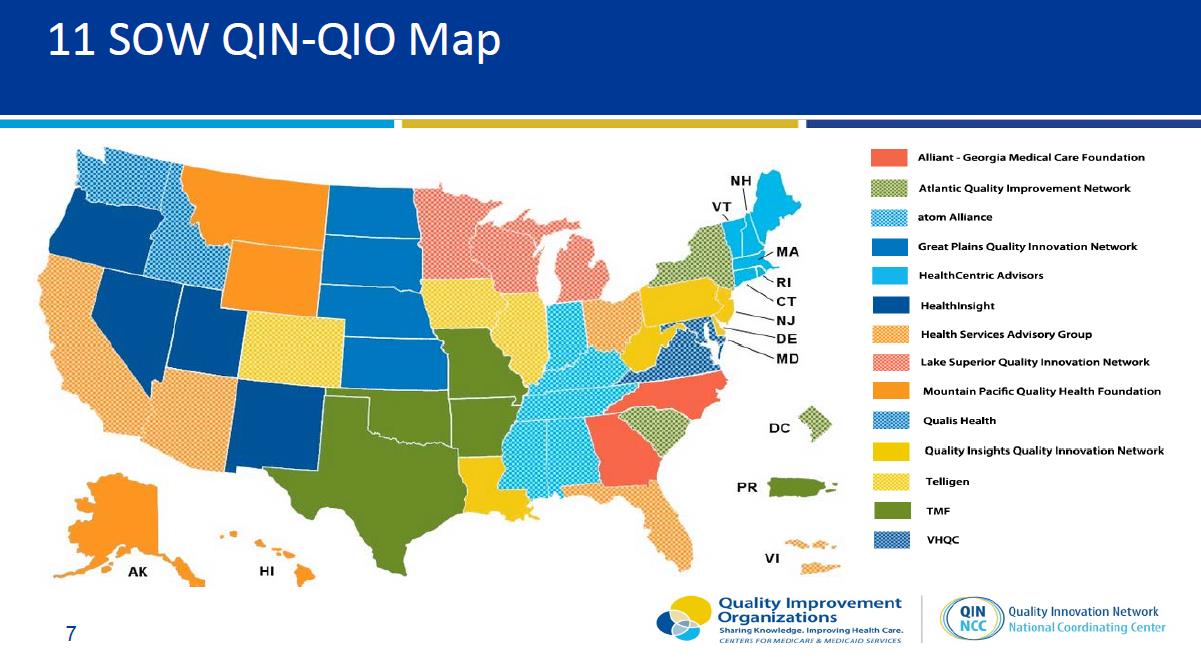
53 This material was prepared by GMCF, for Alliant Quality, the Medicare Quality Innovation Network Quality Improvement Organization for Georgia and North Carolina, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. Publication No. 11SOW-GMCFQIN-NC-B
54 Evaluation Please take < 90 seconds to evaluate this session. Time permitting, speaker will take questions following evaluation. Responses are not displayed and are important in maintaining high quality education.
55 The overall performance of the speaker: 1. Poor 63% 2. Fair 3. Average 4. Good 5. Excellent 29% 8% 0% 0%
56 How well were the learning objectives met? 1. Poor 2. Fair 3. Average 70% 4. Good 22% 5. Excellent 3% 0% 5% Poor Fair Average Good Excellent
57 Did speaker present a balanced view of therapeutic options? 1. Yes 2. No 3. N/A 80% 18% 2% Yes No N/A
58 How useful will this session be in your practice? 47% 1. Poor 2. Fair 29% 3. Average 4. Good 5. Excellent 6% 2% 16% Poor Fair Average Good Excellent
59 As a result of this program, do you intend to change your patient care? 1. Yes 75% 2. No 25% Yes No

60 Thank you!
Improving Clinical Processes: The Million Hearts Hypertension Control Change Package for Clinicians
 Improving Clinical Processes: The Million Hearts Hypertension Control Change Package for Clinicians Hilary K. Wall, MPH Million Hearts Science Lead Division for Heart Disease and Stroke Prevention U.S.
Improving Clinical Processes: The Million Hearts Hypertension Control Change Package for Clinicians Hilary K. Wall, MPH Million Hearts Science Lead Division for Heart Disease and Stroke Prevention U.S.
Blood Pressure Assessment Program Screening Guidelines
 Blood Pressure Assessment Program Screening Guidelines Assessment Pre-Assessment Prior to/during assessment, explain to client the following: What is meant by high blood pressure; What are the effects
Blood Pressure Assessment Program Screening Guidelines Assessment Pre-Assessment Prior to/during assessment, explain to client the following: What is meant by high blood pressure; What are the effects
Division for Heart Disease and Stroke Prevention Million Hearts Clinical Quality Measures Dashboard
 Division for Heart Disease and Stroke Prevention Million Hearts Clinical Quality Measures Dashboard INTRODUCTION Million Hearts web-based Clinical Quality Measures (CQM) Dashboard is designed to monitor
Division for Heart Disease and Stroke Prevention Million Hearts Clinical Quality Measures Dashboard INTRODUCTION Million Hearts web-based Clinical Quality Measures (CQM) Dashboard is designed to monitor
Health risk assessment: a standardized framework
 Health risk assessment: a standardized framework February 1, 2011 Thomas R. Frieden, MD, MPH Director, Centers for Disease Control and Prevention Leading causes of death in the U.S. The 5 leading causes
Health risk assessment: a standardized framework February 1, 2011 Thomas R. Frieden, MD, MPH Director, Centers for Disease Control and Prevention Leading causes of death in the U.S. The 5 leading causes
DIABETES DISEASE MANAGEMENT PROGRAM DESCRIPTION FY11 FY12
 DIABETES DISEASE MANAGEMENT PROGRAM DESCRIPTION FY11 FY12 TABLE OF CONTENTS 1. INTRODUCTION.3 2. SCOPE........3 3. PROGRAM STRUCTURE...4 3.1. General Educational Interventions.....4 3.2. Identification
DIABETES DISEASE MANAGEMENT PROGRAM DESCRIPTION FY11 FY12 TABLE OF CONTENTS 1. INTRODUCTION.3 2. SCOPE........3 3. PROGRAM STRUCTURE...4 3.1. General Educational Interventions.....4 3.2. Identification
CQMs. Clinical Quality Measures 101
 CQMs Clinical Quality Measures 101 BASICS AND GOALS In the past 10 years, clinical quality measures (CQMs) have become an integral component in the Centers for Medicare & Medicaid Services (CMS) drive
CQMs Clinical Quality Measures 101 BASICS AND GOALS In the past 10 years, clinical quality measures (CQMs) have become an integral component in the Centers for Medicare & Medicaid Services (CMS) drive
Coronary Heart Disease (CHD) Brief
 Brief") Coronary Heart Disease (CHD) Brief What is Coronary Heart Disease? Coronary Heart Disease (CHD), also called coronary artery disease 1, is the most common heart condition in the United States. It occurs
Coronary Heart Disease (CHD) Brief What is Coronary Heart Disease? Coronary Heart Disease (CHD), also called coronary artery disease 1, is the most common heart condition in the United States. It occurs
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
Mississippi Delta Health Collaborative Mississippi State Department of Health 1
 The Impact of Community Health Workers on Cardiovascular Risk Reduction : Findings from the Clinical Community Health Worker Initiative Mississippi Delta Health Collaborative Mississippi State Department
The Impact of Community Health Workers on Cardiovascular Risk Reduction : Findings from the Clinical Community Health Worker Initiative Mississippi Delta Health Collaborative Mississippi State Department
The Stopping Elderly Accidents, Deaths & Injuries (STEADI) Tool Kit for Health Care Providers
 Tool Kit for Health Care Providers") The Stopping Elderly Accidents, Deaths & Injuries (STEADI) Tool Kit for Health Care Providers Disclaimer: The findings and conclusions in this presentation are those of the author and do not necessarily
The Stopping Elderly Accidents, Deaths & Injuries (STEADI) Tool Kit for Health Care Providers Disclaimer: The findings and conclusions in this presentation are those of the author and do not necessarily
CDS Starter Kit: Diabetes f ollow-up care
 CDS Starter Kit: Diabetes f ollow-up care Introduction The delivery of high-quality diabetes care is a complex process that requires a provider to consider many pieces of patient information and treatment
CDS Starter Kit: Diabetes f ollow-up care Introduction The delivery of high-quality diabetes care is a complex process that requires a provider to consider many pieces of patient information and treatment
From Concept to Rapid Visualization a Data Analytics Case Study
 From Concept to Rapid Visualization a Data Analytics Case Study Gregory Wozniak, PhD Director of Outcomes Analytics Health Outcomes Group American Medical Association The Journey Objectives Share experiences
From Concept to Rapid Visualization a Data Analytics Case Study Gregory Wozniak, PhD Director of Outcomes Analytics Health Outcomes Group American Medical Association The Journey Objectives Share experiences
Continuity of Care Guide for Ambulatory Medical Practices
 Continuity of Care Guide for Ambulatory Medical Practices www.himss.org t ra n sf o r m i ng he a lth c a re th rou g h IT TM Table of Contents Introduction 3 Roles and Responsibilities 4 List of work/responsibilities
Continuity of Care Guide for Ambulatory Medical Practices www.himss.org t ra n sf o r m i ng he a lth c a re th rou g h IT TM Table of Contents Introduction 3 Roles and Responsibilities 4 List of work/responsibilities
SMD# 13-001 ACA #23. Re: Health Home Core Quality Measures. January 15, 2013. Dear State Medicaid Director:
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-26-12 Baltimore, Maryland 21244-1850 SMD# 13-001 ACA #23 Re: Health Home Core Quality
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-26-12 Baltimore, Maryland 21244-1850 SMD# 13-001 ACA #23 Re: Health Home Core Quality
Achieving Quality and Value in Chronic Care Management
 The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY
 Measure #317: Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up Documented National Quality Strategy Domain: Community / Population Health 2016 PQRS OPTIONS F INDIVIDUAL MEASURES:
Measure #317: Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up Documented National Quality Strategy Domain: Community / Population Health 2016 PQRS OPTIONS F INDIVIDUAL MEASURES:
Quality Improvement Case Study: Improving Blood Pressure Control in a 3- Provider Primary Care Practice
 Quality Improvement Case Study: Improving Blood Pressure Control in a 3- Provider Primary Care Practice EXECUTIVE SUMMARY Organization Ellsworth Medical Clinic 1 is a family medicine practice in Wisconsin
Quality Improvement Case Study: Improving Blood Pressure Control in a 3- Provider Primary Care Practice EXECUTIVE SUMMARY Organization Ellsworth Medical Clinic 1 is a family medicine practice in Wisconsin
Healthy Living with Diabetes. Diabetes Disease Management Program
 Healthy Living with Diabetes Diabetes Disease Management Program Healthy Living With Diabetes Diabetes Disease Management Program Background According to recent reports the incidence of diabetes (type
Healthy Living with Diabetes Diabetes Disease Management Program Healthy Living With Diabetes Diabetes Disease Management Program Background According to recent reports the incidence of diabetes (type
PUBLIC HEALTH SURVEILLANCE FOR DISEASE PREVENTION: LESSONS FROM THE BEHAVIORAL RISK FACTOR SURVEILLANCE SYSTEM
 PUBLIC HEALTH SURVEILLANCE FOR DISEASE PREVENTION: LESSONS FROM THE BEHAVIORAL RISK FACTOR SURVEILLANCE SYSTEM The burden of chronic diseases is increasing worldwide. Surveillance of behavioral risk factors
PUBLIC HEALTH SURVEILLANCE FOR DISEASE PREVENTION: LESSONS FROM THE BEHAVIORAL RISK FACTOR SURVEILLANCE SYSTEM The burden of chronic diseases is increasing worldwide. Surveillance of behavioral risk factors
CDC Grand Rounds: The Million Hearts Initiative
 Page 1 of 7 Morbidity and Mortality Weekly Report (MMWR) CDC Grand Rounds: The Million Hearts Initiative Weekly December 21, 2012 / 61(50);1017-1021 The Magnitude of the Problem Cardiovascular disease,
Page 1 of 7 Morbidity and Mortality Weekly Report (MMWR) CDC Grand Rounds: The Million Hearts Initiative Weekly December 21, 2012 / 61(50);1017-1021 The Magnitude of the Problem Cardiovascular disease,
Improving Diabetes Care for All New Yorkers
 Improving Diabetes Care for All New Yorkers Lynn D. Silver, MD, MPH Assistant Commissioner Bureau of Chronic Disease Prevention and Control Diana K. Berger, MD, MSc Medical Director Diabetes Prevention
Improving Diabetes Care for All New Yorkers Lynn D. Silver, MD, MPH Assistant Commissioner Bureau of Chronic Disease Prevention and Control Diana K. Berger, MD, MSc Medical Director Diabetes Prevention
Nutrition. Type 2 Diabetes: A Growing Challenge in the Healthcare Setting NAME OF STUDENT
 1 Nutrition Type 2 Diabetes: A Growing Challenge in the Healthcare Setting NAME OF STUDENT 2 Type 2 Diabetes: A Growing Challenge in the Healthcare Setting Introduction and background of type 2 diabetes:
1 Nutrition Type 2 Diabetes: A Growing Challenge in the Healthcare Setting NAME OF STUDENT 2 Type 2 Diabetes: A Growing Challenge in the Healthcare Setting Introduction and background of type 2 diabetes:
Using Health Information Technology to Improve Quality of Care: Clinical Decision Support
 Using Health Information Technology to Improve Quality of Care: Clinical Decision Support Vince Fonseca, MD, MPH Director of Medical Informatics Intellica Corporation Objectives Describe the 5 health priorities
Using Health Information Technology to Improve Quality of Care: Clinical Decision Support Vince Fonseca, MD, MPH Director of Medical Informatics Intellica Corporation Objectives Describe the 5 health priorities
Kaiser Permanente of Ohio
 Kaiser Permanente of Ohio Chronic Disease Management Program March 11, 2011 Presenters: Amy Kramer and Audrey L. Callahan 1 Objectives 1. Define the roles and responsibilities of the Care Managers in the
Kaiser Permanente of Ohio Chronic Disease Management Program March 11, 2011 Presenters: Amy Kramer and Audrey L. Callahan 1 Objectives 1. Define the roles and responsibilities of the Care Managers in the
AGENCY-SPECIFIC PLAN FOR THE NATIONAL QUALITY STRATEGY
 AGENCY-SPECIFIC PLAN FOR THE NATIONAL QUALITY STRATEGY Adult Medicaid Quality Grants Program The Adult Medicaid Quality Grants Program is a 2-year funding opportunity designed to support grantee Medicaid
AGENCY-SPECIFIC PLAN FOR THE NATIONAL QUALITY STRATEGY Adult Medicaid Quality Grants Program The Adult Medicaid Quality Grants Program is a 2-year funding opportunity designed to support grantee Medicaid
Division for Heart Disease and Stroke Prevention. Division Budget and Program Briefing for the Institute of Medicine April 9, 2009
 Division for Heart Disease and Stroke Prevention Division Budget and Program Briefing for the Institute of Medicine April 9, 2009 1 Human and Fiscal Resource History Fiscal Year Budget FTEs 2003 $55 million
Division for Heart Disease and Stroke Prevention Division Budget and Program Briefing for the Institute of Medicine April 9, 2009 1 Human and Fiscal Resource History Fiscal Year Budget FTEs 2003 $55 million
JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates. January 30, 2014
 JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates January 30, 2014 GOALS Review key recommendations from recently published guidelines on blood pressure and cholesterol management Discuss
JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates January 30, 2014 GOALS Review key recommendations from recently published guidelines on blood pressure and cholesterol management Discuss
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Promoting CVD Prevention in Your Practice: A New Medicare Reimbursable Service
 Promoting CVD Prevention in Your Practice: A New Medicare Reimbursable Service Richard Josephson, MD, MS, Professor of Medicine, Case Western Reserve University; Medical Director, CICU, UH Case Medical
Promoting CVD Prevention in Your Practice: A New Medicare Reimbursable Service Richard Josephson, MD, MS, Professor of Medicine, Case Western Reserve University; Medical Director, CICU, UH Case Medical
Standing for Equity Eliminating Disparities and Promoting Wellness
 The 2014 Culturally Competent Healthcare Event DiversityInc October 22, 2014 Standing for Equity Eliminating Disparities and Promoting Wellness Winston Wong, MD Medical Director, Community Benefit Director,
The 2014 Culturally Competent Healthcare Event DiversityInc October 22, 2014 Standing for Equity Eliminating Disparities and Promoting Wellness Winston Wong, MD Medical Director, Community Benefit Director,
High Blood Pressure (Essential Hypertension)
") Sacramento Heart & Vascular Medical Associates February 18, 2012 500 University Ave. Sacramento, CA 95825 Page 1 916-830-2000 Fax: 916-830-2001 What is essential hypertension? Blood pressure is the force
Sacramento Heart & Vascular Medical Associates February 18, 2012 500 University Ave. Sacramento, CA 95825 Page 1 916-830-2000 Fax: 916-830-2001 What is essential hypertension? Blood pressure is the force
Hypertension Best Practices Symposium
 essentia health: east region 1 Hypertension Best Practices Symposium RN Hypertension Management Pilot Essentia Health: East Region Duluth, MN ORGANIZATION PROFILE Essentia Health is an integrated health
essentia health: east region 1 Hypertension Best Practices Symposium RN Hypertension Management Pilot Essentia Health: East Region Duluth, MN ORGANIZATION PROFILE Essentia Health is an integrated health
HSAG: The QIN-QIO for Arizona, California, Florida, Ohio, and the U.S. Virgin Islands
 HSAG: The QIN-QIO for Arizona, California, Florida, Ohio, and the U.S. Virgin Islands Jim Barnhart, BSH LNHA Quality Improvement Specialist Carol Saavedra, BA Health Informatics Specialist November 18,
HSAG: The QIN-QIO for Arizona, California, Florida, Ohio, and the U.S. Virgin Islands Jim Barnhart, BSH LNHA Quality Improvement Specialist Carol Saavedra, BA Health Informatics Specialist November 18,
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases
 Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Kaiser Permanente: Health Education. Mei Ling Schwartz, MPH Director, Health & Physician Education Kaiser Permanente Panorama City Medical Center
 Kaiser Permanente: Health Education Mei Ling Schwartz, MPH Director, Health & Physician Education Kaiser Permanente Panorama City Medical Center Who Is Kaiser Permanente? Founded in 1945, Kaiser Permanente
Kaiser Permanente: Health Education Mei Ling Schwartz, MPH Director, Health & Physician Education Kaiser Permanente Panorama City Medical Center Who Is Kaiser Permanente? Founded in 1945, Kaiser Permanente
Diabetes Care 2011-2012
 Clinical Innovations in the Patient Centered Medical Home to Improve Diabetes Care Robert A. Gabbay, MD, PhD, FACP Chief Medical Officer & Senior Vice President Joslin Diabetes Center Harvard Medical School
Clinical Innovations in the Patient Centered Medical Home to Improve Diabetes Care Robert A. Gabbay, MD, PhD, FACP Chief Medical Officer & Senior Vice President Joslin Diabetes Center Harvard Medical School
Approaches to Asthma Management:
 Approaches to Asthma Management: BY CAROL MCPHILLIPS-TANGUM AND CAROLINE M. ERCEG ASTHMA IS A CHRONIC DISEASE that affects millions of people in the United States and disproportionately impacts children,
Approaches to Asthma Management: BY CAROL MCPHILLIPS-TANGUM AND CAROLINE M. ERCEG ASTHMA IS A CHRONIC DISEASE that affects millions of people in the United States and disproportionately impacts children,
Stage 1 Meaningful Use for Specialists. NYC REACH Primary Care Information Project NYC Department of Health & Mental Hygiene
 Stage 1 Meaningful Use for Specialists NYC REACH Primary Care Information Project NYC Department of Health & Mental Hygiene 1 Today s Agenda Meaningful Use Overview Meaningful Use Measures Resources Primary
Stage 1 Meaningful Use for Specialists NYC REACH Primary Care Information Project NYC Department of Health & Mental Hygiene 1 Today s Agenda Meaningful Use Overview Meaningful Use Measures Resources Primary
Connecticut Diabetes Statistics
 Connecticut Diabetes Statistics What is Diabetes? State Public Health Actions (1305, SHAPE) Grant March 2015 Page 1 of 16 Diabetes is a disease in which blood glucose levels are above normal. Blood glucose
Connecticut Diabetes Statistics What is Diabetes? State Public Health Actions (1305, SHAPE) Grant March 2015 Page 1 of 16 Diabetes is a disease in which blood glucose levels are above normal. Blood glucose
WILL EQUITY BE ACHIEVED THROUGH HEALTH CARE REFORM? John Z. Ayanian, MD, MPP
 WILL EQUITY BE ACHIEVED THROUGH HEALTH CARE REFORM? John Z. Ayanian, MD, MPP Brigham and Women s Hospital Harvard Medical School Harvard School of Public Health BWH Patient-Centered Outcomes Seminar April
WILL EQUITY BE ACHIEVED THROUGH HEALTH CARE REFORM? John Z. Ayanian, MD, MPP Brigham and Women s Hospital Harvard Medical School Harvard School of Public Health BWH Patient-Centered Outcomes Seminar April
University of Michigan Health Risk Assessment (HRA) and Trend Management System (TMS)
 and Trend Management System (TMS)") University of Michigan Health Risk Assessment (HRA) and Trend Management System (TMS) CIGNA has entered into a long-term agreement with the University of Michigan, which gives it access to intellectual
University of Michigan Health Risk Assessment (HRA) and Trend Management System (TMS) CIGNA has entered into a long-term agreement with the University of Michigan, which gives it access to intellectual
ADULT HYPERTENSION PROTOCOL STANFORD COORDINATED CARE
 I. PURPOSE To establish guidelines for the monitoring of antihypertensive therapy in adult patients and to define the roles and responsibilities of the collaborating clinical pharmacist and pharmacy resident.
I. PURPOSE To establish guidelines for the monitoring of antihypertensive therapy in adult patients and to define the roles and responsibilities of the collaborating clinical pharmacist and pharmacy resident.
Population Health Management Infrastructure
 Population Health Management Infrastructure William Pagano MD, MPH SVP of Clinical Operations Doreen Colella RN, MSN AVP of Quality Interfaces The Azara reporting tool interfaces with multiple systems.
Population Health Management Infrastructure William Pagano MD, MPH SVP of Clinical Operations Doreen Colella RN, MSN AVP of Quality Interfaces The Azara reporting tool interfaces with multiple systems.
Facts about Diabetes in Massachusetts
 Facts about Diabetes in Massachusetts Diabetes is a disease in which the body does not produce or properly use insulin (a hormone used to convert sugar, starches, and other food into the energy needed
Facts about Diabetes in Massachusetts Diabetes is a disease in which the body does not produce or properly use insulin (a hormone used to convert sugar, starches, and other food into the energy needed
FROM DATA TO KNOWLEDGE: INTEGRATING ELECTRONIC HEALTH RECORDS MEANINGFULLY INTO OUR NURSING PRACTICE
 FROM DATA TO KNOWLEDGE: INTEGRATING ELECTRONIC HEALTH RECORDS MEANINGFULLY INTO OUR NURSING PRACTICE Rayne Soriano MS, RN Manager of Nursing Informatics and Clinical Transformation Program Kaiser Permanente
FROM DATA TO KNOWLEDGE: INTEGRATING ELECTRONIC HEALTH RECORDS MEANINGFULLY INTO OUR NURSING PRACTICE Rayne Soriano MS, RN Manager of Nursing Informatics and Clinical Transformation Program Kaiser Permanente
Measuring Your Blood Pressure at Home. A Review of the Research for Adults
 Measuring Your Blood Pressure at Home A Review of the Research for Adults Is This Information Right for Me? Yes, if: A doctor* has told you that you may have high blood pressure, also called hypertension.
Measuring Your Blood Pressure at Home A Review of the Research for Adults Is This Information Right for Me? Yes, if: A doctor* has told you that you may have high blood pressure, also called hypertension.
Secure Messaging Evidence Table
 APPENDIX E. Evidence Tables Secure Messaging Evidence Table Health Outcomes Simon, 2011 9 RCT; N=208 patients; 04/09-10/09 Elkjaer, 2010 1 Zhou, 2010 2 Harris, 2009 3 Ralston, 2009 6 Tuil, 2007 4 RCT;
APPENDIX E. Evidence Tables Secure Messaging Evidence Table Health Outcomes Simon, 2011 9 RCT; N=208 patients; 04/09-10/09 Elkjaer, 2010 1 Zhou, 2010 2 Harris, 2009 3 Ralston, 2009 6 Tuil, 2007 4 RCT;
Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology
 Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology The chart below lists the measures (and specialty exclusions) that eligible providers must demonstrate
Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology The chart below lists the measures (and specialty exclusions) that eligible providers must demonstrate
QI and the EMR: Identifying and Addressing Disparities in Chronic Disease Management
 QI and the EMR: Identifying and Addressing Disparities in Chronic Disease Management Thomas D. Sequist, MD, MPH Assistant Professor of Medicine and Health Care Policy at Brigham and Women's Hospital and
QI and the EMR: Identifying and Addressing Disparities in Chronic Disease Management Thomas D. Sequist, MD, MPH Assistant Professor of Medicine and Health Care Policy at Brigham and Women's Hospital and
HEDIS 2012 Results
 Capital District Physicians Health Plan, Inc. Nonprofit Health Plan Albany, New York Capital District Physicians Health Plan, Inc. (CDPHP ) is featured as a high performer in cardiovascular care, identified
Capital District Physicians Health Plan, Inc. Nonprofit Health Plan Albany, New York Capital District Physicians Health Plan, Inc. (CDPHP ) is featured as a high performer in cardiovascular care, identified
PPC 8: Performance Reporting and Improvement Element D: Setting Goals and Taking Action
 PPC 8: Performance Reporting and Improvement Element D: Setting Goals and Taking Action sets goals and creates action plans as part of our annual preparation of our Federal Health Plan. Below are examples
PPC 8: Performance Reporting and Improvement Element D: Setting Goals and Taking Action sets goals and creates action plans as part of our annual preparation of our Federal Health Plan. Below are examples
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis
 Population in Connecticut Survey Analysis") Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
An Overview and Guide to Healthy Living with Type 2 Diabetes
 MEETING YOUR GOALS An Overview and Guide to Healthy Living with Type 2 Diabetes MEETING YOUR GOALS This brochure was designed to help you understand the health goals to live a healthy lifestyle with type
MEETING YOUR GOALS An Overview and Guide to Healthy Living with Type 2 Diabetes MEETING YOUR GOALS This brochure was designed to help you understand the health goals to live a healthy lifestyle with type
Meaningful Use - The Basics
 Meaningful Use - The Basics Presented by PaperFree Florida 1 Topics Meaningful Use Stage 1 Meaningful Use Barriers: Observations from the field Help and Questions 2 What is Meaningful Use Meaningful Use
Meaningful Use - The Basics Presented by PaperFree Florida 1 Topics Meaningful Use Stage 1 Meaningful Use Barriers: Observations from the field Help and Questions 2 What is Meaningful Use Meaningful Use
Continuous Quality Improvement using Centricity EMR
 Continuous Quality Improvement using Centricity EMR Jamie Howard, MD David A. Nelsen, Jr, MD, MS Associate Professors, UAMS Family & Preventive Medicine Sept 22-25, 2004 CLINICAL INFORMATION SYSTEMS 1
Continuous Quality Improvement using Centricity EMR Jamie Howard, MD David A. Nelsen, Jr, MD, MS Associate Professors, UAMS Family & Preventive Medicine Sept 22-25, 2004 CLINICAL INFORMATION SYSTEMS 1
Meaningful Use of Electronic Health Records in Hypertension Management
 Meaningful Use of Electronic Health Records in Hypertension Management Maggie Wanis, DrPh U.S. Department of Health & Human Services, Office of the National Coordinator for Health IT, Office of Programs
Meaningful Use of Electronic Health Records in Hypertension Management Maggie Wanis, DrPh U.S. Department of Health & Human Services, Office of the National Coordinator for Health IT, Office of Programs
What is the Cardiovascular Health Awareness Program?
 What is the Cardiovascular Health Awareness Program? 1 What is CHAP? CHAP is a community-based program that brings together local family physicians, pharmacists, volunteers, public health representatives
What is the Cardiovascular Health Awareness Program? 1 What is CHAP? CHAP is a community-based program that brings together local family physicians, pharmacists, volunteers, public health representatives
Meaningful Use Qualification Plan
 Meaningful Use Qualification Plan Overview Certified EHR technology used in a meaningful way is one piece of a broader Health Information Technology infrastructure intended to reform the health care system
Meaningful Use Qualification Plan Overview Certified EHR technology used in a meaningful way is one piece of a broader Health Information Technology infrastructure intended to reform the health care system
Electronic Health Records and Quality Metrics Using the right expertise to make full and meaningful use of your EHR investment
 Electronic Health Records and Quality Metrics Using the right expertise to make full and meaningful use of your EHR investment October 2014 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.challc.net
Electronic Health Records and Quality Metrics Using the right expertise to make full and meaningful use of your EHR investment October 2014 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.challc.net
1992 2001 Aggregate data available; release of county or case-based data requires approval by the DHMH Institutional Review Board
 50 Table 2.4 Maryland Cancer-Related base Summary: bases That Can Be Used for Cancer Surveillance base/system and/or of MD Cancer Registry Administration, Center for Cancer Surveillance and Control 410-767-5521
50 Table 2.4 Maryland Cancer-Related base Summary: bases That Can Be Used for Cancer Surveillance base/system and/or of MD Cancer Registry Administration, Center for Cancer Surveillance and Control 410-767-5521
Resource Guide. Montana. Chronic Disease Improvement. Sharing resources to build healthier lives.
 Montana Chronic Disease Improvement Resource Guide As part of a statewide effort to prevent and improve management of chronic disease, the Montana Department of Public Health & Human Services (MT DPHHS)
Montana Chronic Disease Improvement Resource Guide As part of a statewide effort to prevent and improve management of chronic disease, the Montana Department of Public Health & Human Services (MT DPHHS)
THE ROLE OF CLINICAL DECISION SUPPORT AND ANALYTICS IN IMPROVING LONG-TERM CARE OUTCOMES
 THE ROLE OF CLINICAL DECISION SUPPORT AND ANALYTICS IN IMPROVING LONG-TERM CARE OUTCOMES Long-term and post-acute care (LTPAC) organizations face unique challenges for remaining compliant and delivering
THE ROLE OF CLINICAL DECISION SUPPORT AND ANALYTICS IN IMPROVING LONG-TERM CARE OUTCOMES Long-term and post-acute care (LTPAC) organizations face unique challenges for remaining compliant and delivering
3.5% 3.0% 3.0% 2.4% Prevalence 2.0% 1.5% 1.0% 0.5% 0.0%
 S What is Heart Failure? 1,2,3 Heart failure, sometimes called congestive heart failure, develops over many years and results when the heart muscle struggles to supply the required oxygen-rich blood to
S What is Heart Failure? 1,2,3 Heart failure, sometimes called congestive heart failure, develops over many years and results when the heart muscle struggles to supply the required oxygen-rich blood to
Community Health Profile 2009
 Community Health Profile 2009 American Indian Health Services of Chicago, Inc. Chicago, IL Urban Indian Health Institute Seattle Indian Health Board PO Box 3364 Seattle, WA 98114 Ph. (206) 812-3030 Fx.
Community Health Profile 2009 American Indian Health Services of Chicago, Inc. Chicago, IL Urban Indian Health Institute Seattle Indian Health Board PO Box 3364 Seattle, WA 98114 Ph. (206) 812-3030 Fx.
Know your Numbers The D5 Goals for Diabetes Care. Shelly Hanson RN, CNS, CDE Cuyuna Regional Medical Center November 6, 2014
 Know your Numbers The D5 Goals for Diabetes Care Shelly Hanson RN, CNS, CDE Cuyuna Regional Medical Center November 6, 2014 The D5 What is it 5 different treatment goals identified for optimal diabetes
Know your Numbers The D5 Goals for Diabetes Care Shelly Hanson RN, CNS, CDE Cuyuna Regional Medical Center November 6, 2014 The D5 What is it 5 different treatment goals identified for optimal diabetes
Population Health Management Program
 Population Health Management Program Program (formerly Disease Management) is dedicated to improving our members health and quality of life. Our Population Health Management Programs aim to improve care
Population Health Management Program Program (formerly Disease Management) is dedicated to improving our members health and quality of life. Our Population Health Management Programs aim to improve care
ENGAGING PHARMACISTS IN 1305
 ENGAGING PHARMACISTS IN 1305 UTAH EXAMPLES NICOLE BISSONETTE, MPH, MCHES EPICC PROGRAM MANAGER UTAH PROJECTS INVOLVING PHARMACISTS Prior to 1305 Select Health Pharmacist Hypertension Management Team Based
ENGAGING PHARMACISTS IN 1305 UTAH EXAMPLES NICOLE BISSONETTE, MPH, MCHES EPICC PROGRAM MANAGER UTAH PROJECTS INVOLVING PHARMACISTS Prior to 1305 Select Health Pharmacist Hypertension Management Team Based
Idaho Health Home State Plan Amendment Matrix: Summary Overview. Overview of Approved Health Home SPAs
 Idaho Health Home State Plan Amendment Matrix: Summary Overview This matrix outlines key program design features from health home State Plan Amendments (SPAs) approved by the Centers for Medicare & Medicaid
Idaho Health Home State Plan Amendment Matrix: Summary Overview This matrix outlines key program design features from health home State Plan Amendments (SPAs) approved by the Centers for Medicare & Medicaid
Riverside. Program Description
 Program Description The Chronic Care Model developed by Ed Wagner, MD, director of Improving Chronic Illness Care (ICIC), a national clinical quality initiative was adopted by Kaiser Permanente (KP) Care
Program Description The Chronic Care Model developed by Ed Wagner, MD, director of Improving Chronic Illness Care (ICIC), a national clinical quality initiative was adopted by Kaiser Permanente (KP) Care
Georgia Tobacco Quit Line Sharing Best Practices Webinar Series: Accurate Coding for Maximum Reimbursement. February 20, 2014 ~ 12-12:30 p.m.
 Georgia Tobacco Quit Line Sharing Best Practices Webinar Series: Accurate Coding for Maximum Reimbursement February 20, 2014 ~ 12-12:30 p.m. 1 Tara T McAdoo, MSM Aim Lead, Physician Office Initiatives
Georgia Tobacco Quit Line Sharing Best Practices Webinar Series: Accurate Coding for Maximum Reimbursement February 20, 2014 ~ 12-12:30 p.m. 1 Tara T McAdoo, MSM Aim Lead, Physician Office Initiatives
Submitted Electronically to AdvanceNotice2016@cms.hhs.gov
 March 6, 2015 Marilyn Tavenner, RN, BSN, MHA Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services 200 Independence Avenue, SW Washington, D.C. 20201 Submitted
March 6, 2015 Marilyn Tavenner, RN, BSN, MHA Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services 200 Independence Avenue, SW Washington, D.C. 20201 Submitted
NO RECORDING OF ANY TYPE ALLOWED. Unauthorized Audiotaping or Videotaping or Distribution of any presentation materials is illegal.
 Medicare PQRS Coding With Mario Fucinari DC, MCS-P, MCS-I Certified Insurance Consultant Certified Medical Compliance Specialist (MCS-P) Sponsored by Foot Levelers The information contained in these notes
Medicare PQRS Coding With Mario Fucinari DC, MCS-P, MCS-I Certified Insurance Consultant Certified Medical Compliance Specialist (MCS-P) Sponsored by Foot Levelers The information contained in these notes
Physician Practice Connections Patient Centered Medical Home
 Physician Practice Connections Patient Centered Medical Home Getting Started Any practice assessing its ability to achieve NCQA Physician Recognition in PPC- PCMH is taking a bold step toward aligning
Physician Practice Connections Patient Centered Medical Home Getting Started Any practice assessing its ability to achieve NCQA Physician Recognition in PPC- PCMH is taking a bold step toward aligning
TOBACCO CESSATION WORKS: AN OVERVIEW OF BEST PRACTICES AND STATE EXPERIENCES
 TOBACCO CESSATION WORKS: AN OVERVIEW OF BEST PRACTICES AND STATE EXPERIENCES Despite reductions in smoking prevalence since the first Surgeon General s report on smoking in 1964, approximately 46 million
TOBACCO CESSATION WORKS: AN OVERVIEW OF BEST PRACTICES AND STATE EXPERIENCES Despite reductions in smoking prevalence since the first Surgeon General s report on smoking in 1964, approximately 46 million
Dr. Anna M. Acee, EdD, ANP-BC, PMHNP-BC Long Island University, Heilbrunn School of Nursing
 Dr. Anna M. Acee, EdD, ANP-BC, PMHNP-BC Long Island University, Heilbrunn School of Nursing Overview Depression is significantly higher among elderly adults receiving home healthcare, particularly among
Dr. Anna M. Acee, EdD, ANP-BC, PMHNP-BC Long Island University, Heilbrunn School of Nursing Overview Depression is significantly higher among elderly adults receiving home healthcare, particularly among
DRAFT Health Home Concept Paper
 DRAFT Health Home Concept Paper 1. How are health home services provided? Illinois Medicaid has been primarily a fee-for-service system, involving thousands of healthcare providers who have provided invaluable
DRAFT Health Home Concept Paper 1. How are health home services provided? Illinois Medicaid has been primarily a fee-for-service system, involving thousands of healthcare providers who have provided invaluable
Pharmacy and the Medicaid Accountable Care Organization
 RCCO Pilot Project CDC Grant Increase engagement of non-physician team members (ie., pharmacists) in Hypertension (HTN) and Diabetes Mellitus (DM) management in health care systems; Increase the proportion
RCCO Pilot Project CDC Grant Increase engagement of non-physician team members (ie., pharmacists) in Hypertension (HTN) and Diabetes Mellitus (DM) management in health care systems; Increase the proportion
Stroke: A Public Health Issue
 Stroke: A Public Health Issue American Heart Association / American Stroke Association Cryptogenic Stroke Conference Washington, DC October 9, 2015 Georges C. Benjamin, MD, MACP, FACEP(E), FNAPA Executive
Stroke: A Public Health Issue American Heart Association / American Stroke Association Cryptogenic Stroke Conference Washington, DC October 9, 2015 Georges C. Benjamin, MD, MACP, FACEP(E), FNAPA Executive
HEDIS/CAHPS 101. August 13, 2012 Minnesota Measurement and Reporting Workgroup
 HEDIS/CAHPS 101 Minnesota Measurement and Reporting Workgroup Objectives Provide introduction to NCQA Identify HEDIS/CAHPS basics Discuss various components related to HEDIS/CAHPS usage, including State
HEDIS/CAHPS 101 Minnesota Measurement and Reporting Workgroup Objectives Provide introduction to NCQA Identify HEDIS/CAHPS basics Discuss various components related to HEDIS/CAHPS usage, including State
Medicare 2015 QI Program Evaluation
 Color Code: Red does not meet 5 star threshold, or target. Green meets or exceeds 5 star threshold/target. Improving or Maintaining Physical Health (HOS) Improving or Maintaining Mental Health (HOS) Diabetes
Color Code: Red does not meet 5 star threshold, or target. Green meets or exceeds 5 star threshold/target. Improving or Maintaining Physical Health (HOS) Improving or Maintaining Mental Health (HOS) Diabetes
Implementing an RN Protocol for Uncomplicated Hypertension
 RN Hypertension Protocol Joyce Cheung, RN KP, Orange County Karen Sielbeck, RN KP, South Bay Noshin Afrookhteh, RN KP, Orange County Implementing an RN Protocol for Uncomplicated Hypertension Protocol
RN Hypertension Protocol Joyce Cheung, RN KP, Orange County Karen Sielbeck, RN KP, South Bay Noshin Afrookhteh, RN KP, Orange County Implementing an RN Protocol for Uncomplicated Hypertension Protocol
Best Practices for Optimizing Your EHR: Lessons from the Field
 American College of Physicians Internal Medicine 2014 Best Practices for Optimizing Your EHR: Lessons from the Field Faculty Moderator: Peter Basch, MD, FACP Disclosure: Has no relationship with any proprietary
American College of Physicians Internal Medicine 2014 Best Practices for Optimizing Your EHR: Lessons from the Field Faculty Moderator: Peter Basch, MD, FACP Disclosure: Has no relationship with any proprietary
Diabetes and Blood Pressure PIP Care Coordinator Toolkit. Provided by: - 1 -
 Diabetes and Blood Pressure PIP Care Coordinator Toolkit Provided by: - 1 - Project Summary MSHO/MSC+/SNBC Community & Institutionalized Blood Pressure Control for Members with Diabetes 2010 Performance
Diabetes and Blood Pressure PIP Care Coordinator Toolkit Provided by: - 1 - Project Summary MSHO/MSC+/SNBC Community & Institutionalized Blood Pressure Control for Members with Diabetes 2010 Performance
What is a Heart Attack? 1,2,3
 S What is a Heart Attack? 1,2,3 Heart attacks, otherwise known as myocardial infarctions, are caused when the blood supply to a section of the heart is suddenly disrupted. Without the oxygen supplied by
S What is a Heart Attack? 1,2,3 Heart attacks, otherwise known as myocardial infarctions, are caused when the blood supply to a section of the heart is suddenly disrupted. Without the oxygen supplied by
Butler Memorial Hospital Community Health Needs Assessment 2013
 Butler Memorial Hospital Community Health Needs Assessment 2013 Butler County best represents the community that Butler Memorial Hospital serves. Butler Memorial Hospital (BMH) has conducted community
Butler Memorial Hospital Community Health Needs Assessment 2013 Butler County best represents the community that Butler Memorial Hospital serves. Butler Memorial Hospital (BMH) has conducted community
HIMSS Davies Enterprise Application --- COVER PAGE ---
 HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
Stage 1 measures. The EP/eligible hospital has enabled this functionality
 EMR Name/Model Ingenix CareTracker - version 7 EMR Vendor Ingenix CareTracker Stage 1 objectives Use CPOE Use of CPOE for orders (any type) directly entered by authorizing provider (for example, MD, DO,
EMR Name/Model Ingenix CareTracker - version 7 EMR Vendor Ingenix CareTracker Stage 1 objectives Use CPOE Use of CPOE for orders (any type) directly entered by authorizing provider (for example, MD, DO,
3.b.i Evidence-Based Strategies for Disease Management in High Risk/Affected Populations (Adults Only)
") 3.b.i Evidence-Based Strategies for Disease Management in High Risk/Affected Populations (Adults Only) Objective: To support implementation of evidence-based best practices for disease management in medical
3.b.i Evidence-Based Strategies for Disease Management in High Risk/Affected Populations (Adults Only) Objective: To support implementation of evidence-based best practices for disease management in medical
PROGRAM OVERVIEW. Your Local Contact: Enter your org Information here
 General eligibility The H3 consortium invites small practice providers in SE Wisconsin, NE Illinois and Northern Indiana (including Indianapolis). Clinics are eligible to participate if they: Have 10 providers
General eligibility The H3 consortium invites small practice providers in SE Wisconsin, NE Illinois and Northern Indiana (including Indianapolis). Clinics are eligible to participate if they: Have 10 providers
Healthy People 2020: Who s Leading the Leading Health Indicators?
 Healthy People 2020: Who s Leading the Leading Health Indicators? Don Wright, M.D., M.P.H. Deputy Assistant Secretary for Health Promotion and Disease Prevention Who s Leading the Leading Health Indicators?
Healthy People 2020: Who s Leading the Leading Health Indicators? Don Wright, M.D., M.P.H. Deputy Assistant Secretary for Health Promotion and Disease Prevention Who s Leading the Leading Health Indicators?
Health Care Homes Certification Assessment Tool- With Examples
 Guidelines: Health Care Homes Certification Assessment Form Structure: This is the self-assessment form that HCH applicants should use to determine if they meet the requirements for HCH certification.
Guidelines: Health Care Homes Certification Assessment Form Structure: This is the self-assessment form that HCH applicants should use to determine if they meet the requirements for HCH certification.
Call-A-Nurse Location
 Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
TRENDS IN DIABETES QUALITY MEASUREMENT. Manage patients entire healthcare experience with a more comprehensive approach
 TRENDS IN DIABETES QUALITY MEASUREMENT Manage patients entire healthcare experience with a more comprehensive approach Type 2 diabetes is a complex disease that requires a multifaceted treatment approach
TRENDS IN DIABETES QUALITY MEASUREMENT Manage patients entire healthcare experience with a more comprehensive approach Type 2 diabetes is a complex disease that requires a multifaceted treatment approach
ISSUEBrief. Reducing the Burden of Smoking on Employee Health and Productivity. Center for Prevention
 Center for Prevention and Health ISSUEBrief Services Volume I, Number 5 Reducing the Burden of Smoking on Employee Health and Productivity This issue brief summarizes information presented during the fifth
Center for Prevention and Health ISSUEBrief Services Volume I, Number 5 Reducing the Burden of Smoking on Employee Health and Productivity This issue brief summarizes information presented during the fifth
Quality Improvement in Primary Care Settings
 Quality Improvement in Primary Care Settings Eboni Price Haywood, MD, MPH Chief Medical Officer, Tulane Community Health Medical Director, Tulane Community Health @ Covenant House Team Approach to Quality
Quality Improvement in Primary Care Settings Eboni Price Haywood, MD, MPH Chief Medical Officer, Tulane Community Health Medical Director, Tulane Community Health @ Covenant House Team Approach to Quality
Type 1 Diabetes ( Juvenile Diabetes)
") Type 1 Diabetes W ( Juvenile Diabetes) hat is Type 1 Diabetes? Type 1 diabetes, also known as juvenile-onset diabetes, is one of the three main forms of diabetes affecting millions of people worldwide.
Type 1 Diabetes W ( Juvenile Diabetes) hat is Type 1 Diabetes? Type 1 diabetes, also known as juvenile-onset diabetes, is one of the three main forms of diabetes affecting millions of people worldwide.
Upstate New York adults with diagnosed type 1 and type 2 diabetes and estimated treatment costs
 T H E F A C T S A B O U T Upstate New York adults with diagnosed type 1 and type 2 diabetes and estimated treatment costs Upstate New York Adults with diagnosed diabetes: 2003: 295,399 2008: 377,280 diagnosed
T H E F A C T S A B O U T Upstate New York adults with diagnosed type 1 and type 2 diabetes and estimated treatment costs Upstate New York Adults with diagnosed diabetes: 2003: 295,399 2008: 377,280 diagnosed
Clinical Decision Support as a Tool for Public Health and Healthcare Integration
 Clinical Decision Support as a Tool for Public Health and Healthcare Integration Division of Community Health Webinar September 18, 2013 The findings and conclusions in this presentation are those of the
Clinical Decision Support as a Tool for Public Health and Healthcare Integration Division of Community Health Webinar September 18, 2013 The findings and conclusions in this presentation are those of the
Medical Billing and Data Sharing
 Million Hearts Combined Clinical Data Work Groups Meeting Oct 1, 2104 ATTENDANCE (* = BY PHONE) NAME Bo Greaves, MD Jason Cunningham, DO Michelle Rosaschi Margie Gilford, MD Gary McLeod, MD Eki Abrams,
Million Hearts Combined Clinical Data Work Groups Meeting Oct 1, 2104 ATTENDANCE (* = BY PHONE) NAME Bo Greaves, MD Jason Cunningham, DO Michelle Rosaschi Margie Gilford, MD Gary McLeod, MD Eki Abrams,
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business
 Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business Quality Management Program 2012 Overview Quality Improvement
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business Quality Management Program 2012 Overview Quality Improvement