Figure 1. The challenge confronting U.S. Health Care Spending, Quality -- and the Health of the Public
|
|
|
- Elijah Robertson
- 7 years ago
- Views:
Transcription
1 Figure 1. The challenge confronting U.S. Health Care Spending, Quality -- and the Health of the Public

2 Medicare spending per enrollee (2003) Red dots indicate Wisconsin and Minnesota HRRs 12,000 Medicare spending per enrollee 10,000 8,000 6,000 Milwaukee, WI 6,304 Marshfield, WI 6,116 Rochester, MN 5,876 St. Paul, MN 5,833 Madison, WI 5,472 Minneapolis, MN 5,438 Wausau, WI 5,402 St. Cloud, MN 5,381 Neenah, WI 5,270 Duluth, MN 5,193 Green Bay, WI 5,040 La Crosse, WI 4,649 Appleton, WI 4,587 4,000

3 Inpatient + Part B spending per decedent Figure 2. Variations in spending across medical centers Variations in spending for patients with severe chronic disease across U.S. News and World Reports top 15 Honor Roll academic Medical Centers. 120, ,000 80,000 60,000 40,000 20,000 Spending per Medicare beneficiary with severe chronic disease (Last 2 years of life, ) UCLA Medical Center 72,793 New York-Presbyterian 69,962 Univ. of Pennsylvania 61,290 Johns Hopkins 60,653 UCSF Medical Center 56,859 Brigham and Womens 53,123 Univ. of Washington 50,716 Univ. of Michigan 49,367 Mass. General 47,880 Barnes-Jewish 44,463 Duke University Hosp. 37,765 Mayo Clinic (St. Mary's) 37,271 Cleveland Clinic 35,455 Most of the differences in spending are due to differences in volume (or intensity), not price. For example, 66% of the variation in spending across academic medical centers can be explained by the number of inpatient days and physician visits alone. Dartmouth Atlas of Health Care:

4 Figure 3. What does higher spending buy? Compared to the lowest spending regions, what do residents of higher spending regions get for the additional $3000 per beneficiary (in 2000)? Resource levels 1 Content / Quality of Care 1,2 Supply-sensitive services Health Outcomes 1,2 Physician-reported quality 5 Patient-reported quality 1,3 Trends over time 4 Supply-sensitive services (1) Ann Intern Med: 2003; 138: (2) Health Affairs web exclusives, October 7, 2004 (3) Health Affairs, web exclusives, Nov 16, 2005 (4) Health Affairs web exclusives, Feb 7, 2006 (5) Ann Intern Med: 2006; 144: More hospital beds per capita (32%) More medical specialists (65%) and internists (75%) Technical quality worse No more major elective surgery More hospital stays, visits, specialist use, tests, procedures Slightly higher mortality No better function Worse communication among physicians Greater difficulty ensuring continuity of care Greater difficulty providing high quality care Lower satisfaction with hospital care Worse access to primary care Lower gains in survival (following AMI) Greater growth in per-capita resource use
 More medical specialists (65%) and internists (75%) Technical quality worse No more major elective surgery More hospital stays,")
5 Figure 4. The role of supply and current payment systems Compared to the lowest spending regions (tan) the highest spending regions have 32% more beds and 65% more specialists per-capita Ann Intern Med: 2003; 138: Current payment systems reward high margin services (e.g. angioplasty) and ensure that physicians stay busy: more cardiologists per capita --> more visits Angioplasty (PCI) in Medicare Dartmouth Atlas of Health Care: Cardiologist Visits per 1,000 Medicare Enrollees R 2 = Cardiologists per 100,000 Residents
 and ensure that physicians stay busy: more cardiologists per capita --> more visits Angioplasty (PCI) in Medicare")
6 Figure 5. The role of judgment in discretionary settings For clinical services where judgment is required and no clear guidelines exist physicians in high spending regions are more likely to intervene. Percent of patients for whom physicians would recommend the intervention in low and high spending regions in each scenario: Low Spending Regions High Spending Regions Trend significant Cardiology referral for chest pain and no abnormal stress test Drug treatment of high cholesterol with yes no other risk factors Urology referral for mild symptoms of yes prostatic enlargement MRI for back pain and mildly yes abnormal nerve function Prostate cancer screening test for yes year old white male Visit for patient with isolated high blood yes pressure in 3 months or less Sirovich Archives of Internal Medicine. 165(19):2252-6, 2005 Oct 24 Sirovich, Journal of General Internal Medicine;

7 Figure 6. Why is spending higher? Why might harm occur? Clinical evidence (e.g. RCTs, guidelines) and principles of professionalism are a critically important -- but limited -- influence on clinical decision-making. Physicians practice within a local organizational context and policy environment that profoundly influences their decision-making. Payment system ensures that existing (and new capacity) is fully utilized. Physicians adapt to available resources: more referrals, more admissions, more ICU stays. Consequence: reasonable individual clinical and local decisions lead, in aggregate, to higher utilization rates, greater costs -- and inadvertently -- worse outcomes Policy Environment (e.g. payment system) Local Organizational Context (e.g. capacity - culture) The more complicated care becomes, the more likely mistakes are to occur. Hospitals are dangerous places if you don t need to be there. Clinical Evidence Professionalism Physician - Patient Encounter
 Local Organizational Context (e.")
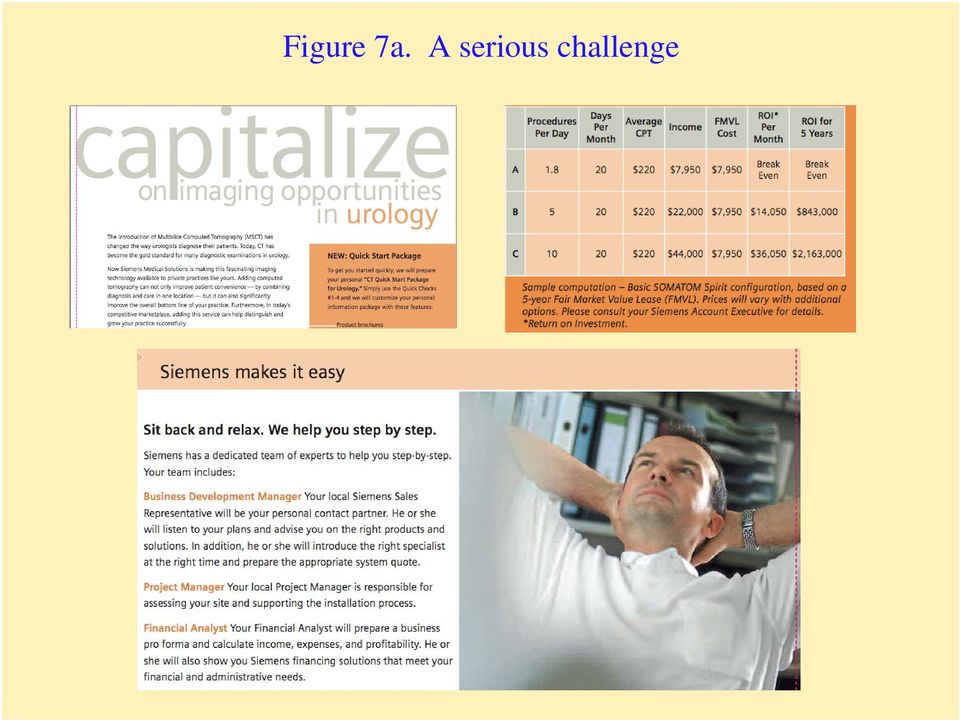
8 Figure 7a. A serious challenge
9 Figure 7b. A serious challenge CT of Pelvis -- Annual Medicare Counts Year

10 Figure 8. Potential policy levers Research priorities (comparative effectiveness) Coverage policy Performance measurement / Public reporting Payment system reform Workforce policy (medical schools, GME) Certificate of need / global budgets Policy Environment (e.g. payment system) Recruitment / practice location decisions Capital investment (hospital, outpatient) Organizational structure (hospital, MD group) Process management (QI, IT adoption) Local Organizational Context (e.g. capacity - culture) Specialty certification Graduate Medical Education Continuing Medical Education HIT for care and decision-support Patient / public education and incentives Physician - Patient Encounter

11 Figure 9. Core strategies in a market-oriented system Underlying cause General Approach Failure to recognize key role of local system (capacity, clinical culture) as driver Assumption that more is better Equating less care with rationing Foster development of local organizations (delivery systems) accountable for care (with incentives to limit future growth): ACOs Balanced information on risks / benefits Comprehensive performance measures Payment system that rewards more care, increased capacity, high margin treatments, entrepreneurial behavior Reform of payment system (long term) Shared savings as interim approach
: ACOs Balanced information on risks / benefits Comprehensive performance measures Payment system that rewards more")
12 Figure 10. Fostering organizational accountability Essential attributes of an Accountable Care Organization Sufficient size to support comprehensive performance measurement Provides (or can effectively manage) continuum of care as a real or virtually integrated local delivery system Capable of prospectively planning budgets, capacity and resource needs Potential Accountable Care Organizations Large multi-specialty group practices that own their own hospitals (Mayo, Virginia Mason, Scott White, Cleveland Clinic, Partners) Physician-Hospital Organizations / Practice Networks (Middlesex Health System) Hospitals that own physician groups (Intermountain Healthcare, many rural hospitals)
")
13 Figure 12. Accountable Care Organizations Extended Hospital Medical Staff Physician referral networks -- around local hospitals MDs with inpatient work (62%): where they do most work MDs with no inpatient work (38%): where their patients are admitted Create highly coherent virtual networks Hospitals and Associated Extended Medical Staff in Wisconsin % of Medicare Population N of Hospitals % of visits within Primary EHMS* % visits within Prim & Secondary EHMS* Large Groups (5000+ Medicare) (65-88) (77-92) Small Groups (Less than 5000) (45-80) (62-89) * Median hospital, with 10th and 90th percentiles shown below in parentheses

14 Figure 13. Why focus on developing ACO s? Most physicians already practice within virtual ACOs Virtually all MDs (95%) and Medicare beneficiaries (93%) can be assigned based on claims data to their local hospital and its medical staff Most care is already delivered within these virtual multi-specialty groups Modest incentives might prompt physicians to establish formal organizations that would not have to disrupt their current practices or patient care. Performance measurement more tractable in the near term All physicians could be included in measurement with adequate sample sizes, less difficulty in attribution. Diverse and important measures are feasible (see Figure 14). ACOs more likely to have capacity to invest in improvement: electronic health records, care management, etc Fisher et al. Creating Accountable Care Organizations: The Extended Hospital Medical Staff Health Affairs; Published online, 12/05/06

15 Figure 14: Feasibility of performance measurement US average performance, stratified by regional intensity* Low Spending High Spending Ratio High to Low Mammography Eye exams, diabetes HBA1c, diabetes Hospital Discharges SNF stays Care transitions Physician services** Acute care hospital $2,085 $2,086 $3,295 $2, * Regional intensity defined using end-of-life intensity index ** Physician and hospital spending calculated using standardized national prices (spending and utilization data are age-sex-race adjusted)

16 Figure 15: Growth in spending can be measured Per-beneficiary spending in EHMS (n = 4772) sorted into quintiles by magnitude of per-beneficiary growth ( ) $4000 Absolute increase per benef. Percent increase ** Average Annual Rate $936 46% 9.9% Average spending* on MD services per beneficiary at EHMS $3000 $675 $551 $431 33% 27% 21% 7.3% 6.1% 4.8% $2000 $198 10% 2.4% * Using standardized payments, using 2003 RVU ** Percent increase calculated relative to average 1999 per-beneficiary spending

17 Figure 16. Summary: It takes a community Reforming health care through shared accountability and payment reform The Paradox of Plenty: In medicine, more isn t better Why not? Underlying causes of the current mess Lack of accountability: for capacity, care coordination, quality Inadequate information: about biotechnology and care delivery A toxic payment system: Prescription for change: a broader conceptual model Foster organizational accountability: ACOs Better information: especially on care delivery (NQF) Reform payment: shared savings for participating ACOs

Accountable Care Organizations
 Accountable Care Organizations June 10, 2008 Elliott Fisher, MD, MPH The Dartmouth Institute for Health Policy and Clinical Practice How can the best medical care in the world cost twice as much as the
Accountable Care Organizations June 10, 2008 Elliott Fisher, MD, MPH The Dartmouth Institute for Health Policy and Clinical Practice How can the best medical care in the world cost twice as much as the
CECS. Creating Accountable Care Organizations Why the Extended Hospital Medical Staff?
 Creating Accountable Care Organizations Why the Extended Hospital Medical Staff? CECS Center for the Evaluative Clinical Sciences Elliott S. Fisher, MD, MPH Professor of Medicine Center for the Evaluative
Creating Accountable Care Organizations Why the Extended Hospital Medical Staff? CECS Center for the Evaluative Clinical Sciences Elliott S. Fisher, MD, MPH Professor of Medicine Center for the Evaluative
Health Care Spending, Quality, and Outcomes
 Health Care Spending, Quality, and Outcomes More Isn t Always Better A Dartmouth Atlas Project Topic Brief February 27, 2009 Elliott Fisher, MD, MPH David Goodman, MD, MS Jonathan Skinner, PhD Kristen
Health Care Spending, Quality, and Outcomes More Isn t Always Better A Dartmouth Atlas Project Topic Brief February 27, 2009 Elliott Fisher, MD, MPH David Goodman, MD, MS Jonathan Skinner, PhD Kristen
Accountable Care Organizations: Forging Stakeholder Partnerships for Health Care Performance and Efficiency
 Accountable Care Organizations: Forging Stakeholder Partnerships for Health Care Performance and Efficiency Julie Lewis Director of Health Policy Dartmouth Institute for Health Policy and Clinical Practice
Accountable Care Organizations: Forging Stakeholder Partnerships for Health Care Performance and Efficiency Julie Lewis Director of Health Policy Dartmouth Institute for Health Policy and Clinical Practice
Geographic Differences in Healthcare Utilization: Moving Forward. Allen J. Taylor MD FACC FAHA
 Geographic Differences in Healthcare Utilization: Moving Forward Allen J. Taylor MD FACC FAHA Director, Advanced Cardiovascular Imaging Washington Hospital Center Professor of Medicine Georgetown University
Geographic Differences in Healthcare Utilization: Moving Forward Allen J. Taylor MD FACC FAHA Director, Advanced Cardiovascular Imaging Washington Hospital Center Professor of Medicine Georgetown University
MedInsight Healthcare Analytics Brief: Population Health Management Concepts
 Milliman Brief MedInsight Healthcare Analytics Brief: Population Health Management Concepts WHAT IS POPULATION HEALTH MANAGEMENT? Population health management has been an industry concept for decades,
Milliman Brief MedInsight Healthcare Analytics Brief: Population Health Management Concepts WHAT IS POPULATION HEALTH MANAGEMENT? Population health management has been an industry concept for decades,
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY
 A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
Accountable Care Organizations and Behavioral Health. Indiana Council of Community Mental Health Centers October 11, 2012
 Accountable Care Organizations and Behavioral Health Indiana Council of Community Mental Health Centers October 11, 2012 What is an ACO? An accountable care organization is a group of providers or suppliers
Accountable Care Organizations and Behavioral Health Indiana Council of Community Mental Health Centers October 11, 2012 What is an ACO? An accountable care organization is a group of providers or suppliers
Measuring and Assigning Accountability for Healthcare Spending
 Measuring and Assigning Accountability for Healthcare Spending Fair and Effective Ways to Analyze the Drivers of Healthcare Costs and Transition to Value-Based Payment Harold D. Miller CONTENTS EXECUTIVE
Measuring and Assigning Accountability for Healthcare Spending Fair and Effective Ways to Analyze the Drivers of Healthcare Costs and Transition to Value-Based Payment Harold D. Miller CONTENTS EXECUTIVE
How To Hold A Hospital And Extended Medical Staff Accountable For A Patient'S Care
 Hospitals & Physicians Creating Accountable Care Organizations: The Extended Hospital Medical Staff A new approach to organizing care and ensuring accountability. by Elliott S. Fisher, Douglas O. Staiger,
Hospitals & Physicians Creating Accountable Care Organizations: The Extended Hospital Medical Staff A new approach to organizing care and ensuring accountability. by Elliott S. Fisher, Douglas O. Staiger,
Co-management (Service Line Agreement 2007)
") Co-management (Service Line Agreement 2007) Orthopedics Neuroscience Cardiology Cardiovascular Surgery Collaboration on a different level Tactical method of increasing alignment and collaboration Agreement
Co-management (Service Line Agreement 2007) Orthopedics Neuroscience Cardiology Cardiovascular Surgery Collaboration on a different level Tactical method of increasing alignment and collaboration Agreement
Care Delivery Transformation in Academic Health Centers
 Care Delivery Transformation in Academic Health Centers William B. Borden, MD Associate Professor of Medicine Director of Healthcare Delivery Transformation George Washington University Chest pain 67 year
Care Delivery Transformation in Academic Health Centers William B. Borden, MD Associate Professor of Medicine Director of Healthcare Delivery Transformation George Washington University Chest pain 67 year
Cornerstone Health Care s ACO Playbook. Grace E. Terrell, MD January 17, 2012
 Cornerstone Health Care s ACO Playbook Grace E. Terrell, MD January 17, 2012 Mission: To be your medical home Vision: To be the model for physician-led health care in America Values: As a physician owned
Cornerstone Health Care s ACO Playbook Grace E. Terrell, MD January 17, 2012 Mission: To be your medical home Vision: To be the model for physician-led health care in America Values: As a physician owned
May 9, 2013. FaithAnn Amond, RN Navigator Care Central Ellis Medicine
 A Systems Approach to Diabetes Care Hospital to Home. Improving Care Transitions and Outcomes Helen Hayes Hospital West Haverstraw, NY James Desemone, MD Director of Medical Staff Quality Diabetes and
A Systems Approach to Diabetes Care Hospital to Home. Improving Care Transitions and Outcomes Helen Hayes Hospital West Haverstraw, NY James Desemone, MD Director of Medical Staff Quality Diabetes and
HealthPartners: Triple Aim Approach to ACO Development
 HealthPartners: Triple Aim Approach to ACO Development Brian Rank, MD Medical Director, HealthPartners Medical Group October 27, 2010 HealthPartners Integrated Care and Financing System 10,300 employees
HealthPartners: Triple Aim Approach to ACO Development Brian Rank, MD Medical Director, HealthPartners Medical Group October 27, 2010 HealthPartners Integrated Care and Financing System 10,300 employees
Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed?
 Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed? Accountable Care Organizations: Implications for Consumers October 14, 2010 Washington, DC Sam Nussbaum, M.D. Executive Vice
Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed? Accountable Care Organizations: Implications for Consumers October 14, 2010 Washington, DC Sam Nussbaum, M.D. Executive Vice
NewYork-Presbyterian 2012 Summer Internship
 NewYork-Presbyterian 2012 Summer Internship 1 Introductions Monica Chopra, MBA, MPH Revenue Cycle Black Belt, Revenue Cycle & Finance Johns Hopkins University, BA graduate, 2000 Carey School of Business/Johns
NewYork-Presbyterian 2012 Summer Internship 1 Introductions Monica Chopra, MBA, MPH Revenue Cycle Black Belt, Revenue Cycle & Finance Johns Hopkins University, BA graduate, 2000 Carey School of Business/Johns
Accountable Care Organizations: An old idea with new potential. Stephen E. Whitney, MD, MBA Testimony to Senate State Affairs September 22, 2010
 Accountable Care Organizations: An old idea with new potential Stephen E. Whitney, MD, MBA Testimony to Senate State Affairs September 22, 2010 Impetus for ACO Formation Increased health care cost From
Accountable Care Organizations: An old idea with new potential Stephen E. Whitney, MD, MBA Testimony to Senate State Affairs September 22, 2010 Impetus for ACO Formation Increased health care cost From
A COMPARISON OF MEDI-CAL MANAGED CARE P4P MEASURE SETS
 A COMPARISON OF MEDI-CAL MANAGED CARE P4P MEASURE SETS The matrix below provides a comparison of all measures included in Medi-Cal P4P programs and the measures includes in DHCS s External Accountability
A COMPARISON OF MEDI-CAL MANAGED CARE P4P MEASURE SETS The matrix below provides a comparison of all measures included in Medi-Cal P4P programs and the measures includes in DHCS s External Accountability
Quality and Efficiency of Care Improved with Analytics and Workflow Redesign
 Quality and Efficiency of Care Improved with Analytics and Workflow Redesign London Health and Care Leaders Forum June 2, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group
Quality and Efficiency of Care Improved with Analytics and Workflow Redesign London Health and Care Leaders Forum June 2, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group
Accountable Care Organizations: What Are They and Why Should I Care?
 Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
A Foundation for Health Care Reform Legislation
 A Foundation for Health Care Reform Legislation Mayo Clinic s Point of View Mayo Clinic believes that U.S. health care urgently needs reform to ensure access to quality, affordable patient care. Each major
A Foundation for Health Care Reform Legislation Mayo Clinic s Point of View Mayo Clinic believes that U.S. health care urgently needs reform to ensure access to quality, affordable patient care. Each major
Sharp HealthCare ACO. Pioneer Introduction to the FSSB November 8, 2012
 Sharp HealthCare ACO Pioneer Introduction to the FSSB November 8, 2012 Sharp HealthCare Not-for-profit serving 3.1 million residents of San Diego County Grew from one hospital in 1955 to an integrated
Sharp HealthCare ACO Pioneer Introduction to the FSSB November 8, 2012 Sharp HealthCare Not-for-profit serving 3.1 million residents of San Diego County Grew from one hospital in 1955 to an integrated
Home Health Care Today: Higher Acuity Level of Patients Highly skilled Professionals Costeffective Uses of Technology Innovative Care Techniques
 Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
After Hospitalization:
 After Hospitalization: A Dartmouth Atlas Report on Post-Acute Care for Medicare Beneficiaries A Report of the Dartmouth Atlas Project After Hospitalization: A Dartmouth Atlas Report on Post-Acute Care
After Hospitalization: A Dartmouth Atlas Report on Post-Acute Care for Medicare Beneficiaries A Report of the Dartmouth Atlas Project After Hospitalization: A Dartmouth Atlas Report on Post-Acute Care
Are You a Hospital Inpatient or Outpatient?
 Are You a Hospital Inpatient or Outpatient? If You Have Medicare Ask! Revised May 2014 Did you know that even if you stay in a hospital overnight, you might still be considered an outpatient? Your hospital
Are You a Hospital Inpatient or Outpatient? If You Have Medicare Ask! Revised May 2014 Did you know that even if you stay in a hospital overnight, you might still be considered an outpatient? Your hospital
CMS Next Generation ACO Model. Payment Models Work Group April 20 th, 2015
 CMS Next Generation ACO Model Payment Models Work Group April 20 th, 2015 1 Why is there a new ACO model? To address concerns about certain design elements of the existing Pioneer Program and the MSSP
CMS Next Generation ACO Model Payment Models Work Group April 20 th, 2015 1 Why is there a new ACO model? To address concerns about certain design elements of the existing Pioneer Program and the MSSP
Financial Implications: The Push from Inpatient to Outpatient Care
 Financial Implications: The Push from Inpatient to Outpatient Care Brian Baumgardner & Mitchell Mongell THE TRANSFORMATION TO CONSUMER-DRIVEN HEALTHCARE FINANCIAL IMPLICATIONS:THE PUSH FROM INPATIENT TO
Financial Implications: The Push from Inpatient to Outpatient Care Brian Baumgardner & Mitchell Mongell THE TRANSFORMATION TO CONSUMER-DRIVEN HEALTHCARE FINANCIAL IMPLICATIONS:THE PUSH FROM INPATIENT TO
Data Shows Reduction in Medicare Hospital Readmission Rates During 2012
 Medicare & Medicaid Research Review 2013: Volume 3, Number 2 A publication of the Centers for Medicare & Medicaid Services, Office of Information Products & Data Analytics Data Shows Reduction in Medicare
Medicare & Medicaid Research Review 2013: Volume 3, Number 2 A publication of the Centers for Medicare & Medicaid Services, Office of Information Products & Data Analytics Data Shows Reduction in Medicare
New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers
 New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers October 28, 2011 Timothy G Ferris, MD, MPH Mass General Physicians Organization, Medical Director Associate Professor,
New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers October 28, 2011 Timothy G Ferris, MD, MPH Mass General Physicians Organization, Medical Director Associate Professor,
How We Make Sure You Get the Best Health Care
 How We Make Sure You Get the Best Health Care Table of Contents Quality Improvement... 1 Care Management... 2 Utilization Management: Working to Get You Covered and Necessary Care... 3 Behavioral Health...
How We Make Sure You Get the Best Health Care Table of Contents Quality Improvement... 1 Care Management... 2 Utilization Management: Working to Get You Covered and Necessary Care... 3 Behavioral Health...
National Medicare Readmission. Centers for Medicare and Medicare Services
 National Medicare Readmission Findings: Recent Data and Trends Office of Information Products and Data Analytics Office of Information Products and Data Analytics Centers for Medicare and Medicare Services
National Medicare Readmission Findings: Recent Data and Trends Office of Information Products and Data Analytics Office of Information Products and Data Analytics Centers for Medicare and Medicare Services
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION)
") ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
Atrius Health ACO Initiative. Agenda
 Atrius Health ACO Initiative November 9, 2012 Mark Yurkofsky MD Mark_yurkofsky@vmed.org 11/13/2012 1 Agenda Why the interest in the Pioneer ACO? What actually is Pioneer ACO anyway? What is Atrius Health?
Atrius Health ACO Initiative November 9, 2012 Mark Yurkofsky MD Mark_yurkofsky@vmed.org 11/13/2012 1 Agenda Why the interest in the Pioneer ACO? What actually is Pioneer ACO anyway? What is Atrius Health?
Using Medicare Hospitalization Information and the MedPAR. Beth Virnig, Ph.D. Associate Dean for Research and Professor University of Minnesota
 Using Medicare Hospitalization Information and the MedPAR Beth Virnig, Ph.D. Associate Dean for Research and Professor University of Minnesota MedPAR Medicare Provider Analysis and Review Includes information
Using Medicare Hospitalization Information and the MedPAR Beth Virnig, Ph.D. Associate Dean for Research and Professor University of Minnesota MedPAR Medicare Provider Analysis and Review Includes information
Model for a Virtual ACO
 Today Tomorrow Model for a Virtual ACO An Emerging Primary care Based Multi- specialty Virtual ACO Responding to Need Small practices operate in isolation Can t t compete with hospital-based delivery systems
Today Tomorrow Model for a Virtual ACO An Emerging Primary care Based Multi- specialty Virtual ACO Responding to Need Small practices operate in isolation Can t t compete with hospital-based delivery systems
Accountable Care Organization
 Accountable Care Organization April 13, 2011 The Indianapolis Association of Health Underwriters Drivers of Payment Reform Increased attention to regional variation in costs and quality Payment for care
Accountable Care Organization April 13, 2011 The Indianapolis Association of Health Underwriters Drivers of Payment Reform Increased attention to regional variation in costs and quality Payment for care
Early Results of a Marketwide ACO Initiative: The Alternative Quality Contract (AQC)
") Early Results of a Marketwide ACO Initiative: The Alternative Quality Contract (AQC) Dana Gelb Safran, Sc.D. Senior Vice President Performance Measurement and Improvement 13 July 2011 Twin Goals of Improving
Early Results of a Marketwide ACO Initiative: The Alternative Quality Contract (AQC) Dana Gelb Safran, Sc.D. Senior Vice President Performance Measurement and Improvement 13 July 2011 Twin Goals of Improving
CMS - ACO Transitions Program
 CMS - ACO Transitions Program March 2011 Thomas R Graf MD Our Legacy Make my hospital right, make it the best. Abigail Geisinger 1827-1921 Geisinger Quality Striving for Perfection Geisinger Health System
CMS - ACO Transitions Program March 2011 Thomas R Graf MD Our Legacy Make my hospital right, make it the best. Abigail Geisinger 1827-1921 Geisinger Quality Striving for Perfection Geisinger Health System
7/31/2014. Medicare Advantage: Time to Re-examine Your Engagement Strategy. Avalere Health. Eric Hammelman, CFA. Overview
 Medicare Advantage: Time to Re-examine Your Engagement Strategy July 2014 avalerehealth.net Avalere Health Avalere Health delivers research, analysis, insight & strategy to leaders in healthcare policy
Medicare Advantage: Time to Re-examine Your Engagement Strategy July 2014 avalerehealth.net Avalere Health Avalere Health delivers research, analysis, insight & strategy to leaders in healthcare policy
Improving Quality and Curbing Health Care Spending: Opportunities for the Congress and the Obama Administration
 An Agenda for Change Improving Quality and Curbing Health Care Spending: Opportunities for the Congress and the Obama Administration Medicare Spending per Beneficiary, 2005 $8,600 to $14,360 $7,800 to
An Agenda for Change Improving Quality and Curbing Health Care Spending: Opportunities for the Congress and the Obama Administration Medicare Spending per Beneficiary, 2005 $8,600 to $14,360 $7,800 to
Online Provider/Pharmacy Directory: New Guidelines and Requirements
 Vol. 3, No. 3 PROVIDER PULSE October - 2015 In This Issue New Guidelines... page 1 Provider Portal...page 2 Part D...page 2 Medical Services... page 3 Quality...page 4 Claims/New Rep...page 5 Online Provider/Pharmacy
Vol. 3, No. 3 PROVIDER PULSE October - 2015 In This Issue New Guidelines... page 1 Provider Portal...page 2 Part D...page 2 Medical Services... page 3 Quality...page 4 Claims/New Rep...page 5 Online Provider/Pharmacy
The Affordable Care Act
 The Affordable Care Act What does it mean for internists? Joshua Becker MD 10/14/2015 VII. 2015 Reforms and Beyond Payment Penalties under Medicare s Pay-for-Reporting Program Value-Based Payment Modifier
The Affordable Care Act What does it mean for internists? Joshua Becker MD 10/14/2015 VII. 2015 Reforms and Beyond Payment Penalties under Medicare s Pay-for-Reporting Program Value-Based Payment Modifier
The Value Quadrant of Healthcare Reform. 2008 Pharos Innovations, LLC. All Rights Reserved.
 The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
Nuts and Bolts Accountable Care Organizations: A New Care Delivery Model for New Expectations
 Nuts and Bolts Accountable Care Organizations: A New Care Delivery Model for New Expectations Presented to The American College of Cardiology October 27, 2012 1 Franciscan Alliance Overview Franciscan
Nuts and Bolts Accountable Care Organizations: A New Care Delivery Model for New Expectations Presented to The American College of Cardiology October 27, 2012 1 Franciscan Alliance Overview Franciscan
MGMA ACA Exchange Implementation Survey Report. May 2014
 MGMA ACA Exchange Implementation Survey Report May 2014 Overview Medical Group Management Association (MGMA) conducted member research in April 2014 to better understand the impact of the Affordable Care
MGMA ACA Exchange Implementation Survey Report May 2014 Overview Medical Group Management Association (MGMA) conducted member research in April 2014 to better understand the impact of the Affordable Care
STRATEGIC INNOVATIONS FOR AFFORDABLE, SUSTAINABLE HEALTH CARE:
 January 2011 STRATEGIC INNOVATIONS FOR AFFORDABLE, SUSTAINABLE HEALTH CARE: A Model for Health System Reform Environmental Scan Accountable Care Organizations Table of Contents ACCOUNTABLE CARE ORGANIZATIONS...
January 2011 STRATEGIC INNOVATIONS FOR AFFORDABLE, SUSTAINABLE HEALTH CARE: A Model for Health System Reform Environmental Scan Accountable Care Organizations Table of Contents ACCOUNTABLE CARE ORGANIZATIONS...
What do ACO s and Hospitals want from SNF s and CCRC s
 What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
Initial Preventive Physical Examination
 Initial Preventive Physical Examination Overview The Medicare Prescription Drug, Improvement, and Modernization Act (MMA) of 2003 expanded Medicare's coverage of preventive services. Central to the Centers
Initial Preventive Physical Examination Overview The Medicare Prescription Drug, Improvement, and Modernization Act (MMA) of 2003 expanded Medicare's coverage of preventive services. Central to the Centers
Observation Coding and Billing
 How do you get paid? Observation Coding and Billing Michael Ross MD FACEP President, Society of Chest Pain Centers Medical Director, Chest Pain Center and Observation Medicine Associate Professor, Department
How do you get paid? Observation Coding and Billing Michael Ross MD FACEP President, Society of Chest Pain Centers Medical Director, Chest Pain Center and Observation Medicine Associate Professor, Department
A Comprehensive Strategy for Coordinating the Care for Patients with Coronary Artery Disease (CAD) and Other Chronic Medical Conditions
 and Other Chronic Medical Conditions") A Comprehensive Strategy for Coordinating the Care for Patients with Coronary Artery Disease (CAD) and Other Chronic Medical Conditions Presented at the Integrated Healthcare Association Meeting Los Angeles,
A Comprehensive Strategy for Coordinating the Care for Patients with Coronary Artery Disease (CAD) and Other Chronic Medical Conditions Presented at the Integrated Healthcare Association Meeting Los Angeles,
Partnerships for Population Health 9/23/2013
 Partnerships for Population Health 9/23/2013 Barbara McCann, Chief Industry Officer, Interim HealthCare Brian Silverstein, MD, President, HC Wisdom Amanda Twiss, President, Garnet Advisors 1 Continuum
Partnerships for Population Health 9/23/2013 Barbara McCann, Chief Industry Officer, Interim HealthCare Brian Silverstein, MD, President, HC Wisdom Amanda Twiss, President, Garnet Advisors 1 Continuum
Compensation 2013: Evolving Models, Emerging Approaches
 Compensation 2013: Evolving Models, Emerging Approaches Results from the AMGA 2013 Medical Group Compensation and Financial Survey By Bradley S.J. Vaudrey, M.B.A., CPA, and Sara Loos, CCP Findings from
Compensation 2013: Evolving Models, Emerging Approaches Results from the AMGA 2013 Medical Group Compensation and Financial Survey By Bradley S.J. Vaudrey, M.B.A., CPA, and Sara Loos, CCP Findings from
Variations in Spending and Quality The Journey to Accountable Care
 Variations in Spending and Quality The Journey to Accountable Care Elliott Fisher, MD, MPH Director, The Dartmouth Institute for Health Policy and Clinical Practice John E. Wennberg Distinguished Professor,
Variations in Spending and Quality The Journey to Accountable Care Elliott Fisher, MD, MPH Director, The Dartmouth Institute for Health Policy and Clinical Practice John E. Wennberg Distinguished Professor,
Accountable Care Organizations. Rick Shinto, MD Aveta Health Inc. July 20, 2010
 Accountable Care Organizations Rick Shinto, MD Aveta Health Inc. July 20, 2010 1 Health Care Reform- New Models of Care Patient Protection and Affordable care Act (PPACA 2010) controlling costs and improving
Accountable Care Organizations Rick Shinto, MD Aveta Health Inc. July 20, 2010 1 Health Care Reform- New Models of Care Patient Protection and Affordable care Act (PPACA 2010) controlling costs and improving
5/10/13 HEALTH CARE REFORM LONGITUDINAL CARE COORDINATION HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO WHY WHAT HOW WHEN WHO
 TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
Don t Delay Hospice Care Referrals
 Don t Delay Hospice Care Referrals Timely hospice admissions provide greater benefits. Among the Medicare population, about nine out of 10 deaths are associated with chronic illnesses, such as cancer,
Don t Delay Hospice Care Referrals Timely hospice admissions provide greater benefits. Among the Medicare population, about nine out of 10 deaths are associated with chronic illnesses, such as cancer,
Rural Health Advisory Committee s Rural Obstetric Services Work Group
 Rural Health Advisory Committee s Rural Obstetric Services Work Group Nov. 30th webinar topic: Training and residency issues for rural obstetric providers in Minnesota Audio: 888-742-5095, conference code
Rural Health Advisory Committee s Rural Obstetric Services Work Group Nov. 30th webinar topic: Training and residency issues for rural obstetric providers in Minnesota Audio: 888-742-5095, conference code
Medicaid Health Plans: Adding Value for Beneficiaries and States
 Medicaid Health Plans: Adding Value for Beneficiaries and States Medicaid is a program with numerous challenges, both for its beneficiaries and the state and federal government. In comparison to the general
Medicaid Health Plans: Adding Value for Beneficiaries and States Medicaid is a program with numerous challenges, both for its beneficiaries and the state and federal government. In comparison to the general
Understanding Group Health Insurance Anthem KeyCare 15+ Plan
 Understanding Group Health Insurance Anthem KeyCare 15+ Plan January 12, 2010 Although it is the intent of the University to continue current benefit plans, the University reserves the right to modify,
Understanding Group Health Insurance Anthem KeyCare 15+ Plan January 12, 2010 Although it is the intent of the University to continue current benefit plans, the University reserves the right to modify,
Summary Evaluation of the Medicare Lifestyle Modification Program Demonstration and the Medicare Cardiac Rehabilitation Benefit
 The Centers for Medicare & Medicaid Services' Office of Research, Development, and Information (ORDI) strives to make information available to all. Nevertheless, portions of our files including charts,
The Centers for Medicare & Medicaid Services' Office of Research, Development, and Information (ORDI) strives to make information available to all. Nevertheless, portions of our files including charts,
WILL EQUITY BE ACHIEVED THROUGH HEALTH CARE REFORM? John Z. Ayanian, MD, MPP
 WILL EQUITY BE ACHIEVED THROUGH HEALTH CARE REFORM? John Z. Ayanian, MD, MPP Brigham and Women s Hospital Harvard Medical School Harvard School of Public Health BWH Patient-Centered Outcomes Seminar April
WILL EQUITY BE ACHIEVED THROUGH HEALTH CARE REFORM? John Z. Ayanian, MD, MPP Brigham and Women s Hospital Harvard Medical School Harvard School of Public Health BWH Patient-Centered Outcomes Seminar April
PHYSICIANS. 202.420.7896 888 16 th St. NW, Suite 800, Washington DC 20006 www.npalliance.org
 N A T I O N A L PHYSICIANS A L L I A N C E My name is Dr. Valerie Arkoosh. I am an Anesthesiologist at the University of Pennsylvania School of Medicine and the President of the National Physicians Alliance.
N A T I O N A L PHYSICIANS A L L I A N C E My name is Dr. Valerie Arkoosh. I am an Anesthesiologist at the University of Pennsylvania School of Medicine and the President of the National Physicians Alliance.
CMS Quality Measurement and Value Based Purchasing Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 CMS Quality Measurement and Value Based Purchasing Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS American Urological Association Quality Improvement Summit
CMS Quality Measurement and Value Based Purchasing Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS American Urological Association Quality Improvement Summit
Triple aim of ACA. Shanty Creek, November 2015. 1. Improved patient experience easier acess 2. Improved quality of healthcare 3.
 Theresa Anderson, West Shore Medical Center Tracey Chappel, West Shore Medical Center Ingemar Johansson, Centra Wellness Network Shanty Creek, November 2015 Triple aim of ACA 1. Improved patient experience
Theresa Anderson, West Shore Medical Center Tracey Chappel, West Shore Medical Center Ingemar Johansson, Centra Wellness Network Shanty Creek, November 2015 Triple aim of ACA 1. Improved patient experience
Pushing the Envelope of Population Health
 Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
Making ACOs Work for You. By Gregory A Culley, MD
 Making ACOs Work for You By Gregory A Culley, MD The continuing increase in medical costs has created a renewed interest in changing the payment method for healthcare providers. In some ways, everything
Making ACOs Work for You By Gregory A Culley, MD The continuing increase in medical costs has created a renewed interest in changing the payment method for healthcare providers. In some ways, everything
AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Verificatoin Criterea EFFECTIVE JANUARY 1, 2015. Criterion. Level (1 or 2) Number
 Number") Criterion AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Criterion Level (1 or 2) Number Criterion BURN CENTER ADMINISTRATION 1. The burn center hospital is currently accredited by The
Criterion AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Criterion Level (1 or 2) Number Criterion BURN CENTER ADMINISTRATION 1. The burn center hospital is currently accredited by The
Health Care Reform: Seizing the Opportunity to Transform the Care Delivery System for Our Elders
 May 5, 2011 Health Care Reform: Seizing the Opportunity to Transform the Care Delivery System for Our Elders WAHSA 2011 Spring Conference & Annual Business Meeting: New Thoughts, New Directions Kathleen
May 5, 2011 Health Care Reform: Seizing the Opportunity to Transform the Care Delivery System for Our Elders WAHSA 2011 Spring Conference & Annual Business Meeting: New Thoughts, New Directions Kathleen
Accountability and Innovation in Care Delivery Models
 Accountability and Innovation in Care Delivery Models Lisa McDonnel Senior Vice President, Network Strategy & Innovation, United Healthcare November 6, 2015 Today s discussion topics Vision Our strategic
Accountability and Innovation in Care Delivery Models Lisa McDonnel Senior Vice President, Network Strategy & Innovation, United Healthcare November 6, 2015 Today s discussion topics Vision Our strategic
UnitedHealth Premium Designation Program. Driving informed choices and quality, efficient care
 UnitedHealth Premium Designation Program Driving informed choices and quality, efficient care Today s health care system is fraught with wide variation in medical practices that often result in inconsistent
UnitedHealth Premium Designation Program Driving informed choices and quality, efficient care Today s health care system is fraught with wide variation in medical practices that often result in inconsistent
Reforming Provider Payments:
 Reforming Provider Payments: A Critical Step for Better Health Care and Lower Costs Aaron McKethan, PhD Engelberg Center for Health Care Reform The Brookings Institution January 8, 2010 Regional Variations
Reforming Provider Payments: A Critical Step for Better Health Care and Lower Costs Aaron McKethan, PhD Engelberg Center for Health Care Reform The Brookings Institution January 8, 2010 Regional Variations
how to choose the health plan that s right for you
 how to choose the health plan that s right for you It s easy to feel a little confused about where to start when choosing a health plan. Some people ask their friends, family, or co-workers for advice.
how to choose the health plan that s right for you It s easy to feel a little confused about where to start when choosing a health plan. Some people ask their friends, family, or co-workers for advice.
A Call to Duty. Transforming Veteran s End-of-Life Care. Julie Benson, MD. Medical Director Hospice and Palliative Care. Jessica Martensen, RN
 A Call to Duty Transforming Veteran s End-of-Life Care Julie Benson, MD Medical Director Hospice and Palliative Care Jessica Martensen, RN Director, Home Care and Hospice Lakewood Health System Staples,
A Call to Duty Transforming Veteran s End-of-Life Care Julie Benson, MD Medical Director Hospice and Palliative Care Jessica Martensen, RN Director, Home Care and Hospice Lakewood Health System Staples,
Health Literacy and Palliative Care Nursing Perspective
 Health Literacy and Palliative Care Nursing Perspective Ginger Marshall, MSN, ACNP-BC, ACHPN, FPCN President Elect, Hospice Palliative Nurses Association National Director of Palliative Care for Compassus
Health Literacy and Palliative Care Nursing Perspective Ginger Marshall, MSN, ACNP-BC, ACHPN, FPCN President Elect, Hospice Palliative Nurses Association National Director of Palliative Care for Compassus
Statement of Robert A. Greene, MD National Vice President, Clinical Analytics UnitedHealthcare
 Statement of Robert A. Greene, MD National Vice President, Clinical Analytics UnitedHealthcare Before the Quality Measures and Clinical Quality Workgroups May 19, 2011 Greene UHC QMWG Statement May 19
Statement of Robert A. Greene, MD National Vice President, Clinical Analytics UnitedHealthcare Before the Quality Measures and Clinical Quality Workgroups May 19, 2011 Greene UHC QMWG Statement May 19
BACKGROUND ON ALLINA AND UNITED HOSPITAL
 BACKGROUND ON ALLINA AND UNITED HOSPITAL Allina Health System ("Allina") is a Minnesota nonprofit corporation which, together with its subsidiaries, delivers health care services to patients in Minnesota
BACKGROUND ON ALLINA AND UNITED HOSPITAL Allina Health System ("Allina") is a Minnesota nonprofit corporation which, together with its subsidiaries, delivers health care services to patients in Minnesota
Challenges Recruiting and Retaining Healthcare Providers
 Challenges Recruiting and Retaining Healthcare Providers A Surplus of Doctors?? For the past 25 years, the AMA and other industry groups have predicted an excess of doctors and worked to limit the number
Challenges Recruiting and Retaining Healthcare Providers A Surplus of Doctors?? For the past 25 years, the AMA and other industry groups have predicted an excess of doctors and worked to limit the number
The Health of Canada s Health Care System M D, M H A, C C F P, F C F P
 The Health of Canada s Health Care System D r. Stewart Kennedy, M D, M H A, C C F P, F C F P E x ecutive Vice President, M edicine and Academics T hunder Bay Regional Health S c i ences Centre Biographical
The Health of Canada s Health Care System D r. Stewart Kennedy, M D, M H A, C C F P, F C F P E x ecutive Vice President, M edicine and Academics T hunder Bay Regional Health S c i ences Centre Biographical
How To Reduce Hospital Readmission
 Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
A Journey to Improve Canada s Healthcare System
 A Journey to Improve Canada s Healthcare System The Quest Can a public/private hospital system coexist and thrive and improve Canada s system? The Journey Visited Australia and New Zealand to find out
A Journey to Improve Canada s Healthcare System The Quest Can a public/private hospital system coexist and thrive and improve Canada s system? The Journey Visited Australia and New Zealand to find out
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT
 ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
Accountable Care for Pharmacy Executives
 Accountable Care for Pharmacy Executives A Prescription for Change L. David Harlow III RPh Director of Pharmacy Carilion Clinic New River Valley Medial Center Objectives At the completion of this knowledge
Accountable Care for Pharmacy Executives A Prescription for Change L. David Harlow III RPh Director of Pharmacy Carilion Clinic New River Valley Medial Center Objectives At the completion of this knowledge
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
The Patient Centered Medical Home (PCMH): Overview of the Model and Movement Part I. July 2010
: Overview of the Model and Movement Part I. July 2010") The Patient Centered Medical Home (PCMH): Overview of the Model and Movement Part I July 2010 Shari M. Erickson, MPH Senior Associate, Center for Practice Improvement & Innovation American College of Physicians
The Patient Centered Medical Home (PCMH): Overview of the Model and Movement Part I July 2010 Shari M. Erickson, MPH Senior Associate, Center for Practice Improvement & Innovation American College of Physicians
Do more of what you love. HealthPartners Wisconsin Freedom (Cost) 2016 Plan Comparison Guide
 2016 Plan Comparison Guide") Do more of what you love. HealthPartners Wisconsin Freedom (Cost) 2016 Plan Comparison Guide H2462_ 82767 Accepted 9/14/2014 H2462_91699_01 Accepted 8/30/2015 WIPlanComp Table of contents Introducing HealthPartners...................................
Do more of what you love. HealthPartners Wisconsin Freedom (Cost) 2016 Plan Comparison Guide H2462_ 82767 Accepted 9/14/2014 H2462_91699_01 Accepted 8/30/2015 WIPlanComp Table of contents Introducing HealthPartners...................................
1900 K St. NW Washington, DC 20006 c/o McKenna Long
 1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
UNIVERSITY OF PITTSBURGH SCHOOL OF MEDICINE MATCH RESULTS FOR CLASS OF 2010. Anesthesiology - 9. Dermatology - 1. Emergency Medicine - 12
 UNIVERSITY OF PITTSBURGH SCHOOL OF MEDICINE MATCH RESULTS FOR CLASS OF 2010 Anesthesiology - 9 Beth Israel Deaconess Medical Center, Boston MA Ohio State University Medical Center, Columbus OH Stanford
UNIVERSITY OF PITTSBURGH SCHOOL OF MEDICINE MATCH RESULTS FOR CLASS OF 2010 Anesthesiology - 9 Beth Israel Deaconess Medical Center, Boston MA Ohio State University Medical Center, Columbus OH Stanford
GOALS OF CARE A TOUR OF THE INDIVIDUAL S LIFE
 GOALS OF CARE A TOUR OF THE INDIVIDUAL S LIFE CHARLES CRECELIUS MD, PHD, FACP, CMD LEARNING OBJECTIVES To develop an understanding of the meaning of goals of care To increase knowledge of how goals of
GOALS OF CARE A TOUR OF THE INDIVIDUAL S LIFE CHARLES CRECELIUS MD, PHD, FACP, CMD LEARNING OBJECTIVES To develop an understanding of the meaning of goals of care To increase knowledge of how goals of
ACA Strategy. Why ACOs? 4/16/2014 ACCOUNTABLE CARE ORGANIZATIONS UNDER THE AFFORDABLE CARE ACT
 ACCOUNTABLE CARE ORGANIZATIONS UNDER THE AFFORDABLE CARE ACT Stephen P. Williams, JD 864 350 5276 1984carrera@gmail.com ACA Strategy One of the main ways the Affordable Care Act seeks to reduce health
ACCOUNTABLE CARE ORGANIZATIONS UNDER THE AFFORDABLE CARE ACT Stephen P. Williams, JD 864 350 5276 1984carrera@gmail.com ACA Strategy One of the main ways the Affordable Care Act seeks to reduce health
Analytic-Driven Quality Keys Success in Risk-Based Contracts. Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst
 Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
Healthcare Beyond The Hospital and the ICT Infrastructure Needed to Support
 Healthcare Beyond The Hospital and the ICT Infrastructure Needed to Support Mark Blatt MD Worldwide Medical Director Intel Corporation Med-e-Tel April 2012 Agenda: Care Beyond The Hospital and the ICT
Healthcare Beyond The Hospital and the ICT Infrastructure Needed to Support Mark Blatt MD Worldwide Medical Director Intel Corporation Med-e-Tel April 2012 Agenda: Care Beyond The Hospital and the ICT
Proposal for Departmental Status: Emergency Medicine. November, 2013
 Proposal for Departmental Status: Emergency Medicine November, 2013 Outline Emergency Medicine national context Emergency Medicine at UW Health History of Emergency Medicine 1960: Emergency Medicine conceived
Proposal for Departmental Status: Emergency Medicine November, 2013 Outline Emergency Medicine national context Emergency Medicine at UW Health History of Emergency Medicine 1960: Emergency Medicine conceived
Certificate of Need Law
 Certificate of Need Law Lake Norman Chamber of Commerce February 21, 2014 F. Del Murphy, Jr. SVP, Planning & Development Mission Statement The mission of Carolinas HealthCare System is to create and operate
Certificate of Need Law Lake Norman Chamber of Commerce February 21, 2014 F. Del Murphy, Jr. SVP, Planning & Development Mission Statement The mission of Carolinas HealthCare System is to create and operate
Value-Based Insurance Design. Using Smarter Cost-sharing to Align Consumer Incentives with Alternative Payment Models
 Value-Based Insurance Design: Using Smarter Cost-sharing to Align Consumer Incentives with Alternative Payment Models A. Mark Fendrick, MD University of Michigan Center for Value-Based Insurance Design
Value-Based Insurance Design: Using Smarter Cost-sharing to Align Consumer Incentives with Alternative Payment Models A. Mark Fendrick, MD University of Michigan Center for Value-Based Insurance Design
Why Are Health Care Costs Rising? Leading Experts/Real-World Data Identify Multiple Factors Across the System. March 2010
 Why Are Health Care Costs Rising? Leading Experts/Real-World Data Identify Multiple Factors Across the System March 2010 Multiple Factors Driving The Cost Of Health Care There is no single cause of the
Why Are Health Care Costs Rising? Leading Experts/Real-World Data Identify Multiple Factors Across the System March 2010 Multiple Factors Driving The Cost Of Health Care There is no single cause of the
The Role of Insurance in Providing Access to Cardiac Care in Maryland. Samuel L. Brown, Ph.D. University of Baltimore College of Public Affairs
 The Role of Insurance in Providing Access to Cardiac Care in Maryland Samuel L. Brown, Ph.D. University of Baltimore College of Public Affairs Heart Disease Heart Disease is the leading cause of death
The Role of Insurance in Providing Access to Cardiac Care in Maryland Samuel L. Brown, Ph.D. University of Baltimore College of Public Affairs Heart Disease Heart Disease is the leading cause of death
Community Physicians of Indiana Engineering Forms to Improve Quality of Care and Physician Efficiency Ryan Houghton, M.D.
 Community Physicians of Indiana Engineering Forms to Improve Quality of Care and Physician Efficiency Ryan Houghton, M.D. Disclosure No additional relationships or conflicts of interest besides employment
Community Physicians of Indiana Engineering Forms to Improve Quality of Care and Physician Efficiency Ryan Houghton, M.D. Disclosure No additional relationships or conflicts of interest besides employment
Corporate Health Care Disjointed, Dysfunctional, Disastrous
 Corporate Health Care Disjointed, Dysfunctional, Disastrous When you have done all you can do what s the next step? THE ISSUES: Three better words could hardly be found to describe the current status of
Corporate Health Care Disjointed, Dysfunctional, Disastrous When you have done all you can do what s the next step? THE ISSUES: Three better words could hardly be found to describe the current status of
How To Teach Nursing
 Chapter 7: Nursing Organization Teaching Goals After finishing this chapter, every student should have a firm concept of both what nursing contributes to high quality, safe, efficient, and effective patient
Chapter 7: Nursing Organization Teaching Goals After finishing this chapter, every student should have a firm concept of both what nursing contributes to high quality, safe, efficient, and effective patient