Medicare Part D: A First Look at Plan Offerings in 2016
|
|
|
- Christopher Norman
- 8 years ago
- Views:
Transcription
1 Medicare Part D: A First Look at Plan Offerings in 2016 During the Medicare open enrollment period, which runs from October 15 to December 7 each year, beneficiaries have the opportunity to enroll in a plan that provides Part D prescription drug coverage, either a stand-alone prescription drug plan (PDP) as a supplement to traditional Medicare, or a Medicare Advantage drug plan (MA-PD), which provides all Medicare-covered benefits including prescription drugs. Of the nearly 40 million beneficiaries enrolled in Part D plans, about 6 in 10 are in PDPs and the rest in MA-PDs. This issue brief provides an overview of the 2016 PDP marketplace, focusing on key changes from 2015, based on our analysis of data from the Centers for Medicare & Medicaid Services (CMS)., In 2016, the typical Medicare beneficiary will have a choice of more than two dozen PDPs. Many will see higher premiums and deductibles if they remain in their current plan. As in the past, Part D enrollees need to consider that their plan may require coinsurance, rather than flat copayments, for brand-name and specialty drugs, and differential cost sharing for prescriptions depending on their choice of pharmacy. These factors, as well as which drugs are included on a plan's formulary, may affect out-of-pocket costs as much as premiums. Other highlights include: In 2016, beneficiaries in each region will have a choice of 26 PDPs, on average, down by 4 from The average PDP premium (weighted by 2015 plan enrollment) is projected to increase by 13 percent from 2015 to 2016, from $36.68 to $41.46 per month. Even if a number of beneficiaries switch or are reassigned to lower-premium plans, the average premium increase for 2016 is likely to be the largest since More than one-third of the 11.2 million PDP enrollees who do not receive Low-Income Subsidies (LIS) would pay premiums of $60 or more per month in 2016 if they stay in the same plan. Nearly 4.4 million of these enrollees not receiving the LIS face a premium increase of at least $10 per month in 2016 if they stay in the same plan. Two-thirds of all PDPs will have deductibles in 2016, a higher share than in previous years. A growing share of PDPs will impose the maximum deductible allowed by law, which increased from $320 in 2015 to $360 in 2016, the largest increase in the deductible since the start of the program. Most PDPs charge coinsurance, rather than flat copayments, for non-preferred brand-name and specialty drugs, which could lead to higher out-of-pocket costs for those who use high-cost drugs. Nearly all PDPs (84 percent in 2016) use tiered pharmacy networks, with lower cost sharing in selected network pharmacies and higher cost sharing in other network pharmacies, a significant increase from just a few years ago when only a small share of plans used this type of preferred pricing (7 percent in 2011). Beneficiaries receiving the LIS will have access to 7 plans for no monthly premium in 2016, on average, fewer than in any past year. About 1.9 million LIS enrollees who are slated to be in PDPs where they will pay premiums must switch plans or be reassigned by CMS in order to have premium-free coverage in 2016.
.")
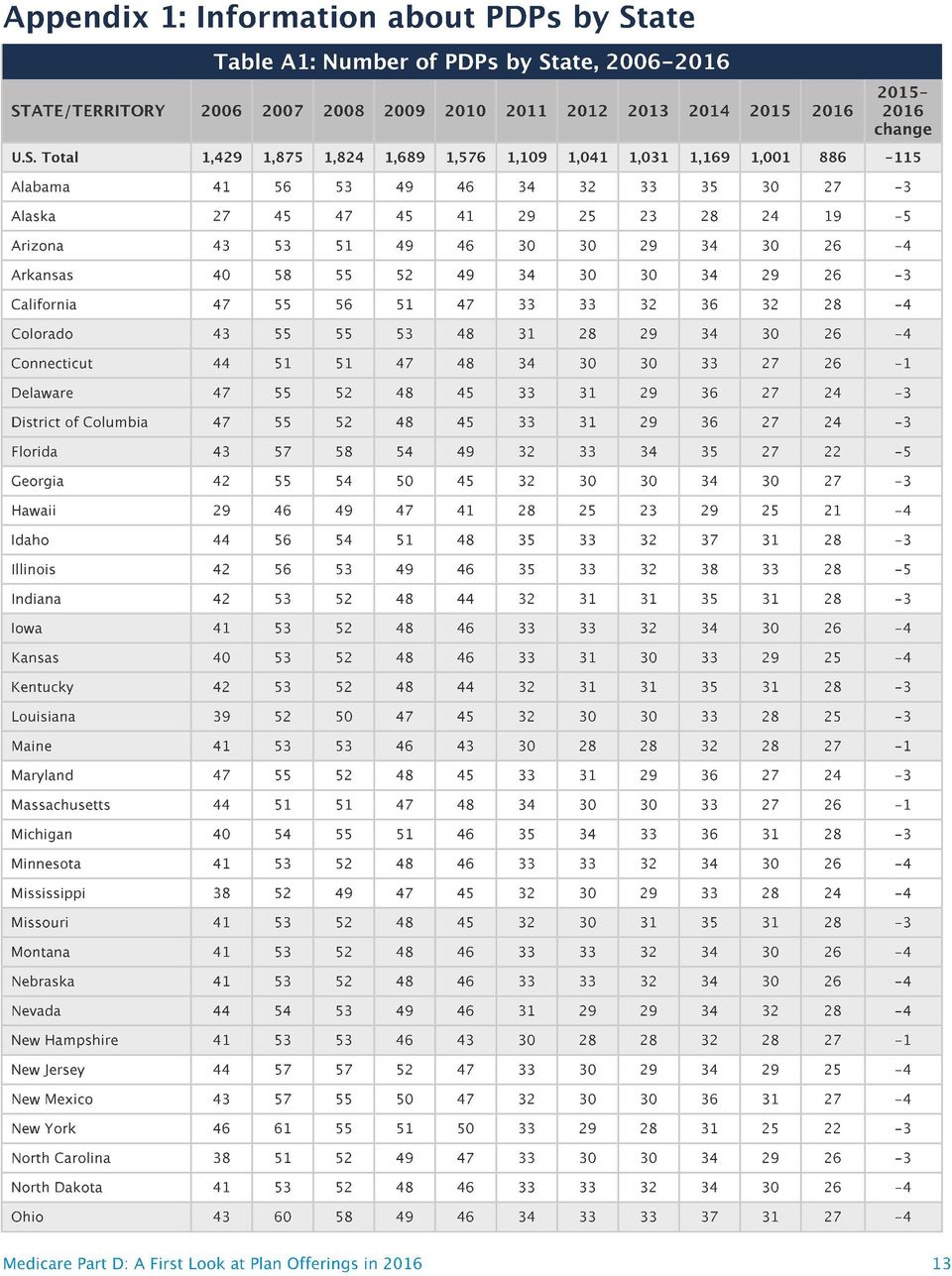
2 In 2016, beneficiaries across the country continue to have a substantial number of Part D plan choices. The average beneficiary will have a choice of 26 PDPs in 2016, down from 30 in 2015 and 55 at the peak in 2007 (Figure 1). Beneficiaries will also have access to 16 Medicare Advantage prescription drug plans, on average. The number of PDPs per region in 2016 will range from a low of 19 PDPs in the Alaska region to a high of 29 PDPs in the Pennsylvania/West Virginia region (Figure 2; Appendix 1, Table A1). The number of plans is lower in all but one region (Pennsylvania/West Virginia) compared to 2015; there are five fewer PDPs in Alaska, Florida, and Illinois in A total of 886 PDPs will be offered nationwide in 2016, down by 11 percent from the 1,001 PDPs offered in 2015 and the lowest number of PDPs in the program s history (Figure 3). The total number of PDPs in 2016 represents less than half the number offered at the peak level in 2007 of 1,875 plans. The lower number of plans reflects both the cumulative effect of mergers among plan sponsors and the response to CMS policies that encourage plan sponsors to eliminate low-enrollment plans and to drop multiple Figure 1 Figure 2 PDPs that are not meaningfully different from each other. In 2016, there are 11 plan sponsors offering 23 PDPs on a national or near-national basis. The number of national or near-national plan sponsors is down from 18 in 2009, as a result of corporate acquisitions and some firms exiting the market after not achieving a substantial market share. In addition, more sponsors are offering two PDPs, whereas it was more common to offer three in the program s early years. In July 2015, the PDP sponsor Torchmark Corporation was placed under a sanction that banned marketing activities and new enrollments. Its PDPs, marketed under the United American name, have 208,000 enrollees in 91 PDPs across all regions in September Average Number of PDPs Offered to Medicare Beneficiaries, OR, WA Number of PDPs, by Region, ID, UT 26 IA, MN, MT, NE, ND, SD, WY IN, KY AL, TN HI 46 Average Number of PDPs Per Region = plans plans 27 plans plans 6 regions 10 regions 8 regions 10 regions 27 ME, NH PA, WV 26 CT, MA, RI, VT 25 NJ 24 DE, DC, MD NOTE: PDP is prescription drug plan. Excludes plans in the territories. Includes 91 plans under CMS sanction and closed to new enrollees as of September SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS 2016 PDP landscape source files NOTE: PDP is prescription drug plan. Estimates are beneficiary weighted. Excludes plans in the territories; includes plans under CMS sanction and closed to new enrollees. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP enrollment, crosswalk, and landscape source files
.")
3 For 2016, 31 new PDPs are entering the Figure 3 market, and 146 PDPs are exiting the Number of PDPs, program. (See Appendix 2 for more detail 1,875 1,824 1,689 on market dynamics.) Two new sponsors are entering the PDP 1,429 1,576 market in 2016: Magellan Rx America, offering PDPs in 20 regions, and QualChoice Advantage, offering a PDP 1,109 1,041 1,031 1,169 1, only in Arkansas. Among the 146 exiting plans, 143 are offered by sponsors that offer other PDPs, and enrollees in most of them (137 of 143) will be automatically assigned to another PDP offered by that sponsor. This process should ensure a seamless transition and minimize disruption that would otherwise result from plan terminations. The other 3 exiting PDPs are offered by sponsors (each operating in a single region) leaving the market entirely NOTE: PDP is prescription drug plan. Excludes plans in the territories. Total for 2016 includes 91 plans under CMS sanction and closed to new enrollees as of September SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP landscape source files. The national average monthly PDP premium is expected to increase for 2016, marking a significant departure from recent years when premiums were essentially flat. Even if a number of beneficiaries switch or are reassigned to lower-premium plans, effective in January 2016, the average premium increase for 2016 is likely to be the largest amount in any year since The projected average monthly PDP premium for 2016 will be $41.46 (weighted by September 2015 enrollment, assuming beneficiaries remain in their current plan) (Figure 4). This is a 13 percent projected increase ($4.66) from the weighted average monthly premium of $36.68 in 2015, and a 60 percent increase from $25.93 in 2006, the first year of the Medicare Part D drug benefit. As a point of comparison, since 2006, the medical care consumer price index (CPI) has increased 34 percent and the CPI for all items has increased 18 percent. In prior years, the average premium after the end of the open enrollment period has been 4 percent to 5 percent lower than the projection made during the open enrollment period, due to existing enrollees switching to a lower premium plan, new enrollees choosing low-premium plans, and reassignments of some LIS Figure 4 Weighted Average Monthly Premiums for PDPs, $45 $40 $35 $30 $25 $20 $15 $10 $5 $0 $25.93 $27.39 $29.89 $35.09 $37.25 $38.29 $37.78 $38.54 $37.75 $ : 60% increase Projected $ NOTE: PDP is prescription drug plan. Average premiums are weighted by enrollment in each year (September 2015 enrollment used for 2015 and 2016). Excludes plans in the territories. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP enrollment and landscape source files : 13% projected increase
 will be automatically assigned to another PDP offered by that sponsor.")
4 beneficiaries to cheaper plans. For example, the average premium in February 2015 was $37.20,which is about 4 percent ($1.63) below the projected premium of $38.83 calculated prior to enrollment changes. Applying a similar adjustment to our projected premium for 2016 suggests that the premium increase, after open enrollment, is likely to be lower, but still larger than in any year since For PDPs offering only the basic benefit, the 2016 weighted average premium is projected to be 8 percent higher in 2016 than in 2015 (based on current enrollment patterns), whereas premiums for enhanced PDPs are projected to rise by about 17 percent. A growing share of PDP enrollees are paying premiums that are well above the national average. In 2016, over one-third of PDP enrollees not receiving the LIS (36 percent) are projected to have premiums of at least $60 per month if they stay in their plans a substantial increase from the 10 percent of enrollees paying premiums at this level in 2015 (Figure 5). Among them, nearly 400,000 are projected to pay premiums of at least $100 per month. By contrast, 14 percent of these PDP enrollees are scheduled to pay premiums of less than $20 per month. CMS reported that the average premium for standard Part D coverage offered by PDPs and Medicare Advantage drug plans will remain stable at an estimated $32.50 in The higher premium reported here is based on PDPs only, including PDPs offering both basic and enhanced coverage. Enhanced plans typically have higher premiums than basic PDPs. Our estimate does not assume any voluntary switches by beneficiaries and reassignments by CMS of Low-Income Subsidy enrollees to different plans, nor do we make any assumptions about plan choices made by new enrollees in Figure 5 Distribution of PDP Enrollees By Monthly Premium, 2015 (Actual) and 2016 (Projected) Excluding Enrollees Who Receive Low-Income Subsidies Figure 6 10% 43% Distribution of Changes in Monthly Premiums for PDP Enrollees Between 2015 and 2016 If Enrollees Do Not Switch Plans Between 2015 and 2016 Decrease of $10 or more Decrease of less than $10 36% 20% 35% 30% 13% 14% Non-LIS PDP Enrollment = 11.2 million Increase of less than $10 Increase of $10 or more More than $60 $40-$60 $20-$40 Less than $20 NOTE: LIS is low-income subsidy. PDP is prescription drug plan. Analysis excludes enrollees for whom CMS provides no crosswalk between their 2015 and 2016 PDPs distribution assumes no plan changes during the open enrollment period. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP enrollment, crosswalk, and landscape source files. Underneath these national trends, premium changes for individual PDPs from 2015 to 2016 vary widely (Figure 6). Non-LIS enrollees (n=11.2 million) 4% 13% 44% 39% Among the 11.2 million Part D PDP enrollees who are responsible for paying the entire premium (which excludes LIS recipients), most (83 percent) are projected to have a higher premium in All PDP enrollees (n=19.3 million) 2% 18% 52% 28% NOTE: PDP is prescription drug plan. LIS is Low-Income Subsidy. Analysis excludes enrollees for whom CMS provides no crosswalk between their 2015 and 2016 PDPs. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP enrollment, crosswalk, and landscape source files.
, whereas premiums for")
5 2016 if they stay in their current plans, including 4.4 million (39 percent) who are projected to have a premium increase of at least $10 per month. Conversely, nearly half a million (448,000) are projected to experience a premium decrease of $10 or more. Taking into account all PDP enrollees, including the LIS enrollees whose premiums are partially paid by the government, 80 percent are in plans in which premiums are projected to rise in 2016 if they stay in their current plans; this includes 28 percent in plans that will have an increase of $10 or more in their monthly premium in 2016 assuming no enrollment changes. By contrast, 2 percent of all PDP enrollees are in plans projected to have a premium decrease of $10 or more. Changes to premiums from 2015 to 2016, averaged across regions and weighted by 2015 enrollment, vary widely across some of the most popular PDPs (Figure 7). These variations reflect factors such as higher premiums in older plans and substantial geographic variations. Although variation in benefits is also a factor, premium variation persists even among PDPs that offer benefits actuarially equivalent to the basic benefit defined in law. Average premiums for seven of the eight largest PDPs will increase for Five of these seven PDPs will have larger average percentage increases than the national average. Average premiums for three of these PDPs are projected to increase by at least 20 percent in The highest increases, in percentage terms, are for Humana Enhanced PDP, with 1.1 million enrollees in 2015, and AARP MedicareRx Saver Plus, with 1.4 million enrollees. On average, premiums for both PDPs will rise 25 percent (from $52.86 to $66.25 for Humana Enhanced and from $28.13 to $35.23 for AARP MedicareRx Saver Plus). The average monthly premium for the PDP with the most enrollees in 2015, AARP MedicareRx Preferred, with 3.5 million enrollees, will increase by 21 percent between 2015 and 2016, from $50.19 to $ By contrast, enrollees in one of the largest PDPs will experience a modest decrease in their monthly premium if they stay in the same plan. The average monthly premium for SilverScript Choice will decrease by 2 percent ($22.56 in 2016 versus $23.13 in 2015). Enrollees in some of the most popular PDPs could see bigger or smaller premium increases than the national average, depending on the region where they live. Figure 7 Name of PDP AARP MedicareRx Preferred UnitedHealth s AARP MedicareRx Preferred PDP is raising premiums by as little as 9 percent (in Oregon/Washington) but as high as 37 percent (in Alaska) (Figure 8). The range is even greater for CVS Health s SilverScript Choice PDP, which is reducing premiums by as much as 36 percent (in Arkansas) and increasing premiums by as much as 24 percent (in Florida). Monthly Premiums for PDPs with Highest 2015 Enrollment Type of plan First year offered 2015 Enrollment (in millions) # % of Total Weighted Average Monthly Premium 1 First year % Change First year Enhanced % $26.31 $50.19 $ % +131% SilverScript Choice Basic % $28.32 $23.13 $ % -20% Humana Preferred Rx Basic % $14.80 $26.45 $ % +92% Humana Walmart Rx Enhanced % $12.60 $15.67 $ % +46% AARP MedicareRx Saver Plus Basic % $15.00 $28.13 $ % +135% Humana Enhanced Enhanced % $14.73 $52.86 $ % +350% Cigna-HealthSpring Rx Secure Basic % $35.05 $30.84 $ % +4% WellCare Classic Basic % $15.80 $31.05 $ % +103% TOTAL % $25.93 $36.68 $ % +59% NOTE: PDP is prescription drug plan. Plan names can change from year to year; plans are designated the same if they have the same contract/plan ID. 1 Average premiums are weighted by enrollment in each region for each year. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP enrollment, crosswalk, and landscape source files.

6 Monthly premiums for the most popular PDPs available since the start of the Part D program in 2006 have changed in different ways. The average premium for Humana PDP Enhanced, with 1.1 million enrollees in 2015, is more than four times higher than it was in 2006, having increased from $14.73 to $ Of the eight most popular PDPs, this plan is projected to have the most expensive monthly premium in The average premium for UnitedHealth s AARP Preferred MedicareRx PDP, the PDP with the most enrollees in 2015 (3.5 million), has more than doubled since 2006, from $26.31 to $60.79 in Figure Percentage Change in Monthly Premiums for Top Three PDPs by 2015 Enrollment Average and Highest-Lowest Percentage Change in Premiums By Region Highest By contrast, the monthly premium for SilverScript Choice, operated by CVS Health, with 2.5 million enrollees in 2015, is 20 percent lower in 2016 ($22.56) than it was in 2006 ($28.32). 50% 40% 30% 20% 10% 0% -10% -20% -30% -40% -50% 37% (AK) 21% 9% (OR/WA) AARP MedicareRx Preferred 2016 average premium: $ % (FL) -2% -36% (AR) SilverScript Choice 2016 average premium: $ % (FL) 7% -18% (AR) Humana Preferred Rx 2016 average premium: $28.39 NOTE: PDP is prescription drug plan. State abbreviations included in parentheses correspond to regions with highest and lowest percentage change. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS 2016 PDP enrollment, crosswalk, and landscape source files. percentage change, , by region Average percentage change, Lowest percentage change, , by region Average PDP monthly premiums, weighted by 2015 enrollment, will vary widely in 2016 across regions, along with the change in premiums from 2015 to Average PDP premiums will range from $29.70 per month in the New Mexico region (one of only three regions with an average under $35) to $49.61 per month in New Jersey and $45.31 in Florida (Appendix 1, Table A2). Premium changes from 2015 to 2016 vary considerably by region. For example, average premiums in Arkansas are projected to fall by about 1 percent, whereas average premiums will be at least 20 percent higher in Arizona and Florida (Figure 9). Figure 9 Change in Weighted Average Premiums for PDPs, by Region, % +7% OR, WA +16% +13% +9% ID, UT +3% IA, MN, MT, NE, ND, SD, WY +16% +11% +13% +9% +13% PA, WV +14% +15% +16% +11% +19% +10% IN, KY +12% +24% +12% +11% +16% -1% +6% AL, TN +7% +17% +17% +7% +17% HI National Average = +13% 1% 3-9% 10-15% 16-25% decrease increase increase increase 1 region 7 regions 13 regions 13 regions +17% ME, NH +13% CT, MA, RI, VT +17% NJ +15% DE, DC, MD +21% FL NOTE: PDP is prescription drug plan. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP enrollment, crosswalk, and landscape source files. Average and plan-level premium amounts do not take into account the income-related Part D premium that took effect in 2011 for Part D enrollees with higher annual incomes ($85,000/individual and $170,000/couple). Established by the Affordable Care Act of 2010 (ACA), the income-related Part D premium
, has more than doubled since 2006, from $26.31 to $60.79 in 2016.")
7 requires higher-income enrollees to make an additional payment to the government for Part D coverage, regardless of the plan selected. In 2016, the monthly surcharge will range from $12.70 to $72.90, depending on income, in addition to the monthly premium payment for the specific Part D plan. Nearly 6 percent of Part D enrollees are expected to make these additional payments in Under current law, the income thresholds are not indexed to increase annually until 2020, meaning that by 2019, a projected 8 percent of Part D enrollees will pay income-related premiums. In 2016, for the second year in a row, all Part D PDPs will offer an alternative benefit design to the defined standard benefit, which has a $360 deductible in 2016 and 25 percent coinsurance for all covered drugs. Some plans modify or eliminate the deductible, and all PDPs use some type of varying cost-sharing tiers for covered generic and brand-name drugs. The standard (maximum) Part D deductible is increasing by $40 in 2016, the largest one-year increase since the program began. It is adjusted each year by a statutory formula based on the annual percentage increase in average per capita aggregate expenditures for covered Part D drugs. Other amounts for the standard benefit design parameters are increasing as well (see Appendix 3 for the standard benefit amounts). Two-thirds of PDPs (67 percent) will charge a deductible in 2016, up from 58 percent in 2015 (Figure 10). The share of PDPs with a deductible is the highest ever in the program. Most PDPs adding deductibles have relatively few enrollees, so the share of PDP enrollees facing a deductible is likely to change more modestly. Nearly two-thirds of all Part D enrollees are in plans that are increasing the deductible for Figure 10 Share of PDPs, By Deductible Amount, No deductible Partial deductible Standard deductible 58% 60% 59% 8% 8% 8% 55% 11% 34% 32% 33% 34% 36% 40% 42% 24% 18% 10% 47% 45% 47% 10% 4% 14% 40% 43% 45% 49% 42% 44% 33% 14% 53% Most PDPs with a deductible (53 percent) will charge the standard $360 amount, which is also the highest share in the program s history. Another 14 percent of all Standard deductible amount: PDPs have a deductible below the standard amount $250 $265 $275 $295 $310 $310 $320 $325 $310 $320 $360 NOTE: PDP is prescription drug plan. Estimates may not sum to total due to rounding. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP landscape source files. The use of formulary tiers has been common since the program s beginning in 2006, but for the second year in a row, all PDPs will use tiered cost sharing. Similar to 2015, most PDPs will use five tiers (two for generic drugs, two for brand-name drugs, and one for higher-cost specialty drugs). Over the years, there has been a trend toward the use of coinsurance in place of flat copayments for some formulary tiers. Coinsurance typically means higher out-of-pocket costs for more expensive drugs, such as those over $200 per month. Coinsurance has been used by nearly all plans for the specialty tier since 2006,

8 and that coinsurance cannot exceed 33 percent. For all PDPs, the specialty tier coinsurance is set between 25 percent and 33 percent. In the program s early years coinsurance was uncommon for other tiers, but in 2016, over 90 percent of PDPs are using coinsurance for their non-preferred brand tiers; about 40 percent do so for their preferred brand tiers. For brand tiers, the typical coinsurance is 20 percent for preferred brands and 40 percent for non-preferred brands. CMS guidance allows coinsurance for these tiers to be set as high as 25 percent and 50 percent, respectively. Some PDPs have elected to set coinsurance at these maximum levels. The coverage gap, or doughnut hole, is gradually becoming a less salient feature of the Part D benefit design, as a result of changes made by the ACA. It will be fully eliminated as of 2020, when beneficiaries will only be responsible for 25 percent of their total drug costs in the gap. Since 2011, any beneficiary with drug costs high enough to reach the gap has paid less than the full cost of the price of their drugs. In 2016, manufacturer prices for brand-name drugs purchased in the gap will be discounted by 50 percent, with plans paying an additional 5 percent of the cost and enrollees paying the remaining 45 percent. Plans will pay 42 percent of the cost for generic drugs in the gap, with enrollees paying 58 percent. In 2016, the coverage gap begins after an enrollee incurs $2,960 in total drug spending and ends after an enrollee has spent a total of $4,850 out of pocket (or $7,515 in total drug costs under the standard benefit). At that point, catastrophic coverage begins, where enrollees generally pay only 5 percent of drug costs. Most Part D plans will offer no gap coverage in 2016 beyond what is required by the ACA under the standard benefit. With all Part D enrollees now getting coverage for a share of their costs in the gap, the value of additional gap coverage offered by plans will become lower each year until 2020, when the gap is fully closed. In 2016, about 78 percent of all PDPs will offer no additional gap coverage. This is a small increase from 2015, when 74 percent of PDPs offered no additional gap coverage meaning a slightly smaller share of plans will offer some gap coverage beyond what the ACA requires in 2016 than in One national PDP (First Health Part D Value Plus) added gap coverage, and one near-national plan (Symphonix PrimeSaver Rx) dropped gap coverage. Nearly all PDPs (85 percent) use tiered pharmacy networks. In these networks, enrollees pay preferred (lower) cost sharing for their prescriptions when they use selected network pharmacies and higher cost sharing in other network pharmacies. The share of PDPs with tiered preferred pharmacy networks is down slightly from 87 percent in 2015, but still a significant increase from just a few years ago when only a small share of plans used this type of preferred pricing (7 percent in 2011). The cost implications of tiered pharmacy networks for enrollees vary across PDPs. For example, among the national and near-national PDPs with tiered pharmacy networks, the AARP MedicareRx Saver Plus PDP charges a $20 copayment for a preferred brand drug in a pharmacy that offers preferred cost sharing and $33 in another network pharmacy that does not offer preferred cost sharing. The Humana Walmart Rx PDP charges a $1 copayment for preferred generic drugs and $4 for non-preferred

9 generics at a pharmacy with preferred cost sharing, compared to $10 and $33, respectively, at other network pharmacies where preferred cost sharing is not offered. These differentials are somewhat smaller than in In 2016, the total availability of premium-free (benchmark) plans that is, PDPs available for no monthly premium to Low-Income Subsidy (LIS) enrollees will be at its lowest level in the program s ten years (Figure 11; Appendix 1, Table A3). In 2016, 226 plans will be available for enrollment of LIS recipients for zero premium. This represents a 20 percent decrease in plans for LIS recipients, or 57 fewer plans than in 2015 and 126 fewer plans than in On average (weighted by enrollment), LIS have 7 benchmark plans available to them for 2016, or about one-fourth the number of PDP choices available overall. All LIS enrollees retain the option to select other plans offered in their area, but if they enroll in a non-benchmark plan, they must pay a share of the monthly premium. Of the 226 benchmark plans in 2016, about one in four (57 plans) qualify through the de minimis policy about the same number as the 54 de minimis plans in Policies adopted by CMS in previous years make it easier for PDPs to qualify as benchmark plans, including the de minimis policy that allows plans to waive a premium amount of up to $2 in order to retain their LIS enrollees. Among the 2015 benchmark plans, 72 PDPs have lost their benchmark status due to either higher premiums in 2016 or to a lower regional benchmark in 2016 (one other exited the market completely). About 742,000 LIS beneficiaries (9 percent of LIS enrollment in PDPs in 2015) are enrolled in these 73 plans, meaning these beneficiaries may experience some disruption in their coverage for In 2016, 25 PDPs will newly qualify for benchmark status: 14 PDPs new to the program and 11 older PDPs (in nine other cases, two benchmark PDPs were consolidated by the plan sponsor). Figure 11 Number of PDPs Available Without a Premium to Low-Income Subsidy Recipients, Share of PDPs: De minimis plans* Benchmark plans % 34% 27% 18% 19% 30% 31% 32% 30% 28% 26% NOTE: PDP is prescription drug plan. Excludes plans in the territories. *De minimis plans can retain Low-Income Subsidy beneficiaries despite exceeding the benchmark premium by up to $2 in 2007, $1 in 2008, and $2 in SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP landscape source files The number of benchmark plans available in 2016 will vary by region, from 10 benchmark PDPs in the Arizona, Idaho/Utah, and Pennsylvania/West Virginia regions to just 2 benchmark PDPs in the Hawaii region (out of 21 PDPs overall) and 3 (of 22) in the Florida region (Figure 12).
. In 2016, 226 plans will be available for enrollment of LIS recipients for zero premium.")
10 Benchmark plan availability will decline in 26 of 34 regions between 2015 and 2016, while one additional benchmark plan will be available in 3 regions (Figure 13). Year-to-year changes in most regions are relatively modest; the largest change is the loss of seven benchmark plans in the Hawaii region, after gaining five benchmark plans for 2015 and losing six for As a result of losing this many benchmark plans, 92 percent of Hawaii s LIS beneficiaries are projected to pay a premium unless they are reassigned or switch plans. In five other regions, between 40 percent and 50 percent of LIS beneficiaries are in this same situation. In regions where the availability of benchmark plans is more stable, the share of affected LIS beneficiaries is much smaller. About 1.9 million people about one in four LIS beneficiaries (24 percent) are enrolled in PDPs in 2015 that will not qualify as benchmark plans in 2016 (Figure 14). This group includes 742,000 beneficiaries who were in benchmark plans in 2015; the remaining three-fifths (60 percent) of these beneficiaries are currently enrolled in non-benchmark plans and thus paid a premium in About 764,000 LIS enrollees will pay premiums of at least $20 per month and about 53,000 LIS enrollees will pay premiums of at least $50 per month if they do not switch to other PDPs. The number of LIS beneficiaries who will potentially pay a premium in 2016 unless they enroll in (or are switched to) Figure 12 Number of Part D Benchmark Plans, by Region, 2016 Figure 13 Change in Number of Part D Benchmark Plans, By Region, Net Change in Benchmark Plans Across All Regions = OR, WA -- Decrease of Decrease of No Increase of 3-7 plans 1-2 plans change (--) 1 plan 9 regions 17 regions 5 regions 3 regions ID, UT -- IA, MN, MT, NE, ND, SD, WY IN, KY AL, TN HI NOTE: indicates no change in number of benchmark plans. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP landscape source files. Figure ME, NH PA, WV +1 CT, MA, RI, VT -2 NJ -1 DE, DC, MD Part D Low-Income Subsidy (LIS) Enrollment by Benchmark Plan Status, as of 2016 Open Enrollment Period 2015 plan IS a benchmark plan in 2016 Total Number of Benchmark Plans Across All Regions = OR, WA plans 5-6 plans 7-8 plans 9-10 plans 6 regions 10 regions 11 regions 7 regions 10 ID, UT 6.1 million LIS enrollees (76%) 5 IA, MN, MT, NE, ND, SD, WY IN, KY AL, TN HI 1.9 million LIS enrollees (24%) Total LIS Enrollment in PDPs in 2015 = 7.9 million 2015 plan IS NOT a benchmark plan in 2016 NOTE: PDP is prescription drug plan. Analysis includes enrollment in PDPs only. Estimates do not sum to total due to rounding. Analysis excludes enrollees for whom CMS provides no crosswalk between their 2015 and 2016 PDPs. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP enrollment, crosswalk, and landscape source files ME, NH 8 10 PA, WV 6 CT, MA, RI, VT 8 NJ 9 DE, DC, MD NOTE: Includes de minimis plans that can retain Low-Income Subsidy beneficiaries despite exceeding the benchmark premium by up to $2 in SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS 2016 PDP landscape source file.

11 benchmark plans (1.9 million) is up slightly from the 1.8 million LIS beneficiaries who were in a similar situation at the time of the open enrollment period for CMS will reassign those LIS enrollees who were randomly assigned by CMS to their current plan, and several states will help reassign those enrolled in their state pharmacy assistance programs (SPAPs). Effective for January 2015, CMS reassigned about one-fifth of those scheduled to pay a premium. Many other LIS beneficiaries who are currently not enrolled in plans that will be premium-free in 2016 must switch plans on their own or pay a premium if they remain in their 2015 plan. Those in the latter group will not be automatically reassigned by CMS because in the past they or someone assisting them made a choice to switch plans. Most affected LIS beneficiaries will receive a letter from CMS or their SPAP either informing them of their reassignment or reminding them that they can choose a different plan and avoid paying a premium. The number of premium-free plans for LIS enrollees offered by the major Part D organizations has fluctuated substantially over the years. For 2016, six PDP sponsors will offer benchmark plans in at least half of the 34 regions. No sponsor will offer benchmark plans in all 34 regions in 2016; three sponsors (Aetna, CVS Health, and Humana) offer benchmark plans in at least 33 regions. In 2015, about 70 percent of LIS enrollees in PDPs are in plans operated by just four plan sponsors (CVS Health, Humana, UnitedHealthcare, and Cigna) (Figure 15). The first two of these sponsors offer PDPs that qualify as benchmark plans in at least 32 of the 34 PDP regions in By contrast, UnitedHealth offers PDPs that qualify as premium-free in 15 regions in 2016, down from 33 in Cigna offers PDPs that qualify as premium-free in 12 regions in 2016, down from 23 in Over half of the LIS beneficiaries projected to pay premiums are currently enrolled in UnitedHealth or Cigna PDPs. Figure 15 Availability of Benchmark Plans Offered by Four Major Part D Organizations Across the 34 PDP Regions, Number of PDP regions (out of 34): CVS Health 2,210,000 LIS enrollees in Humana 1,265,000 LIS enrollees in 2015 UnitedHealth 1,258,000 LIS enrollees in 2015 NOTE: PDP is prescription drug plan. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP landscape source files. Cigna 877,000 LIS enrollees in 2015 The LIS enrollees in PDPs offered by these sponsors are split between premium-free benchmark plans and other plans operated by these sponsors. For example, 64 percent of UnitedHealthcare s LIS enrollees are in non-benchmark PDPs and thus pay premiums of $21.06 on average. Many of them are in the AARP MedicareRx Preferred PDP, which qualified as a benchmark PDP in the program s earlier years.

12 This review of the Part D plan landscape for 2016 and changes over time indicates that most PDP enrollees can expect to see some changes in their prescription drug coverage and costs in For most enrollees, premiums are projected to be higher in 2016 than in 2015, and many will also see higher deductibles and more cost-sharing tiers with coinsurance. LIS enrollees will have fewer PDP options available at a zero premium, and many be reassigned to different plans or will need to switch to a different plan to continue without a premium. Beneficiaries have options during open enrollment to select plans that better meet their needs, including plans with lower premiums. Although premiums tend to be the most visible feature when comparing plans, beneficiaries need to consider other factors, especially whether their drugs are on a plan s formulary, whether their usual pharmacy offers preferred cost sharing, and the total out-of-pocket costs (including both premiums, deductibles, and cost sharing) for coverage of their prescription drug needs. Changes in Part D plan costs and benefit design from one year to the next have been a defining featuring of the program since its beginning. The reduced number of PDPs for 2016 could make the process of comparing and reviewing plan options a little easier for beneficiaries to undertake during the open enrollment period, but the more than two dozen PDP options in each region may still discourage many from reevaluating their choices. While the annual enrollment period is the best opportunity for people on Medicare to evaluate their plan options and make changes, our analysis of plan switching by PDP enrollees not receiving the LIS showed that about 87 percent stayed in the same plan in annual enrollment periods between 2006 and Even when they were projected to face large premium increases, a majority of PDP enrollees stayed in the same plan from one year to the next. Among LIS enrollees, although many are reassigned each year to new plans by CMS, few (14 percent) of those not eligible for reassignment by CMS and projected to pay a premium switched to new plans in Finding ways to get more Part D enrollees engaged in comparing and reviewing plans and making changes that could save them money remains an ongoing challenge for CMS and policymakers.

13
14 NOTE: PDP is prescription drug plan. Analysis for 2016 includes 91 plans under CMS sanction and closed to new enrollees as of September SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP crosswalk and landscape source files.

15

16 NOTE: PDP is prescription drug plan. Analysis for 2016 includes 91 plans under CMS sanction and closed to new enrollees as of September Average monthly premium is weighted by 2015 enrollments for the region in which the state is located. Terminated plans are excluded in calculation of premium change. SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP crosswalk and landscape source files.

17

18 NOTE: Benchmark plans are not designated (N/A) in the territories because low-income beneficiaries residing in the territories are not eligible for the low-income subsidy. Analysis for 2016 includes 91 plans under CMS sanction and closed to new enrollees as of September SOURCE: Georgetown/Kaiser Family Foundation analysis of CMS PDP landscape source files.

19 Among the 31 new PDPs in the market, 21 are offered by sponsors totally new to the program: Magellan Rx America (20 PDPs in 20 regions) and QualChoice Advantage (1 PDP in Arkansas). The other new PDPs are additional offerings in a few regions by three national or near-national plan sponsors (EnvisionRxPlus, Symphonix Heath, and WellCare). Four firms that offer PDPs on a national or near-national basis are eliminating one of the PDPs they offer in all or most regions. Aetna continued consolidating the PDPs it acquired from Coventry and now sponsors three PDPs instead of four, eliminating the Aetna Medicare Rx Premier PDP (42,000 enrollees across all regions). Two of its three offerings in each region are marketed under the First Health name. Cigna, after consolidating PDPs from its acquisition of HealthSpring, is eliminating one of its three PDPs (Cigna- HealthSpring Rx Secure-Max PDP with 22,000 enrollees). Express Scripts is eliminating the SmartD Rx Saver PDPs it acquired in 2014 (73,000 enrollees), leaving only two PDPs per region. Finally, TransAmerica eliminated its MedicareRx Choice PDPs (20,000 enrollees), leaving it with just a single PDP per region (and also dropped all PDPs in three regions, affecting another 2,000 enrollees). Three plan sponsors, each operating a single PDP in just one region, left the program completely: Alliance Medicare RX PDP, Colorado Access Vista Medicare PDP, Health Alliance Medicare Prescription Plan - Basic PDP. Each PDP had about 1,000 enrollees. Four other plan sponsors (EnvisionRxPlus, MedicareBlue Rx, SmartSaver Rx, and United American) made small adjustments to their offerings. The decision by Blue Cross Blue Shield plans in the upper Midwest region to drop their Value Plus PDP will affect about 100,000 enrollees, but the other changes have much smaller effects.
.")
20 $8,000 $7,000 $6,000 $5,000 $4,000 $3,000 $5,100 $3,600 $2,250 Catastrophic Limit $6,955 $6,730 $6,440 $6,484 $6,154 $5,726 $5,451 True Out-of-Pocket Spending (TrOOP) $4,700 $4,750 $4,550 $4,550 $4,350 $4,050 $3,850 Initial Coverage Limit $2,700 $2,830 $2,840 $2,930 $2,970 $2,400 $2,510 $7,062 $6,691 $4,700 $4,550 $2,850 $2,960 $7,515 $4,850 $3,310 $2,000 $1,000 $0 Deductible $250 $265 $275 $295 $310 $310 $320 $325 $310 $320 $ NOTE: Estimates are rounded to nearest whole dollar. SOURCE: Data from the Centers for Medicare & Medicaid Services.

21 1 These enrollment counts include nearly 7 million Part D enrollees in employer-only plans, not otherwise analyzed for this spotlight. 2 Centers for Medicare and Medicaid Services, Medicare Advantage Premiums Remain Stable; Enrollment at All-Time High, September 21, 2015; 2016 PDP, MA, and SNP Landscape Source Files and related files are available at 3 For analysis of the 2015 Part D marketplace and ten-year trends, see Jack Hoadley, Juliette Cubanski, and Tricia Neuman, "Medicare Part D at Ten Years: The 2015 Marketplace and Key Trends, ," Kaiser Family Foundation, October 2015, available at analysis of the Part D marketplace for earlier years is available at 4 The average is weighted by enrollment. 5 Gretchen Jacobson, Anthony Damico, and Tricia Neuman, What s In and What s Out? Medicare Advantage Market Entries and Exits for 2016, Kaiser Family Foundation, October In addition, two PDPs offered by First Health (Aetna) changed contract numbers. 7 Based on authors' analysis using the CMS 2016 Part D Crosswalk file. 8 During 2015, the average premium continued to drop, most likely due to plan elections by newly eligible beneficiaries, who are likely to enroll in plans with below-average premiums. The average PDP premium fell from $37.20 in February to $37.02 in April to $36.68 in September, a net drop of 1 percent in seven months. 9 The average premium will increase from $28.18 in 2015 to $30.41 in 2016 for basic-benefit PDPs and will increase from $47.15 to $55.06 for enhanced-benefit PDPs. Enrollees in 37 PDPs will switch from enhanced to basic, but excluding them does not affect the rates of increase. 10 CMS, Medicare Prescription Drug Premiums Projected to Remain Stable, available at 11 Jack Hoadley, Juliette Cubanski, and Tricia Neuman, "Medicare Part D at Ten Years: The 2015 Marketplace and Key Trends, ," Kaiser Family Foundation, October 2015, available at marketplace-and-key-trends /. 12 Centers for Medicare & Medicaid Services, Annual Release of Part D National Average Bid Amount and Other Part C & D Bid Related Information, July 29, Juliette Cubanski and Tricia Neuman, Medicare's Income-Related Premiums: A Data Note, June 2015, available at 14 These calculations are made from the Plan Finder for one region and cover only national and near-national plans. 15 This amount corresponds to the estimated catastrophic coverage limit for non-low-income Subsidy enrollees ($7,063 for LIS enrollees), which corresponds to True Out-of-Pocket (TrOOP) spending of $4,850 (the amount used to determine when an enrollee reaches the catastrophic coverage threshold). 16 Plans qualifying through the de minimis policy are eligible for new enrollees, but will not receive auto-assigned enrollees. 17 Estimates for the total number of beneficiaries subject to paying a premium are based on plan data from the landscape and crosswalk files, together with CMS enrollment reports. The number to be reassigned will be released by CMS in November or December These counts of benchmark plans include those designated as de minimis plans, which will not receive auto-assigned enrollees. 19 Jack Hoadley, Elizabeth Hargrave, Laura Summer, Juliette Cubanski, and Tricia Neuman, To Switch or Not to Switch: Are Medicare Beneficiaries Switching Drug Plans To Save Money? Kaiser Family Foundation, October 2013, available at 20 Jack Hoadley, Laura Summer, Elizabeth Hargrave, Samuel Stromberg, Juliette Cubanski, and Tricia Neuman, To Switch or Be Switched: Examining Changes in Drug Plan Enrollment among Medicare Part D Low-Income Subsidy Beneficiaries Kaiser Family Foundation, July 2015, available at The Henry J. Kaiser Family Foundation Headquarters: 2400 Sand Hill Road, Menlo Park, CA Phone Washington Offices and Barbara Jordan Conference Center: 1330 G Street, NW, Washington, DC Phone Alerts: kff.org/ facebook.com/kaiserfamilyfoundation twitter.com/kaiserfamfound Filling the need for trusted information on national health issues, the Kaiser Family Foundation is a nonprofit organization based in Menlo Park, California.
Medicare Part D Prescription Drug Plans: The Marketplace in 2013 and Key Trends, 2006-2013
 December 2013 Issue Brief Medicare Part D Prescription Drug Plans: The Marketplace in 2013 and Key Trends, 2006-2013 Jack Hoadley and Laura Summer, Georgetown University Elizabeth Hargrave, NORC at the
December 2013 Issue Brief Medicare Part D Prescription Drug Plans: The Marketplace in 2013 and Key Trends, 2006-2013 Jack Hoadley and Laura Summer, Georgetown University Elizabeth Hargrave, NORC at the
Status report on Part D
 C h a p t e r14 Status report on Part D C H A P T E R 14 Status report on Part D Chapter summary In this chapter Each year the Commission provides a status report on the Medicare prescription drug benefit
C h a p t e r14 Status report on Part D C H A P T E R 14 Status report on Part D Chapter summary In this chapter Each year the Commission provides a status report on the Medicare prescription drug benefit
Medicare Part D Open Enrollment for 2014: Popular Plans Continue to Evolve
 Fact Sheet Medicare Part D Open Enrollment for 2014: Popular Plans Continue to Evolve By Leigh Purvis AARP Public Policy Institute AARP Public Policy Institute Premiums for many popular stand-alone Medicare
Fact Sheet Medicare Part D Open Enrollment for 2014: Popular Plans Continue to Evolve By Leigh Purvis AARP Public Policy Institute AARP Public Policy Institute Premiums for many popular stand-alone Medicare
Medicare Part D Open Enrollment for 2012: Increasing Plan Complexity Highlights Need for Careful Evaluation
 Fact Sheet Medicare Part D Open Enrollment for 202: Increasing Plan Complexity Highlights Need for Careful Evaluation Leigh Purvis, MPA, and N. Lee Rucker, MSPH AARP Public Policy Institute Medicare beneficiaries
Fact Sheet Medicare Part D Open Enrollment for 202: Increasing Plan Complexity Highlights Need for Careful Evaluation Leigh Purvis, MPA, and N. Lee Rucker, MSPH AARP Public Policy Institute Medicare beneficiaries
THE MEDICARE PART D LOW-INCOME SUBSIDY PROGRAM Experience to Date and Policy Issues for Consideration
 THE MEDICARE DRUG BENEFIT THE MEDICARE PART D LOW-INCOME SUBSIDY PROGRAM Experience to Date and Policy Issues for Consideration Prepared By Laura Summer Georgetown University Jack Hoadley Georgetown University
THE MEDICARE DRUG BENEFIT THE MEDICARE PART D LOW-INCOME SUBSIDY PROGRAM Experience to Date and Policy Issues for Consideration Prepared By Laura Summer Georgetown University Jack Hoadley Georgetown University
Medicare Advantage 2014 Spotlight: Plan Availability And Premiums
 December 2013 Issue Brief Medicare Advantage 2014 Spotlight: Plan Availability And Premiums Marsha Gold, Gretchen Jacobson, Anthony Damico, and Tricia Neuman Under the current Medicare program, beneficiaries
December 2013 Issue Brief Medicare Advantage 2014 Spotlight: Plan Availability And Premiums Marsha Gold, Gretchen Jacobson, Anthony Damico, and Tricia Neuman Under the current Medicare program, beneficiaries
To Switch or Not to Switch: Are Medicare Beneficiaries Switching Drug Plans To Save Money?
 October 2013 Issue Brief To Switch or Not to Switch: Are Medicare Beneficiaries Switching Drug Plans To Save Money? Jack Hoadley, Elizabeth Hargrave, Laura Summer, Juliette Cubanski, and Tricia Neuman
October 2013 Issue Brief To Switch or Not to Switch: Are Medicare Beneficiaries Switching Drug Plans To Save Money? Jack Hoadley, Elizabeth Hargrave, Laura Summer, Juliette Cubanski, and Tricia Neuman
Status report on Part D
 C h a p t e r15 Status report on Part D C H A P T E R 15 Status report on Part D Chapter summary In this chapter Each year the Commission provides a status report on Part D to: provide information on
C h a p t e r15 Status report on Part D C H A P T E R 15 Status report on Part D Chapter summary In this chapter Each year the Commission provides a status report on Part D to: provide information on
Part D. 2016 Medicare Prescription Drug Plans in Virginia
 Part D 2016 Medicare Prescription Drug Plans in Virginia Source - U.S. Department of Health and Human Services Center for Medicare & Medicaid Services CMS Publication No. 10050-33 - September 2015 Medicare
Part D 2016 Medicare Prescription Drug Plans in Virginia Source - U.S. Department of Health and Human Services Center for Medicare & Medicaid Services CMS Publication No. 10050-33 - September 2015 Medicare
Your 2014 Guide to. Medicare Part D. Have you done your yearly Medicare Part D Plan review?
 Your 2014 Guide to Medicare Part D Have you done your yearly Medicare Part D Plan review? The Fall Open Enrollment Period, during which people with Medicare can make unrestricted changes to their coverage
Your 2014 Guide to Medicare Part D Have you done your yearly Medicare Part D Plan review? The Fall Open Enrollment Period, during which people with Medicare can make unrestricted changes to their coverage
2013 CIGNA MEDICARE RX (PDP) A MEDICARE PRESCRIPTION DRUG PLAN
 A MEDICARE PRESCRIPTION DRUG PLAN") 2013 CIGNA MEDICARE RX (PDP) A MEDICARE PRESCRIPTION DRUG PLAN 805978 i 08/12 S5617_5978i CMS Approved TABLE OF CONTENTS page Medicare overview 3 Medicare Part D 5 Cigna Medicare Rx (PDP) plans 12 Additional
2013 CIGNA MEDICARE RX (PDP) A MEDICARE PRESCRIPTION DRUG PLAN 805978 i 08/12 S5617_5978i CMS Approved TABLE OF CONTENTS page Medicare overview 3 Medicare Part D 5 Cigna Medicare Rx (PDP) plans 12 Additional
Understanding Medicare Part D. Cynthia Tudor, Ph.D. Acting Director, Medicare Drug Benefit Group
 Understanding Medicare Part D Cynthia Tudor, Ph.D. Acting Director, Medicare Drug Benefit Group Medicare Modernization Act Prescription Drug Coverage The Medicare Modernization Act (MMA) of 2003 provides
Understanding Medicare Part D Cynthia Tudor, Ph.D. Acting Director, Medicare Drug Benefit Group Medicare Modernization Act Prescription Drug Coverage The Medicare Modernization Act (MMA) of 2003 provides
Choosing a Medicare Part D Plan: Are Medicare Beneficiaries Choosing Low-Cost Plans?
 THE MEDICARE DRUG BENEFIT Choosing a Medicare Part D Plan: Are Medicare Beneficiaries Choosing Low-Cost Plans? Prepared By: Jonathan Gruber MIT For: The Henry J. Kaiser Family Foundation March 2009 This
THE MEDICARE DRUG BENEFIT Choosing a Medicare Part D Plan: Are Medicare Beneficiaries Choosing Low-Cost Plans? Prepared By: Jonathan Gruber MIT For: The Henry J. Kaiser Family Foundation March 2009 This
Part D payment system
 Part D payment system paymentbasics Revised: October 204 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 70 Washington, DC 2000 ph: 202-220-3700 fax: 202-220-3759
Part D payment system paymentbasics Revised: October 204 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 70 Washington, DC 2000 ph: 202-220-3700 fax: 202-220-3759
The Medicare Drug Benefit (Part D)
") THE BASICS The Medicare Drug Benefit (Part D) The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) established a voluntary outpatient prescription drug benefit for Medicare
THE BASICS The Medicare Drug Benefit (Part D) The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) established a voluntary outpatient prescription drug benefit for Medicare
Guide to Choosing a Medicare Prescription Drug Plan in Connecticut
 Medicare Prescription Drug - Choosing the Plan that s Right for You! Guide to Choosing a Medicare Prescription Drug Plan in Connecticut Medicare Prescription Drug, also called Part D or Medicare Rx, is
Medicare Prescription Drug - Choosing the Plan that s Right for You! Guide to Choosing a Medicare Prescription Drug Plan in Connecticut Medicare Prescription Drug, also called Part D or Medicare Rx, is
What is the Low Income Subsidy? Ginger Rogers Medicare Part D Disability Drug Benefit Helpline Disability Rights Wisconsin
 What is the Low Income Subsidy? Ginger Rogers Medicare Part D Disability Drug Benefit Helpline Disability Rights Wisconsin 1 What is the Low Income Subsidy? Also known as LIS or Extra Help Medicare beneficiaries
What is the Low Income Subsidy? Ginger Rogers Medicare Part D Disability Drug Benefit Helpline Disability Rights Wisconsin 1 What is the Low Income Subsidy? Also known as LIS or Extra Help Medicare beneficiaries
2016 Plan Decision Guide Your guide to making an informed Medicare Part D choice
 2016 Plan Decision Guide Your guide to making an informed Medicare Part D choice SilverScript is a Prescription Drug Plan with a Medicare contract offered by SilverScript Insurance Company. Enrollment
2016 Plan Decision Guide Your guide to making an informed Medicare Part D choice SilverScript is a Prescription Drug Plan with a Medicare contract offered by SilverScript Insurance Company. Enrollment
Dartmouth / SilverScript Retiree Prescription Drug Plan
 Dartmouth / SilverScript Retiree Prescription Drug Plan Agenda What s Happening /Why the Change? What is Medicare Part-D? Who is SilverScript? How is this affecting my Dartmouth coverage? What do I need
Dartmouth / SilverScript Retiree Prescription Drug Plan Agenda What s Happening /Why the Change? What is Medicare Part-D? Who is SilverScript? How is this affecting my Dartmouth coverage? What do I need
Quality Ratings of Medicare Advantage Plans, 2011
 Issue Brief Quality Ratings of Medicare Advantage Plans, 2011 February 2011 This information was reprinted with permission from the Henry J. Kaiser Family Foundation. The Kaiser Family Foundation is a
Issue Brief Quality Ratings of Medicare Advantage Plans, 2011 February 2011 This information was reprinted with permission from the Henry J. Kaiser Family Foundation. The Kaiser Family Foundation is a
Article from: Health Watch. January 2013 Issue 71
 Article from: Health Watch January 2013 Issue 71 Similarities between Medicare Prescription Drug Plans and Commercial Exchanges By Shelly S. Brandel and Douglas A. Proebsting The Affordable Care Act (ACA)
Article from: Health Watch January 2013 Issue 71 Similarities between Medicare Prescription Drug Plans and Commercial Exchanges By Shelly S. Brandel and Douglas A. Proebsting The Affordable Care Act (ACA)
AN OVERVIEW OF THE MEDICARE PROGRAM AND MEDICARE BENEFICIARIES COSTS AND SERVICE USE
 AN OVERVIEW OF THE MEDICARE PROGRAM AND MEDICARE BENEFICIARIES COSTS AND SERVICE USE Statement of Juliette Cubanski, Ph.D. Associate Director, Program on Medicare Policy The Henry J. Kaiser Family Foundation
AN OVERVIEW OF THE MEDICARE PROGRAM AND MEDICARE BENEFICIARIES COSTS AND SERVICE USE Statement of Juliette Cubanski, Ph.D. Associate Director, Program on Medicare Policy The Henry J. Kaiser Family Foundation
Medicare Advantage 2015 Spotlight: Enrollment Market Update
 Medicare Advantage 2015 Spotlight: Enrollment Market Update Gretchen Jacobson, Anthony Damico, Tricia Neuman, and Marsha Gold Despite concerns that reductions in payments to Medicare Advantage plans enacted
Medicare Advantage 2015 Spotlight: Enrollment Market Update Gretchen Jacobson, Anthony Damico, Tricia Neuman, and Marsha Gold Despite concerns that reductions in payments to Medicare Advantage plans enacted
Regional PPOs in Medicare: What Are The Prospects?
 Regional PPOs in Medicare: What Are The Prospects? How Do They Contain Rising Costs? By Steven D. Pizer, Austin B. Frakt and Roger Feldman* February 2007 * Steven D. Pizer, Ph.D. is assistant professor
Regional PPOs in Medicare: What Are The Prospects? How Do They Contain Rising Costs? By Steven D. Pizer, Austin B. Frakt and Roger Feldman* February 2007 * Steven D. Pizer, Ph.D. is assistant professor
MONTANA 2007 MEDICARE PART D STAND-ALONE PRESCRIPTION DRUG PLANS
 MONTANA 2007 MEDICARE PART D STAND-ALONE PRESCRIPTION DRUG PLANS DATE AS OF SEPTEMBER 12, 2006. INCLUDES ALL CONTRACTS/PLANS REGARDLESS OF 2007 APPROVAL STATUS Company Name Plan Name Benefit Type $0 Premium
MONTANA 2007 MEDICARE PART D STAND-ALONE PRESCRIPTION DRUG PLANS DATE AS OF SEPTEMBER 12, 2006. INCLUDES ALL CONTRACTS/PLANS REGARDLESS OF 2007 APPROVAL STATUS Company Name Plan Name Benefit Type $0 Premium
Insurance Trust for Delta Retirees 2013 Prescription Drug Plan (PDP)
") Your Plan Explained Insurance Trust for Delta Retirees 2013 Prescription Drug Plan (PDP) UnitedHealthcare MedicareRx for Groups (PDP) Y0066_PDP_896487_000 What is Medicare Part D? Medicare Part D is a
Your Plan Explained Insurance Trust for Delta Retirees 2013 Prescription Drug Plan (PDP) UnitedHealthcare MedicareRx for Groups (PDP) Y0066_PDP_896487_000 What is Medicare Part D? Medicare Part D is a
Trends in Medigap Coverage and Enrollment, 2011
 Trends in Medigap Coverage and Enrollment, 2011 May 2012 SUMMARY This report presents trends in enrollment in Medicare Supplement (Medigap) insurance coverage, using data on the number of policies in force
Trends in Medigap Coverage and Enrollment, 2011 May 2012 SUMMARY This report presents trends in enrollment in Medicare Supplement (Medigap) insurance coverage, using data on the number of policies in force
Montana. Medicare Drug Plan Ratings. Analytics by Avalere Health
 This AARP rating tool contains information about stand-alone Medicare plans in your state that cover only prescription drugs. Each year, from November 15 to December 31, people enrolled in a Medicare drug
This AARP rating tool contains information about stand-alone Medicare plans in your state that cover only prescription drugs. Each year, from November 15 to December 31, people enrolled in a Medicare drug
Medicare Part D Prescription Drug Coverage
 Medicare Part D Prescription Drug Coverage Part 3 Version 6.0 September 25, 2012 Terms and Conditions This training program is protected under United States Copyright laws, 17 U.S.C.A. 101, et seq. and
Medicare Part D Prescription Drug Coverage Part 3 Version 6.0 September 25, 2012 Terms and Conditions This training program is protected under United States Copyright laws, 17 U.S.C.A. 101, et seq. and
Medicare Advantage 2014 Spotlight: Enrollment Market Update
 Medicare Advantage 2014 Spotlight: Enrollment Market Update Marsha Gold, Gretchen Jacobson, Anthony Damico, and Tricia Neuman Despite concerns that payment changes enacted in the Affordable Care Act of
Medicare Advantage 2014 Spotlight: Enrollment Market Update Marsha Gold, Gretchen Jacobson, Anthony Damico, and Tricia Neuman Despite concerns that payment changes enacted in the Affordable Care Act of
2013 California Medicare Prescription Drug Plans (PDPs)
") 2013 California Medicare Prescription Plans (PDPs) The following Medicare prescription drug plans are available to California residents. This information was taken from the Medicare Web site, www.medicare.gov.
2013 California Medicare Prescription Plans (PDPs) The following Medicare prescription drug plans are available to California residents. This information was taken from the Medicare Web site, www.medicare.gov.
Kaiser Family Foundation/eHealthInsurance. August 2004
 AUGUST 2004 Revised Update on Individual Health Insurance Kaiser Family Foundation/eHealthInsurance August 2004 Revised Update on Individual Health Insurance B a c k g r o u n d In recent years, President
AUGUST 2004 Revised Update on Individual Health Insurance Kaiser Family Foundation/eHealthInsurance August 2004 Revised Update on Individual Health Insurance B a c k g r o u n d In recent years, President
a Medicare Prescription Drug Plan in Connecticut
 Medicare Prescription Drug Coverage - Choosing the Plan that s Right for You! %(OL.4. ftqve cfloicrs * dflid~,i,,na * S l~ataxtpqnin t LOCAL HELP FOR PEOPlE WITH MEDICARE Empowering SenIors To Prevent
Medicare Prescription Drug Coverage - Choosing the Plan that s Right for You! %(OL.4. ftqve cfloicrs * dflid~,i,,na * S l~ataxtpqnin t LOCAL HELP FOR PEOPlE WITH MEDICARE Empowering SenIors To Prevent
Medicare Part D s competitive design: Do Part D enrollees switch plans? Shinobu Suzuki June 23, 2013
 Medicare Part D s competitive design: Do Part D enrollees switch plans? Shinobu Suzuki June 23, 2013 Part D s competitive design Intended to provide sponsors incentives to offer attractive coverage while
Medicare Part D s competitive design: Do Part D enrollees switch plans? Shinobu Suzuki June 23, 2013 Part D s competitive design Intended to provide sponsors incentives to offer attractive coverage while
Medicare Advantage 2013 Spotlight:
 issue brief Medicare Advantage 2013 Spotlight: June 2013 Enrollment Market Update Prepared by Marsha Gold i ; and Gretchen Jacobson, Anthony Damico, and Tricia Neuman ii In 2013, 14.4 million Medicare
issue brief Medicare Advantage 2013 Spotlight: June 2013 Enrollment Market Update Prepared by Marsha Gold i ; and Gretchen Jacobson, Anthony Damico, and Tricia Neuman ii In 2013, 14.4 million Medicare
Prescription Drug Coverage for Medicare Beneficiaries: A Summary of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003
 Prescription Drug Coverage for Medicare Beneficiaries: A Summary of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 Prepared by Health Policy Alternatives, Inc. for The Henry
Prescription Drug Coverage for Medicare Beneficiaries: A Summary of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 Prepared by Health Policy Alternatives, Inc. for The Henry
It Pays to Shop: Variation in Out-of-Pocket Costs for Medicare Part D Enrollees in 2016
 It Pays to Shop: Variation in Out-of-Pocket Costs for Medicare Part D Enrollees in 2016 Medicare Part D drug plans differ considerably in the drugs they list on their formularies, their use of formulary
It Pays to Shop: Variation in Out-of-Pocket Costs for Medicare Part D Enrollees in 2016 Medicare Part D drug plans differ considerably in the drugs they list on their formularies, their use of formulary
Successes and Challenges in the Affordable Care Act: Beyond Access
 Successes and Challenges in the Affordable Care Act: Beyond Access Robert Greenwald Clinical Professor of Law, Harvard Law School Director, Center for Health Law and Policy Innovation/Treatment Access
Successes and Challenges in the Affordable Care Act: Beyond Access Robert Greenwald Clinical Professor of Law, Harvard Law School Director, Center for Health Law and Policy Innovation/Treatment Access
What s New with Medicare in 2015
 November 2014 What s New with Medicare in 2015 Audio Portion: 1-866-740-1260 Web Portion: www.readytalk.com Code: 4796976 1 What we ll cover today 2015 Medicare cost sharing Part D in 2015 What s the big
November 2014 What s New with Medicare in 2015 Audio Portion: 1-866-740-1260 Web Portion: www.readytalk.com Code: 4796976 1 What we ll cover today 2015 Medicare cost sharing Part D in 2015 What s the big
Trends in Medigap Enrollment and Coverage Options, 2013
 November 2014 Trends in Medigap Enrollment and Coverage Options, 2013 www.ahipresearch.org LIST OF TABLES AND FIGURES TABLE 1. TABLE 2. TABLE 3. TABLE 4. Distribution of Medigap Companies with Standardized
November 2014 Trends in Medigap Enrollment and Coverage Options, 2013 www.ahipresearch.org LIST OF TABLES AND FIGURES TABLE 1. TABLE 2. TABLE 3. TABLE 4. Distribution of Medigap Companies with Standardized
The 80/20 Rule: How Insurers Spend Your Health Insurance Premiums
 SUMMARY The 80/20 Rule: How Insurers Spend Your Health Insurance Premiums The Affordable Care Act holds health insurers accountable to consumers and ensures that American families receive value for their
SUMMARY The 80/20 Rule: How Insurers Spend Your Health Insurance Premiums The Affordable Care Act holds health insurers accountable to consumers and ensures that American families receive value for their
Medicare Part D Plans: A Cost Rollercoaster for Seniors
 Medicare Part D Plans: A Cost Rollercoaster for Seniors Tracking sample finds cost increases, frequent cost fluctuations in Medicare prescription drug plans February 2007 EMBARGOED UNTIL 6 p.m. EST, WEDNESDAY,
Medicare Part D Plans: A Cost Rollercoaster for Seniors Tracking sample finds cost increases, frequent cost fluctuations in Medicare prescription drug plans February 2007 EMBARGOED UNTIL 6 p.m. EST, WEDNESDAY,
ehealth Price Index Trends and Costs in the Short-Term Health Insurance Market, 2013 and 2014
 ehealth Price Index Trends and Costs in the Short-Term Health Insurance Market, 2013 and 2014 June 2015 1 INTRODUCTION In this report, ehealth provides an analysis of consumer shopping trends and premium
ehealth Price Index Trends and Costs in the Short-Term Health Insurance Market, 2013 and 2014 June 2015 1 INTRODUCTION In this report, ehealth provides an analysis of consumer shopping trends and premium
MEDICARE PART D THE BASICS
 THE BASICS Participation is voluntary. The income level and assets of beneficiaries determine the level of prescription assistance they will receive. Beneficiaries with incomes over 150% of the Federal
THE BASICS Participation is voluntary. The income level and assets of beneficiaries determine the level of prescription assistance they will receive. Beneficiaries with incomes over 150% of the Federal
Significance of the Coverage Gap Under Medicare Part D
 June 8, 2006 Significance of the Coverage Gap Under Medicare Part D The gap in coverage between spending levels of $2,250 and $3,600 in true out-of-pocket spending is one of the most discussed aspects
June 8, 2006 Significance of the Coverage Gap Under Medicare Part D The gap in coverage between spending levels of $2,250 and $3,600 in true out-of-pocket spending is one of the most discussed aspects
Health Insurance Price Index Report for Open Enrollment and Q1 2014. May 2014
 Health Insurance Price Index Report for Open Enrollment and May 2014 ehealth 5.2014 Table of Contents Introduction... 3 Executive Summary and Highlights... 4 Nationwide Health Insurance Costs National
Health Insurance Price Index Report for Open Enrollment and May 2014 ehealth 5.2014 Table of Contents Introduction... 3 Executive Summary and Highlights... 4 Nationwide Health Insurance Costs National
Medicare Advantage Plan Landscape Data Summary
 2013 Medicare Advantage Plan Landscape Data Summary Table of Contents Report Overview...3 Medicare Advantage Costs and Benefits...4 The Maximum Out of Pocket (MOOP) Benefit How It Works...4 The Prescription
2013 Medicare Advantage Plan Landscape Data Summary Table of Contents Report Overview...3 Medicare Advantage Costs and Benefits...4 The Maximum Out of Pocket (MOOP) Benefit How It Works...4 The Prescription
Recent Trends in Medicaid and CHIP Enrollment: Analysis of CMS Performance Measure Data through August 2014
 Recent Trends in and CHIP Enrollment: Analysis of CMS Performance Measure Data through August Samantha Artiga, Robin Rudowitz, Jessica Stephens and Laura Snyder Starting in December 2013, the Centers for
Recent Trends in and CHIP Enrollment: Analysis of CMS Performance Measure Data through August Samantha Artiga, Robin Rudowitz, Jessica Stephens and Laura Snyder Starting in December 2013, the Centers for
Improving Medicare Part D. Shinobu Suzuki and Rachel Schmidt March 3, 2016
 Improving Medicare Part D Shinobu Suzuki and Rachel Schmidt March 3, 2016 Future challenges require changes to Part D s original structure Designed to encourage broad participation by plans and beneficiaries
Improving Medicare Part D Shinobu Suzuki and Rachel Schmidt March 3, 2016 Future challenges require changes to Part D s original structure Designed to encourage broad participation by plans and beneficiaries
Get Ready! Get Set! Go! Medicare Part D in Minnesota
 Get Ready! Get Set! Go! Medicare Part D in Minnesota Videoconference Training For State Operated Services January 31, 2006 Kelli Jo Greiner, Minnesota Board on Aging and MN-DHS Continuing Care MMA: Overview
Get Ready! Get Set! Go! Medicare Part D in Minnesota Videoconference Training For State Operated Services January 31, 2006 Kelli Jo Greiner, Minnesota Board on Aging and MN-DHS Continuing Care MMA: Overview
Medicare Part D: 2010. Presented by: Howard Houghton Virginia Insurance Counseling & Assistance Program (VICAP)
") Medicare Part D: 2010 Presented by: Howard Houghton Virginia Insurance Counseling & Assistance Program (VICAP) 1 The Basics Medicare Part D is available to all Medicare beneficiaries regardless of their
Medicare Part D: 2010 Presented by: Howard Houghton Virginia Insurance Counseling & Assistance Program (VICAP) 1 The Basics Medicare Part D is available to all Medicare beneficiaries regardless of their
HEALTH INSURANCE PRICE INDEX REPORT FOR THE 2015
 HEALTH INSURANCE PRICE INDEX REPORT FOR THE 2015 OPEN ENROLLMENT PERIOD March 2015 ehealth 3.2015 Table of Contents Introduction... 3 Executive Summary and Highlights... 4 Nationwide Health Insurance Costs
HEALTH INSURANCE PRICE INDEX REPORT FOR THE 2015 OPEN ENROLLMENT PERIOD March 2015 ehealth 3.2015 Table of Contents Introduction... 3 Executive Summary and Highlights... 4 Nationwide Health Insurance Costs
kaiser medicaid and the uninsured commission on The Cost and Coverage Implications of the ACA Medicaid Expansion: National and State-by-State Analysis
 kaiser commission on medicaid and the uninsured The Cost and Coverage Implications of the ACA Medicaid Expansion: National and State-by-State Analysis John Holahan, Matthew Buettgens, Caitlin Carroll,
kaiser commission on medicaid and the uninsured The Cost and Coverage Implications of the ACA Medicaid Expansion: National and State-by-State Analysis John Holahan, Matthew Buettgens, Caitlin Carroll,
HIV Services, Ryan White Programs and the Affordable Care Act: What do we know now?
 HIV Services, Ryan White Programs and the Affordable Care Act: What do we know now? Thursday April 10, 2014 Presented by Carole Treston, RN, MPH Chief Nursing Officer Association of Nurses in AIDS Care
HIV Services, Ryan White Programs and the Affordable Care Act: What do we know now? Thursday April 10, 2014 Presented by Carole Treston, RN, MPH Chief Nursing Officer Association of Nurses in AIDS Care
Health Insurance Exchanges and the Medicaid Expansion After the Supreme Court Decision: State Actions and Key Implementation Issues
 Health Insurance Exchanges and the Medicaid Expansion After the Supreme Court Decision: State Actions and Key Implementation Issues Sara R. Collins, Ph.D. Vice President, Affordable Health Insurance The
Health Insurance Exchanges and the Medicaid Expansion After the Supreme Court Decision: State Actions and Key Implementation Issues Sara R. Collins, Ph.D. Vice President, Affordable Health Insurance The
Revolution or Evolution: What s Happening Next for MedAdv and Prescription Drug Plans
 Revolution or Evolution: What s Happening Next for MedAdv and Prescription Drug Plans Issues & Trends in Medicare Supplement Insurance 2012 Conference Presented by: T. Scott Bentley, FSA, MAAA Consulting
Revolution or Evolution: What s Happening Next for MedAdv and Prescription Drug Plans Issues & Trends in Medicare Supplement Insurance 2012 Conference Presented by: T. Scott Bentley, FSA, MAAA Consulting
Medicare Open Enrollment. 1-800-MEDICARE www.medicare.gov
 Medicare Open Enrollment 1-800-MEDICARE www.medicare.gov Objectives Following this session you should be able to Provide an overview of key dates Know how to compare Medicare plans Describe how to join
Medicare Open Enrollment 1-800-MEDICARE www.medicare.gov Objectives Following this session you should be able to Provide an overview of key dates Know how to compare Medicare plans Describe how to join
Fact Sheet - 2014 Star Ratings
 Fact Sheet - 2014 Star Ratings Star Ratings are driving improvements in Medicare quality. This year there have been significant increases in the number of Medicare beneficiaries in high-performing Medicare
Fact Sheet - 2014 Star Ratings Star Ratings are driving improvements in Medicare quality. This year there have been significant increases in the number of Medicare beneficiaries in high-performing Medicare
Comparing Affordability and Benefits Between CHIP and Qualified Health Plans in 35 States: Which Coverage is Best for Kids?
 Comparing Affordability and Benefits Between CHIP and Qualified Health Plans in 35 States: Which Coverage is Best for Kids? The Children s Health Insurance Program (CHIP) was enacted in 1997 by a bipartisan
Comparing Affordability and Benefits Between CHIP and Qualified Health Plans in 35 States: Which Coverage is Best for Kids? The Children s Health Insurance Program (CHIP) was enacted in 1997 by a bipartisan
State Pharmacy Assistance Programs vs. Medicare Prescription Drug Plans:
 State Pharmacy Assistance Programs vs. Medicare Prescription Drug Plans: How Do They Contain Rising Costs? By Sarah Goodell, Jack Hoadley, Ellen O Brien, and Claudia Williams* October 2005 This policy
State Pharmacy Assistance Programs vs. Medicare Prescription Drug Plans: How Do They Contain Rising Costs? By Sarah Goodell, Jack Hoadley, Ellen O Brien, and Claudia Williams* October 2005 This policy
REPORT. A Primer on Medicare. March 2015 KEY FACTS ABOUT THE MEDICARE PROGRAM AND THE PEOPLE IT COVERS
 REPORT A Primer on Medicare March 2015 KEY FACTS ABOUT THE MEDICARE PROGRAM AND THE PEOPLE IT COVERS This primer was prepared by Juliette Cubanski, Christina Swoope, Cristina Boccuti, Gretchen Jacobson,
REPORT A Primer on Medicare March 2015 KEY FACTS ABOUT THE MEDICARE PROGRAM AND THE PEOPLE IT COVERS This primer was prepared by Juliette Cubanski, Christina Swoope, Cristina Boccuti, Gretchen Jacobson,
More Dental Benefits Options in 2015 Health Insurance Marketplaces
 More Dental Benefits Options in 2015 Health Insurance Marketplaces Authors: Cassandra Yarbrough, M.P.P.; Marko Vujicic, Ph.D.; Kamyar Nasseh, Ph.D. The Health Policy Institute (HPI) is a thought leader
More Dental Benefits Options in 2015 Health Insurance Marketplaces Authors: Cassandra Yarbrough, M.P.P.; Marko Vujicic, Ph.D.; Kamyar Nasseh, Ph.D. The Health Policy Institute (HPI) is a thought leader
More Dental Benefits Options in 2015 Health Insurance Marketplaces
 More Dental Benefits Options in 2015 Health Insurance Marketplaces Authors: Cassandra Yarbrough, M.P.P.; Marko Vujicic, Ph.D.; Kamyar Nasseh, Ph.D. The Health Policy Institute (HPI) is a thought leader
More Dental Benefits Options in 2015 Health Insurance Marketplaces Authors: Cassandra Yarbrough, M.P.P.; Marko Vujicic, Ph.D.; Kamyar Nasseh, Ph.D. The Health Policy Institute (HPI) is a thought leader
Medicare Part D. MMA establishes a standard Part D drug benefit, which consists of four components or phases.
 Medicare Part D The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) added voluntary prescription drug coverage to Medicare, the federal health insurance program for seniors
Medicare Part D The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) added voluntary prescription drug coverage to Medicare, the federal health insurance program for seniors
New Federal Rating Rules
 New Federal Rating Rules The Patient Protection and Affordable Care Act ( PPACA ) includes new federal rules limiting the extent to which insurance companies can impose premium surcharges on individuals
New Federal Rating Rules The Patient Protection and Affordable Care Act ( PPACA ) includes new federal rules limiting the extent to which insurance companies can impose premium surcharges on individuals
How To Regulate Rate Regulation
 Rate Regulation Introduction Concerns over the fairness and equity of insurer rating practices that attempt to charge higher premiums to those with higher actual and expected claims costs have increased
Rate Regulation Introduction Concerns over the fairness and equity of insurer rating practices that attempt to charge higher premiums to those with higher actual and expected claims costs have increased
Health Reform. Health Insurance Market Reforms: Pre-Existing Condition Exclusions
 Health Insurance Market Reforms: Pre-Existing Cditi Exclusis SEPTEMBER 2012 Overview What is a pre-existing cditi? Pre-existing cditis are medical cditis or other health problems that existed before the
Health Insurance Market Reforms: Pre-Existing Cditi Exclusis SEPTEMBER 2012 Overview What is a pre-existing cditi? Pre-existing cditis are medical cditis or other health problems that existed before the
2016 Individual Exchange Premiums updated November 4, 2015
 2016 Individual Exchange Premiums updated November 4, 2015 Within the document, you'll find insights across 50 states and DC with available findings (i.e., carrier participation, price leadership, gross
2016 Individual Exchange Premiums updated November 4, 2015 Within the document, you'll find insights across 50 states and DC with available findings (i.e., carrier participation, price leadership, gross
MEDIGAP: Spotlight on Enrollment, Premiums, and recent TrendS 1
 MEDIGAP: Spotlight on Enrollment, Premiums, and Recent Trends EXECUTIVE SUMMARY Medicare supplemental insurance, also known as Medigap, is an important source of supplemental coverage for nearly one in
MEDIGAP: Spotlight on Enrollment, Premiums, and Recent Trends EXECUTIVE SUMMARY Medicare supplemental insurance, also known as Medigap, is an important source of supplemental coverage for nearly one in
Basic Reimbursement - Medicare Part D Specifics
 Basic Reimbursement - Medicare Part D Specifics 60889-R8-V1 (c) 2012 Amgen Inc. All rights reserved 2 This information is provided for your background education and is not intended to serve as guidance
Basic Reimbursement - Medicare Part D Specifics 60889-R8-V1 (c) 2012 Amgen Inc. All rights reserved 2 This information is provided for your background education and is not intended to serve as guidance
MEDICARE PART D PRESCRIPTION DRUG COVERAGE 2016
 PO Box 350 Willimantic, Connecticut 06226 (860)456-7790 (800)262-4414 1025 Connecticut Ave, NW Suite 709 Washington, DC 20036 (202)293-5760 MEDICARE PART D PRESCRIPTION DRUG COVERAGE 2016 Se habla español
PO Box 350 Willimantic, Connecticut 06226 (860)456-7790 (800)262-4414 1025 Connecticut Ave, NW Suite 709 Washington, DC 20036 (202)293-5760 MEDICARE PART D PRESCRIPTION DRUG COVERAGE 2016 Se habla español
Health Insurance Coverage of Children Under Age 19: 2008 and 2009
 Health Insurance Coverage of Children Under Age 19: 2008 and 2009 American Community Survey Briefs Issued September 2010 ACSBR/09-11 IntroductIon Health insurance, whether private or public, improves children
Health Insurance Coverage of Children Under Age 19: 2008 and 2009 American Community Survey Briefs Issued September 2010 ACSBR/09-11 IntroductIon Health insurance, whether private or public, improves children
MEDIGAP: Spotlight on Enrollment, Premiums, and Recent Trends. Jennifer Huang Policy Analyst, Program on Medicare Policy Kaiser Family Foundation
 MEDIGAP: Spotlight on Enrollment, Premiums, and Recent Trends Jennifer Huang Policy Analyst, Program on Medicare Policy Kaiser Family Foundation AcademyHealth 2013 Annual Research Meeting Tuesday, June
MEDIGAP: Spotlight on Enrollment, Premiums, and Recent Trends Jennifer Huang Policy Analyst, Program on Medicare Policy Kaiser Family Foundation AcademyHealth 2013 Annual Research Meeting Tuesday, June
Marketplaces (Exchanges): Information for Employers and Individuals Lisa Klinger, J.D. www.leavitt.com/healthcarereform.com
: Information for Employers and Individuals Lisa Klinger, J.D. www.leavitt.com/healthcarereform.com") 10-21- 2013 As of January 1, 2014, the Patient Protection and Affordable Care Act (PPACA) requires most U.S. citizens and lawful residents to either have minimum essential coverage or to pay a federal
10-21- 2013 As of January 1, 2014, the Patient Protection and Affordable Care Act (PPACA) requires most U.S. citizens and lawful residents to either have minimum essential coverage or to pay a federal
Prescription Drug Benefits Under Part D of the Medicare Modernization Act The Genie s Out of the Bottle
 ISSUE BRIEF VOL. 5, NO. 10, 2005 This ongoing series provides information on how to develop programs to educate Medicare beneficiaries and their families. Additional information about this and other projects
ISSUE BRIEF VOL. 5, NO. 10, 2005 This ongoing series provides information on how to develop programs to educate Medicare beneficiaries and their families. Additional information about this and other projects
MEDICARE.GOV DRUG PLAN FINDER TOOL
 MEDICARE.GOV DRUG PLAN FINDER TOOL Part 1 Part 2 A General Search is adequate for most people --The only required entry is your zip code Page 1 of 12 Part 3 Check the appropriate box under each section
MEDICARE.GOV DRUG PLAN FINDER TOOL Part 1 Part 2 A General Search is adequate for most people --The only required entry is your zip code Page 1 of 12 Part 3 Check the appropriate box under each section
2015 Medicare Low-Income Subsidy (LIS), or Extra Help
, or Extra Help") 2015 Medicare Low-Income Subsidy (LIS), or Extra Help Extra Help with Prescription Drug Costs Medicare LIS Overview Patient Eligibility and Application Process How LIS Affects Patient Responsibility for
2015 Medicare Low-Income Subsidy (LIS), or Extra Help Extra Help with Prescription Drug Costs Medicare LIS Overview Patient Eligibility and Application Process How LIS Affects Patient Responsibility for
THE EMERITI PROGRAM in your retirement years
 2014 Benefits THE EMERITI PROGRAM in your retirement years Helping you achieve healthcare security in retirement This presentation is copyrighted exclusively by Emeriti 1 2 TODAY S AGENDA What s new in
2014 Benefits THE EMERITI PROGRAM in your retirement years Helping you achieve healthcare security in retirement This presentation is copyrighted exclusively by Emeriti 1 2 TODAY S AGENDA What s new in
AIDS Drug Assistance Programs (ADAPs)
") AIDS Drug Assistance Programs (ADAPs) AIDS Drug Assistance Programs (ADAPs) provide HIV-related prescription drugs to low-income people with HIV/AIDS who have limited or no prescription drug coverage.
AIDS Drug Assistance Programs (ADAPs) AIDS Drug Assistance Programs (ADAPs) provide HIV-related prescription drugs to low-income people with HIV/AIDS who have limited or no prescription drug coverage.
Summary of Medicare Provisions in the President s Budget for Fiscal Year 2016
 Summary of Medicare Provisions in the President s Budget for Fiscal Year 2016 Gretchen Jacobson, Cristina Boccuti, Juliette Cubanski, Christina Swoope, and Tricia Neuman On February 2, 2015, the Office
Summary of Medicare Provisions in the President s Budget for Fiscal Year 2016 Gretchen Jacobson, Cristina Boccuti, Juliette Cubanski, Christina Swoope, and Tricia Neuman On February 2, 2015, the Office
PEACE-OF-MIND IN RETIREMENT. Income Security + Healthcare Security = Retirement Readiness
 PEACE-OF-MIND IN RETIREMENT Income Security + Healthcare Security = Retirement Readiness 1 What s New In 2015 The Traditional Choice Plan will be discontinued A new, significantly enhanced Medicare Advantage
PEACE-OF-MIND IN RETIREMENT Income Security + Healthcare Security = Retirement Readiness 1 What s New In 2015 The Traditional Choice Plan will be discontinued A new, significantly enhanced Medicare Advantage
How To Get A Health Insurance Plan From Ctf
 Overview of Health Insurance Options for Medicare-Eligible Members The following pages offer general descriptions of the types of plans offered to CTPF retirees who are eligible for and maintain active
Overview of Health Insurance Options for Medicare-Eligible Members The following pages offer general descriptions of the types of plans offered to CTPF retirees who are eligible for and maintain active
UPDATED: NOVEMBER 2009 344.1 RESOURCES THIRD PARTY RESOURCES
 UPDATED: NOVEMBER 2009 344.1 NOTE: Enrollment in Medicare is a condition of eligibility for Medicaid. Beginning in 2006, persons entitled to Part A and/or enrolled in Part B are eligible for the prescription
UPDATED: NOVEMBER 2009 344.1 NOTE: Enrollment in Medicare is a condition of eligibility for Medicaid. Beginning in 2006, persons entitled to Part A and/or enrolled in Part B are eligible for the prescription
Seniors and the Affordable Care Act
 Seniors and the Affordable Care Act Jon M. Bailey Director of Research and Analysis October 2013 Since the Patient Protection and Affordable Care Act (ACA) was signed into law in March 2010, we have conducted
Seniors and the Affordable Care Act Jon M. Bailey Director of Research and Analysis October 2013 Since the Patient Protection and Affordable Care Act (ACA) was signed into law in March 2010, we have conducted
Prescription Drug Plan Sponsors, Medicare Advantage Organizations, Cost Plans, and Demonstration Organizations
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244-1850 CENTER FOR MEDICARE DATE: February 15, 2012 TO: FROM: SUBJECT: Prescription
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244-1850 CENTER FOR MEDICARE DATE: February 15, 2012 TO: FROM: SUBJECT: Prescription
Medicare Part D & Ryan White HIV/AIDS Program As of November 2008
 Medicare Part D & Ryan White HIV/AIDS Program As of November 2008 The below discussion can guide Ryan White HIV/AIDS programs in understanding implications of the Medicare Part D prescription drug benefit
Medicare Part D & Ryan White HIV/AIDS Program As of November 2008 The below discussion can guide Ryan White HIV/AIDS programs in understanding implications of the Medicare Part D prescription drug benefit
How To Know If You Can Pay More For Health Insurance
 JUNE 2012 Health Insurance Market Reforms: Rate Restrictis Overview What are rate restrictis? Rate restrictis limit how much insurance companies can vary premiums charged to individuals and businesses
JUNE 2012 Health Insurance Market Reforms: Rate Restrictis Overview What are rate restrictis? Rate restrictis limit how much insurance companies can vary premiums charged to individuals and businesses
OPPORTUNITIES IN THE AFFORDABLE CARE ACT TO IMPROVE HEALTH CARE COORDINATION AND DELIVERY FOR PEOPLE LIVING WITH HIV
 OPPORTUNITIES IN THE AFFORDABLE CARE ACT TO IMPROVE HEALTH CARE COORDINATION AND DELIVERY FOR PEOPLE LIVING WITH HIV Center for Health Law and Policy Innovation chlpi@law.harvard.edu www.chlpi.org CARMEL
OPPORTUNITIES IN THE AFFORDABLE CARE ACT TO IMPROVE HEALTH CARE COORDINATION AND DELIVERY FOR PEOPLE LIVING WITH HIV Center for Health Law and Policy Innovation chlpi@law.harvard.edu www.chlpi.org CARMEL
Frequently Asked Questions: Medicare Supplement & Medicare Advantage
 Frequently Asked Questions: Medicare Supplement & Medicare Advantage Who is eligible for CBIA s Medicare program? A CBIA Health Connections participant is eligible for either plan if they are qualified
Frequently Asked Questions: Medicare Supplement & Medicare Advantage Who is eligible for CBIA s Medicare program? A CBIA Health Connections participant is eligible for either plan if they are qualified
Annual Notice of Changes for 2015
 First Health Part D Value Plus (PDP) Plan offered by First Health Life & Health Insurance Company Annual Notice of Changes for 2015 You are currently enrolled as a member of First Health Part D Essentials
First Health Part D Value Plus (PDP) Plan offered by First Health Life & Health Insurance Company Annual Notice of Changes for 2015 You are currently enrolled as a member of First Health Part D Essentials
Texas Grantee Meeting
 Texas Grantee Meeting AmeriCorps Health Insurance Update March 27-28, 2014 Agenda Major Issues Situation for Current Program and Members Looking Ahead (September 1, 2014) Caveats Not Legal Advice Represent
Texas Grantee Meeting AmeriCorps Health Insurance Update March 27-28, 2014 Agenda Major Issues Situation for Current Program and Members Looking Ahead (September 1, 2014) Caveats Not Legal Advice Represent
First Health Part D Value Plus (PDP) offered by First Health Life & Health Insurance Company
 offered by First Health Life & Health Insurance Company") First Health Part D Value Plus (PDP) offered by First Health Life & Health Insurance Company Annual Notice of Changes for 2016 You are currently enrolled as a member of First Health Part D Value Plus (PDP).
First Health Part D Value Plus (PDP) offered by First Health Life & Health Insurance Company Annual Notice of Changes for 2016 You are currently enrolled as a member of First Health Part D Value Plus (PDP).
Choosing the Best Plan for You: A Tool for Purchasing Coverage in the Health Insurance Exchange
 Choosing the Best Plan for You: A Tool for Purchasing Coverage in the Health Insurance Exchange The Affordable Care Act (ACA) makes health insurance available to nearly all Americans and the law requires
Choosing the Best Plan for You: A Tool for Purchasing Coverage in the Health Insurance Exchange The Affordable Care Act (ACA) makes health insurance available to nearly all Americans and the law requires
Helping You Prepare For Your Upcoming Health Insurance Enrollment
 Helping You Prepare For Your Upcoming Health Insurance Enrollment Who We Are Transitions Can Be A Good Thing! OneExchange For Your Benefit A Deeper Dive Benefit Advisors, Private Exchange, Optimize Savings,
Helping You Prepare For Your Upcoming Health Insurance Enrollment Who We Are Transitions Can Be A Good Thing! OneExchange For Your Benefit A Deeper Dive Benefit Advisors, Private Exchange, Optimize Savings,
Office of the Actuary
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop N3-01-21 Baltimore, Maryland 21244-1850 Office of the Actuary DATE: March 25, 2008 FROM:
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop N3-01-21 Baltimore, Maryland 21244-1850 Office of the Actuary DATE: March 25, 2008 FROM:
2016 Group Retiree Medicare Plans
 2016 Group Retiree Medicare Plans Blue Cross MedicareRx (PDP) Medicare Part D Prescription Drug Plans Anthem Blue Cross is a stand-alone prescription drug plan with a Medicare contract. Enrollment in Anthem
2016 Group Retiree Medicare Plans Blue Cross MedicareRx (PDP) Medicare Part D Prescription Drug Plans Anthem Blue Cross is a stand-alone prescription drug plan with a Medicare contract. Enrollment in Anthem
LexisNexis Law Firm Billable Hours Survey Top Line Report. June 11, 2012
 LexisNexis Law Firm Billable Hours Survey Top Line Report June 11, 2012 Executive Summary by Law Firm Size According to the survey, we found that attorneys were not billing all the time they worked. There
LexisNexis Law Firm Billable Hours Survey Top Line Report June 11, 2012 Executive Summary by Law Firm Size According to the survey, we found that attorneys were not billing all the time they worked. There
Summary of Benefits. (PDP), Blue MedicareRx Plus SM. (PDP) and Blue MedicareRx Premier SM
, Blue MedicareRx Plus SM. (PDP) and Blue MedicareRx Premier SM") Summary of Benefits for SM, Plus SM and Premier SM Available in Maine and New Hampshire A -approved Part D sponsor. Anthem Insurance Companies, Inc. (AICI) is the legal entity who has contracted with the
Summary of Benefits for SM, Plus SM and Premier SM Available in Maine and New Hampshire A -approved Part D sponsor. Anthem Insurance Companies, Inc. (AICI) is the legal entity who has contracted with the
Chartpack. August 2008
 Chartpack Examining Sources of Coverage Among Medicare Beneficiaries: Supplemental Insurance, Medicare Advantage, and Prescription Drug Coverage Findings from the Medicare Current Beneficiary Survey, 2006
Chartpack Examining Sources of Coverage Among Medicare Beneficiaries: Supplemental Insurance, Medicare Advantage, and Prescription Drug Coverage Findings from the Medicare Current Beneficiary Survey, 2006
Medicare Part D Prescription Drug Coverage
 Medicare Part D Prescription Drug Coverage Part 3 Version 9.0 June 22, 2015 Terms and Conditions This training program is protected under United States Copyright laws, 17 U.S.C.A. 101, et seq. and international
Medicare Part D Prescription Drug Coverage Part 3 Version 9.0 June 22, 2015 Terms and Conditions This training program is protected under United States Copyright laws, 17 U.S.C.A. 101, et seq. and international