Buprenorphine/Naloxone Training Workshop for Medical Practitioners
|
|
|
- Drusilla Ross
- 8 years ago
- Views:
Transcription
1 Buprenorphine/Naloxone Training Workshop for Medical Practitioners Program developed by Dr Nicholas Lintzeris MBBS, PhD, FAChAM (RACP) Turning Point Alcohol and Drug Centre, Melbourne, Australia Federation of Private Medical Practitioners Associations, Malaysia Ministry of Health Malaysia

2 Workshop Overview Module 1 Working with heroin users» Drugs, dependence and harms» Overview of services» Clinical assessment of drug users Module 2 Treatment with Suboxone (Buprenorphine-naloxone)» Clinical Pharmacology» Therapeutic guidelines Module 3 Addressing co-morbidity» BPN abuse» Polydrug use» Psychiatric comorbidity» Medical comorbidity 2

3 Module 2 Prescribing Buprenorphine / Naloxone Clinical Pharmacology & Therapeutic Guidelines

4 Learning Objectives 1. To understand the rationale, goals, potential benefits and problems associated with Suboxone treatment 2. To understand and communicate the pharmacology of Suboxone treatment 3. To be able to safely initiate and stabilise patients in Suboxone treatment 4. To be familiar with the components of effective maintenance treatment 5. To be familiar with the processes for discontinuing Suboxone treatment 4

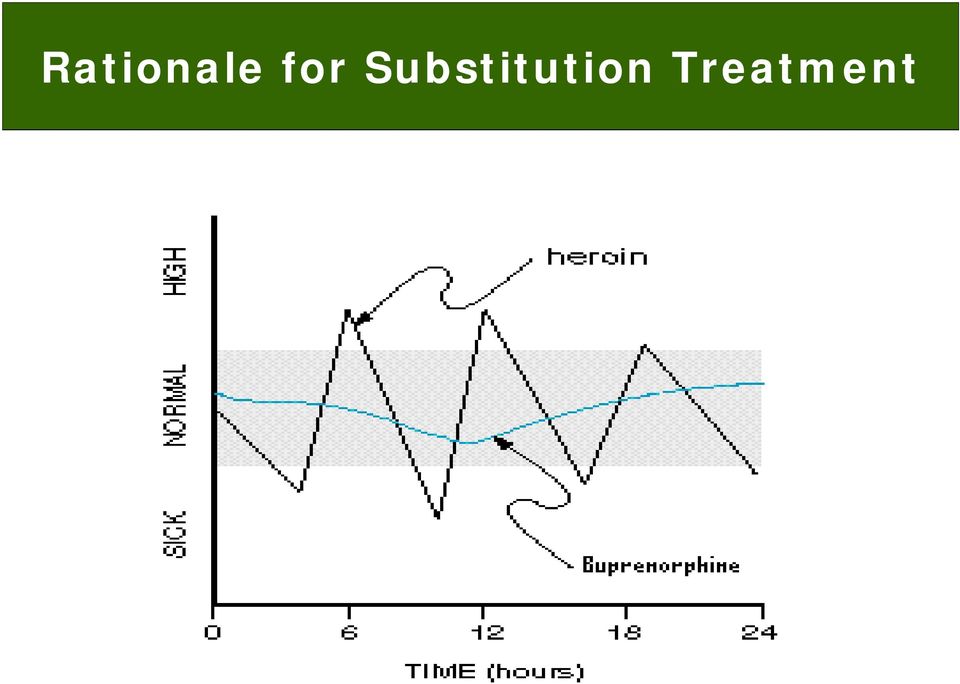
5 Overview of substitution maintenance treatment Provision of a long acting opioid (e.g. methadone, buprenorphine) enables patient to cease / reduce their heroin use and related behaviours Long term treatment approach: provides opportunity for patients to distance themselves from drug-using lifestyle Combines medication with psychosocial services 5
 enables patient to cease / reduce their heroin use and")
6 Rationale for Substitution Treatment 6
7 SUBOXONE Buprenorphine naloxone Clinical Pharmacology

8 Classification of Opioids 100 Full Agonists: Heroin, morphine, methadone, codeine Size of Opiate Agonist Effect 0 Threshold for respiratory depression Drug Dose Partial Agonists: Buprenorphine Antagonists: Naltrexone, naloxone 8

9 Buprenorphine Partial agonist at the μ opiate receptor - Low intrinsic activity only partially activates receptors High affinity for the μ receptor - Binds more tightly to receptors than other opiates 9

10 Buprenorphine: Pharmacological & Clinical Properties Pharmacological property Clinical implication Substitutes for heroin Mild opiate-like effects Blocks other opiates due to high affinity Long duration of action Ceiling effects Prevents withdrawal Reduces cravings & increases treatment retention Reduces heroin use Daily (or alternate day) dosing Greater safety profile 10
 dosing Greater")
11 Buprenorphine: Safety Aspects Less risk of overdose c/w full opiate agonists Less respiratory depression & sedation than methadone BPN tolerated by individuals with low levels of opiate dependence Potential concerns re: safety BPN-related deaths reported in combination with other sedatives (alcohol, BZDs) Some respiratory depression seen in opiate naïve individuals Safety concerns are much less than methadone 11
 Some respiratory depression seen in opiate naïve individuals Safety concerns are much less than")
12 BPN effects in ex-opiate addicts (Walsh et al 1994) 12

13 Respiratory depression in non-opiate users Dose peak ventilatory depression relationships for (A) IV fentanyl and (B) IV buprenorphine in opiate naïve healthy volunteers. Dahan et al British Journal of Anaesthesia

14 Buprenorphine: Clinical Pharmacology Sublingual tablets (30-40% bioavailability) 2 & 8 mg tablets available 3 to 10 minutes to dissolve Time course Onset: min; peak effects: 1 4 hours Duration of action: dose related (4 hrs to 3 days) Side Effects Typical for opioid class Withdrawal syndrome Milder than full agonists 14

15 Buprenorphine: Common Side Effects Side effects occur early & then usually subside Headache Constipation Nausea Drowsiness, sedation Tiredness, lethargy Sleep disturbances Sweating Precipitated withdrawal on commencing buprenorphine 15

16 Understanding Precipitated Withdrawal BPN competes with and displaces full opioid agonists (heroin, methadone) from receptors BPN has lower intrinsic opioid activity than full agonists Reduction in opioid activity experienced as withdrawal Only likely to occur if first dose of BPN is given whilst patient is experiencing effects of other opiates 16

17 Precipitated Withdrawal Profile More common features include: Autonomic withdrawal features, such as sweating, anxiety, GI symptoms (cramps, diarrhoea, nausea) If not aware of risks: confusion, disillusionment Symptoms related to peak effects of BPN Start ~30 60 min after first BPN dose Peak within 1½-2 hrs after first dose, then subside Induction treatment procedures aim to avoid precipitated withdrawal 17

18 Buprenorphine: Drug Interactions Sedatives - In combination with alcohol, BZDs can produce respiratory depression, heavy sedation, coma, death Opioid agonists Will reduce the effects of other opioids used for analgesia Hepatic CYP 450 enzyme inhibitors / inducers Fewer interactions with CYP450 related drugs than methadone (HAART, HCV & TB treatment, anticonvulsants). Usually not clinically relevant with BPN 18
.")
19 Buprenorphine Abuse: Injecting BPN (like all opioids) is subject to abuse by injecting Laboratory data indicates IV BPN greater euphoria, sedation and drug liking than SL Epidemiological data indicates BPN injecting linked to Low levels of supervised consumption Small doses of BPN prescribed Erratic / poor availability of other opioids Local cultural variations 19

20 Concerns with Buprenorphine Injecting IV BPN combined with CNS depressants (e.g. benzodiazepines) may be associated with respiratory depression and death Localised injecting problems (abscesses, thrombosis, etc..) Systemic fungal infections HIV/HCV if shared equipment Cytolytic hepatitis: rare Bad reputation for treatment 20

21 SUBOXONE
22 Why was Suboxone developed? Developed in response to reports of BPN injecting Aim of introducing BPN treatment outside of clinic based system in USA with little capacity for supervised dispensing Designed to decrease BPN s injectable abuse potential 22
23 Suboxone: Combination Medication Buprenorphine : naloxone 4:1 ratio Preparations 2 mg BPN:0.5 mg NLX 8 mg BPN:2 mg NLX 23
24 Naloxone Short acting opioid antagonist: will reverse opioid agonist effects Clinical applications reversing opiate overdoses: 0.8 to 2mg IV/IM naloxone challenge tests: mg IV/IM Duration of effect: ~30-60 minutes (t 1/2 ~70 min) Poor sublingual absorption (<10%) Naloxone has comparable receptor affinity to BPN 24
25 Rationale for Suboxone Combination buprenorphine - naloxone tablet Pharmacology If taken sublingually: naloxone poorly absorbed, so get BPN effects only & no naloxone effect If injected by heroin user, naloxone produces antagonist effect (severe withdrawal) & deterrent to further injecting 25
26 Suboxone Value of a Dose in Dollars Dollars (USD) MS BUP Bup 2:1 4:1 8:1 Minutes MS 4.1 PBO 2:1 Plac 8:1 Subjects stabilized on 60 mg/day i.m. morphine and given IV doses of BPN (2 mg), MS (morphine sulfate, 15 mg); 8:1 (BPN, 2 mg; NLX, 0.25 mg); 4:1 (BPN, 2 mg; NLX, 0.5 mg); 2:1 (BPN, 2 mg; NLX, 1 mg) and Placebo. (Mendelson et al 1996) Left: Observer rating of antagonist effects (CINA Scale) Right: Subjective ratings (willingness to pay) 26
27 Will Suboxone stop all injecting? No. Suboxone patients can still inject Suboxone Naloxone has comparable receptor affinity to BPN If already on BPN, then IV naloxone unlikely to displace BPN and cause severe antagonist effects Variable effects of injecting Suboxone will blunt or reduce the euphoric effects of IV use may cause minor antagonist effects Makes Suboxone injecting less pleasurable & less sought after than Subutex / heroin injecting 27
28 Comparing Subutex and Suboxone effects in different groups SL BPN IV BPN Abuse potential Subutex SL BPN-NLX IV BPN-NLX Abuse potential Suboxone Opiate naive LOW LOW Opiate abuser HIGH MOD Heroin addict / HIGH Methadone patient LOW BPN patient HIGH / V.LOW V.LOW MOD 28
29 Why prescribe Suboxone? Reduces likelihood that medication will be injected Fewer risks of overdose, injecting problems Reduces street value of diverted medication Greater adherence to medication regime Greater confidence in providing take-away doses Better reputation for treatment 29
30 Are there any patients who should not be prescribed Suboxone? Pregnant women (Category C drug) Allergy or sensitivity to naloxone (rare) Patients transferring from high dose methadone Use Subutex for the first 2-3 days, then Suboxone 30
31 Transferring Patients from Subutex to Suboxone Use equivalent doses (e.g. 8mg Subutex = 8/2mg Suboxone) In context where transfer is involuntary proportion of patients report side effects (anxiety, nausea, headache, fatigue), which tend to subside with time In context where transfer voluntary few reports of adverse events & few difficulties Patients complaining of intolerance of Suboxone often expectancy issues may be attempt to continue Subutex injecting should be referred to a specialist clinic for further assessment 31
32 Therapeutic Guidelines Induction procedures, maintenance and withdrawal
33 Eligibility for Suboxone Treatment Opiate dependent + informed consent Precautions for primary care settings: High risk polydrug use Low-level physical dependence <18 y.o.a Severe active psychiatric conditions Medical (severe hepatic / respiratory) disease) Chronic pain 33
34 Goals of Treatment Induction To initiate patient into appropriate treatment To minimise adverse events Opioid side effects Avoid toxicity with methadone Avoid precipitated withdrawal with BPN Stabilise dose and patient so that not in withdrawal/intoxicated To retain patient in treatment 34
35 Principles of Safe Induction I. Comprehensive assessment Establish opioid dependence & tolerance history presence of withdrawal features examination of injecting sites urine drug screen Identify risk factors use of sedative drugs (e.g. alcohol, BZDs, TCAs) medical (severe liver / respiratory disease, current infections) / psychiatric (depression) comorbidity 35 DO NOT RUSH THE ASSESSMENT DO NOT CUT CORNERS
36 Principles of Safe Induction II. Patient Information Inform patient of process of treatment Inform patient of potential side effects Warn against additional drug use Warn against driving, operating machinery Inform patient of the rules (e.g. missed doses, intoxicated presentations, appointments) Informed consent 36
37 Principles of Safe Induction III. Initiate BPN dosing safely & effectively 1. Commence BPN 2. Avoid adverse effects precipitated withdrawal 3. Increase dose quickly to achieve target dose not in withdrawal/intoxicated to retain patient in treatment 37
38 Buprenorphine Partial agonist at the μ opiate receptor - Low intrinsic activity only partially activates receptors High affinity for the μ receptor - Binds more tightly to receptors than other opiates 38
39 Understanding precipitated withdrawal BPN competes with and displaces full opioid agonists (heroin, methadone) from receptors BPN has lower intrinsic opioid activity than full agonists Reduction in opioid activity experienced as withdrawal Only likely to occur if first dose of BPN is given whilst patient is experiencing effects of other opiates 39
40 Precipitated withdrawal profile More common features include: Autonomic withdrawal features, such as sweating, anxiety, GI symptoms (cramps, diarrhoea, nausea) If not aware of risks: confusion, disillusionment Symptoms related to peak effects of BPN Start ~30 60 min after first BPN dose Peak within 1½-2 hrs after first dose, then subside Precipitated withdrawal profile 40
41 Factors impacting precipitated withdrawal Amount of opioid agonist in system: Dose & duration of action of opioid used Heroin use Low methadone doses (e.g. <40mg) Higher methadone doses / Size first BPN dose greater precipitated withdrawal with higher first dose Patient expectancy 41
42 Factors impacting precipitated withdrawal Methadone to BPN (Strain et al, 1992, 1994) 42
43 Principles of Buprenorphine Induction Day 1 BPN dosing 1. Assessment & prepare the patient (information) 2. Avoid precipitated withdrawal Delay first BPN dose until patient in mild-opiate withdrawal* >6 8 hrs after last use of heroin >24 hrs after low methadone dose (<40 mg) >36 48 hrs after medium methadone dose (40 60 mg) First BPN dose = 2 4 mg as test dose Dose with more BPN >2 hrs after first dose Aim for at least 8 mg total dose day 1 If patient in significant opiate withdrawal and no concurrent sedative intoxication, can dose with 8mg start dose 43 * Role of dispensing clinician
44 After day 1 Once concerns re: precipitated withdrawal abated, aim to achieve target dose ASAP Maintenance Rx: 8 16mg by days 2-3 Detox treatment: dose required to minimise withdrawal & stop heroin use (at least 4-8mg in most patients) 44
45 Examples of induction doses (heroin users) Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 A B C
46 Faster Buprenorphine Induction Improves Early Treatment Retention Kakko et al Fudala et al Ortner et al Amadi et al Fischer et al Gerra et al Petitjean et al Pani et al Krook et al % retained at 4 weeks Time (days) to at least 8 mg Subutex 46
47 Transferring from Methadone to Buprenorphine (M to B) Individual variation Why transfer? side effects, rapid metabolisers, drug interactions Common difficulties with methadone Rx reluctance to be on effective methadone doses convenience & safety of take-away BPN doses convenience of primary care setting Patient request curiosity, stigma, expectancy Ease of withdrawal attempt to withdraw from maintenance treatment 47
48 Minimising precipitated withdrawal in M to B Educate the patient Reduce methadone dose as far as possible Below 40mg if possible Transfers can be done from higher doses (40-80mg) Delay time interval between last methadone dose & first BPN dose Wait for patient to be in early-mod withdrawal hrs Initial test dose of 2 4mg BPN & then add more BPN doses >1 2 hrs after test dose Aim for at least 8mg day 1 48
49 Follow-up after Transfers Review patients regularly in first 1 2 weeks on BPN Common for side effects during this time Sleep problems Dysphoria, anxiety Flooded with emotions Most difficulties with BPN settle within this time Some patients will want to transfer back to methadone 49
50 Maintenance & Treatment Cessation
51 Principles of Effective Treatment Dose Duration of treatment Quality of therapeutic relationship Regular review & monitoring Participating in psychosocial services Structured dispensing arrangements Bio-psycho-social model for chronic condition 51
52 Maintenance Dosing What is the correct BPN dose? The correct dose is as much as required to Stop withdrawal symptoms Achieve treatment goals (stop heroin use) Avoid side effects (of too little / too much medication) Most patients need 8-16mg to achieve this e.g. blockade effects at>8mg BPN Continued heroin use is usually an indication for a dose increase. 52
53 Efficacy of Buprenorphine & Methadone for maintenance treatment High dose MMT (> 80 mg) better than Medium dose MMT(40-80mg) = Medium dose BMT (8-12mg) better than Low dose MMT (< 40 mg) = Low dose BMT (< 8 mg) Note: No RCTs of high dose BMT ( 16mg) to high dose MMT 53
54 Alternate Day Dispensing Safety of Suboxone allows for alternate day & 3-day dosing Reduces inconvenience of daily dispensing without takeaway risks Can be initiated once dose stable (> 2 weeks) Alternate (2) day dosing = 2 x daily dose e.g. daily dose 8/2mg = ADD of 16/4mg Three day dosing = 3 x daily dose e.g. daily dose of 8/2mg = 3 day dose of 24/6mg Not all patients stabilise on 2 or 3 day dosing Withdrawal features, increased cravings, poor sleep on non-dispensed days 54
55 Responding to continued drug use Must review: drug use, risk practices, medical, psychiatric, social circumstances patient goals of treatment & drug use frequency of reviews and monitoring (urine tests) medication regimes Suboxone dose take-aways patient adherence (missed doses) other prescribed drugs psychosocial interventions and supports precipitants to continued drug use 55
56 Counseling Approaches Early phase of treatment (first 1-3 months): Focus on ongoing assessment, providing information & developing rapport Motivational & supportive counselling approaches Stabilising drug use & unstable social / medical issues Avoiding drug related harms (overdoses, needle sharing) Once stability achieved: (+2 months) Relapse prevention strategies Address medical, psychiatric, social & relationship issues Long-term patients (>12 months) referral for insight oriented therapy? discussions of withdrawal from maintenance 56
57 When should we stop treatment? Chronic condition needs long term treatment Premature cessation of treatment usually results in relapse to dependent heroin use Consider ending treatment when no illicit drug use for months / years stable social environment stable medical / psychiatric conditions patient has a life that does not revolve around drugs patient informed consent Trial of reduction 57
58 Withdrawal Procedures Withdrawal severity greatest in 1-2 weeks after stopping BPN Strategy is to reduce dose slowly (e.g. 2mg every 2-4 weeks), review often & reassess treatment plans frequently High risk of relapse to heroin / other drug use If patient not coping (severe cravings / withdrawal, drug use), then slow down or cease reduction. Try again at later stage, or under different circumstances Limit other medications until final stages of withdrawal, or else tolerance to their effects Beware BZD use beyond 1-2 weeks 58
59 Managing Heroin Detox with Suboxone
60 Objectives of Detoxification Detox is not a cure for heroin dependence Most heroin users relapse after withdrawal Need long-term treatment to achieve long-term changes Short-term intervention that aims to: Interrupt a pattern of heavy & regular drug use Alleviate withdrawal discomfort Prevent complications of withdrawal Facilitate post-withdrawal treatment linkages
61 Components of Detox Program Supportive care safe environment (inpatient / outpatient) patient information & supportive counselling regular monitoring Medication Buprenorphine is preferred medication Avoid benzodiazepines in outpatient settings Limit access to medications (supervised, daily) Post-withdrawal linkages Counselling, rehab, naltrexone, self-help groups, community supports 61
62 Buprenorphine for Detoxification Short inpatient / outpatient regimes (3-14 days) BPN reduces main heroin withdrawal features minimal rebound withdrawal on stopping BPN Example short regime Day 1: 8mg Day 2: 8mg Day 3: 6mg Day 4: 4mg Day 5: 2mg Gradual outpatient regimes (1 6months) allows more time for stability to be achieved greater withdrawal rebound on stopping BPN no / minimal other medication required Example Stabilise on 8mg / day. After 1 month reduce by 2mg every 2-4 weeks 62
63 Case Studies
64 Exercise: Induction Dose 1. New patient, states injecting 2 times / day for past 3/12; 5 yrs regular heroin use; occasional binge BZD 10 tabs at a time. HCV+(ve). States last used 3 hrs ago. O/E ++ injection marks; no intoxication or withdrawal. No significant medical conditions. 2. Patient with past Subutex treatment. Reports using heroin 4 to 5 times / day until went into inpatient detox, where lasted 6 days before leaving yesterday. States used heroin only once since leaving detox. Pupils 2 mm, quiet demeanor. 3. Patient discharged from government clinic for ongoing benzo & heroin use. Was on methadone 40mg/day, last methadone dose 2 days ago (confirmed with clinic). Presents anxious, sweaty, piloerection, pupils 5mm and wants treatment. How would you induct each patient onto Suboxone (include doses)? 64
65 Case Study: Sue Sue, a 27-year old presents to your practice for the first time. She states that she has been using heroin for the past 4 years - in recent months has been using 2 to 3 times a day, and recently started injecting (to get more effects). Her boyfriend also injects heroin. She wants treatment to stop using heroin. What further assessment do you do? 65
66 Case Study: Sue (2) Full drug history: Syabu (smoked) once every 2 weeks. Last used 5 days ago Diazepam 5-20mg once a week when heroin not available or after syabu use. Last used 2 days ago. Irregular alcohol /cannabis use reported No prior addiction treatment Nil significant medical / psychiatric history. Uncertain HIV/HBV/HCV. Irregular menstrual periods LMP?10/52 ago Lived with boyfriend (heroin user), who was recently arrested & in prison. Not working, occasional sex-work. O/E: anxious, sweaty, pupils 4mm, new & old injection marks Urine screen: opiate, BZD, amphetamines, cannabis positive She requests outpatient treatment. How do you respond & commence treatment? 66
67 Case Study: Sue (3) Discuss Suboxone treatment & get informed consent. You suggest 4/1mg Suboxone as starting dose AND for her to present later in day for?additional dose She does not return that day, but attends next day stating that was OK until 2 am then experienced stomach cramps, sweats, bone aches. She states that she is worried that Suboxone not working. Could she also have some diazepam to help her sleep tonight? How do you respond? What other issues do you want to address with Sue? 67
68 Case Study: Sue (4) Increase Suboxone dose to 8/2mg Avoid diazepam and educate that best way to respond to opiate withdrawal is with adequate Suboxone dose. Continue with daily supervised dispensing Review regularly & regular UDS Need to address Contraception / Pregnancy test HIV/HCV/HBV testing Safe sex & injecting practices if continues these 68
69 Case Study: Steven A 29 yr old with 10 yr history heroin dependence in treatment on BPN last 18/12. Initially was injecting heroin 1-2 times / week whilst on 4mg BPN. After 6/12 in treatment, increased dose to 8mg & subsequent cessation heroin use. Clean UDS for next 9 months & started work again with his parent s business. Reduced BPN dispensing from daily to two times / week (5 TA s / week). He presents 2 days late for his medical review. You see that he has missed his last 2 appointments with his worker, and no UDS in past 2/12. He is looking well but says he cannot stay long as he has to get back to work. Everything is fine can you sign my prescription as I need my dose What do you do? 69
70 Case Study: Steven (2) On enquiry, he denies any illicit drug use & states that he just went to the toilet before coming to the clinic so he cannot give a UDS. On examination you notice 3-4 recent injection marks. He then admits to having used IV heroin 3 to 5 days ago (a friend dropped by), and he did not take his BPN for 3 days. Took 8mg BPN yesterday & now has run out. Adamant that he will not be using heroin again. How do you respond? 70
71 Case Study: Steven (3) Concerns that recent lapse may become more prolonged relapse Schedule regular reviews & UDS Counselling to address relapse prevention Review take-away doses. Either Provide clean UDS to avoid losing take-aways; or stop take-aways & get them back when clean UDS 71
72 Self Assessment of Learning
73 1. Which of the following statement(s) is/are TRUE? A. The general principle of Suboxone treatment is to withdraw Suboxone after the patient has achieved a 1 to 2 month period without heroin use. B. Suboxone treatment is generally most effective when patients remain in treatment for several years. treatment is generally most effective in reducing e with doses in the range of 2 to 4mg per day. ion in Suboxone treatment should only be allowed if the nt participates in regular counselling. l, patients who continue to use heroin during the Suboxone program should have their dose reduced. 73
74 2. How do you commence treatment? Alex is a 32 year old presenting for Suboxone treatment. In recent weeks he describes injecting either heroin three times a day, or 3 x 30 mg morphine ampoules (obtained from his sick aunt). He has no major medical problems, and says he last used heroin 4 hours ago. He has a runny nose, dilated pupils and is sweating profusely during the interview. A. Delay Suboxone for a further 2 hours (at least 6 hours since last use) B. Start with 2mg, and review tomorrow. C. Start with 4mg and a further 4 mg after 2 hours D. Start with 8mg and review tomorrow E. Start with 8mg and a further 8mg after 2 hours. 74
75 3. Which of the following strategies are appropriate courses of management? James, a 27 year old commenced Suboxone three days ago an a dose of 4/1 mg. He now presents complaining of poor sleep, mild nausea and withdrawal discomfort each morning before his next dose. He reports using heroin once since starting treatment. A. Prescribe metoclopramide 10 mg tds prn for nausea B. Prescribe mg diazepam to help with sleep and withdrawal discomfort C. Increase the Suboxone dose to 8/2mg D. Increase the Suboxone dose to 16/4mg E. Reassure the patient that these are common side effects that usually subside within a few days 75
76 1. Which of the following statement(s) is/are TRUE? A. The general principle of Suboxone treatment is to withdraw Suboxone after the patient has achieved a 1 to 2 month period without heroin use. B. Suboxone treatment is generally most effective when patients remain in treatment for several years. C. Suboxone treatment is generally most effective in reducing heroin use with doses in the range of 2 to 4mg per day. D. Continuation in Suboxone treatment should only be allowed if the patient participates in regular counselling. E. In general, patients who continue to use heroin during the Suboxone program should have their dose reduced. 76
77 2. How do you commence treatment? Alex is a 32 year old presenting for Suboxone treatment. In recent weeks he describes injecting either heroin three times a day, or 3 x 30 mg morphine ampoules (obtained from his sick aunt). He has no major medical problems, and says he last used heroin 4 hours ago. He has a runny nose, dilated pupils and is sweating profusely during the interview. A. Delay Suboxone for a further 2 hours (at least 6 hours since last use) B. Start with 2mg, and review tomorrow. C. Start with 4mg and a further 4 mg after 2 hours D.Start with 8mg and review tomorrow E. Start with 8mg and a further 8mg after 2 hours. 77
78 3. Which of the following strategies are appropriate courses of management? James, a 27 year old commenced Suboxone three days ago an a dose of 4/1 mg. He now presents complaining of poor sleep, mild nausea and withdrawal discomfort each morning before his next dose. He reports using heroin once since starting treatment. A. Prescribe metoclopramide 10 mg tds prn for nausea B. Prescribe mg diazepam to help with sleep and withdrawal discomfort C. Increase the Suboxone dose to 8/2mg D. Increase the Suboxone dose to 16/4mg E. Reassure the patient that these are common side effects that usually subside within a few days 78
Buprenorphine: what is it & why use it?
 Buprenorphine: what is it & why use it? Dr Nicholas Lintzeris, MBBS, PhD, FAChAM Locum Consultant, Oaks Resource Centre, SLAM National Addiction Centre, Institute of Psychiatry Overview of presentation
Buprenorphine: what is it & why use it? Dr Nicholas Lintzeris, MBBS, PhD, FAChAM Locum Consultant, Oaks Resource Centre, SLAM National Addiction Centre, Institute of Psychiatry Overview of presentation
Buprenorphine/Naloxone Training Workshop for Medical Practitioners
 Buprenorphine/Naloxone Training Workshop for Medical Practitioners Program developed by Dr Nicholas Lintzeris MBBS, PhD, FAChAM (RACP) Turning Point Alcohol and Drug Centre, Melbourne, Australia Federation
Buprenorphine/Naloxone Training Workshop for Medical Practitioners Program developed by Dr Nicholas Lintzeris MBBS, PhD, FAChAM (RACP) Turning Point Alcohol and Drug Centre, Melbourne, Australia Federation
Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone )
") Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone ) Elinore F. McCance-Katz, M.D., Ph.D. Professor and Chair, Addiction Psychiatry Virginia Commonwealth University Neurobiology of Opiate
Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone ) Elinore F. McCance-Katz, M.D., Ph.D. Professor and Chair, Addiction Psychiatry Virginia Commonwealth University Neurobiology of Opiate
Substitution Therapy for Opioid Dependence The Role of Suboxone. Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015
 Substitution Therapy for Opioid Dependence The Role of Suboxone Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015 Objectives Recognize the options available in treating opioid
Substitution Therapy for Opioid Dependence The Role of Suboxone Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015 Objectives Recognize the options available in treating opioid
COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE
 COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE INTRODUCTION High dose sublingual buprenorphine (Subutex) tablets are available in the following strengths 0.4 mg, 2 mg, and 8 mg. Suboxone tablets,
COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE INTRODUCTION High dose sublingual buprenorphine (Subutex) tablets are available in the following strengths 0.4 mg, 2 mg, and 8 mg. Suboxone tablets,
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2011 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2011 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION
 MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Adminstrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids and
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Adminstrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids and
Integrating Medication- Assisted Treatment (MAT) for Opioid Use Disorders into Behavioral and Physical Healthcare Settings
 for Opioid Use Disorders into Behavioral and Physical Healthcare Settings") Integrating Medication- Assisted Treatment (MAT) for Opioid Use Disorders into Behavioral and Physical Healthcare Settings All-Ohio Conference 3/27/2015 Christina M. Delos Reyes, MD Medical Consultant,
Integrating Medication- Assisted Treatment (MAT) for Opioid Use Disorders into Behavioral and Physical Healthcare Settings All-Ohio Conference 3/27/2015 Christina M. Delos Reyes, MD Medical Consultant,
One example: Chapman and Huygens, 1988, British Journal of Addiction
 This is a fact in the treatment of alcohol and drug abuse: Patients who do well in treatment do well in any treatment and patients who do badly in treatment do badly in any treatment. One example: Chapman
This is a fact in the treatment of alcohol and drug abuse: Patients who do well in treatment do well in any treatment and patients who do badly in treatment do badly in any treatment. One example: Chapman
Update on Buprenorphine: Induction and Ongoing Care
 Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
Treatment of opioid use disorders
 Treatment of opioid use disorders Gerardo Gonzalez, MD Associate Professor of Psychiatry Director, Division of Addiction Psychiatry Disclosures I have no financial conflicts to disclose I will review evidence
Treatment of opioid use disorders Gerardo Gonzalez, MD Associate Professor of Psychiatry Director, Division of Addiction Psychiatry Disclosures I have no financial conflicts to disclose I will review evidence
Information for Pharmacists
 Page 43 by 42 CFR part 2. A general authorization for the release of medical or other information is NOT sufficient for this purpose. Information for Pharmacists SUBOXONE (buprenorphine HCl/naloxone HCl
Page 43 by 42 CFR part 2. A general authorization for the release of medical or other information is NOT sufficient for this purpose. Information for Pharmacists SUBOXONE (buprenorphine HCl/naloxone HCl
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery
 Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
Considerations in Medication Assisted Treatment of Opiate Dependence. Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT
 Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
Opioids Research to Practice
 Opioids Research to Practice CRIT/FIT 2015 May 2015 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research
Opioids Research to Practice CRIT/FIT 2015 May 2015 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research
EPIDEMIOLOGY OF OPIATE USE
 Opiate Dependence EPIDEMIOLOGY OF OPIATE USE Difficult to estimate true extent of opiate dependence Based on National Survey of Health and Mental Well Being: 1.2% sample used opiates in last 12 months
Opiate Dependence EPIDEMIOLOGY OF OPIATE USE Difficult to estimate true extent of opiate dependence Based on National Survey of Health and Mental Well Being: 1.2% sample used opiates in last 12 months
Joanna L. Starrels. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume VIII, 2003-2004. A. Study Purpose and Rationale
 Outpatient Treatment of Opiate Dependence with Sublingual Buprenorphine/Naloxone versus Methadone Maintenance: a Randomized Trial of Alternative Treatments in Real Life Settings Joanna L. Starrels A. Study
Outpatient Treatment of Opiate Dependence with Sublingual Buprenorphine/Naloxone versus Methadone Maintenance: a Randomized Trial of Alternative Treatments in Real Life Settings Joanna L. Starrels A. Study
Medications for Alcohol and Drug Dependence Treatment
 Medications for Alcohol and Drug Dependence Treatment Robert P. Schwartz, M.D. Medical Director Rschwartz@friendsresearch.org Friends Research Institute Medications for Alcohol Dependence Treatment Disulfiram
Medications for Alcohol and Drug Dependence Treatment Robert P. Schwartz, M.D. Medical Director Rschwartz@friendsresearch.org Friends Research Institute Medications for Alcohol Dependence Treatment Disulfiram
A G U I D E F O R U S E R S N a l t r e x o n e U
 A GUIDE FOR USERS UNaltrexone abstinence not using a particular drug; being drug-free. opioid antagonist a drug which blocks the effects of opioid drugs. dependence the drug has become central to a person
A GUIDE FOR USERS UNaltrexone abstinence not using a particular drug; being drug-free. opioid antagonist a drug which blocks the effects of opioid drugs. dependence the drug has become central to a person
methadonefact.qxd 8/11/01 2:05 PM Page 1 INFORMATION Advantages of methadone treatment DEPRESSANT Methadone maintenance Pregnancy METHADONE
 methadonefact.qxd 8/11/01 2:05 PM Page 1 INFORMATION Advantages of methadone treatment 10 DEPRESSANT Methadone maintenance Pregnancy METHADONE methadonefact.qxd 8/11/01 2:05 PM Page 2 WHAT IS METHADONE
methadonefact.qxd 8/11/01 2:05 PM Page 1 INFORMATION Advantages of methadone treatment 10 DEPRESSANT Methadone maintenance Pregnancy METHADONE methadonefact.qxd 8/11/01 2:05 PM Page 2 WHAT IS METHADONE
Opioid dependence is a chronic relapsing condition that
 PEER REVIEWED FEATURE Treatment of patients with opioid dependence NICHOLAS LINTZERIS BMedSci, MB BS, PhD, FAChAM The prevalence of opioid dependence is growing in Australia with the increased use of pharmaceutical
PEER REVIEWED FEATURE Treatment of patients with opioid dependence NICHOLAS LINTZERIS BMedSci, MB BS, PhD, FAChAM The prevalence of opioid dependence is growing in Australia with the increased use of pharmaceutical
Like cocaine, heroin is a drug that is illegal in some areas of the world. Heroin is highly addictive.
 Heroin Introduction Heroin is a powerful drug that affects the brain. People who use it can form a strong addiction. Addiction is when a drug user can t stop taking a drug, even when he or she wants to.
Heroin Introduction Heroin is a powerful drug that affects the brain. People who use it can form a strong addiction. Addiction is when a drug user can t stop taking a drug, even when he or she wants to.
Prior Authorization Guideline
 Prior Authorization Guideline Guideline: CSD - Suboxone Therapeutic Class: Central Nervous System Agents Therapeutic Sub-Class: Analgesics and Antipyretics (Opiate Partial Agonists) Client: County of San
Prior Authorization Guideline Guideline: CSD - Suboxone Therapeutic Class: Central Nervous System Agents Therapeutic Sub-Class: Analgesics and Antipyretics (Opiate Partial Agonists) Client: County of San
SUBOXONE for Opioid Addiction Medication Assisted Therapy. Dr. Jennifer Melamed MBChB, ABAM, CISAM, CCSAM
 N SUBOXONE for Opioid Addiction Medication Assisted Therapy Dr. Jennifer Melamed MBChB, ABAM, CISAM, CCSAM CONTENTS Part 1 Introduction to N SUBOXONE Part 2 Pharmacology of N SUBOXONE Part 3 Pharmacokinetics
N SUBOXONE for Opioid Addiction Medication Assisted Therapy Dr. Jennifer Melamed MBChB, ABAM, CISAM, CCSAM CONTENTS Part 1 Introduction to N SUBOXONE Part 2 Pharmacology of N SUBOXONE Part 3 Pharmacokinetics
Care Management Council submission date: August 2013. Contact Information
 Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
Use of Buprenorphine in the Treatment of Opioid Addiction
 Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary Which of the following is an
Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary Which of the following is an
How To Treat Anorexic Addiction With Medication Assisted Treatment
 Medication Assisted Treatment for Opioid Addiction Tanya Hiser, MS, LPC Premier Care of Wisconsin, LLC October 21, 2015 How Did We Get Here? Civil War veterans and women 19th Century physicians cautious
Medication Assisted Treatment for Opioid Addiction Tanya Hiser, MS, LPC Premier Care of Wisconsin, LLC October 21, 2015 How Did We Get Here? Civil War veterans and women 19th Century physicians cautious
Guidelines for the Prescribing, Supply and Administration of Methadone and Buprenorphine on Transfer of Care
 Hull & East Riding Prescribing Committee Guidelines for the Prescribing, Supply and Administration of Methadone and Buprenorphine on Transfer of Care 1. BACKGROUND Patients who are physically dependent
Hull & East Riding Prescribing Committee Guidelines for the Prescribing, Supply and Administration of Methadone and Buprenorphine on Transfer of Care 1. BACKGROUND Patients who are physically dependent
Non medical use of prescription medicines existing WHO advice
 Non medical use of prescription medicines existing WHO advice Nicolas Clark Management of Substance Abuse Team WHO, Geneva Vienna, June 2010 clarkn@who.int Medical and Pharmaceutical role Recommendations
Non medical use of prescription medicines existing WHO advice Nicolas Clark Management of Substance Abuse Team WHO, Geneva Vienna, June 2010 clarkn@who.int Medical and Pharmaceutical role Recommendations
OVERVIEW WHAT IS POLyDRUG USE? Different examples of polydrug use
 Petrol, paint and other Polydrug inhalants use 237 11 Polydrug use Overview What is polydrug use? Reasons for polydrug use What are the harms of polydrug use? How to assess a person who uses several drugs
Petrol, paint and other Polydrug inhalants use 237 11 Polydrug use Overview What is polydrug use? Reasons for polydrug use What are the harms of polydrug use? How to assess a person who uses several drugs
Heroin. How Is Heroin Abused? How Does Heroin Affect the Brain? What Other Adverse Effects Does Heroin Have on Health?
 Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Buprenorphine/Naloxone Training Workshop for Medical Practitioners
 Buprenorphine/Naloxone Training Workshop for Medical Practitioners Program developed by Dr Nicholas Lintzeris MBBS, PhD, FAChAM (RACP) Turning Point Alcohol and Drug Centre, Melbourne, Australia Federation
Buprenorphine/Naloxone Training Workshop for Medical Practitioners Program developed by Dr Nicholas Lintzeris MBBS, PhD, FAChAM (RACP) Turning Point Alcohol and Drug Centre, Melbourne, Australia Federation
Opioid Agonist Therapy: The Duration Dilemma Edwin A. Salsitz, MD, FASAM Mount Sinai Beth Israel, New York, NY March 10, 2015
 Q: I have read 40 mg of methadone stops withdrawal, so why don t we start at 30mg and maybe later in the day add 10mg? A: Federal Regulations stipulate that 30mg is the maximum first dose in an Opioid
Q: I have read 40 mg of methadone stops withdrawal, so why don t we start at 30mg and maybe later in the day add 10mg? A: Federal Regulations stipulate that 30mg is the maximum first dose in an Opioid
The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office
 The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office Adopted April 2013 for Consideration by State Medical Boards 2002 FSMB Model Guidelines
The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office Adopted April 2013 for Consideration by State Medical Boards 2002 FSMB Model Guidelines
Use of Vivitrol for Alcohol and Opioid Addiction
 Use of Vivitrol for Alcohol and Opioid Addiction Ken Bachrach, Ph.D. Clinical Director, Tarzana Treatment Centers, Inc. kbachrach@tarzanatc.org What is Vivitrol? An injectable from of naltrexone, which
Use of Vivitrol for Alcohol and Opioid Addiction Ken Bachrach, Ph.D. Clinical Director, Tarzana Treatment Centers, Inc. kbachrach@tarzanatc.org What is Vivitrol? An injectable from of naltrexone, which
Using Buprenorphine to Treat Acute Opioid Withdrawal in the ED
 Using Buprenorphine to Treat Acute Opioid Withdrawal in the ED Dr. Karine Meador MD CCFP DABAM Assistant Director Inner City Health and Wellness Team Physician Addiction Recovery and Community Health (ARCH)
Using Buprenorphine to Treat Acute Opioid Withdrawal in the ED Dr. Karine Meador MD CCFP DABAM Assistant Director Inner City Health and Wellness Team Physician Addiction Recovery and Community Health (ARCH)
This module reviews the following: Opioid addiction and the brain Descriptions and definitions of opioid agonists,
 BUPRENORPHINE TREATMENT: A Training For Multidisciplinary Addiction Professionals Module II Opioids 101 Goals for Module II This module reviews the following: Opioid addiction and the brain Descriptions
BUPRENORPHINE TREATMENT: A Training For Multidisciplinary Addiction Professionals Module II Opioids 101 Goals for Module II This module reviews the following: Opioid addiction and the brain Descriptions
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction. Frequently Asked Questions
 Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently Asked Questions What is Naltrexone? Naltrexone is a prescription drug that effectively blocks the effects of heroin, alcohol,
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently Asked Questions What is Naltrexone? Naltrexone is a prescription drug that effectively blocks the effects of heroin, alcohol,
Heroin. How Is Heroin Abused? How Does Heroin Affect the Brain? What Other Adverse Effects Does Heroin Have on Health?
 Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
A prisoners guide to buprenorphine
 A prisoners guide to buprenorphine 2 The Opium poppy In the land of far, far away the opium poppy grows. The seed pods of this poppy are scratched until they drip with a sticky resin called opium. Raw
A prisoners guide to buprenorphine 2 The Opium poppy In the land of far, far away the opium poppy grows. The seed pods of this poppy are scratched until they drip with a sticky resin called opium. Raw
DRUG AND ALCOHOL DETOXIFICATION: A GUIDE TO OUR SERVICES
 01736 850006 www.bosencefarm.co.uk DRUG AND ALCOHOL DETOXIFICATION: A GUIDE TO OUR SERVICES An environment for change Boswyns provides medically-led drug and alcohol assessment, detoxification and stabilisation.
01736 850006 www.bosencefarm.co.uk DRUG AND ALCOHOL DETOXIFICATION: A GUIDE TO OUR SERVICES An environment for change Boswyns provides medically-led drug and alcohol assessment, detoxification and stabilisation.
Dosing Guide. For Optimal Management of Opioid Dependence
 Dosing Guide For Optimal Management of Opioid Dependence KEY POINTS The goal of induction is to safely suppress opioid withdrawal as rapidly as possible with adequate doses of Suboxone (buprenorphine HCl/naloxone
Dosing Guide For Optimal Management of Opioid Dependence KEY POINTS The goal of induction is to safely suppress opioid withdrawal as rapidly as possible with adequate doses of Suboxone (buprenorphine HCl/naloxone
Opioid Treatment Services, Office-Based Opioid Treatment
 Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
Prescription Drug Addiction
 Prescription Drug Addiction Dr Gilbert Whitton FAChAM Clinical Director Drug & Alcohol Loddon Mallee Murray Medicare Local Deniliquin 14 th May 2014 Prescription Drug Addiction Overview History Benzodiazepines
Prescription Drug Addiction Dr Gilbert Whitton FAChAM Clinical Director Drug & Alcohol Loddon Mallee Murray Medicare Local Deniliquin 14 th May 2014 Prescription Drug Addiction Overview History Benzodiazepines
Guidelines for Titration onto Buprenorphine in Opioid Dependence
 NHS Fife Community Health Partnership Addiction Services Guidelines for Titration onto Buprenorphine in Opioid Dependence Intranet Procedure No. A7 Author Dr L. Cockayne Copy No 1 Reviewer Lead Clinician
NHS Fife Community Health Partnership Addiction Services Guidelines for Titration onto Buprenorphine in Opioid Dependence Intranet Procedure No. A7 Author Dr L. Cockayne Copy No 1 Reviewer Lead Clinician
Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal
 Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal Roger Cicala, M. D. Assistant Medical Director Tennessee Physician s Wellness Program Step 1 Don t 1 It is legal in
Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal Roger Cicala, M. D. Assistant Medical Director Tennessee Physician s Wellness Program Step 1 Don t 1 It is legal in
Frequently Asked Questions (FAQ s): Medication-Assisted Treatment for Opiate Addiction
: Medication-Assisted Treatment for Opiate Addiction") Frequently Asked Questions (FAQ s): Medication-Assisted Treatment for Opiate Addiction March 3, 2008 By: David Rinaldo, Ph.D., Managing Partner, The Avisa Group In this FAQ What medications are currently
Frequently Asked Questions (FAQ s): Medication-Assisted Treatment for Opiate Addiction March 3, 2008 By: David Rinaldo, Ph.D., Managing Partner, The Avisa Group In this FAQ What medications are currently
SCOTTISH PRISON SERVICE DRUG MISUSE AND DEPENDENCE OPERATIONAL GUIDANCE
 SCOTTISH PRISON SERVICE DRUG MISUSE AND DEPENDENCE OPERATIONAL GUIDANCE 1 P a g e The following Operational Guidance Manual has been prepared with input from both community and prison addictions specialists
SCOTTISH PRISON SERVICE DRUG MISUSE AND DEPENDENCE OPERATIONAL GUIDANCE 1 P a g e The following Operational Guidance Manual has been prepared with input from both community and prison addictions specialists
Neurobiology and Treatment of Opioid Dependence. Nebraska MAT Training September 29, 2011
 Neurobiology and Treatment of Opioid Dependence Nebraska MAT Training September 29, 2011 Top 5 primary illegal drugs for persons age 18 29 entering treatment, % 30 25 20 15 10 Heroin or Prescription Opioids
Neurobiology and Treatment of Opioid Dependence Nebraska MAT Training September 29, 2011 Top 5 primary illegal drugs for persons age 18 29 entering treatment, % 30 25 20 15 10 Heroin or Prescription Opioids
Hulpverleningsmodellen bij opiaatverslaving. Frieda Matthys 6 juni 2013
 Hulpverleningsmodellen bij opiaatverslaving Frieda Matthys 6 juni 2013 Prevalence The average prevalence of problem opioid use among adults (15 64) is estimated at 0.41%, the equivalent of 1.4 million
Hulpverleningsmodellen bij opiaatverslaving Frieda Matthys 6 juni 2013 Prevalence The average prevalence of problem opioid use among adults (15 64) is estimated at 0.41%, the equivalent of 1.4 million
Opiate Abuse and Mental Illness
 visited on Page 1 of 5 LEARN MORE (HTTP://WWW.NAMI.ORG/LEARN-MORE) FIND SUPPORT (HTTP://WWW.NAMI.ORG/FIND-SUPPORT) GET INVOLVED (HTTP://WWW.NAMI.ORG/GET-INVOLVED) DONATE (HTTPS://NAMI360.NAMI.ORG/EWEB/DYNAMICPAGE.ASPX?
visited on Page 1 of 5 LEARN MORE (HTTP://WWW.NAMI.ORG/LEARN-MORE) FIND SUPPORT (HTTP://WWW.NAMI.ORG/FIND-SUPPORT) GET INVOLVED (HTTP://WWW.NAMI.ORG/GET-INVOLVED) DONATE (HTTPS://NAMI360.NAMI.ORG/EWEB/DYNAMICPAGE.ASPX?
Methadone treatment Information for service users Page
 South London and Maudsley NHS Foundation Trust Methadone treatment Information for service users Page What can happen if I stop using heroin? If you are addicted to or dependent on heroin, you develop
South London and Maudsley NHS Foundation Trust Methadone treatment Information for service users Page What can happen if I stop using heroin? If you are addicted to or dependent on heroin, you develop
OVERVIEW OF MEDICATION ASSISTED TREATMENT
 Sarah Akerman MD Assistant Professor of Psychiatry Director of Addiction Services Geisel School of Medicine/Dartmouth-Hitchcock Medical Center OVERVIEW OF MEDICATION ASSISTED TREATMENT Conflicts of Interest
Sarah Akerman MD Assistant Professor of Psychiatry Director of Addiction Services Geisel School of Medicine/Dartmouth-Hitchcock Medical Center OVERVIEW OF MEDICATION ASSISTED TREATMENT Conflicts of Interest
Heroin. How is Heroin Abused? What Other Adverse Effects Does Heroin Have on Health? How Does Heroin Affect the Brain?
 Heroin Heroin is a synthetic opiate drug that is highly addictive. It is made from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears
Heroin Heroin is a synthetic opiate drug that is highly addictive. It is made from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears
Financial Disclosures
 Opioid Agonist Therapy: To Maintain or Not To Maintain - A Case Discussion PCSS-MAT American Psychiatric Association Drs. Ed Salsitz, John Renner, Timothy Fong April 14, 2015 Financial Disclosures Edwin
Opioid Agonist Therapy: To Maintain or Not To Maintain - A Case Discussion PCSS-MAT American Psychiatric Association Drs. Ed Salsitz, John Renner, Timothy Fong April 14, 2015 Financial Disclosures Edwin
Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence
 Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence Information for Family Members Family members of patients who have been prescribed buprenorphine/naloxone for treatment of opioid addiction
Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence Information for Family Members Family members of patients who have been prescribed buprenorphine/naloxone for treatment of opioid addiction
Program Assistance Letter
 Program Assistance Letter DOCUMENT NUMBER: 2004-01 DATE: December 5, 2003 DOCUMENT TITLE: Use of Buprenorphine in Health Center Substance Abuse Treatment Programs TO: All Bureau of Primary Health Care
Program Assistance Letter DOCUMENT NUMBER: 2004-01 DATE: December 5, 2003 DOCUMENT TITLE: Use of Buprenorphine in Health Center Substance Abuse Treatment Programs TO: All Bureau of Primary Health Care
Oxford Health NHS Foundation Trust. A guide to Opioid Detoxification
 Oxford Health NHS Foundation Trust A guide to Opioid Detoxification If you re considering detox, congratulations. You have obviously been visualising a drug free life and planning your future goals. Detox
Oxford Health NHS Foundation Trust A guide to Opioid Detoxification If you re considering detox, congratulations. You have obviously been visualising a drug free life and planning your future goals. Detox
Frequently asked questions
 Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently asked questions What is Naltrexone? Naltrexone is a prescription drug that completely blocks the effects of all opioid drugs
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently asked questions What is Naltrexone? Naltrexone is a prescription drug that completely blocks the effects of all opioid drugs
Adjunctive psychosocial intervention. Conditions requiring dose reduction. Immediate, peak plasma concentration is reached within 1 hour.
 Shared Care Guideline for Prescription and monitoring of Naltrexone Hydrochloride in alcohol dependence Author(s)/Originator(s): (please state author name and department) Dr Daly - Consultant Psychiatrist,
Shared Care Guideline for Prescription and monitoring of Naltrexone Hydrochloride in alcohol dependence Author(s)/Originator(s): (please state author name and department) Dr Daly - Consultant Psychiatrist,
Opioid Dependence Treatment with Buprenorphine/Naloxone: An Overview for Pharmacists and Physicians
 Opioid Dependence Treatment with Buprenorphine/Naloxone: An Overview for Pharmacists and Physicians Phyllis A. Grauer, PharmD, CGP, CPE Clinical Pharmacist Legislation Passed Enabling Office Based Treatment
Opioid Dependence Treatment with Buprenorphine/Naloxone: An Overview for Pharmacists and Physicians Phyllis A. Grauer, PharmD, CGP, CPE Clinical Pharmacist Legislation Passed Enabling Office Based Treatment
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery
 New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
Using Buprenorphine in an Opioid Treatment Program
 Using Buprenorphine in an Opioid Treatment Program Thomas E. Freese, PhD Director of Training, UCLA Integrated Substance Abuse Programs Director, Pacific Southwest Addiction Technology Transfer Center
Using Buprenorphine in an Opioid Treatment Program Thomas E. Freese, PhD Director of Training, UCLA Integrated Substance Abuse Programs Director, Pacific Southwest Addiction Technology Transfer Center
OPIOIDS. Petros Levounis, MD, MA Chair Department of Psychiatry Rutgers New Jersey Medical School
 OPIOIDS Petros Levounis, MD, MA Chair Department of Psychiatry Rutgers New Jersey Medical School Rutgers New Jersey Medical School Fundamentals of Addiction Medicine Summer Series Newark, NJ July 24, 2013
OPIOIDS Petros Levounis, MD, MA Chair Department of Psychiatry Rutgers New Jersey Medical School Rutgers New Jersey Medical School Fundamentals of Addiction Medicine Summer Series Newark, NJ July 24, 2013
IN THE GENERAL ASSEMBLY STATE OF. Ensuring Access to Medication Assisted Treatment Act
 IN THE GENERAL ASSEMBLY STATE OF Ensuring Access to Medication Assisted Treatment Act 1 Be it enacted by the People of the State of Assembly:, represented in the General 1 1 1 1 Section 1. Title. This
IN THE GENERAL ASSEMBLY STATE OF Ensuring Access to Medication Assisted Treatment Act 1 Be it enacted by the People of the State of Assembly:, represented in the General 1 1 1 1 Section 1. Title. This
NORTHERN IRELAND GUIDELINES ON SUBSTITUTION TREATMENT FOR OPIATE DEPENDENCE
 NORTHERN IRELAND GUIDELINES ON SUBSTITUTION TREATMENT FOR OPIATE DEPENDENCE Department of Health, Social Services & Public Safety February 2004 NORTHERN IRELAND GUIDELINES ON SUBSTITUTION TREATMENT FOR
NORTHERN IRELAND GUIDELINES ON SUBSTITUTION TREATMENT FOR OPIATE DEPENDENCE Department of Health, Social Services & Public Safety February 2004 NORTHERN IRELAND GUIDELINES ON SUBSTITUTION TREATMENT FOR
The ABCs of Medication Assisted Treatment
 The ABCs of Medication Assisted Treatment J E F F R E Y Q U A M M E, E X E C U T I V E D I R E C T O R C O N N E C T I C U T C E R T I F I C A T I O N B O A R D The ABCs of Medication Assisted Treatment
The ABCs of Medication Assisted Treatment J E F F R E Y Q U A M M E, E X E C U T I V E D I R E C T O R C O N N E C T I C U T C E R T I F I C A T I O N B O A R D The ABCs of Medication Assisted Treatment
Discontinuation: Involuntary Discharge
 Discontinuation: Involuntary Discharge TYPICALLY A PROCESS NOT AN EVENT Objectives 2 Review indications for discharge. Develop a therapeutic approach, in the context of the nature of Substance Use Disorders.
Discontinuation: Involuntary Discharge TYPICALLY A PROCESS NOT AN EVENT Objectives 2 Review indications for discharge. Develop a therapeutic approach, in the context of the nature of Substance Use Disorders.
Opioid Addiction and Methadone: Myths and Misconceptions. Nicole Nakatsu WRHA Practice Development Pharmacist
 Opioid Addiction and Methadone: Myths and Misconceptions Nicole Nakatsu WRHA Practice Development Pharmacist Learning Objectives By the end of this presentation you should be able to: Understand how opioids
Opioid Addiction and Methadone: Myths and Misconceptions Nicole Nakatsu WRHA Practice Development Pharmacist Learning Objectives By the end of this presentation you should be able to: Understand how opioids
Applicant Webinar for BJA s Drug Court Discretionary Grant Solicitation
 Applicant Webinar for BJA s Drug Court Discretionary Grant Solicitation Cynthia Caporizzo, Senior Criminal Justice Advisor, Office of National Drug Control Policy (ONDCP) - Review of the administration
Applicant Webinar for BJA s Drug Court Discretionary Grant Solicitation Cynthia Caporizzo, Senior Criminal Justice Advisor, Office of National Drug Control Policy (ONDCP) - Review of the administration
MEDICALLY SUPERVISED OPIATE WITHDRAWAL FOR THE DEPENDENT PATIENT. An Outpatient Model
 MEDICALLY SUPERVISED OPIATE WITHDRAWAL FOR THE DEPENDENT PATIENT An Outpatient Model OBJECTIVE TO PRESENT A PROTOCOL FOR THE EVALUATION AND TREATMENT OF PATIENTS WHO ARE CHEMICALLY DEPENDENT ON OR SEVERLY
MEDICALLY SUPERVISED OPIATE WITHDRAWAL FOR THE DEPENDENT PATIENT An Outpatient Model OBJECTIVE TO PRESENT A PROTOCOL FOR THE EVALUATION AND TREATMENT OF PATIENTS WHO ARE CHEMICALLY DEPENDENT ON OR SEVERLY
Pain, Addiction & Methadone
 Pain, Addiction & Methadone A CHALLENGING INTERFACE METHADONE AND SUBOXONE OPIOID SUBSTITUTION CONFERENCE Objectives 2 Explore the interface between concurrent pain and addiction. Appreciate the challenges
Pain, Addiction & Methadone A CHALLENGING INTERFACE METHADONE AND SUBOXONE OPIOID SUBSTITUTION CONFERENCE Objectives 2 Explore the interface between concurrent pain and addiction. Appreciate the challenges
Section Editor Andrew J Saxon, MD
 Official reprint from UpToDate www.uptodate.com 2015 UpToDate Pharmacotherapy for opioid use disorder Author Eric Strain, MD Section Editor Andrew J Saxon, MD Deputy Editor Richard Hermann, MD All topics
Official reprint from UpToDate www.uptodate.com 2015 UpToDate Pharmacotherapy for opioid use disorder Author Eric Strain, MD Section Editor Andrew J Saxon, MD Deputy Editor Richard Hermann, MD All topics
Methadone and Pregnancy
 Methadone and Pregnancy Methadone 101/Hospitalist Workshop Launette Rieb, MD, MSc, CCFP, CCSAM, FCFP Clinical Associate Professor, Dept. Family Practice, UBC American Board of Addiction Medicine Certified
Methadone and Pregnancy Methadone 101/Hospitalist Workshop Launette Rieb, MD, MSc, CCFP, CCSAM, FCFP Clinical Associate Professor, Dept. Family Practice, UBC American Board of Addiction Medicine Certified
Beyond SBIRT: Integrating Addiction Medicine into Primary Care
 Beyond SBIRT: Integrating Addiction Medicine into Primary Care Community Clinic Association of Los Angeles County 14 th Annual Health Care Symposium March 6, 2015 Keith Heinzerling MD, Karen Lamp MD; Allison
Beyond SBIRT: Integrating Addiction Medicine into Primary Care Community Clinic Association of Los Angeles County 14 th Annual Health Care Symposium March 6, 2015 Keith Heinzerling MD, Karen Lamp MD; Allison
Treatment of Opioid Dependence: A Randomized Controlled Trial. Karen L. Sees, DO, Kevin L. Delucchi, PhD, Carmen Masson, PhD, Amy
 Category: Heroin Title: Methadone Maintenance vs 180-Day psychosocially Enriched Detoxification for Treatment of Opioid Dependence: A Randomized Controlled Trial Authors: Karen L. Sees, DO, Kevin L. Delucchi,
Category: Heroin Title: Methadone Maintenance vs 180-Day psychosocially Enriched Detoxification for Treatment of Opioid Dependence: A Randomized Controlled Trial Authors: Karen L. Sees, DO, Kevin L. Delucchi,
 Medication-Assisted Treatment (MAT) & What It Means Long-Term Gary K. Byrd., M.Ed., MAC, CCS, CAMS Methadone is the Gold Standard for treatment of chronic heroin addiction Gary Byrd 2015 1 Gary Byrd 2015
Medication-Assisted Treatment (MAT) & What It Means Long-Term Gary K. Byrd., M.Ed., MAC, CCS, CAMS Methadone is the Gold Standard for treatment of chronic heroin addiction Gary Byrd 2015 1 Gary Byrd 2015
Overview What are some commonly used opioids? Effects of opioids on the body How to recognise harms from opioid use How to recognise opioid
 Tobacco Opioids 139 5 Opioids Overview What are some commonly used opioids? Effects of opioids on the body How to recognise harms from opioid use How to recognise opioid dependence How to recognise opioid
Tobacco Opioids 139 5 Opioids Overview What are some commonly used opioids? Effects of opioids on the body How to recognise harms from opioid use How to recognise opioid dependence How to recognise opioid
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION
 MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Administrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Administrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids
1. According to recent US national estimates, which of the following substances is associated
 1 Chapter 36. Substance-Related, Self-Assessment Questions 1. According to recent US national estimates, which of the following substances is associated with the highest incidence of new drug initiates
1 Chapter 36. Substance-Related, Self-Assessment Questions 1. According to recent US national estimates, which of the following substances is associated with the highest incidence of new drug initiates
MAT Counselor Education Course Exam Questions Packet Part 1
 MAT Counselor Education Course Exam Questions Packet Part 1 Course No: Course Title: Course Objective: MA-1901P1 Medication-Assisted Treatment (MAT) Counselor Education Course Part 1 Includes primer on
MAT Counselor Education Course Exam Questions Packet Part 1 Course No: Course Title: Course Objective: MA-1901P1 Medication-Assisted Treatment (MAT) Counselor Education Course Part 1 Includes primer on
Detoxification. Dr Keron Fletcher Shropshire
 Detoxification Dr Keron Fletcher Shropshire 1 Stages of treatment Getting stable Staying stable Detoxifying (withdrawing) Staying drug-free 2 Getting stable Medical right dose of methadone/sbx Holds for
Detoxification Dr Keron Fletcher Shropshire 1 Stages of treatment Getting stable Staying stable Detoxifying (withdrawing) Staying drug-free 2 Getting stable Medical right dose of methadone/sbx Holds for
Treatments for drug misuse
 Understanding NICE guidance Information for people who use NHS services Treatments for drug misuse NICE clinical guidelines advise the NHS on caring for people with specific conditions or diseases and
Understanding NICE guidance Information for people who use NHS services Treatments for drug misuse NICE clinical guidelines advise the NHS on caring for people with specific conditions or diseases and
Using Drugs to Treat Drug Addiction How it works and why it makes sense
 Using Drugs to Treat Drug Addiction How it works and why it makes sense Jeff Baxter, MD University of Massachusetts Medical School May 17, 2011 Objectives Biological basis of addiction Is addiction a chronic
Using Drugs to Treat Drug Addiction How it works and why it makes sense Jeff Baxter, MD University of Massachusetts Medical School May 17, 2011 Objectives Biological basis of addiction Is addiction a chronic
A Guide to Treatment
 A Guide to Treatment A Guide to Treatment Acknowledgements This booklet was prepared by: Dr Adrian Dunlop, Turning Point Alcohol and Drug Centre Jay Jordens, Turning Point Alcohol and Drug Centre With
A Guide to Treatment A Guide to Treatment Acknowledgements This booklet was prepared by: Dr Adrian Dunlop, Turning Point Alcohol and Drug Centre Jay Jordens, Turning Point Alcohol and Drug Centre With
Opiate Abusers What can the GP do?
 Opiate Abusers What can the GP do? Office Based management of Opiate Addiction Dr Nigel Hawkins 1 Managing opiate abuse in General Practice The extent of Opiate Abuse in Australia What treatment options
Opiate Abusers What can the GP do? Office Based management of Opiate Addiction Dr Nigel Hawkins 1 Managing opiate abuse in General Practice The extent of Opiate Abuse in Australia What treatment options
Reintegration. Recovery. Medication-Assisted Treatment for Alcohol Dependence. Reintegration. Resilience
 Reintegration Recovery Medication-Assisted Treatment for Alcohol Dependence Reintegration Resilience 02 How do you free yourself from the stress and risks of alcohol dependence? Most people cannot do it
Reintegration Recovery Medication-Assisted Treatment for Alcohol Dependence Reintegration Resilience 02 How do you free yourself from the stress and risks of alcohol dependence? Most people cannot do it
Conceptualizing and Integrating Medication Assistant Treatment into your Court s Armamentarium
 Conceptualizing and Integrating Medication Assistant Treatment into your Court s Armamentarium Ted Parran JR. M.D. FACP Carter and Isabel Wang Professor of Medical Education CWRU School of Medicine tvp@case.edu
Conceptualizing and Integrating Medication Assistant Treatment into your Court s Armamentarium Ted Parran JR. M.D. FACP Carter and Isabel Wang Professor of Medical Education CWRU School of Medicine tvp@case.edu
ARCHIVED BULLETIN. Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E
 BULLETIN INTELLIGENCE Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E NDIC Within the past 2 years buprenorphine a Schedule III drug has been made available for use
BULLETIN INTELLIGENCE Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E NDIC Within the past 2 years buprenorphine a Schedule III drug has been made available for use
Dependence and Addiction. Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania
 Dependence and Addiction Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania Overview Heroin and other opiates The disease of heroin addiction or dependence Effective
Dependence and Addiction Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania Overview Heroin and other opiates The disease of heroin addiction or dependence Effective
DEVELOPING MANUFACTURING SUPPLYING. Naltrexone Implants. Manufactured by NalPharm Ltd WWW.NALPHARM.COM
 DEVELOPING MANUFACTURING SUPPLYING Naltrexone Implants Background to Nalpharm NalPharm is a specialist pharmaceutical company supplying proprietary branded medications and generic drugs in the area of
DEVELOPING MANUFACTURING SUPPLYING Naltrexone Implants Background to Nalpharm NalPharm is a specialist pharmaceutical company supplying proprietary branded medications and generic drugs in the area of
Substance Abuse lifestyle Concern for mother - fetus - and - neonate
 OBJECTIVES Learn about types of opioids and associated withdrawal symptoms Learn what medications are available to treat opioid addiction Understand the pros and cons associated with each medication Understand
OBJECTIVES Learn about types of opioids and associated withdrawal symptoms Learn what medications are available to treat opioid addiction Understand the pros and cons associated with each medication Understand
Suboxone A GUIDE TO TREATMENT
 Suboxone A GUIDE TO TREATMENT Acknowledgements This booklet was prepared by: Dr Adrian Dunlop, Turning Point Alcohol and Drug Centre Jay Jordens, Turning Point Alcohol and Drug Centre With contributions
Suboxone A GUIDE TO TREATMENT Acknowledgements This booklet was prepared by: Dr Adrian Dunlop, Turning Point Alcohol and Drug Centre Jay Jordens, Turning Point Alcohol and Drug Centre With contributions
Ever wish you could... Quit using heroin? Protect yourself from HIV infection? Get healthier?
 Ever wish you could... Quit using heroin? Protect yourself from HIV infection? Get healthier? Good News: Medical treatments called opioid (oh-pee-oyd) maintenance can help you! Injecting heroin puts you
Ever wish you could... Quit using heroin? Protect yourself from HIV infection? Get healthier? Good News: Medical treatments called opioid (oh-pee-oyd) maintenance can help you! Injecting heroin puts you
Medications Used in the Treatment of Addiction Developed by Randall Webber, MPH. Alcohol Withdrawal
 Medications Used in the Treatment of Addiction Developed by Randall Webber, MPH Alcohol Withdrawal MEDICATION Long/intermediateacting benzodiazepines (e.g., chlordiazepoxide/ Librium, diazepam/valium)
Medications Used in the Treatment of Addiction Developed by Randall Webber, MPH Alcohol Withdrawal MEDICATION Long/intermediateacting benzodiazepines (e.g., chlordiazepoxide/ Librium, diazepam/valium)
The Results of a Pilot of Vivitrol: A Medication Assisted Treatment for Alcohol and Opioid Addiction
 The Results of a Pilot of Vivitrol: A Medication Assisted Treatment for Alcohol and Opioid Addiction James H. Barger, MD SAPC Medical Director and Science Officer Desiree A. Crevecoeur-MacPhail, Ph.D.
The Results of a Pilot of Vivitrol: A Medication Assisted Treatment for Alcohol and Opioid Addiction James H. Barger, MD SAPC Medical Director and Science Officer Desiree A. Crevecoeur-MacPhail, Ph.D.
Support to Primary Care from Derbyshire Substance Misuse Service for prescribed / OTC drug dependence
 Support to Primary Care from Derbyshire Substance Misuse Service for prescribed / OTC drug dependence SUMMARY 1) Derbyshire Substance misuse service provides Psycho-social treatment interventions for ALL
Support to Primary Care from Derbyshire Substance Misuse Service for prescribed / OTC drug dependence SUMMARY 1) Derbyshire Substance misuse service provides Psycho-social treatment interventions for ALL
Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop
 Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop Launette Rieb, MSc, MD, CCFP, FCFP Clinical Associate Professor, Dept. Family Practice UBC American Board of Addiction Medicine Certified
Triage, Assessment & Treatment Methadone 101/Hospitalist Workshop Launette Rieb, MSc, MD, CCFP, FCFP Clinical Associate Professor, Dept. Family Practice UBC American Board of Addiction Medicine Certified
KAP Keys. For Physicians. Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine in the Treatment. of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Knowledge Application Program KAP Keys For Physicians Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Knowledge Application Program KAP Keys For Physicians Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine
Detox Day. RCGP June 13 th 2006. Daphne Rumball Addictions Psychiatrist. Norfolk. Daphne Rumball RCGP Detox Day June 2006 1
 Detox Day RCGP June 13 th 2006 Daphne Rumball Addictions Psychiatrist Norfolk Daphne Rumball RCGP Detox Day June 2006 1 Scope of presentation Undertaking detox in the community A review of evidence and
Detox Day RCGP June 13 th 2006 Daphne Rumball Addictions Psychiatrist Norfolk Daphne Rumball RCGP Detox Day June 2006 1 Scope of presentation Undertaking detox in the community A review of evidence and