|
|
|
- Heather Murphy
- 8 years ago
- Views:
Transcription
1 Jamie Dow MBA MD Émilie Turmel BSc Société de l assurance automobile du Québec NMEDA, Quebec 23 septembre septembre ( ) Société de l'assurance automobile du Québec, 2010 Page 1

2 The study 5-year project To examine : crash risk associated with medical conditions the effect of the severity of medical conditions upon crash risk the effectiveness of voluntary reporting of medical conditions the effectiveness of physician reporting (possibly) crash risk associated with medications
 crash risk associated with")
3 Situation Quebec has 4.9 million drivers /7.7 million population Universal health care coverage (RAMQ) Universal insurance coverage for personal injury caused by a road accident One agency administers road injury insurance, drivers permits and vehicle matriculation (SAAQ) Four-year approval process in order to combine both data banks SAAQ and RAMQ
 Four-year approval process")
4 Method Health insurance, hospitalisation and medications data obtained from Health Insurance Board (RAMQ) for all drivers with permits All health data grouped using the 3M CRG software Each driver assigned to a unique Clinical Risk Group (CRG) The CRG assigned reflects the nature and the severity of the driver s medical condition The basic health data may still be accessed (dx)

5 Data permit holders submitted to RAMQ were matched with their health data Health data obtained 1 July June drivers retained for study CRGs were assigned for each driver CRGs were then assigned to groupings that corresponded to the sub-divisions of the QC medical standards for drivers Data was analysed according to age, sex and permit class

6 Our population male drivers female drivers Age: 16 to 100 Permit class: Beginners:

7 Clinical Risk Groups Nine levels with increasing severity 1 Healthy 2 Significant acute illness 3 Single minor chronic disease 4 - Minor chronic disease in multiple organ systems 5 Single dominant or moderate chronic disease 6 Significant chronic disease in multiple organ systems 7 Dominant chronic disease in 3 or more organ systems 8 Dominant, metastatic and complicated malignancies 9 Catastrophic conditions

8 CRG Distribution

9 CRG Distribution 1,48% 0,73% 0,21% 7,20% 1 - Healthy + 17,43% 4 - Minor chronic disease multiple systems 2,50% 70,46% 5 - Single dominant or moderate chronic disease 6 - Significant chronic disease multiple systems 7 - Dominant chronic disease 3 or more systems 8 - Dominant, metastasic and complicated malignancies 9 - Catastrophic conditions

10 Drivers health 2003 Dementia 0% Endocrinology 4% Cancer 9% Other 20% Cardiac 22% Locomotor 6% Multiple 7% Diabetes 12% Psychiatry 10% Neurology 4% Vision 3% Respiratory 3%

11 Predicted versus observed medical conditions Predicted Study Healthy Cardiac Diabetes Predictions: Institut de la statistique du Québec: 2009

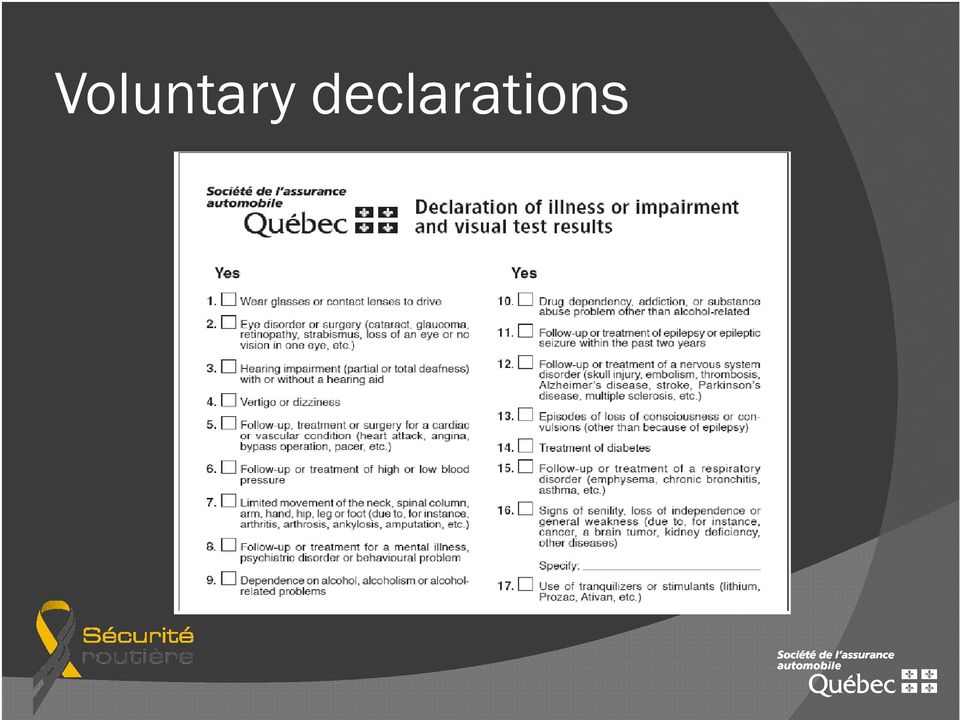
12 Voluntary declarations
13 Drivers health ,40% 70,60% Healthy/Minor Identified Condition

14 Drivers declarations 33,45% 66,55% Declaration No declaration

15 Voluntary declarations 80,00% 70,00% 60,00% 50,00% 40,00% 30,00% 20,00% 10,00% 0,00%

16 Diabetes declarations Dx Diabetes Declaration

17 Psychiatric declarations Psychiatric Dx Declaration

18 Class 1 drivers declarations 19,21% 80,79% Declaration No declaration

19 Class 1 drivers declarations 80,00% 79,43% 70,00% 60,00% 50,00% 40,00% 30,00% 20,00% 10,00% 0,00% 4,15% 6,07% 4,06% 0,86%1,25% 0,08% 0,87%0,35%0,07%0,04%0,07%0,32%0,05% 0,78% 0,99% 0,56%

20 Comparison declarations Class 1 versus all classes 80,00% 70,00% 60,00% 50,00% 40,00% 30,00% Class 1 All classes 20,00% 10,00% 0,00%

21 >65 drivers Men: Women: Total: % of the total driving population Page 21
22 Comparison >65 drivers with general driving population >65 All Men 61.24% 53.53% Women 38.76% 46.47%
23 Age groups Men Women Total > Total Page 23
24 Classes of permit Class % Class % Class % Class 4a % Class 4b % Class 4c % Class % Class 5 & motorcycle % Class 5 Learner %
25 Older drivers health 2003 Healthy General population 39.66% Population > % Of all who are healthy Men > % Women > % Of those > 65 who are healthy Men 57.54% Women 42.46%
26 Healthy Men >65 Men Healthy % % % % % % % % Total %
27 Healthy women >65 Women Healthy % % % % % % % % Total %
28 Healthy Men versus women drivers > 65 Men Women % 13.56% % 9.23% % 6.88% % 4.79% % 4.35% % 7.19% % 7.69% Total 8.97% 10.85%
29 Older drivers health 2003 Heart attack General population 1.47% Population > % Of all who had a heart attack Men > % Women > % Of those > 65 who had a heart attack Men 80.42% Women 19.58%
30 Heart attacks Men drivers > 65 Men With heart attack % % % % % % % % Total %
31 Heart attacks women drivers > 65 % Women With heart attacks % % % % % % Total %
32 Heart attacks Men versus women drivers > 65 Men Women % 2.25% % 3.33% % 4.78% % 6.54% % 9.08% % 10.07% % 15.38% Total 8.97% 3.45%
33 Older drivers health cataracts Cataracts General population 3.02% Population > % Of all who have cataracts Men > % Women > % Of those > 65 who have cataracts Men 56.46% Women 45.54%
34 Cataracts Men drivers > 65 Men With cataracts % % % % % % % % Total %
35 Cataracts women drivers > 65 Women With cataracts % % % % % % % % Total %
36 Cataracts Men versus women drivers > 65 Men Women % 14.25% % 24.38% % 31.76% % 34.95% % 32.63% % 25.90% % 38.46% Total 18.29% 22.28%
37 Older drivers health 2003 high blood pressure High blood pressure General population 16.10% Population > % Of all who have high blood pressure Men > % Women > % Of those > 65 who have high blood pressure Men 59.44% Women 40.56%
38 High blood pressure Men drivers >65 Men With HBP % % % % % % % % Total %
39 High blood pressure Women drivers >65 % Women With HBP % % % % % % % Total %
40 High blood pressure Men versus women drivers > 65 Men Women % 49.07% % 58.21% % 64.08% % 68.79% % 70.94% % 71.22% % 61.54% Total 52.25% 56.34%
41 Older drivers health diabetes Diabetes General population 6.28% Population > % Of all who have diabetes Men > % Women > % Of those > 65 who have diabetes Men 70.09% Women 29.91%
42 Older drivers health stroke Stroke (including TIA) General population 1.06% Population > % Of all who have had a stroke Men > % Women > % Of those > 65 who have had a stroke Men 69.67% Women 30.33%
43 Older drivers health 2003 substance abuse/dependency Substance abuse/dependency General population 1.59% Population > % Of all who have substance abuse/dependency Men > % Women > % Of those > 65 who have substance abuse/dependency Men 78.63% Women 21.37%
44 Older drivers health 2003 dementia Dementia General population 0.48% Population > % Of all who have dementia Men > % Women > % Of those > 65 who have dementia Men 68.77% Women 31.23%
45 Voluntary declaration >65 drivers 14,00% Drivers >65 with diagnosed condition 12,00% 10,00% 8,00% 6,00% 4,00% Drivers >65 with diagnosed condition 2,00% 0,00%
46 Declarations to the SAAQ by physicians for drivers >75 Chest pain/angina Age of drivers Health records Declared to SAAQ
47 Declarations to the SAAQ by physicians for drivers >75 Chest pain/angina 25.00% Heart attack 35.76% Congestive heart failure 24.03% High blood pressure 62.57% Respiratory (asthma, etc) 27.60% Cataracts 63.84% Glaucoma 33.73% Macular degeneration 39.49% Epilepsy 42.33% Diabetes 64.67%
48 Voluntary versus physicians declarations 70,00% 60,00% 50,00% 40,00% 30,00% Voluntary Physicians 20,00% 10,00% 0,00% Epilepsy Diabetes HBP Resp
49 Conclusions Most drivers report medical conditions they believe will not influence permit retention Voluntary disclosure of medical conditions is an unreliable source of information on the medical status of the driver Physicians tend to be selective in reporting conditions that may influence permit status Consequently, health data solicited without the accompanying health records is suspect
50 This study is financed and conducted by the SAAQ The study has been approved by the Commission d accès à l information du Québec and complies with all privacy of personal information laws. No personal information acquired through the study may be utilised by the SAAQ in its daily operations. Use of the CRG programme was made possible through an arrangement with 3M Canada. Particular thanks to Dr Marc Berlinguet and Jon Eisenhandler, 3M HIS Inc., USA Queries and correspondence: Dr Jamie Dow: jamie.dow@saaq.gouv.qc.ca
1MFBTF GJMM PVU GPSNT BOE GBY 'PSNT XJMM CF TJHOFE BU ZPVS BQQPJOUNFOU
 CELL PHONE: PATIENT HISTORY FORM - CONFIDENTIAL DATE: PATIENT: (LAST NAME) (FIRST NAME) (Ml) (NICKNAME) DOB: Primary Physician/ Family Doctor: Phone: Past Medical History (Click all that apply) High blood
CELL PHONE: PATIENT HISTORY FORM - CONFIDENTIAL DATE: PATIENT: (LAST NAME) (FIRST NAME) (Ml) (NICKNAME) DOB: Primary Physician/ Family Doctor: Phone: Past Medical History (Click all that apply) High blood
Personal Health Insurance Add family member
 Personal Health Insurance Add family member Policy 037000 ID number of owner A Plan information Health Coverage Choice (HCC) plan - Only complete section A, B and D. Add my spouse and/or child. I am aware
Personal Health Insurance Add family member Policy 037000 ID number of owner A Plan information Health Coverage Choice (HCC) plan - Only complete section A, B and D. Add my spouse and/or child. I am aware
RHODE ISLAND SERVICES FOR THE BLIND AND VISUALLY IMPAIRED ORS/DHS THE INDEPENDENT LIVING FOR OLDER BLIND PROGRAM
 RHODE ISLAND SERVICES FOR THE BLIND AND VISUALLY IMPAIRED ORS/DHS THE INDEPENDENT LIVING FOR OLDER BLIND PROGRAM FINAL EVALUATION REPORT OCTOBER 1, 2005 - SEPTEMBER 30, 2006 Prepared by Kristine L. Chadwick,
RHODE ISLAND SERVICES FOR THE BLIND AND VISUALLY IMPAIRED ORS/DHS THE INDEPENDENT LIVING FOR OLDER BLIND PROGRAM FINAL EVALUATION REPORT OCTOBER 1, 2005 - SEPTEMBER 30, 2006 Prepared by Kristine L. Chadwick,
Medicare Patient Information. Patient Name: SS#: - - Date of Birth: / / Sex: Female Male. City: State: Zip Code:
 Medicare Patient Information Patient Name: SS#: - - Date of Birth: / / Sex: Female Male Address: Street: City: State: Zip Code: Home Phone: ( ) - Work/Mobile Phone: ( ) - Please print your name as it Appears
Medicare Patient Information Patient Name: SS#: - - Date of Birth: / / Sex: Female Male Address: Street: City: State: Zip Code: Home Phone: ( ) - Work/Mobile Phone: ( ) - Please print your name as it Appears
19235 N Cave Creek Rd #104 Phoenix, AZ 85024 Phone: (602) 485-3414 Fax: (602) 788-0405
 485-3414 Fax: (602) 788-0405") 19235 N Cave Creek Rd #104 Phoenix, AZ 85024 Phone: (602) 485-3414 Fax: (602) 788-0405 Welcome to our practice. We are happy that you selected us as your eye care provider and appreciate the opportunity
19235 N Cave Creek Rd #104 Phoenix, AZ 85024 Phone: (602) 485-3414 Fax: (602) 788-0405 Welcome to our practice. We are happy that you selected us as your eye care provider and appreciate the opportunity
Retinal Consultants of San Antonio Diseases and Surgery of the Retina and Vitreous www.retinasanantonio. com
 Retinal Consultants of San Antonio Diseases and Surgery of the Retina and Vitreous www.retinasanantonio. com 1 Calvin E. Mein, MD 9480 Huebner Rd, Suite 310 (210) 615-1311 Moises A. Chica, MD San Antonio,
Retinal Consultants of San Antonio Diseases and Surgery of the Retina and Vitreous www.retinasanantonio. com 1 Calvin E. Mein, MD 9480 Huebner Rd, Suite 310 (210) 615-1311 Moises A. Chica, MD San Antonio,
MEDICAL-SURGICAL EYE CARE, P.A.
 MEDICAL-SURGICAL EYE CARE, P.A. DATE PATIENT'S NAME: ADDRESS: CITY/STATE/ZIP: DATE OF BIRTH: MARTIAL STATUS: M S D W HOME PHONE: ( ) SEX: M F AGE: CELLPHONE: ( ) IF CHILD; PARENT OR GUARDIAN NAME: EMERGENCY
MEDICAL-SURGICAL EYE CARE, P.A. DATE PATIENT'S NAME: ADDRESS: CITY/STATE/ZIP: DATE OF BIRTH: MARTIAL STATUS: M S D W HOME PHONE: ( ) SEX: M F AGE: CELLPHONE: ( ) IF CHILD; PARENT OR GUARDIAN NAME: EMERGENCY
NHS outcomes framework and CCG outcomes indicators: Data availability table
 NHS outcomes framework and CCG outcomes indicators: Data availability table December 2012 NHS OF objectives Preventing people from dying prematurely DOMAIN 1: preventing people from dying prematurely Potential
NHS outcomes framework and CCG outcomes indicators: Data availability table December 2012 NHS OF objectives Preventing people from dying prematurely DOMAIN 1: preventing people from dying prematurely Potential
Personal Health Insurance application form
 Personal Health Insurance application form In this application, you and your refer to the proposed insured and the applicant. We, us, our and the company refer to Sun Life Assurance Company of Canada,
Personal Health Insurance application form In this application, you and your refer to the proposed insured and the applicant. We, us, our and the company refer to Sun Life Assurance Company of Canada,
Critical Illness Insurance. What is Critical Illness Insurance
 Critical Illness Insurance What is Critical Illness Insurance Whereas life insurance has been readily available for literally hundreds of years, critical illness insurance is a relatively recent development.
Critical Illness Insurance What is Critical Illness Insurance Whereas life insurance has been readily available for literally hundreds of years, critical illness insurance is a relatively recent development.
Experience and Quality Assurance MES Vision Provider Network nationwide Four
 Experience and Quality Assurance MESVision has been providing exceptional vision care services to millions of individuals and thousands of employer groups since 1976 MESVision is the only medically led
Experience and Quality Assurance MESVision has been providing exceptional vision care services to millions of individuals and thousands of employer groups since 1976 MESVision is the only medically led
Application for Whole Life Insurance SIMPLIFIED ISSUE APPLICATION FORM
 Application for Whole Life Insurance Underwritten by Western Life Assurance Mail Application to: Everest Team, c/o HP Enterprise Services, 5150 Spectrum Way, Mailstop 4002, Mississauga, ON L4W 5G1 1 800
Application for Whole Life Insurance Underwritten by Western Life Assurance Mail Application to: Everest Team, c/o HP Enterprise Services, 5150 Spectrum Way, Mailstop 4002, Mississauga, ON L4W 5G1 1 800
Medical History Questionnaire
 Medical History Questionnaire Name: Date: Allergies (including latex): List all medications that you are currently taking, either prescription or non- prescription. Please specify dosage and length of
Medical History Questionnaire Name: Date: Allergies (including latex): List all medications that you are currently taking, either prescription or non- prescription. Please specify dosage and length of
Lake Oswego Eye Clinic 530 First ST, Suite A Lake Oswego, OR 97068 Office: (503) 636-9608 Fax: (503) 636-9600
 636-9608 Fax: (503) 636-9600") PAYMENT AGREEMENT: We accept most insurance plans as a courtesy. We encourage you to familiarize yourself with your individual plan. Insurance coverage is an agreement between patient and insurance company
PAYMENT AGREEMENT: We accept most insurance plans as a courtesy. We encourage you to familiarize yourself with your individual plan. Insurance coverage is an agreement between patient and insurance company
Louisiana Report 2013
 Louisiana Report 2013 Prepared by Louisiana State University s Public Policy Research Lab For the Department of Health and Hospitals State of Louisiana December 2015 Introduction The Behavioral Risk Factor
Louisiana Report 2013 Prepared by Louisiana State University s Public Policy Research Lab For the Department of Health and Hospitals State of Louisiana December 2015 Introduction The Behavioral Risk Factor
SUMMARY OF FINDINGS: OMF 2015 MEDICAL NEEDS ASSESSMENT
 SUMMARY OF FINDINGS: OMF 2015 MEDICAL NEEDS ASSESSMENT DEMOGRAPHICS Total surveys completed: 341 62 % Eastsound area 13 % Deer Harbor area 16 % Olga area 9 % Orcas Ferry area Age 2 % 25 34 8 % 35 44 13
SUMMARY OF FINDINGS: OMF 2015 MEDICAL NEEDS ASSESSMENT DEMOGRAPHICS Total surveys completed: 341 62 % Eastsound area 13 % Deer Harbor area 16 % Olga area 9 % Orcas Ferry area Age 2 % 25 34 8 % 35 44 13
Medical Matters Action Checklists
 Medical Matters Action Checklists The following Action Checklists are included in Chapter 5: Medical History Personal Medication Record Health Care Power of Attorney Medical Orders (Do Not Resuscitate/POLST)
Medical Matters Action Checklists The following Action Checklists are included in Chapter 5: Medical History Personal Medication Record Health Care Power of Attorney Medical Orders (Do Not Resuscitate/POLST)
Patient Demographic Sheet
 Patient Demographic Sheet Patient Name: Date of Birth: Address: City, State, Zip Code: Home Phone: Cell Phone: Work Phone: E-Mail: Sex: Male Female Marital Status: Married Single Other Occupation: Employer:
Patient Demographic Sheet Patient Name: Date of Birth: Address: City, State, Zip Code: Home Phone: Cell Phone: Work Phone: E-Mail: Sex: Male Female Marital Status: Married Single Other Occupation: Employer:
PATIENT INFORMATION: PATIENT CONTACT PHONE NUMBERS: PHYSICIAN INFORMATION: HEALTH INSURANCE INFORMATION:
 PATIENT INFORMATION: TODAY S DATE: HOW DID YOU HEAR ABOUT US?: LAST NAME: FIRST NAME: STREET CITY: STATE: ZIP: EMAIL MARTIAL STATUS: SINGLE MARRIED DIVORCED WIDOWED SEPARATED BIRTHDATE: AGE: SEX: MALE
PATIENT INFORMATION: TODAY S DATE: HOW DID YOU HEAR ABOUT US?: LAST NAME: FIRST NAME: STREET CITY: STATE: ZIP: EMAIL MARTIAL STATUS: SINGLE MARRIED DIVORCED WIDOWED SEPARATED BIRTHDATE: AGE: SEX: MALE
CORONADO EYE ASSOCIATES GLENN B. COOK, M.D., PhD 801 ORANGE AVENUE, STE. 204 - CORONADO, CA 92118 619.437-4406 FAX 619.522-7983
 Dear Please allow us to welcome you to our practice. Our first priority is to provide you with the best care possible. Enclosed is your patient information sheet and medical history questionnaire. Please
Dear Please allow us to welcome you to our practice. Our first priority is to provide you with the best care possible. Enclosed is your patient information sheet and medical history questionnaire. Please
RIDGE PHYSICAL THERAPY & WELLNESS CENTER. Intake Form
 Intake Form : Personal Information please print clearly Name: last first middle initial Home Address: Home Telephone: ( ) Cell Phone: E-Mail Address: Social Security #: of Birth: Age: Sex: M F Marital
Intake Form : Personal Information please print clearly Name: last first middle initial Home Address: Home Telephone: ( ) Cell Phone: E-Mail Address: Social Security #: of Birth: Age: Sex: M F Marital
INSTRUCTIONS CHECKLIST
 These instructions have been designed for you to simplify the application process. Read these instructions in full before you begin. If you have any questions, please call Medipac for further assistance
These instructions have been designed for you to simplify the application process. Read these instructions in full before you begin. If you have any questions, please call Medipac for further assistance
How To Write A Recipe Card
 Joanne R. Festa, PhD (PLEASE PRINT) NAME: DATE OF BIRTH: NEUROPSYCHOLOGY INITIAL VISIT DATE: AGE: Do you have any areas of concern about your cognitive functioning? (i.e., problems with memory, attention,
Joanne R. Festa, PhD (PLEASE PRINT) NAME: DATE OF BIRTH: NEUROPSYCHOLOGY INITIAL VISIT DATE: AGE: Do you have any areas of concern about your cognitive functioning? (i.e., problems with memory, attention,
NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only)
") PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
Group Benefits Evidence of Insurability for Comprehensive Optional Critical Illness Insurance
 Group Benefits Evidence of Insurability for Comprehensive Optional Critical Illness Insurance INSTRUCTIONS - Please print all answers If required, retain a photocopy for your files. 1a) Plan contract number(s)
Group Benefits Evidence of Insurability for Comprehensive Optional Critical Illness Insurance INSTRUCTIONS - Please print all answers If required, retain a photocopy for your files. 1a) Plan contract number(s)
UK Patients with Chronic Conditions Believe the Ability to Access Electronic Medical Records Outweighs Concern of Privacy Invasion
 Insight Driven Health UK Patients with Chronic Conditions Believe the Ability to Access Electronic Medical Records Outweighs Concern of Privacy Invasion Accenture s research shows patients with chronic
Insight Driven Health UK Patients with Chronic Conditions Believe the Ability to Access Electronic Medical Records Outweighs Concern of Privacy Invasion Accenture s research shows patients with chronic
Personal Insurance. Do I need Trauma cover? a safety. to help get you back on track
 Personal Insurance Do I need Trauma cover? a safety to help get you back on track Being able to focus on your recovery after suffering a traumatic event is going to be your primary concern. Having trauma
Personal Insurance Do I need Trauma cover? a safety to help get you back on track Being able to focus on your recovery after suffering a traumatic event is going to be your primary concern. Having trauma
Personal Disability Income Protector Individual Short-Term Disability Insurance
 Personal Disability Income Protector Individual Short-Term Disability Insurance Plan Highlights Selection of: monthly benefit amount elimination period benefit period Benefits paid regardless of any other
Personal Disability Income Protector Individual Short-Term Disability Insurance Plan Highlights Selection of: monthly benefit amount elimination period benefit period Benefits paid regardless of any other
PATIENT REGISTRATION
 Evan Wolf, MD PhD Jacob Frank, OD PATIENT REGISTRATION Welcome to our office. In order to serve you properly, we will need the following information. (Please Print) Patient First Name Middle Initial Last
Evan Wolf, MD PhD Jacob Frank, OD PATIENT REGISTRATION Welcome to our office. In order to serve you properly, we will need the following information. (Please Print) Patient First Name Middle Initial Last
How To Write Long Term Care Insurance
 By Lori Boyce, AVP Risk Management and R&D Underwriting long term care insurance: a primer Every day Canadians die, are diagnosed with cancer, have heart attacks and become disabled and our insurance solutions
By Lori Boyce, AVP Risk Management and R&D Underwriting long term care insurance: a primer Every day Canadians die, are diagnosed with cancer, have heart attacks and become disabled and our insurance solutions
Voluntary Benefits Employee Enrollment and Change Form
 Voluntary Benefits Employee Enrollment and Change Form LifeMap Assurance Company TM For residents of Oregon and Washington, the definition of a Spouse includes your legal husband or wife or your State
Voluntary Benefits Employee Enrollment and Change Form LifeMap Assurance Company TM For residents of Oregon and Washington, the definition of a Spouse includes your legal husband or wife or your State
HEALTH MANAGEMENT PLAN PROGRAMME
 HEALTH MANAGEMENT PLAN PROGRAMME Medical Controls for Referees and Candidates The FIVB believes that Referees and Referees Candidates health is very important therefore in accordance with the Medical and
HEALTH MANAGEMENT PLAN PROGRAMME Medical Controls for Referees and Candidates The FIVB believes that Referees and Referees Candidates health is very important therefore in accordance with the Medical and
Application for Optional Life Insurance
 Application for Optional Life Insurance Contract number 50146 Please PRINT clearly. 1 General information Graduate Students Association of the University of Alberta In this application you and your refer
Application for Optional Life Insurance Contract number 50146 Please PRINT clearly. 1 General information Graduate Students Association of the University of Alberta In this application you and your refer
AMERICAN HERITAGE LIFE INSURANCE COMPANY (AHL) 1776 AMERICAN HERITAGE LIFE DRIVE JACKSONVILLE, FLORIDA 32224
 1776 AMERICAN HERITAGE LIFE DRIVE JACKSONVILLE, FLORIDA 32224") AMERICAN HERITAGE LIFE INSURANCE COMPANY (AHL) 1776 AMERICAN HERITAGE LIFE DRIVE JACKSONVILLE, FLORIDA 32224 For AHL Home Office use only tes EVIDENCE OF INSURABILITY AND ENROLLMENT FORM Check appropriate
AMERICAN HERITAGE LIFE INSURANCE COMPANY (AHL) 1776 AMERICAN HERITAGE LIFE DRIVE JACKSONVILLE, FLORIDA 32224 For AHL Home Office use only tes EVIDENCE OF INSURABILITY AND ENROLLMENT FORM Check appropriate
Part 3 Disease incidence, prevalence and disability
 Part 3 Disease incidence, prevalence and disability 9. How many people become sick each year? 28 10. Cancer incidence by site and region 29 11. How many people are sick at any given time? 31 12. Prevalence
Part 3 Disease incidence, prevalence and disability 9. How many people become sick each year? 28 10. Cancer incidence by site and region 29 11. How many people are sick at any given time? 31 12. Prevalence
PATIENT REGISTRATION FORM PATIENT INFORMATION
 Siepser Laser Eye Care PATIENT REGISTRATION FORM : PATIENT INFORMATION First Name Middle Initial: Last Name: Birth : Gender: Male Female Marital Status: SSN: Driver s License #: Address: City: State: Zip:
Siepser Laser Eye Care PATIENT REGISTRATION FORM : PATIENT INFORMATION First Name Middle Initial: Last Name: Birth : Gender: Male Female Marital Status: SSN: Driver s License #: Address: City: State: Zip:
P.S. Please remember to bring your completed forms to your office visit!
 Dear Patient: Please print the following forms and complete them as accurately as possible and bring them with you to your office visit. If you have any questions about the forms you can call my office
Dear Patient: Please print the following forms and complete them as accurately as possible and bring them with you to your office visit. If you have any questions about the forms you can call my office
Stonebridge Adult Medicine, P.A. Registration Form (Please Print)
") Stonebridge Adult Medicine, P.A. Registration Form (Please Print) PATIENT INFORMATION Last Name: First Name: Is this your legal name? Yes No If not what is your legal name: Date of Birth: Sex: male female
Stonebridge Adult Medicine, P.A. Registration Form (Please Print) PATIENT INFORMATION Last Name: First Name: Is this your legal name? Yes No If not what is your legal name: Date of Birth: Sex: male female
Please allow us to welcome you to our practice. Our first priority is to provide you with the best care possible.
 PAUL L. TREGER, M.D. RANDALL CONRAD, O.D. GLENN B. COOK, M.D., PhD TARA BROWN, M.D. 7877 PARKWAY DRIVE SUITE 100 - LA MESA, CA 91942 619.286.3711 FAX 619.286.2184 Dear Please allow us to welcome you to
PAUL L. TREGER, M.D. RANDALL CONRAD, O.D. GLENN B. COOK, M.D., PhD TARA BROWN, M.D. 7877 PARKWAY DRIVE SUITE 100 - LA MESA, CA 91942 619.286.3711 FAX 619.286.2184 Dear Please allow us to welcome you to
Driver indicated a loss or impairment of consciousness within last: 6 months 12 months or more Date: / /
 PHYSICIAN S STATEMENT OF EXAMINATION Michigan Department of State Driver Assessment and Appeal Division P.O. Box 30196, Lansing, Michigan 48909-7696 Phone: (517) 335-7051; Fax: (517) 335-2189; E-mail:
PHYSICIAN S STATEMENT OF EXAMINATION Michigan Department of State Driver Assessment and Appeal Division P.O. Box 30196, Lansing, Michigan 48909-7696 Phone: (517) 335-7051; Fax: (517) 335-2189; E-mail:
SUBSTANDARD UNDERWRITING
 H I G H L I G H T E R SUBSTANDARD UNDERWRITING Substandard Marketing Opportunities Tips for Selling Life Insurance in the Substandard Market Recognizing a Substandard Marketing Situation The substandard
H I G H L I G H T E R SUBSTANDARD UNDERWRITING Substandard Marketing Opportunities Tips for Selling Life Insurance in the Substandard Market Recognizing a Substandard Marketing Situation The substandard
Traveller s medical appraisal form
 Traveller s medical appraisal form Please email your completed medical appraisal form to travel.emc@qbe.com or fax to 1300 657 127. Before completing the medical appraisal form, please ensure you have
Traveller s medical appraisal form Please email your completed medical appraisal form to travel.emc@qbe.com or fax to 1300 657 127. Before completing the medical appraisal form, please ensure you have
Disability Claim Form Initial Request
 GROUP INSURANCE Disability Claim Form A partner you can trust. www.inalco.com According to your region, please submit the completed form to: Quebec All Other Provinces PO Box 790, Station B 522 University
GROUP INSURANCE Disability Claim Form A partner you can trust. www.inalco.com According to your region, please submit the completed form to: Quebec All Other Provinces PO Box 790, Station B 522 University
PATIENT REGISTRATION FORM PATIENT INFORMATION
 Siepser Laser Eye Care PATIENT REGISTRATION FORM : PATIENT INFORMATION First Name Middle Initial: Last Name: Birth : Gender: Male Female Marital Status: SSN: Driver s License #: Address: City: State: Zip:
Siepser Laser Eye Care PATIENT REGISTRATION FORM : PATIENT INFORMATION First Name Middle Initial: Last Name: Birth : Gender: Male Female Marital Status: SSN: Driver s License #: Address: City: State: Zip:
Overview. Geriatric Overview. Chapter 26. Geriatrics 9/11/2012
 Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary.
 PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary. Today s : Are you here for an injury that is work-related? YES NO N/A Patient Name (First-Middle-Last)
PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary. Today s : Are you here for an injury that is work-related? YES NO N/A Patient Name (First-Middle-Last)
THE EYE INSTITUTE. Dear Patient:
 THE EYE INSTITUTE Eye Associates of Wayne P.A. 968 Hamburg Turnpike Wayne, NJ 07470 p. 973-696-0300 f. 973-696-0464 Eye Institute North, LLC 5677 Berkshire Valley Rd. Oak Ridge, NJ 07438 p. 973-208-0600
THE EYE INSTITUTE Eye Associates of Wayne P.A. 968 Hamburg Turnpike Wayne, NJ 07470 p. 973-696-0300 f. 973-696-0464 Eye Institute North, LLC 5677 Berkshire Valley Rd. Oak Ridge, NJ 07438 p. 973-208-0600
Dr. David Y. Liao, D.O. Orthopedic Center, LLC. Release of Information
 Release of Information The purpose of this form is to alert our office as to those family members and/or friends who may be scheduling or canceling appointments on your behalf and/or will need to have
Release of Information The purpose of this form is to alert our office as to those family members and/or friends who may be scheduling or canceling appointments on your behalf and/or will need to have
Complete coverage. Unbeatable value.
 Quest Travel Insurance Complete coverage. Unbeatable value. Quest with confidence, anytime, anywhere! Quest protects you when nothing else can, with: Future stability coverage: Stable now? Not sure you
Quest Travel Insurance Complete coverage. Unbeatable value. Quest with confidence, anytime, anywhere! Quest protects you when nothing else can, with: Future stability coverage: Stable now? Not sure you
Business Loan Insurance Plan Critical Illness Claim - Policy 57903
 Business Loan Insurance Plan Critical Illness Claim - Policy 57903 RBC use only Before submitting a critical illness claim: Complete and sign the Claimant s Statement for your critical illness. Please
Business Loan Insurance Plan Critical Illness Claim - Policy 57903 RBC use only Before submitting a critical illness claim: Complete and sign the Claimant s Statement for your critical illness. Please
Insurance (Let us make a copy of your insurance card and you can skip this section)
") Today s Date: Name: What do you prefer to be called: Male / Female (please circle) Birth Date: Mailing Address: City: State: Zip: Home Phone: Cell Phone: Email: Referred By: Employer: How long employed:
Today s Date: Name: What do you prefer to be called: Male / Female (please circle) Birth Date: Mailing Address: City: State: Zip: Home Phone: Cell Phone: Email: Referred By: Employer: How long employed:
How to Remove a Social History Smoke?
 AUSTIN RETINA ASSOCIATES PATIENT INFORMATION NAME: MAILING ADDRESS or NURSING HOME NAME & ADDRESS: Last First Middle Initial CITY: STATE: ZIP CODE: - TELEPHONE: HOME:( ) CELL: ( ) WORK:( ) DATE OF BIRTH:
AUSTIN RETINA ASSOCIATES PATIENT INFORMATION NAME: MAILING ADDRESS or NURSING HOME NAME & ADDRESS: Last First Middle Initial CITY: STATE: ZIP CODE: - TELEPHONE: HOME:( ) CELL: ( ) WORK:( ) DATE OF BIRTH:
Patient Information. Name: Soc Security #: Date of Birth: Age: Male / Female. LOCAL Address: Street City State Zip. Phone: Home: Cell / Work:
 Patient Information PERSONAL INFORMATION (Please Print Clearly) Name: Soc Security #: Date of Birth: Age: Male / Female LOCAL Address: Street City State Zip Phone: Home: Cell / Work: Email Address: Out
Patient Information PERSONAL INFORMATION (Please Print Clearly) Name: Soc Security #: Date of Birth: Age: Male / Female LOCAL Address: Street City State Zip Phone: Home: Cell / Work: Email Address: Out
Voluntary Benefits Employee Enrollment and Change Form
 LifeMap Assurance Company TM P.O. Box 1271, MS E-3A Portland, OR 97207-1271 (503) 721-7161 (800) 794-5390 Voluntary Benefits Employee Enrollment and Change Form For residents of Oregon and Washington,
LifeMap Assurance Company TM P.O. Box 1271, MS E-3A Portland, OR 97207-1271 (503) 721-7161 (800) 794-5390 Voluntary Benefits Employee Enrollment and Change Form For residents of Oregon and Washington,
TALLAHASSEE EYE CENTER
 TALLAHASSEE EYE CENTER PATIENT INFORMATION Date: Name: Gender: M / F First MI Last Date of Birth: / / Address: City: State: ZIP: Phone Numbers: Home: Cellular: Work: E-Mail: SS#: - - What is the best way
TALLAHASSEE EYE CENTER PATIENT INFORMATION Date: Name: Gender: M / F First MI Last Date of Birth: / / Address: City: State: ZIP: Phone Numbers: Home: Cellular: Work: E-Mail: SS#: - - What is the best way
PATIENT INFORMATION FORM. Name: Address: City: State: Zip: Social Security Number: Telephone Numbers Home: Age: Sex: M / F Work: Email: Cell:
 PATIENT INFORMATION FORM Name: Address: City: State: Zip: Social Security Number: Telephone Numbers DOB: Home: Age: Sex: M / F Work: Email: Cell: Marital Status: Single Married Spouse s Name: Widowed Divorced
PATIENT INFORMATION FORM Name: Address: City: State: Zip: Social Security Number: Telephone Numbers DOB: Home: Age: Sex: M / F Work: Email: Cell: Marital Status: Single Married Spouse s Name: Widowed Divorced
Key Health Areas Mapped to Out of Hospital Programme Areas
 1 Key Area (according to letter from David Nicholson) Reducing the number of years of life lost by the people of England from treatable conditions (e.g. including cancer, stroke, heart disease, respiratory
1 Key Area (according to letter from David Nicholson) Reducing the number of years of life lost by the people of England from treatable conditions (e.g. including cancer, stroke, heart disease, respiratory
Nearest Relative Information (Not in same household)
") Patient Information Name Male Female Address City State Zip Birth Date Age Responsible Party Information Name: Self Parent/Guardian Birth Date SSN# Drivers License# Email Employer Employer Phone# Employer
Patient Information Name Male Female Address City State Zip Birth Date Age Responsible Party Information Name: Self Parent/Guardian Birth Date SSN# Drivers License# Email Employer Employer Phone# Employer
Depression in Older Persons
 Depression in Older Persons How common is depression in later life? Depression affects more than 6.5 million of the 35 million Americans aged 65 or older. Most people in this stage of life with depression
Depression in Older Persons How common is depression in later life? Depression affects more than 6.5 million of the 35 million Americans aged 65 or older. Most people in this stage of life with depression
APPLICATION FOR MEDICARE SUPPLEMENT COVERAGE
 CENTRAL STATES INDEMNITY CO. OF OMAHA Home Office: Omaha, NE Administration: P.O. Box 10816 Clearwater, Florida 33757-8816 APPLICATION FOR MEDICARE SUPPLEMENT COVERAGE SECTION A. PROPOSED INSURED INFORMATION
CENTRAL STATES INDEMNITY CO. OF OMAHA Home Office: Omaha, NE Administration: P.O. Box 10816 Clearwater, Florida 33757-8816 APPLICATION FOR MEDICARE SUPPLEMENT COVERAGE SECTION A. PROPOSED INSURED INFORMATION
Personal Injury Intake Form
 Personal Injury Intake Form Patient Information: Name Home Phone Address Work Phone Cell Phone Date of Birth Social Security # Sex Male Female Height Weight lbs Occupation Marital Status Employer No of
Personal Injury Intake Form Patient Information: Name Home Phone Address Work Phone Cell Phone Date of Birth Social Security # Sex Male Female Height Weight lbs Occupation Marital Status Employer No of
Thank you for making an appointment with our office. We look forward to serving your visual needs.
 Dear New Patient, Thank you for making an appointment with our office. We look forward to serving your visual needs. Enclosed you will find our New Patient Questionnaires. Please complete these and fax
Dear New Patient, Thank you for making an appointment with our office. We look forward to serving your visual needs. Enclosed you will find our New Patient Questionnaires. Please complete these and fax
THE ROWANS SURGERY MEDICAL HISTORY QUESTIONNAIRE MALE & FEMALE 18+
 THE ROWANS SURGERY MEDICAL HISTORY QUESTIONNAIRE MALE & FEMALE 18+ Surname: First Name: Date of Birth: NHS Number: / / Mobile Telephone No: Male / Female If you wish to sign up for Vision On-Line services
THE ROWANS SURGERY MEDICAL HISTORY QUESTIONNAIRE MALE & FEMALE 18+ Surname: First Name: Date of Birth: NHS Number: / / Mobile Telephone No: Male / Female If you wish to sign up for Vision On-Line services
Administrator means the administrator of giraffe & friends RESP, being Giraffe & Friends Life Insurance Company.
 Completion Insurance Life & Total & Permanent Disability Insurance Important information about your insurance Customer Service Inquiries - Please contact Giraffe & Friends Life Insurance Company at 1-844-MY-GANDF
Completion Insurance Life & Total & Permanent Disability Insurance Important information about your insurance Customer Service Inquiries - Please contact Giraffe & Friends Life Insurance Company at 1-844-MY-GANDF
HEALTH RISK ASSESSMENT (HRS) QUESTIONNAIRE
 QUESTIONNAIRE") HEALTH RISK ASSESSMENT (HRS) QUESTIONNAIRE The Health Risk Assessment (HRA) questionnaire provides participants with an evaluation of their current health and quality of life. The assessment promotes health
HEALTH RISK ASSESSMENT (HRS) QUESTIONNAIRE The Health Risk Assessment (HRA) questionnaire provides participants with an evaluation of their current health and quality of life. The assessment promotes health
Supplemental Technical Information
 An Introductory Analysis of Potentially Preventable Health Care Events in Minnesota Overview Supplemental Technical Information This document provides additional technical information on the 3M Health
An Introductory Analysis of Potentially Preventable Health Care Events in Minnesota Overview Supplemental Technical Information This document provides additional technical information on the 3M Health
STATISTICAL BRIEF #8. Conditions Related to Uninsured Hospitalizations, 2003. Highlights. Introduction. Findings. May 2006
 HEALTHCARE COST AND UTILIZATION PROJECT STATISTICAL BRIEF #8 Agency for Healthcare Research and Quality May 2006 Conditions Related to Uninsured Hospitalizations, 2003 Anne Elixhauser, Ph.D. and C. Allison
HEALTHCARE COST AND UTILIZATION PROJECT STATISTICAL BRIEF #8 Agency for Healthcare Research and Quality May 2006 Conditions Related to Uninsured Hospitalizations, 2003 Anne Elixhauser, Ph.D. and C. Allison
Welcome! Thank you for choosing our practice for your eye care needs! Please fill out our new patient registration paperwork.
 Welcome! Thank you for choosing our practice for your eye care needs! Please fill out our new patient registration paperwork. So we may eliminate any potential waiting time, please fax the completed forms
Welcome! Thank you for choosing our practice for your eye care needs! Please fill out our new patient registration paperwork. So we may eliminate any potential waiting time, please fax the completed forms
Personal Disability Income Protector Short-Term Disability Insurance
 Personal Disability Income Protector Short-Term Disability Insurance Plan Highlights Selection of: monthly benefit amount elimination period benefit period Benefits paid regardless of any other insurance
Personal Disability Income Protector Short-Term Disability Insurance Plan Highlights Selection of: monthly benefit amount elimination period benefit period Benefits paid regardless of any other insurance
SOUTH TAMPA MULTIPLE SCLEROSIS CENTER
 SOUTH TAMPA MULTIPLE SCLEROSIS CENTER PATIENT/CARE GIVER QUESTIONNAIRE DEMOGRAPHIC INFORMATION Patient's Name: City: State: Zip Code: Phone: Marital Status: Spouse/Care Giver Name: Phone (H) (W) Occupation:
SOUTH TAMPA MULTIPLE SCLEROSIS CENTER PATIENT/CARE GIVER QUESTIONNAIRE DEMOGRAPHIC INFORMATION Patient's Name: City: State: Zip Code: Phone: Marital Status: Spouse/Care Giver Name: Phone (H) (W) Occupation:
ALBANY PLASTIC SURGEONS, PLLC 4 Executive Park Drive Albany NY 12203 (518) 438-1434 PATIENT INFORMATION FORM
 438-1434 PATIENT INFORMATION FORM") ALBANY PLASTIC SURGEONS, PLLC 4 Executive Park Drive Albany NY 12203 (518) 438-1434 PATIENT INFORMATION FORM Today s Date: PERSONAL INFORMATION First Name: Last Name: MI: Address: City: State/Province:
ALBANY PLASTIC SURGEONS, PLLC 4 Executive Park Drive Albany NY 12203 (518) 438-1434 PATIENT INFORMATION FORM Today s Date: PERSONAL INFORMATION First Name: Last Name: MI: Address: City: State/Province:
Depression often coexists with other chronic conditions
 Depression A treatable disease PROPORTION OF PATIENTS WHO ARE DEPRESSED, BY CHRONIC CONDITION Diabetes 33% Parkinson s Disease % Recent Stroke % Hospitalized with Cancer 42% Recent Heart Attack 45% SOURCE:
Depression A treatable disease PROPORTION OF PATIENTS WHO ARE DEPRESSED, BY CHRONIC CONDITION Diabetes 33% Parkinson s Disease % Recent Stroke % Hospitalized with Cancer 42% Recent Heart Attack 45% SOURCE:
Western Center Eye Care 2720 Western Center Blvd Ste 316 Fort Worth, TX 76131
 Today s Date Western Center Eye Care WELCOME TO OUR OFFICE Patient s Name (First, Middle, Last): Address: City: State: Zip Code: Email: Main Contact #: Alternate#: Date of Birth: / / Sex: Male Female Primary
Today s Date Western Center Eye Care WELCOME TO OUR OFFICE Patient s Name (First, Middle, Last): Address: City: State: Zip Code: Email: Main Contact #: Alternate#: Date of Birth: / / Sex: Male Female Primary
Advantage Physical Therapy Patient Registration
 Appointment Date/Time: Therapist: Advantage Physical Therapy Patient Registration ****Please note ALL patients are required to have a prescription for Physical Therapy from a referring Physician prior
Appointment Date/Time: Therapist: Advantage Physical Therapy Patient Registration ****Please note ALL patients are required to have a prescription for Physical Therapy from a referring Physician prior
We understand you want support right from the beginning
 PROTECT We understand you want support right from the beginning PRUearly stage crisis cover Should an illness strike, the earlier it is diagnosed, the easier it is to manage and the higher the chances
PROTECT We understand you want support right from the beginning PRUearly stage crisis cover Should an illness strike, the earlier it is diagnosed, the easier it is to manage and the higher the chances
Carefree. Travel ANYWHERE IN THE WORLD
 Carefree Travel ANYWHERE IN THE WORLD Information contained in this document is of an indicative nature only and does not bind the Société de l assurance automobile du Québec. Legal deposit Bibliothèque
Carefree Travel ANYWHERE IN THE WORLD Information contained in this document is of an indicative nature only and does not bind the Société de l assurance automobile du Québec. Legal deposit Bibliothèque
MEDICAL & OCULAR HISTORY QUESTIONAIRRE
 MEDICAL & OCULAR HISTORY QUESTIONAIRRE Name: Date: Age: Preferred Pharmacy Name: Address: 1. Please describe briefly the main reason you are being examined today. 2. Do you have any of the following conditions
MEDICAL & OCULAR HISTORY QUESTIONAIRRE Name: Date: Age: Preferred Pharmacy Name: Address: 1. Please describe briefly the main reason you are being examined today. 2. Do you have any of the following conditions
Home Address (Street/PO Box) F M Date of Birth (mm/dd/yyyy) State Zip Code Home Phone # Scheduled Number of Work Hours per Week Work Phone #
 F M Date of Birth (mm/dd/yyyy) State Zip Code Home Phone # Scheduled Number of Work Hours per Week Work Phone #") Unum Life Insurance Company of America 2211 Congress Street Portland, Maine 04122 APPLICATION FOR GROUP CRITICAL ILLNESS INSURANCE Evidence of Insurability Application Type: New Enrollee Change to Existing
Unum Life Insurance Company of America 2211 Congress Street Portland, Maine 04122 APPLICATION FOR GROUP CRITICAL ILLNESS INSURANCE Evidence of Insurability Application Type: New Enrollee Change to Existing
CARDIA 288 MONTH FOLLOW-UP SUPPLEMENTAL FORM (FORM B) HOSPITALIZATION CASE #: INTERVIEWER ID FY288BIVID2. Page 1 of 6 FY288BH4CN
 HOSPITALIZATION CASE #: INTERVIEWER ID FY288BIVID2. Page 1 of 6 FY288BH4CN") HOSPITALIZATION CASE #: 2 8 8 0 H FY288BH4CN Has the participant indicated any of the following reasons for being admitted overnight for this case? 1. Suspected or confirmed problems with the heart, circulation,
HOSPITALIZATION CASE #: 2 8 8 0 H FY288BH4CN Has the participant indicated any of the following reasons for being admitted overnight for this case? 1. Suspected or confirmed problems with the heart, circulation,
Patient History Information
 Date: Body Technic Systems, Inc. 33790 Bainbridge Rd. Ste. 205 Solon, Ohio 44139 440-248-9255 phone 440-248-3608 fax Patient History Information Name: Date of birth: Address: City: State: Zip: Home phone:
Date: Body Technic Systems, Inc. 33790 Bainbridge Rd. Ste. 205 Solon, Ohio 44139 440-248-9255 phone 440-248-3608 fax Patient History Information Name: Date of birth: Address: City: State: Zip: Home phone:
Medicare Supplement plan application
 Medicare Supplement plan application SECTION 1 Personal information Last name First name Middle initial Social Security number - - Primary Street address City State ZIP code Mailing Street address (if
Medicare Supplement plan application SECTION 1 Personal information Last name First name Middle initial Social Security number - - Primary Street address City State ZIP code Mailing Street address (if
Income Protection. Pillar Series
 Pillar Series Income Protection La Capitale: a leader in the insurance and financial services industry La Capitale Financial Security is a member company of the La Capitale Financial Group. La Capitale
Pillar Series Income Protection La Capitale: a leader in the insurance and financial services industry La Capitale Financial Security is a member company of the La Capitale Financial Group. La Capitale
NATIONAL HEALTH FUND PRESENTATION
 NATIONAL HEALTH FUND PRESENTATION WYNDHAM KINGSTON HOTEL KINGSTON JULY 28, 2012 TOPICS FOR PRESENTATION NHF - HISTORY - BENEFITS - APPLICATION - ENROLMENT JADEP - CONDITIONS COVERED NHFCARD - CONDITIONS
NATIONAL HEALTH FUND PRESENTATION WYNDHAM KINGSTON HOTEL KINGSTON JULY 28, 2012 TOPICS FOR PRESENTATION NHF - HISTORY - BENEFITS - APPLICATION - ENROLMENT JADEP - CONDITIONS COVERED NHFCARD - CONDITIONS
Full name DOB Age Address Email Phone numbers (H) (W) (C) Emergency contact Phone
 (W) (C) Emergency contact Phone") DEMOGRAPHIC INFORMATION Full name DOB Age Address Email Phone numbers (H) (W) (C) Emergency contact Phone CARE INFORMATION Primary care physician: Address Phone Fax Referring physician: Specialty Address
DEMOGRAPHIC INFORMATION Full name DOB Age Address Email Phone numbers (H) (W) (C) Emergency contact Phone CARE INFORMATION Primary care physician: Address Phone Fax Referring physician: Specialty Address
Older Drivers Guide to Driving Safely
 Fit to Drive Traffic Safety for Older Drivers Are you fit to drive? The aging process may increase your risk of being in a traffic crash, and it affects the severity of injuries you experience. Drivers
Fit to Drive Traffic Safety for Older Drivers Are you fit to drive? The aging process may increase your risk of being in a traffic crash, and it affects the severity of injuries you experience. Drivers
A Report on the Health and Cultural Status of Alaska Native Elders
 A Report on the Health and Cultural Status of Alaska Native Elders Rosellen M. Rosich, Ph.D. Director Summer Institute 2008 1 Specific Aims of Presentation Enhance and strengthen medical students understanding
A Report on the Health and Cultural Status of Alaska Native Elders Rosellen M. Rosich, Ph.D. Director Summer Institute 2008 1 Specific Aims of Presentation Enhance and strengthen medical students understanding
How To Get A Medical Insurance Policy From Unum
 APPLICATION FOR GROUP CRITICAL ILLNESS INSURANCE Evidence of Insurability Unum Life Insurance Company of America ( Unum ) 2211 Congress Street Portland, Maine 04122 Application Type: Newly Eligible Late
APPLICATION FOR GROUP CRITICAL ILLNESS INSURANCE Evidence of Insurability Unum Life Insurance Company of America ( Unum ) 2211 Congress Street Portland, Maine 04122 Application Type: Newly Eligible Late
Healthy ageing and disease prevention: The case in South Africa and The Netherlands
 Healthy ageing and disease prevention: The case in South Africa and The Netherlands Sebastiana Kalula, 1 Ger Tielen 2 and Monica Ferreira 1 Medical advances, improved health care and prudent health behaviour
Healthy ageing and disease prevention: The case in South Africa and The Netherlands Sebastiana Kalula, 1 Ger Tielen 2 and Monica Ferreira 1 Medical advances, improved health care and prudent health behaviour
2013 Diabetes and Eye Disease Fact Sheet
 The Georgia Department of Public Health 2013 Diabetes and Eye Disease Fact Sheet Diabetes is the leading cause of new cases of blindness among United States adults. 1-3 As Georgia s population ages and
The Georgia Department of Public Health 2013 Diabetes and Eye Disease Fact Sheet Diabetes is the leading cause of new cases of blindness among United States adults. 1-3 As Georgia s population ages and
PELED PLASTIC SURGERY HEADACHE HISTORY FORM
 HEADACHE HISTORY FORM IF THIS IS YOUR FIRST VISIT, PLEASE TAKE THE TIME TO FILL THIS FORM OUT COMPLETELY. Patient Name: Age: Date of Birth: Weight: Height: Address: City: State: Zip: Home Phone: Cell Phone:
HEADACHE HISTORY FORM IF THIS IS YOUR FIRST VISIT, PLEASE TAKE THE TIME TO FILL THIS FORM OUT COMPLETELY. Patient Name: Age: Date of Birth: Weight: Height: Address: City: State: Zip: Home Phone: Cell Phone:
Home Address (Street/PO Box) F M Date of Birth (mm/dd/yyyy) State Zip Code Home Phone # Scheduled Number of Work Hours per Week Work Phone #
 F M Date of Birth (mm/dd/yyyy) State Zip Code Home Phone # Scheduled Number of Work Hours per Week Work Phone #") Unum Life Insurance Company of America 2211 Congress Street Portland, Maine 04122 APPLICATION FOR GROUP CRITICAL ILLNESS INSURANCE Evidence of Insurability Application Type: New Enrollee Change to Existing
Unum Life Insurance Company of America 2211 Congress Street Portland, Maine 04122 APPLICATION FOR GROUP CRITICAL ILLNESS INSURANCE Evidence of Insurability Application Type: New Enrollee Change to Existing
CHAPTER 17: HEALTH PROMOTION AND DISEASE MANAGEMENT
 CHAPTER 17: HEALTH PROMOTION AND DISEASE MANAGEMENT HEALTH SERVICES AND PROGRAMS The Plan s Health Promotion and Disease Management Department seeks to improve the health and overall well-being of our
CHAPTER 17: HEALTH PROMOTION AND DISEASE MANAGEMENT HEALTH SERVICES AND PROGRAMS The Plan s Health Promotion and Disease Management Department seeks to improve the health and overall well-being of our
Simple, Affordable & SAFE!
 The Insurance & Benefits Trust of PORAC Simple, Affordable & SAFE! Group Term Life Insurance Application (10-Year Level Term Rate) Group Term Life Application for 10-Year Level Term Rate Reference to Spouse
The Insurance & Benefits Trust of PORAC Simple, Affordable & SAFE! Group Term Life Insurance Application (10-Year Level Term Rate) Group Term Life Application for 10-Year Level Term Rate Reference to Spouse
Patient Case Information (Please Fill Out Forms Completely) (IF PATIENT IS UNDER 18 YEARS OF AGE LEGAL GUARDIAN MUST SIGN ALL PAPERWORK)
 (IF PATIENT IS UNDER 18 YEARS OF AGE LEGAL GUARDIAN MUST SIGN ALL PAPERWORK)") Patient Name: Patient Case Information (Please Fill Out Forms Completely) (IF PATIENT IS UNDER 18 YEARS OF AGE LEGAL GUARDIAN MUST SIGN ALL PAPERWORK) (Last), (First) (Middle Initial) Address: City: State:
Patient Name: Patient Case Information (Please Fill Out Forms Completely) (IF PATIENT IS UNDER 18 YEARS OF AGE LEGAL GUARDIAN MUST SIGN ALL PAPERWORK) (Last), (First) (Middle Initial) Address: City: State:
ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION
 Outpatient Services 2381 Lawrenceville Road 609-896-9500 voice Patient Name: Account #: ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION Your first day of outpatient
Outpatient Services 2381 Lawrenceville Road 609-896-9500 voice Patient Name: Account #: ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION Your first day of outpatient
Markle Survey: Demographics of Public and Doctors Surveyed
 Markle Survey: Demographics of Public and Doctors Surveyed January 2011 Markle Survey on Health In a Networked Life General Comparisons Between the Public and Doctors Surveyed Age : Doctors 90% 80% 70%
Markle Survey: Demographics of Public and Doctors Surveyed January 2011 Markle Survey on Health In a Networked Life General Comparisons Between the Public and Doctors Surveyed Age : Doctors 90% 80% 70%
PATIENT/PARENT/GUARDIAN SIGNATURE
 PATIENT REGISTRATION PATIENT S NAME: SEX MALE FEMALE DOB: SOCIAL SECURITY #: CITY/STATE/ZIP: PHONE # GUARANTOR INFORMATION (if responsible party is not the patient) MOTHER S NAME: DOB: SS#: CITY/STATE/ZIP:
PATIENT REGISTRATION PATIENT S NAME: SEX MALE FEMALE DOB: SOCIAL SECURITY #: CITY/STATE/ZIP: PHONE # GUARANTOR INFORMATION (if responsible party is not the patient) MOTHER S NAME: DOB: SS#: CITY/STATE/ZIP:
Patient Information. Date: Date of Birth: / / Name: Social Security: _- - Address: Street City State Zip
 Personal Insurance Intake Form Patient Information Date of Birth: / / Social Security: _- - Address: Street City State Zip Email Address: Home Phone: Sex: M or F Work Phone:. Cell Phone: Height: Weight:
Personal Insurance Intake Form Patient Information Date of Birth: / / Social Security: _- - Address: Street City State Zip Email Address: Home Phone: Sex: M or F Work Phone:. Cell Phone: Height: Weight:
CENTRAL STATES INDEMNITY CO. OF OMAHA Home Office: Omaha, NE Administration: P.O. Box 10816 Clearwater, Florida 33757-8816
 CENTRAL STATES INDEMNITY CO. OF OMAHA Home Office: Omaha, NE Administration: P.O. Box 10816 Clearwater, Florida 33757-8816 APPLICATION FOR MEDICARE SUPPLEMENT COVERAGE SECTION A. PROPOSED INSURED INFORMATION
CENTRAL STATES INDEMNITY CO. OF OMAHA Home Office: Omaha, NE Administration: P.O. Box 10816 Clearwater, Florida 33757-8816 APPLICATION FOR MEDICARE SUPPLEMENT COVERAGE SECTION A. PROPOSED INSURED INFORMATION
Medicare Supplement Application Aetna Life Insurance Company Aetna Administrator, P.O. Box 10374, Des Moines, IA 50306
 Medicare Supplement Application Aetna Administrator, P.O. Box 10374, Des Moines, IA 50306 INSTRUCTIONS: To be considered complete, all sections on this form must be filled out, unless marked optional.
Medicare Supplement Application Aetna Administrator, P.O. Box 10374, Des Moines, IA 50306 INSTRUCTIONS: To be considered complete, all sections on this form must be filled out, unless marked optional.