Code Stroke: Early Recognition and Emergency Management of the Acute Stroke Patient
|
|
|
- Randell Morrison
- 8 years ago
- Views:
Transcription
1 Code Stroke: Early Recognition and Emergency Management of the Acute Stroke Patient Ali Grubbs, RN BSN Clinical Staff Leader VUMC Adult Emergency Department

2 Vanderbilt Adult Emergency Department

3 Patient Population: STROKE STEMI SEPSIS TRAUMA BURN PHSYCH ORTHO PLASTICS OB/PEDS CLINIC/FAST TRACK GENERALIZED ILLNESS Vanderbilt Adult Emergency Department..AND THE LIST GOES ON

4
5

6

7 Narrowing the Focus How do we focus and sort through the many patients we see everyday to determine who is the most severe???

8 Rule Out Stroke Patients

9 Identification Does the patient show/express signs and symptoms of stroke? TIME LOST IS BRAIN LOST

10 A code stroke alert is activated anytime a patient with signs or symptoms of stroke/tia presents to VUMC within 8 hours of symptom onset. What Is A Code Stroke Alert?

11 CODE STROKE What is a CODE STROKE? Code Stroke activation allows members of the Code Stroke team to quickly mobilize to the E.D. so that treatment of the acute stroke patient can begin as soon as possible.

12 Prehospital Providers Air Medical (Life Flight) EMS Emergency Room Nurses Emergency Medicine Physicians Radiology/CT Technicians Paramedics Patient Care Technicians Registration Staff Neurology Neurology Physicians Neurology Nurses 6 CCT and 6 North Identification and Mobilization It takes a TEAM!

13 Identification and Mobilization Patients who present from Triage Patient is triaged by triage staff who then alerts a physician of potential rule out stroke/code stroke patients. Information gathered in triage (in relation specifically to stroke patients) includes: Chief complaint Signs and symptoms Symptom onset (last seen normal) Vital signs Bedside glucose and istat The patient is then taken directly to the CT scanner while the charge/flow nurse arranges bed placement. After the scan is complete, the pt goes to their ED room where their workup is continued.
 Vital signs Bedside glucose and istat The patient is then taken directly to the CT scanner while the charge/flow nurse arranges")
14 Identification and Mobilization Patients from prehospital providers Pt goes directly to CT Based on report, a code stroke may be called ahead of time, which enables the members of the ED as well as the code stroke team to meet in the scanner.

15 Identification and Mobilization If it is feasible and does not prolong the CT scan, an IV may be placed (if one is not already in place) and labs may be drawn during transfer and positioning of pt for scan. Although the EMS or flight crew may have already obtained a glucose, we still do an accucheck on every rule out/code stroke patient. The charge/flow nurse has already arranged an ED bed for the patient and so they go to that room after the scan is complete where their workup is continued Obtain report from the EMS provider including referring hospital records. Be sure to inquire about specifics. If the pt is actively receiving a tpa infusion, ask about the following things: Ordered dose Bolus dose (was it given, how much, when) Infusion dose (what is the dose, where is the pt in the 60 minute infusion time)

16 Continued Monitoring All patients are to remain on a portable cardiac monitor (MRX) for their entire stay in the ED. Vitals signs and Neuro checks are to be continued throughout all testing and procedures. The patient should be transported on a MRX monitor by the primary RN, float RN, or Paramedic who can continue to perform these checks and monitor vitals.

17 Even though the patient is currently in the emergency department, it is important to alert the Code Stroke team so that initial workup and decisions about treatment options can be made as quickly as possible.

18 Time Lost Is Brain Lost Remember that there is only a hour window from the time of symptom onset during which IV tpa may be considered to be administered. The window for Interventional therapy is less than or equal to eight hours from symptom onset. When obtaining information from family members, ask when was the last time the patient was seen NORMAL?

19 Emergency Department Stroke Protocol How does all of this work??? The Stroke Experts for the hospital developed a stroke protocol for the ED to help ensure that the process for acute stroke patients is smooth and streamlined

20 ED ACUTE STROKE ALGORITHM
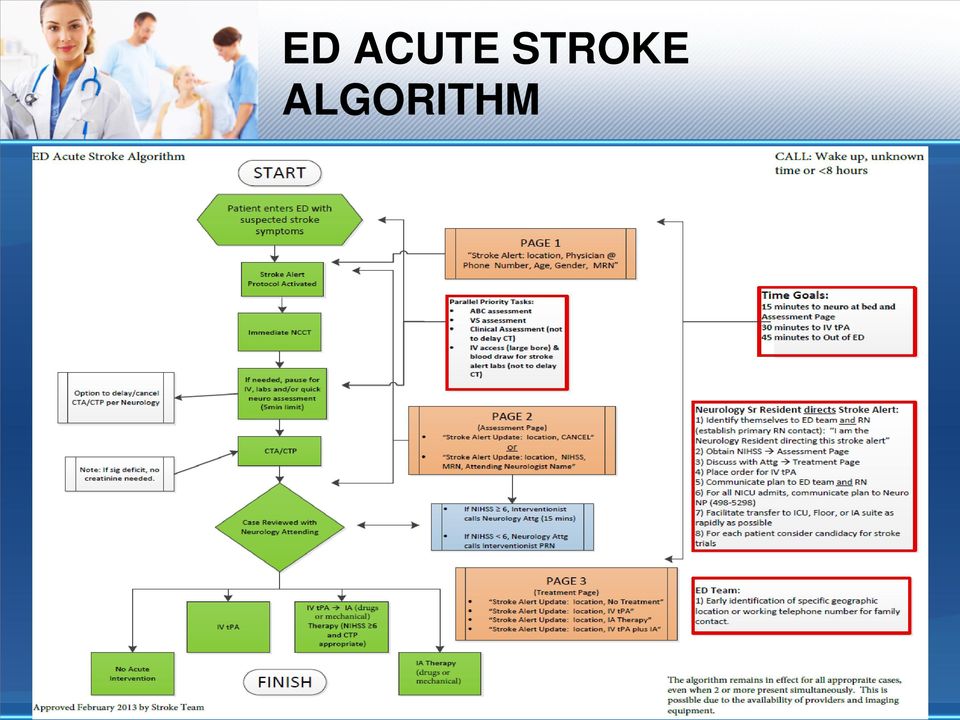
21 As a TJC Primary Stroke Center, we are given a window of 45 minutes from the time that the order is written for the initial imaging scan on an acute stroke patient (non-contrast CT head) until it is completed and interpreted and a treatment decision is made.
22 Recognize the signs and symptoms of acute stroke Assist in getting the initial imaging study completed in a timely fashion Draw the blood for the ordered lab work as quickly as possible (use the button in the room to call for assistance if you need additional help in getting blood drawn quickly) and document the time blood is drawn What Is My Role In A Code Stroke?
23 As a TJC Primary Stroke Center we are given a window of less than 45 minutes from the time that the acute stroke patient has orders entered for lab work until the initial lab work is drawn and the results are made available.
24 What Is My Role In A Code Stroke? STROKE Place the blood tubes in a biohazard bag with an purple STROKE sticker on it as this will alert the laboratory that this blood is to be run ahead of any other STAT bloodwork received at the same time Tube the biohazard bag with the blood tubes to the laboratory immediately
25 What Is My Role In A Code Stroke? ALL rule out/code stroke patients are to be kept NPO (which includes no po medications) until a swallow screening is complete!!
26 DOCUMENTATION What do you document???? EVERYTHING
27 Documentation Tool For Code Stroke ACUTE ISCHEMIC STROKE WORKSHEET >>> Adult ED Arrival (Door): Ambulatory EMS Lifeflight CodeStroke Activation by: Time of known symptom onset Triage/exam Weight (kg) O2 bnc to keep SaO2 >92%, (continuous cardiac monitor/nibp/sao2) STAT bedside glucose, if not done *NPO until swallow screen completed! IV access x2 (one IV lock, one NS.rate per MD order) STAT EKG & labs (cbc, platelet count, PT/PTT, INR, chemistries, lipid profile) **anticipate possible cardiac enzymes, tox screen, type/screen, ABGs, liver function, blood alcohol, urine pregnancy if pt of childbearing years)»»»send labs specimens in biohazard bags with STROKE label!!
28 What Is My Role In A Code Stroke? Document: What time your patient gets to their room Code stroke activation time Presenting stroke symptoms Date and time of symptom onset What time the stroke team arrives to see patient Be sure to obtain correct weight on triage form What time your patient goes to CT What time your patient returns from CT
29 Document: Time of blood draw for labs If tpa indicated, make sure you are documenting patient weight; dosage given (including bolus amount, drip amount and waste), VS & neuro status along with any adverse reactions that may occur after the infusion begins Other pertinent data i.e. intubation times, changes in condition, blood glucose, etc. What Is My Role In A Code Stroke?
30 Documentation Tool For Code Stroke This is now a permanent part of the patients chart! This is only a guide to ensure correct documentation on all code stroke patients. Scan the Code Stroke Form promptly into star panel after patient is stable or transferred to the Neuro ICU. Be sure you sign the form on both sides and that your signiture is legible. You may want to also print your name to ensure this.
31 Alteplase (tpa) Indications Alteplase (tpa) is indicated for the management of acute ischemic stroke in adults for improving neurologic recovery and reducing the incidence of disability. Treatments should only be initiated after exclusion of intracranial hemorrhage by CT-Scan or other diagnostic imaging methods sensitive for the presence of hemorrhage.
32 IV tpa: High Alert Medication IV tpa is now a high-alert medication at VUMC which means that staff should follow safety strategies and defined procedures during all steps in the medication use process in order to minimize risk. Being a High Alert medication means that IV tpa bears a heightened risk of causing significant patient harm when used in error. Administration of IV tpa as a high alert drug involves: Primary nurse verifies drug indication corresponds to patient diagnosis and appropriate monitoring has been reviewed Two licensed staff will verify the following prior to administration of IV tpa: Drug and dose based on patient weight Amount of waste Amount of bolus to be administered over one minute Amount of IV infusion via infusion pump to be administered over one hour Primary nurse will verify waste amount withdrawn from vial followed by bolus dose withdrawn from vial followed by infusion dose administered via infusion pump Primary nurse will document waste amount and name of second licensed staff member who witnessed waste, bolus dose amount and time administered and infusion dose amount and time initiated in EMR. **Review the Policy: High Alert and Look-Alike Sound-Alike Medications CL
33 Mechanism of Action Onset Clot lysis often occurs within minutes of administration Duration ½ an hour 80% cleared within 10 minutes of administration
34 Inclusion/Eligibility Criteria for tpa Administration Age 18 years of age or older (or at discretion of stroke team neurologist). Signs of a measurable neurologic deficit from an ischemic stroke on examination and/or measureable on NIHSS. Time of onset less than or equal to three hours. Currently, the FDA has approved the use of IV tpa for patients up to three hours after stroke symptom onset. The ECASE III trial results released in the Spring of 2009 showed comparable outcomes when IV tpa was given in the extended hour window with some additional contraindications noted. We do administer IV tpa in the extended time window at VUMC when applicable or appropriate. Baseline CT scan with no evidence of Intracranial Hemorrhage.
35 Exclusion/Contraindications Criteria for IV tpa Evidence of intracranial hemorrhage on pretreatment CTscan. Minor or rapidly improving symptoms (treatment considered at the discretion of the stroke team neurologist) Clinical Presentation suggestive of subarachnoid hemorrhage. Known AVM or aneurysm. Post myocardial infarction or pericarditis. Another stroke, intracranial surgery or serious head trauma within the preceding three months. Delay in patient arrival (> 4.5 hours from symptom onset).
36 Exclusion/Contraindications Criteria for IV tpa Age less than 18 years old (treatment considered at the discretion of the stroke team neurologist). Seizure at onset. Major surgery within 14 days. History of intracranial hemorrhage. Active internal bleeding. Patients taking anticoagulants or who have received heparin within the 48 hours preceding the onset of stroke and have an elevated ptt. PT >15 seconds. Platelet Count <100,000 per cubic millimeter.
37 Exclusion/Contraindications Criteria for IV tpa HTN: SBP >185mmHg or DBP >110mmHg on repeated measurements at time of treatment (not responsive to antihypertensive medications). Abnormal blood glucose level (<50mg / deciliter or >400mg / deciliter). History of GI or Urinary Tract hemorrhage within 21 days Arterial pressure puncture at non-compressible site within the previous 7 days. Recent Lumbar Puncture. Inclusion/Exclusion Criteria based upon tpa Stroke Study Group Guidelines Disclaimer: This acute Stroke Algorithm is meant to serve as a guide only. It is not reflective of all treatment options for all patients. Ultimate treatment decisions are at the discretion of the treating physician.
38 IV tpa IV tpa is only administered by the M.D. or R.N. In the ED, tpa is available in the accudose refrigerator. In the rest of the hospital, tpa is mixed in the pharmacy and brought to the bedside.
39 tpa Dosing and Administration tpa Dosing Formula 0.9mg x (patient weight in kg) = mg total tpa dose It is very important to remember that the max dose for any patient is 90 mg. Administration tpa is stored in the refrigerator. Reconstitute per directions. Do not shake vials, gently roll them to mix the powder with the sterile saline. Important Note: A 10mg waste should be removed prior to administration of bolus or infusion. 10% of the calculated dose is given as a bolus over 1 minute. The remaining 90% is to be administered over 60 minutes. IV administration only!! tpa must be ordered by an Attending Physician. Double check for correct dose (MD, RN) Document bolus dose and infusion amount with another RN, MD witness.
40 tpa Calculations The Patient weight is 121 lbs. Calculate the bolus and infusion dose.
41 Answer 0.9 mg x 55 kg = 49.5 mg total tpa dose for this patient mg is the bolus dose mg is the infusion dose
42 tpa Calculations The Patient weight is 92 kg. Calculate the bolus and infusion dose.
43 Answer 0.9 mg x 92 kg = 82.8 mg total tpa dose for this patient mg is the bolus dose mg is the infusion dose
44 tpa Calculations The Patient weight is 242 lbs. Calculate the bolus and infusion dose.
45 Answer 0.9 mg x 110 kg = 99 mg total tpa dose for this patient. IMPORTANT NOTE: 90 mg is the max dose for any patient!! Recalculate the dose based on this information. 9 mg is the bolus dose 81 mg is the infusion dose
46 tpa Calculations How much do you waste from each bottle of tpa at least? A minimum of 10 mg must be wasted for every patient!
47 tpa Calculations What is the MAX dose for any given patient regardless of waste? 90 mg is the MAX dose for every patient!
48 tpa Calculations Over what time period do you administer a bolus? A bolus is administered over 1 minute An infusion? An infusion is administered over 60 minutes
49 During and After IV tpa Treatment Monitor B/P for the first 24 hours after starting treatment: *Every 15 minutes for 2 hours after starting the infusion *Every 30 minutes for 6 hours *Every hour for 16 hours Monitor Neurologic status every 30 min x4 Watch for bleeding puncture sites, urine, stool etc. Know signs/symptoms of Intracerebral Hemorrhage: Any acute neurological deterioration, new HA, N/V, sudden HTN Foley catheter must be placed with order in WIZ PRIOR to IV tpa infusion/bolus, otherwise avoid placement for hours post IV tpa infusion.
50 During and After IV tpa Treatment Who spends more time at the patient s bedside?? YOU DO!! Know the complications and adverse reactions to IV tpa.
51 During and After IV tpa Treatment Post tpa Infusion: Continue to monitor for signs/symptoms of intracerebral hemorrhage or other types of hemorrhage No unnecessary blood draws or invasive procedures for 12 hours after tpa No aspirin, heparin, warfarin, or other antithrombotic or antiplatelet drugs 24 hours after tpa Observe for other adverse reactions to tpa such as: cerebral edema, cerebral herniation, seizure, new ischemic stroke. These events may be life threatening and may lead to death.
52 During and After IV tpa Treatment If Hemorrhage is suspected: STOP TPA INFUSION Call MD immediately Be prepared to transport the patient to CT for a STAT head CT without contrast Be prepared to draw blood for PT, PTT, platelet count, fibrinogen, type and hold, other lab work as ordered Be prepared to administer cryo and/or platelets as ordered
53 When the tpa is complete, hang a 50 ml bag of NS to flush the remainder of the tpa through the line to be sure the patient receives the entire drug amount prescribed. Post tpa infusion
54 Documentation During and After tpa IV Treatment In the ED, remember to use the green Acute Code Stroke Documentation Checklist to assure accurate documentation of times and completion of required tasks Obtain/document vital signs/neuro checks as indicated on Acute Code Stroke worksheet Be sure to inform nurse in the Neurosciences ICU where you are with post-tpa vital signs frequency during your SBAR report at transfer Important: The Green Code Stroke Documentation Tool IS a permanent chart document. Complete it and place in Jacki Ashburn s box located at the charge nurse desk.
55 Stroke Box The Stroke Box is located in T2. It is important to restock the box after every use replacing the items that were used. A list of the enclosed contents is located inside the box. After each use, return the box promptly to T2. A new lock must be placed on the box and logged into the log book.
56 Stroke Box Contents IV insertion tools (IV catheter and line setup equipment). Blood tubes, vacutainers and empty 10cc syringes for drawing blood while in CT-scan. Code Stroke Worksheets (more worksheets are located at the charge nurse desk if needed). IV tpa administration information. Stroke scale assessment tools. Educational pamphlets for patients and family members. IV phenylephrine and IV labatelol with dosing drip calculations. IV tubing and NS for mixing drips. Purple STROKE stickers. Calculator, pen lights and extra locks located in the lid.
57 Patient and Family Education Stroke Awareness Education for patients and family members includes: Recognizing the signs and symptoms of stroke and to activate the 911 system. Teaching patients and families about correcting those risk factors that can be modified and accepting those that cannot.
58 Modifiable Risk Factors
59 Non-Modifiable Risk Factors
60 What is a CODE STROKE? Important Times to Remember: Door to CT Scan: 15 minutes Door to Decision (MD): 45 minutes Door to Treatment (tpa): 60 minutes Order for tpa to Administration (Nurse): 15 minutes Order to Lab Results: 45 minutes
61 ATYPICAL PRESENTATIONS
62
63 For More Information Visit The Vanderbilt Stroke Center Website for educational opportunities, events in the community and clinical research in the field of Neurosciences. OR
64 References American Heart Association (2003). Know the signs of stroke educational pamphlet
65 QUESTIONS?
Acute Myocardial Infarction (the formulary thrombolytic for AMI at AAMC is TNK, please see the TNK monograph in this manual for information)
") ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
Level III Stroke Center Data Collection Requirements
 Who? Level III Stroke Center Data Collection Requirements All LERN Level III Stroke Centers. LERN Level I and II Stroke Centers have reporting requirements to The Joint Commission or other Board approved
Who? Level III Stroke Center Data Collection Requirements All LERN Level III Stroke Centers. LERN Level I and II Stroke Centers have reporting requirements to The Joint Commission or other Board approved
EMS Management of Stroke. Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D.
 EMS Management of Stroke Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D. Financial Disclosure: No relevant financial relationship exists Working Together to End Stroke Formed in 2013 Identified
EMS Management of Stroke Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D. Financial Disclosure: No relevant financial relationship exists Working Together to End Stroke Formed in 2013 Identified
TPA, STROKE, & TELEMEDICINE. Improving utilization and improving outcomes in a constantly evolving field
 TPA, STROKE, & TELEMEDICINE Improving utilization and improving outcomes in a constantly evolving field OVERVIEW tpa inclusion and exclusion evolution Challenges to tpa administration Target:Stroke Telemedicine
TPA, STROKE, & TELEMEDICINE Improving utilization and improving outcomes in a constantly evolving field OVERVIEW tpa inclusion and exclusion evolution Challenges to tpa administration Target:Stroke Telemedicine
Stroke Reperfusion Therapy: IV t-pa Treatment Phase
 Stroke Reperfusion Therapy: IV t-pa Treatment Phase IV tpa Administration for Adult Patients Arriving Within 3 Hours. Page Contents Consent Form Indications for IV tpa Contraindications Warnings t-pa Dosing
Stroke Reperfusion Therapy: IV t-pa Treatment Phase IV tpa Administration for Adult Patients Arriving Within 3 Hours. Page Contents Consent Form Indications for IV tpa Contraindications Warnings t-pa Dosing
TIME LOST IS BRAIN LOST. TARGET: STROKE CAMPAIGN MANUAL
 TIME LOST IS BRAIN LOST. TARGET: STROKE CAMPAIGN MANUAL 2010, American Heart Association TARGET: STROKE CAMPAIGN MANUAL 01 INTRODUCTION Welcome to the Target: Stroke. The purpose of this manual is to provide
TIME LOST IS BRAIN LOST. TARGET: STROKE CAMPAIGN MANUAL 2010, American Heart Association TARGET: STROKE CAMPAIGN MANUAL 01 INTRODUCTION Welcome to the Target: Stroke. The purpose of this manual is to provide
Direct-to-CT. QuICR Webinar November 4 2015
 Direct-to-CT QuICR Webinar November 4 2015 Our ER Camrose offers 24 hour Emergency Room Care to our community We serve an approximate city/county population of 26,000 people Our ER visits totaled 17,931
Direct-to-CT QuICR Webinar November 4 2015 Our ER Camrose offers 24 hour Emergency Room Care to our community We serve an approximate city/county population of 26,000 people Our ER visits totaled 17,931
Stroke/VTE Quality Measure Build for Meaningful Use Stage 1
 Stroke/VTE Quality Measure Build for Meaningful Use Stage 1 Presented by Susan Haviland, BSN RN Senior Consult, Santa Rosa Consulting Meaningful Use Quality Measures Centers for Medicare and Medicaid Services
Stroke/VTE Quality Measure Build for Meaningful Use Stage 1 Presented by Susan Haviland, BSN RN Senior Consult, Santa Rosa Consulting Meaningful Use Quality Measures Centers for Medicare and Medicaid Services
Planning: Patient Goals and Expected Outcomes The patient will: Remain free of unusual bleeding Maintain effective tissue perfusion Implementation
 Obtain complete heath history including allergies, drug history and possible drug Assess baseline coagulation studies and CBC Assess for history of bleeding disorders, GI bleeding, cerebral bleed, recent
Obtain complete heath history including allergies, drug history and possible drug Assess baseline coagulation studies and CBC Assess for history of bleeding disorders, GI bleeding, cerebral bleed, recent
A Collaborative Effort to Improve Emergency Stroke Care: Mobile Stroke Unit
 A Collaborative Effort to Improve Emergency Stroke Care: Mobile Stroke Unit What can we do to cut down the time it takes to give a clot dissolving drug (tpa)? MOBILE STROKE UNIT! Mobile Stroke Unit Mobile
A Collaborative Effort to Improve Emergency Stroke Care: Mobile Stroke Unit What can we do to cut down the time it takes to give a clot dissolving drug (tpa)? MOBILE STROKE UNIT! Mobile Stroke Unit Mobile
Developing a Dynamic Team Approach to Stroke Care. Emergency Medical Services 2015
 Developing a Dynamic Team Approach to Stroke Care Emergency Medical Services 2015 Why Stroke, Why now? A recent study showed that 80 percent of people in the United States live within an hour s drive of
Developing a Dynamic Team Approach to Stroke Care Emergency Medical Services 2015 Why Stroke, Why now? A recent study showed that 80 percent of people in the United States live within an hour s drive of
Stroke Systems of Care
 Stroke Systems of Care Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA Stroke chain of survival
Stroke Systems of Care Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA Stroke chain of survival
Inpatient Anticoagulation Safety. To provide safe and effective anticoagulation therapy through a collaborative approach.
 Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
STATEMENT OF STANDARD
 OHSU HEALTH CARE SYSTEM PRACTICE STANDARD Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11
OHSU HEALTH CARE SYSTEM PRACTICE STANDARD Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11
SUFFOLK COUNTY COMMUNITY COLLEGE NURSING DEPARTMENT MEDICATION ADMINISTRATION TEST NR 40 Practice test questions READ INSTRUCTIONS CAREFULLY
 NR40 MEDICATION MATH TEST Practice questions page 1 SUFFOLK COUNTY COMMUNITY COLLEGE NURSING DEPARTMENT MEDICATION ADMINISTRATION TEST NR 40 Practice test questions READ INSTRUCTIONS CAREFULLY Students
NR40 MEDICATION MATH TEST Practice questions page 1 SUFFOLK COUNTY COMMUNITY COLLEGE NURSING DEPARTMENT MEDICATION ADMINISTRATION TEST NR 40 Practice test questions READ INSTRUCTIONS CAREFULLY Students
Building an Emergency Response to Acute Stroke
 Great Lakes Stroke Network August 2006 Building an Emergency Response to Acute Stroke Wende N. Fedder RN, BSN, MBA Director, Stroke & Neurovascular Services Alexian Brothers Hospital Network Elk Grove
Great Lakes Stroke Network August 2006 Building an Emergency Response to Acute Stroke Wende N. Fedder RN, BSN, MBA Director, Stroke & Neurovascular Services Alexian Brothers Hospital Network Elk Grove
How To Help A Stroke Patient
 Rishi Gupta, MD Susan Zimmermann, RN, BSN, CNRN Kerrin Connelly, RN, MSN, MPH Cheri Kommor, RN, CEN, CFRN, NREMT-P Rishi Gupta FINANCIAL DISCLOSURE: Consultant: Stryker Neurovascular, Covidien DSMB: Rapid
Rishi Gupta, MD Susan Zimmermann, RN, BSN, CNRN Kerrin Connelly, RN, MSN, MPH Cheri Kommor, RN, CEN, CFRN, NREMT-P Rishi Gupta FINANCIAL DISCLOSURE: Consultant: Stryker Neurovascular, Covidien DSMB: Rapid
SCRN Medication Review. Susan M. Gaunt MS APRN ACNS-BC CCRN CNRN Gwinnett Medical Center
 SCRN Medication Review Susan M. Gaunt MS APRN ACNS-BC CCRN CNRN Gwinnett Medical Center Objectives To explain the indications, contraindications, interaction, timing, dosing, side effects of: Thrombolytics
SCRN Medication Review Susan M. Gaunt MS APRN ACNS-BC CCRN CNRN Gwinnett Medical Center Objectives To explain the indications, contraindications, interaction, timing, dosing, side effects of: Thrombolytics
Acute Ischemic Stroke with tpa
 Admission/Condition/Diagnosis Admission: Admitting Physician Attending Physician Assign to Inpatient Status Transfer to Level of Care: Physician MUST document in notes the risk, severity, and skilled nursing
Admission/Condition/Diagnosis Admission: Admitting Physician Attending Physician Assign to Inpatient Status Transfer to Level of Care: Physician MUST document in notes the risk, severity, and skilled nursing
PROTOCOL TITLE: Ambulatory Initiation and Management of Warfarin for Adults
 PROTOCOL NUMBER: 7 PROTOCOL TITLE: Ambulatory Initiation and Management of Warfarin for Adults THIS PROTOCOL APPLIES TO: UW Health Clinics: all adult outpatients with an active order for warfarin TARGET
PROTOCOL NUMBER: 7 PROTOCOL TITLE: Ambulatory Initiation and Management of Warfarin for Adults THIS PROTOCOL APPLIES TO: UW Health Clinics: all adult outpatients with an active order for warfarin TARGET
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
Ischemic Stroke Clinical Pathway
 Ischemic Stroke Clinical Pathway Legal Treatments Advance Directives Refer to the ED Stroke Algorithm Patient exam: review history, Check VS/Neuro every 2 hour or per M.D. order Strict I & O s Cardiac
Ischemic Stroke Clinical Pathway Legal Treatments Advance Directives Refer to the ED Stroke Algorithm Patient exam: review history, Check VS/Neuro every 2 hour or per M.D. order Strict I & O s Cardiac
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 MED Hospitalist Stroke-TIA Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24 hours then Up ad lib Up Ad Lib
MED Hospitalist Stroke-TIA Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24 hours then Up ad lib Up Ad Lib
UPDATED INCLUSION AND EXCLUSION CRITERIA FOR IV TPA ADMINISTRATION ACUTE STROKE TREATMENT: AN UPDATE GOALS OF TALK
 ACUTE STROKE TREATMENT: AN UPDATE James M. Gebel MD MS FAHA Medical Director Akron General Medical Center Cerebrovascular Center GOALS OF TALK Review changes to IV tpa administration as per new 2013 AHA
ACUTE STROKE TREATMENT: AN UPDATE James M. Gebel MD MS FAHA Medical Director Akron General Medical Center Cerebrovascular Center GOALS OF TALK Review changes to IV tpa administration as per new 2013 AHA
Dabigatran (Pradaxa) Guidelines
 Guidelines") Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
S9 Administer thrombolytic treatment in acute ischaemic stroke
 S9 Administer thrombolytic treatment in acute ischaemic Screening and initiating treatment, overseeing competency of treatment About this workforce competence This competence is about the emergency administration
S9 Administer thrombolytic treatment in acute ischaemic Screening and initiating treatment, overseeing competency of treatment About this workforce competence This competence is about the emergency administration
Medications or therapeutic solutions may be injected directly into the bloodstream
 Intravenous Therapy Medications or therapeutic solutions may be injected directly into the bloodstream for immediate circulation and use by the body. State practice acts designate which health care professionals
Intravenous Therapy Medications or therapeutic solutions may be injected directly into the bloodstream for immediate circulation and use by the body. State practice acts designate which health care professionals
A Patient s Guide to Primary and Secondary Prevention of Cardiovascular Disease Using Blood-Thinning (Anticoagulant) Drugs
 Drugs") A Patient s Guide to Primary and Secondary Prevention of PATIENT EDUCATION GUIDE What Is Cardiovascular Disease? Cardiovascular disease (CVD) is a broad term that covers any disease of the heart and circulatory
A Patient s Guide to Primary and Secondary Prevention of PATIENT EDUCATION GUIDE What Is Cardiovascular Disease? Cardiovascular disease (CVD) is a broad term that covers any disease of the heart and circulatory
Approved: Acute Stroke Ready Hospital Advanced Certification Program
 Approved: Acute Stroke Ready Hospital Advanced Certification Program The Joint Commission recently developed a new Disease- Specific Care Advanced Certification program for Acute Stroke Ready Hospitals
Approved: Acute Stroke Ready Hospital Advanced Certification Program The Joint Commission recently developed a new Disease- Specific Care Advanced Certification program for Acute Stroke Ready Hospitals
THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT
 THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT Stroke Prevention in Atrial Fibrillation Gregory Albers, M.D. Director Stanford Stroke Center Professor of Neurology and Neurological
THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT Stroke Prevention in Atrial Fibrillation Gregory Albers, M.D. Director Stanford Stroke Center Professor of Neurology and Neurological
Documentation Guidelines for Physicians Interventional Pain Services
 Documentation Guidelines for Physicians Interventional Pain Services Pamela Gibson, CPC Assistant Director, VMG Coding Anesthesia and Surgical Divisions 343.8791 1 General Principles of Medical Record
Documentation Guidelines for Physicians Interventional Pain Services Pamela Gibson, CPC Assistant Director, VMG Coding Anesthesia and Surgical Divisions 343.8791 1 General Principles of Medical Record
REGIONAL SUSPECTED STROKE PROTOCOL
 1. Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed. Strokes should be treated emergently. During a stroke, up to 2 million
1. Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed. Strokes should be treated emergently. During a stroke, up to 2 million
The Clinical Evaluation of the Comatose Patient in the Emergency Department
 The Clinical Evaluation of the Comatose Patient in the Emergency Department patients with altered mental status (AMS) and coma. treat patients who present to the Emergency Department with altered mental
The Clinical Evaluation of the Comatose Patient in the Emergency Department patients with altered mental status (AMS) and coma. treat patients who present to the Emergency Department with altered mental
Therapeutic Management Options for. Acute Ischemic Stroke Anna Rosenbaum, MD
 Therapeutic Management Options for Acute Ischemic Stroke Anna Rosenbaum, MD Epidemiology Epidemiology 4 th leading cause of death in the United States 1 Leading cause of disability Increase in projected
Therapeutic Management Options for Acute Ischemic Stroke Anna Rosenbaum, MD Epidemiology Epidemiology 4 th leading cause of death in the United States 1 Leading cause of disability Increase in projected
Central Line Blood Draw
 Central Line Blood Draw Welcome to the Central Line dressing blood draw refresher. Please use the navigation below to advance to the next page. The Central Line blood draw module is also available as a
Central Line Blood Draw Welcome to the Central Line dressing blood draw refresher. Please use the navigation below to advance to the next page. The Central Line blood draw module is also available as a
An Infusion of Quality and Safety STAT!
 Quality is not an act, it is a habit. Aristotle An Infusion of Quality and Safety STAT! Quality is not an act, it is a habit. Mary Kakenmaster MSN, RN, CNE Oakton Community College mkakenma@oakton.edu
Quality is not an act, it is a habit. Aristotle An Infusion of Quality and Safety STAT! Quality is not an act, it is a habit. Mary Kakenmaster MSN, RN, CNE Oakton Community College mkakenma@oakton.edu
Stroke Transfers. Downstate Receiving Hospital Perspective
 Stroke Transfers Downstate Receiving Hospital Perspective Jeffrey M. Katz, MD Director, North Shore University Hospital Stroke Center Assistant Professor of Neurology, Hofstra North Shore-LIJ School of
Stroke Transfers Downstate Receiving Hospital Perspective Jeffrey M. Katz, MD Director, North Shore University Hospital Stroke Center Assistant Professor of Neurology, Hofstra North Shore-LIJ School of
UMHS In-Patient Acute Ischemic Stroke Treatment Guidelines*
 Page 1 UMHS In-Patient Acute Ischemic Stroke Treatment Guidelines* Table of Contents 1) Physician Acute Stroke Checklist 2-3 2) Nursing Orders for Initial Evaluation of Patients with Acute Stroke 3) tpa
Page 1 UMHS In-Patient Acute Ischemic Stroke Treatment Guidelines* Table of Contents 1) Physician Acute Stroke Checklist 2-3 2) Nursing Orders for Initial Evaluation of Patients with Acute Stroke 3) tpa
CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014
 CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014 e 55 0495 2 Emergency Department (ED)- 1 Emergency Department Throughput Median time from
CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014 e 55 0495 2 Emergency Department (ED)- 1 Emergency Department Throughput Median time from
Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins)
 SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins)") Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins) I HEAR YA KNOCKING BUT YOU CAN T COME IN (electrolytes) TAKE MY BREATH AWAY (Opiates-morphine) OUT WITH
Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins) I HEAR YA KNOCKING BUT YOU CAN T COME IN (electrolytes) TAKE MY BREATH AWAY (Opiates-morphine) OUT WITH
Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations
 for stroke prevention in atrial fibrillation Special situations") Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations Dardo E. Ferrara MD Cardiac Electrophysiology North Cascade Cardiology PeaceHealth Medical Group Which anticoagulant
Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations Dardo E. Ferrara MD Cardiac Electrophysiology North Cascade Cardiology PeaceHealth Medical Group Which anticoagulant
Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I
 Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I Page # 1 Instructions for students: Case study # 1 For this lab, you are planning to provide care to the following client: CB
Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I Page # 1 Instructions for students: Case study # 1 For this lab, you are planning to provide care to the following client: CB
9/5/14. Objectives. Atrial Fibrillation (AF)
") Novel Anticoagulation for Prevention of Stroke in Patients with Atrial Fibrillation Objectives 1. Review current evidence on use of warfarin in individuals with atrial fibrillation 2. Compare the three
Novel Anticoagulation for Prevention of Stroke in Patients with Atrial Fibrillation Objectives 1. Review current evidence on use of warfarin in individuals with atrial fibrillation 2. Compare the three
Guidelines and Protocols
 TITLE: HEAD TRAUMA PURPOSE: To provide guidelines for rapid, accurate assessment of the head and intracranial structures for traumatic injury and to plan and implement appropriate interventions for identified
TITLE: HEAD TRAUMA PURPOSE: To provide guidelines for rapid, accurate assessment of the head and intracranial structures for traumatic injury and to plan and implement appropriate interventions for identified
Inter-facility Patient Transfers
 Date: September 2004 Page 1 of 6 Inter-facility Patient Transfers Purpose: The purpose of this policy is to establish a uniform procedure for inter-facility transfers. 1. Responsibility: a. Patient transfer
Date: September 2004 Page 1 of 6 Inter-facility Patient Transfers Purpose: The purpose of this policy is to establish a uniform procedure for inter-facility transfers. 1. Responsibility: a. Patient transfer
South Denver Prehospital Services 2014
 South Denver Prehospital Services 2014 Overview of 2014 BACKBOARD EMS PATIENT OUTCOMES EMS Pain management MED RECONCILIATION Attention! BACKBOARD DRILL!! BEFORE AND AFTER PROTOCOL CHANGE Measure: Injury:
South Denver Prehospital Services 2014 Overview of 2014 BACKBOARD EMS PATIENT OUTCOMES EMS Pain management MED RECONCILIATION Attention! BACKBOARD DRILL!! BEFORE AND AFTER PROTOCOL CHANGE Measure: Injury:
Making the Case for CPG s Jean Luciano, MSN, RN, CNRN, SCRN, CRNP, FAHA Claranne Mathiesen, MSN, RN, CNRN, SCRN, FAHA
 Making the Case for CPG s Jean Luciano, MSN, RN, CNRN, SCRN, CRNP, FAHA Claranne Mathiesen, MSN, RN, CNRN, SCRN, FAHA Disclosures Jeanie Luciano Genentech speakers bureau Claranne Mathiesen - none 1 Objective
Making the Case for CPG s Jean Luciano, MSN, RN, CNRN, SCRN, CRNP, FAHA Claranne Mathiesen, MSN, RN, CNRN, SCRN, FAHA Disclosures Jeanie Luciano Genentech speakers bureau Claranne Mathiesen - none 1 Objective
Appendix L: HQO Year 1 Implementation Priorities
 Appendix L: HQO Year 1 Implementation Priorities Chronic Obstructive Pulmonary Disease (Source: COPD Chairs) Non-Invasive Positive Pressure Ventilation Early Ambulation If possible, seek patient preferences
Appendix L: HQO Year 1 Implementation Priorities Chronic Obstructive Pulmonary Disease (Source: COPD Chairs) Non-Invasive Positive Pressure Ventilation Early Ambulation If possible, seek patient preferences
convey the clinical quality measure's title, number, owner/developer and contact
 CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
Improving PCI Benchmark times in a Non-PCI World
 Improving PCI Benchmark times in a Non-PCI World May 2011 St David s Georgetown Hospital, Georgetown Texas Margaret Connors BSN, RN, CEN Kirk Sinclair BSN, RN, CEN National Processes/ Mission LifeLine
Improving PCI Benchmark times in a Non-PCI World May 2011 St David s Georgetown Hospital, Georgetown Texas Margaret Connors BSN, RN, CEN Kirk Sinclair BSN, RN, CEN National Processes/ Mission LifeLine
REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY QEH/HH PCH KCMH Souris Western Stewart Memorial O'Leary PATIENT ID INCLUSION CRITERIA* All patients admitted to hosptial with a suspected diagnosis of acute ischemic stroke
ACUTE STROKE CLINICAL PATHWAY QEH/HH PCH KCMH Souris Western Stewart Memorial O'Leary PATIENT ID INCLUSION CRITERIA* All patients admitted to hosptial with a suspected diagnosis of acute ischemic stroke
Protocol: Initial Evaluation and Management of Patients with Ischemic or Hemorrhagic Stroke
 PAGE NO. 1 of 6 Original Date of Issue: 7/12/05 Patient Population Neonate Pediatric Reviewed: 2.7.07 1.20.08 3.09 1.10 Adolescent Revised: NA Yes No Yes Adult Geriatric Protocol: Initial Evaluation and
PAGE NO. 1 of 6 Original Date of Issue: 7/12/05 Patient Population Neonate Pediatric Reviewed: 2.7.07 1.20.08 3.09 1.10 Adolescent Revised: NA Yes No Yes Adult Geriatric Protocol: Initial Evaluation and
ORAL ANTICOAGULANTS - RIVAROXABAN (XARELTO) FOR ATRIAL FIBRILLATION
 FOR ATRIAL FIBRILLATION") ORAL ANTICOAGULANTS - RIVAROXABAN (XARELTO) FOR ATRIAL FIBRILLATION Information Leaflet Your Health. Our Priority. Page 2 of 6 What Are Anticoagulants And What Do They Do? This information leaflet has
ORAL ANTICOAGULANTS - RIVAROXABAN (XARELTO) FOR ATRIAL FIBRILLATION Information Leaflet Your Health. Our Priority. Page 2 of 6 What Are Anticoagulants And What Do They Do? This information leaflet has
Duration of Dual Antiplatelet Therapy After Coronary Stenting
 Duration of Dual Antiplatelet Therapy After Coronary Stenting C. DEAN KATSAMAKIS, DO, FACC, FSCAI INTERVENTIONAL CARDIOLOGIST ADVOCATE LUTHERAN GENERAL HOSPITAL INTRODUCTION Coronary artery stents are
Duration of Dual Antiplatelet Therapy After Coronary Stenting C. DEAN KATSAMAKIS, DO, FACC, FSCAI INTERVENTIONAL CARDIOLOGIST ADVOCATE LUTHERAN GENERAL HOSPITAL INTRODUCTION Coronary artery stents are
STROKE PREVENTION AND TREATMENT MARK FISHER, MD PROFESSOR OF NEUROLOGY UC IRVINE
 STROKE PREVENTION AND TREATMENT MARK FISHER, MD PROFESSOR OF NEUROLOGY UC IRVINE CASE REPORT: ACUTE STROKE MANAGEMENT 90 YEAR OLD WOMAN, PREVIOUSLY ACTIVE AND INDEPENDENT, CHRONIC ATRIAL FIBRILLATION,
STROKE PREVENTION AND TREATMENT MARK FISHER, MD PROFESSOR OF NEUROLOGY UC IRVINE CASE REPORT: ACUTE STROKE MANAGEMENT 90 YEAR OLD WOMAN, PREVIOUSLY ACTIVE AND INDEPENDENT, CHRONIC ATRIAL FIBRILLATION,
Stroke Care First week
 Stroke Care First week Florence Nightingale (1820 1910) Stroke Unit Dedicated personnel trained in stroke management Stepwise guidelines supported by explicit checklists Continuous monitoring available
Stroke Care First week Florence Nightingale (1820 1910) Stroke Unit Dedicated personnel trained in stroke management Stepwise guidelines supported by explicit checklists Continuous monitoring available
New Treatments for Stroke Prevention in Atrial Fibrillation. John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013
 New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
4/24/2015. Urgent, STAT, Super STAT, ASAP! Achieving timely lab testing for the Emergency Department. Learning Objectives.
 Urgent, STAT, Super STAT, ASAP! Achieving timely lab testing for the Emergency Department Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning Objectives Describe
Urgent, STAT, Super STAT, ASAP! Achieving timely lab testing for the Emergency Department Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning Objectives Describe
INR: RUPTURED ANEURYSM: POST EMBOLIZATION Patient Identification Page 1 of 5. Allergies: Weight: kg Diagnosis:
 Page 1 of 5 Allergies: Weight: kg Diagnosis: Service: Admission Admit to Inpatient Admit to Daypatient Place on Outpatient Observation Status Hospital Attending: Attending Physician Attending Provider:
Page 1 of 5 Allergies: Weight: kg Diagnosis: Service: Admission Admit to Inpatient Admit to Daypatient Place on Outpatient Observation Status Hospital Attending: Attending Physician Attending Provider:
Adverse Events in Clinical Trials: Definitions and Documentation
 Clinical and Translational Science Institute / CTSI at the University of California, San Francisco Welcome to Online Training for Clinical Research Coordinators Adverse Events in Clinical Trials: Definitions
Clinical and Translational Science Institute / CTSI at the University of California, San Francisco Welcome to Online Training for Clinical Research Coordinators Adverse Events in Clinical Trials: Definitions
Emerging therapies for Intracerebral Hemorrhage
 Emerging therapies for Intracerebral Hemorrhage Chitra Venkat, MBBS, MD, MSc. Associate Professor of Neurology and Neurological Sciences Stroke and Neurocritical Care. Stanford University Learning objectives
Emerging therapies for Intracerebral Hemorrhage Chitra Venkat, MBBS, MD, MSc. Associate Professor of Neurology and Neurological Sciences Stroke and Neurocritical Care. Stanford University Learning objectives
A Patient s Guide to Antithrombotic Therapy in Atrial Fibrillation
 Patient s Guide to Antithrombotic Therapy in Atrial Fibrillation A Patient s Guide to Antithrombotic Therapy in Atrial Fibrillation PATIENT EDUCATION GUIDE What is atrial fibrillation? Atrial fibrillation
Patient s Guide to Antithrombotic Therapy in Atrial Fibrillation A Patient s Guide to Antithrombotic Therapy in Atrial Fibrillation PATIENT EDUCATION GUIDE What is atrial fibrillation? Atrial fibrillation
University of Pennsylvania RESEARCH Subject Informed Consent Form AND RESEARCH SUBJECT HIPAA AUTHORIZATION
 University of Pennsylvania RESEARCH Subject Informed Consent Form AND RESEARCH SUBJECT HIPAA AUTHORIZATION Protocol Title: Evaluating the impact of cocaine use and HIV infection in arterial wall inflammation
University of Pennsylvania RESEARCH Subject Informed Consent Form AND RESEARCH SUBJECT HIPAA AUTHORIZATION Protocol Title: Evaluating the impact of cocaine use and HIV infection in arterial wall inflammation
Care of Gastrostomy Tubes for Adults with IDD in Community Settings: The Nurse s Role. Lillian Khalil, BSN, RN Volunteers of America, Chesapeake
 Care of Gastrostomy Tubes for Adults with IDD in Community Settings: The Nurse s Role Lillian Khalil, BSN, RN Volunteers of America, Chesapeake Objectives The participants will be able to identify the
Care of Gastrostomy Tubes for Adults with IDD in Community Settings: The Nurse s Role Lillian Khalil, BSN, RN Volunteers of America, Chesapeake Objectives The participants will be able to identify the
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Building a Plan for Process Improvement
 Building a Plan for Process Improvement (Rapid Fire PI Workshop) Lynn Hundley MSN,APRN,CNRN,CCNS,ANVP Melissa Richardson MSN,RN,SCRN Questions Does your organization have legacy problems that go unresolved?
Building a Plan for Process Improvement (Rapid Fire PI Workshop) Lynn Hundley MSN,APRN,CNRN,CCNS,ANVP Melissa Richardson MSN,RN,SCRN Questions Does your organization have legacy problems that go unresolved?
ALBERTA PROVINCIAL STROKE STRATEGY (APSS)
") ALBERTA PROVINCIAL STROKE STRATEGY (APSS) Stroke Systems of Care Key Components APSS Pillar Recommendations March 28, 2007 1 The following is a summary of the key components and APSS Pillar recommendations
ALBERTA PROVINCIAL STROKE STRATEGY (APSS) Stroke Systems of Care Key Components APSS Pillar Recommendations March 28, 2007 1 The following is a summary of the key components and APSS Pillar recommendations
TOTAL PARENTERAL NUTRITION (TPN) Revised January 2013
 Revised January 2013") TOTAL PARENTERAL NUTRITION (TPN) Revised January 2013 OBJECTIVES Definition Indications for TPN administration Composition of TPN solutions Access routes for TPN administration Monitoring TPN administration
TOTAL PARENTERAL NUTRITION (TPN) Revised January 2013 OBJECTIVES Definition Indications for TPN administration Composition of TPN solutions Access routes for TPN administration Monitoring TPN administration
SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE
 UNIT: INTENSIVE CARE UNIT - ICU SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE STANDARD #: EFFECTIVE DATE: REVISED DATE: STANDARD TYPE: INTENSIVE CARE UNIT-ICU STANDARD I - SAFETY 3/88
UNIT: INTENSIVE CARE UNIT - ICU SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE STANDARD #: EFFECTIVE DATE: REVISED DATE: STANDARD TYPE: INTENSIVE CARE UNIT-ICU STANDARD I - SAFETY 3/88
National Patient Safety Goals Effective January 1, 2015
 National Patient Safety Goals Goal 1 Nursing are enter ccreditation Program Improve the accuracy of patient and resident identification. NPSG.01.01.01 Use at least two patient or resident identifiers when
National Patient Safety Goals Goal 1 Nursing are enter ccreditation Program Improve the accuracy of patient and resident identification. NPSG.01.01.01 Use at least two patient or resident identifiers when
Electronic Medication Administration Record (emar) (For Cerner Sites Only)
 (For Cerner Sites Only)") POLICY NO. 1009 Approved: 12/05 Effective: 12/05 Reviewed: 9/10; 5/12 1. Purpose: Electronic Medication Administration Record (emar) (For Cerner Sites Only) To provide direction for the transcription and
POLICY NO. 1009 Approved: 12/05 Effective: 12/05 Reviewed: 9/10; 5/12 1. Purpose: Electronic Medication Administration Record (emar) (For Cerner Sites Only) To provide direction for the transcription and
Chapter 15. Reconstitution and Dosages Measured in Units. Copyright 2012, 2007 Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
 Chapter 15 Reconstitution and Dosages Measured in Units 1 Objectives Calculating drug dosage problems that first require reconstitution of a powdered drug into a liquid form Using a proportion to solve
Chapter 15 Reconstitution and Dosages Measured in Units 1 Objectives Calculating drug dosage problems that first require reconstitution of a powdered drug into a liquid form Using a proportion to solve
Overview of the TJC/CMS VTE Core Measures
 Overview of the TJC/CMS VTE Core Measures CMS Specification Manual 4.2 January 1, 2013 June 30, 2013 Victoria Agramonte, RN, MSN Project Manager, IPRO VTE Regional Learning Sessions NYS Partnership for
Overview of the TJC/CMS VTE Core Measures CMS Specification Manual 4.2 January 1, 2013 June 30, 2013 Victoria Agramonte, RN, MSN Project Manager, IPRO VTE Regional Learning Sessions NYS Partnership for
Using the Pupillometer in Clinical Practice
 Using the Pupillometer in Clinical Practice Claude Hemphill MD M.A.S. chmephill@sfgh.ucsf.edu Kathy Johnson RN, MSN KJOHNSON@queens.org Mary Kay Bader RN, MSN, CCNS Badermk@aol.com Pupillometry: How It
Using the Pupillometer in Clinical Practice Claude Hemphill MD M.A.S. chmephill@sfgh.ucsf.edu Kathy Johnson RN, MSN KJOHNSON@queens.org Mary Kay Bader RN, MSN, CCNS Badermk@aol.com Pupillometry: How It
National Patient Safety Goals Effective January 1, 2015
 National Patient Safety Goals Effective January 1, 2015 Goal 1 Improve the accuracy of resident identification. NPSG.01.01.01 Long Term are ccreditation Program Medicare/Medicaid ertification-based Option
National Patient Safety Goals Effective January 1, 2015 Goal 1 Improve the accuracy of resident identification. NPSG.01.01.01 Long Term are ccreditation Program Medicare/Medicaid ertification-based Option
PHYSICIAN ORDERS TRANSIENT ISCHEMIC ATTACK (TIA) OBSERVATION
 OBSERVATION") SCREENING- ABCD-2 Score The ABCD2 score is a risk assessment tool designed to improve the prediction of short-term stroke risk after a transient ischemic attack (TIA). Higher ABCD2 scores are associated
SCREENING- ABCD-2 Score The ABCD2 score is a risk assessment tool designed to improve the prediction of short-term stroke risk after a transient ischemic attack (TIA). Higher ABCD2 scores are associated
What You Need to KnowWhen Taking Anticoagulation Medicine
 What You Need to KnowWhen Taking Anticoagulation Medicine What are anticoagulant medicines? Anticoagulant medicines are a group of medicines that inhibit blood clotting, helping to prevent blood clots.
What You Need to KnowWhen Taking Anticoagulation Medicine What are anticoagulant medicines? Anticoagulant medicines are a group of medicines that inhibit blood clotting, helping to prevent blood clots.
Ischaemic stroke 85% (85 in every 100 strokes)
") UNDERSTANDING STROKE DUE TO INTRACEREBRAL HAEMORRHAGE This factsheet provides information for people who have had a stroke due to an intracerebral (bleed in the brain) and for their families and carers.
UNDERSTANDING STROKE DUE TO INTRACEREBRAL HAEMORRHAGE This factsheet provides information for people who have had a stroke due to an intracerebral (bleed in the brain) and for their families and carers.
Administrative Policies and Procedures for MOH hospitals /PHC Centers. TITLE: Organization & Management Of Medication Use APPLIES TO: Hospital-wide
 Administrative Policies and Procedures for MOH hospitals /PHC Centers TITLE: Organization & Management Of Medication Use APPLIES TO: Hospital-wide NO. OF PAGES: ORIGINAL DATE: REVISION DATE : السیاسات
Administrative Policies and Procedures for MOH hospitals /PHC Centers TITLE: Organization & Management Of Medication Use APPLIES TO: Hospital-wide NO. OF PAGES: ORIGINAL DATE: REVISION DATE : السیاسات
The author has no disclosures
 Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 Mary.bradbury@inova.org This presentation will discuss unlabeled and investigational use of products The author
Mary Bradbury, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Surgery September 18, 2012 Mary.bradbury@inova.org This presentation will discuss unlabeled and investigational use of products The author
Collection Guidelines for Routine & Special Coagulation Testing
 Revised May 2010 Collection Guidelines for Routine & Special Coagulation Testing Best samples come from peripheral stick with evacuated tube system 19 to 22 gauge needle (smaller or bigger could cause
Revised May 2010 Collection Guidelines for Routine & Special Coagulation Testing Best samples come from peripheral stick with evacuated tube system 19 to 22 gauge needle (smaller or bigger could cause
Procedure for Inotrope Administration in the home
 Procedure for Inotrope Administration in the home Purpose This purpose of this procedure is to define the care used when administering inotropic agents intravenously in the home This includes: A. Practice
Procedure for Inotrope Administration in the home Purpose This purpose of this procedure is to define the care used when administering inotropic agents intravenously in the home This includes: A. Practice
High Risk Emergency Medicine
 High Risk Emergency Medicine Minor Head Injuries in Patients on Oral Anticoagulants David Thompson, MD, MPH Assistant Professor Department of Emergency Medicine No relevant financial relationships to disclose
High Risk Emergency Medicine Minor Head Injuries in Patients on Oral Anticoagulants David Thompson, MD, MPH Assistant Professor Department of Emergency Medicine No relevant financial relationships to disclose
Tranexamic Acid. Tranexamic Acid. Overview. Blood Conservation Strategies. Blood Conservation Strategies. Blood Conservation Strategies
 Overview Where We Use It And Why Andreas Antoniou, M.D., M.Sc. Department of Anesthesia and Perioperative Medicine University of Western Ontario November 14 th, 2009 Hemostasis Fibrinolysis Aprotinin and
Overview Where We Use It And Why Andreas Antoniou, M.D., M.Sc. Department of Anesthesia and Perioperative Medicine University of Western Ontario November 14 th, 2009 Hemostasis Fibrinolysis Aprotinin and
King County EMS Stroke Quality Improvement Program
 King County EMS Stroke Quality Improvement Program A Report from the King County EMS Medical QI Section March 2012 Prepared by Sofia Husain, Jim Duren, and Norm Nedell OBJECTIVE The goal of the King County
King County EMS Stroke Quality Improvement Program A Report from the King County EMS Medical QI Section March 2012 Prepared by Sofia Husain, Jim Duren, and Norm Nedell OBJECTIVE The goal of the King County
Administration of Medications & Fluids via a Peripheral Intravenous Cannula
 Administration of Medications & Fluids via a Peripheral Intravenous Cannula Clinical S.O.P. No.: 22.0 Compiled by: Approved by: Review date: November 2016 Administration of Medications & Fluids via S.O.P.
Administration of Medications & Fluids via a Peripheral Intravenous Cannula Clinical S.O.P. No.: 22.0 Compiled by: Approved by: Review date: November 2016 Administration of Medications & Fluids via S.O.P.
ED PATIENT INTERFACILITY TRANSFERS
 Page 1 ED PATIENT INTERFACILITY TRANSFERS APPROVED: EMS Medical Director EMS Administrator 1. Purpose 1.1. To provide guidance for emergency departments on ground ambulance transport of patients that require
Page 1 ED PATIENT INTERFACILITY TRANSFERS APPROVED: EMS Medical Director EMS Administrator 1. Purpose 1.1. To provide guidance for emergency departments on ground ambulance transport of patients that require
LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION
 LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION Hospital Policy Manual Purpose: To define the components of the paper and electronic medical record
LOUISIANA STATE UNIVERSITY HEALTH SCIENCES CENTER - SHREVEPORT MEDICAL RECORDS CONTENT/DOCUMENTATION Hospital Policy Manual Purpose: To define the components of the paper and electronic medical record
Is this pt s brain dysfunction due to ischemia? Onset & progression of sx; location of deficit
 CEREBROVASCULAR ACCIDENTS & TIA s Maggie Kelly History: Onset of symptoms exact time Previous sxs suggestive of TIA s Progression of symptoms Headache? Medications Past history of CVA, clotting events
CEREBROVASCULAR ACCIDENTS & TIA s Maggie Kelly History: Onset of symptoms exact time Previous sxs suggestive of TIA s Progression of symptoms Headache? Medications Past history of CVA, clotting events
ORAL ANTICOAGULANTS RIVAROXABAN (XARELTO) FOR PULMONARY EMBOLISM (PE)
 FOR PULMONARY EMBOLISM (PE)") ORAL ANTICOAGULANTS RIVAROXABAN (XARELTO) FOR PULMONARY EMBOLISM (PE) Information Leaflet Your Health. Our Priority. Page 2 of 6 What Are Anticoagulants And What Do They Do? This information leaflet has
ORAL ANTICOAGULANTS RIVAROXABAN (XARELTO) FOR PULMONARY EMBOLISM (PE) Information Leaflet Your Health. Our Priority. Page 2 of 6 What Are Anticoagulants And What Do They Do? This information leaflet has
Clinical Reasoning Case Study: I. Data Collection Chief complaint/history of Present Illness:
 Clinical Reasoning Case Study: I. Data Collection Chief complaint/history of Present Illness: What data is relevant that must be recognized as clinically significant to the nurse? Rationale: Personal/Social
Clinical Reasoning Case Study: I. Data Collection Chief complaint/history of Present Illness: What data is relevant that must be recognized as clinically significant to the nurse? Rationale: Personal/Social
WHAT TO DO WHEN THE URR IS UNDER 65
 Everest Healthcare Services Corporation August 4, 2000 WHAT TO DO WHEN THE URR IS UNDER 65 (See Model: Low URR Checklist adapted from Midwest Kidney Centers, Peoria, IL and presented in an Excel spreadsheet
Everest Healthcare Services Corporation August 4, 2000 WHAT TO DO WHEN THE URR IS UNDER 65 (See Model: Low URR Checklist adapted from Midwest Kidney Centers, Peoria, IL and presented in an Excel spreadsheet
ACUTE STROKE REGISTRY (NJASR) VERSION 2.0) (Continued)
 VERSION 2.0) (Continued)") New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.0 A. DEMOGRAPHIC DATA *Hospital Type (1): 1=Primary 2=Comprehensive 3=Other *Hospital Code (2): *Hospital Transferred From Code (3):
New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.0 A. DEMOGRAPHIC DATA *Hospital Type (1): 1=Primary 2=Comprehensive 3=Other *Hospital Code (2): *Hospital Transferred From Code (3):
STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE
 STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE WHAT IS A NURSING DIAGNOSIS? A nursing diagnosis is a clinical judgment about individual, family, or community responses to
STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE WHAT IS A NURSING DIAGNOSIS? A nursing diagnosis is a clinical judgment about individual, family, or community responses to
Policies and Procedures. Related to. IABP Therapy
 Policies and Procedures Related to IABP Therapy Courtesy of Datascope Corp. Clinical Support Services The following policies and procedures are intended to serve as guidelines for developing hospital policy.
Policies and Procedures Related to IABP Therapy Courtesy of Datascope Corp. Clinical Support Services The following policies and procedures are intended to serve as guidelines for developing hospital policy.
Note to Teachers about The Virtual Stroke Lab Student Handout
 Note to Teachers about The Virtual Stroke Lab Student Handout This document contains a handout that can be distributed for students to fill out as they complete The Virtual Stroke Lab, a free online Virtual
Note to Teachers about The Virtual Stroke Lab Student Handout This document contains a handout that can be distributed for students to fill out as they complete The Virtual Stroke Lab, a free online Virtual
Providence Telemedicine Network
 Providence Telemedicine Network Around the clock, around the region, our specialists are with you when every minute counts. Telemedicine brings our specialists to your hospital It is exciting to report
Providence Telemedicine Network Around the clock, around the region, our specialists are with you when every minute counts. Telemedicine brings our specialists to your hospital It is exciting to report
Ultrasound or Computed Tomography. PATIENT GUIDE and PREPARATION. Liver Biopsy
 Ultrasound or Computed Tomography PATIENT GUIDE and PREPARATION Liver Biopsy What is a Liver Biopsy? A Liver Biopsy is a procedure that involves taking a specimen ( a small amount of tissue) from within
Ultrasound or Computed Tomography PATIENT GUIDE and PREPARATION Liver Biopsy What is a Liver Biopsy? A Liver Biopsy is a procedure that involves taking a specimen ( a small amount of tissue) from within
Preparing Your Hospital for Primary Stroke Certification Authors: Wendy J. Smith, BS, MA, RES, RCEP, RN Claranne Mathiesen, MSN, RN, CNRN
 Preparing Your Hospital for Primary Stroke Certification Authors: Wendy J. Smith, BS, MA, RES, RCEP, RN Claranne Mathiesen, MSN, RN, CNRN Disclosures Wendy J. Smith-I have no actual or potential conflict
Preparing Your Hospital for Primary Stroke Certification Authors: Wendy J. Smith, BS, MA, RES, RCEP, RN Claranne Mathiesen, MSN, RN, CNRN Disclosures Wendy J. Smith-I have no actual or potential conflict
MISSISSIPPI BOARD OF NURSING IV THERAPY COURSE FOR THE EXPANDED ROLE LICENSED PRACTICAL NURSE COURSE OUTLINE
 THEORY MINIMUM 40 HOURS COURSE OUTLINE UNIT TOPIC HOURS* I LEGAL ASPECTS AND PRACTICE OF IV THERAPY 1 II REVIEW OF ANATOMY AND PHYSIOLOGY 6 III FLUID AND ELECTROLYTE BALANCE 10 IV EQUIPMENT AND PROCEDURES
THEORY MINIMUM 40 HOURS COURSE OUTLINE UNIT TOPIC HOURS* I LEGAL ASPECTS AND PRACTICE OF IV THERAPY 1 II REVIEW OF ANATOMY AND PHYSIOLOGY 6 III FLUID AND ELECTROLYTE BALANCE 10 IV EQUIPMENT AND PROCEDURES