Anti Leukotrienes. Allergic Rhinitis in children
|
|
|
- Linette Logan
- 8 years ago
- Views:
Transcription
1 Selection and Use of Essential Medicines Review of the role of Anti Leukotrienes in the therapy of Allergic Rhinitis in children Jan 12 th, 2013 Reviewed by: Dr Achal Gulati, MS; FIAMS Director Professor, Department of ENT & Head and Neck surgery, Maulana Azad Medical College, New Delhi. India Page 1 of 70

2 Summary: Allergic rhinitis (AR) is considered a significant global health challenge. AR is a major cause of patient visits to physicians in the United States, and commonly complicating management of other conditions such as asthma and chronic sinusitis. If AR is left untreated, the individual is at increased risk of missing work, school, prevalent sleep disruption and diminished day time performance, resulting in impaired quality of life. The economic burden of allergic rhinitis is substantial, due to a rising prevalence of AR in both children and adults. The peak onset of AR occurs primarily in the adolescent years. Research studies estimate prevalence of AR in children, to be about 10-20%. The current burden of allergic diseases, estimated by both direct and indirect costs, is approximately $4-10 billion/year in the United States. The economic burden of AR in Europe is also substantial, costing 1089 Euros per child/adolescent and 1543 Euros per adult in Europe. In addition, if asthma is considered a co-morbidity of AR, the costs involved for disease management, increase manifold. Treatment goals for AR, is relief of symptoms. Therapeutic options available to achieve this goal include avoidance measures, oral antihistamines, intranasal corticosteroids, leukotriene receptor antagonists (LTRA), and allergen immunotherapy. Daily use of an LTRA, antihistamine or decongestant, or a combination can be considered instead of, nasal steroids. The newer, secondgeneration (i.e. non-sedating) antihistamines are usually preferable to the older first-generation antihistamines to avoid sedation and other adverse side effects associated with them. LTRA s may be preferable to manage AR symptomology, independently or in combination with intra nasal steroid sprays. The following molecules in this (LTRAs) group are Monteluakst, Pranlukast and Zafirlukast. All are readily available for use. Montelukast is indicated in adult and Page 2 of 70

3 pediatric patients 6 months of age and older for the prophylaxis and chronic treatment of asthma, including the prevention of day and night-time symptoms from AR, the treatment of aspirin-sensitive asthmatic patients, and the prevention of exercise induced broncho-constriction. Research studies involving LTRA treatment for AR and associated co-morbidities, resulted in significantly less symptom severity after the treatment compared to control. Studies showed a positive correlation between severity of rhinitis, and effectiveness of LTRA intervention, resulting in improved nasal symptoms and quality of life (QOL). It was also noted that addition of an Intra Nasal Steroid Spray (INS) when added to the LTRA, enhanced the efficacy of the management of both, AR and Asthma. This better enhancement could be achieved by either a higher dose of LTRA or a lower dose of LTRA in case an INS is added. Due to LTRAs recent inclusion for AR treatment, there are no current studies evaluating LTRAs efficacy in children less than 6 years of age. Recent studies however, have found favorable results using Montelukast is safe for all age groups during short-term and long-term administration, even at doses substantially higher than the recommended dose. The safety profile of Montelukast did not change with long-term use. Montelukast has the advantage of being able to be administered orally whereas intranasal steroids may not be practical for small children. This is one of the aspects that needed to be considered as even though efficacy might be less, the effectiveness may be more. This is an important point which must be addressed. It is an important contributing factor (inadequate drug delivery to the tissue/improper technique of drug delivery, administration/inconvenient method of drug administration etc.) has been shown to be major contributory factors in the non efficacy of treatment schedules involving inhalant therapy. This is partly Page 3 of 70
.")
4 responsible in poor control of AR/Asthma in pediatric age group or in fact any age group. The treatment modality is a multi-modal therapy ie INS with anti histamine versus INS with LTRA. So the comparison comes down to the use of anti histamine or LTRA in combination with the INS. The drawbacks of the use of anti histamine are more than with LTRA. Considering these two factors, we could say that LTRA may a better option being safe to use and devoid of harmful side effect and and should be included in WHO-EML for children to be used as a stand alone or in augmentation with the INS. In summary, initiating therapy with Montelukast was associated with better asthma and AR control and resulted in reduced use of healthcare resources and lower costs of asthma rescue and allergy medications compared with initiating inhaled corticosteroid (ICS) therapy or with a placebo. Moreover, a decrease in prescription rates and costs were observed in the Montelukast cohort for rescue medications. Even in case of using Montelukast with an INS, it would be preferable to use Montelukast as the the choice option in management of AR. Recommendations: Leukotriene antagonists should be included in the WHO Essential Medicines List for children. The recommended molecule is Montelukast in the dose of 5mg once daily for children aged 6-14 years as Chewable tablets and Oral Granules.. Page 4 of 70

5 Aims & Objective: Review the role of Leukotriene antagonists in the management of childhood allergic rhinitis. Introduction: The first recorded case of allergic rhinitis (catarrhus aestivus) was described by Sir John Bostock, who presented himself as a case report to the Medical and Surgical Society of London in At the dawn of the 20th century, there were only several thousand members of the U.S. Ragweed Association. One hundred years later, allergic rhinitis has become the most common allergic or immunologic disorder in the U.S. population and it now affects an estimated one in seven Americans. Allergic rhinitis is acknowledged as a significant health challenge on a global scale. Allergic rhinitis is a major cause of patient visits to physicians in the United States, commonly complicates management of other conditions(eg.asthma, chronic sinusitis), and if untreated or undertreated can lead to considerable morbidity including missed work or school, sleep disruption, diminished daytime performance, and impaired quality of life The economic burden of allergic rhinitis is substantial. A rising prevalence of allergic rhinitis has been found not only in children but also in adults. The peak in incidence of allergic rhinitis occurs during the young adult years. Although prevalence declines with age, allergic rhinitis is also an important health concern in older adults. Incidence of allergic rhinitis is equal in male and female patients. Epidemiologic studies have consistently demonstrated that allergic rhinitis and asthma commonly coexist. Allergic rhinitis is often associated with asthma and Page 5 of 70

6 is a risk factor for developing asthma; in addition, many patients with allergic rhinitis demonstrate increased bronchial hyper responsiveness to inhalation challenge with histamine or methacholine 1. Methods: To review the role of Leukotriene antagonists in the management of childhood allergic rhinitis, we reviewed the references in pubmed, Cochrane, Medline and other web portals i.e. Medscape, Google wild search to collate the relevant information on safety and efficacy of Leucotriene antagonists (Montelukast) in human subjects. Note: The following molecules in this Leukotriene Receptor Antagonists (LTRAs) group: Monteluakst, Pranlukast and Zafirlukast are available. We searched for LTRA and their utility in AR. We found most of the studies with these LTRAs were conducted in Asthmatic and we found very few in AR and then in pediatric patient. Secondly they represent their class effects mostly. However in some of the articles Montelukast was considered a better molecule as compared to others. We therefore choose to mention the Montelukast as a reference for our review. However, it may be mentioned that most of the controlled trials comparing the 3 drugs did not find any significant difference in the action and effects of the 3 drugs and that is the other reason that we decided to take Montelukast as the prototype drug in this group We have explored and evaluated Montelukast and its relevant studies as a reference to describe tolerability, safety and efficacy and advantages of using LTRAs in managing AR in children since it was a widely available molecule. Page 6 of 70

7 Prevalence of Allergic Rhinitis (Public health need): Approximately 20% of the world population suffers from allergic diseases that cause a substantial health care burden 2. Allergic rhinitis is a prevalent yet underappreciated inflammatory disorder of nasal mucosa, which is characterized by pruritus, sneezing, rhinorrhea, and nasal congestion. Allergic rhinitis affects 400 million people worldwide, with high prevalence recorded in industrialized nations, especially English-speaking ones. Researchers on the International Study of Asthma and Allergies in Childhood (ISAAC) project investigated the prevalence and possible causes of atopic diseases, using standardized methods to describe the prevalence and severity of asthma, rhinitis and eczema with validated questionnaires in children around the world. The first phase of ISAAC took place between 1992 and Prevalence of rhinitis with itchy watery eyes was estimated to be around 0.8% 14.9% (median 6.9%) in children aged 6-7 years and 1.4% 39.7% (median 13.6%) in those aged years. The lowest prevalence was in parts of Eastern Europe and south and central Asia. The third phase of ISAAC (at least 5 years later) showed prevalence of rhinitis with itchy watery eyes in the past year was 1.8% 24.2% in children aged 6-7 years (median 8.5%) and 1.0% 45.0% (median 14.6%) in those aged years 3. But most studies put the figure of the prevalence of allergic rhinitis in children to about 10% to 20%. In selected other international studies, the prevalence was reported as follows: Germany (1992; ages 9 to 11), 9.5%; Germany (1994; ages 13 to 16), 22.7%; Italy (1988; ages 9 to 15), 13.1%; Japan (1994; ages 6 to 15), 12.9%; Norway (1994; 7 to 12), 20.6%; Poland (1995; ages 6 to 15), 16.7%; Sweden (1995; age 7), 13%; UK (1989; age 12), 14.9%; UK (1992; ages 8 to 13), 11.9%; U.S. (1994; age 6), 42% 4. In a community-based study in London, the Page 7 of 70
 project investigated the prevalence and possible causes of atopic diseases, using standardized methods to describe")
8 minimum prevalence of hay fever (SAR is also termed as Hay fever) in adults between age 16 and 65 was 16%. Of these, 8% had perennial symptoms, 6% had both perennial and seasonal symptoms, and 2% had seasonal symptoms 5. Estimates of the prevalence of hay fever vary between 2% and 15% depending on the diagnostic criteria chosen, method of investigation, and the age groups studied. Worldwide the prevalence of hay fever in school-age children appears to be lower in European countries than in America. The prevalence of diagnosed hay fever among patients consulting general practitioners is reported to be 11 per 1000 in Denmark, 19.7 per 1000 in England and Wales, and 86 per 1000 in Australia 6. Allergic Rhinitis and Asthma may be a spectrum of the same disease based on the surmise of One airway, one disease. So it will not be wrong to say that the burden of Allergic Rhinitis is a subset of the total burden of the disease complex of Allergic Rhinitis and asthma. The economic burden of the disease: The current burden of allergic diseases, estimated by both direct and indirect costs, is very relevant. In fact the cost estimation for rhinitis amount globally to 4-10 billion dollars/year in the U.S. and to an average annual cost of 1089 Euros per child/adolescent and 1543 Euros per adult in Europe 7. If we consider Asthma as a co-morbidity of Allergic Rhinitis, the costs involved in the disease complex grow manifold. A few global facts and figures for two common allergic diseases: asthma and rhinitis are as follows 8. Page 8 of 70


9 * Direct costs: Expenditure on medications and health care provision ** Indirect costs: Cost to society from loss of work, social support, loss of taxation income, home modifications, lower productivity at work, etc Thus it may be comfortable to say that the global costs involved in the management of Asthma may be curtailed to a great amount if we can manage to bring a lowering of the Allergic Rhinitis burden of the disease complex Management of Allergic Rhinitis: The treatment goal for allergic rhinitis is relief of symptoms. Atopy has a genetic component involved. Thus the management of such individuals would be a control of symptoms or managing the disease prophylectically. These atopic individuals can only be provided either symptomatic or prophylactic treatment for their symptoms in addition to the specific measures as immunotherapy, allergen avoidance etc. Therapeutic options available to achieve this goal include avoidance measures, oral antihistamines, intranasal corticosteroids, leukotriene receptor antagonists, and Page 9 of 70

10 allergen immunotherapy (see Figure). Other therapies that may be useful in select patients include decongestants and oral corticosteroids. If the patient s symptoms persist despite appropriate treatment, referral to an allergollogist should be considered. As mentioned earlier, allergic rhinitis and asthma appear to represent a combined airway inflammatory disease and, therefore, treatment of asthma is also an important consideration in patients with allergic rhinitis 9. Most cases of allergic rhinitis respond to pharmacotherapy. Patients with intermittent symptoms are often treated adequately with oral antihistamines, decongestants, or both as needed. Regular use of an intranasal steroid spray may be more appropriate for patients with chronic symptoms. Daily use of a leukotriene receptor antagonist, antihistamine or decongestant, or a combination can be considered instead of or in addition to nasal steroids. The newer, second-generation (ie. Non-sedating) antihistamines are usually preferable to the older first-generation antihistamines to avoid sedation and other adverse effects associated with them. Leukotriene receptor antagonists may be preferable to manage the allergic rhinitis symptom either alone or in combination with intra nasal steroid sprays. Ocular antihistamine drops (for eye symptoms), intranasal antihistamine sprays, intranasal cromolyn, intranasal anti cholinergic sprays, and short courses of oral corticosteroids (reserved for severe, acute episodes only) may also provide relief 10. ARIA (Allergic Rhinitis and its Impact on Asthma) guidelines give a recommended algorithm to manage Allergic rhinitis: Page 10 of 70

11 ARIA recommendations: Page 11 of 70
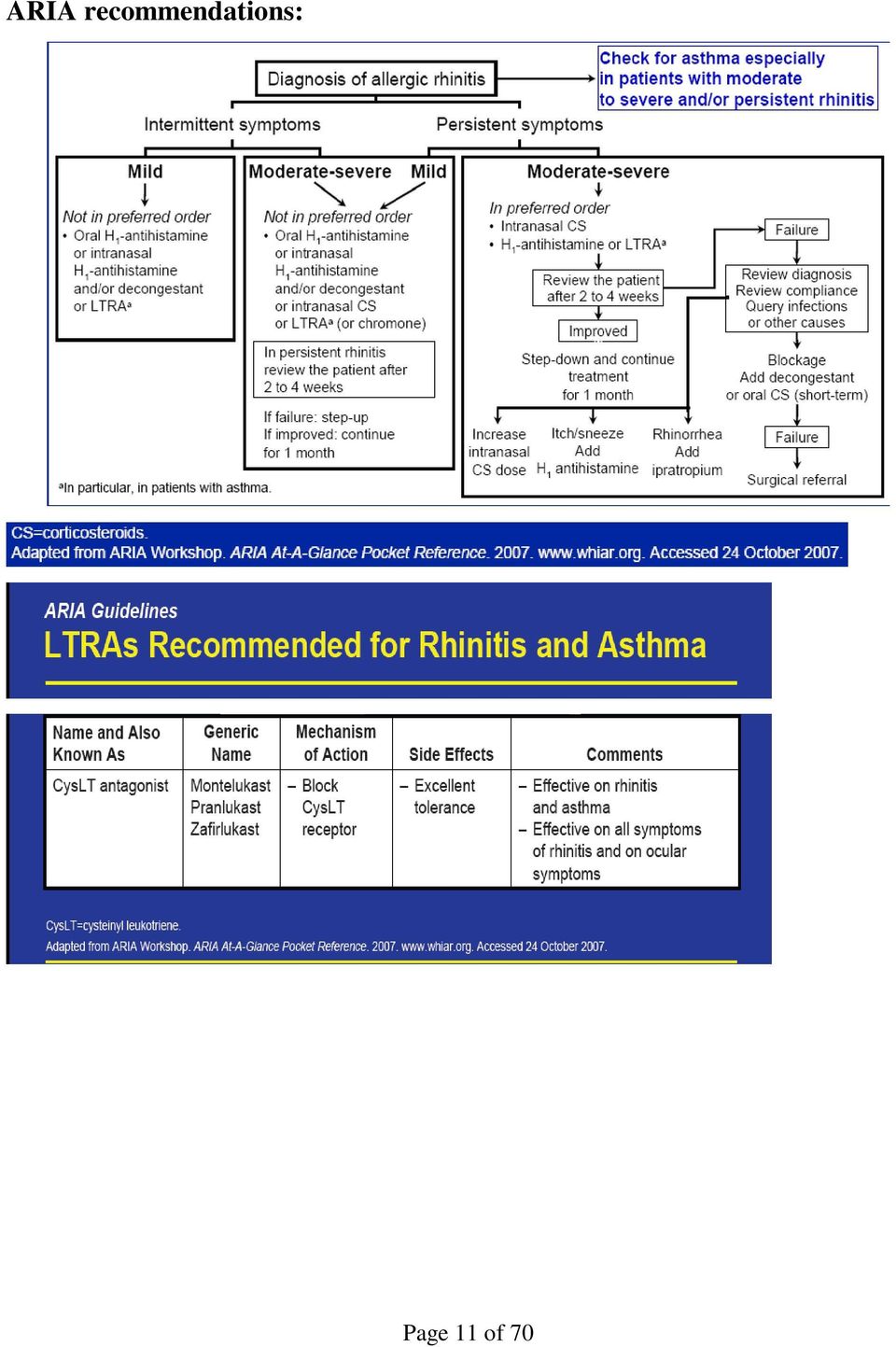


12 A simplified, stepwise algorithm for the treatment of allergic rhinitis. Note: Treatments can be used individually or in any combination 9. Page 12 of 70

13 Drugs Available for management of Allergic Rhinitis: Glossary of Rhinitis Medications: Name and Also known as Generic name Mechanism of action Side effects Comments Oral H-1 antihistamines H-1 blockers 2 nd generation Cetrizine Ebastine Fexofenadine Loratadine Mizolastine Acrivastine Azelastine Mequizatine New Products Desloratadine Levocetrizine Rupatadine -Blockage of H-1 receptor Some anti allergic activity New generation drug can be used once daily No development of tachyphylaxis 2 nd generation no sedation for most drugs No anti cholinergic effects No cardiotoxocit y Acrivastine has sedative effects Oral Azelastine may induce sedation and a bitter taste -First line therapy except in moderate/severe persistent allergic rhinitis -2 nd generation oral H- 1 blockers are preferred for their favorable efficacy/safety ratio and pharmacokinetics; first generation molecules are no longer recommended because of their unfavorable safety/efficacy ratio. Rapidly effective (less than 1hr)on nasal and ocular symptoms moderately effective on nasal congestion Cardiotoxic drugs (Astemizole, Terfenadine) are no longer marketed in most countries Page 13 of 70

14 Local H-1 antihistamines (intranasal, intraocular) Intranasal glucocorticosteroids Azelastine Levocabastine Olopatadine Beclomethason e dipropionate Budesonide Ciclosenide Flunisolide Fluticasone propionate Mometasone furoate Triamcinolone acetonide -Blockage of H-1 receptor Some anti allergic activity for Azelastine -Potently reduce nasal inflammation Reduce nasal hyperreactivity -Minor local side effects Azelastine: bitter taste in some patients Minor local side effects Wide margin for systemic side effects growth concerns with Beclomethas one dipropionate (BDP) only In young children consider the combination of intranasal and inhaled drugs Rapidly effective (less than 30 min) on nasal or ocular symptoms The most effective pharmacologic treatment of allergic rhinitis; first line treatment for moderate/severe persistent allergic rhinitis. It may be reiterated that the best control in AR is achieved by a multi modal delivery in a combination of INS and LTRA which are preferable over anti histamines Effective on nasal congestion Effective on smell Effect observed after 6-12 hrs but maximal effect after a few days Patient should be advised on the proper method of administering intranasal Glucocorticosteroids, including the importance of directing the spray laterally Page 14 of 70
 on nasal or ocular symptoms The most effective pharmacologic treatment of allergic rhinitis;")
15 rather than medially (toward the septum) in the nose. Oral/IM gluco corticosteroids Local cromones (intranasal, intraocular) Oral decongestants Dexamethason e Hydrocortisone Methylprednis olone Prednisolone Prednisone Triamcinolone Betamethasone Deflazacort Cromoglycate Nedocromil Ephidrine Phenylephrine Phenyl propanolamine Pseudoephedri ne Oral H-1 antihistamine decongestant combination -Potently reduce nasal inflammation Reduce nasal hyperreactivity -Mechanism of action poorly known Sympathomim etic drug Relieve symptoms of nasal congestion -Systemic side effects common in particular for IM drugs Depot injections may cause local tissue atrohy - Minor local side effects Hypertension Palpitation Restlessness Agitation Tremor Insomnia Headache Dry mucous membranes When possible intranasal glucocorticosteroids should replace oral or IM drugs -Intraocular cromones are very effective intranasal cromones are less effective and their effect is short lasting overall excellent safety Use oral decongestants with caution in patients with heart disease oral H-1 antihistamine decongestant combination products may be more effective than either product alone but side effects are combined Page 15 of 70

16 Intranasal decongestants Intra nasal anticholinergic s CysLT antagonist Antileukotriene s Oxymetazoline Others Ipratropium Montelukast Pranlukast Zafirlukast Sympathomim etic drugs Relieve symptoms of nasal congestion Anticholinergic s block almost exclusively rhinorrhea Block CysLT receptor Urinary retention Exacerbation of glaucoma/ thyrotoxicosi s - Same side effects as oral decongestants but less intense Rhinitis medicamento sa is a rebound phenomenon occurring with prolonged use (over 10days) Minor local side effects almost no systemic anticholinergi c activity Excellent tolerance Act more rapidly and more effectively than oral decongestants limit duration of treatment to less than 10 days to avoid rhinitis medicamentosa Effective in allergic and non allergic patients with rhinorrhea. (Note: Rhinorrhoea due to other non allergic causes like tumors, polyps etc would not be responsive to any medical treatment. Effective on rhinitis and asthma Effective on all symptoms of rhinitis Page 16 of 70

17 and on ocular symptoms Reference: 1 International Primary Care Airways Group (IPAG) Handbook available at 2. Allergic rhinitis and its impact on Asthma (ARIA) 2007 documents and resources. Pharmacology of LTRA The following molecules in this (LTRAs) group: Monteluakst, Pranlukast and Zafirlukast are available. We have explored and evaluated Montelukast and it relevant studies as a reference to describe tolerability, safety and efficacy and advantages of using LTRAs in managing AR in children. General Information on Montelukast 11: Nomenclature International Non-proprietary Name: Montelukast Sodium British Approved Name: Montelukast British Approved Name, modified: Montelukast Sodium U.S. Adopted Name: Montelukast Sodium ChemicalName:[R-(E)]-1-[[[1-[3-[2-(7-Chloro-2- uinolinyl)ethenyl]phenyl]-3-[2- (1-hydroxy-1-methylethyl)phenyl]-propyl]thio]methyl]cyclopropane acetic acid sodium salt Page 17 of 70

18 Montelukast sodium is a selective and orally active leukotriene receptor antagonist that specifically inhibits the cysteinyl leukotriene CysLT1 receptor. Montelukast sodium is described chemically as [R-(E)]-1-[[[1-[3-[2-(7-chloro-2- quinolinyl)ethenyl]phenyl]-3-[2-(1-hydroxy-1 methylethyl)phenyl]propyl]thio]methyl]cyclopropaneaceticacid, monosodium salt. The empirical formula is C35H35ClNNaO3S, and its molecular weight is Montelukast sodium is a hygroscopic, optically active, and white to off-white powder. Montelukast sodium is freely soluble in ethanol, methanol, and water and practically insoluble in acetonitrile. Montelukast is indicated in adult and pediatric patients 6 months of age and older for the prophylaxis and chronic treatment of asthma, including the prevention of day- and nighttime symptoms, the treatment of aspirin-sensitive asthmatic patients, and the prevention of exercise induced bronchoconstriction. Montelukast is indicated for the relief of daytime and nighttime symptoms of allergic rhinitis (seasonal allergic rhinitis in adults and pediatric patients 2 years of age and older, and perennial allergic rhinitis in adults and pediatric patients 6 months of age and older). (Refer to ARIA guidelines). Availability Active ingredient: Montelukast Sodium Forms and strength available: Tablet; oral: 10 mg, 5 mg, and 4 mg Oral Granules: 4 mg Commonly used brand names: Montelukast, Montair, Romilast etc. Page 18 of 70

19 The product is available as: Oral granules form, 4mgm: 4-mg oral granules contains 4.2 mg montelukast sodium, which is equivalent to 4 mg of montelukast. The oral granule formulation contains the following inactive ingredients: mannitol, hydroxypropyl cellulose, and magnesium stearate. Oral chewable tablet form, 5 mgm: 5-mg chewable MONTELUKAST tablet contains 5.2 mg montelukast sodium, respectively, which are equivalent to 5 mg of Montelukast.. Chewable tablets contain the following inactive ingredients: mannitol, microcrystalline cellulose, hydroxypropyl cellulose, red ferric oxide, croscarmellose sodium, cherry flavor, aspartame, and magnesium stearate. Oral tablets, 10mgm: 10-mg film-coated MONTELUKAST tablet contains 10.4 mg montelukast sodium, which is equivalent to 10mg of montelukast, and the following inactive ingredients: microcrystalline cellulose, lactose monohydrate, croscarmellose sodium, hydroxypropyl cellulose, and magnesium stearate. The film coating consists of: hydroxypropyl methylcellulose, hydroxypropyl cellulose, titanium dioxide, red ferric oxide, yellow ferric oxide, and carnauba wax. DOSAGE AND ADMINISTRATION 11 : Patients with both asthma and allergic rhinitis should take only one tablet daily in the evening. Pediatric Patients 6 to 14 Years of Age with Asthma and/or Allergic Rhinitis The dosage for pediatric patients 6 to 14 years of age is one 5-mg chewable tablet daily. Pediatric Patients 2 to 5 Years of Age with Asthma and/or Allergic Rhinitis Page 19 of 70

20 The dosage for pediatric patients 2 to 5 years of age is one 4-mg chewable tablet daily or one packet of 4-mg oral granules daily Pediatric Patients 6 Months to 2 Years of Age with Asthma or Perennial Allergic Rhinitis The dosage for pediatric patients 6 months to 2 years of age is one packet of 4-mg oral granules daily. Administration of oral granules 11 : Montelukast oral granules can be administered either directly in the mouth, mixed with a spoonful of cold or room temperature soft food (e.g., applesauce), or dissolved in 1 teaspoonful (5 ml) of cold or room temperature baby formula or breast milk. The packet should not be opened until ready to use. After opening the packet, the full dose of Montelukast oral granules must be administered immediately (within 15 minutes). If mixed with food, or dissolved in baby formula or breast milk, Montelukast oral granules must not be stored for future use. Montelukast oral granules are not intended to be dissolved in any liquid other than baby formula or breast milk for administration. However, liquids may be taken subsequent to administration. General Recommendations for intake 11 : Montelukast tablets, chewable tablets, and oral granules can be taken with or without food. No dosage adjustment is necessary for pediatric patients, for the elderly, for patients with renal insufficiency, or mild-to-moderate hepatic impairment, or for patients of either gender. Page 20 of 70
.")
21 PEDIATRIC USE 11 : Montelukast has been studied in pediatric patients 6 months to 14 years of age (see Dosage and Administration). Safety and effectiveness in pediatric patients younger than 6 months of age have not been studied. Studies have shown that SINGULAIR does not affect the growth rate of pediatric patients. CLINICAL PHARMACOLOGY 11 Mechanism of Action 11 The cysteinyl leukotrienes (LTC4, LTD4, LTE4), are potent inflammatory eicosanoids released from various cells including mast cells and eosinophils. These important pro-asthmatic mediators bind to cysteinyl leukotriene (CysLT) receptors. The CysLT type-1 (CysLT1) receptor is found in the human airway (including airway smooth muscle cells and airway macrophages) and on other proinflammatory cells (including eosinophils and certain myeloid stem cells). CysLTs have been correlated with the pathophysiology of asthma and allergic rhinitis. In asthma, leukotriene-mediated effects include a number of airway actions, including bronchoconstriction, mucous secretion, increased vascular permeability, and eosinophil recruitment. In allergic rhinitis, CysLTs are released from the nasal mucosa after allergen exposure during both early- and late-phase reactions and are associated with symptoms of allergic rhinitis. Intranasal challenge with CysLTs has been shown to increase nasal airway resistance and symptoms of nasal obstruction. Montelukast is a potent, orally active compound that significantly improves parameters of asthmatic inflammation. Based on biochemical and pharmacological bioassays, it binds with high affinity and selectivity to the CysLT1 receptor (in Page 21 of 70
22 preference to other pharmacologically important airway receptors such as the -adrenergic receptor). Montelukast potently inhibits physiologic actions of LTC4, LTD4, and LTE4 at the CysLT1 receptor without any agonist activity. Pharmacokinetics 11 Absorption 11 : Montelukast is rapidly and nearly completely absorbed following oral administration. For the 10-mg film-coated tablet, the mean peak plasma concentration (Cmax) is achieved 3 hours (Tmax) after administration in adults in the fasted state. The mean oral bioavailability is 64%. The oral bioavailability and Cmax are not influenced by a standard meal. For the 5-mg chewable tablet, the Cmax is achieved 2 hours after administration in adults in the fasted state. The mean oral bioavailability is 73%. Food does not have a clinically important influence with chronic administration. For the 4-mg chewable tablet, Cmax is achieved 2 hours after administration in pediatric patients 2 to 5 years of age in the fasted state. The 4-mg oral granule formulation is bioequivalent to the 4-mg chewable tablet when administered to adults in the fasted state. The co-administration of applesauce or a standard meal with the oral granule formulation did not have a clinically meaningful effect on the pharmacokinetics of Montelukast as determined by AUC ( vs ng.hr/ml with and without applesauce, respectively, and vs ng.hr/ml with and without a standard meal, respectively). Safety and efficacy were demonstrated in clinical studies where the 4-mg chewable tablet, 5-mg chewable tablet, and 10-mg film-coated tablet were administered without regard to the timing of food ingestion. The safety of Montelukast was also Page 22 of 70
23 demonstrated in a clinical study in which the 4-mg oral granules were administered without regard to the timing of food ingestion. Distribution 11 : Montelukast is more than 99% bound to plasma proteins. The steady-state volume of distribution of Montelukast averages 8 to 11 liters. Studies in rats with radio labeled Montelukast indicate minimal distribution across the blood-brain barrier. In addition, concentrations of radio labeled material at 24 hours post dose were minimal in all other tissues. Metabolism 11 : Montelukast is extensively metabolized. In studies with therapeutic doses, plasma concentrations of metabolites of Montelukast are undetectable at steady state in adults and pediatric patients. In vitro studies using human liver microsomes indicate that cytochrome P450 3A4 and 2C9 are involved in the metabolism of Montelukast. Based on further in vitro results in human liver microsomes, therapeutic plasma concentrations of Montelukast do not inhibit cytochromes P450 3A4, 2C9, 1A2, 2A6, 2C19, or 2D6. Elimination 11 : The plasma clearance of Montelukast averages 45 ml/min in healthy adults. Following an oral dose of radio labeled Montelukast, 86% of the radioactivity was recovered in 5-day fecal collections and less than 0.2% was recovered in urine. Coupled with estimates of Montelukast oral bioavailability, this indicates Montelukast and its metabolites are excreted almost exclusively via the bile. In several studies, the mean plasma half-life of Montelukast ranged from 2.7 to 5.5 hours in healthy young adults. The pharmacokinetics of Montelukast is nearly linear for oral doses up to 50 mg. No difference in pharmacokinetics was noted Page 23 of 70
24 between dosing in the morning or in the evening. During once-daily dosing with 10 mg Montelukast, there is little accumulation of the parent drug in plasma (~14%). (refer: SPC.SGA-5mg.12.UK.3624.II-070-WS-007; Date of revision of text Dec-2012) Undesirable effects Montelukast has been evaluated in clinical studies as follows: 10 mg film-coated tablets in approximately 4,000 adult patients 15 years of age and older, and 5 mg chewable tablets in approximately 1,750 paediatric patients 6 to 14 years of age. The following drug-related adverse reactions in clinical studies were reported commonly ( 1/100 to <1/10) in patients treated with montelukast and at a greater incidence than in patients treated with placebo: Body System Class Adult Patients 15 years and older (two 12-week studies; n=795) Nervous disorders Gastro-intestinal disorders system headache abdominal pain Paediatric Patients 6 to 14 years old (one 8-week study; n=201) (two 56-week studies; n=615) headache With prolonged treatment in clinical trials with a limited number of patients for up to 2 years for adults, and up to 12 months for paediatric patients 6 to 14 years of age, the safety profile did not change. Page 24 of 70
25 Post-marketing Experience Adverse reactions reported in post-marketing use are listed, by System Organ Class and specific Adverse Experience Term, in the table below. Frequency Categories were estimated based on relevant clinical trials. System Organ Frequency Adverse Experience Term Class Category Infections and Very upper respiratory infection infestations Blood and lymphatic system disorders Immune system disorder Psychiatric disorders Nervous system disorder increased bleeding tendency hypersensitivity reactions including anaphylaxis hepatic eosinophilic infiltration dream abnormalities including nightmares, insomnia, somnambulism, irritability, anxiety, restlessness, agitation including aggressive behaviour or hostility, depression tremor hallucinations, disorientation, suicidal thinking and behaviour (suicidality) dizziness, drowsiness paraesthesia/hypoesthesia, seizure Common Rare Uncommon Very Rare Uncommon Rare Cardiac disorders palpitations Rare Respiratory, thoracic and mediastinal disorders Gastrointestinal disorders Hepatobiliary disorders epistaxis Churg-Strauss Syndrome (CSS) (see section 4.4) diarrhoea, nausea, vomiting dry mouth, dyspepsia elevated levels of serum transaminases (ALT, AST) Very Rare Uncommon Uncommon Very Rare Common Uncommon Common Page 25 of 70
26 Skin and subcutaneous tissue disorders Musculoskeletal, connective tissue and bone disorders General disorders and administration site conditions Hepatitis (including cholestatic, hepatocellular, and mixed-pattern liver injury). rash bruising, urticaria, pruritus angiooedema erythema nodosum, erythema multiforme arthralgia, myalgia including muscle cramps pyrexia Very Rare Common Uncommon Rare Very Rare Uncommon Common Uncommon asthenia/fatigue, malaise, oedema *Frequency Category: Defined for each Adverse Experience Term by the incidence reported in the clinical trials data base: Very Common ( 1/10), Common ( 1/100 to <1/10), Uncommon ( 1/1000 to <1/100), Rare ( 1/10,000 to <1/1000), Very Rare (<1/10,000). This adverse experience, reported as Very Common in the patients who received montelukast, was also reported as Very Common in the patients who received placebo in clinical trials. This adverse experience, reported as Common in the patients who received montelukast, was also reported as Common in the patients who received placebo in clinical trials. Page 26 of 70
27 (refer: SPC.SGA-5mg.12.UK.3624.II-070-WS-007; Date of revision of text Dec-2012) Overdose No specific information is available on the treatment of overdose with montelukast. In chronic asthma studies, montelukast has been administered at doses up to 200 mg/day to patients for 22 weeks and in short-term studies, up to 900 mg/day to patients for approximately one week without clinically important adverse experiences. There have been reports of acute overdose in post-marketing experience and clinical studies with montelukast. These include reports in adults and children with a dose as high as 1000 mg (approximately 61 mg/kg in a 42 month old child). The clinical and laboratory findings observed were consistent with the safety profile in adults and paediatric patients. There were no adverse experiences in the majority of overdose reports. The most frequently occurring adverse experiences were consistent with the safety profile of montelukast and included abdominal pain, somnolence, thirst, headache, vomiting, and psychomotor hyperactivity. It is not known whether montelukast is dialysable by peritoneal- or haemo-dialysis ANIMAL TOXICOLOGY 11 Acute Toxicity No mortality occurred following a single oral administration of montelukast sodium at doses up to 5000 mg/kg, in mice and rats, (15,000 mg/m2 and 29,500 mg/m2 in mice and rats, respectively) the maximum dose tested (oral LD50 >5000 mg/kg). This dose is equivalent to 25,000 times the recommended daily adult human dose*. (* Based on an adult patient weight of 50 kg) Page 27 of 70
28 Chronic Toxicity The toxic potential of montelukast sodium was evaluated in a series of repeated dose toxicity studies of up to 53 weeks in monkeys and rats and up to 14 weeks in infant monkeys and in mice. Montelukast sodium was well tolerated at doses which provide a wide margin of safety based on total dose administered. The no effect level for all toxicological parameters in any of the species tested was at least 125 times the recommended human dose*. There were no findings that would preclude administration at the therapeutic dosage level for both adults and pediatric patients. (* Based on an adult patient weight of 50 kg). Carcinogenicity Montelukast sodium was not carcinogenic when administered at oral doses of up to 200 mg/kg/day in a 106-week study in rats, or at oral doses of up to 100 mg/kg/day in a 92-week study in mice. These doses are equivalent to 1000 times and 500 times the recommended adult human dose*.(* Based on an adult patient weight of 50 kg). Mutagenesis Montelukast sodium was found to be neither genotoxic nor mutagenic. Montelukast sodium was negative in the in vitro microbial mutagenesis assay and the V-79 mammalian cell mutagenesis assays, with and without metabolic activation. There was no evidence of genotoxicity in the in vitro alkaline elution assay in rat hepatocytes and the in vitro chromosomal aberration assays in Chinese hamster ovary cells, with or without a microsomal enzyme activation system. Similarly, there was no induction of chromosomal aberrations in bone marrow cells of male or female mice after the administration of oral doses of up to 1200 mg/kg (3600 mg/m2) (6000 times the recommended daily adult dose*). (* Based on an adult patient weight of 50 kg). Page 28 of 70
29 Reproduction Fertility and reproductive performance were not affected in studies with male rats given oral doses of up to 800 mg/kg/day or with female rats given doses of up to 100 mg/kg/day. These dosages provide margins of 4000-fold and 500-fold, respectively, above the recommended adult human dose*. (* Based on an adult patient weight of 50 kg). Development In developmental toxicity studies, there were no treatment related adverse effects at doses up to 400 mg/kg/day in rats and up to 100 mg/kg/day in rabbits. Fetal exposure of montelukast sodium in rats and rabbits does occur and significant concentrations of drug were observed in milk of lactating rats. REGULATORY STATUS: Montelukast (Montelukast) was covered by U.S. Patent No. 5,565,473 which expired on August 3, The same day, the FDA approved several generic versions of Montelukast. The U.S. Food and Drug Administration today approved the first generic versions of Montelukast (montelukast sodium) for use in adults and children to control asthma symptoms and to help relieve symptoms of indoor and outdoor allergies. Apotex Inc., Aurobindo Pharma, Endo Pharmaceuticals, Glenmark Generics, Kudco Ireland Inc., Mylan Inc., Roxane Laboratories, Sandoz Inc., Teva Pharmaceuticals Inc., and Torrent Pharmaceuticals have gained FDA approval for generic montelukast tablets. Page 29 of 70
30 Apotex, Aurobindo, Endo, Kudco, Mylan, Roxane, Sandoz, Teva, and Torrent have received approval for chewable tablets. Teva has received approval for the oral granule form. (Ref: FDA News Release: For Immediate Release: Aug. 3, 2012; Media Inquiries: Sandy Walsh, , FDA approves first generic versions of Montelukast to treat asthma, allergies ) The presence of the above companies is distributed among various countries and the web search revealed that Momtelukast is available in China, Indinesia, Hongkong, India, Malaysia, Philipines, Singapore, Thailand, Taiwan, Vietnam, US and Europe. Whilst patent protection for the Montelukast molecule expired in Canada in October 2011, protection extends to August 2012 in the US. In Europe, many Supplementary Protection Certificate SPCs protecting the Montelukast molecule were granted with expiries in August However, Merck successfully complied with the agreed paediatric investigation plan (PIP) and successfully applied for 6 month extensions to the terms of several SPCs, giving a potential expiry of February 2013 in some of western Europe s largest markets, namely France, Germany and the UK, as well as in many of the region s smaller markets. Due to later authorisation of the product in Australia, the s70 extension on the molecule patent in this jurisdiction extends to April Patent family US A claims crystalline Montelukast sodium and processes for its preparation. (Ref: GenericsWeb - January 2012; News letter 'INNsight') Page 30 of 70
31 Safety and efficacy Search methods for identification of Data: An online database search for articles published from 1950 to present was conducted. The relevant articles were studied and summarized in combination with other resources. Electronic searches 1. Cochrane library 2. Pubmed Searching other resources: multiple sources were used wherever possible to validate the data. ARIA Guideline available on ARIA website and the flow charts for selecting the included articles. Inclusion criteria: English language articles Human subjects Types of studies: 1. Systematic reviews 2. Randomized controlled trials which subjects were assigned to treatment or control group (placebo-controlled or different drug) on the basis of random allocation. 3. Reviews 4. Observational studies Types of participant: Children between 0-14 years old Page 31 of 70
32 Types of interventions: the treatment group received Montelukast at any dose for any duration at any time Exclusion Criteria: Non English language articles Animal studies Studies not targeting pediatric population Studies including pediatric populations, but pediatric specific data not reported separately Studies without clear specification of intervention or dose Individual case reports Description of the included studies: Efficacy: A number of studies were conducted to generate evidences on Montelukast use in controlling allergic airway diseases. Some of the relevant evidences available are as follows: To assess the effectiveness of anti-leukotrienes prophylactic treatment on the course of seasonal allergic rhinitis, a study which enrolled 48 patients aged 6 12 years were done in Italy 12. From those 28 patients with already diagnosed seasonal allergic rhinitis conducted main group who received the Montelukast once per day and 20 patients without any previous treatment consist the second control group. The symptom severity scores and its correlation to quality of life questionnaire were assessed in both groups. The most frequent symptom was nasal secretion, but Page 32 of 70
33 the most serious or disturbing symptom, that affects quality of life was nasal obstruction. The results showed that in main group all nasal symptom scores (sneezing, nose blows, nasal obstruction, interference with daily living, and symptom comparison with the previous year) has significantly less symptom severity after the treatment compared to control. All subscales of PRQLQ (Pediatric Rhino-conjunctivitis Quality of Life Questionnaire) indicated higher scores for group main group. The quality of life scores depend on treatment duration; the longer the treatment period, the higher the QOL (Quality of Life) score 12. The result showed correlation between severity of rhinitis and quality of life and effectiveness of using anti-leukotrienes in treatment for improvement of nasal symptom scores as well as quality of life of patients with seasonal rhinitis 12. However it was noted in the study there was not much difference between the treatment groups in the primary outcome while there was some difference in secondary outcomes from there been some minor differences The study noted that the dosing schedule for Montelukast was once daily evening time. And the onset of action is approx 3-6 hrs after ingestion. The impact of addition of Montelukast on PNTS was observed. Secondly the mean percent change in decreased turbinate swelling was significantly greater in the Montelukast group. This also strengthens the importance of using Montelukast in controlling AR symptom and underlying inflammation as well. Another study was conducted to compare the effectiveness of Montelukast combined with Loratadine once daily to Loratadine alone for a 2-week treatment course of allergic rhinitis in a randomized, double-blind placebo controlled trial which enrolled 115 children, 6-15 years old 13. The patients were randomly assigned to receive Montelukast and Loratadine (treatment group) or placebo and Page 33 of 70
34 Loratadine (control group). The primary outcome was the mean percent change of the total daytime nasal symptom scores (PDTS) and secondary outcomes were the mean percent changes of the nighttime nasal, daytime eye and composite symptom scores (PNTS, PES, PCS), as well as the nasal secretion, turbinate swelling and nasal congestion scores (PNSS, PTSS, PNCS). There were no significant differences in the PDTS of the 2 groups. The change in the night time nasal congestion score (PNTS-congestion) was higher in the treatment group, but not statistically significant (p = 0.077). Only the mean percent change in decreased turbinate swelling was significantly greater in the Montelukast and Loratadine group than the Loratadine alone group (-22 +/- 7 vs. -1 +/- 5, p less than 0.05). A randomized, placebo-controlled study was conducted to compare Montelukast plus Loratadine and Loratadine alone with respect to efficacy in the treatment of allergic rhinitis in 115 children ages 6-15 yr 13. Patients received Loratadine 5 or 10 mg depending on weight and Montelukast 5 mg (n=56) or Loratadine plus placebo (n=59) at bedtime for 2 wk. Patients completed daily rhinitis diary cards. The primary outcome was mean percent change in total daytime nasal symptom scores (PDTS). Secondary outcomes were mean percent change in nighttime nasal symptoms scores (PNTS), daytime eye symptoms scores (PES), composite symptoms scores (PCS), nasal secretion (PNSS), turbinate swelling (PTSS), and nasal congestion scores (PNCS). The combination group had significant improvement in turbinate swelling compared to the Loratadine group. The combination group also had greater improvements in PNTS, PDTS, PES, and PCS than the Loratadine group, but the differences were not significant. The authors conclude that Montelukast plus Loratadine had a significant effect on nasal congestion but not on other symptoms in children with allergic rhinitis 13. Leukotriene receptor antagonists (LTRAs) were recently added to the method of treating allergic rhinitis (AR). However, in children under 6 yr old, there has been Page 34 of 70
35 no study about its efficacy in treating AR. To compare the clinical efficacy of Montelukast, Cetirizine and placebo in the treatment of children from 2 to 6 yr old with perennial allergic rhinitis (PAR), to see if there are any significant differences 14. Sixty children were selected and treated with Montelukast, or Cetirizine, or placebo once daily 14. The efficacy of the three agents was compared with the Pediatric Rhino conjunctivitis Quality of Life Questionnaire (PRQLQ) and Total Symptom Score (TSS) by diary. In addition, Serum IgE, serum eosinophil cationic protein (ECP), blood eosinophil counts, nasal airway resistance (NAR) and eosinophil percentage in nasal smears were also examined. The results revealed that both Montelukast and Cetirizine were significantly efficacious compared with placebo in NAR, eosinophil percentage in nasal smears, PRQLQ, TSS and all symptom items except nasal itching, throat itching and tearing. For nasal itching, only Cetirizine was significantly efficacious. On the other hand, for night sleep quality, Montelukast was significantly superior to Cetirizine 14. A randomized, double-blind, placebo-controlled, parallel-group study was performed to compare the effects of oral Montelukast 4 mg once daily at bedtime (n=20; 11 M, 9 F, mean age 4.49 yr) with those of oral Cetirizine 5 mg once daily at bedtime (n=20; 12 M, 8 F mean age 4.53 yr) for 12 wk in 40 children (age 2-6 yr) with perennial allergic rhinitis; 20 children received placebo 14. After 12 wk of therapy, total symptoms scores had decreased significantly in the Montelukast and Cetirizine groups (both P<0.001); however, total symptoms scores were lower in the Cetirizine group than in the Montelukast group (P less than 0.05 between groups). Nasal itching decreased to a greater degree in the Cetirizine group than in the Montelukast group, while the quality of night sleep improved more in the Montelukast group than in the Cetirizine group. Pediatric Rhino conjunctivitis Quality of Life Questionnaire scores improved significantly in the Montelukast and Cetirizine groups over 12 wk of therapy (P=0.028 and P<0.001, respectively). Page 35 of 70
36 There were no significant changes in levels of serum IgE, serum eosinophil cationic protein, or blood eosinophil counts over 12 wk of therapy with Montelukast or Cetirizine. Nasal airway resistance values decreased significantly in the Montelukast and Cetirizine groups after 8 (P=0.007 and P=0.026, respectively) and 12 wk of therapy (P=0.007 and P=0.013, respectively). Similarly, the number of eosinophils in nasal smears decreased significantly in the Montelukast and Cetirizine groups over 12 wk of therapy (P=0.045 and P=0.004, respectively). Two children in the Cetirizine group experienced mild Cetirizineinduced sedation. The authors conclude that both Montelukast and Cetirizine are effective for the treatment of perennial allergic rhinitis in children 14. It was noted that Cetrizine has associated side effect of sedation, which is not associated with Montelukast. Also, the Quality of night sleep was better in Montelukast group as compared to cetrizine.considering therapeutic index (Efficacy and Side effect ratio) profile, Montelukast would be the preferred choice. Another study was carried out to investigate the role of treatment with Montelukast on symptoms, eno levels, and peripheral eosinophil counts of children with seasonal allergic rhinitis during pollen season 15. METHODS: A randomized, double-blind, parallel-group study performed between April and June 2005 in 57 children aged 7 to 14 years with seasonal allergic rhinitis was performed. The study comprised a 1-week screening period, a 1-week run-in period, and a 2-week treatment period with once daily Montelukast, 5 mg, or matching placebo. RESULTS: No significant difference at baseline was found in symptom scores, eno levels, and blood eosinophil counts between the treatment and placebo groups. After 2 weeks of Montelukast treatment, improvements from the baseline in the daytime nasal, composite, and daytime eye symptoms scores were significantly greater in the Montelukast group compared with the placebo group (P <.001, P Page 36 of 70
Montelukast Sodium. -A new class of seasonal allergic rhinitis therapy
 Montelukast Sodium -A new class of seasonal allergic rhinitis therapy Symptoms of Seasonal Allergic Rhinitis Nasal itch Sneezing Rhinorrhoea Nasal stuffiness Pathogenesis of Allergic Rhinitis Mast cells,
Montelukast Sodium -A new class of seasonal allergic rhinitis therapy Symptoms of Seasonal Allergic Rhinitis Nasal itch Sneezing Rhinorrhoea Nasal stuffiness Pathogenesis of Allergic Rhinitis Mast cells,
ARIA. At-A-Glance Pocket Reference 2007
 ARIA At-A-Glance Pocket Reference 2007 1 st Edition NEW ARIA UPDATE BASED ON THE ALLERGIC RHINITIS AND ITS IMPACT ON ASTHMA WORKSHOP REPORT In collaboration with the World Health Organisation, GA 2 LEN,
ARIA At-A-Glance Pocket Reference 2007 1 st Edition NEW ARIA UPDATE BASED ON THE ALLERGIC RHINITIS AND ITS IMPACT ON ASTHMA WORKSHOP REPORT In collaboration with the World Health Organisation, GA 2 LEN,
New Zealand Consumer Medicine Information
 New Zealand Consumer Medicine Information SINGULAIR montelukast sodium 4 mg, 5 mg & 10 mg tablets What is in this leaflet This leaflet answers some common questions about SINGULAIR. It does not contain
New Zealand Consumer Medicine Information SINGULAIR montelukast sodium 4 mg, 5 mg & 10 mg tablets What is in this leaflet This leaflet answers some common questions about SINGULAIR. It does not contain
SINGULAIR. Composition Each tablet/sachet contains:
 SINGULAIR TABLETS/CHEWABLE TABLETS/ORAL GRANULES Composition Each tablet/sachet contains: Active Ingredient Each 10 mg film-coated tablet contains 10.4 mg montelukast sodium, which is the molar equivalent
SINGULAIR TABLETS/CHEWABLE TABLETS/ORAL GRANULES Composition Each tablet/sachet contains: Active Ingredient Each 10 mg film-coated tablet contains 10.4 mg montelukast sodium, which is the molar equivalent
MANAGEMENT OF ALLERGIC RHINITIS SYMPTOMS IN THE PHARMACY
 ARIA_Pharm_PG 1/6/06 12:00 PM Page cov1 MANAGEMENT OF ALLERGIC RHINITIS SYMPTOMS IN THE PHARMACY POCKET GUIDE A Pocket Guide for Pharmacists 2003 BASED ON THE ALLERGIC RHINITIS AND ITS IMPACT ON ASTHMA
ARIA_Pharm_PG 1/6/06 12:00 PM Page cov1 MANAGEMENT OF ALLERGIC RHINITIS SYMPTOMS IN THE PHARMACY POCKET GUIDE A Pocket Guide for Pharmacists 2003 BASED ON THE ALLERGIC RHINITIS AND ITS IMPACT ON ASTHMA
SUMMARY OF PRODUCT CHARACTERISTICS 2 QUALITATIVE AND QUANTITATIVE COMPOSITION
 SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Montelukast 10 mg film-coated tablets 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One film-coated tablet contains montelukast sodium, which
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Montelukast 10 mg film-coated tablets 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One film-coated tablet contains montelukast sodium, which
APO-MONTELUKAST TABLET
 APO-MONTELUKAST TABLET NAME OF THE MEDICINE Montelukast sodium. Chemical Name: [R-(E)]-1-[[[1-[3-[2-(7-chloro-2-quinolinyl)ethenyl]phenyl]-3-[2-(1-hydroxy-1- methylethyl)phenyl]propyl]thio]methyl] cyclopropane
APO-MONTELUKAST TABLET NAME OF THE MEDICINE Montelukast sodium. Chemical Name: [R-(E)]-1-[[[1-[3-[2-(7-chloro-2-quinolinyl)ethenyl]phenyl]-3-[2-(1-hydroxy-1- methylethyl)phenyl]propyl]thio]methyl] cyclopropane
PRODUCT INFORMATION SINGULAIR. (montelukast sodium) Tablets NAME OF THE MEDICINE
 Tablets NAME OF THE MEDICINE") PRODUCT INFORMATION SINGULAIR (montelukast sodium) Tablets NAME OF THE MEDICINE Montelukast sodium SINGULAIR, (montelukast sodium) is described chemically as [R-(E)]-1-[[[1-[3-[2-(7- chloro-2-quinolinyl)ethenyl]phenyl]-3-[2-(1-hydroxy-1-methylethyl)phenyl]propyl]thio]methyl]
PRODUCT INFORMATION SINGULAIR (montelukast sodium) Tablets NAME OF THE MEDICINE Montelukast sodium SINGULAIR, (montelukast sodium) is described chemically as [R-(E)]-1-[[[1-[3-[2-(7- chloro-2-quinolinyl)ethenyl]phenyl]-3-[2-(1-hydroxy-1-methylethyl)phenyl]propyl]thio]methyl]
White, circular, biconvex, uncoated tablets with a score line on one side, plain on the other.
 Nausicalm Cyclizine hydrochloride Ph. Eur. 50 mg Presentation White, circular, biconvex, uncoated tablets with a score line on one side, plain on the other. Uses Actions The active ingredient-cyclizine
Nausicalm Cyclizine hydrochloride Ph. Eur. 50 mg Presentation White, circular, biconvex, uncoated tablets with a score line on one side, plain on the other. Uses Actions The active ingredient-cyclizine
PATIENT INFORMATION ABOUT TREATMENTS FOR ASTHMA AND ALLERGIC RHINITIS, PRESCRIPTIONS & OVER THE COUNTER MEDICINE
 PATIENT INFORMATION ABOUT TREATMENTS FOR ASTHMA AND ALLERGIC RHINITIS, PRESCRIPTIONS & OVER THE COUNTER MEDICINE The content of this booklet was developed by Allergy UK. MSD reviewed this booklet to comment
PATIENT INFORMATION ABOUT TREATMENTS FOR ASTHMA AND ALLERGIC RHINITIS, PRESCRIPTIONS & OVER THE COUNTER MEDICINE The content of this booklet was developed by Allergy UK. MSD reviewed this booklet to comment
PRODUCT INFORMATION (This PI contains all registered presentations of Avamys.) AVAMYS Nasal Spray
 AVAMYS Nasal Spray") PRODUCT INFORMATION (This PI contains all registered presentations of Avamys.) AVAMYS Nasal Spray NAME OF THE MEDICINE: Fluticasone furoate Structure: 21 F O 2 3 28 HO 19 1 10 5 4 O 20 S 18 12 O 11 13
PRODUCT INFORMATION (This PI contains all registered presentations of Avamys.) AVAMYS Nasal Spray NAME OF THE MEDICINE: Fluticasone furoate Structure: 21 F O 2 3 28 HO 19 1 10 5 4 O 20 S 18 12 O 11 13
Seasonal Allergies. 1995-2012 The Patient Education Institute, Inc. www.x-plain.com im010101 Last reviewed: 05/30/2012 1
 Seasonal Allergies Introduction Seasonal allergies are allergies that develop during certain times of the year. Seasonal allergies are usually a response to pollen from trees, grasses, and weeds. Constant
Seasonal Allergies Introduction Seasonal allergies are allergies that develop during certain times of the year. Seasonal allergies are usually a response to pollen from trees, grasses, and weeds. Constant
Public Assessment Report. Pharmacy to General Sales List Reclassification. Pirinase Hayfever Relief for Adults 0.05% Nasal Spray.
 Public Assessment Report Pharmacy to General Sales List Reclassification Pirinase Hayfever Relief for Adults 0.05% Nasal Spray (Fluticasone) PL 00079/0688 Glaxo Wellcome UK Limited TABLE OF CONTENTS Introduction
Public Assessment Report Pharmacy to General Sales List Reclassification Pirinase Hayfever Relief for Adults 0.05% Nasal Spray (Fluticasone) PL 00079/0688 Glaxo Wellcome UK Limited TABLE OF CONTENTS Introduction
A ragweed pollen as a treatment for a ragweed allergy? It s called immunotherapy.
 A ragweed pollen as a treatment for a ragweed allergy? It s called immunotherapy. RAGWITEK is a prescription medicine used for sublingual (under the tongue) immunotherapy to treat ragweed pollen allergies
A ragweed pollen as a treatment for a ragweed allergy? It s called immunotherapy. RAGWITEK is a prescription medicine used for sublingual (under the tongue) immunotherapy to treat ragweed pollen allergies
VISTARIL (hydroxyzine pamoate) Capsules and Oral Suspension
 Capsules and Oral Suspension") VISTARIL (hydroxyzine pamoate) Capsules and Oral Suspension DESCRIPTION Hydroxyzine pamoate is designated chemically as 1-(p-chlorobenzhydryl) 4- [2-(2-hydroxyethoxy) ethyl] diethylenediamine salt of 1,1
VISTARIL (hydroxyzine pamoate) Capsules and Oral Suspension DESCRIPTION Hydroxyzine pamoate is designated chemically as 1-(p-chlorobenzhydryl) 4- [2-(2-hydroxyethoxy) ethyl] diethylenediamine salt of 1,1
Nursing 113. Pharmacology Principles
 Nursing 113 Pharmacology Principles 1. The study of how drugs enter the body, reach the site of action, and are removed from the body is called a. pharmacotherapeutics b. pharmacology c. pharmacodynamics
Nursing 113 Pharmacology Principles 1. The study of how drugs enter the body, reach the site of action, and are removed from the body is called a. pharmacotherapeutics b. pharmacology c. pharmacodynamics
SUMMARY OF PRODUCT CHARACTERISTICS FOR MYTEKA 10MG TABLETS. Myteka (Montelukast Sodium) 10mg Film Coated Tablets.
 10mg Film Coated Tablets.") Trade Name: Myteka Generic Name: (Montelukast Sodium) Dosage: 10mg Film Coated Tablets Manufacturer Name: Hilton Pharma (Pvt.) Ltd, Karachi, Pakistan. Agent Name: Raheeg Medical Company SUMMARY OF PRODUCT
Trade Name: Myteka Generic Name: (Montelukast Sodium) Dosage: 10mg Film Coated Tablets Manufacturer Name: Hilton Pharma (Pvt.) Ltd, Karachi, Pakistan. Agent Name: Raheeg Medical Company SUMMARY OF PRODUCT
Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis, and asthma
 Chapter 31 Drugs Used to Treat Lower Respiratory Disease Learning Objectives Describe the physiology of respirations Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis,
Chapter 31 Drugs Used to Treat Lower Respiratory Disease Learning Objectives Describe the physiology of respirations Compare the physiologic responses of the respiratory system to emphysema, chronic bronchitis,
ASTHMA IN INFANTS AND YOUNG CHILDREN
 ASTHMA IN INFANTS AND YOUNG CHILDREN What is Asthma? Asthma is a chronic inflammatory disease of the airways. Symptoms of asthma are variable. That means that they can be mild to severe, intermittent to
ASTHMA IN INFANTS AND YOUNG CHILDREN What is Asthma? Asthma is a chronic inflammatory disease of the airways. Symptoms of asthma are variable. That means that they can be mild to severe, intermittent to
RSPT 2317 Non-steroidal anti-asthma agents
 RSPT 2317 Non-steroidal Anti-asthma Agents Mechanisms of Inflammation in Asthma Mechanisms of Inflammation in Asthma Asthma is a chronic inflammatory disorder of the airways It is divided into extrinsic
RSPT 2317 Non-steroidal Anti-asthma Agents Mechanisms of Inflammation in Asthma Mechanisms of Inflammation in Asthma Asthma is a chronic inflammatory disorder of the airways It is divided into extrinsic
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Letter Date March 27, 2007 Stamp Date March 28, 2007 PDUFA Goal Date January 28, 2008
 CLINICAL REVIEW Application Type NDA Submission Number 22-157 Submission Code Letter Date March 27, 2007 Stamp Date March 28, 2007 PDUFA Goal Date January 28, 2008 Reviewer Name Review Completion Date
CLINICAL REVIEW Application Type NDA Submission Number 22-157 Submission Code Letter Date March 27, 2007 Stamp Date March 28, 2007 PDUFA Goal Date January 28, 2008 Reviewer Name Review Completion Date
Get Your Head In The Game. Matthew Voorman, MD Hutchinson Clinic March 21, 2016
 Get Your Head In The Game Matthew Voorman, MD Hutchinson Clinic March 21, 2016 About Me Otolaryngology Head & Neck Surgery Geisinger Medical Center General Surgery University of California San Francisco
Get Your Head In The Game Matthew Voorman, MD Hutchinson Clinic March 21, 2016 About Me Otolaryngology Head & Neck Surgery Geisinger Medical Center General Surgery University of California San Francisco
Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age
 Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age Components of Severity Symptoms Intermittent 2 days/week Classification of Asthma Severity (0 4 years of age) Persistent
Classifying Asthma Severity and Initiating Treatment in Children 0 4 Years of Age Components of Severity Symptoms Intermittent 2 days/week Classification of Asthma Severity (0 4 years of age) Persistent
Medication Guide EQUETRO (ē-kwĕ-trō) (carbamazepine) Extended-Release Capsules
 (carbamazepine) Extended-Release Capsules") Medication Guide EQUETRO (ē-kwĕ-trō) (carbamazepine) Extended-Release Capsules Read this Medication Guide before you start taking EQUETRO and each time you get a refill. There may be new information. This
Medication Guide EQUETRO (ē-kwĕ-trō) (carbamazepine) Extended-Release Capsules Read this Medication Guide before you start taking EQUETRO and each time you get a refill. There may be new information. This
1. LAMICTAL may cause a serious skin rash that may cause you to be hospitalized or even cause death.
 MEDICATION GUIDE LAMICTAL (la-mik-tal) (lamotrigine) tablets LAMICTAL (lamotrigine) chewable dispersible tablets LAMICTAL ODT (lamotrigine) orally disintegrating tablets What is the most important information
MEDICATION GUIDE LAMICTAL (la-mik-tal) (lamotrigine) tablets LAMICTAL (lamotrigine) chewable dispersible tablets LAMICTAL ODT (lamotrigine) orally disintegrating tablets What is the most important information
Patient Medication Guide Brochure
 Patient Medication Guide Brochure 1 MEDICATION GUIDE TASIGNA (ta-sig-na) (nilotinib) Capsules Read this Medication Guide before you start taking TASIGNA and each time you get a refill. There may be new
Patient Medication Guide Brochure 1 MEDICATION GUIDE TASIGNA (ta-sig-na) (nilotinib) Capsules Read this Medication Guide before you start taking TASIGNA and each time you get a refill. There may be new
Guidance for Industry Safety Testing of Drug Metabolites
 Guidance for Industry Safety Testing of Drug Metabolites U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER) February 2008 Pharmacology
Guidance for Industry Safety Testing of Drug Metabolites U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER) February 2008 Pharmacology
Medication Guide TASIGNA (ta-sig-na) (nilotinib) Capsules
 (nilotinib) Capsules") Medication Guide TASIGNA (ta-sig-na) (nilotinib) Capsules Read this Medication Guide before you start taking Tasigna and each time you get a refill. There may be new information. This information does
Medication Guide TASIGNA (ta-sig-na) (nilotinib) Capsules Read this Medication Guide before you start taking Tasigna and each time you get a refill. There may be new information. This information does
Supplement Questions asked in the 1st International Basic Allergy Course
 Supplement Questions asked in the 1st International Basic Allergy Course 1. CLINICAL MANIFESTATION What is the percentage of people who have both combined food and inhalant? What is the difference between
Supplement Questions asked in the 1st International Basic Allergy Course 1. CLINICAL MANIFESTATION What is the percentage of people who have both combined food and inhalant? What is the difference between
treat nasal congestion that happens with seasonal allergic rhinitis in adults and children 2 years of age and older.
 Patient Information NASONEX [nā-zə-neks] (mometasone furoate monohydrate) Nasal Spray, 50 mcg FOR INTRANASAL USE ONLY Read the Patient Information that comes with NASONEX before you start using it and
Patient Information NASONEX [nā-zə-neks] (mometasone furoate monohydrate) Nasal Spray, 50 mcg FOR INTRANASAL USE ONLY Read the Patient Information that comes with NASONEX before you start using it and
Treatments for allergy are usually straightforward, safe and effective. Common treatments include:
 Allergy Medications The treatments prescribed for allergy control the symptoms and reactions; they do not cure the condition. However, using treatments as prescribed can show a huge change in a patient
Allergy Medications The treatments prescribed for allergy control the symptoms and reactions; they do not cure the condition. However, using treatments as prescribed can show a huge change in a patient
READ THIS FOR SAFE AND EFFECTIVE USE OF YOUR MEDICINE PATIENT MEDICATION INFORMATION. [new-ka la]
![READ THIS FOR SAFE AND EFFECTIVE USE OF YOUR MEDICINE PATIENT MEDICATION INFORMATION. [new-ka la]](/thumbs/35/17235501.jpg "READ THIS FOR SAFE AND EFFECTIVE USE OF YOUR MEDICINE PATIENT MEDICATION INFORMATION. [new-ka la]") READ THIS FOR SAFE AND EFFECTIVE USE OF YOUR MEDICINE PATIENT MEDICATION INFORMATION Pr NUCALA [new-ka la] mepolizumab lyophilized powder for subcutaneous injection Read this carefully before you start
READ THIS FOR SAFE AND EFFECTIVE USE OF YOUR MEDICINE PATIENT MEDICATION INFORMATION Pr NUCALA [new-ka la] mepolizumab lyophilized powder for subcutaneous injection Read this carefully before you start
PACKAGE LEAFLET: INFORMATION FOR THE USER. /.../ 2.5 mg orodispersible tablets. Desloratadine
 PACKAGE LEAFLET PACKAGE LEAFLET: INFORMATION FOR THE USER /.../ 2.5 mg orodispersible tablets Desloratadine Read all of this leaflet carefully before you start taking this medicine. - Keep this leaflet.
PACKAGE LEAFLET PACKAGE LEAFLET: INFORMATION FOR THE USER /.../ 2.5 mg orodispersible tablets Desloratadine Read all of this leaflet carefully before you start taking this medicine. - Keep this leaflet.
APC/DTC Briefing Document
 London New Drugs Group Page 1 APC/DTC Briefing Document Intranasal corticosteroids for allergic rhinitis SUMMARY Contents Summary 1 Recommendations 2 Background 2 Treatment 3 Intranasal corticosteroids
London New Drugs Group Page 1 APC/DTC Briefing Document Intranasal corticosteroids for allergic rhinitis SUMMARY Contents Summary 1 Recommendations 2 Background 2 Treatment 3 Intranasal corticosteroids
From the Text. Clinical Indications. Clinical Indications. RSPT 2217 Non-steroidal Anti-asthma Agents. RSPT 2317 Non-steroidal Antiasthma Agents
 From the Text RSPT 2317 Non-steroidal Antiasthma Agents Gardenhire Chapter 12 Key Terms and Definitions Page 226 Nonsteroidal Antiasthma Meds Table 12-1; page 228 Comparative Features of Antileukotriene
From the Text RSPT 2317 Non-steroidal Antiasthma Agents Gardenhire Chapter 12 Key Terms and Definitions Page 226 Nonsteroidal Antiasthma Meds Table 12-1; page 228 Comparative Features of Antileukotriene
Allergies and Autoimmune Inner Ear Disease
 Allergies and Autoimmune Inner Ear Disease Allergy is the term used to describe an over-reaction of the body to a substance that is normally harmless to most people. This substance is called an allergen,
Allergies and Autoimmune Inner Ear Disease Allergy is the term used to describe an over-reaction of the body to a substance that is normally harmless to most people. This substance is called an allergen,
Sponsor Novartis. Generic Drug Name Secukinumab. Therapeutic Area of Trial Psoriasis. Approved Indication investigational
 Clinical Trial Results Database Page 2 Sponsor Novartis Generic Drug Name Secukinumab Therapeutic Area of Trial Psoriasis Approved Indication investigational Clinical Trial Results Database Page 3 Study
Clinical Trial Results Database Page 2 Sponsor Novartis Generic Drug Name Secukinumab Therapeutic Area of Trial Psoriasis Approved Indication investigational Clinical Trial Results Database Page 3 Study
Package leaflet: Information for the patient. Bricanyl Tablets 5 mg terbutaline sulfate
 Package leaflet: Information for the patient Bricanyl Tablets 5 mg terbutaline sulfate Read all of this leaflet carefully before you start taking this medicine because it contains important information
Package leaflet: Information for the patient Bricanyl Tablets 5 mg terbutaline sulfate Read all of this leaflet carefully before you start taking this medicine because it contains important information
RAGWITEK TM (Short Ragweed Pollen Allergen Extract) Tablet for Sublingual Use Initial U.S. Approval: 2014
 Tablet for Sublingual Use Initial U.S. Approval: 2014") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use RAGWITEK safely and effectively. See full prescribing information for RAGWITEK. RAGWITEK TM (Short
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use RAGWITEK safely and effectively. See full prescribing information for RAGWITEK. RAGWITEK TM (Short
DO YOU HAVE ITCHY ALLERGY EYES? Find out about lasting relief
 DO YOU HAVE ITCHY ALLERGY EYES? Find out about lasting relief Common causes of itching due to eye allergies include: Pollen from trees, grasses, and ragweed Dust mites Cat dander Approximately 10 million
DO YOU HAVE ITCHY ALLERGY EYES? Find out about lasting relief Common causes of itching due to eye allergies include: Pollen from trees, grasses, and ragweed Dust mites Cat dander Approximately 10 million
Anaphylaxis Management. Pic 1 Severe allergic reaction which led to anaphylaxis
 1 Anaphylaxis Management Pic 1 Severe allergic reaction which led to anaphylaxis What is an allergic reaction? 2 An allergy is when someone has a reaction to something (usually a protein) which is either
1 Anaphylaxis Management Pic 1 Severe allergic reaction which led to anaphylaxis What is an allergic reaction? 2 An allergy is when someone has a reaction to something (usually a protein) which is either
Share the important information in this Medication Guide with members of your household.
 MEDICATION GUIDE BUPRENORPHINE (BUE-pre-NOR-feen) Sublingual Tablets, CIII IMPORTANT: Keep buprenorphine sublingual tablets in a secure place away from children. Accidental use by a child is a medical
MEDICATION GUIDE BUPRENORPHINE (BUE-pre-NOR-feen) Sublingual Tablets, CIII IMPORTANT: Keep buprenorphine sublingual tablets in a secure place away from children. Accidental use by a child is a medical
Montelukast Sodium Singulair, Merck. Development and Pharmacology: 1
 Montelukast Sodium Singulair, Merck Development and Pharmacology: 1 Asthma is a chronic inflammatory disease of the airways that is complicated by episodes of acute inflammation. Even patients with mild
Montelukast Sodium Singulair, Merck Development and Pharmacology: 1 Asthma is a chronic inflammatory disease of the airways that is complicated by episodes of acute inflammation. Even patients with mild
See 17 for PATIENT COUNSELING INFORMATION. Revised: 3/2016 FULL PRESCRIBING INFORMATION: CONTENTS* WARNING: ADRENAL CRISIS IN THE SETTING OF SHOCK OR
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LYSODREN safely and effectively. See full prescribing information for LYSODREN. LYSODREN (mitotane)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LYSODREN safely and effectively. See full prescribing information for LYSODREN. LYSODREN (mitotane)
PATIENT INFORMATION LEAFLET. CEFALEXIN 250 mg AND 500 mg CAPSULES CEFALEXIN
 PATIENT INFORMATION LEAFLET CEFALEXIN 250 mg AND 500 mg CAPSULES CEFALEXIN Read all of this leaflet carefully before you start taking this medicine. - Keep this leaflet. You may need to read it again.
PATIENT INFORMATION LEAFLET CEFALEXIN 250 mg AND 500 mg CAPSULES CEFALEXIN Read all of this leaflet carefully before you start taking this medicine. - Keep this leaflet. You may need to read it again.
MEDICATION GUIDE Savella (Sa-vel-la) (milnacipran HCl) Tablets
 (milnacipran HCl) Tablets") MEDICATION GUIDE Savella (Sa-vel-la) (milnacipran HCl) Tablets Savella is not used to treat depression, but it acts like medicines that are used to treat depression (antidepressants) and other psychiatric
MEDICATION GUIDE Savella (Sa-vel-la) (milnacipran HCl) Tablets Savella is not used to treat depression, but it acts like medicines that are used to treat depression (antidepressants) and other psychiatric
Allergy Shots and Allergy Drops for Adults and Children. A Review of the Research
 Allergy Shots and Allergy Drops for Adults and Children A Review of the Research Is This Information Right for Me? This information may be helpful to you if: Your doctor* has said that you or your child
Allergy Shots and Allergy Drops for Adults and Children A Review of the Research Is This Information Right for Me? This information may be helpful to you if: Your doctor* has said that you or your child
patient group direction
 DICLOFENAC v01 1/8 DICLOFENAC PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
DICLOFENAC v01 1/8 DICLOFENAC PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
Adjunctive psychosocial intervention. Conditions requiring dose reduction. Immediate, peak plasma concentration is reached within 1 hour.
 Shared Care Guideline for Prescription and monitoring of Naltrexone Hydrochloride in alcohol dependence Author(s)/Originator(s): (please state author name and department) Dr Daly - Consultant Psychiatrist,
Shared Care Guideline for Prescription and monitoring of Naltrexone Hydrochloride in alcohol dependence Author(s)/Originator(s): (please state author name and department) Dr Daly - Consultant Psychiatrist,
The Annual Direct Care of Asthma
 The Annual Direct Care of Asthma The annual direct health care cost of asthma in the United States is approximately $11.5 billion; indirect costs (e.g. lost productivity) add another $4.6 billion for a
The Annual Direct Care of Asthma The annual direct health care cost of asthma in the United States is approximately $11.5 billion; indirect costs (e.g. lost productivity) add another $4.6 billion for a
Core Safety Profile. Pharmaceutical form(s)/strength: 50mg tablets IE/H/PSUR/0028/002 Date of FAR: 17.07.2013
/strength: 50mg tablets IE/H/PSUR/0028/002 Date of FAR: 17.07.2013") Core Safety Profile Active substance: Naltrexone Hydrochloride Pharmaceutical form(s)/strength: 50mg tablets P-RMS: IE/H/PSUR/0028/002 Date of FAR: 17.07.2013 4.2 Posology and method of administration
Core Safety Profile Active substance: Naltrexone Hydrochloride Pharmaceutical form(s)/strength: 50mg tablets P-RMS: IE/H/PSUR/0028/002 Date of FAR: 17.07.2013 4.2 Posology and method of administration
PHOSPHATE-SANDOZ Tablets (High dose phosphate supplement)
") 1 PHOSPHATE-SANDOZ Tablets (High dose phosphate supplement) PHOSPHATE-SANDOZ PHOSPHATE-SANDOZ Tablets are a high dose phosphate supplement containing sodium phosphate monobasic. The CAS registry number
1 PHOSPHATE-SANDOZ Tablets (High dose phosphate supplement) PHOSPHATE-SANDOZ PHOSPHATE-SANDOZ Tablets are a high dose phosphate supplement containing sodium phosphate monobasic. The CAS registry number
Anaphylaxis: a severe, life threatening allergic reaction usually involving swelling, trouble breathing, and can progress to shock
 Allergy is a condition in which the immune system causes sneezing, itching, rashes, and wheezing, or sometimes even life-threatening allergic reactions. The more you know about allergies, the better prepared
Allergy is a condition in which the immune system causes sneezing, itching, rashes, and wheezing, or sometimes even life-threatening allergic reactions. The more you know about allergies, the better prepared
Medicines Use Review Supporting Information for Asthma Patients
 Medicines Use Review Supporting Information for Asthma Patients What is asthma? Asthma is a chronic inflammatory disorder of the airways. The inflammation causes an associated increase in airway hyper-responsiveness,
Medicines Use Review Supporting Information for Asthma Patients What is asthma? Asthma is a chronic inflammatory disorder of the airways. The inflammation causes an associated increase in airway hyper-responsiveness,
**Form 1: - Consultant Copy** Telephone Number: Fax Number: Email: Author: Dr Bernard Udeze Pharmacist: Claire Ault Date of issue July 2011
 Effective Shared Care Agreement for the treatment of Dementia in Alzheimer s Disease Donepezil tablets / orodispersible tablets (Aricept / Aricept Evess ) These forms (1 and 2) are to be completed by both
Effective Shared Care Agreement for the treatment of Dementia in Alzheimer s Disease Donepezil tablets / orodispersible tablets (Aricept / Aricept Evess ) These forms (1 and 2) are to be completed by both
9/16/2014. Anti-Immunoglobulin E (IgE) Omalizumab (Xolair ) Dosing Guidance
 Omalizumab (Xolair ) Dosing Guidance") Disclosure Statement of Financial Interest New Therapies for Asthma Including Omalizumab and Anti-Cytokine Therapies Marsha Dangler, PharmD, BCACP Clinical Pharmacy Specialist James H. Quillen VA Medical
Disclosure Statement of Financial Interest New Therapies for Asthma Including Omalizumab and Anti-Cytokine Therapies Marsha Dangler, PharmD, BCACP Clinical Pharmacy Specialist James H. Quillen VA Medical
MEDICATION GUIDE WELLBUTRIN (WELL byu-trin) (bupropion hydrochloride) Tablets
 (bupropion hydrochloride) Tablets") MEDICATION GUIDE WELLBUTRIN (WELL byu-trin) (bupropion hydrochloride) Tablets Read this Medication Guide carefully before you start using WELLBUTRIN and each time you get a refill. There may be new information.
MEDICATION GUIDE WELLBUTRIN (WELL byu-trin) (bupropion hydrochloride) Tablets Read this Medication Guide carefully before you start using WELLBUTRIN and each time you get a refill. There may be new information.
Biologic Treatments for Rheumatoid Arthritis
 Biologic Treatments Rheumatoid Arthritis (also known as cytokine inhibitors, TNF inhibitors, IL 1 inhibitor, or Biologic Response Modifiers) Description Biologics are new class of drugs that have been
Biologic Treatments Rheumatoid Arthritis (also known as cytokine inhibitors, TNF inhibitors, IL 1 inhibitor, or Biologic Response Modifiers) Description Biologics are new class of drugs that have been
DRUG INTERACTIONS: WHAT YOU SHOULD KNOW. Council on Family Health
 DRUG INTERACTIONS: WHAT YOU SHOULD KNOW Council on Family Health Drug Interactions There are more opportunities today than ever before to learn about your health and to take better care of yourself. It
DRUG INTERACTIONS: WHAT YOU SHOULD KNOW Council on Family Health Drug Interactions There are more opportunities today than ever before to learn about your health and to take better care of yourself. It
1. NAME OF THE MEDICINAL PRODUCT. Impavido 10 mg capsules Impavido 50 mg capsules 2. QUALITATIVE AND QUANTITATIVE COMPOSITION. 1 capsule contains:
 1. NAME OF THE MEDICINAL PRODUCT Impavido 10 mg capsules Impavido 50 mg capsules 2. QUALITATIVE AND QUANTITATIVE COMPOSITION 1 capsule contains: Impavido 10 mg capsules 10 mg Miltefosine. Impavido 50 mg
1. NAME OF THE MEDICINAL PRODUCT Impavido 10 mg capsules Impavido 50 mg capsules 2. QUALITATIVE AND QUANTITATIVE COMPOSITION 1 capsule contains: Impavido 10 mg capsules 10 mg Miltefosine. Impavido 50 mg
MEDGUIDE SECTION. What is the most important information I should know about SEROQUEL? SEROQUEL may cause serious side effects, including:
 MEDGUIDE SECTION Medication Guide SEROQUEL (SER-oh-kwell) (quetiapine fumarate) Tablets Read this Medication Guide before you start taking SEROQUEL and each time you get a refill. There may be new information.
MEDGUIDE SECTION Medication Guide SEROQUEL (SER-oh-kwell) (quetiapine fumarate) Tablets Read this Medication Guide before you start taking SEROQUEL and each time you get a refill. There may be new information.
MEDICATION GUIDE KOMBIGLYZE XR (kom-be-glyze X-R) (saxagliptin and metformin HCl extended-release) tablets
 (saxagliptin and metformin HCl extended-release) tablets") MEDICATION GUIDE KOMBIGLYZE XR (kom-be-glyze X-R) (saxagliptin and metformin HCl extended-release) tablets Read this Medication Guide carefully before you start taking KOMBIGLYZE XR and each time you get
MEDICATION GUIDE KOMBIGLYZE XR (kom-be-glyze X-R) (saxagliptin and metformin HCl extended-release) tablets Read this Medication Guide carefully before you start taking KOMBIGLYZE XR and each time you get
Update and Review of Medication Assisted Treatments
 Update and Review of Medication Assisted Treatments for Opiate and Alcohol Use Disorders Richard N. Whitney, MD Medical Director Addiction Services Shepherd Hill Newark, Ohio Medication Assisted Treatment
Update and Review of Medication Assisted Treatments for Opiate and Alcohol Use Disorders Richard N. Whitney, MD Medical Director Addiction Services Shepherd Hill Newark, Ohio Medication Assisted Treatment
Package Leaflet: Information for the user. <Levetiracetam 750 mg, film-coated tablets> <Levetiracetam 1000 mg, film-coated tablets> Levetiracetam
 Package Leaflet: Information for the user
Package Leaflet: Information for the user
Summary of the risk management plan (RMP) for Otezla (apremilast)
 for Otezla (apremilast)") EMA/741412/2014 Summary of the risk management plan (RMP) for Otezla (apremilast) This is a summary of the risk management plan (RMP) for Otezla, which details the measures to be taken in order to ensure
EMA/741412/2014 Summary of the risk management plan (RMP) for Otezla (apremilast) This is a summary of the risk management plan (RMP) for Otezla, which details the measures to be taken in order to ensure
ZOVIRAX Cold Sore Cream
 Data Sheet ZOVIRAX Cold Sore Cream Aciclovir 5% w/w Presentation Topical cream Indications ZOVIRAX Cold Sore Cream is indicated for the treatment of Herpes simplex virus infections of the lips and face
Data Sheet ZOVIRAX Cold Sore Cream Aciclovir 5% w/w Presentation Topical cream Indications ZOVIRAX Cold Sore Cream is indicated for the treatment of Herpes simplex virus infections of the lips and face
MEDICATION GUIDE. (topiramate) Tablets. Sprinkle Capsules
 Tablets. Sprinkle Capsules") MEDICATION GUIDE TOPAMAX (TOE-PA-MAX) (topiramate) Tablets TOPAMAX (TOE-PA-MAX) (topiramate) Sprinkle Capsules Read this Medication Guide before you start taking TOPAMAX and each time you get a refill.
MEDICATION GUIDE TOPAMAX (TOE-PA-MAX) (topiramate) Tablets TOPAMAX (TOE-PA-MAX) (topiramate) Sprinkle Capsules Read this Medication Guide before you start taking TOPAMAX and each time you get a refill.
ICH Topic S 1 A The Need for Carcinogenicity Studies of Pharmaceuticals. Step 5
 European Medicines Agency July 1996 CPMP/ICH/140/95 ICH Topic S 1 A The Need for Carcinogenicity Studies of Pharmaceuticals Step 5 NOTE FOR GUIDANCE ON THE NEED FOR CARCINOGENICITY STUDIES OF PHARMACEUTICALS
European Medicines Agency July 1996 CPMP/ICH/140/95 ICH Topic S 1 A The Need for Carcinogenicity Studies of Pharmaceuticals Step 5 NOTE FOR GUIDANCE ON THE NEED FOR CARCINOGENICITY STUDIES OF PHARMACEUTICALS
JANUVIA sitagliptin phosphate 25 mg, 50 mg & 100 mg tablets
 JANUVIA sitagliptin phosphate 25 mg, 50 mg & 100 mg tablets What is in this leaflet This leaflet answers some common questions about JANUVIA. It does not contain all the available information. It does
JANUVIA sitagliptin phosphate 25 mg, 50 mg & 100 mg tablets What is in this leaflet This leaflet answers some common questions about JANUVIA. It does not contain all the available information. It does
Drugs for MS.Drug fact box cannabis extract (Sativex) Version 1.0 Author
 Version 1.0 Author") Version History Policy Title Drugs for MS.Drug fact box cannabis extract (Sativex) Version 1.0 Author West Midlands Commissioning Support Unit Publication Date Jan 2013 Review Date Supersedes/New (Further
Version History Policy Title Drugs for MS.Drug fact box cannabis extract (Sativex) Version 1.0 Author West Midlands Commissioning Support Unit Publication Date Jan 2013 Review Date Supersedes/New (Further
SR 5. W2364A_NT.XATRAL SR5 PAK/SA 5/12/05 9:47 Page 1
 W2364A_NT.XATRAL SR5 PAK/SA 5/12/05 9:47 Page 1 alfuzosin SR 5 mg (Alfuzosin HCI) COMPOSITION Each sustained-release, film-coated tablet contains: Alfuzosin hydrochloride......... 5 mg Excipients... q.s.
W2364A_NT.XATRAL SR5 PAK/SA 5/12/05 9:47 Page 1 alfuzosin SR 5 mg (Alfuzosin HCI) COMPOSITION Each sustained-release, film-coated tablet contains: Alfuzosin hydrochloride......... 5 mg Excipients... q.s.
MEDICATION GUIDE. TOPAMAX (TOE-PA-MAX) (topiramate) Tablets and Sprinkle Capsules
 (topiramate) Tablets and Sprinkle Capsules") MEDICATION GUIDE TOPAMAX (TOE-PA-MAX) (topiramate) Tablets and Sprinkle Capsules Read this Medication Guide before you start taking TOPAMAX and each time you get a refill. There may be new information.
MEDICATION GUIDE TOPAMAX (TOE-PA-MAX) (topiramate) Tablets and Sprinkle Capsules Read this Medication Guide before you start taking TOPAMAX and each time you get a refill. There may be new information.
Guidelines for anaphylaxis emergency medication (adrenaline [epinephrine] autoinjector) prescription
![Guidelines for anaphylaxis emergency medication (adrenaline [epinephrine] autoinjector) prescription](/thumbs/33/15971578.jpg "Guidelines for anaphylaxis emergency medication (adrenaline [epinephrine] autoinjector) prescription") Guidelines for anaphylaxis emergency medication (adrenaline [epinephrine] autoinjector) prescription Introduction The aim of these guidelines is to outline the appropriate prescription of adrenaline (epinephrine)
Guidelines for anaphylaxis emergency medication (adrenaline [epinephrine] autoinjector) prescription Introduction The aim of these guidelines is to outline the appropriate prescription of adrenaline (epinephrine)
Travel to Africa 2005. David V. Diamond, MD MIT Medical Department
 Travel to Africa 2005 David V. Diamond, MD MIT Medical Department 1 General Advice: Overall risks are low for diseases other than Traveler's diarrhea Preventative measures to avoid exposure to mosquito
Travel to Africa 2005 David V. Diamond, MD MIT Medical Department 1 General Advice: Overall risks are low for diseases other than Traveler's diarrhea Preventative measures to avoid exposure to mosquito
Guide to. Allergies 020 8742 7042. A guide to allergies
 If you need advice on taking over-the-counter medicines speak to a pharmacist or call the Consumer Health Information Centre s Over-the-Counter Medicines Advice Line on 020 8742 7042. The advice line is
If you need advice on taking over-the-counter medicines speak to a pharmacist or call the Consumer Health Information Centre s Over-the-Counter Medicines Advice Line on 020 8742 7042. The advice line is
I B2.4. Design of the patient information leaflet for VariQuin
 (English translation of official Dutch version) I B2.4. Design of the patient information leaflet for VariQuin Information for the Patient: Read this package leaflet carefully when you have some time to
(English translation of official Dutch version) I B2.4. Design of the patient information leaflet for VariQuin Information for the Patient: Read this package leaflet carefully when you have some time to
Wobenzym. Wobenzym Keeps you moving.
 Wobenzym PS Helps to maintain healthy joints, mobility and flexibility Relief from everyday aches, pains and muscle soreness Speeds recovery following exertion Supported by over 200 clinical trials Wobenzym
Wobenzym PS Helps to maintain healthy joints, mobility and flexibility Relief from everyday aches, pains and muscle soreness Speeds recovery following exertion Supported by over 200 clinical trials Wobenzym
Naloxone Hydrochloride Injection PRODUCT INFORMATION
 Naloxone Hydrochloride Injection PRODUCT INFORMATION DESCRIPTION Naloxone hydrochloride is 17-allyl-4,5α-epoxy-3,14-dihydroxymorphinan-6-one hydrochloride; C 19 H 21 NO 4.HCl. It is an off-white powder
Naloxone Hydrochloride Injection PRODUCT INFORMATION DESCRIPTION Naloxone hydrochloride is 17-allyl-4,5α-epoxy-3,14-dihydroxymorphinan-6-one hydrochloride; C 19 H 21 NO 4.HCl. It is an off-white powder
(NON-PRESCRIPTION) LEAFLET: USER INFORMATION. CALTRATE VITAMIN D3 600mg/400 IU, film-coated tablet Calcium and Cholecalciferol
 LEAFLET: USER INFORMATION. CALTRATE VITAMIN D3 600mg/400 IU, film-coated tablet Calcium and Cholecalciferol") (NON-PRESCRIPTION) LEAFLET: USER INFORMATION CALTRATE VITAMIN D3 600mg/400 IU, film-coated tablet Calcium and Cholecalciferol Read all of this leaflet carefully because it contains important information
(NON-PRESCRIPTION) LEAFLET: USER INFORMATION CALTRATE VITAMIN D3 600mg/400 IU, film-coated tablet Calcium and Cholecalciferol Read all of this leaflet carefully because it contains important information
Pre-Operative Services Teaching Rounds 2 Jan 2011
 Pre-Operative Services Teaching Rounds 2 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 2 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Stepping toward a different treatment option LEARN WHAT ACTHAR CAN DO FOR YOU
 FOR MS RELAPSES Stepping toward a different treatment option LEARN WHAT ACTHAR CAN DO FOR YOU As a person with multiple sclerosis (MS), you know firsthand the profound impact MS relapses can have on your
FOR MS RELAPSES Stepping toward a different treatment option LEARN WHAT ACTHAR CAN DO FOR YOU As a person with multiple sclerosis (MS), you know firsthand the profound impact MS relapses can have on your
PACKAGE LEAFLET: INFORMATION FOR THE USER. Alvesco 40, 80 and 160 mcg Inhaler Ciclesonide
 PACKAGE LEAFLET PACKAGE LEAFLET: INFORMATION FOR THE USER Alvesco 40, 80 and 160 mcg Inhaler Ciclesonide Read all of this leaflet carefully before you start using this medicine because it contains important
PACKAGE LEAFLET PACKAGE LEAFLET: INFORMATION FOR THE USER Alvesco 40, 80 and 160 mcg Inhaler Ciclesonide Read all of this leaflet carefully before you start using this medicine because it contains important
Review of Pharmacological Pain Management
 Review of Pharmacological Pain Management CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation The WHO Pain Ladder The World Health Organization
Review of Pharmacological Pain Management CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation The WHO Pain Ladder The World Health Organization
Clinical Study Synopsis for Public Disclosure
 abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis - which is part of the clinical
abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis - which is part of the clinical
Elements for a Public Summary
 VI.2 Elements for a Public Summary VI.2.1 Overview of Disease Epidemiology Hunter syndrome is a rare genetic disease which mainly affects males of all ethnicities. The incidence rate ranges from 0.6 to
VI.2 Elements for a Public Summary VI.2.1 Overview of Disease Epidemiology Hunter syndrome is a rare genetic disease which mainly affects males of all ethnicities. The incidence rate ranges from 0.6 to
MEDICATION GUIDE. Bupropion Hydrochloride (bue-proe-pee-on HYE-droe-KLOR-ide) Extended-Release Tablets, USP (SR)
 Extended-Release Tablets, USP (SR)") MEDICATION GUIDE Bupropion Hydrochloride (bue-proe-pee-on HYE-droe-KLOR-ide) Extended-Release Tablets, USP (SR) Read this Medication Guide carefully before you start taking bupropion hydrochloride extendedrelease
MEDICATION GUIDE Bupropion Hydrochloride (bue-proe-pee-on HYE-droe-KLOR-ide) Extended-Release Tablets, USP (SR) Read this Medication Guide carefully before you start taking bupropion hydrochloride extendedrelease
Immunology and immunotherapy in allergic disease
 Immunology and immunotherapy in allergic disease Jing Shen, MD Faculty Advisor: Matthew Ryan, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation February 2005
Immunology and immunotherapy in allergic disease Jing Shen, MD Faculty Advisor: Matthew Ryan, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation February 2005
Acamprosate calcium APOLLO 91991 46 950 950
 Acamprosate calcium APOLLO 91991 46 950 950 Acamprosate calcium APOLLO 91991 46 950 950 Acamprosate calcium CAS Number : 77337-73-6 Molecular Weight : 400.48 g/mol Molecular Formula : 2C5H10NO4S.Ca Systematic
Acamprosate calcium APOLLO 91991 46 950 950 Acamprosate calcium APOLLO 91991 46 950 950 Acamprosate calcium CAS Number : 77337-73-6 Molecular Weight : 400.48 g/mol Molecular Formula : 2C5H10NO4S.Ca Systematic
Cough, as a leading symptom, would certainly be in the top 10 of reasons for seeing a GP.
 COUGH Cough, as a leading symptom, would certainly be in the top 10 of reasons for seeing a GP. A cough in a child seems to cause more concern, even when it has not been present very long, whereas in adults
COUGH Cough, as a leading symptom, would certainly be in the top 10 of reasons for seeing a GP. A cough in a child seems to cause more concern, even when it has not been present very long, whereas in adults
Self Treatment for Seasonal Allergies. Veena Toledo, Pharm D LifeConnections Pharmacy
 Self Treatment for Seasonal Allergies Veena Toledo, Pharm D LifeConnections Pharmacy Agenda Topics Oral Antihistamines and Decongestants Nasal Sprays Eye drops Non-drug Alternatives evidence / efficacy
Self Treatment for Seasonal Allergies Veena Toledo, Pharm D LifeConnections Pharmacy Agenda Topics Oral Antihistamines and Decongestants Nasal Sprays Eye drops Non-drug Alternatives evidence / efficacy
Montelukast 10mg film-coated tablets PL 17907/0474
 Montelukast 10mg film-coated tablets PL 17907/0474 UKPAR TABLE OF CONTENTS Lay Summary Page 2 Scientific Discussion Page 4 Steps Taken for Assessment Page 11 Steps Taken After Initial Authorisation Page
Montelukast 10mg film-coated tablets PL 17907/0474 UKPAR TABLE OF CONTENTS Lay Summary Page 2 Scientific Discussion Page 4 Steps Taken for Assessment Page 11 Steps Taken After Initial Authorisation Page
Low Molecular Weight Heparin. All Wales Medicines Strategy Group (AWMSG) Recommendations and advice
 Recommendations and advice") Low Molecular Weight Heparin All Wales Medicines Strategy Group (AWMSG) Recommendations and advice Starting Point Low Molecular Weight Heparin (LMWH): Inhibits factor Xa and factor IIa (thrombin) Small
Low Molecular Weight Heparin All Wales Medicines Strategy Group (AWMSG) Recommendations and advice Starting Point Low Molecular Weight Heparin (LMWH): Inhibits factor Xa and factor IIa (thrombin) Small
Package leaflet: Information for the user Naltrexone Hydrochloride 50 mg film-coated tablets Naltrexone Hydrochloride
 Package leaflet: Information for the user Naltrexone Hydrochloride 50 mg film-coated tablets Naltrexone Hydrochloride Read all of this leaflet carefully before you start taking this medicine because it
Package leaflet: Information for the user Naltrexone Hydrochloride 50 mg film-coated tablets Naltrexone Hydrochloride Read all of this leaflet carefully before you start taking this medicine because it
Human Clinical Study for Free Testosterone & Muscle Mass Boosting
 Human Clinical Study for Free Testosterone & Muscle Mass Boosting GE Nutrients, Inc. 920 E. Orangethorpe Avenue, Suite B Anaheim, California 92801, USA Phone: +1-714-870-8723 Fax: +1-732-875-0306 Contact
Human Clinical Study for Free Testosterone & Muscle Mass Boosting GE Nutrients, Inc. 920 E. Orangethorpe Avenue, Suite B Anaheim, California 92801, USA Phone: +1-714-870-8723 Fax: +1-732-875-0306 Contact
Stowe School Medications Policy
 INTRODUCTION Most pupils will need medication at some stage of their school life. Although this will mainly be for short periods there are a few pupils with chronic conditions who may require regular medication
INTRODUCTION Most pupils will need medication at some stage of their school life. Although this will mainly be for short periods there are a few pupils with chronic conditions who may require regular medication
ALBERTA IMMUNIZATION POLICY GUIDELINES
 ALBERTA IMMUNIZATION POLICY GUIDELINES Hepatitis Vaccines. Hepatitis A Vaccines Refer to the vaccine product monograph and the Canadian Immunization Guide for further Product monographs are available on
ALBERTA IMMUNIZATION POLICY GUIDELINES Hepatitis Vaccines. Hepatitis A Vaccines Refer to the vaccine product monograph and the Canadian Immunization Guide for further Product monographs are available on
Teriflunomide (Aubagio) 14mg once daily tablet
 14mg once daily tablet") Teriflunomide (Aubagio) 14mg once daily tablet Exceptional healthcare, personally delivered Your Consultant Neurologist has suggested that you may benefit from treatment with Teriflunomide. The decision
Teriflunomide (Aubagio) 14mg once daily tablet Exceptional healthcare, personally delivered Your Consultant Neurologist has suggested that you may benefit from treatment with Teriflunomide. The decision
INTERNATIONAL CONFERENCE ON HARMONISATION OF TECHNICAL REQUIREMENTS FOR REGISTRATION OF PHARMACEUTICALS FOR HUMAN USE S1A. Current Step 4 version
 INTERNATIONAL CONFERENCE ON HARMONISATION OF TECHNICAL REQUIREMENTS FOR REGISTRATION OF PHARMACEUTICALS FOR HUMAN USE ICH HARMONISED TRIPARTITE GUIDELINE GUIDELINE ON THE NEED FOR CARCINOGENICITY STUDIES
INTERNATIONAL CONFERENCE ON HARMONISATION OF TECHNICAL REQUIREMENTS FOR REGISTRATION OF PHARMACEUTICALS FOR HUMAN USE ICH HARMONISED TRIPARTITE GUIDELINE GUIDELINE ON THE NEED FOR CARCINOGENICITY STUDIES
Bayer Receives FDA Approval for BETACONNECT First and Only Electronic Autoinjector in Relapsing-Remitting Multiple Sclerosis (RRMS) Treatment
 Treatment") News Release Intended for U.S. Media Only Bayer Receives FDA Approval for BETACONNECT First and Only Electronic Autoinjector in Relapsing-Remitting Multiple Sclerosis (RRMS) Treatment Whippany, N.J., September
News Release Intended for U.S. Media Only Bayer Receives FDA Approval for BETACONNECT First and Only Electronic Autoinjector in Relapsing-Remitting Multiple Sclerosis (RRMS) Treatment Whippany, N.J., September