S T A T E O F C A L I F O R N I A SAVINGS PLUS PROGRAM
|
|
|
- Derick Rich
- 8 years ago
- Views:
Transcription
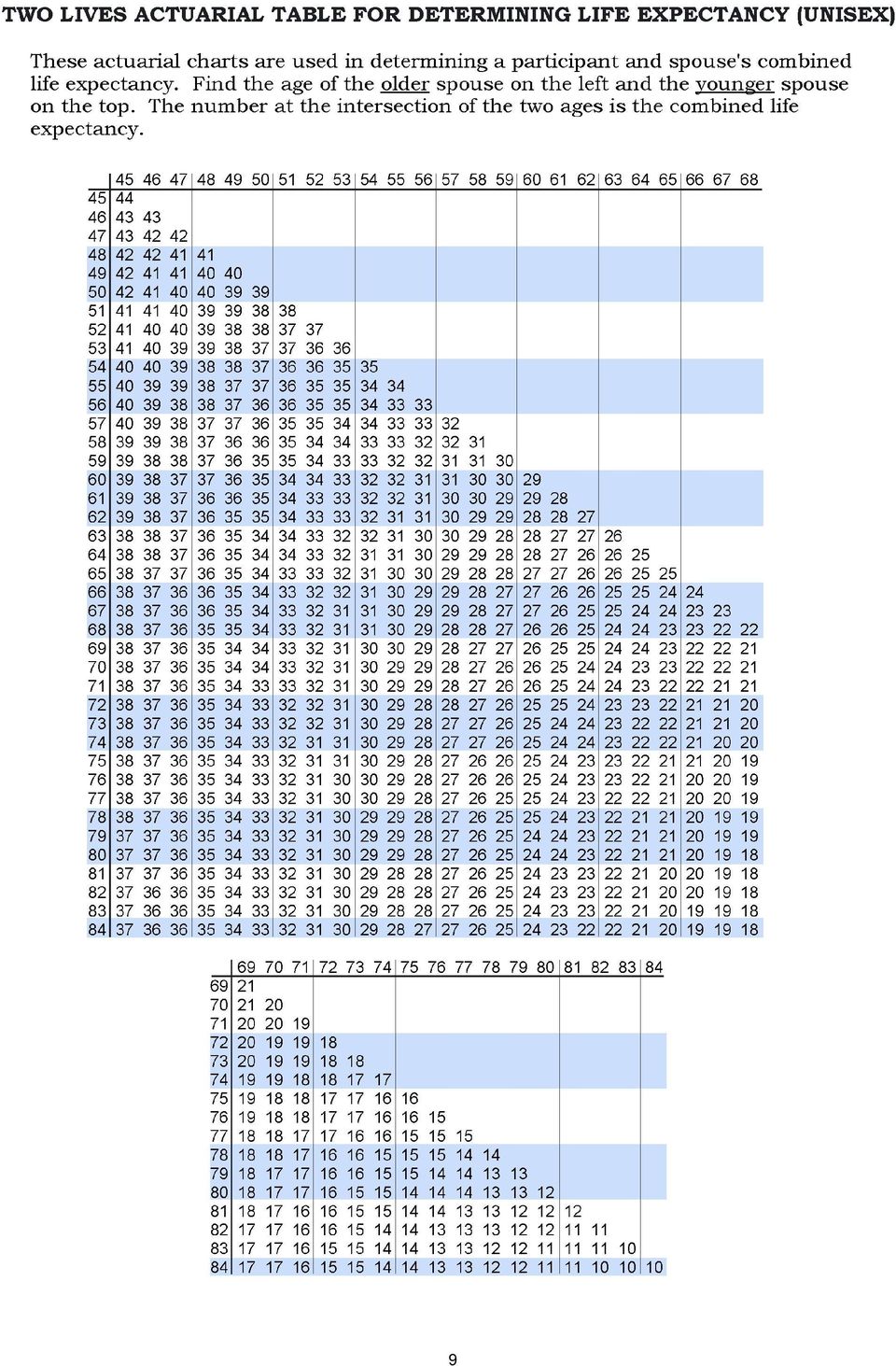
1 STATE OF CALIFORNIA SAVINGS PLUS PROGRAM 457 Deferred Compensation Plan BENEFIT PAYMENT APPLICATION Many of the decisions you make relating to receiving benefits payments from your 457 DCP have restrictions, such as the commencement date and method of payment. Your decisions will have financial consequences as well as income tax implications. Therefore, you may wish to obtain the advice of a professional tax advisor and/or retirement planner before you request a payment of your benefits. This package contains these forms: 457 Deferred Compensation Plan Benefit Payment Application 457 Deferred Compensation Plan Beneficiary Designation Form Direct Deposit Application Specific Investment Designation Certification to Delay Commencement of Payments Annuity Quotation Request Form Annuity Purchase Application IRS FormW-4 Employee s Withholding Allowance Certificate These instructions summarize the Federal and State of California tax rules that may apply to your payment. The tax rules are complex and contain many conditions and exceptions that are not included in these instructions. Therefore, you may want to consult with a professional tax advisor and/or retirement planner before you request a payment of your benefits from the Plan. You can find more specific information on the tax treatment of payments from qualified retirement plans in Internal Revenue Service (IRS) Publication 575, Pension and Annuity Income, and IRS Publication 590, Individual Retirement Arrangements. These publications are available from your local IRS office or by calling TAX-FORM ( ). DC-3516 (12/00) 1

2 This page is intentionally left blank. 2

3 PAYMENT METHODS LUMP SUM PAYMENT A request for a lump sum payment means that a check will be issued to you for your entire account balance. Lump sum payments are reported to the IRS as ordinary income. You may submit a W-4 form for tax withholding. Your lump sum payment check will be mailed to your address as indicated on your Benefit Payment Application (BPA) and will change your address of record. A W-4 form is included in this packet or can be requested from NRS or received from the Internal Revenue Service. PARTIAL LUMP SUM PAYMENT This option allows you to select a specific dollar amount (partial lump sum) upon your commencement date and your choice of periodic payments for a fixed number of years or for a fixed amount. Or you may select a partial lump sum payment and purchase an annuity with the remainder. Partial Lump Sum payment with the remainder as Periodic payments If you select to receive the balance of your 457 DCP in periodic payments, the periodic payments must begin no later than December 31 st of the year following your partial lump sum payment. Please review the Periodic Payment instructions to determine the frequency and amount of your periodic payments. Your partial lump sum check will be mailed to your address as indicated on your BPA and will change your address of record. Example: If you elect to receive a partial lump sum payment in October 2000, with the remainder in periodic payments, you will have to begin the periodic payments no later than December Partial Lump Sum Payment with the remainder as an Annuity Purchase If you choose to purchase an annuity, the premium amount (purchase price of the annuity) will be the remaining value of your account after the partial lump sum is deducted. Please review the information in this package on Annuities and submit the Annuity Quotation Request form to Nationwide Retirement Solutions (NRS) before submitting the payment application packet. Example: If your account balance is $100,000 and you elect to receive $15,000 as a partial lump sum payment, the premium amount for your annuity purchase will be $85,000 (the remaining value of your account). PERIODIC PAYMENTS The Periodic payment option permits you to choose monthly or annual payments. You can specify either:! Fixed Period the length of time over which you will receive your funds; or! Fixed Amount the specific dollar amount that you designate Payments may be spread over a minimum of one year and maximum of your life expectancy, or, the combined life expectancy of you and your beneficiary. Refer to the Life Expectancy Charts in this package. Funds are withdrawn from your account on the designated day you elect to create your periodic payment. See page 7 (Payment Dates) for more information on the NRS periodic payment process. Investment Options and periodic payments If you have monies in more than one investment fund, your periodic payments will be prorated among all of your core options unless you elect a Specific Investment Designation. The Specific Investment Designation allows you to choose one of your existing funds from which your periodic payments will be withdrawn. Only one payment (check or direct deposit) will be issued, regardless of the number of investments you maintain. Personal Choice Retirement Account (PCRA) 1 If you have assets in a PCRA, your selected method of payment applies to both the PCRA and your core account. Your account value for all purposes includes the total value of your core account plus the value of your PCRA. Payments will be 1 Formerly known as the Self Directed Account. 3

4 made from your core account only. You are not required to liquidate all PCRA assets before payments begin. However, you must retain sufficient assets in your core account to cover the upcoming three months of distributions or 50% of your total account value, whichever is greater. PERIODIC PAYMENT METHODS Fixed Period Payments You can choose to receive monthly or annual payments. Your payments are calculated by dividing your account balance by the number of payments that you wish to receive. Your payments will be recalculated each month (if on monthly payout), or each year (if on annual payout), so your account balance will be exhausted at the end of your payment schedule. Example: Lois retired with a 457 DCP account of $50,000. She elected to receive 10 annual payments. Assume an annual account growth rate of 6% your account will be distributed per its actual rate of growth. Payout Year Account Balance $50,000 47,700 44,944 41,685 37,873 33,454 28,369 22,553 15,938 8,447 Annual Payment $5,000 5,300 5,618 5,955 6,312 6,690 7,092 7,517 7,969 8,447 Fixed Amount Payments This option allows you to receive payments of the same amount within each year. Beginning the second calendar year, your fixed amount will increase each year based on the federally defined Cost of Living Adjustment (COLA). If your payments continue beyond age 70½, your payment amount may increase to ensure that your funds are paid within your life expectancy in accordance with Internal Revenue Code regulations. Your life expectancy, for purposes of the Fixed Amount Payment option, will be based on the birth dates you provide. You may only use your designated beneficiary s birth date or age in combination with your own for determining your joint life expectancy. If you have multiple designated beneficiaries you may only use the eldest beneficiary s birth date or age in determining your joint life expectancy. If you do not wish to select a joint life expectancy do not provide your beneficiary s birth date. The SPP will automatically use your single life expectancy if you only provide your birth date. Minimum Fixed Amount Requirement Your specified dollar amount must be at least equal to the following: Annual Payments Divide your current account value by the number of years according to your life expectancy. Monthly Payments Divide your current account value by the number of years according to your life expectancy. Divide the dollar value you arrived at by 12 (number of months in the year). Example #1 Example #2 Example #3 Bob has a current balance of $40,000 and is selecting Fixed Amount payments of $2,000 annually. He is sixty-five years old with a single life expectancy of twenty years. Since his Fixed Amount is equal to the amount derived by dividing his account balance by his life expectancy ($40,000 divided by 20 years = $2,000), his request would comply with the requirement. Sally has a current balance of $60,000 and is selecting Fixed Amount payments of $1,500 monthly. She is currently fifty-five years old and her spouse is sixty-two years old therefore she has a joint life expectancy of thirty-one years. Since her Fixed Amount is more than the amount derived by dividing her account balance by her joint life expectancy divided by twelve months ($60,000 divided by 31 years = $1,935 divided by 12 months = $161), her request would comply with the requirement. Marie has a current balance of $35,000 and is selecting Fixed Amount payments of $1,000 annually. She is currently fifty-seven years old with a single life expectancy of twenty-six years. Since her Fixed amount is less that the amount derived by dividing her account balance by her life expectancy ($35,000 divided by 26 years = $1,346), her request would not comply with the requirement. 4

5 Annual test at age 70½ If there are funds remaining in your account at age 70½, an annual test will be performed to determine if your payments at the current rate will extend beyond your life expectancy. This test is performed by dividing the value of your account balance on the last working day in December (beginning in the year you attain age 70½) by the maximum number of payments allowed, pursuant to your life expectancy. If the test determines that the life expectancy dollar amount is greater than the predetermined fixed dollar amount (including COLA increase), your payment amount will increase accordingly. Why an annual test at age 70½ is performed Section 457 of the IRC incorporates the required minimum distribution regulations of Section 401(a). These sections require your funds to be distributed within your applicable single or joint life expectancy. An adjustment to increase your payment amount may be necessary to ensure payments do not extend beyond your life expectancy. PURCHASE OF AN ANNUITY If you are considering the purchase of an annuity with your 457 Deferred Compensation Account, you must first complete the attached Annuity Quotation Form and submit to NRS. Several types of fixed annuities are available through Savings Plus. NRS will mail the quotations within 7-10 business days. Annuity quotations disclose how much you would receive each month from each form of annuity, based on a given premium. The amount of the monthly payment will depend on the form of annuity, the annuity provider, and premium amount for purchase. What is an Annuity? An annuity is a binding agreement between an individual (the annuitant) and a specific life insurance company. The life insurance company agrees to provide fixed monthly payments for the annuitant s lifetime (variable annuities are not available through this plan). The annuity is purchased with a single cash payment (the premium) in return for guaranteed monthly payments commencing immediately. Annuity purchases are subject to the following charges: An administrative fee to the insurance company. The tax laws of some states, including California, require that a premium tax be paid on the purchase of all annuities. The tax rate is set by the California Constitution as a percentage of the purchase price. As of the date this package was printed, the premium tax for the 457 Plan is 2.35%. Insurance companies issuing annuities deduct the amount of this premium tax from the gross proceeds of your 457 account and apply the net proceeds to the purchase of your annuity. Forms of annuities Life Only: The annuitant receives monthly payments commencing immediately and continuing throughout his/her lifetime. There will be no benefits payable to a beneficiary after the annuitant s death. Period certain and life: A specific term of 5, 10, or 15 years is selected when the annuity is purchased. The annuitant receives monthly payments throughout his or her lifetime. If he or she dies within a 5-year, 10-year, or 15-year period, the designated beneficiary will receive payments equal to the amount the annuitant was receiving for the remainder of the term. If the annuitant dies after the 5-year,10-year or 15-year period, the designated beneficiary will not receive any benefits pursuant to this option. Life with installment refund: The annuitant receives monthly payments throughout his or her lifetime. If he or she dies, the difference (if any) between the amount paid to purchase the annuity and the total amount received will be paid in a lump sum to the designated beneficiary. Joint and survivor : This form of annuity is purchased with either 50% or 100% survivor benefits. The primary annuitant receives monthly payments throughout his or her lifetime. In the event the primary annuitant dies, the survivor annuitant continues to receive payments throughout his or her lifetime at either 50% or 100% of the amount paid to the primary annuitant. Period certain with joint and survivor: This form of annuity is purchased with either 50% or 100% survivor benefits, and it requires the primary annuitant to name a survivor annuitant (usually the primary annuitant s spouse). This form of annuity also has a term of 5, 10, or 15 years, selected when the annuity is purchased. The primary annuitant receives monthly payments throughout his or her lifetime. If the primary annuitant predeceases the survivor annuitant within a 5-year, 10-year, or 15-year period, the survivor annuitant will receive payments equal to the amount the primary annuitant was receiving for the remainder of the term. At the end of the term, the survivor annuitant will receive payments for the remainder of his or her lifetime at either 50% or 100% of the amount paid to the primary annuitant. If both the primary annuitant and the survivor annuitant die within the term 5
, your payment amount will increase")
6 selected, payments will be made to a secondary beneficiary for the rest of the term, in the same amount the primary annuitant was receiving. GENERAL INFORMATION Changing the method of payment You can change the method of payment before payments begin by providing a written notice to this effect to NRS at least 60 days before your first payment. Once your payment schedule has begun, Internal Revenue Code (IRC) regulations and the annuity providers prohibit the suspension of payment and any change in the method of payment. You may not close out your deferred compensation account any earlier than the final payment determined according to the payment schedule you selected, unless you meet the eligibility criteria for an Unforeseeable Emergency Withdrawal. If you are granted an Unforeseeable Emergency Withdrawal, your account balance will be reduced by the amount granted; however, your payment schedule will remain the same. Specific Investment Designation (Optional Partial Lump Sum and Periodic Payments Only) Specific investment designations only apply to Partial Lump Sum and Periodic (Fixed Amount or Fixed Period, monthly or annual) payments. The designation of a specific investment is optional. Do not complete a designation if you want your periodic payments to be prorated from all of your core investments, or if you have monies in only one core option. You are responsible for ensuring the investments you designate has a value sufficient to satisfy the full payment amount. If, on the day assets will be surrendered to create the payment being made, the amount of the periodic payment exceeds the value of the investment designated, this designation shall be deemed void. Your periodic payments will then be prorated from among all of your core funds. You will be notified by mail when and if this occurs. All future periodic payments will also be prorated from among your core account until you submit a new Specific Investment Designation form. Annual review of the account occurs in January. If the payment is for a greater amount than the investment has available, the withdrawal would be pro-rated from the core account. You may submit a new designation at any time while you are receiving periodic payments. NRS must receive the completed designation no later than the month prior to make the change effective with your next periodic payment. Direct Deposit Information (Periodic Payments Only) You may request direct deposit if you are requesting periodic payments. If you are requesting a partial lump sum with the remainder of your account paid in periodic payments, you can use this section to have only your periodic payments directly deposited. Account Information If your payment is to be deposited into a checking account, you must attach a check marked VOID to your Direct Deposit Form. ACH Routing Number Include the nine-digit Automated Clearinghouse (ACH) routing number for your bank. If you leave the routing number blank but complete the remainder of this section, a check will be mailed to your bank. The fee for mailing each check is $2.00. Bank Mailing Address Your bank s mailing address is required for your first periodic payment to be mailed to your bank before direct deposit begins in the event your application is processed too late to make the first payment by direct deposit. No fee will be charged for mailing this first check to your bank or for any payment made by direct deposit. Updating and changing your direct deposit information You are responsible for providing the above information and updating it as needed. If the account number changes, you must submit a direct deposit form with the correct account number. The same applies if your bank name, bank mailing address, account type, or routing number changes. Instructions to change this information will not be accepted from anyone other than the participant, including your bank. If problems occur with direct deposit NRS will notify you if your bank reports any problems with the direct deposit process. Your direct deposit request will be cancelled and checks will be mailed to your mailing address of record until we receive a new direct deposit form. The fee for mailing each check is $

7 Payment Dates Payments are processed and issued on the designated day you elect. Assets will be surrendered on that date and a check or ACH will be sent according to NRS payment process. Your first payment cannot be processed unless NRS receives all necessary forms at least 60 days before the payment commencement date. NRS directly deposits or mails payments within three (3) working days from the date assets were surrendered. The payments are generated weekly. Payments will be paid based on the date range into which each falls. The date ranges are the 1 st through the 7 th, the 8 th through the 14 th, the 15 th through the 21 st, and the 22 nd through the end of the month. For each date range, the checks will be mailed on the second business day of the range. For example, if you request a payment date on the 20 th day of the month, this date falls between the 15 th through the 21 st. Therefore, NRS will mail a check on the 2 nd business day of the range (the 17 th if it is not on a weekend or holiday). Be sure to allow for appropriate mail or federal reserve processing time for distribution payments. Lost or Stolen checks If a check is mailed to you or your bank, it can be reported lost or stolen if it is not received after 14 days from check issuance. Check mailing fee (periodic payments only) If you have not selected direct deposit to your bank account, your check will be mailed to you or your bank. The fee for mailing each check is $2.00. Certification to Delay Commencement of Payments The Certification to Delay Commencement of Payments allows you to postpone the date your payments begin. You can use this option if you decide that you do not want to begin payments on the date you had originally selected. You may only use the Certification to Delay Commencement of Payments once. The Certification to Delay Commencement of Payments must be received by NRS no later than 30 days before the month in which your first payment is scheduled to begin. American General and Nationwide Accumulation Annuities If you have assets invested in American General and/or Nationwide annuities, please call NRS [(866) ] for an additional application. You must submit a specific American General and/or Nationwide payment application in order to begin your payments. W-4 FORM INSTRUCTIONS The W-4 Form instructs NRS how much State and Federal income tax to withhold from your payments. If you do not complete a W-4 Form, taxes will be withheld at the rate of single with zero allowances. If you choose to complete a W-4, you are required to complete the Employee Withholding Allowance Certificate portion of the W-4 Form. You must enter your name, address, and Social Security Number. You are not required to complete the Personal Allowances Worksheet or the Deductions and Adjustments Worksheet. A W-2 will be issued by January 31 st of the following year for tax reporting purposes. Tax Withholding Information If you live outside of California California cannot impose income tax on your deferred compensation payments if you live in another state. Therefore, State taxes will not automatically be withheld if your mailing address is outside of California. However, if you wish to have State taxes withheld, print a specific instruction in the bottom margin of the W-4 Form. Be sure to specify the state for which you wish to have taxes withheld. The following states do not have State income tax: Alaska, Florida, Hawaii, Nevada, New Hampshire, Pennsylvania, South Dakota, Tennessee, Texas, Washington, and Wyoming. Tax withholding rate Your tax withholding for your deferred compensation payments does not take into account any other income you may receive. At any time you may request a W-4 Form to change your tax withholding. Exemption from withholding 7

8 If you claim exemption from tax withholding in box 7 of the W-4 Form, taxes will not be withheld. However, IRS regulations require you to renew your exempt status by February 15 th of each year. You can do this by requesting, completing, and submitting a new W-4 Form. Failure to do so may result in the change of your tax withholding status to a rate of single and zero allowances. 8

9 9
10 UNISEX - ONE LIFE ACTUARIAL TABLE FOR DETERMINING LIFE EXPECTANCY The following chart should be used to determine your life expectancy. Age Life Expectancy in Years Age Life Expectancy in Years

11 STATE OF CALIFORNIA SAVINGS PLUS PROGRAM 457 DEFERRED COMPENSATION PLAN BENEFIT PAYMENT APPLICATION LAST NAME FIRST NAME MI SOCIAL SECURITY NUMBER ADDRESS PARTICIPANT S BIRTH DATE MONTH DATE YEAR CITY STATE ZIP CODE BENEFICIARY S BIRTH DATE (JOINT LIFE EXPECTANCY) MONTH DATE YEAR RETIREMENT/SEPARATION DATE ADDRESS DAYTIME TELEPHONE NUMBER WITH AREA CODE ( ) Privacy Statement: The Information Practices Act of 1977 (Civil Code Section ) and the Federal Privacy Act (Public Law ) require that this notice be provided when collecting personal information from individuals. Information requested on this form is used by the Savings Plus Program for purposes of identification and account processing. It is mandatory that you furnish all information requested on this form. Failure to provide mandatory information may result in action requested not being processed. Commencement Date Election Payment will begin on the commencement date you elect. Your commencement date cannot be deferred beyond March of the year after you attain age 70 ½. You may choose to postpone your commencement date, as long as payments have not begun. You may only postpone your commencement date one time. Issue Payment immediately (within 60 days) Issue payment on / / Month Day Year Method of Payment Lump Sum Payment (total account balance) OR; Partial Lump Sum Amount $ AND Periodic Payment (complete the Periodic Payment Method box below) or Annuity Purchase (see note) OR; Periodic Payments (complete the Periodic Payment Method box below) OR; Annuity Purchase (see note) Periodic Payments /Annuity to begin / / MONTH DAY YEAR Periodic Payment Method (select one) Fixed Period Fixed Amount $ specify number of years Monthly payments Annual payments Monthly payments Annual payments Note: You must request an Annuity Quotation and an annuity payment application from NRS before submitting form Participant Certification I request distribution to be made in accordance with the Plan regulations and my election above. I understand it is within the authority of the State of California to approve or disapprove this request. I hereby certify under penalty of perjury that this information is true and accurate to the best of my knowledge. " Signature Date 11
 and the Federal Privacy Act (Public Law 93-579) require that this notice be provided when collecting personal information from individuals.")
12 457 DCP BENEFIT PAYMENT APPLICATION INFORMATION Commencement Date Election You must elect a commencement date (a date that your payments will begin) and method of payment within 60 days after your date of retirement or separation. (Once your payment begins, you cannot change your payment method or the length of time over which you will receive them. This decision is irrevocable.) However, you may postpone commencement date one time so long as payments have not begun. You cannot receive payment before the original commencement date. Proof of Eligibility to Withdraw Funds Your eligibility to withdraw funds is verified before payment is issued. To facilitate faster processing of your application, you may provide proof of separation. For most State employees, a Notice of Personnel Action (NOPA) is issued to you by your personnel office upon separation. If you do not have a NOPA, a letter from your employer is acceptable. The letter must be on letterhead and reference your date of retirement or separation. Maximum Duration To Defer Payment If you have retired or separated, you must begin payment by March of the year after you attain age 70½. If you have continued State employment beyond age 70½, you may choose to receive payment or to defer payment for a maximum of 60 days (March) after the year in which you retire or separate. Failure to Respond If you do not return the completed application within 60 days, you are deemed to have elected a lump sum payment. Payment will be issued 180 days from date of separation or retirement. Methods of Payment You have a choice of payment methods. Please review the attached material for more information about the options and complete the forms applicable for the payment options you have selected. Payment choices are as follows: Lump Sum Payment Partial Lump Sum payment with remainder as Periodic Payments or Annuity Purchase Periodic Payments Purchase of an Annuity Returning Forms Return all applicable forms with your application. If you wish to purchase an annuity, please enclose a copy of the current annuity quotation for the annuity provider you have selected. Send your completed application and form to: Nationwide Retirement Solutions One Nationwide Plaza PW Columbus, OH

13 STATE OF CALIFORNIA SAVINGS PLUS PROGRAM 457 DEFERRED COMPENSATION PLAN BENEFICIARY DESIGNATION FORM PARTICIPANT INFORMATION LAST NAME FIRST NAME MI SOCIAL SECURITY NUMBER ADDRESS (STREET, CITY, STATE, ZIP CODE) MARITAL STATUS # NOT MARRIED (WIDOWED, DIVORCED, OR SINGLE) # MARRIED DAYTIME TELEPHONE NUMBER ( ) DATE OF BIRTH MONTH DAY YEAR The Information Privacy Act of 1977 (Civil Code Section ) and the Federal Privacy Act (Public Law ) require that this notice be provided when collecting personal information from individuals. The Savings Plus Program uses information requested on this form for purposes of identification and account processing. It is mandatory that you furnish all information requested on this form. Failure to provide mandatory information may result in action requested not being processed. BENEFICIARY INFORMATION I HEREBY DESIGNATE THE FOLLOWING PRIMARY BENEFICIARY(IES) TO RECEIVE MY FUNDS UPON MY DEATH. IN THE EVENT I SURVIVE THE PRIMARY BENEFICIARY(IES) DESIGNATED BELOW, I DESIGNATE THE FOLLOWING CONTINGENT BENEFICIARY(IES) TO RECEIVE MY FUNDS UPON MY DEATH. LAST NAME FIRST NAME MI RELATIONSHIP % SOCIAL SECURITY NUMBER ADDRESS (STREET, CITY, STATE, ZIP CODE) # PRIMARY # CONTINGENT LAST NAME FIRST NAME MI RELATIONSHIP % SOCIAL SECURITY NUMBER ADDRESS (STREET, CITY, STATE, ZIP CODE) # PRIMARY # CONTINGENT LAST NAME FIRST NAME MI RELATIONSHIP % SOCIAL SECURITY NUMBER ADDRESS (STREET, CITY, STATE, ZIP CODE) # PRIMARY # CONTINGENT # Additional beneficiaries are listed on an attached sheet of paper (identified as Primary or Contingent). A Trust can be named as a primary beneficiary or a contingent beneficiary. A trust can also be designated to be a Sole beneficiary or to Share and Share Alike with co-beneficiaries. Please indicate in the appropriate boxes how you want your trust to be designated. TRUST INFORMATION TRUST NAME DATE OF TRUST % # PRIMARY # CONTINGENT ADDRESS (STREET, CITY, STATE, ZIP CODE) NAME OF TRUSTEE PARTICIPANT CERTIFICATION I hereby certify under penalty of perjury that the information on this form is true and accurate to the best of my knowledge. " SIGNATURE DATE [DC-3496 (12/00)] 13

14 STATE OF CALIFORNIA SAVINGS PLUS PROGRAM 457 DEFERRED COMPENSATION PLAN BENEFICIARY DESIGNATION FORM INSTRUCTIONS Please read carefully before completing the designation. To designate a beneficiary, complete and sign the Beneficiary Designation form. Any change, including the address of a beneficiary, requires that you submit a completed Beneficiary Designation form. Changes will be effective upon receipt. Please retain a copy for your records. If you fail to designate a specific beneficiary(s), your account will be paid to your Estate or Trust. You may designate as many primary beneficiaries as you wish. If needed, attach an additional sheet of paper that includes your social security number, signature, and the date. You are not required to provide your beneficiary s social security number, however, the absence of that number may hinder the ability to locate/identify your beneficiary. If more than one Primary Beneficiaries is listed, your funds will be divided equally unless you clearly state otherwise. Should a primary beneficiary predecease you, funds will be paid/divided among any remaining primary beneficiaries designated. If there are no primary beneficiaries, funds will be paid/divided among any contingent beneficiaries designated. You may designate as many contingent beneficiaries as you wish. The contingent beneficiaries will not receive any portion of your funds if any primary beneficiary is living. If more than one contingent beneficiary is listed, your funds will be divided equally unless you clearly state otherwise. You may designate a trust as your beneficiary to be paid in lieu of your estate. Special rules may apply to estates and trusts. You are advised to contact a tax or estate planning professional before designating your estate or trust as beneficiary. Your beneficiary designation generally supercedes any other designation such as by a Will, Trust, Estate, etc. It is extremely important that you keep your designation consistent with your wishes. Nationwide Retirement Solutions One Nationwide Plaza PW Columbus, OH Voice Response System: (866) available 24 hours per day, 7 days per week Customer Service (866) available 8:30 a.m. 4:00 p.m. Monday Friday TDD (916) [DC-3496 (12/00)] 14

15 STATE OF CALIFORNIA SAVINGS PLUS PROGRAM SPECIFIC INVESTMENT DESIGNATION PARTICIPANT INFORMATION LAST NAME FIRST NAME MI SOCIAL SECURITY NUMBER ADDRESS ADDRESS CITY STATE ZIP CODE DAYTIME TELEPHONE NUMBER WITH AREA CODE ( ) Privacy Statement: The Information Practices Act of 1977 (Civil Code Section ) and the Federal Privacy Act (Public Law ) require that this notice be provided when collecting personal information from individuals. Information requested on this form is used by the Savings Plus Program for purposes of identification and account processing. It is mandatory that you furnish all information requested on this form. Failure to provide mandatory information may result in action requested not being processed. SPECIFIC INVESTMENT DESIGNATION I understand that all payments will be withdrawn from one specified investment option, so long as the value of the option is sufficient for the payment amount. Please withdraw my periodic payment from the option checked below: Dwight Asset Management Guaranteed Insurance Contract Savings Pool CalPERS U.S. Treasury Short-Term Fund CalPERS U.S. Treasury Intermediate-Term Bond Vanguard Total Bond Market Index Fund Vanguard GNMA Fund Hartford Advisors HLS Fund Domini Social Equity Fund Hartford Stock Fund HLS Fund CalPERS S & P 500 Index Fund Vanguard U.S. Growth Fund Federated Stock Trust Institutional Fund T. Rowe Price Mid-Cap. Growth Fund Accessor Small to Mid-Cap. Fund Franklin Balance Sheet Investment Fund Glenmede Institutional International Equity Fund Investor Destinations Conservative Fund Investor Destinations Moderately Conservative Fund Investor Destinations Moderate Fund Investor Destinations Moderately Aggressive Fund Investor Destinations Aggressive PARTICIPANT CERTIFICATION I authorize Savings Plus to withdraw my payments from the investment options designated above. I certify I have read the Privacy Statement and the instructions on completing this designation and agree to all the terms. " SIGNATURE DATE 15

16 INSTRUCTIONS FOR COMPLETING THE SPECIFIC INVESTMENT OPTIONS DESIGNATION FORM 1. Specific investment designations only apply to partial lump sum and periodic (fixed amount or fixed period, monthly or annual) payments. Specific investment designations do not apply to Lump Sum payments or to the purchase of an annuity. 2. The designation of a specific investment is optional. Do not complete a designation if you want your periodic payments to be prorated from all of your core account, or if you have assets in only one core option. 3. You are responsible for ensuring the investment you designate has a value sufficient to satisfy the full payment amount. If, on the day that assets will be surrendered to create the payment being made, the amount of the periodic payment exceeds the value of the fund you have designated, this designation shall be deemed void. Your periodic payments will then be prorated from among all of your core funds. You will be notified by mail when and if this occurs. All future periodic payments will also be prorated from among all of your core funds until you submit a new Specific Investment Designation form. 4. You may submit this designation at any time while you are receiving periodic payments. The recordkeeper must receive the completed designation no later than the month prior to make the change effective with your next periodic payment. Note: You may not change the designated fund or cancel this designation once submitted, except as indicated above. If you have any questions, please call (866) between 8:30 a.m. and 4:00 p.m., Monday - Friday to speak with a Customer Service Representative. RETURN FORM TO : Nationwide Retirement Solutions One Nationwide Plaza PW Columbus, OH

17 STATE OF CALIFORNIA SAVINGS PLUS PROGRAM DIRECT DEPOSIT FORM New (ESTABLISHES DIRECT DEPOSIT) Change (MODIFIES EXISTING DIRECT DEPOSIT INFORMATION) Cancel Direct Deposit (A check will be mailed to address of record) Participant Information LAST NAME FIRST NAME MI SOCIAL SECURITY NUMBER ADDRESS DATE OF BIRTH CITY STATE ZIP CODE DAYTIME TELEPHONE NUMBER WITH AREA CODE ( ) Privacy Statement: The Information Practices Act of 1977 (Civil Code Section ) and the Federal Privacy Act (Public Law ) require that this notice be provided when collecting personal information from individuals. Information requested on this form is used by the Savings Plus Program for purposes of identification and account processing. It is mandatory that you furnish all information requested on this form. Failure to provide mandatory information may result in action requested not being processed. ACCOUNT INFORMATION Account Type: Checking (Check marked void attached) Savings ACH Routing Number (9 digits) Account Number (Not to exceed 17 digits) BANK INFORMATION BANK NAME BANK MAILING ADDRESS CITY STATE ZIP CODE PARTICIPANT CERTIFICATION I authorize Savings Plus to make direct deposits to the account identified above effective immediately. I certify I have read the instructions on completing this application and the information regarding direct deposits " SIGNATURE DATE 17
 and the Federal Privacy Act (Public Law 93-579) require that this notice be provided when collecting personal information from individuals.")
18 INSTRUCTIONS FOR COMPLETING THE DIRECT DEPOSIT FORM: 1. Check New if this direct deposit application establishes a direct deposit. 2. Check Change if this direct deposit application modifies existing direct deposit information. 3. Check Cancel Direct Deposit if you no longer wish to receive a direct deposit. A check will be mailed to your address of record. A $2.00 fee will be charged for mailing each check. 4. Participant Information Provide all information requested. 5. Account Information Include the nine-digit Automated clearinghouse (ACH) routing number for your bank. Attach a check marked void for an electronic fund transfer to your checking account. Attach a deposit slip marked void for an electronic fund transfer to your savings account. If you do not have a savings account deposit slip, it can be obtained from your banking institution. Include your account number. 6. Bank Information Provide the name and mailing address of your bank. The bank mailing address is necessary because we may mail a check to your bank before the direct deposit begins. 7. Participant Signature Sign and date the application. INFORMATION: 1. Direct deposit is available for periodic (annual or monthly) payments only. Lump sum and partial payments will be mailed to your address of record. 2. You are responsible for providing the direct deposit information and updating it as needed. If your account number changes, you must submit another direct deposit application with the correct account number. The same applies if your bank name, bank mailing address, account type, or routing number changes. 3. Changes to these instructions will not be accepted from anyone except you, including your bank. Your signature is required to change or cancel your direct deposit. 4. We will notify you if your bank reports any problems with the direct deposit process. We will cancel your direct deposit request if this occurs. We will then mail payments to your mailing address of record until we receive a new direct deposit application. The fee for mailing each check is $ If you submit a completed application 30 days or more before your first payment, the first payment can usually be made through direct deposit. If you are already receiving payments, direct deposit changes will begin days after the completed application is received. We will mail one payment to your bank free of charge. After that time, we will make payments through direct deposit. If you have any questions, please call (866) between 8:30 a.m. and 4:00 p.m., Monday - Friday to speak with a Customer Service Representative. RETURN FORM TO: Nationwide Retirement Solutions One Nationwide Plaza PW Columbus, OH
 routing number for your bank. Attach a check marked void for an electronic fund transfer to your checking account.")
19 STATE OF CALIFORNIA SAVINGS PLUS PROGRAM CERTIFICATION TO DELAY COMMENCEMENT OF PAYMENTS The Federal Small Business Job Protection Act of 1996 was signed into law effective January 1, This law made several favorable changes to Internal Revenue Code section 457 with authorizes and regulates the tax aspects of deferred compensation programs for state and local government employees. Specifically, if you separated or retired and had elected a commencement date of January 1997 or later for distribution from your account, the law permits a one-time delay in the election of the commencement date. The new commencement date becomes irrevocable. Payment must commence by March of the year after you attain age 70 ½. PARTICIPANT INFORMATION LAST NAME FIRST NAME MI SOCIAL SECURITY NUMBER ADDRESS DATE OF BIRTH MONTH DAY YEAR CITY STATE ZIP CODE DAYTIME TELEPHONE NUMBER WITH AREA CODE ( ) Privacy Statement - The Information Practices Act of 1977 (Civil Code Section ) and the Federal Privacy Act (public Law ) require that this notice be provided when collecting personal information from individuals. Information requested on this form is used by the Savings Plus Program for purposes of information and account processing and will be kept confidential in accordance with the Information Practices Act. It is mandatory that you furnish all information requested on this form. Failure to provide such information may result in actions requested not being processed. COMMENCEMENT DATE CHANGE THIS DATE CAN ONLY BE POSTPONED, NOT ACCELERATED. Original commencement date: New commencement date: PARTICIPANT CERTIFICATION I certify I have read the information and understand that my signature below authorizes Savings Plus to delay the start date of my deferred compensation distribution. I understand that this certification is irrevocable as this date can only be postponed not accelerated and that payment must commence by March of the year after I attain age 70 ½. " SIGNATURE DATE If you have any questions, please call (866) between 8:30 a.m. and 4:00 p.m. to speak with Customer Service Representative. RETURN FORM TO: Nationwide Retirement Solutions One Nationwide Plaza PW Columbus, OH

20 This page is intentionally left blank. 20

21 STATE OF CALIFORNIA SAVINGS PLUS PROGRAM ANNUITY QUOTATION REQUEST FORM SECTION 1 ANNUITANT INFORMATION Name Street Address City/State/Zip Code Social Security Number Home Phone Number Work Phone Number Participant s Date of Birth Survivor s Date of Birth Gender Month day year Month day year Male Female Privacy Statement The Information Practices Act of 1977 (Civil Code Section ) and the Federal Privacy Act (public Law ) require that this notice be provided when collecting personal information from individuals. Information requested on this form is used by the Savings Plus Program for purposes of information and account processing and will be kept confidential in accordance with the information Practices Act. It is mandatory that you furnish all information requested on this form. Failure to provide such information may result in actions requested not being processed. SECTION 2 ANNUITY INFORMATION AND QUOTATIONS REQUESTED Date payments are expected to begin (Commencement Date): Month/Year / Please indicate # 401 (k) Thrift Plan Account Balance $ # 457 Deferred Compensation Plan Account Balance $ ANNUITY TYPE Life Only Period Certain and Life 5 years 10 years 15 years Life with Installment Refund Joint and 50% Survivor Joint and 100% Survivor Period Certain 5 years 10 years 15 years WITH Joint and 50% or Joint and 100% Survivor ANNUITY PROVIDERS Please submit your annuity quotation request directly to NRS. Allow at least 7 business days for the quotation to be mailed to you from NRS. You will receive a quotation and product information from each of the following: Hartford Life Insurance Company Metropolitan Life Insurance Valic Life Insurance Travelers Life Insurance Principal Capital Management " SIGNATURE DATE DC-3502 (12/00) 21
22 This page is intentionally left blank. 22
23 STATE OF CALIFORNIA SAVINGS PLUS PROGRAM ANNUITY PURCHASE APPLICATION SECTION 1 ANNUITANT INFORMATION Please indicate # 457 Deferred Compensation Plan457 Deferred Compensation Plan # 401(k) Thrift Plan Name Street Address City/State/Zip Code Social Security Number Home Phone Number Work Phone Number Date of Birth Month date year Marital Status # Married # Single Gender # Male # Female SECTION 2 ANNUITY PAYMENT INFORMATION (Indicate Name) PURCHASE ANNUITY FROM: TOTAL PREMIUM (FROM QUOTE): $ MONTHLY BENEFIT (FROM QUOTE): ANNUITY START DATE: ANNUITY TYPE: # Life Only $ # Period Certain & Life # 5 years # 10 years # 15 years # Life with Installment Refund # Joint and 50% Survivor # Joint and 100% Survivor # Period Certain # 5 years # 10 years # 15 years with # Joint and 50% or # Joint and 100% Survivor SECTION 3 SURVIVOR DATA Name (Complete only if Joint & Survivor Annuity is selected) Social Security Number Street Address Home Phone Number City/State/Zip Code Date of Birth 23 Month day year Relationship to Participant # Spouse # Other DC-3503 (12/00)
24 SECTION 4 BENEFICIARY DESIGNATION If Spouse-Survivor Annuity is indicated in Section 3, the Spouse-Survivor Annuitant will also be the primary beneficiary of any Death Benefits before considering payment to any beneficiary. If you wish to name multiple primary beneficiaries or a contingent beneficiary(ies) to receive benefits in the event the primary beneficiary(ies) predeceases you, attach a separate sheet showing the name, date of birth, relationship, social security number and mailing address for each listed beneficiary. Primary Beneficiary Name Street Address City/State/Zip Code Relationship to Participant # Spouse # Other Social Security Number Home Phone Number Date of Birth Percentage of Proceeds % SECTION 5 ANNUITANT CERTIFICATION I hereby direct that my entire # 401(k) Thrift Plan # 457 Deferred Compenation Plan account balance be used to purchase the applied for annuity. I acknowledge that I may be charged an administrative fee, the dollar amount may vary depending on the company selected. A state premium tax will be assessed, if applicable, based on the state in which I reside. The state premium tax in California is 0.5% for the 401(k) Plan and 2.35% for the 457 Plan. I understand that in order to defer income tax liability until each periodic annuity payment is received, the State of California must retain ownership of the annuity and that the value of any annuity benefits not yet paid must remain subject to general creditor claims against the State of California. I certify that the information I have provided for the purchase of this annuity is true and correct and that the insurance company has the right to recover any benefits paid to me in error as a result of any false statements. I further certify that I fully understand the annuity payment option I have selected. " Annuitant Signature Date SECTION 6 SPOUSAL WAIVER (must be completed if purchasing other than a survivor benefit) I acknowledge the Beneficiary Designation named on this form. I understand the terms of this contract and that I will not receive benefits in the event my spouse, as the Annuitant, predeceases me. " Signature of Spouse Date 24
25 PRINTER TO INSERT W-4 FORM HERE 25
Sacramento Metropolitan Fire District Retirement Benefit Options
 Personal Information Sacramento Metropolitan Fire District Retirement Benefit Options If this is an initial request, and not a change in a current distribution, remember to have your former employer complete
Personal Information Sacramento Metropolitan Fire District Retirement Benefit Options If this is an initial request, and not a change in a current distribution, remember to have your former employer complete
Important Information For Participants Age 70 ½ or Older
 Important Information For Participants Age 70 ½ or Older The Worker, Retiree, and Employer Recovery Act (the Act ) signed in 2008, temporarily suspends required minimum distributions (RMD) for tax year
Important Information For Participants Age 70 ½ or Older The Worker, Retiree, and Employer Recovery Act (the Act ) signed in 2008, temporarily suspends required minimum distributions (RMD) for tax year
DEATH BENEFIT DISTRIBUTION CLAIM
 DEATH BENEFIT DISTRIBUTION CLAIM - 2 DEATH BENEFIT DISTRIBUTION CLAIM INSTRUCTIONS AND OPTIONS If you believe you have been named a beneficiary of a Plan Participant s assets in the New York State Deferred
DEATH BENEFIT DISTRIBUTION CLAIM - 2 DEATH BENEFIT DISTRIBUTION CLAIM INSTRUCTIONS AND OPTIONS If you believe you have been named a beneficiary of a Plan Participant s assets in the New York State Deferred
County of Fresno Retirement Benefit Options
 County of Fresno Retirement Benefit Options NRM-13003CA-FR.1 Things to Remember c Complete all of the sections on the Retirement Benefit Options form that apply to your request. c If you are requesting
County of Fresno Retirement Benefit Options NRM-13003CA-FR.1 Things to Remember c Complete all of the sections on the Retirement Benefit Options form that apply to your request. c If you are requesting
Participant Distributions
 City of Los Angeles Deferred Compensation Plan Participant Distributions considering your options living your dreams Severance of Employment Table of Contents Introduction... 1 What Are My Choices?...
City of Los Angeles Deferred Compensation Plan Participant Distributions considering your options living your dreams Severance of Employment Table of Contents Introduction... 1 What Are My Choices?...
This booklet contains information and an application for your use.
 State of California Savings Plus Program Part-time, Seasonal, and Temporary Employees Retirement Program Benefit Payment BOOKLET All information contained in this booklet was current as of the printing
State of California Savings Plus Program Part-time, Seasonal, and Temporary Employees Retirement Program Benefit Payment BOOKLET All information contained in this booklet was current as of the printing
DISTRIBUTION/DIRECT ROLLOVER REQUEST - 401(k) Plan Refer to the Participant Distribution Guide while completing this form. Use blue or black ink only.
 Plan Refer to the Participant Distribution Guide while completing this form. Use blue or black ink only.") DISTRIBUTION/DIRECT ROLLOVER REQUEST - 401(k) Plan Refer to the Participant Distribution Guide while completing this form. Use blue or black ink only. HEALTH MIDWEST RETIREMENT SAVINGS PLAN 1009529-02
DISTRIBUTION/DIRECT ROLLOVER REQUEST - 401(k) Plan Refer to the Participant Distribution Guide while completing this form. Use blue or black ink only. HEALTH MIDWEST RETIREMENT SAVINGS PLAN 1009529-02
BENEFIT DISTRIBUTION REQUEST
 BENEFIT DISTRIBUTION REQUEST BENEFIT DISTRIBUTION REQUEST INSTRUCTIONS AND OPTIONS INTRODUCTION This package is designed to help you understand your 457 Deferred Compensation Plan Distribution options
BENEFIT DISTRIBUTION REQUEST BENEFIT DISTRIBUTION REQUEST INSTRUCTIONS AND OPTIONS INTRODUCTION This package is designed to help you understand your 457 Deferred Compensation Plan Distribution options
Retirement Benefit Options
 Retirement Benefit Options Things to Remember Complete all of the sections on the Retirement Benefit Options form that apply to your request. If this is an initial request, and not a change in a current
Retirement Benefit Options Things to Remember Complete all of the sections on the Retirement Benefit Options form that apply to your request. If this is an initial request, and not a change in a current
APPLICATION FOR SURVIVORS BENEFITS
 APPLICATION FOR SURVIVORS BENEFITS ALL APPLICATIONS FOR SURVIVORS BENEFITS SHOULD BE SENT TO: UMWA Health and Retirement Funds 2121 K Street, NW Suite 350 Washington, DC 20037-1879 1-800-291-1425 Fax:
APPLICATION FOR SURVIVORS BENEFITS ALL APPLICATIONS FOR SURVIVORS BENEFITS SHOULD BE SENT TO: UMWA Health and Retirement Funds 2121 K Street, NW Suite 350 Washington, DC 20037-1879 1-800-291-1425 Fax:
Payment Options. Retirement Benefit
 Payment Options Retirement Benefit Table of contents Choosing your benefit payment option... 2 Life Annuities... 5 Fixed Period Benefit... 7 Installment Benefit... 8 Combination of Benefits... 10 Single
Payment Options Retirement Benefit Table of contents Choosing your benefit payment option... 2 Life Annuities... 5 Fixed Period Benefit... 7 Installment Benefit... 8 Combination of Benefits... 10 Single
Last Name First Name MI Social Security Number
 Distribution/Direct Rollover Request 401(a) Plan Refer to the Participant Distribution Guide while completing this form. Use blue or black ink only. All pages must be returned excluding the Participant
Distribution/Direct Rollover Request 401(a) Plan Refer to the Participant Distribution Guide while completing this form. Use blue or black ink only. All pages must be returned excluding the Participant
Annuitant Mailing Address Street Address City State ZIP Code. Annuitant Social Security Number/Tax I.D. Number Annuitant Date of Birth (mm/dd/yyyy)
") Annuitization Questions? Call our National Service Center at 1-800-888-2461. Instructions Please type or print. Use this form to begin annuity payments. Complete each section of the form. If you select
Annuitization Questions? Call our National Service Center at 1-800-888-2461. Instructions Please type or print. Use this form to begin annuity payments. Complete each section of the form. If you select
Table of Contents. Participant Section
 Table of Contents Participant Section Introduction...1 Planning Ahead...1 Distribution Making Your Choice...2 Other Considerations...5 Joint Life and Survivor Expectancy Table...7 Single Life Expectancy
Table of Contents Participant Section Introduction...1 Planning Ahead...1 Distribution Making Your Choice...2 Other Considerations...5 Joint Life and Survivor Expectancy Table...7 Single Life Expectancy
Allstate ChoiceRate Annuity
 Allstate ChoiceRate Annuity Allstate Life Insurance Company P.O. Box 80469 Lincoln, NE 68501-0469 Telephone Number: 1-800-203-0068 Fax Number: 1-866-628-1006 Prospectus dated May 1, 2008 Allstate Life
Allstate ChoiceRate Annuity Allstate Life Insurance Company P.O. Box 80469 Lincoln, NE 68501-0469 Telephone Number: 1-800-203-0068 Fax Number: 1-866-628-1006 Prospectus dated May 1, 2008 Allstate Life
QUALIFIED PLAN DISTRIBUTION NOTICE
 QUALIFIED PLAN DISTRIBUTION NOTICE Introduction As a participant in your employer s Qualified Retirement Plan, you have accumulated a vested account balance. You may receive your vested account balance
QUALIFIED PLAN DISTRIBUTION NOTICE Introduction As a participant in your employer s Qualified Retirement Plan, you have accumulated a vested account balance. You may receive your vested account balance
Participant Name (First) (Middle Initial) (Last) Social Security Number I.D. Number. Participant Address (Street) City State ZIP Code + 4
 (Middle Initial) (Last) Social Security Number I.D. Number. Participant Address (Street) City State ZIP Code + 4") Mailing Address: Des Moines, IA 50392-0001 Principal Life Insurance Company Early Withdrawal of Benefits Without Guaranteed Accounts No Spousal Consent Needed CTD00603 Complete this form to withdraw part
Mailing Address: Des Moines, IA 50392-0001 Principal Life Insurance Company Early Withdrawal of Benefits Without Guaranteed Accounts No Spousal Consent Needed CTD00603 Complete this form to withdraw part
ANNUITY FUND OF STAGE EMPLOYEES LOCAL NO.4, I.A.T.S.E. APPLICATION FOR BENEFITS INSTRUCTIONS
 INSTRUCTIONS 1. Carefully read this application in its entirety before answering any questions. It is particularly important that you read and understand the Special Tax Notice Regarding Plan Payments.
INSTRUCTIONS 1. Carefully read this application in its entirety before answering any questions. It is particularly important that you read and understand the Special Tax Notice Regarding Plan Payments.
KENTUCKY PUBLIC EMPLOYEES DEFERRED COMPENSATION AUTHORITY
 KENTUCKY PUBLIC EMPLOYEES DEFERRED COMPENSATION AUTHORITY Deemed IRA Account Withdrawal Form Instructions/Definitions (attachment to Deemed IRA Account Withdrawal Form) Rules and Conditions. For proper
KENTUCKY PUBLIC EMPLOYEES DEFERRED COMPENSATION AUTHORITY Deemed IRA Account Withdrawal Form Instructions/Definitions (attachment to Deemed IRA Account Withdrawal Form) Rules and Conditions. For proper
If you are 55 years or older and are retiring or separating from the County of San Diego, your
 UTerminal Pay Plan Frequently Asked Questions If you are 55 years or older and are retiring or separating from the County of San Diego, your accrued sick and vacation leave will be paid out through the
UTerminal Pay Plan Frequently Asked Questions If you are 55 years or older and are retiring or separating from the County of San Diego, your accrued sick and vacation leave will be paid out through the
Alaska Supplemental Annuity Plan Benefit Payment Election
 Alaska Supplemental Annuity Plan Benefit Payment Election FOR OFFICE USE ONLY S T A T E O F A L A S K A Toll-Free: 1-800-821-2251 www.state.ak.us/drb Division of Retirement and Benefits PO Box 110203 Juneau,
Alaska Supplemental Annuity Plan Benefit Payment Election FOR OFFICE USE ONLY S T A T E O F A L A S K A Toll-Free: 1-800-821-2251 www.state.ak.us/drb Division of Retirement and Benefits PO Box 110203 Juneau,
Annuity Contract Proof of Death
 Annuity Contract Proof of Death Questions? Call our National Service Center at 1-800-888-2461. Instructions This form is to be completed in order to claim proceeds payable upon death. A separate Proof
Annuity Contract Proof of Death Questions? Call our National Service Center at 1-800-888-2461. Instructions This form is to be completed in order to claim proceeds payable upon death. A separate Proof
Annuity Election. Instructions. Section A. Employer Information. Section B. Participant Information. Section C. Distribution Information
 Annuity Election Instructions To elect an annuity, complete all applicable sections of this form, obtain any required signatures, and return the form to Diversified at the above address. The following
Annuity Election Instructions To elect an annuity, complete all applicable sections of this form, obtain any required signatures, and return the form to Diversified at the above address. The following
Request for Distribution from Individual Retirement Annuity, 403(b) Tax-Sheltered Annuity or Pension Plan
 Tax-Sheltered Annuity or Pension Plan") Request for Distribution from Individual Retirement Annuity, 403(b) Tax-Sheltered Annuity or Pension Plan Standard Insurance Company Individual Annuities 800.247.6888 Tel 800.378.4570 Fax 1100 SW Sixth
Request for Distribution from Individual Retirement Annuity, 403(b) Tax-Sheltered Annuity or Pension Plan Standard Insurance Company Individual Annuities 800.247.6888 Tel 800.378.4570 Fax 1100 SW Sixth
403(b)(7) or Texas Optional Retirement Program (ORP) distribution request
(7) or Texas Optional Retirement Program (ORP) distribution request") 403(b)(7) or Texas Optional Retirement Program (ORP) distribution request Introduction Instructions Please use this form for John Hancock custodial 403(b)(7) or Texas ORP accounts. This form allows you
403(b)(7) or Texas Optional Retirement Program (ORP) distribution request Introduction Instructions Please use this form for John Hancock custodial 403(b)(7) or Texas ORP accounts. This form allows you
CASH DISTRIBUTION FORM For VALIC Annuity Accounts Only All Plan Types
 1. CLIENT INFORMATION Name: Daytime Phone: ( ) Date of Birth: SSN or Tax ID: 2. DISTRIBUTION REQUEST Please select either OPTION A or OPTION B below. Selecting both options will delay processing your distribution
1. CLIENT INFORMATION Name: Daytime Phone: ( ) Date of Birth: SSN or Tax ID: 2. DISTRIBUTION REQUEST Please select either OPTION A or OPTION B below. Selecting both options will delay processing your distribution
Texa$aver 401(k) Plan 98960-01
 Plan 98960-01") In-Service Withdrawal Request 401(k) Plan Texa$aver 401(k) Plan 98960-01 When would I use this form? When I am requesting a withdrawal and I am still employed by the employer/company sponsoring this Plan.
In-Service Withdrawal Request 401(k) Plan Texa$aver 401(k) Plan 98960-01 When would I use this form? When I am requesting a withdrawal and I am still employed by the employer/company sponsoring this Plan.
CHECK LIST FOR REFUND REQUESTS FROM PUBLIC SAFETY
 CHECK LIST FOR REFUND REQUESTS FROM PUBLIC SAFETY (1) Please Complete and Submit a Form P6 Application For A Separation Refund Or Deferred Retirement: Complete the top portion of the P6 form Initial under
CHECK LIST FOR REFUND REQUESTS FROM PUBLIC SAFETY (1) Please Complete and Submit a Form P6 Application For A Separation Refund Or Deferred Retirement: Complete the top portion of the P6 form Initial under
Disability Coverage. This brochure can also be made available in alternative formats, such as large print, Braille, or on tape. Rev.
 Disability Coverage This brochure summarizes many features of your retirement plan and disability coverage. If a discrepancy develops between this summary and state law, the law will govern. This brochure
Disability Coverage This brochure summarizes many features of your retirement plan and disability coverage. If a discrepancy develops between this summary and state law, the law will govern. This brochure
Governmental 457(b) Application For Distribution
 Application For Distribution") #1303-PS (5/14/2008) Governmental 457(b) Application For Distribution GENERAL INFORMATION Name of Plan Name of Employer Address City State Zip Name of Participant Date of Birth Complete the following section
#1303-PS (5/14/2008) Governmental 457(b) Application For Distribution GENERAL INFORMATION Name of Plan Name of Employer Address City State Zip Name of Participant Date of Birth Complete the following section
Trustee-to-Trustee Transfer Out of the ICMA Retirement Corporation Packet
 I C M A R E T I R E M E N T C O R P O R A T I O N Trustee-to-Trustee Transfer Out of the ICMA Retirement Corporation Packet Included in this packet: Trustee-to-Trustee Transfer Out of the ICMA Retirement
I C M A R E T I R E M E N T C O R P O R A T I O N Trustee-to-Trustee Transfer Out of the ICMA Retirement Corporation Packet Included in this packet: Trustee-to-Trustee Transfer Out of the ICMA Retirement
Howard 457 Deemed IRA Participation Agreement for Deferred Compensation Plan
 Howard 457 Deemed IRA Participation Agreement for Deferred Compensation Plan DC-4803 (09/2015) For help, please call 1-877-677-3678 www.howard457.com 1 2 DC-4803 (09/2015) For help, please call 1-877-677-3678
Howard 457 Deemed IRA Participation Agreement for Deferred Compensation Plan DC-4803 (09/2015) For help, please call 1-877-677-3678 www.howard457.com 1 2 DC-4803 (09/2015) For help, please call 1-877-677-3678
REQUEST FOR DISBURSEMENT Form - Tax-Sheltered Annuities 403(b)
") Policy Number Owner / Annuitant Phone Number Owner s Legal Address--Street City State Zip CONDITIONS FOR WITHDRAWAL One of the conditions below must be met for a withdrawal to be processed. Please review
Policy Number Owner / Annuitant Phone Number Owner s Legal Address--Street City State Zip CONDITIONS FOR WITHDRAWAL One of the conditions below must be met for a withdrawal to be processed. Please review
Retirement Plan DISTRIBUTION FORM
 Retirement Plan Services P.O. Box 2978 5910 Mineral Point Road Madison, WI 53701-2978 Phone: 800.999.8786 Fax: 608.236.8017 www.benefitsforyou.com Retirement Plan DISTRIBUTION FORM DEFINED CONTRIBUTION
Retirement Plan Services P.O. Box 2978 5910 Mineral Point Road Madison, WI 53701-2978 Phone: 800.999.8786 Fax: 608.236.8017 www.benefitsforyou.com Retirement Plan DISTRIBUTION FORM DEFINED CONTRIBUTION
Service Retirement Guide Public Employees' Retirement System of Mississippi
 Service Retirement Guide Public Employees' Retirement System of Mississippi As a public employee in Mississippi, retirement is a benefit you have worked toward your entire covered career. Your years of
Service Retirement Guide Public Employees' Retirement System of Mississippi As a public employee in Mississippi, retirement is a benefit you have worked toward your entire covered career. Your years of
DISTRIBUTION REQUEST FORM
 DISTRIBUTION REQUEST FORM Previously, there was little oversight regarding the withdrawal of money from 403(b) plans. The recent law changes now apply sanctions on Plans that do not carefully monitor and
DISTRIBUTION REQUEST FORM Previously, there was little oversight regarding the withdrawal of money from 403(b) plans. The recent law changes now apply sanctions on Plans that do not carefully monitor and
Baltimore 457 Deemed IRA Participant Agreement
 Baltimore 457 Deemed IRA Participant Agreement NRM-8296MD-BA.2-0314 1 2 Employer Plan IRA Type Personal Information Baltimore Deemed IRA Participation Agreement Payroll Deduction Authorization & Service
Baltimore 457 Deemed IRA Participant Agreement NRM-8296MD-BA.2-0314 1 2 Employer Plan IRA Type Personal Information Baltimore Deemed IRA Participation Agreement Payroll Deduction Authorization & Service
Service Retirement. Plans of Payment AND. For members enrolled in the Defined Contribution Plan
 Service Retirement AND Plans of Payment For members enrolled in the Defined Contribution Plan 2015 2016 Service Retirement Overview Table of Contents Service Retirement Overview...1 Benefit calculation...2
Service Retirement AND Plans of Payment For members enrolled in the Defined Contribution Plan 2015 2016 Service Retirement Overview Table of Contents Service Retirement Overview...1 Benefit calculation...2
Plan Distribution Form
 Plan Distribution Form Capitol Plaza Bldg, Suite 110 120 Father Dueñas Ave. Hagåtña, Guam 96910 Phone: (671) 477-2724 Fax: (671) 477-2729 www.ascpac.com You are about to make a decision that could greatly
Plan Distribution Form Capitol Plaza Bldg, Suite 110 120 Father Dueñas Ave. Hagåtña, Guam 96910 Phone: (671) 477-2724 Fax: (671) 477-2729 www.ascpac.com You are about to make a decision that could greatly
Southern California Pipe Trades
 Southern California Pipe Trades LO56050514 (Retired) Defined Contribution Fund Retirement/Disability/Termination Distribution LO56050517 (Disabled) Application Complete all applicable sections and return
Southern California Pipe Trades LO56050514 (Retired) Defined Contribution Fund Retirement/Disability/Termination Distribution LO56050517 (Disabled) Application Complete all applicable sections and return
New Hanover Regional Medical Center 403(b) and 457(b) Retirement Savings Plans
 and 457(b) Retirement Savings Plans") New Hanover Regional Medical Center 403(b) and 457(b) Retirement Savings Plans Mutual Fund Safe Harbor Request For Hardship Withdrawal Group ID# 45944003 Group ID# 45944002 1. CLIENT INFORMATION Name:
New Hanover Regional Medical Center 403(b) and 457(b) Retirement Savings Plans Mutual Fund Safe Harbor Request For Hardship Withdrawal Group ID# 45944003 Group ID# 45944002 1. CLIENT INFORMATION Name:
UTAH RETIREMENT SYSTEMS 401(K) WITHDRAWAL
 WITHDRAWAL") Utah Retirement Systems PO Box 1590 Salt Lake City, Utah 84110-1590 801-366-7720 or 800-688-4015 Fax 801-366-7445 or 800-753-7445 Email: dcplans@urs.org www.urs.org INSTRUCTIONS: 1. Use this form to request
Utah Retirement Systems PO Box 1590 Salt Lake City, Utah 84110-1590 801-366-7720 or 800-688-4015 Fax 801-366-7445 or 800-753-7445 Email: dcplans@urs.org www.urs.org INSTRUCTIONS: 1. Use this form to request
QP/401(k) Separation From Service Distribution Request Form
 Separation From Service Distribution Request Form") #10486 (3/2004) QP/401(k) Separation From Service Distribution Request Form This form may be used if you have separated from service due to termination, disability or attainment of normal retirement age
#10486 (3/2004) QP/401(k) Separation From Service Distribution Request Form This form may be used if you have separated from service due to termination, disability or attainment of normal retirement age
Mailing Address: P.O. Box 9394 Des Moines, IA 50306-9394 FAX (866) 704-3481. Principal Life Insurance Company
 704-3481. Principal Life Insurance Company") Mailing Address: P.O. Box 9394 Des Moines, IA 50306-9394 FAX (866) 704-3481 Principal Life Insurance Company Complete this form to withdraw part of your retirement funds while still employed. Participant
Mailing Address: P.O. Box 9394 Des Moines, IA 50306-9394 FAX (866) 704-3481 Principal Life Insurance Company Complete this form to withdraw part of your retirement funds while still employed. Participant
PERSI Choice 401(k) Plan 95270-01
 Plan 95270-01") Separation from Employment Withdrawal Request 401(k) Plan PERSI Choice 401(k) Plan 95270-01 When would I use this form? When I am requesting a withdrawal and I am no longer employed by the employer/company
Separation from Employment Withdrawal Request 401(k) Plan PERSI Choice 401(k) Plan 95270-01 When would I use this form? When I am requesting a withdrawal and I am no longer employed by the employer/company
G You are totally and permanently disabled. If you have checked this box, complete Sections III, IV and V of this application.
 THE NATIONAL ASBESTOS WORKERS SUPPLEMENTAL PENSION PLAN BENEFIT APPLICATION For Distributions Over $5,000 INSTRUCTIONS: Please read this application carefully and completely before answering any questions.
THE NATIONAL ASBESTOS WORKERS SUPPLEMENTAL PENSION PLAN BENEFIT APPLICATION For Distributions Over $5,000 INSTRUCTIONS: Please read this application carefully and completely before answering any questions.
CASH DISTRIBUTION FORM For VALIC Annuity Accounts Only All Plan Types
 1. CLIENT INFORMATION Name: Daytime Phone: ( ) Date of Birth: SSN or Tax ID: 2. DISTRIBUTION REQUEST Please select either OPTION A or OPTION B below. Selecting both options will delay processing your distribution
1. CLIENT INFORMATION Name: Daytime Phone: ( ) Date of Birth: SSN or Tax ID: 2. DISTRIBUTION REQUEST Please select either OPTION A or OPTION B below. Selecting both options will delay processing your distribution
New York Life Insurance and Annuity Corporation NYL Guaranteed Lifetime Income Annuity II - Single Life
 Annuitant & Policy Information New York Life Insurance and Annuity Corporation Summary Name: Valued Client Type of Funds: Non-Qualified Date of Birth: 07/18/1949 Payment Frequency: Monthly Sex: Male Purchase
Annuitant & Policy Information New York Life Insurance and Annuity Corporation Summary Name: Valued Client Type of Funds: Non-Qualified Date of Birth: 07/18/1949 Payment Frequency: Monthly Sex: Male Purchase
Distribution Form Subject to Joint & Survivor Annuity
 Distribution Form Subject to Joint & Survivor Annuity Please refer to the Plan s Summary Plan Description (SPD) for reasons distributions that are allowed in your plan. You may review the SPD, your account
Distribution Form Subject to Joint & Survivor Annuity Please refer to the Plan s Summary Plan Description (SPD) for reasons distributions that are allowed in your plan. You may review the SPD, your account
403(b) Program Highlights
 Program Highlights") 403(b) Program Highlights As part of Henry Ford Health System s (HFHS) commitment to helping employees plan for their future financial wellness, HFHS offers a 403(b) program whereby employees can save
403(b) Program Highlights As part of Henry Ford Health System s (HFHS) commitment to helping employees plan for their future financial wellness, HFHS offers a 403(b) program whereby employees can save
SCP POFF ROLLOVER SOURCE DISTRIBUTION REQUEST FORM
 CalPERS Supplemental Contributions Plan 452001 SCP POFF ROLLOVER SOURCE DISTRIBUTION REQUEST FORM q INITIAL DISTRIBUTION q CURRENT DISTRIBUTION CHANGE q ALTERNATE PAYEE DISTRIBUTION PER QUALIFIED DOMESTIC
CalPERS Supplemental Contributions Plan 452001 SCP POFF ROLLOVER SOURCE DISTRIBUTION REQUEST FORM q INITIAL DISTRIBUTION q CURRENT DISTRIBUTION CHANGE q ALTERNATE PAYEE DISTRIBUTION PER QUALIFIED DOMESTIC
Security Benefit Advanced Choice Annuity Application Individual Single Purchase Payment Deferred Annuity
 Security Benefit Advanced Choice Annuity Application Individual Single Purchase Payment Deferred Annuity Issued by Security Benefit Life Insurance Company. Questions? Call our National Service Center at
Security Benefit Advanced Choice Annuity Application Individual Single Purchase Payment Deferred Annuity Issued by Security Benefit Life Insurance Company. Questions? Call our National Service Center at
FMPTF 401(a) Defined Contribution and 457(b) Deferred Compensation BENEFICIARY DISTRIBUTION REQUEST
 Defined Contribution and 457(b) Deferred Compensation BENEFICIARY DISTRIBUTION REQUEST") FMPTF 401(a) Defined Contribution and 457(b) Deferred Compensation BENEFICIARY DISTRIBUTION REQUEST If you have any questions, please contact the Florida Municipal Pension Trust Fund (FMPTF) by calling
FMPTF 401(a) Defined Contribution and 457(b) Deferred Compensation BENEFICIARY DISTRIBUTION REQUEST If you have any questions, please contact the Florida Municipal Pension Trust Fund (FMPTF) by calling
Tile Layers Local 7 Annuity Fund 253 West 35 th Street 12 th Floor, New York, NY 10001 Phone: (212) 505-5050 Fax: (212) 714-1455
 505-5050 Fax: (212) 714-1455") Instructions for Withdrawal 1) Please read the Federal Income Taxation Distributions Notice. 2) Make sure that Page 8 is notarized. 3) Fill out the Application for Annuity Fund Benefit Withdrawal form
Instructions for Withdrawal 1) Please read the Federal Income Taxation Distributions Notice. 2) Make sure that Page 8 is notarized. 3) Fill out the Application for Annuity Fund Benefit Withdrawal form
MAKE NO ALTERATIONS TO THIS FORM.
 Office of the New York State Comptroller New York State and Local Retirement System Employees Retirement System Police and Fire Retirement System 110 State Street, Albany, New York 12244-0001 Retirement
Office of the New York State Comptroller New York State and Local Retirement System Employees Retirement System Police and Fire Retirement System 110 State Street, Albany, New York 12244-0001 Retirement
1. Participant Information Please print clearly in CAPITAL LETTERS.
 REQUIRED MINIMUM DISTRIBUTION FORM PLAN NAME: PLAN NUMBER: Use this form to request a required minimum distribution following attainment of age 70½, unless you are still employed and are not a 5% owner.
REQUIRED MINIMUM DISTRIBUTION FORM PLAN NAME: PLAN NUMBER: Use this form to request a required minimum distribution following attainment of age 70½, unless you are still employed and are not a 5% owner.
PSERS Divorce Guidelines
 PSERS Divorce Guidelines Publication # 9681 09/2012 PSERS Divorce Guidelines Revised September 11, 2012 Public School Employees' Retirement System - Who are we?... 1 How is a PSERS retirement benefit affected
PSERS Divorce Guidelines Publication # 9681 09/2012 PSERS Divorce Guidelines Revised September 11, 2012 Public School Employees' Retirement System - Who are we?... 1 How is a PSERS retirement benefit affected
How To Get A Pension From The Pension Fund
 Member s Guide to: DROP Deferred Retirement Option Plan www.op-f.org PLAN DEFERRED RETIREMENT DROP The Deferred Retirement Option Plan (DROP) is an optional benefit that allows eligible police officers
Member s Guide to: DROP Deferred Retirement Option Plan www.op-f.org PLAN DEFERRED RETIREMENT DROP The Deferred Retirement Option Plan (DROP) is an optional benefit that allows eligible police officers
Benefit Claim Form Deferred Profit-Sharing Plan (DPSP) / Retirement Plan (RP) OFIS #0001
 / Retirement Plan (RP) OFIS #0001") BENEFIT OPTIONS All terminating participants, regardless of age and service, may elect one of the following forms of benefit from each plan: A. Direct Rollover (Lump Sum Distribution) tax-deferred rollover
BENEFIT OPTIONS All terminating participants, regardless of age and service, may elect one of the following forms of benefit from each plan: A. Direct Rollover (Lump Sum Distribution) tax-deferred rollover
Single Purchase Payment
 CONTRACT SUMMARY Pacific Life Insurance Company P.O. Box 2378 Omaha, NE 68103-2378 (800) 722-4448 Contract Owners (800) 722-2333 Registered Representatives www.pacificlife.com Pacific Income Provider Individual
CONTRACT SUMMARY Pacific Life Insurance Company P.O. Box 2378 Omaha, NE 68103-2378 (800) 722-4448 Contract Owners (800) 722-2333 Registered Representatives www.pacificlife.com Pacific Income Provider Individual
ASC IRA Distribution Form
 ASC IRA Distribution Form 120 Father Dueñas Ave. Ste.110 Hagåtña, Guam 96910 Phone: (671) 477-2724 Fax: (671) 477-2729 Email: Info@ASCTrust.com Website: www.asctrust.com You are about to make a decision
ASC IRA Distribution Form 120 Father Dueñas Ave. Ste.110 Hagåtña, Guam 96910 Phone: (671) 477-2724 Fax: (671) 477-2729 Email: Info@ASCTrust.com Website: www.asctrust.com You are about to make a decision
COLLIERS INTERNATIONAL USA, LLC And Affiliated Employers 401(K) Plan DISTRIBUTION ELECTION
 Plan DISTRIBUTION ELECTION") 1. EMPLOYEE INFORMATION (Please print) COLLIERS INTERNATIONAL USA, LLC And Affiliated Employers 401(K) Plan DISTRIBUTION ELECTION Name: Address: Social Security No.: Birth Date: City: State: Zip: Termination
1. EMPLOYEE INFORMATION (Please print) COLLIERS INTERNATIONAL USA, LLC And Affiliated Employers 401(K) Plan DISTRIBUTION ELECTION Name: Address: Social Security No.: Birth Date: City: State: Zip: Termination
Request for Disbursement / Systematic Withdrawal Form for Qualified Annuities
 for Qualified Annuities INSURER OM Financial Life Insurance Company Policy Number Owner / Annuitant Phone Number Owner s Address--Street City State Zip Check if new address Payment requests will be mailed
for Qualified Annuities INSURER OM Financial Life Insurance Company Policy Number Owner / Annuitant Phone Number Owner s Address--Street City State Zip Check if new address Payment requests will be mailed
rollover/transfer out form
 1. Client Information rollover/transfer out form For VALIC Annuity 403(b) Plan Accounts Only Original Form Required for Processing The Variable annuity life insurance Company (ValiC), Houston, texas Mail
1. Client Information rollover/transfer out form For VALIC Annuity 403(b) Plan Accounts Only Original Form Required for Processing The Variable annuity life insurance Company (ValiC), Houston, texas Mail
STAY IN THE SMART PLAN
 STAY IN THE SMART PLAN Even if you are no longer employed by the Commonwealth of Massachusetts or a local municipality, you can keep your Massachusetts Deferred Compensation SMART Plan (SMART Plan) account
STAY IN THE SMART PLAN Even if you are no longer employed by the Commonwealth of Massachusetts or a local municipality, you can keep your Massachusetts Deferred Compensation SMART Plan (SMART Plan) account
Janus Qualified Retirement Accounts Distribution Form
 Janus Qualified Retirement Accounts Distribution Janus Qualified PO Box 55932 Form Retirement Accounts Distribution Form Boston, MA 02205-5932 800-525-1093 PO Box 55932 Boston, MA 02205-5932 800-525-1093
Janus Qualified Retirement Accounts Distribution Janus Qualified PO Box 55932 Form Retirement Accounts Distribution Form Boston, MA 02205-5932 800-525-1093 PO Box 55932 Boston, MA 02205-5932 800-525-1093
TAX SHELTERED ANNUITY ROLLOVER / PARTIAL WITHDRAWAL / FULL SURRENDER REQUEST
 General American Retirement & Investment Services PO Box 19098 Greenville, SC 29602 Customer Service: 800-449-6447 Fax: 866-214-0926 TAX SHELTERED ANNUITY ROLLOVER / PARTIAL WITHDRAWAL / FULL SURRENDER
General American Retirement & Investment Services PO Box 19098 Greenville, SC 29602 Customer Service: 800-449-6447 Fax: 866-214-0926 TAX SHELTERED ANNUITY ROLLOVER / PARTIAL WITHDRAWAL / FULL SURRENDER
MSRP Withdrawal Requirements, Options & Beneficiaries
 MSRP Withdrawal Requirements, Options & Beneficiaries You have been deferring into your account for many years, and retirement is just around the corner. How might this money be distributed? What options
MSRP Withdrawal Requirements, Options & Beneficiaries You have been deferring into your account for many years, and retirement is just around the corner. How might this money be distributed? What options
Annuity Withdrawal Request - 457 Deferred Compensation Plan Annuities
 Mailing Instructions: A. Plan/Trust Information Plan/Trust Name: LSW Annuities - Life Insurance Company of the Southwest NL Annuities - National Life Insurance Company PO Box 569080, Dallas, TX 75356 Service:
Mailing Instructions: A. Plan/Trust Information Plan/Trust Name: LSW Annuities - Life Insurance Company of the Southwest NL Annuities - National Life Insurance Company PO Box 569080, Dallas, TX 75356 Service:
How To Defer Federal Income Tax On Your Retirement Savings In The Cahill Pipe Trades Local No. 777 Annuity Fund
 Connecticut Pipe Trades Local 777 Annuity Fund 1155 Silas Deane Hwy. Wethersfield, CT 06109 Phone (860) 571-9191 Fax (860) 571-9221 www.connecticutpipetrades.com ANNUITY HARDSHIP WITHDRAWAL PROVISIONS
Connecticut Pipe Trades Local 777 Annuity Fund 1155 Silas Deane Hwy. Wethersfield, CT 06109 Phone (860) 571-9191 Fax (860) 571-9221 www.connecticutpipetrades.com ANNUITY HARDSHIP WITHDRAWAL PROVISIONS
DISTRIBUTION GUIDE This Distribution Guide provides educational information to help you successfully transition into retirement.
 DISTRIBUTION GUIDE This Distribution Guide provides educational information to help you successfully transition into retirement. As a participant, you will receive unbiased and accurate information for
DISTRIBUTION GUIDE This Distribution Guide provides educational information to help you successfully transition into retirement. As a participant, you will receive unbiased and accurate information for
IRA Beneficiary Election Form For assistance, please contact us at 1-800-243-1574 or visit our website at Virtus.com
 Virtus Investment Partners PO Box 9874 Providence, RI 02940-8074 IRA Beneficiary Election Form For assistance, please contact us at 1-800-243-1574 or visit our website at Virtus.com Important Information
Virtus Investment Partners PO Box 9874 Providence, RI 02940-8074 IRA Beneficiary Election Form For assistance, please contact us at 1-800-243-1574 or visit our website at Virtus.com Important Information
How To Rollover From A Pension Plan
 Hardship Withdrawal Form READ THE ATTACHED IRS SPECIAL TAX NOTICE: IF YOUR PLAN ALLOWS FOR AN ANNUITY OPTION, READ THE WRITTEN EXPLANATION OF QUALIFIED JOINT AND 50% CONTINGENT SURVIVIOR ANNUITY FORM OF
Hardship Withdrawal Form READ THE ATTACHED IRS SPECIAL TAX NOTICE: IF YOUR PLAN ALLOWS FOR AN ANNUITY OPTION, READ THE WRITTEN EXPLANATION OF QUALIFIED JOINT AND 50% CONTINGENT SURVIVIOR ANNUITY FORM OF
INSTRUCTIONS TO EMPLOYER. What to do when a participant terminates employment
 INSTRUCTIONS TO EMPLOYER What to do when a participant terminates employment 1. Print the following distribution forms and give them to the terminated participant. The required forms include: a. Instructions
INSTRUCTIONS TO EMPLOYER What to do when a participant terminates employment 1. Print the following distribution forms and give them to the terminated participant. The required forms include: a. Instructions
Distribution Request Checklist
 Distribution Request Checklist PENTEGRA TRUST COMPANY A Distribution Request Form must be completed, signed and returned to the Employer/Plan Administrator to request a distribution from your Plan Account.
Distribution Request Checklist PENTEGRA TRUST COMPANY A Distribution Request Form must be completed, signed and returned to the Employer/Plan Administrator to request a distribution from your Plan Account.
The IRA Rollover. Making Sense Out of Your Retirement Plan Distribution
 The IRA Rollover Making Sense Out of Your Retirement Plan Distribution Expecting a Distribution? You have been a participant in your employer s retirement plan for a number of years, and you have earned
The IRA Rollover Making Sense Out of Your Retirement Plan Distribution Expecting a Distribution? You have been a participant in your employer s retirement plan for a number of years, and you have earned
Minimum Premium: Qualified [$5,000] Non-Qualified [$10,000] Maximum Premium: [$250,000]
![Minimum Premium: Qualified [$5,000] Non-Qualified [$10,000] Maximum Premium: [$250,000]](/thumbs/34/16991506.jpg "Minimum Premium: Qualified [$5,000] Non-Qualified [$10,000] Maximum Premium: [$250,000]") 2721 North Central Avenue, Phoenix, Arizona 85004-1172 (866) 641-9999 Oxford Life Insurance Company Single Premium Multi-Year Guarantee Annuity With Market Value Adjustment Feature Benefit Summary and
2721 North Central Avenue, Phoenix, Arizona 85004-1172 (866) 641-9999 Oxford Life Insurance Company Single Premium Multi-Year Guarantee Annuity With Market Value Adjustment Feature Benefit Summary and
6) Any other form acceptable to the appropriate GAIG company.
 Any other form acceptable to the appropriate GAIG company.") Member Companies: Great American Life Insurance Company Annuity Investors Life Insurance Company Manhattan National Life Insurance Company Administrator for: Loyal American Life Insurance Company United
Member Companies: Great American Life Insurance Company Annuity Investors Life Insurance Company Manhattan National Life Insurance Company Administrator for: Loyal American Life Insurance Company United
Distribution Request Form
 The 3121 Premier Plan Eligible Full-Time, Part-Time, Seasonal, and Temporary Employees Social Security Alternative Retirement Plan Employer (please print or type): Distribution Request Form Name of Participant:
The 3121 Premier Plan Eligible Full-Time, Part-Time, Seasonal, and Temporary Employees Social Security Alternative Retirement Plan Employer (please print or type): Distribution Request Form Name of Participant:
Loan Application Form
 Loan Application Form READ THE ATTACHED IRS SPECIAL TAX NOTICE AND WRITTEN EXPLANATION OF QUALIFIED J OINT AND 50% CONTINGENT SUVIVIOR ANNUITY FORM OF BENEFIT BEFORE COMPLETING THIS FORM Please Note: Do
Loan Application Form READ THE ATTACHED IRS SPECIAL TAX NOTICE AND WRITTEN EXPLANATION OF QUALIFIED J OINT AND 50% CONTINGENT SUVIVIOR ANNUITY FORM OF BENEFIT BEFORE COMPLETING THIS FORM Please Note: Do
o NOTICE OF TERMINATION AND/OR o CURRENT DISTRIBUTION CHANGE o ALTERNATE PAYEE DISTRIBUTION PER QUALIFIED
 CalPERS Supplemental Income 457 Plan DISTRIBUTION REQUEST FORM o NOTICE OF TERMINATION AND/OR o CURRENT DISTRIBUTION CHANGE o ALTERNATE PAYEE DISTRIBUTION PER QUALIFIED INITIAL DISTRIBUTION DOMESTIC RELATIONS
CalPERS Supplemental Income 457 Plan DISTRIBUTION REQUEST FORM o NOTICE OF TERMINATION AND/OR o CURRENT DISTRIBUTION CHANGE o ALTERNATE PAYEE DISTRIBUTION PER QUALIFIED INITIAL DISTRIBUTION DOMESTIC RELATIONS
Teachers Retirement Plan Participants (All CSO and WTU Employees Only)
") Teachers Retirement Plan Participants (All CSO and WTU Employees Only) If you are enrolled in the Teachers Retirement Plan, you must complete the following steps to secure your refund: Obtain a copy of
Teachers Retirement Plan Participants (All CSO and WTU Employees Only) If you are enrolled in the Teachers Retirement Plan, you must complete the following steps to secure your refund: Obtain a copy of
State of Arizona Deferred Compensation Payout Request Form
 State of Arizona Deferred Compensation Payout Request Form Personal Information Plan Type: c 457(b) c 401(a) c 403(b) c All Participant Name: Participant SSN: Mailing Address: City, State* & Zip Code:
State of Arizona Deferred Compensation Payout Request Form Personal Information Plan Type: c 457(b) c 401(a) c 403(b) c All Participant Name: Participant SSN: Mailing Address: City, State* & Zip Code:
Franklin Templeton Retirement Plan Beneficiary Distribution Request
 Franklin Templeton Retirement Plan Beneficiary Distribution Request For assistance, please call your financial advisor or Franklin Templeton Retirement Services at 1-800/527-2020. 1 PARTICIPANT (DECEDENT)
Franklin Templeton Retirement Plan Beneficiary Distribution Request For assistance, please call your financial advisor or Franklin Templeton Retirement Services at 1-800/527-2020. 1 PARTICIPANT (DECEDENT)
Small Amounts Benefit Election
 Mailing Address: P.O. Box 9394 Des Moines, IA 50306-9394 Principal Life Insurance Company Small Amounts Benefit Election You are entitled to a distribution according to the Small Amounts provision of the
Mailing Address: P.O. Box 9394 Des Moines, IA 50306-9394 Principal Life Insurance Company Small Amounts Benefit Election You are entitled to a distribution according to the Small Amounts provision of the
Distribution Options. For Defined Contribution and 403(b) Plans Without Life Annuities
 Plans Without Life Annuities") Distribution Options For Defined Contribution and 403(b) Plans Without Life Annuities Take the Time to Decide What will you do with your retirement savings? Life is full of changes. We retire. We change
Distribution Options For Defined Contribution and 403(b) Plans Without Life Annuities Take the Time to Decide What will you do with your retirement savings? Life is full of changes. We retire. We change
UNITED HERITAGE CREDIT UNION DEFINED BENEFIT PLAN INSTRUCTIONS FOR DESIGNATING OR CHANGING BENEFICIARY
 Beneficiary Form Instructions INSTRUCTIONS FOR DESIGNATING OR CHANGING BENEFICIARY These instructions will assist you in properly completing the DESIGNATION OF BENEFICIARY form. 1. To designate one person,
Beneficiary Form Instructions INSTRUCTIONS FOR DESIGNATING OR CHANGING BENEFICIARY These instructions will assist you in properly completing the DESIGNATION OF BENEFICIARY form. 1. To designate one person,
Member / Beneficiary Request To Withdraw Contributions / Elect Rollover
 Orange County Employees Retirement System 2223 E. Wellington Avenue. Suite 100 Santa Ana, CA 92701 (714) 558-6200 www.ocers.org Member / Beneficiary Request To Withdraw Contributions / Elect Rollover Please
Orange County Employees Retirement System 2223 E. Wellington Avenue. Suite 100 Santa Ana, CA 92701 (714) 558-6200 www.ocers.org Member / Beneficiary Request To Withdraw Contributions / Elect Rollover Please
Service Retirement Application
 Do not separate page from application. State Teachers Retirement System Of Ohio Service Retirement Application for Members Enrolled in the Defined Benefit Plan Choosing to retire is an important life decision.
Do not separate page from application. State Teachers Retirement System Of Ohio Service Retirement Application for Members Enrolled in the Defined Benefit Plan Choosing to retire is an important life decision.
Federal Employees Group Life Insurance Program
 FEGLI Federal Employees Group Life Insurance Federal Employees Group Life Insurance Program Office of Personnel Management Retirement & Insurance Service RI 76-12 Previous editions are not usable Revised
FEGLI Federal Employees Group Life Insurance Federal Employees Group Life Insurance Program Office of Personnel Management Retirement & Insurance Service RI 76-12 Previous editions are not usable Revised
To: Plan Member From: Service Center Subject: Age 59½ Withdrawal Request ELCA Retirement Plan
 To: Plan Member From: Service Center Subject: Age 59½ Withdrawal Request ELCA Retirement Plan Enclosed is the information you requested regarding making a withdrawal from your ELCA Retirement Plan account.
To: Plan Member From: Service Center Subject: Age 59½ Withdrawal Request ELCA Retirement Plan Enclosed is the information you requested regarding making a withdrawal from your ELCA Retirement Plan account.
BENEFIT DISTRIBUTION REQUEST FORM (For Distributions due to Termination, Death, Disability, and Retirement) Date: EIN: 16-6184130 TIN: 611256314
 Date: EIN: 16-6184130 TIN: 611256314") BENEFIT DISTRIBUTION REQUEST FORM (For Distributions due to Termination, Death, Disability, and Retirement) : EIN: 16-6184130 TIN: 611256314 Plan Name: UFCW LOCAL ONE 401(K) SAVINGS PLAN Participant Data
BENEFIT DISTRIBUTION REQUEST FORM (For Distributions due to Termination, Death, Disability, and Retirement) : EIN: 16-6184130 TIN: 611256314 Plan Name: UFCW LOCAL ONE 401(K) SAVINGS PLAN Participant Data
Annuity Full Surrender Request
 Annuity Full Surrender Request Annuities are issued by Pruco Life Insurance Company, in New York, by Pruco Life Insurance Company of New Jersey and The Prudential Insurance Company of America (PICA) (these
Annuity Full Surrender Request Annuities are issued by Pruco Life Insurance Company, in New York, by Pruco Life Insurance Company of New Jersey and The Prudential Insurance Company of America (PICA) (these
How To Get A Pension From The Retirement Plan
 Defined Contribution Plan Distribution Kit for CSU Safe Harbor Participants University of California Retirement System (UCRS) UBEN 143 CSU (R3/99) Use the form in the back of this kit if you have left
Defined Contribution Plan Distribution Kit for CSU Safe Harbor Participants University of California Retirement System (UCRS) UBEN 143 CSU (R3/99) Use the form in the back of this kit if you have left
APPLICATION FOR ANNUITY. Proposed Annuitant Name: FIRST MIDDLE LAST. Address: STREET CITY STATE ZIP
 APPLICATION FOR ANNUITY Proposed Annuitant Name: FIRST MIDDLE LAST Address: STREET CITY STATE ZIP Social Security Number: Date of Birth: / / Sex: q Male q Female Proposed Second Annuitant Name: (if applicable
APPLICATION FOR ANNUITY Proposed Annuitant Name: FIRST MIDDLE LAST Address: STREET CITY STATE ZIP Social Security Number: Date of Birth: / / Sex: q Male q Female Proposed Second Annuitant Name: (if applicable
Elevator Constructors Annuity and 401(k) Retirement Plan Distribution Form
 Retirement Plan Distribution Form") Elevator Constructors Annuity and 401(k) Retirement Plan Distribution Form Account Number 60041-1 Name: Social Security No. Address: Date: Legal State of Residence:. If the Legal State of Residence is
Elevator Constructors Annuity and 401(k) Retirement Plan Distribution Form Account Number 60041-1 Name: Social Security No. Address: Date: Legal State of Residence:. If the Legal State of Residence is
YOUR ROLLOVER OPTIONS GENERAL INFORMATION ABOUT ROLLOVERS
 SPECIAL TAX NOTICE REGARDING PAYMENTS FROM QUALIFIED PLANS YOUR ROLLOVER OPTIONS You are receiving this notice because all or a portion of a payment you are receiving from your Employer s plan (the "Plan")
SPECIAL TAX NOTICE REGARDING PAYMENTS FROM QUALIFIED PLANS YOUR ROLLOVER OPTIONS You are receiving this notice because all or a portion of a payment you are receiving from your Employer s plan (the "Plan")
403(b)(7) Retirement Plan. Account Registration. Distribution Information. Employer Authorization. 403(b) Owner. Designated Beneficiary
(7) Retirement Plan. Account Registration. Distribution Information. Employer Authorization. 403(b) Owner. Designated Beneficiary") 403(b)(7) Retirement Plan D I S T R I B U T I O N R E Q U E S T F 1 Account Registration 403(b) Owner FOR ASSISTANCE with this form, call Shareholder Services at (800) 662-0201, or the Timothy Plan at
403(b)(7) Retirement Plan D I S T R I B U T I O N R E Q U E S T F 1 Account Registration 403(b) Owner FOR ASSISTANCE with this form, call Shareholder Services at (800) 662-0201, or the Timothy Plan at
Ohio Public Employees Retirement System 277 East Town Street, Columbus, Ohio 43215-4642 1-800-222-PERS (7377) www.opers.org
 www.opers.org") Ohio Public Employees Retirement System 277 East Town Street, Columbus, Ohio 43215-4642 1-800-222-PERS (7377) www.opers.org Traditional Pension Plan Refund Application When you leave public employment,
Ohio Public Employees Retirement System 277 East Town Street, Columbus, Ohio 43215-4642 1-800-222-PERS (7377) www.opers.org Traditional Pension Plan Refund Application When you leave public employment,
New Alternatives Fund, Inc. INDIVIDUAL RETIREMENT ACCOUNT (IRA) TRADITIONAL IRA SEP IRA ROTH IRA
 TRADITIONAL IRA SEP IRA ROTH IRA") New Alternatives Fund, Inc. INDIVIDUAL RETIREMENT ACCOUNT (IRA) TRADITIONAL IRA SEP IRA ROTH IRA TABLE OF CONTENTS COMBINED DISCLOSURE STATEMENT 3 TRADITIONAL INDIVIDUAL RETIREMENT ACCOUNT DISCLOSURE 4
New Alternatives Fund, Inc. INDIVIDUAL RETIREMENT ACCOUNT (IRA) TRADITIONAL IRA SEP IRA ROTH IRA TABLE OF CONTENTS COMBINED DISCLOSURE STATEMENT 3 TRADITIONAL INDIVIDUAL RETIREMENT ACCOUNT DISCLOSURE 4