Laparoscopic gastric pouch and remnant resection: a novel approach to. refractory anastomotic ulcers after Roux-en-Y Gastric Bypass: Case report
|
|
|
- Kelly Bryan
- 8 years ago
- Views:
Transcription
1 Laparoscopic gastric pouch and remnant resection: a novel approach to refractory anastomotic ulcers after Roux-en-Y Gastric Bypass: Case report Daniel C. Steinemann 1, ; Marc Schiesser 1 ; Pierre-Alain Clavien 1 ; Antonio Nocito 1 1 Department of Visceral and Transplantation Surgery, University Hospital Zurich, Raemistrasse 0, 01 Zurich, Switzerland Department of Surgery, Cantonal Hospital Bruderholz, Bruderholz, Switzerland 1 corresponding author adresses: DCS: MS : PAC : AN: daniel.steinemann@gmx.ch marc.schiesser@usz.ch clavien@access.uzh.ch antonio.nocito@usz.ch

2 Abstract Background: Anastomotic or marginal ulcers occur in 0. to 1 % of patients after laparoscopic Roux-en-Y-Gastric Bypass. Initial therapy aims at eliminating known risk factors including smoking, Helicobacter pylori infection, use of non-steroidal antiinflammatory drugs and inhibition of gastric acid secretion. While this approach is successful in to % of the cases, up to one third of patients need a subsequent surgical revision. However, marginal ulcers still recur in up to % of cases after revisional surgery, thus constituting a serious challenge for bariatric surgeons. Case presentation: We herein report a case of an insidious marginal ulcer refractory to both medical therapy with high-dosed proton pump inhibitors and sucralfate as well as surgical therapy consisting of the lengthening of a short alimentary limb and later resection of the gastroenterostomy and construction of a new tension-free anastomosis. Only after gastrectomy by laparoscopic en-bloc resection of the gastrojejunostomy, the gastric pouch and resection of the gastric remnant with reconstruction by esophagojejunostomy the patient remained free of symptoms. Conclusion: By laparoscopic resection of the entire gastric pouch and the gastric remnant the risk to leave a suboptimally vascularised or even ischemic pouch in situ was avoided. The esophagojejunostomy was then created in healthy, good vascularised tissue. In our case this novel approach was effective in the management of a refractory anastomotic ulcer and might represent a rescue option when simple revision of the gastrojejunostomy fails. Keywords: Roux-en-Y-Gastric Bypass, bariatric surgery, anastomotic ulcer, marginal ulcer, obesity

3 Background A specific complication after laparoscopic Roux-en-Y-Gastric-Bypass (LRYGB) is a marginal or anastomotic ulcer (AU) occurring at the gastrojejunal anastomosis. While AU can remain asymptomatic in -% of the cases [1-], they can frequently cause disabling pain or complications such as perforation and bleeding [, ]. The incidence of AU varies from 0.% to 1% in endoscopic studies [1-] The etiology of AU is unclear. Two classes of risk factors have been suggested: operative and patient related factors. Although large gastric pouch, vertically oriented pouch[], gastro-gastric fistula[], local tissue ischemia due to anastomotic tension [] or presence of foreign bodies in the ulcer ground (e.g. nonabsorbable sutures) [] have been previously discussed, there is still a lack of high level of evidence demonstrating these factors to be significant. In contrast, better data exist for patient related factors, showing that smoking (odds ratio (OR) 0.), use of nonsteroidal anti-inflammatory drugs (OR.) and lack of proton pump inhibitor (PPI) prophylaxis (OR ) represent significant risk factors []. Therefore, ulcer therapy starts with elimination of patient related risk factors and inhibition of gastric acid secretion. While this approach is successful in to %, up to one third of the patients need a subsequent surgical revision [, 1]. Although revision surgery is successful in most cases, AU recur in up to % [], thus leading to a distressing situation for both patients and bariatric surgeons.
![% to 1% in endoscopic studies [1-]. 1 1 1 1 1 1 1 1 0 1 The etiology of AU is unclear. Two classes of risk factors have been suggested: operative and patient related factors.](/docs-images/49/17035271/images/page_3.jpg "Although large gastric pouch, vertically oriented pouch[], gastro-gastric fistula[], local tissue ischemia due to anastomotic tension [] or presence of foreign bodies in the ulcer ground (e.g. nonabsorbable sutures) [] have been previously discussed, there is still a lack of high level of evidence demonstrating these factors to be significant.")
4 We herein report a case of an insidious AU refractory medical and surgical therapy, which finally required an aggressive approach consisting of laparoscopic gastric pouch and gastric remnant resection.

5 Case presentation In a 0 year male patient with a BMI of kg/m an antecolic, antegastric LRYGB with a 0 cm alimentary and a 0 cm biliary limb was performed. The gastrojejunostomy was constructed using a mm circular stapler (EEA,. mm Staples, Covidien ). Simultaneously, a cm silastic (Fobi) ring was placed around the gastrojejunostomy. A few weeks after discharge, the patient, who continued smoking after surgery, presented with strong epigastric pain, postprandial regurgitation and vomiting. He was unable to eat solid food and to attend work. Endoscopy revealed two AU at the gastrojejunostomy. Oral PPI therapy (esomeprazole, 0mg/die) was initiated and, since it was thought to be partly responsible for the symptoms, the silastic ring was removed. Intravenous highdose PPI (esomeprazole, 0mg/die) led to healing of the AU. However, epigastric pain and regurgitation did not ameliorate. A m Tc-mebrofenin scintigraphy revealed severe biliary reflux. Seven months after LRYGB the patient was referred to our department At the initial consultation the patient was taking up to 00 mg/ day esomeprazole and 00 mg/ day tilidin orally. As an AU could not be detected further diagnostic investigations were performed: Upper gastrointestinal (GI) contrast series revealing a small gastric pouch without signs of a gastric fistula and normal passage. Double balloon push enteroscopy demonstrating a short (0 cm) alimentary limb. High-resolution esophageal manometry revealing a normotensive propulsive peristalsis and a normotense lower esophageal sphincter.

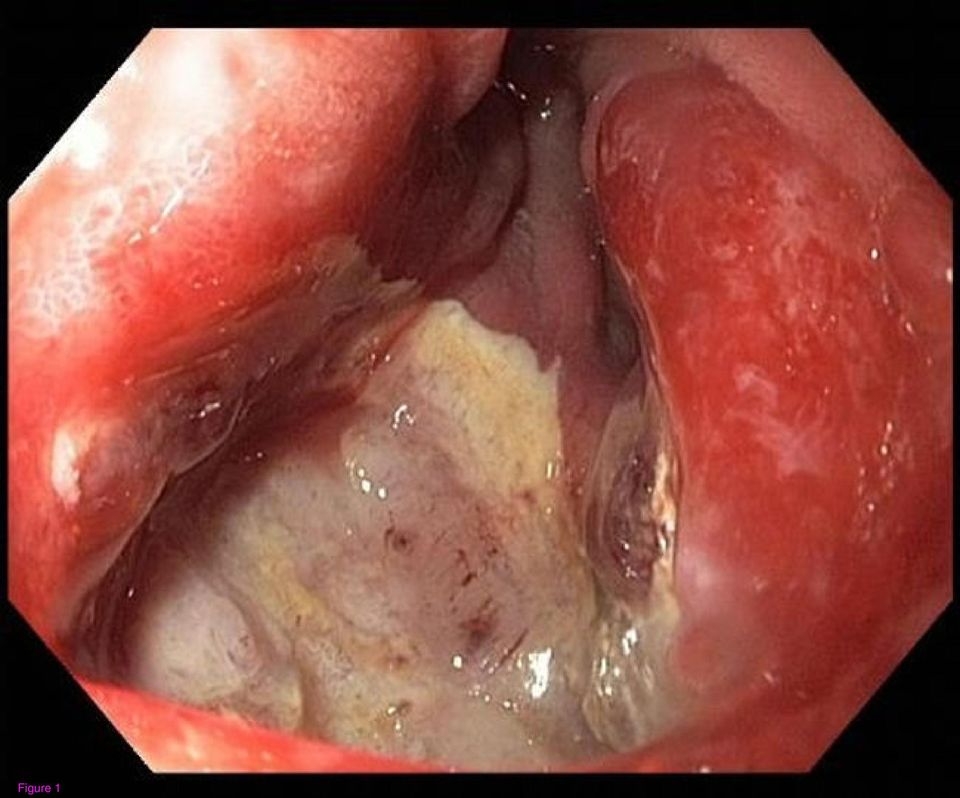
6 h-impedance ph-metry - performed under antacid medication - showing no pathological acid or non-acid reflux. MRI in Sellink technique showing no obstruction of the small bowel. Apart from the biliary reflux diagnosed by scintigraphy consistent with a very short Rouxlimb by push-enteroscopy, no other reason for the epigastric pain was detected. We performed a laparoscopic lengthening of the Roux limb by additional cm resulting in a new alimentary limb of cm. Oral PPI therapy (0 mg/day) was continued and sucralfate (g/d) was added After a short period without pain and regurgitation, symptoms recurred two weeks after Roux limb lengthening. Despite PPI therapy endoscopy revealed a recurrent AU at the gastrojejunostomy (Figure 1). Therefore a laparoscopic resection of the gastrojejunostomy was performed followed by a construction of a new, tension-free anastomosis using a mm circular stapler (EEA,. mm Staples, Covidien ). PPI therapy and sucralfate were continued. Again the patient was discharged free of symptoms on postoperative day five One month later and one year after initial LRYGB surgery, the patient was again not free of epigastric pain. Gastroscopy showed again a large AU at the gastroenterostomy. Meanwhile, the patient was finally motivated enough to quit smoking and was enrolled in a stop-smoking program. Since gastrin level was not elevated (1 ng/l) an underlying gastrinoma could be excluded. Furthermore, Helicobacter pylori and

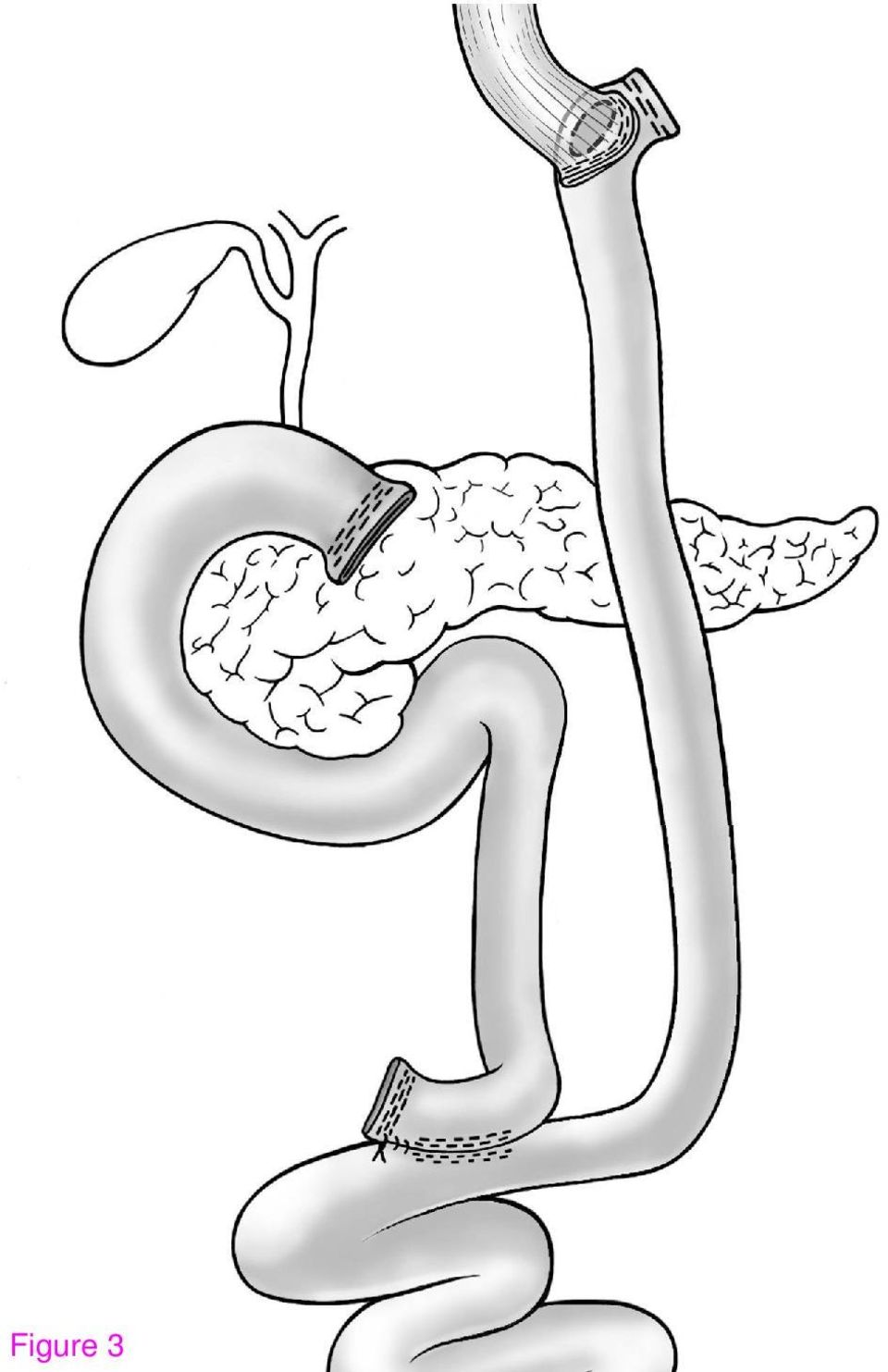
7 hyperparathyroidism as additional potential causes for anastomotic ulcers were also ruled out. Nevertheless, epigastric pain and the AU persisted. At this point an aggressive approach was decided consisting of a gastrectomy by laparoscopic en-bloc resection of the gastrojejunostomy and the gastric pouch with transsection cm proximal to the angle of His and resection of the gastric remnant (Figure ). The gastrointestinal continuity was re-established by the construction of an esophagojejunostomy using a mm circular stapler (Figure ). Two days after surgery an upper GI contrast series showed no leakage or stenosis at the level of the esophagojejunostomy. The patient was discharged on postoperative day. Six months later the patient was free of symptoms, he was able to start opioid weaning and had regained kg of weight. Finally, endoscopy showed a regular esophagojejunostomy. 1

8 Discussion and conclusion Our case of a persistently recurring AU is representative for the current shortcomings in understanding the pathogenesis and thus optimal treatment of AU. We describe a successful approach for the management of intractable AU After LRYGB up to % of patients develop upper GI symptoms. Analysis and management of this condition is often challenging as % of symptomatic patients show a normal anatomy at endoscopy [1]. Conservative therapy has been reported to be successful in %-% of the cases [, 1]. In our case, endoscopy showed no abnormalities apart from a short Roux limb at the time of referral. As a short Roux limb may facilitate biliary reflux causing postoperative pain and AU [1], we decided to lengthen the alimentary limb. Despite improvement of regurgitation symptoms, epigastric pain and AU recurred Approximately one third of AU recur after medical therapy. For these cases a redo of the gastrojejunostomy with a success rate of % has been advised []. Before we embarked on this strategy, we reevaluated whether putative factors leading to a recurrence were present. Endoscopy and GI contrast series excluded potential operative risk factors. Therefore a resection of the gastrojejunostomy with subsequent PPI therapy was performed. However, the ulcer recurred potentially due to the inability of the patient to quit smoking.
![Analysis and management of this condition is often challenging as % of symptomatic patients show a normal anatomy at endoscopy [1].](/docs-images/49/17035271/images/page_8.jpg "Conservative therapy has been reported to be successful in %-% of the cases [, 1]. In our case, endoscopy showed no abnormalities apart from a short Roux limb at the time of referral.")
9 After revision surgery for AU, a recurrence rate of % has been described. In these cases, revision of the gastrojejunostomy combined with gastric remnant resection has been advocated reducing gastrin-producing- and parietal cells []. 1 1 In contrast to the proposed simple revision of the anastomosis, we opted for a laparoscopic resection of the entire gastric pouch and the gastric remnant. By this means, the risk to leave a suboptimally vascularised or even ischemic pouch in situ was avoided since the resection was taken back to esophageal tissue. The circular esophagojejunostomy was then created in healthy, good vascularised tissue. Subsequently, the patient was free of symptoms and no recurrence was observed after a follow-up of months. Hence, in our case this novel approach was effective in the management of a refractory AU and might represent a rescue option when simple revision of the gastrojejunostomy fails

10 Competing interests The authors declare that they have no competing interests. No financial support has been received. Consent Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Permissions None of the material has been previously published Authors contributions DCS drafted and finalized the manuscript, MS and PAC reviewed the manuscript, AN performed the surgery, monitored the drafting and critically reviewed the manuscript and has given final approve for publication. All authors read and approved the final manuscript Acknowledgments We thank Marco Bueter and Paul Schneider of the Department of Visceral and Transplantation Surgery, University Hospital Zurich, for the critical review of the manuscript. This study is not externally funded by government or charity foundations. No funding or assistance is received from commercial organizations.

11 References Garrido Jr AB, Rossi M, Lima Jr SE, Brenner AS, Gomes Jr CA: Early marginal ulcer following Roux-en-Y gastric bypass under proton pump inhibitor treatment: prospective multicentric study. Arq Gastroenterol 0, ():-1.. Csendes A, Burgos AM, Altuve J, Bonacic S: Incidence of marginal ulcer 1 month and 1 to years after gastric bypass: a prospective consecutive endoscopic evaluation of patients with morbid obesity. Obes Surg 00, 1():1-1.. Vasquez JC, Wayne Overby D, Farrell TM: Fewer gastrojejunostomy strictures and marginal ulcers with absorbable suture. Surg Endosc 00, (): D'Hondt MA, Pottel H, Devriendt D, Van Rooy F, Vansteenkiste F: Can a short course of prophylactic low-dose proton pump inhibitor therapy prevent stomal ulceration after laparoscopic Roux-en-Y gastric bypass? Obes Surg 0, 0():-.. Wheeler AA, de la Torre RA, Fearing NM: Laparoscopic repair of perforated marginal ulcer following Roux-en-Y gastric bypass: a case series. J Laparoendosc Adv Surg Tech A 0, 1(1):-0.. Avgerinos DV, Llaguna OH, Seigerman M, Lefkowitz AJ, Leitman IM: Incidence and risk factors for the development of anemia following gastric bypass surgery. World J Gastroenterol 0, 1(1):1-.. Sapala JA, Wood MH, Sapala MA, Flake TM, Jr.: Marginal ulcer after gastric bypass: a prospective -year study of 1 patients. Obes Surg 1, ():0-1.. Patel RA, Brolin RE, Gandhi A: Revisional operations for marginal ulcer after Rouxen-Y gastric bypass. Surg Obes Relat Dis 00, ():1-.

12 Nguyen NT, Hinojosa M, Fayad C, Varela E, Wilson SE: Use and outcomes of laparoscopic versus open gastric bypass at academic medical centers. J Am Coll Surg 00, 0():-.. Sacks BC, Mattar SG, Qureshi FG, Eid GM, Collins JL, Barinas-Mitchell EJ, Schauer PR, Ramanathan RC: Incidence of marginal ulcers and the use of absorbable anastomotic sutures in laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis 00, (1):- 1.. Wilson JA, Romagnuolo J, Byrne TK, Morgan K, Wilson FA: Predictors of endoscopic findings after Roux-en-Y gastric bypass. Am J Gastroenterol 00, 1(): Carrodeguas L, Szomstein S, Soto F, Whipple O, Simpfendorfer C, Gonzalvo JP, Villares A, Zundel N, Rosenthal R: Management of gastrogastric fistulas after divided Rouxen-Y gastric bypass surgery for morbid obesity: analysis of 1, consecutive patients and review of literature. Surg Obes Relat Dis 00, 1():-. 1. Lee JK, Van Dam J, Morton JM, Curet M, Banerjee S: Endoscopy is accurate, safe, and effective in the assessment and management of complications following gastric bypass surgery. Am J Gastroenterol 00, ():-; quiz. 1. Swartz DE, Mobley E, Felix EL: Bile reflux after Roux-en-Y gastric bypass: an unrecognized cause of postoperative pain. Surg Obes Relat Dis 00, (1):

13 Figure legends Figure 1: Figure : Figure : Recurrent anastomotic ulcer in the intestinal part of the gastrojejunostomy Situs after en-bloc resection of the gastric pouch and the gastrojejunostomy (1=esophagus, =hepatoduodenal ligament, =caudate lobe) Roux-Y reconstruction with esophagojejunostomy 1
 Roux-Y reconstruction with")
14 Figure 1
15 Figure

16 Figure
Acute Abdominal Pain following Bariatric Surgery. Disclosure. Objectives 8/17/2015. I have nothing to disclose
 Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
Endoscopic gastric pouch plication - a novel endoluminal incision free approach to revisional bariatric surgery
 Endoscopic gastric pouch plication - a novel endoluminal incision free approach to revisional bariatric surgery Authors: Chiranjiv S Virk, I Michael Leitman and Elliot R Goodman. Location: Beth Israel
Endoscopic gastric pouch plication - a novel endoluminal incision free approach to revisional bariatric surgery Authors: Chiranjiv S Virk, I Michael Leitman and Elliot R Goodman. Location: Beth Israel
Types of Bariatric Procedures. Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012
 Types of Bariatric Procedures Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012 A Brief History of Bariatric Surgery First seen in pts with short bowel syndrome weight loss First
Types of Bariatric Procedures Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012 A Brief History of Bariatric Surgery First seen in pts with short bowel syndrome weight loss First
11/10/2014. I have nothing to Disclose. Covered Stents discussed are NOT FDA approved for the indications covered in my presentation
 I have nothing to Disclose Ramsey Dallal, MD, FACS Vice Chair Department of Surgery Chief Bariatric i and Minimally i Invasive Surgery Einstein Healthcare Network Nemacolin, PA 2014 Covered Stents discussed
I have nothing to Disclose Ramsey Dallal, MD, FACS Vice Chair Department of Surgery Chief Bariatric i and Minimally i Invasive Surgery Einstein Healthcare Network Nemacolin, PA 2014 Covered Stents discussed
Roux-en-y gastric bypass - clinical perspectives
 Roux-en-y gastric bypass - clinical perspectives Tom Mala Consultant surgeon Department of Gastroenterologic Surgery Oslo University Hospital Bariatric surgery weight loss Sjøstrøm L, JAMA 2012 Five-year
Roux-en-y gastric bypass - clinical perspectives Tom Mala Consultant surgeon Department of Gastroenterologic Surgery Oslo University Hospital Bariatric surgery weight loss Sjøstrøm L, JAMA 2012 Five-year
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201420 APRIL 29, 2014
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201420 APRIL 29, 2014 IHCP to cover sleeve gastrectomy surgery The Indiana Health Coverage Programs (IHCP) covers bariatric surgery for individuals with
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201420 APRIL 29, 2014 IHCP to cover sleeve gastrectomy surgery The Indiana Health Coverage Programs (IHCP) covers bariatric surgery for individuals with
Emergencies in Post- Bariatric Surgery Patients
 Emergencies in Post- Patients Disclosures Dr. Birnbaumer has no financial disclosures Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator
Emergencies in Post- Patients Disclosures Dr. Birnbaumer has no financial disclosures Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator
Laparoscopic Revisional Gastric Bypass after open bariatric surgeries. Haider Alshurafa 1
 Laparoscopic Revisional Gastric Bypass after open bariatric surgeries 1 Surgery Department, Riyadh Military Hospital, Riyadh, Saudi Arabia Haider Alshurafa 1 Objective: To confirm the feasibility of the
Laparoscopic Revisional Gastric Bypass after open bariatric surgeries 1 Surgery Department, Riyadh Military Hospital, Riyadh, Saudi Arabia Haider Alshurafa 1 Objective: To confirm the feasibility of the
Dept. of Medical Imaging University of Ottawa
 ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
Endoscopic therapy for obesity and complications of bariatric surgery
 Endoscopic therapy for obesity and complications of bariatric surgery Jacques Devière, MD, PhD Erasme University Hospital Brussels Belgium jacques.deviere@erasme.ulb.ac.be Obesity Affects 300 millions
Endoscopic therapy for obesity and complications of bariatric surgery Jacques Devière, MD, PhD Erasme University Hospital Brussels Belgium jacques.deviere@erasme.ulb.ac.be Obesity Affects 300 millions
The hidden endoscopic burden of sleeve gastrectomy and its comparison with Roux-en-Y gastric bypass
 ORIGINAL ARTICLE Annals of Gastroenterology (2015) 28, 1-6 The hidden endoscopic burden of sleeve gastrectomy and its comparison with Roux-en-Y gastric bypass Katherine Arndtz a, Helen Steed b, James Hodson
ORIGINAL ARTICLE Annals of Gastroenterology (2015) 28, 1-6 The hidden endoscopic burden of sleeve gastrectomy and its comparison with Roux-en-Y gastric bypass Katherine Arndtz a, Helen Steed b, James Hodson
Endoscopic Management of Strictures and Leaks. Prepared by Aurora D. Pryor, MD Presented by Dana Portenier, MD Duke University Medical Center
 Endoscopic Management of Strictures and Leaks Prepared by Aurora D. Pryor, MD Presented by Dana Portenier, MD Duke University Medical Center What can go wrong? Bleeding (2%) Sleeve too big Angulated Too
Endoscopic Management of Strictures and Leaks Prepared by Aurora D. Pryor, MD Presented by Dana Portenier, MD Duke University Medical Center What can go wrong? Bleeding (2%) Sleeve too big Angulated Too
Bariatric i Surgery: Optimalizing Outcome Results. Dr. B. Dillemans AZ Sint-Jan AV Brugge-Oostende BARIATRIC SURGERY
 Bariatric i Surgery: Optimalizing i Outcome Results Dr. B. Dillemans AZ Sint-Jan AV Brugge-Oostende THE OBESE PATIENT : A CHALLENGE FOR ANAESTHESIA, Ostend,14/11/09 BARIATRIC SURGERY 50 s : First Reported
Bariatric i Surgery: Optimalizing i Outcome Results Dr. B. Dillemans AZ Sint-Jan AV Brugge-Oostende THE OBESE PATIENT : A CHALLENGE FOR ANAESTHESIA, Ostend,14/11/09 BARIATRIC SURGERY 50 s : First Reported
Gastric Bypass and Other Bariatric Surgical Procedures*
 Subject: Gastric Bypass and Other Bariatric Surgical Procedures* Updated: February 24, 2009 Department(s): Policy: Objective: Utilization Management Medically necessary bariatric surgical procedures are
Subject: Gastric Bypass and Other Bariatric Surgical Procedures* Updated: February 24, 2009 Department(s): Policy: Objective: Utilization Management Medically necessary bariatric surgical procedures are
Intraoperative Prevention of Stenosis for Laparoscopic Sleeve Gastrectomy
 CASE REPORT Intraoperative Prevention of Stenosis for Laparoscopic Sleeve Gastrectomy Ramon Vilallonga, MD, PhD, Jacques Himpens, MD Division of Bariatric Surgery, AZ St. Blasius, Dendermonde, Belgium
CASE REPORT Intraoperative Prevention of Stenosis for Laparoscopic Sleeve Gastrectomy Ramon Vilallonga, MD, PhD, Jacques Himpens, MD Division of Bariatric Surgery, AZ St. Blasius, Dendermonde, Belgium
Laparoscopic Adjustable Gastric Banding as a Type of Weight Loss
 Laparoscopic Adjustable Gastric Banding as a Type of Weight Loss Abstract Obesity has become a global health crisis. Traditional treatments try to modify behavior in regard to diet and exercise. Laparoscopic
Laparoscopic Adjustable Gastric Banding as a Type of Weight Loss Abstract Obesity has become a global health crisis. Traditional treatments try to modify behavior in regard to diet and exercise. Laparoscopic
Valk J.W., Gypen B., Abdelgabar A., Hendrickx L. Schijns W., Aarts E., Janssen I., Berends F. Rheinwalt K.P., Schneider S., Plamper A.
 Revisional Surgery for Weight Regain or Insufficient Weight Loss after Gastric Bypass using the Minimizer Ring: Short Term Results of a Multi Center Study Valk J.W., Gypen B., Abdelgabar A., Hendrickx
Revisional Surgery for Weight Regain or Insufficient Weight Loss after Gastric Bypass using the Minimizer Ring: Short Term Results of a Multi Center Study Valk J.W., Gypen B., Abdelgabar A., Hendrickx
When, Why, and How to Revise a Failed Sleeve Gastrectomy
 When, Why, and How to Revise a Failed Sleeve Gastrectomy Jin S. Yoo M.D. Assistant Professor of Surgery Duke University Medical Center April 6, 2013 When and Why Already Covered Let s Talk About How Overview
When, Why, and How to Revise a Failed Sleeve Gastrectomy Jin S. Yoo M.D. Assistant Professor of Surgery Duke University Medical Center April 6, 2013 When and Why Already Covered Let s Talk About How Overview
Laparoscopic One Anastomosis Gastric Bypass (LOAGB) How I do it
 How I do it") CENTER OF EXCELLENCE FOR THE STUDY AND OBESITY TREATMENT Laparoscopic One Anastomosis Gastric Bypass (LOAGB) How I do it Concepts and Results in a series of 11-years experience with 2,200 patients Miguel-A.
CENTER OF EXCELLENCE FOR THE STUDY AND OBESITY TREATMENT Laparoscopic One Anastomosis Gastric Bypass (LOAGB) How I do it Concepts and Results in a series of 11-years experience with 2,200 patients Miguel-A.
Revisional Bariatric Surgery
 Revisional Bariatric Surgery Todd Andrew Kellogg, MD KEYWORDS Bariatric surgery Revision Reoperation OVERVIEW With the increasing number of bariatric procedures being performed annually, it is expected
Revisional Bariatric Surgery Todd Andrew Kellogg, MD KEYWORDS Bariatric surgery Revision Reoperation OVERVIEW With the increasing number of bariatric procedures being performed annually, it is expected
Surgical & Nutritional Complications of Bariatric Surgery: What Every GI Doc Needs to Know Brian R. Smith, MD, FACS Associate Clinical Professor of
 Surgical & Nutritional Complications of Bariatric Surgery: What Every GI Doc Needs to Know Brian R. Smith, MD, FACS Associate Clinical Professor of Surgery & Associate Residency Program Director UC Irvine
Surgical & Nutritional Complications of Bariatric Surgery: What Every GI Doc Needs to Know Brian R. Smith, MD, FACS Associate Clinical Professor of Surgery & Associate Residency Program Director UC Irvine
The GaBP Ring for Banding the Pouch in Gastric Bypass and Sleeve Gastrectomy Operations BARIATEC.COM
 The GaBP Ring for Banding the Pouch in Gastric Bypass and Sleeve Gastrectomy Operations BARIATEC.COM GaBP Ring The GaBP Ring is a prefabricated, caliberated and sterilized silicone coated implantable device
The GaBP Ring for Banding the Pouch in Gastric Bypass and Sleeve Gastrectomy Operations BARIATEC.COM GaBP Ring The GaBP Ring is a prefabricated, caliberated and sterilized silicone coated implantable device
Overview of Bariatric Surgery
 Overview of Bariatric Surgery To better understand how weight loss surgery works, it is helpful to know how the normal digestive process works. As food moves along the digestive tract, special digestive
Overview of Bariatric Surgery To better understand how weight loss surgery works, it is helpful to know how the normal digestive process works. As food moves along the digestive tract, special digestive
Aaron B. House MD, PGY-5 University of Kentucky Department of General Surgery Grand Rounds October 23, 2013
 Aaron B. House MD, PGY-5 University of Kentucky Department of General Surgery Grand Rounds October 23, 2013 Objectives Briefly illustrate the recent obesity trends in the U.S Give a brief history of bariatric
Aaron B. House MD, PGY-5 University of Kentucky Department of General Surgery Grand Rounds October 23, 2013 Objectives Briefly illustrate the recent obesity trends in the U.S Give a brief history of bariatric
Weight loss surgery more than just a gastric band
 Weight loss surgery more than just a gastric band Presented by Ms Beth Murgatroyd Honorary Bariatric Nurse Practitioner Mr Ameet G Patel Consultant Surgeon Director of Bariatric Surgery at King s College
Weight loss surgery more than just a gastric band Presented by Ms Beth Murgatroyd Honorary Bariatric Nurse Practitioner Mr Ameet G Patel Consultant Surgeon Director of Bariatric Surgery at King s College
Vertical Sleeve Gastrectomy (VSG) - Also known as Sleeve Gastrectomy, Vertical Gastrectomy
 - Also known as Sleeve Gastrectomy, Vertical Gastrectomy") Vertical Sleeve Gastrectomy (VSG) - Also known as Sleeve Gastrectomy, Vertical Gastrectomy The Vertical Sleeve Gastrectomy procedure (also called Sleeve Gastrectomy, Vertical Gastrectomy, Greater Curvature
Vertical Sleeve Gastrectomy (VSG) - Also known as Sleeve Gastrectomy, Vertical Gastrectomy The Vertical Sleeve Gastrectomy procedure (also called Sleeve Gastrectomy, Vertical Gastrectomy, Greater Curvature
Effect of Gastric Bypass on Barrett s Esophagus and Intestinal Metaplasia of the Cardia in Patients With Morbid Obesity
 Effect of Gastric Bypass on Barrett s Esophagus and Intestinal Metaplasia of the Cardia in Patients With Morbid Obesity Attila Csendes, M.D., F.A.C.S. (Hon), Ana Maria Burgos, M.D., Gladys Smok, M.D.,
Effect of Gastric Bypass on Barrett s Esophagus and Intestinal Metaplasia of the Cardia in Patients With Morbid Obesity Attila Csendes, M.D., F.A.C.S. (Hon), Ana Maria Burgos, M.D., Gladys Smok, M.D.,
BARIATRIC SURGERY AND OTHER INVASIVE TREATMENTS FOR OBESITY
 Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline must be read in its
Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline must be read in its
5. Conversion Procedures that change from an index procedure to a different type of procedure.
 Benefit Coverage Covered Benefit for lines of business including Health Benefits Exchange (HBE), Rite Care (MED), Children with Special Needs (CSN), Substitute Care (SUB), Rhody Health Partners (RHP),
Benefit Coverage Covered Benefit for lines of business including Health Benefits Exchange (HBE), Rite Care (MED), Children with Special Needs (CSN), Substitute Care (SUB), Rhody Health Partners (RHP),
Obesity When to Recommend Surgery. Lily Chang, MD September 27, 2013
 Obesity When to Recommend Surgery Lily Chang, MD September 27, 2013 Obesity BMI >30 Trends Among U.S. Adults Source: Behavioral Risk Factor Surveillance System, CDC, 2012 Obesity Related Co-Morbidities
Obesity When to Recommend Surgery Lily Chang, MD September 27, 2013 Obesity BMI >30 Trends Among U.S. Adults Source: Behavioral Risk Factor Surveillance System, CDC, 2012 Obesity Related Co-Morbidities
White Paper: Treating Clinical Obesity: When is Bariatric Surgery or Bariatric Surgery Revision Medically Necessary?
 White Paper: Treating Clinical Obesity: When is Bariatric Surgery or Bariatric Surgery Revision Medically Necessary? For Health Plans, Medical Management Organizations and TPAs Introduction More than one
White Paper: Treating Clinical Obesity: When is Bariatric Surgery or Bariatric Surgery Revision Medically Necessary? For Health Plans, Medical Management Organizations and TPAs Introduction More than one
Maximal weight loss after banded and unbanded laparoscopic Roux-en-Y gastric bypass: a randomized controlled trial
 Surgery for Obesity and Related Diseases 4 (2008) 507 511 Original article Maximal weight loss after banded and unbanded laparoscopic Roux-en-Y gastric bypass: a randomized controlled trial Ricardo Arceo-Olaiz,
Surgery for Obesity and Related Diseases 4 (2008) 507 511 Original article Maximal weight loss after banded and unbanded laparoscopic Roux-en-Y gastric bypass: a randomized controlled trial Ricardo Arceo-Olaiz,
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy. Patient Name
 Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Technical Aspects of Bariatric Surgical Procedures. Robert O. Carpenter, MD, MPH, FACS Department of Surgery Scott & White Memorial Hospital
 Technical Aspects of Bariatric Surgical Procedures Robert O. Carpenter, MD, MPH, FACS Department of Surgery Scott & White Memorial Hospital Disclosures Allergan, Inc. (Past) Faculty Member Educational
Technical Aspects of Bariatric Surgical Procedures Robert O. Carpenter, MD, MPH, FACS Department of Surgery Scott & White Memorial Hospital Disclosures Allergan, Inc. (Past) Faculty Member Educational
Richard M Peterson, MD MPH FACS Chief UT Medicine Center for Bariatric and Metabolic Surgery Director Christus Weight Loss Institute Assistant
 Richard M Peterson, MD MPH FACS Chief UT Medicine Center for Bariatric and Metabolic Surgery Director Christus Weight Loss Institute Assistant Professor of Surgery UTHSCSA None Laparoscopic adjustable
Richard M Peterson, MD MPH FACS Chief UT Medicine Center for Bariatric and Metabolic Surgery Director Christus Weight Loss Institute Assistant Professor of Surgery UTHSCSA None Laparoscopic adjustable
Early jejunojejunostomy obstruction after laparoscopic gastric bypass: case series and treatment algorithm
 Surgery for Obesity and Related Diseases 5 (2009) 203 207 Original article Early jejunojejunostomy obstruction after laparoscopic gastric bypass: case series and treatment algorithm Catherine E. Lewis,
Surgery for Obesity and Related Diseases 5 (2009) 203 207 Original article Early jejunojejunostomy obstruction after laparoscopic gastric bypass: case series and treatment algorithm Catherine E. Lewis,
Novel treatments for complications after bariatric surgery
 DOI 10.1186/s13022-015-0021-2 REVIEW Open Access Novel treatments for complications after bariatric surgery Julián Hernández 1 and Camilo Boza 2* Abstract Bariatric surgery has been considered one of best
DOI 10.1186/s13022-015-0021-2 REVIEW Open Access Novel treatments for complications after bariatric surgery Julián Hernández 1 and Camilo Boza 2* Abstract Bariatric surgery has been considered one of best
Gastric Stenosis After Laparoscopic Sleeve Gastrectomy in Morbidly Obese Patients
 OBES SURG (2013) 23:1481 1486 DOI 10.1007/s11695-013-0963-6 REVIEW Gastric Stenosis After Laparoscopic Sleeve Gastrectomy in Morbidly Obese Patients Ana María Burgos & Attila Csendes & Italo Braghetto
OBES SURG (2013) 23:1481 1486 DOI 10.1007/s11695-013-0963-6 REVIEW Gastric Stenosis After Laparoscopic Sleeve Gastrectomy in Morbidly Obese Patients Ana María Burgos & Attila Csendes & Italo Braghetto
Small Bowel Obstruction After Laparoscopic Roux En - Y Gastric Bypass
 14 Small Bowel Obstruction After Laparoscopic Roux En - Y Gastric Bypass Hugo Sánchez and Miguel F Herrera The Obesity clinic. ABC Medical Center México 1. Introduction Obesity is an important health problem
14 Small Bowel Obstruction After Laparoscopic Roux En - Y Gastric Bypass Hugo Sánchez and Miguel F Herrera The Obesity clinic. ABC Medical Center México 1. Introduction Obesity is an important health problem
Informed Consent for Laparoscopic Roux en Y Gastric Bypass. Patient Name
 Informed Consent for Laparoscopic Roux en Y Gastric Bypass Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Roux en Y Gastric
Informed Consent for Laparoscopic Roux en Y Gastric Bypass Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Roux en Y Gastric
Marginal Ulcers. Marginal Ulcers. Gastric Remnant Ulcers. Double Balloon Enteroscopy. Marginal Ulcer. Gastrojejunal Stricture.
 Upper Abdominal Pain in the Bariatric Surgery Patient Martin L. Freeman, M.D., FASGE,FACG Professor of Medicine Director, Pancreaticobiliary Endoscopy Fellowship Interim Director, Division of GI, Hepatology
Upper Abdominal Pain in the Bariatric Surgery Patient Martin L. Freeman, M.D., FASGE,FACG Professor of Medicine Director, Pancreaticobiliary Endoscopy Fellowship Interim Director, Division of GI, Hepatology
PATIENT CONSENT TO PROCEDURE - ROUX-EN-Y GASTRIC BYPASS
 As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
BARIATRIC SURGERY MAY CURE TYPE 2 DIABETES IN SOME PATIENTS
 BARIATRIC SURGERY MAY CURE TYPE 2 DIABETES IN SOME PATIENTS Thomas Rogula MD, Stacy Brethauer MD, Bipand Chand MD, and Philip Schauer, MD. "Gastric bypass surgery has become a popular option for obese
BARIATRIC SURGERY MAY CURE TYPE 2 DIABETES IN SOME PATIENTS Thomas Rogula MD, Stacy Brethauer MD, Bipand Chand MD, and Philip Schauer, MD. "Gastric bypass surgery has become a popular option for obese
Use of bioabsorbable staple reinforcement material in gastric bypass: a prospective randomized clinical trial
 Surgery for Obesity and Related Diseases 3 (2007) 417 422 Original article Use of bioabsorbable staple reinforcement material in gastric bypass: a prospective randomized clinical trial Karl A. Miller,
Surgery for Obesity and Related Diseases 3 (2007) 417 422 Original article Use of bioabsorbable staple reinforcement material in gastric bypass: a prospective randomized clinical trial Karl A. Miller,
Sleeve gastrectomy or gastric bypass as revisional bariatric procedures: retrospective evaluation of outcomes. Abstract Background Methods:
 Sleeve gastrectomy or gastric bypass as revisional bariatric procedures: retrospective evaluation of outcomes. Mousa Khoursheed, Ibtisam Al-Bader, Ali Mouzannar, Abdulla Al-Haddad, Ali Sayed, Ali Mohammad,
Sleeve gastrectomy or gastric bypass as revisional bariatric procedures: retrospective evaluation of outcomes. Mousa Khoursheed, Ibtisam Al-Bader, Ali Mouzannar, Abdulla Al-Haddad, Ali Sayed, Ali Mohammad,
Feasibility of Sleeve Gastrectomy as a Revision Operation for Failed Silastic Ring Vertical Gastroplasty
 DOI 10.1007/s11695-008-9714-5 RESEARCH ARTICLE Feasibility of Sleeve Gastrectomy as a Revision Operation for Failed Silastic Ring Vertical Gastroplasty Ram Elazary & David Hazzan & Liat Appelbaum & Avraham
DOI 10.1007/s11695-008-9714-5 RESEARCH ARTICLE Feasibility of Sleeve Gastrectomy as a Revision Operation for Failed Silastic Ring Vertical Gastroplasty Ram Elazary & David Hazzan & Liat Appelbaum & Avraham
Endoluminal Bariatric Revision. Todd David Wilson, MD
 Endoluminal Bariatric Revision Todd David Wilson, MD Surgical Endoscopy and the Bariatric Surgeon Preoperative Endoscopy Postoperative Endoscopy Revisional Endoscopy Primary Endoluminal Bariatrics Preoperative
Endoluminal Bariatric Revision Todd David Wilson, MD Surgical Endoscopy and the Bariatric Surgeon Preoperative Endoscopy Postoperative Endoscopy Revisional Endoscopy Primary Endoluminal Bariatrics Preoperative
MEDICAL POLICY No. 91595-R2 SURGICAL TREATMENT OF OBESITY
 SURGICAL TREATMENT OF OBESITY Effective Date: October 1, 2015 Review Dates: 8/11, 12/11, 2/12, 2/13, 2/14, 11/14, 2/15 Date Of Origin: August 10, 2011 Status: Current Note: This medical policy does not
SURGICAL TREATMENT OF OBESITY Effective Date: October 1, 2015 Review Dates: 8/11, 12/11, 2/12, 2/13, 2/14, 11/14, 2/15 Date Of Origin: August 10, 2011 Status: Current Note: This medical policy does not
Why a loop and new approach makes sense!
 IP: tomach Intestinal Pylorus paring urgery Why a loop and new approach makes sense! Mitchell Roslin, MD, FAC Chief of Bariatric and Metabolic urgery Lenox Hill Hospital Northern Westchester Hospital Center
IP: tomach Intestinal Pylorus paring urgery Why a loop and new approach makes sense! Mitchell Roslin, MD, FAC Chief of Bariatric and Metabolic urgery Lenox Hill Hospital Northern Westchester Hospital Center
MH. Huang Show Chwan Memorial Hospital Changhua, Taïwan
 PROGRAM ENDOLUMIINAL AND LAPAROSCOPIIC BARIIATRIIC AND METABOLIIC SURGERY COURSE SEPTEMBER 10 12,, 2015 CHHAAIIRRMMAANN MH. Huang Show Chwan Memorial Hospital Changhua, Taïwan PPRREESSIIDDEENNTT SSUUPPEERRIINNTTEENNDDEENNTT
PROGRAM ENDOLUMIINAL AND LAPAROSCOPIIC BARIIATRIIC AND METABOLIIC SURGERY COURSE SEPTEMBER 10 12,, 2015 CHHAAIIRRMMAANN MH. Huang Show Chwan Memorial Hospital Changhua, Taïwan PPRREESSIIDDEENNTT SSUUPPEERRIINNTTEENNDDEENNTT
Obesity Epidemic - Costs
 What Clinicians should know about Bariatric Surgery Complications Dmitry Nepomnayshy MD Center for Surgical Weight Loss Lahey Clinic Disclosure None Thank Dr. Brams and Dr. Scheiry 1 Obesity Epidemic -
What Clinicians should know about Bariatric Surgery Complications Dmitry Nepomnayshy MD Center for Surgical Weight Loss Lahey Clinic Disclosure None Thank Dr. Brams and Dr. Scheiry 1 Obesity Epidemic -
Some of the diseases and conditions associated with obesity include:
 WEIGHT-LOSS SURGERY facts about obesity Obesity is rapidly becoming the nation s number-one health problem. Of the 97 million Americans who are overweight, 10 million are considered morbidly obese. Obesity
WEIGHT-LOSS SURGERY facts about obesity Obesity is rapidly becoming the nation s number-one health problem. Of the 97 million Americans who are overweight, 10 million are considered morbidly obese. Obesity
Scott A. Shikora, MD, FACS. Sleeve Gastrectomy. Sleeve Gastrectomy. Sleeve Gastrectomy 11/8/2013
 DISCLOSURE Scott A. Shikora, MD, FACS Scott A. Shikora, MD, FACS Associate Professor of Surgery Harvard Medical School Director, Center for Metabolic and Bariatric Surgery Brigham and Women s Hospital
DISCLOSURE Scott A. Shikora, MD, FACS Scott A. Shikora, MD, FACS Associate Professor of Surgery Harvard Medical School Director, Center for Metabolic and Bariatric Surgery Brigham and Women s Hospital
Teresa LaMasters MD, FACS Minimally Invasive Bariatric Surgeon Iowa Health Weight Loss Specialists Throckmorton Surgical Society May 4, 2012
 Laparoscopic Sleeve Gastrectomy Teresa LaMasters MD, FACS Minimally Invasive Bariatric Surgeon Iowa Health Weight Loss Specialists Throckmorton Surgical Society May 4, 2012 Objectives Understand the anatomy
Laparoscopic Sleeve Gastrectomy Teresa LaMasters MD, FACS Minimally Invasive Bariatric Surgeon Iowa Health Weight Loss Specialists Throckmorton Surgical Society May 4, 2012 Objectives Understand the anatomy
Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD)
") ACCEPTED MAN U SCRIPT EARLY VIEW ARTICLE Early View Article: Online published version of an accepted article before inclusion in an issue of International Journal of Hepatobiliary and Pancreatic Diseases
ACCEPTED MAN U SCRIPT EARLY VIEW ARTICLE Early View Article: Online published version of an accepted article before inclusion in an issue of International Journal of Hepatobiliary and Pancreatic Diseases
Bariatric Weight Loss Surgery
 BARIATRIC SURGERY Bariatric Weight Loss Surgery The heart and science of medicine. Weight loss surgery, also known as bariatric surgery, was developed as a tool to help people with morbid obesity reduce
BARIATRIC SURGERY Bariatric Weight Loss Surgery The heart and science of medicine. Weight loss surgery, also known as bariatric surgery, was developed as a tool to help people with morbid obesity reduce
Removal of Peri-Gastric Fat Prevents Acute Obstruction after Lap-Band Surgery
 Obesity Surgery, 14, 224-229 Removal of Peri-Gastric Fat Prevents Acute Obstruction after Lap-Band Surgery Roy Shen, MD; Christine J. Ren, MD Department of Surgery, NYU School of Delivered Medicine, by
Obesity Surgery, 14, 224-229 Removal of Peri-Gastric Fat Prevents Acute Obstruction after Lap-Band Surgery Roy Shen, MD; Christine J. Ren, MD Department of Surgery, NYU School of Delivered Medicine, by
Laparoscopic Roux-En-Y Gastric Bypass Versus Laparoscopic Adjustable Gastric Banding in the
 553148SJS0010.1177/1457496914553148LRYGB vs LAGB in super-obese patients (BMI >50)S. Giordano, et al. research-article2015 Original Article Scandinavian Journal of Surgery 104: 5 9, 2015 Laparoscopic Roux-En-Y
553148SJS0010.1177/1457496914553148LRYGB vs LAGB in super-obese patients (BMI >50)S. Giordano, et al. research-article2015 Original Article Scandinavian Journal of Surgery 104: 5 9, 2015 Laparoscopic Roux-En-Y
Morbid obesity is a chronic condition that
 COSMETIC A Review of Bariatric Surgery Procedures Morbid obesity is a chronic condition that is extremely difficult to treat. In addition to unhealthy food choices and lifestyles, effective treatment for
COSMETIC A Review of Bariatric Surgery Procedures Morbid obesity is a chronic condition that is extremely difficult to treat. In addition to unhealthy food choices and lifestyles, effective treatment for
Surgical Treatment of Obesity: A Surgeon s View
 Surgical Treatment of Obesity: A Surgeon s View Jenny J. Choi, MD Director of Bariatrics Associate Director of Clinical Affairs Assistant Professor of Surgery Albert Einstein School of Medicine Montefiore
Surgical Treatment of Obesity: A Surgeon s View Jenny J. Choi, MD Director of Bariatrics Associate Director of Clinical Affairs Assistant Professor of Surgery Albert Einstein School of Medicine Montefiore
Endoscopic findings and their clinical correlations in patients with symptoms after gastric bypass surgery
 Endoscopic findings and their clinical correlations in patients with symptoms after gastric bypass surgery Christopher S. Huang, MD, R. Armour Forse, MD, Brian C. Jacobson, MD, MPH, Francis A. Farraye,
Endoscopic findings and their clinical correlations in patients with symptoms after gastric bypass surgery Christopher S. Huang, MD, R. Armour Forse, MD, Brian C. Jacobson, MD, MPH, Francis A. Farraye,
Dealing with weight regain after Rouxen-Y gastric bypass: surgical approach
 Dealing with weight regain after Rouxen-Y gastric bypass: surgical approach Robin Blackstone, MD, FACS Masters of Minimally Invasive Bariatric Surgery April 5, 2013 Orlando, Florida Disclosures PI Enteromedics
Dealing with weight regain after Rouxen-Y gastric bypass: surgical approach Robin Blackstone, MD, FACS Masters of Minimally Invasive Bariatric Surgery April 5, 2013 Orlando, Florida Disclosures PI Enteromedics
d EFFECTIVE DATE: 11 5 2014 POLICY LAST UPDATED: 5 29 2015
 Medical Coverage Policy Bariatric Surgery-Not medically necessary procedures d EFFECTIVE DATE: 11 5 2014 POLICY LAST UPDATED: 5 29 2015 OVERVIEW Surgery for obesity, termed bariatric surgery, is a treatment
Medical Coverage Policy Bariatric Surgery-Not medically necessary procedures d EFFECTIVE DATE: 11 5 2014 POLICY LAST UPDATED: 5 29 2015 OVERVIEW Surgery for obesity, termed bariatric surgery, is a treatment
Medical Policy Bariatric Surgery
 Medical Policy Bariatric Surgery Document Number: 001 Commercial MassHealth and Qualified Health Plans Authorization required X X Notification within 24 hours of service or next business day No notification
Medical Policy Bariatric Surgery Document Number: 001 Commercial MassHealth and Qualified Health Plans Authorization required X X Notification within 24 hours of service or next business day No notification
UW MEDICINE PATIENT EDUCATION. Weight Loss Surgery. What is bariatric surgery?
 UW MEDICINE PATIENT EDUCATION Weight Loss Surgery Divided proximal roux-y-gastric bypass, laparoscopic adjustable gastric banding, and laparoscopic sleeve gastrectomy. This section of the Guide to Your
UW MEDICINE PATIENT EDUCATION Weight Loss Surgery Divided proximal roux-y-gastric bypass, laparoscopic adjustable gastric banding, and laparoscopic sleeve gastrectomy. This section of the Guide to Your
Why the band in the Gastric Bypass Operation.
 Center for Surgical Treatment of Obesity, Los Angeles, California C.S.T.O. Why the band in the Gastric Bypass Operation. M.A.L. Fobi, MD F.A.C.S. H. Lee, MD; B. Felahy, MD; N. Fobi, MD; P. Ako, MD Chi
Center for Surgical Treatment of Obesity, Los Angeles, California C.S.T.O. Why the band in the Gastric Bypass Operation. M.A.L. Fobi, MD F.A.C.S. H. Lee, MD; B. Felahy, MD; N. Fobi, MD; P. Ako, MD Chi
ERCP in Post Surgical Anatomy
 ERCP in Post Surgical Anatomy ACG Western Regional Course, 2013 John G. Lee, MD Division of Gastroenterology University of California, Irvine Medical Center Common surgical alterations Intact pancreaticobiliary
ERCP in Post Surgical Anatomy ACG Western Regional Course, 2013 John G. Lee, MD Division of Gastroenterology University of California, Irvine Medical Center Common surgical alterations Intact pancreaticobiliary
Argon Plasma Coagulation of Gastrojejunal Anastomosis for Weight Regain After Gastric Bypass
 Argon Plasma Coagulation of Gastrojejunal Anastomosis for Weight Regain After Gastric Bypass Giorgio A. P. Baretta, Helga C. A. W. Alhinho, Jorge Eduardo F. Matias, João Batista Marchesini, João Henrique
Argon Plasma Coagulation of Gastrojejunal Anastomosis for Weight Regain After Gastric Bypass Giorgio A. P. Baretta, Helga C. A. W. Alhinho, Jorge Eduardo F. Matias, João Batista Marchesini, João Henrique
Emerging Concepts in Bariatric Surgery
 Emerging Concepts in Bariatric Surgery C Y N T H I A L. L O N G, M D, F A C S S I N A I H O S P I T A L O F B A L T I M O R E D E P A R T M E N T O F S U R G E R Y D I V I S I O N O F M I N I M A L L Y
Emerging Concepts in Bariatric Surgery C Y N T H I A L. L O N G, M D, F A C S S I N A I H O S P I T A L O F B A L T I M O R E D E P A R T M E N T O F S U R G E R Y D I V I S I O N O F M I N I M A L L Y
BOMSS POSITION STATEMENT ON MINI GASTRIC BYPASS (LOOP OR SINGLE ANASTOMOSIS GASTRIC BYPASS)
") 1 BOMSS POSITION STATEMENT ON MINI GASTRIC BYPASS (LOOP OR SINGLE ANASTOMOSIS GASTRIC BYPASS) A. Mini Gastric Bypass: Definitions and Procedural Consideration 1. Loop Gastric Bypass Mason and Ito described
1 BOMSS POSITION STATEMENT ON MINI GASTRIC BYPASS (LOOP OR SINGLE ANASTOMOSIS GASTRIC BYPASS) A. Mini Gastric Bypass: Definitions and Procedural Consideration 1. Loop Gastric Bypass Mason and Ito described
BARIATRIC SURGERY. Prerequisites. Authorization, Notification and Referral
 BARIATRIC SURGERY Policy NHP reimburses participating providers for specific types of medically necessary bariatric surgery when needed to either alleviate or correct medical problems caused by severe
BARIATRIC SURGERY Policy NHP reimburses participating providers for specific types of medically necessary bariatric surgery when needed to either alleviate or correct medical problems caused by severe
1HXURJDVWURHQWHURORJ\ 6XUJHU\ BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB /XQG 8QLYHUVLW\ 3XEOLFDWLRQV
 1HXURJDVWURHQWHURORJ\ 6XUJHU\ BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB /XQG 8QLYHUVLW\ 3XEOLFDWLRQV Institutional Repository of Lund University Found at http://lup.lub.lu.se 7KLV LV DQ DXWKRU SURGXFHG YHUVLRQ
1HXURJDVWURHQWHURORJ\ 6XUJHU\ BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB /XQG 8QLYHUVLW\ 3XEOLFDWLRQV Institutional Repository of Lund University Found at http://lup.lub.lu.se 7KLV LV DQ DXWKRU SURGXFHG YHUVLRQ
Endoluminal and Laparoscopic Bariatric & Metabolic Surgery Advanced Course
 Endoluminal and Laparoscopic Bariatric & Metabolic Surgery Advanced Course Directors of the course: Jacques MARESCAUX Michel VIX Manoel GALVAO NETO Silvana PERRETTA France France Brazil Italy Faculty:
Endoluminal and Laparoscopic Bariatric & Metabolic Surgery Advanced Course Directors of the course: Jacques MARESCAUX Michel VIX Manoel GALVAO NETO Silvana PERRETTA France France Brazil Italy Faculty:
Bariatric Surgery. Overview of Procedural Options
 Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Results of Gastric Bypass Plus Resection of the Distal Excluded Gastric Segment in Patients With Morbid Obesity
 Results of Gastric Bypass Plus Resection of the Distal Excluded Gastric Segment in Patients With Morbid Obesity Attila Csendes, M.D., Patricio Burdiles, M.D., Karin Papapietro, M.D., Juan Carlos Diaz,
Results of Gastric Bypass Plus Resection of the Distal Excluded Gastric Segment in Patients With Morbid Obesity Attila Csendes, M.D., Patricio Burdiles, M.D., Karin Papapietro, M.D., Juan Carlos Diaz,
BRIGHAM AND WOMEN S HOSPITAL HARVARD MEDICAL SCHOOL
 BRIGHAM AND WOMEN S HOSPITAL HARVARD MEDICAL SCHOOL Bariatric Surgery Patient and Endoscopic Treatment Christopher Thompson MD, MSc, FACG, FASGE Director of Therapeutic Endoscopy Division i i of Gastroenterology
BRIGHAM AND WOMEN S HOSPITAL HARVARD MEDICAL SCHOOL Bariatric Surgery Patient and Endoscopic Treatment Christopher Thompson MD, MSc, FACG, FASGE Director of Therapeutic Endoscopy Division i i of Gastroenterology
Transoral gastric volume reduction for weight management: technique and feasibility in 18 patients
 Surgery for Obesity and Related Diseases 6 (2010) 689 694 Video original article Transoral gastric volume reduction for weight management: technique and feasibility in 18 patients Stacy A. Brethauer, M.D.
Surgery for Obesity and Related Diseases 6 (2010) 689 694 Video original article Transoral gastric volume reduction for weight management: technique and feasibility in 18 patients Stacy A. Brethauer, M.D.
Weight Loss before Hernia Repair Surgery
 Weight Loss before Hernia Repair Surgery What is an abdominal wall hernia? The abdomen (commonly called the belly) holds many of your internal organs. In the front, the abdomen is protected by a tough
Weight Loss before Hernia Repair Surgery What is an abdominal wall hernia? The abdomen (commonly called the belly) holds many of your internal organs. In the front, the abdomen is protected by a tough
O. A. Khan, K. M. Reddy Department of Upper GI Surgery, St George s Hospital, London, UK
 BARIATRIC SURGERY: A MEDICOLEGAL PERSPECTIVE O. A. Khan, K. M. Reddy Department of Upper GI Surgery, St George s Hospital, London, UK Correspondence: Omar Khan, Department of Upper GI Surgery, St George
BARIATRIC SURGERY: A MEDICOLEGAL PERSPECTIVE O. A. Khan, K. M. Reddy Department of Upper GI Surgery, St George s Hospital, London, UK Correspondence: Omar Khan, Department of Upper GI Surgery, St George
en-y Y Gastric Bypass Types of Bariatric Surgery Gastric Bypass BARIATRIC SURGERY PROCEDURES Imaging the Gastric Bypass Patient
 I have no financial disclosures Imaging the Gastric Bypass Patient Christine O. Menias, MD Associate Professor of Radiology Mallinckrodt Institute of Radiology Washington University St Louis, Missouri,
I have no financial disclosures Imaging the Gastric Bypass Patient Christine O. Menias, MD Associate Professor of Radiology Mallinckrodt Institute of Radiology Washington University St Louis, Missouri,
Case Report Successful Management of a Gastric Sleeve Leak with an Endoscopic Stent
 Case Reports in Gastrointestinal Medicine Volume 2012, Article ID 205979, 4 pages doi:10.1155/2012/205979 Case Report Successful Management of a Gastric Sleeve Leak with an Endoscopic Stent Albin Abraham,
Case Reports in Gastrointestinal Medicine Volume 2012, Article ID 205979, 4 pages doi:10.1155/2012/205979 Case Report Successful Management of a Gastric Sleeve Leak with an Endoscopic Stent Albin Abraham,
The obesity epidemic has grown in severity over the. Bariatric Surgery: A Review of Procedures and Outcomes
 GASTROENTEROLOGY 2007;132:2253 2271 Bariatric Surgery: A Review of Procedures and Outcomes KATHERINE A. ELDER and BRUCE M. WOLFE Department of Surgery, Oregon Health & Science University, Portland, Oregon
GASTROENTEROLOGY 2007;132:2253 2271 Bariatric Surgery: A Review of Procedures and Outcomes KATHERINE A. ELDER and BRUCE M. WOLFE Department of Surgery, Oregon Health & Science University, Portland, Oregon
DECISION MAKING IN BARIATRIC AND METABOLIC SURGERY Antonianum Auditorium, Roma - October 24-26, 2013
 DECISION MAKING IN BARIATRIC AND METABOLIC SURGERY Antonianum Auditorium, Roma - October 24-26, 2013 Thursday, October, 24th 8.30 REGISTRATION 09.00 IFSO Presidential Address L. Angrisani (Napoli) 09.05
DECISION MAKING IN BARIATRIC AND METABOLIC SURGERY Antonianum Auditorium, Roma - October 24-26, 2013 Thursday, October, 24th 8.30 REGISTRATION 09.00 IFSO Presidential Address L. Angrisani (Napoli) 09.05
Internal Hernia After Laparoscopic Roux-en-Y Gastric Bypass: a Correlation Between Radiological and Operative Findings
 DOI 10.1007/s11695-014-1433-5 ORIGINAL CONTRIBUTIONS Internal Hernia After Laparoscopic Roux-en-Y Gastric Bypass: a Correlation Between Radiological and Operative Findings Françis Goudsmedt & Bert Deylgat
DOI 10.1007/s11695-014-1433-5 ORIGINAL CONTRIBUTIONS Internal Hernia After Laparoscopic Roux-en-Y Gastric Bypass: a Correlation Between Radiological and Operative Findings Françis Goudsmedt & Bert Deylgat
The University of Hong Kong Department of Surgery Division of Esophageal and Upper Gastrointestinal Surgery
 Program Overview The University of Hong Kong Department of Surgery Division of Esophageal and Upper Gastrointestinal Surgery Weight Control and Metabolic Surgery Program The Weight Control and Metabolic
Program Overview The University of Hong Kong Department of Surgery Division of Esophageal and Upper Gastrointestinal Surgery Weight Control and Metabolic Surgery Program The Weight Control and Metabolic
Medical Nutrition Therapy for Upper Gastrointestinal Tract Disorders. By: Jalal Hejazi PhD, MSc.
 Medical Nutrition Therapy for Upper Gastrointestinal Tract Disorders By: Jalal Hejazi PhD, MSc. Digestive Disorders Common problem; more than 50 million outpatient visits per year Dietary habits and nutrition
Medical Nutrition Therapy for Upper Gastrointestinal Tract Disorders By: Jalal Hejazi PhD, MSc. Digestive Disorders Common problem; more than 50 million outpatient visits per year Dietary habits and nutrition
Short- and Long-Term Outcomes of Vertical Banded Gastroplasty Converted to Roux-en-Y Gastric Bypass
 DOI 10.1007/s11695-012-0796-8 CLINICAL RESEARCH Short- and Long-Term Outcomes of Vertical Banded Gastroplasty Converted to Roux-en-Y Gastric Bypass Peter Vasas & Bruno Dillemans & Sebastiaan Van Cauwenberge
DOI 10.1007/s11695-012-0796-8 CLINICAL RESEARCH Short- and Long-Term Outcomes of Vertical Banded Gastroplasty Converted to Roux-en-Y Gastric Bypass Peter Vasas & Bruno Dillemans & Sebastiaan Van Cauwenberge
The digestive system. Medicine and technology. Normal structure and function Diagnostic methods Example diseases and therapies
 The digestive system Medicine and technology Normal structure and function Diagnostic methods Example diseases and therapies The digestive system An overview (1) Oesophagus Liver (hepar) Biliary system
The digestive system Medicine and technology Normal structure and function Diagnostic methods Example diseases and therapies The digestive system An overview (1) Oesophagus Liver (hepar) Biliary system
Digestive System (continued) Digestive System. Stomach. Peptic Ulcer Disease
 Digestive System. Stomach. Peptic Ulcer Disease") Digestive System Digestive System (continued) Responsible for breaking down food, absorbing nutrients, eliminating wastes Alimentary canal Also known as gastrointestinal tract Reaches from mouth to anus
Digestive System Digestive System (continued) Responsible for breaking down food, absorbing nutrients, eliminating wastes Alimentary canal Also known as gastrointestinal tract Reaches from mouth to anus
MEDICAL COVERAGE POLICY. SERVICE: Bariatric (Weight Loss) Surgery Policy Number: 053 Effective Date: 5/27/2014 Last Review: 4/24/2014
 Surgery Policy Number: 053 Effective Date: 5/27/2014 Last Review: 4/24/2014") Page 1 of 6 MEDICAL COVERAGE POLICY Important note Even though this policy may indicate that a particular service or supply is considered covered, this conclusion is not necessarily based upon the terms
Page 1 of 6 MEDICAL COVERAGE POLICY Important note Even though this policy may indicate that a particular service or supply is considered covered, this conclusion is not necessarily based upon the terms
Case Report Gastric Adenocarcinoma after Gastric Bypass for Morbid Obesity: A Case Report and Review of the Literature
 Case Reports in Medicine Volume 2013, Article ID 609727, 4 pages http://dx.doi.org/10.1155/2013/609727 Case Report Gastric Adenocarcinoma after Gastric Bypass for Morbid Obesity: A Case Report and Review
Case Reports in Medicine Volume 2013, Article ID 609727, 4 pages http://dx.doi.org/10.1155/2013/609727 Case Report Gastric Adenocarcinoma after Gastric Bypass for Morbid Obesity: A Case Report and Review
A. Ketorolac*** B. Naproxen C. Ibuprofen D. Celecoxib
 1. A man, 66 years of age, with a history of knee osteoarthritis (OA) is experiencing increasing pain at rest and with physical activity. He also has a history of depression and coronary artery disease.
1. A man, 66 years of age, with a history of knee osteoarthritis (OA) is experiencing increasing pain at rest and with physical activity. He also has a history of depression and coronary artery disease.
The Evolution of Bariatric Surgery. History of the Development of a Successful Bariatric Program at the University of Iowa Hospitals & Clinics
 The Evolution of Bariatric Surgery History of the Development of a Successful Bariatric Program at the University of Iowa Hospitals & Clinics It s a BIG Problem & it s Getting Worse Obesity is now a disease
The Evolution of Bariatric Surgery History of the Development of a Successful Bariatric Program at the University of Iowa Hospitals & Clinics It s a BIG Problem & it s Getting Worse Obesity is now a disease
Bariatric Surgery: What the Internist Needs to Know
 Bariatric Surgery: What the Internist Needs to Know Richard Stahl, MD, FACS Assistant Professor of Surgery Medical Director of Bariatric Surgery Disclosures None (sadly) Objectives Describe several myths
Bariatric Surgery: What the Internist Needs to Know Richard Stahl, MD, FACS Assistant Professor of Surgery Medical Director of Bariatric Surgery Disclosures None (sadly) Objectives Describe several myths
NHRMC General Surgery Specialists. Minimally Invasive Gastrointestinal Surgery Phone: 910-662-9300 Fax: 910-662-9303
 Minimally Invasive Gastrointestinal Surgery Phone: 910-662-9300 Fax: 910-662-9303 W. Borden Hooks III, MD 1725 New Hanover Medical Park Drive Wilmington, NC 28403 Thank you for choosing NHRMC General Surgery
Minimally Invasive Gastrointestinal Surgery Phone: 910-662-9300 Fax: 910-662-9303 W. Borden Hooks III, MD 1725 New Hanover Medical Park Drive Wilmington, NC 28403 Thank you for choosing NHRMC General Surgery
Sleeve Gastrectomy Surgery & Follow Up Care
 Sleeve Gastrectomy Surgery & Follow Up Care Sleeve Gastrectomy Restrictive surgical weight loss procedure Able to eat a smaller amount of food to feel satiety, less than 6 ounces at a meal Surgery The
Sleeve Gastrectomy Surgery & Follow Up Care Sleeve Gastrectomy Restrictive surgical weight loss procedure Able to eat a smaller amount of food to feel satiety, less than 6 ounces at a meal Surgery The
Choices Around Bariatric Surgery
 Choices Around Bariatric Surgery What should you know? Richard Stubbs MD FRCS FRACS Wakefield Obesity Clinic, Wellington 152 kg / BMI 59 74 kg / BMI 29 Indications (NIH Consensus Statement 1991) BMI >
Choices Around Bariatric Surgery What should you know? Richard Stubbs MD FRCS FRACS Wakefield Obesity Clinic, Wellington 152 kg / BMI 59 74 kg / BMI 29 Indications (NIH Consensus Statement 1991) BMI >
Laparoscopic Sleeve Gastrectomy, 529 Cases Without a Leak: Short-Term Results and Technical Considerations
 DOI 10.1007/s11695-010-0320-y CLINICAL RESEARCH Laparoscopic Sleeve Gastrectomy, 529 Cases Without a Leak: Short-Term Results and Technical Considerations Drake Eric Bellanger & Frank L. Greenway # Springer
DOI 10.1007/s11695-010-0320-y CLINICAL RESEARCH Laparoscopic Sleeve Gastrectomy, 529 Cases Without a Leak: Short-Term Results and Technical Considerations Drake Eric Bellanger & Frank L. Greenway # Springer
Laparoscopic sleeve gastrectomy as an initial weight-loss procedure for high-risk patients with morbid obesity
 Surg Endosc (2005) xx: 1 6 DOI: 10.1007/s00464-005-0134-5 Ó Springer Science+Business Media, Inc. 2005 Laparoscopic sleeve gastrectomy as an initial weight-loss procedure for high-risk patients with morbid
Surg Endosc (2005) xx: 1 6 DOI: 10.1007/s00464-005-0134-5 Ó Springer Science+Business Media, Inc. 2005 Laparoscopic sleeve gastrectomy as an initial weight-loss procedure for high-risk patients with morbid