Attitudes of nursing staff towards involvement in medical end-of-life decisions: a national survey study
|
|
|
- Shana Cobb
- 8 years ago
- Views:
Transcription
1 Postprint Version 1.0 Journal website Pubmed link DOI /j.pec Attitudes of nursing staff towards involvement in medical end-of-life decisions: a national survey study GWENDA ALBERS A, ANNEKE L. FRANCKE B, C, D, ANKE JE DE VEER B, JOHAN BILSEN A, E, BREGJE D. ONWUTEAKA-PHILIPSEN C, D a End-of-Life Care Research Group, Ghent University & Vrije Universiteit Brussel, Brussels, Belgium b NIVEL, Netherlands Institute of Health Services Research, Utrecht c Department of Public and Occupational Health, EMGO Institute for Health and Care Research, VU University Medical Center Amsterdam d Expertise Center for Palliative Care Amsterdam, VU University Medical Center, Amsterdam, Netherlands e Department of Public Health, Vrije Universiteit Brussel, Brussels, Belgium ABSTRACT Objectives To investigate nursing staff attitudes towards involvement and role in end-of-life decisions (ELD) and the relationships with sociodemographic and work-related characteristics. Methods Survey study among nationally representative Dutch research sample consisting of care professionals. Nursing Staff working in hospitals, home care, nursing homes or homes for the elderly were sent ELD-questionnaire. Results Response: 66% (n = 587). Most respondents had been involved in ELD. Three quarters wanted to be involved in whole ELD process; 58% agreed that decisions to withhold/withdraw treatment ought to be discussed with the nurses involved; 64% believed patients would talk rather to nurses than physicians; 72% thought physicians are usually prepared to listen to nurses opinions. Hospital and highly educated nursing staff indicated relatively more often that they want to be involved in ELD. Conclusion Majority of nursing staff want to be involved in ELD. Work setting and educational level are determining factors in attitudes of nursing staff regarding involvement in ELD. Practice Implications: Awareness on the important role nurses have and want to have in ELD should be raised, and taken into account in trainings on end-of-life care for nurses and physicians and development of guidelines for communication about ELD between patients, nursing staff and physicians.

2 1. INTRODUCTION Populations in developed nations are ageing rapidly. Numbers of deaths are expected to rise each year in the coming decades, most of them due to chronic diseases such as cancer, heart disease, chronic respiratory diseases and dementia [1]. The progression of chronic diseases generally entails a period of impaired health and a protracted process of care and ultimately dying. Suffering from severe chronic illness and disability may require a period of complex decision making by patients, family, caregivers and the clinical team in the last stage of the patient's life. Medical end of life decision-making often involve weighing up the burden of implementing, withholding, continuing or withdrawing treatments, and the benefits such as improvement of the quality of life of patient and family by prevention and relief of suffering. A number of studies found that dying and death are frequently preceded by medical end-of-life decisions in different European countries [2], [3] and [4]. In a robust comparative study in six European countries, the proportion of all deaths preceded by any medical end-of-life decision (ELD) ranged from 23% in Italy to 51% in Switzerland, while in the Netherlands this percentage was 44% [4]. Decision-making at the end of life might be related to medical treatments with a definite life-shortening effect (e.g. euthanasia and physician-assisted suicide). However, this paper focuses on ELD with a possible life-shortening effect, including withholding or withdrawing a potentially life-prolonging treatment such as artificial hydration and nutrition, intensifying drug treatment to alleviate symptoms but with possible life-shortening side effects, and palliative sedation. These decisions can take place in any setting where patients die, e.g. hospitals, hospices, nursing homes, and at home. Although physicians are formally responsible for ELD, nurses are likely to be involved in the decision-making process. Nurses often have closer and more frequent contact with patients than physicians. The contact between nursing staff and patients who are severely ill or dying is often informal and personal, and patients are therefore likely to speak to nurses about their hopes, wishes and concerns. Consequently, nurses can be an important source of information for a physician who has to decide about forgoing or starting a medical treatment. Two studies performed in the Netherlands showed that nurses were involved in end-of-life decision-making by the physician in more than half of all cases [5] and [6]. The study by Van Bruchem-van de Scheur et al. indicated that there were consultations between physicians and nursing staff in 56% of the decisions about intensifying drug treatment to alleviate pain or other symptoms [6]. In the study by De Veer et al., it was found that 84% of Dutch nurses had been involved in decisions about stopping parenteral hydration and nutrition during the previous two years and 91% had been involved in decisions about intensifying drug treatment to alleviate symptoms [5]. The studies mentioned above suggest that consultation between nurses and physicians about medical ELD is quite common. However, whether physicians consult a nurse or not in case of ELD may be related to nurses own attitudes regarding their roles and desired involvement in ELD. Inghelbrecht and colleagues investigated the attitudes of nurses in Flanders (the Dutch-speaking part of Belgium) to ELD. Most nurses in Flanders indicated that they have an important role to play in

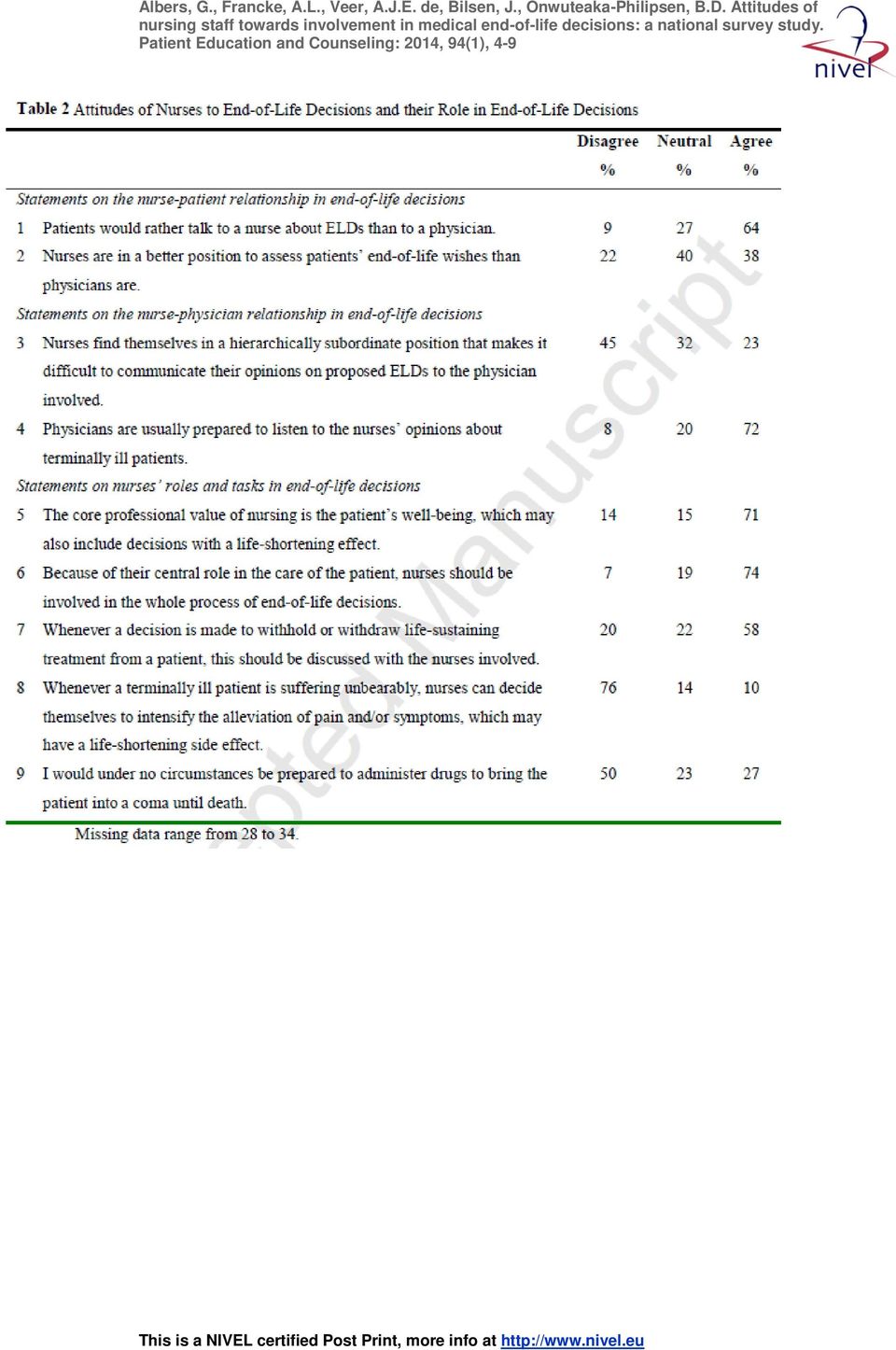
3 ELD. However, nurses work settings appeared to be related to their attitudes to their role in end-of-life decision-making [7]. To gain more insight into the attitudes of Dutch nursing staff in particular to involvement and roles in ELD as well as of the relationships between those attitudes on the one hand and sociodemographic and work-related characteristics on the other hand, we carried out the survey study described in this paper. 2. METHODS 2.1. Sample The study sample was recruited from a pre-existing nationally representative research sample of nursing staff in the Netherlands, hereinafter referred to as the Nursing Staff Panel [5], [8], [9] and [10]. This Panel consists of a permanent group of Certified Nursing Assistants (CNAs) and Registered Nurses (RNs) who are prepared to fill in questionnaires (at least twice a year) on current topics in nursing care. Compared to CNAs in most other countries, Dutch CNAs go through a rather lengthy vocational nursing training program lasting three years. Dutch RNs are educated at two different levels and comprise nursing staff at associate degree level (3 3.5 years of basic nursing education) and nursing staff at a bachelor's level (at least 4 years of basic nursing education). The Nursing Staff Panel is representative of nursing staff in the main healthcare settings in the Netherlands, i.e. hospitals, home care, nursing homes and homes for the elderly, psychiatry, and care for the mentally disabled. However, data from nursing staff working in psychiatry or in organizations for the mentally disabled were not included in the analysis for this paper, as end-oflife care is less common in these settings than in the other healthcare settings mentioned Data collection and survey questionnaire In 2011, all 903 participants of the Nursing Staff panel who worked in hospitals, home care, nursing homes and homes for the elderly were sent our survey questionnaire. A total of 587 completed the questionnaire. The questionnaire contained questions on actual experiences and attitudes regarding involvement and roles in ELD. These statements were derived from an existing survey questionnaire developed, tested and used in research in Flanders [7]. The participants were asked to what extent they agreed with each statement (strongly disagree = -2, disagree = -1, neutral = 0, agree = 1, strongly agree = 2). The nine statements fall into three main topics: the perceived position of the nurse with respect to the patient when an ELD is being considered (two statements), the perceived position of the nurse with respect to the physician when an ELD is being considered (two statements), and the perceived role of nursing staff in ELD (5 statements). The statements are listed in Table 2. We also asked some questions on background characteristics and work-related characteristics Analysis Descriptive statistics were used to describe the sociodemographic and work-related characteristics of the Nursing Staff Panel as a whole and broken down by work

4 setting. The five response categories for the statements were condensed into three: 1) agree or strongly agree, 2) neutral and 3) disagree or strongly disagree. Percentages were then presented. In order to explore if there were any sociodemographic and work-related characteristics associated with the agreement of nursing staff on the statements a backward multiple logistic regression (removal at p < 0.05) was performed and odds ratios and 95% confidence intervals were calculated. We split the response categories of the dependent variables into two, agreement (agree and strongly agree) versus the other categories (neutral, disagree and strongly disagree). The following factors were entered in the analysis: age, gender, level of education, having a belief or religion important in one's life, work setting, had been involved in some kind of ELD in the previous two years, and having had basic education or continuing education about ELD. The independent variables have been dichotomized for this analysis. Then separate logistic regression models were fitted for each statement. All analyses were performed using SPSS RESULTS 3.1. Response and characteristics of nursing staff The overall response rate was 66%, ranging from 59% in nursing homes to 74% in academic hospitals. Table 1 shows the characteristics of the study participants. The majority were female and aged over 40. Fifty-three per cent of respondents were CNAs, of whom most were working in homes for the elderly and nursing homes. Hospital nursing staff consisted mainly of RNs (99%). Fourteen per cent were working in a team or at a department specialized in palliative care. Eighty-four per cent had cared for a terminally ill patient over the last two years and 83% had been involved in some kind of ELD during the last two years. Respondents working in nursing homes and homes for the elderly were most often involved in end-of-life care and ELD. More than half of the nursing staff received basic education or continuing education about ELD, except for those working in homes for the elderly (43%). [TABLE 1. ] 3.2. Attitudes of nursing staff Table 2 shows that 64% agreed that patients would rather talk to a nurse about ELD than to a physician, and 38% agreed that nurses are in a better position to assess patients end-of-life wishes than a physician. A quarter of all nurses find themselves in a subordinate position that makes communication with the physician difficult, and 72% thought that physicians are usually prepared to listen to nurses opinions about terminally ill patients. Approximately three-quarters of the respondents believed that decisions with a life-shortening effect were part of their job (71%), and agreed that they should be involved in the whole process of ELD (74%). Fifty-eight per cent agreed that decisions to withhold or withdraw life-sustaining treatment have to be discussed with the nurses involved. Ten per cent believed that nurses should be able to decide themselves in cases of unbearable suffering to intensify the alleviation of pain and/or other symptoms, even with a possible life-shortening effect. Half of
 versus the other categories (neutral, disagree and strongly disagree).")
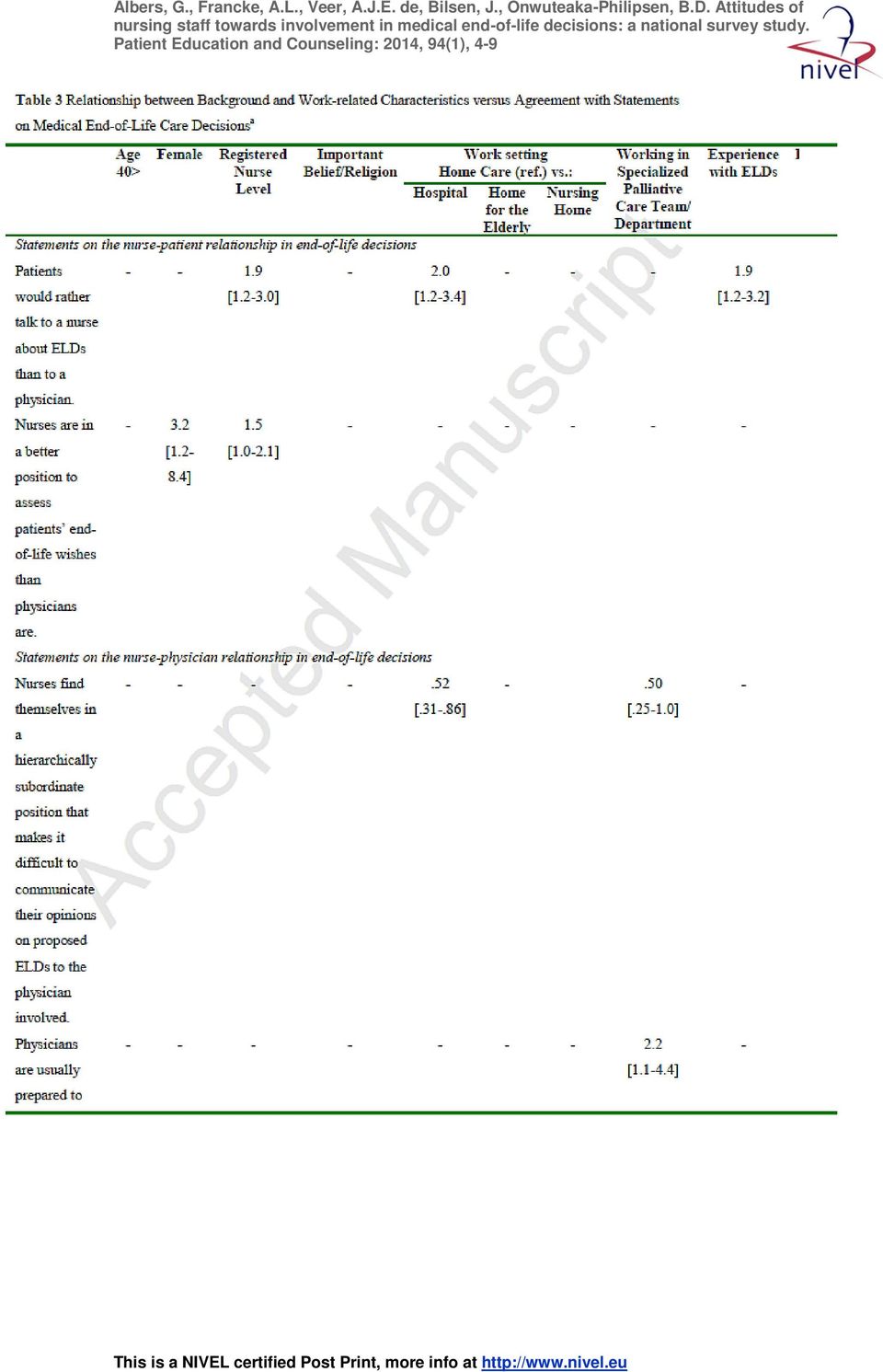
5 nursing staff members (50%) would be prepared in some cases to administer drugs to bring the patient into a coma until death. [TABLE 2.] 3.3. Factors associated with the attitudes of nursing staff Table 3 shows the determining factors in the attitudes of nursing staff regarding involvement in ELD. There were no associations found between age (40 < ) and the attitudes of nursing staff. All other variables tested were associated to nurses attitudes towards ELD on at least one statement (having experience with ELD) and at most with 5 statements (working in a hospital versus home care). In comparison to male nursing staff, female nursing staff thought more often that they were in a better position than physicians to assess patients end-of-life wishes (OR = 3,2) and that nurses should be involved in the whole ELD process (OR = 2,7), though they agreed less often that decisions with a life-shortening effect could be part of the nursing profession (OR = 0,35). Nursing staff with a life stance or religion that they considered important in their own lives agreed relatively frequently with the statement that they would never be prepared to administer drugs to bring a patient into a coma until death (OR = 1,9), and these professionals agreed less frequently with the statement that decisions with a life-shortening effect may be part of the nursing profession (OR = 0,45). [TABLE 3. ] RNs were more likely than CNAs to think that patients talk rather to them than to a physician (OR = 1,9) and that they were in a better position to assess patient's wishes compared (OR = 1,5). In addition, RNs agreed more often that decisions to withhold or withdraw life-sustaining treatment ought to be discussed with the nursing staff (OR = 2,7). The proportion of RNs who would be prepared to administer drugs to bring a patient into a coma was higher than for CNAs (OR = 1,7). Nursing staff working in hospitals were significantly more likely than home care nursing staff to think that patients rather talk to a nurse about ELD than to a physician (OR = 2,0). In addition, nursing staff in hospitals thought less often than home care staff that they find themselves in a subordinate position (OR = 0,52). In comparison with home care staff, those working in hospitals agreed more often that nurses should be involved in the whole process of end-of-life decision-making (OR = 4,2), and that decisions on withholding or withdrawing life-sustaining treatment should be discussed with the involved nursing staff (OR = 6,8). In addition, hospital nursing staff thought relatively often that nurses could decide for themselves to intensify the alleviation of pain and/or symptoms, even if this could have a lifeshortening side effect (OR = 2,4). Nursing staff working in a team or department specialized in palliative care were less likely to think that they would find themselves in a subordinate position that makes it difficult to communicate their opinions on ELD (OR = 0,50). Additionally, they believed more often that physicians are usually prepared to listen to nurses opinions (OR = 2,2).
 and at most with 5 statements (working in a hospital versus home")
6 Respondents who had basic education or continuing education about ELD (OR = 1,9), and those who had been involved in medical end-of-life decisions (OR = 1,6) in the last two years agreed more often that patients would rather talk to nurses than to physicians about ELD. Those who had education or continuing education about ELD were also more likely to think that physicians are usually willing to listen to them (OR = 1,9). 4. DISCUSSION AND CONCLUSION 4.1. Discussion The opinion of the majority of nursing staff is that they should be involved in the process of end-of-life decision-making. In addition, most nurses think that patients would rather talk to them about ELD than to physicians. This is possibly a consequence of the frequent and close contacts that nurses have with patients. Accordingly, nurses also believe that physicians are prepared to listen to their opinions, which is an important point given that nurses can be an important source of information about patients wishes. In comparison with home care staff, hospital nursing staff agreed significantly more that they should be involved in the whole process of end-of-life decision-making. In addition, RNs also agreed more often than CNAs with the statement that they ought to be involved in this process. The way in which ELDs are made might explain why hospital nursing staff indicate that they want to be involved in ELD more often than home care staff do. Nursing staff in hospitals work relatively closely with medical specialists and may have more interdisciplinary team meetings to discuss ELD, whereas home care nurses often work separately from general practitioners. The more frequent contacts between physicians and nursing staff working in a hospital might also explain why respondents working in hospitals were less likely to find themselves in a subordinate position that hinders communication with the physician than home care staff were. However, allowance should be made for the fact that the large majority of hospital nursing staff are RNs whereas half of all home care staff are CNAs. The finding that hospital nursing staff more often than home care nurses agreed with the statement nurses could decide for themselves to intensify the alleviation of pain and/or symptoms, even if this could have a life shortening side effect might be explained by the difference in educational level of nursing staff working in a hospital and those working in a home care setting. RNs working in a hospital setting may possibly be more competent and self-confident than home care nursing staff (often CNAs) to choose whether or not to give or intensify medication. Moreover, we also found that RNs agreed more often than CNAs that patients would rather talk to them than to a physician. Furthermore, respondents who had received (continuing or basic) education about ELD agreed more often that patients would rather talk to them than to a physician. In addition, nursing staff working at a specialized palliative care unit or in a team specialized in palliative care were less likely to think that nurses find themselves in a hierarchically subordinate position, and were more likely to think that physicians are prepared to listen to nurses. Remarkably, age and level of
. 4. DISCUSSION AND CONCLUSION 4.1. Discussion The opinion of the majority of nursing staff is that they should be involved in the process of end-of-life decision-making.")
7 education were not related to how nursing staff perceived physicians willingness to listen to nurses opinions about terminally ill patients. A previous study in Flanders also found that nurses are in general positive about their own potential involvement in ELD [7]. The Netherlands and Flanders have both high standards of palliative care and a liberal policy regarding medical ELD. However, there are some cultural differences: compared to the Flemish, the Dutch known for their more blunt communication style and the flatter hierarchical setups. The Netherlands also has a strong tradition of direct and open communication and a culture within which anything can be discussed, even death and dying [11]. This might explain why, in comparison to Dutch nurses, Flemish nurses found themselves in hierarchically subordinate positions more often (35% vs. 23%) and disagreed more often with the statement that physicians are willing to listen to nurses opinions (21% vs. 8%). An important strength of this study is that respondents were recruited from the large and nationally representative Nursing Staff Panel. We were therefore able to provide insights into how nurses working in hospitals, home care and residential elderly care settings in the Netherlands consider their role and involvement in ELD. Another strength is the relatively high response rate; this might be due to the fact that all participants in the Nursing Staff Panel are in principle willing to complete survey questionnaires regularly. However, using the existing Nursing Staff Panel has also a disadvantage in the sense that nursing staff who are highly committed and dedicated to the nursing profession will probably be over-represented in our study sample. Additionally, there is a limitation in that most questions and statements in the current study were about attitudes to involvement in ELD in general. Future research should therefore focus more on nurses attitudes to specific types of ELD and on nurses actual involvement in ELD. 5. CONCLUSION The majority of nursing staff working in hospitals, home care or residential elderly care would like to be involved in ELD. Work setting and level of nursing education were found to be strong determinants of nurses attitudes to their involvement in ELD. Through the frequent and intense contact nursing staff have with patients and their close relatives nursing staff can function as an important source of information and can provide physicians with relevant information regarding patient's situation and wishes at the end of life. However, hierarchically subordinate positions make it difficult for nursing staff to communicate their opinions on proposed end-of-life decisions to the physician involved. It is interesting to note that nursing staff in specialized palliative care settings or teams were less likely to think that nurses find themselves in a hierarchically subordinate position and were more likely to think that physicians are prepared to listen to nurses. The multidisciplinary nature of specialized palliative care, implying close collaboration and communication between doctors and nursing staff, may explain this finding and may also act as an example for general care settings and care providers.

8 5.1. Practice implications We recommend that the awareness on the important role nurses have and would like to have in ELD with a potential or definite life-shortening effect should be raised, and taken into account in trainings on end-of-life care for nurses and physicians. We also recommend the involvement of nursing staff in the development of multidisciplinary guidelines or standards on ELD in order to improve communication about ELD between patients, nursing staff and physicians. FUNDING The study was funded by the Dutch Ministry of Health. CONFLICTS OF INTEREST The authors have declared no conflicts of interest. REFERENCES [1] Hall S, Petkova P, Tsouros AD, Costantini M, Higginson IJ. Palliative care for older people: better practices; 2011 in press. [2] Deliens L, Mortier F, Bilsen J, Cosyns M, Vander Stichele R, Vanoverloop J, Ingels K. End-of-life decisions in medical practice in Flanders, Belgium: a nationwide survey. Lancet 2000 November 25;356: [3] H. Kuhse, P. Singer, P. Baume, M. Clark, M. Rickard End-of-life decisions in Australian medical practice Med J Aust, 166 (1997), pp [4] A. van der Heide, L. Deliens, K. Faisst, T. Nilstun, M. Norup, E. Paci, G. van der Wal, P.J. van der Maas End-of-life decision-making in six European countries: descriptive study Lancet, 362 (2003), pp [5] A.J. de Veer, A.L. Francke, E.P. Poortvliet Nurses involvement in end-of-life decisions Cancer Nurs, 31 (2008), pp [6] van Bruchem-van de Scheur GA, van der Arend AJ, bu-saad HH, van Wijmen FC, Spreeuwenberg C, ter Meulen RH. Alleviation of pain and symptoms with a life-shortening intention. Nurs Ethics 2008;15: [7] E. Inghelbrecht, J. Bilsen, F. Mortier, L. Deliens Nurses attitudes towards end-of-life decisions in medical practice: a nationwide study in Flanders, Belgium Palliat Med, 23 (2009), pp [8] A.J. de Veer, A.L. Francke, R. Buijse, R.D. Friele The use of physical restraints in home care in the Netherlands J Am Geriatr Soc, 57 (2009), pp [9] A.J. de Veer, A.L. Francke Attitudes of nursing staff towards electronic patient records: a questionnaire survey Int J Nurs Stud, 47 (2010), pp [10] A.J. de Veer, M.A. Fleuren, N. Bekkema, A.L. Francke Successful implementation of new technologies in nursing care: a questionnaire survey of nurse-users BMC Med Inform Decis Mak, 11 (2011), p. 67 [11] J. Kennedy A well-considered death Uitgeverij Bert Bakker, Amsterdam (2002)

9 TABLES

10
11
Changes in medical end-of-life practices during the legalization process of euthanasia in Belgium
 ARTICLE IN PRESS Social Science & Medicine ] (]]]]) ]]] ]]] Short report Changes in medical end-of-life practices during the legalization process of euthanasia in Belgium Johan Bilsen a,d,, Robert Vander
ARTICLE IN PRESS Social Science & Medicine ] (]]]]) ]]] ]]] Short report Changes in medical end-of-life practices during the legalization process of euthanasia in Belgium Johan Bilsen a,d,, Robert Vander
Annicka G. M. van der Plas. Kris C. Vissers. Anneke L. Francke. Gé A. Donker. Wim J. J. Jansen. Luc Deliens. Bregje D. Onwuteaka-Philipsen
 CHAPTER 8. INVOLVEMENT OF A CASE MANAGER IN PALLIATIVE CARE REDUCES HOSPITALISATIONS AT THE END OF LIFE IN CANCER PATIENTS; A MORTALITY FOLLOW-BACK STUDY IN PRIMARY CARE. Annicka G. M. van der Plas Kris
CHAPTER 8. INVOLVEMENT OF A CASE MANAGER IN PALLIATIVE CARE REDUCES HOSPITALISATIONS AT THE END OF LIFE IN CANCER PATIENTS; A MORTALITY FOLLOW-BACK STUDY IN PRIMARY CARE. Annicka G. M. van der Plas Kris
Care provision in primary palliative care case management; association with organisational and with patient characteristics.
 Care provision in primary palliative care case management; association with organisational and with patient characteristics. Annicka van der Plas EMGO+ Institute for health and care research, Quality of
Care provision in primary palliative care case management; association with organisational and with patient characteristics. Annicka van der Plas EMGO+ Institute for health and care research, Quality of
End of Life Care in Dutch Nursing Homes: Dying with Dignity?
 EAPC Trondheim session End of life care and quality of death End of Life Care in Dutch Nursing Homes: Dying with Dignity? Prof dr Luc Deliens 1/2 Professor of Public Health and Palliative Care 1. Palliative
EAPC Trondheim session End of life care and quality of death End of Life Care in Dutch Nursing Homes: Dying with Dignity? Prof dr Luc Deliens 1/2 Professor of Public Health and Palliative Care 1. Palliative
Training needs of nurses and social workers in the end-of-life care for people with intellectual disabilities: A national survey
 Postprint Version Journal website Pubmed link DOI 1.0 http://www.nurseeducationtoday.com/article/s0260-6917(13)00269-4/abstract http://www.ncbi.nlm.nih.gov/pubmed/23972684 10.1016/j.nedt.2013.07.018 Training
Postprint Version Journal website Pubmed link DOI 1.0 http://www.nurseeducationtoday.com/article/s0260-6917(13)00269-4/abstract http://www.ncbi.nlm.nih.gov/pubmed/23972684 10.1016/j.nedt.2013.07.018 Training
Attitudes of nursing staff towards electronic patient records: A questionnaire survey
 Postprint 1.0 Version Journal website http://dx.doi.org/10.1016/j.ijnurstu.2009.11.016 Pubmed link http://www.ncbi.nlm.nih.gov/pubmed/20022007 DOI 10.1016/j.ijnurstu.2009.11.016 Attitudes of nursing staff
Postprint 1.0 Version Journal website http://dx.doi.org/10.1016/j.ijnurstu.2009.11.016 Pubmed link http://www.ncbi.nlm.nih.gov/pubmed/20022007 DOI 10.1016/j.ijnurstu.2009.11.016 Attitudes of nursing staff
Specialist training programme for elderly care physicians (previously: nursing home physicians) in the Netherlands
 in the Netherlands") Specialist training programme for elderly care physicians (previously: nursing home physicians) in the Netherlands For its population of 16.5 million inhabitants, the Netherlands has approximately 350
Specialist training programme for elderly care physicians (previously: nursing home physicians) in the Netherlands For its population of 16.5 million inhabitants, the Netherlands has approximately 350
TEXAS MEDICAL POWER OF ATTORNEY
 TEXAS MEDICAL POWER OF ATTORNEY NAME DATE BHS 80000246 v1 11/13 baptisthealthsystem.com That s Baptist Care. Page 1 of 5 INFORMATION CONCERNING THE MEDICAL POWER OF ATTORNEY THIS IS AN IMPORTANT LEGAL
TEXAS MEDICAL POWER OF ATTORNEY NAME DATE BHS 80000246 v1 11/13 baptisthealthsystem.com That s Baptist Care. Page 1 of 5 INFORMATION CONCERNING THE MEDICAL POWER OF ATTORNEY THIS IS AN IMPORTANT LEGAL
Opinions of health care professionals and the public after eight years of euthanasia legislation in the Netherlands: A mixed methods Approach
 Postprint 1.0 Version Journal website http://pmj.sagepub.com/content/27/3/273.long Pubmed link http://www.ncbi.nlm.nih.gov/pubmed/22695742 DOI 10.1177/0269216312448507 Opinions of health care professionals
Postprint 1.0 Version Journal website http://pmj.sagepub.com/content/27/3/273.long Pubmed link http://www.ncbi.nlm.nih.gov/pubmed/22695742 DOI 10.1177/0269216312448507 Opinions of health care professionals
Abstract. Background. Objectives. Methods
 RESEARCH ARTICLE Involvement of a Case Manager in Palliative Care Reduces Hospitalisations at the End of Life in Cancer Patients; A Mortality Follow- Back Study in Primary Care Annicka G. M. van der Plas
RESEARCH ARTICLE Involvement of a Case Manager in Palliative Care Reduces Hospitalisations at the End of Life in Cancer Patients; A Mortality Follow- Back Study in Primary Care Annicka G. M. van der Plas
How To Write A Values History Form
 VALUES HISTORY A form to assist you in making health care choices in accordance with your values It is important that your medical treatment be your choice. The purpose of this form is to assist you in
VALUES HISTORY A form to assist you in making health care choices in accordance with your values It is important that your medical treatment be your choice. The purpose of this form is to assist you in
KENTUCKY Living Will Directive Planning for Important Health Care Decisions
 KENTUCKY Living Will Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of the National
KENTUCKY Living Will Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of the National
end-of-life decisions Honoring the wishes of a person with Alzheimer's disease
 end-of-life decisions Honoring the wishes of a person with Alzheimer's disease Preparing for the end of life When a person with late-stage Alzheimer s a degenerative brain disease nears the end of life
end-of-life decisions Honoring the wishes of a person with Alzheimer's disease Preparing for the end of life When a person with late-stage Alzheimer s a degenerative brain disease nears the end of life
You know them well They know you well You trust them to do what you desire And, you trust them to do what is best for you.
 Advanced Directive Act of Texas Part III Medical Power of Attorney and Content of a DNR By James L. Holly, MD Your Life Your Health The Examiner April 21, 2005 There are many decisions which are made in
Advanced Directive Act of Texas Part III Medical Power of Attorney and Content of a DNR By James L. Holly, MD Your Life Your Health The Examiner April 21, 2005 There are many decisions which are made in
A CATHOLIC ADVANCE DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES
 A CATHOLIC ADVANCE DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES THIS IS AN IMPORTANT LEGAL DOCUMENT KNOWN AS AN ADVANCE DIRECTIVE. ITS PURPOSE IS TO COMMUNICATE YOUR WISHES REGARDING LIFE-SUSTAINING
A CATHOLIC ADVANCE DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES THIS IS AN IMPORTANT LEGAL DOCUMENT KNOWN AS AN ADVANCE DIRECTIVE. ITS PURPOSE IS TO COMMUNICATE YOUR WISHES REGARDING LIFE-SUSTAINING
OHIO DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Ohio Revised Code 1337.11 to 1337.17)
") OHIO DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Ohio Revised Code 1337.11 to 1337.17) The following Notice to Adult Executing This Document (Durable Power of Attorney for Health Care) is required by Ohio
OHIO DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Ohio Revised Code 1337.11 to 1337.17) The following Notice to Adult Executing This Document (Durable Power of Attorney for Health Care) is required by Ohio
Palliative care for terminally ill. patients in the Netherlands. Dutch Government Policy
 Palliative care for terminally ill patients in the Netherlands Dutch Government Policy International Publication Series Health, Welfare and Sport No 16 Ministerie van Volksgezondheid, Welzijn en Sport
Palliative care for terminally ill patients in the Netherlands Dutch Government Policy International Publication Series Health, Welfare and Sport No 16 Ministerie van Volksgezondheid, Welzijn en Sport
What services are provided by JSSA Hospice? Our personalized services for patients and family members include:
 FAQ S ABOUT HOSPICE What is Hospice? Hospice is a specialized type of healthcare for patients and families who are faced with a terminal illness. A team of physicians, nurses, social workers, bereavement
FAQ S ABOUT HOSPICE What is Hospice? Hospice is a specialized type of healthcare for patients and families who are faced with a terminal illness. A team of physicians, nurses, social workers, bereavement
KENTUCKY Living Will Directive Planning for Important Health Care Decisions
 KENTUCKY Living Will Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of the National
KENTUCKY Living Will Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of the National
Palliative Care Services. Consultant Teams in Hospitals. Adult/Children 4 84 50 NK NK 138 Paediatric only 0 4 4 2 0 10
 NETHERLANDS Population: 16,407,491 Current Directory: Printed version Online version None identified x Key Contact/National Association Key contact: Marijke Wulp, Staff member, Agora, National Information
NETHERLANDS Population: 16,407,491 Current Directory: Printed version Online version None identified x Key Contact/National Association Key contact: Marijke Wulp, Staff member, Agora, National Information
NEW YORK Advance Directive Planning for Important Healthcare Decisions
 NEW YORK Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of
NEW YORK Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of
CHAPTER 3. PALLIATIVE CARE CASE MANAGEMENT IN PRIMARY CARE SETTINGS: A NATIONWIDE SURVEY.
 CHAPTER 3. PALLIATIVE CARE CASE MANAGEMENT IN PRIMARY CARE SETTINGS: A NATIONWIDE SURVEY. 33 Annicka G.M. van der Plas Luc Deliens Marlies van de Watering Wim J.J. Jansen Kris C. Vissers Bregje D. Onwuteaka-Philipsen
CHAPTER 3. PALLIATIVE CARE CASE MANAGEMENT IN PRIMARY CARE SETTINGS: A NATIONWIDE SURVEY. 33 Annicka G.M. van der Plas Luc Deliens Marlies van de Watering Wim J.J. Jansen Kris C. Vissers Bregje D. Onwuteaka-Philipsen
Engaging Spirituality in Social Work for Palliative Care and Hospice
 Engaging Spirituality in Social Work for Palliative Care and Hospice Conversations about Comfort, Support, and Quality of Life written by Palliative Care Consulting Team and Hwi-Ja Canda Lawrence Memorial
Engaging Spirituality in Social Work for Palliative Care and Hospice Conversations about Comfort, Support, and Quality of Life written by Palliative Care Consulting Team and Hwi-Ja Canda Lawrence Memorial
Advance Care Planning
 Advance Care Planning Planning for the future Having an Advance Care Plan for health care is a smart thing to do. Like all planning for the future, it involves thinking ahead. Most of us make plans for
Advance Care Planning Planning for the future Having an Advance Care Plan for health care is a smart thing to do. Like all planning for the future, it involves thinking ahead. Most of us make plans for
Palliative Care Nursing
 Palliative Care Nursing A ccording to the most recent National Vital Statistics Reports, 2,436,652 deaths occurred in 2009, of which 568,688 were due to cancer, second only to heart disease. 1 In 2009,
Palliative Care Nursing A ccording to the most recent National Vital Statistics Reports, 2,436,652 deaths occurred in 2009, of which 568,688 were due to cancer, second only to heart disease. 1 In 2009,
Advance Directives for Health Care
 Advance Directives for Health Care & Mental Health Care for ADVANCE HEALTH CARE DIRECTIVE EXPLANATION You have the right to give instructions about your own health care to the extent allowed by law. You
Advance Directives for Health Care & Mental Health Care for ADVANCE HEALTH CARE DIRECTIVE EXPLANATION You have the right to give instructions about your own health care to the extent allowed by law. You
MULTIDISCIPLINARY COMPETENCIES IN THE CARE OF OLDER ADULTS AT THE COMPLETION OF THE ENTRY-
 ENTRY- LEVEL HEALTH PROFESSIONAL DEGREE Developed by the Partnership for Health in Aging Workgroup on Multidisciplinary Competencies in Geriatrics With Support from the American Geriatrics Society (AGS)
ENTRY- LEVEL HEALTH PROFESSIONAL DEGREE Developed by the Partnership for Health in Aging Workgroup on Multidisciplinary Competencies in Geriatrics With Support from the American Geriatrics Society (AGS)
ADVANCE HEALTH CARE DIRECTIVE (Under Authority of California Probate Code Sections 4670 et seq.)
") ADVANCE HEALTH CARE DIRECTIVE (Under Authority of California Probate Code Sections 4670 et seq.) CATHOLIC TEACHING CONCERNING EUTHANASIA Death Is A Normal Part of the Human Condition. Death is neither
ADVANCE HEALTH CARE DIRECTIVE (Under Authority of California Probate Code Sections 4670 et seq.) CATHOLIC TEACHING CONCERNING EUTHANASIA Death Is A Normal Part of the Human Condition. Death is neither
NEW YORK Advance Directive Planning for Important Healthcare Decisions
 NEW YORK Advance Directive Planning for Important Healthcare Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
NEW YORK Advance Directive Planning for Important Healthcare Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
Treatment-Resistant Major Depressive Disorder and Assisted Dying
 Treatment-Resistant Major Depressive Disorder and Assisted Dying Udo Schuklenk, PhD Tweet me, I ll tweet ya back @schuklenk Suzanne van de Vathorst, MD PhD Erasmus University, Netherlands Conflict of interest
Treatment-Resistant Major Depressive Disorder and Assisted Dying Udo Schuklenk, PhD Tweet me, I ll tweet ya back @schuklenk Suzanne van de Vathorst, MD PhD Erasmus University, Netherlands Conflict of interest
Human Services. The Master's Degree. Professional Development Sequence in Gerontology (blended format)
") University of Illinois Springfield 1 Human Master of Arts Joint Graduate Degree HMS/MPH Graduate Certificate 1 www.uis.edu/humanservices/ Email: hms@uis.edu Office Phone: (217) 206-6687 Office Location:
University of Illinois Springfield 1 Human Master of Arts Joint Graduate Degree HMS/MPH Graduate Certificate 1 www.uis.edu/humanservices/ Email: hms@uis.edu Office Phone: (217) 206-6687 Office Location:
The JOURNEY OF ELDERCARE
 The JOURNEY OF ELDERCARE ELDERSPEAK Glossary Terms commonly used by Professionals in Aging Acute v. Chronic Acute - care delivered in a hospital that is usually shortterm and recuperative. Chronic - condition
The JOURNEY OF ELDERCARE ELDERSPEAK Glossary Terms commonly used by Professionals in Aging Acute v. Chronic Acute - care delivered in a hospital that is usually shortterm and recuperative. Chronic - condition
Ohio s Do-Not-Resuscitate Law
 Ohio s Do-Not-Resuscitate Law Copied from Choices: Living Well at the End of Life developed in collaboration with the Ohio Hospice and Palliative Care Organization, the Ohio State Medical Association,
Ohio s Do-Not-Resuscitate Law Copied from Choices: Living Well at the End of Life developed in collaboration with the Ohio Hospice and Palliative Care Organization, the Ohio State Medical Association,
A Catholic Guide to Health Care Directives. & Indiana Catholic Health Care Directive
 A Catholic Guide to Health Care Directives A Resource for Indiana Catholics that includes end of life care & Indiana Catholic Health Care Directive A Supplement Published as a pastoral service by the Indiana
A Catholic Guide to Health Care Directives A Resource for Indiana Catholics that includes end of life care & Indiana Catholic Health Care Directive A Supplement Published as a pastoral service by the Indiana
NEW HAMPSHIRE Advance Directive Planning for Important Health Care Decisions
 NEW HAMPSHIRE Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National
NEW HAMPSHIRE Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National
OTTAWA 1800-160 Elgin St. Tel: (613) 230-2200 Ottawa, Ontario, Canada Fax: (613) 230-3793 K2P 2P7
 230-2200 Ottawa, Ontario, Canada Fax: (613) 230-3793 K2P 2P7") What Canadians Say: The Way Forward Survey Report December 2013 Proprietary Warning The information contained herein is proprietary to the Canadian Hospice Palliative Care Association (CHPCA) and may not
What Canadians Say: The Way Forward Survey Report December 2013 Proprietary Warning The information contained herein is proprietary to the Canadian Hospice Palliative Care Association (CHPCA) and may not
Hospice Care It s About How You Live
 Hospice Care It s About How You Live Beth Mahar, Director of Member Services Hospice & Palliative Care Association of NYS Thank you to: Elizabeth Peters RN The Community Hospice of Columbia/Greene Mission
Hospice Care It s About How You Live Beth Mahar, Director of Member Services Hospice & Palliative Care Association of NYS Thank you to: Elizabeth Peters RN The Community Hospice of Columbia/Greene Mission
GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE
 GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE Revised April 2012 Purpose: In recognizing the right of individuals to (1) control all aspects of his or her personal care and medical treatment, (2) insist upon
GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE Revised April 2012 Purpose: In recognizing the right of individuals to (1) control all aspects of his or her personal care and medical treatment, (2) insist upon
GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE
 Purpose: GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE In recognizing the right of individuals to (1) control all aspects of his or her personal care and medical treatment, (2) insist upon medical treatment,
Purpose: GEORGIA ADVANCE DIRECTIVE FOR HEALTH CARE In recognizing the right of individuals to (1) control all aspects of his or her personal care and medical treatment, (2) insist upon medical treatment,
The La Crosse Region Power of Attorney for Healthcare Document and The Instructions for Completing this Document
 Overview The La Crosse Region Power of Attorney for Healthcare Document and The Instructions for Completing this Document The attached power of attorney for healthcare form is a legal document, developed
Overview The La Crosse Region Power of Attorney for Healthcare Document and The Instructions for Completing this Document The attached power of attorney for healthcare form is a legal document, developed
ILLINOIS Advance Directive Planning for Important Health Care Decisions
 ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
PART 1 ALASKA DURABLE POWER OF ATTORNEY FOR HEALTH CARE DECISIONS (1) DESIGNATION OF AGENT.
 DESIGNATION OF AGENT.") Page1 PART 1 ALASKA DURABLE POWER OF ATTORNEY FOR HEALTH CARE DECISIONS (1) DESIGNATION OF AGENT. I designate the following individual as my agent to make health care decisions for me: Name Phone: Home
Page1 PART 1 ALASKA DURABLE POWER OF ATTORNEY FOR HEALTH CARE DECISIONS (1) DESIGNATION OF AGENT. I designate the following individual as my agent to make health care decisions for me: Name Phone: Home
Seeking consent: working with older people
 Seeking consent: working with older people Contents Page Introduction 1 Seeking consent: people with capacity 3 When adults lack capacity 9 Research 13 Withdrawing and withholding life-prolonging treatment
Seeking consent: working with older people Contents Page Introduction 1 Seeking consent: people with capacity 3 When adults lack capacity 9 Research 13 Withdrawing and withholding life-prolonging treatment
ADVANCE HEALTH CARE DIRECTIVES Under Hawai i Law
 ADVANCE HEALTH CARE DIRECTIVES Under Hawai i Law Checklist How to Start and What to Do Information about Advance Health Care Directives Sample Advance Directive Forms Including: Individual Instructions
ADVANCE HEALTH CARE DIRECTIVES Under Hawai i Law Checklist How to Start and What to Do Information about Advance Health Care Directives Sample Advance Directive Forms Including: Individual Instructions
Survey of Nurses. End of life care
 Survey of Nurses 28 End of life care HELPING THE NATION SPEND WISELY The National Audit Office scrutinises public spending on behalf of Parliament. The Comptroller and Auditor General, Tim Burr, is an
Survey of Nurses 28 End of life care HELPING THE NATION SPEND WISELY The National Audit Office scrutinises public spending on behalf of Parliament. The Comptroller and Auditor General, Tim Burr, is an
Multidisciplinary hospital palliative care team (in-patient, outpatient) José, Josien, Jolanda, Patricia, Joep Sake, Gert-Jan, Jacques, Caro
 José, Josien, Jolanda, Patricia, Joep Sake, Gert-Jan, Jacques, Caro") Euthanasia and physician assisted suicide in the Netherlands Joep Douma, medical oncologist / palliative care services Rijnstate Hospital Arnhem The Netherlands 1 The context of euthanasia and physician
Euthanasia and physician assisted suicide in the Netherlands Joep Douma, medical oncologist / palliative care services Rijnstate Hospital Arnhem The Netherlands 1 The context of euthanasia and physician
Creative Commons Image courtesy of mmmswan on Flickr. Palliative Care: Theories, Principles, and Innovations for Case Management
 Creative Commons Image courtesy of mmmswan on Flickr Palliative Care: Theories, Principles, and Innovations for Case Management OBJECTIVES: Define what Palliative care means. Describe the principles of
Creative Commons Image courtesy of mmmswan on Flickr Palliative Care: Theories, Principles, and Innovations for Case Management OBJECTIVES: Define what Palliative care means. Describe the principles of
404.800. Sections 404.800 to 404.865 may be cited as the "Durable Power of Attorney for Health Care Act".
 MISSOURI STATE STATUTES 404.800. Sections 404.800 to 404.865 may be cited as the "Durable Power of Attorney for Health Care Act". 404.805. 1. As used in sections 404.800 to 404.865, the following terms
MISSOURI STATE STATUTES 404.800. Sections 404.800 to 404.865 may be cited as the "Durable Power of Attorney for Health Care Act". 404.805. 1. As used in sections 404.800 to 404.865, the following terms
Combined Living Will & Health Care Power of Attorney PART I
 Combined Living Will & Health Care Power of Attorney Example Form from Pennsylvania Act 169 of 2006 PART I Introductory Remarks on Health Care Decision Making You have the right to decide the type of health
Combined Living Will & Health Care Power of Attorney Example Form from Pennsylvania Act 169 of 2006 PART I Introductory Remarks on Health Care Decision Making You have the right to decide the type of health
Advance Health Care Directive
 Advance Health Care Directive of This form was developed by the Committee on Law and the Elderly of the Delaware Bar Association and approved for use by the Office of the Attorney General of the State
Advance Health Care Directive of This form was developed by the Committee on Law and the Elderly of the Delaware Bar Association and approved for use by the Office of the Attorney General of the State
Advance Health Care Directive Instructions
 Advance Health Care Directive Instructions 1) Review the form completely before filling in any section. 2) If possible, name a first agent AND at least one alternative agent (in case something happens
Advance Health Care Directive Instructions 1) Review the form completely before filling in any section. 2) If possible, name a first agent AND at least one alternative agent (in case something happens
Recommended Geropsychiatric Competency Enhancements for Nurse Practitioners Who Provide Care to Older Adults but are not Geriatric Specialists
 Recommended Geropsychiatric Competency Enhancements for Nurse Practitioners Who Provide Care to Older Adults but are not Geriatric Specialists These recommended competency enhancement statements are not
Recommended Geropsychiatric Competency Enhancements for Nurse Practitioners Who Provide Care to Older Adults but are not Geriatric Specialists These recommended competency enhancement statements are not
HAWAI I ADVANCE HEALTH CARE DIRECTIVE
 HAWAI I ADVANCE HEALTH CARE DIRECTIVE My name is: Last First Middle initial Date of Birth Date PART 1: HEALTH CARE POWER OF ATTORNEY DESIGNATION OF AGENT: I designate the following individual as my agent
HAWAI I ADVANCE HEALTH CARE DIRECTIVE My name is: Last First Middle initial Date of Birth Date PART 1: HEALTH CARE POWER OF ATTORNEY DESIGNATION OF AGENT: I designate the following individual as my agent
TEXAS Advance Directive Planning for Important Health Care Decisions
 TEXAS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National (NHPCO),
TEXAS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National (NHPCO),
EUROPEAN CITIZENS DIGITAL HEALTH LITERACY
 Flash Eurobarometer EUROPEAN CITIZENS DIGITAL HEALTH LITERACY REPORT Fieldwork: September 2014 Publication: November 2014 This survey has been requested by the European Commission, Directorate-General
Flash Eurobarometer EUROPEAN CITIZENS DIGITAL HEALTH LITERACY REPORT Fieldwork: September 2014 Publication: November 2014 This survey has been requested by the European Commission, Directorate-General
Administration of Emergency Medicine
 doi:10.1016/j.jemermed.2005.07.008 The Journal of Emergency Medicine, Vol. 30, No. 4, pp. 455 460, 2006 Copyright 2006 Elsevier Inc. Printed in the USA. All rights reserved 0736-4679/06 $ see front matter
doi:10.1016/j.jemermed.2005.07.008 The Journal of Emergency Medicine, Vol. 30, No. 4, pp. 455 460, 2006 Copyright 2006 Elsevier Inc. Printed in the USA. All rights reserved 0736-4679/06 $ see front matter
Health Literacy and Palliative Care Nursing Perspective
 Health Literacy and Palliative Care Nursing Perspective Ginger Marshall, MSN, ACNP-BC, ACHPN, FPCN President Elect, Hospice Palliative Nurses Association National Director of Palliative Care for Compassus
Health Literacy and Palliative Care Nursing Perspective Ginger Marshall, MSN, ACNP-BC, ACHPN, FPCN President Elect, Hospice Palliative Nurses Association National Director of Palliative Care for Compassus
END OF LIFE CARE AND DECISION MAKING
 END OF LIFE CARE AND DECISION MAKING Opinions and experiences of the general public, bereaved relatives, and professionals Natasja Johanna Helena Raijmakers END OF LIFE CARE AND DECISION MAKING Opinions
END OF LIFE CARE AND DECISION MAKING Opinions and experiences of the general public, bereaved relatives, and professionals Natasja Johanna Helena Raijmakers END OF LIFE CARE AND DECISION MAKING Opinions
Palliative Care Certification Requirements
 Palliative Care Certification Requirements Provision of Care, Treatment, and Services PCPC.1 1 Patients know how to access and use the program s care, treatment, and services. 2 3 Patients and families
Palliative Care Certification Requirements Provision of Care, Treatment, and Services PCPC.1 1 Patients know how to access and use the program s care, treatment, and services. 2 3 Patients and families
Quality End of Life Care: A Team Approach
 Quality End of Life Care: A Team Approach Presented by Dann Baker, MDiv Director Pastoral Care & Ethics, JPS Health Network; Adjunct Assistant Professor, UNTHSC-TCOM Janet Lieto, DO, FACOFP Assistant Professor
Quality End of Life Care: A Team Approach Presented by Dann Baker, MDiv Director Pastoral Care & Ethics, JPS Health Network; Adjunct Assistant Professor, UNTHSC-TCOM Janet Lieto, DO, FACOFP Assistant Professor
ADVANCE DIRECTIVES. A Guide to Maryland Law. Health Care Decisions. (Forms Included) State of Maryland. Office of the Attorney General
 State of Maryland. Office of the Attorney General") ADVANCE DIRECTIVES A Guide to Maryland Law on Health Care Decisions (Forms Included) State of Maryland Office of the Attorney General J. Joseph Curran, Jr. Attorney General Dear Fellow Marylander: I am
ADVANCE DIRECTIVES A Guide to Maryland Law on Health Care Decisions (Forms Included) State of Maryland Office of the Attorney General J. Joseph Curran, Jr. Attorney General Dear Fellow Marylander: I am
Continuing Professional Development for Registered and Enrolled Nurses
 Continuing Professional Development for Registered and Enrolled Nurses Contents Introduction: Aged Care Learning Solutions CPD Solution 0-04 Learning Plans and Catalogue CPD Solution Resources Learning
Continuing Professional Development for Registered and Enrolled Nurses Contents Introduction: Aged Care Learning Solutions CPD Solution 0-04 Learning Plans and Catalogue CPD Solution Resources Learning
Deciding About. Health Care A GUIDE FOR PATIENTS AND FAMILIES. New York State Department of Health
 Deciding About Health Care A GUIDE FOR PATIENTS AND FAMILIES New York State Department of Health 1 A GUIDE FOR PATIENTS AND FAMILIES Introduction Who should read this guide? This guide is for New York
Deciding About Health Care A GUIDE FOR PATIENTS AND FAMILIES New York State Department of Health 1 A GUIDE FOR PATIENTS AND FAMILIES Introduction Who should read this guide? This guide is for New York
Advance Directives/ Decisions
 Advance Directives/ Decisions Promoting end-of-life choices Introduction There are many different templates available for what were previously known as Living Wills and are now called Advance Directives
Advance Directives/ Decisions Promoting end-of-life choices Introduction There are many different templates available for what were previously known as Living Wills and are now called Advance Directives
KENTUCKY LIVING WILL PACKET. The Office of the Attorney General Jack Conway, Attorney General
 KENTUCKY LIVING WILL PACKET The Office of the Attorney General Jack Conway, Attorney General Living Wills in Kentucky A Living Will gives you a voice in decisions about your medical care when you are unconscious
KENTUCKY LIVING WILL PACKET The Office of the Attorney General Jack Conway, Attorney General Living Wills in Kentucky A Living Will gives you a voice in decisions about your medical care when you are unconscious
Department of Anesthesiology and Critical Care Medicine Hadassah Medical Center THE ISRAELI TERMINALLY ILL LAW. Charles L.
 Department of Anesthesiology and Critical Care Medicine Hadassah Medical Center THE ISRAELI TERMINALLY ILL LAW Charles L. Sprung MD CHANGE IN DYING PROCESS 50 Years ago Person stopped breathing Died 1950s
Department of Anesthesiology and Critical Care Medicine Hadassah Medical Center THE ISRAELI TERMINALLY ILL LAW Charles L. Sprung MD CHANGE IN DYING PROCESS 50 Years ago Person stopped breathing Died 1950s
Ethics and Palliative Care Nursing. Laurie Read, MN James Read, Ph.D.
 Ethics and Palliative Care Nursing Laurie Read, MN James Read, Ph.D. 1. Terminology 2. A list of typical ethical issues in clinical palliative care 3. An ethics discussion of a case 4. Review, last questions
Ethics and Palliative Care Nursing Laurie Read, MN James Read, Ph.D. 1. Terminology 2. A list of typical ethical issues in clinical palliative care 3. An ethics discussion of a case 4. Review, last questions
Minnesota Health Care Directive
 Minnesota Health Care Directive A Health Care Directive is a written document that informs others of your wishes about your health care. It allows you to name a person ( agent ) to decide for you if you
Minnesota Health Care Directive A Health Care Directive is a written document that informs others of your wishes about your health care. It allows you to name a person ( agent ) to decide for you if you
Release: 1. HLTEN515B Implement and monitor nursing care for older clients
 Release: 1 HLTEN515B Implement and monitor nursing care for older clients HLTEN515B Implement and monitor nursing care for older clients Modification History Not Applicable Unit Descriptor Descriptor This
Release: 1 HLTEN515B Implement and monitor nursing care for older clients HLTEN515B Implement and monitor nursing care for older clients Modification History Not Applicable Unit Descriptor Descriptor This
Chapter 1: Nursing Today: A Time of Transformation Test Bank
 hapter 1: Nursing Today: Time of Transformation Test ank MULTIPLE HOIE 1. Which of the following could eventually change the historical status of nursing as a female-dominated profession? a. More men graduating
hapter 1: Nursing Today: Time of Transformation Test ank MULTIPLE HOIE 1. Which of the following could eventually change the historical status of nursing as a female-dominated profession? a. More men graduating
Making Health Care Decisions in North Dakota:
 Making Health Care Decisions in North Dakota: A Summary of North Dakota Law Regarding Health Care Directives Published by: North Dakota Department of Human Services Aging Services Division 1237 W.Divide
Making Health Care Decisions in North Dakota: A Summary of North Dakota Law Regarding Health Care Directives Published by: North Dakota Department of Human Services Aging Services Division 1237 W.Divide
Ambitions for Palliative and End of Life Care:
 Ambitions for Palliative and End of Life Care: A national framework for local action 2015-2020 National Palliative and End of Life Care Partnership Association for Palliative Medicine; Association of Ambulance
Ambitions for Palliative and End of Life Care: A national framework for local action 2015-2020 National Palliative and End of Life Care Partnership Association for Palliative Medicine; Association of Ambulance
Frequently Asked Questions about Pediatric Hospice and Pediatric Palliative Care
 Frequently Asked Questions about Pediatric Hospice and Pediatric Palliative Care Developed by the New Jersey Hospice and Palliative Care Organization Pediatric Council Items marked with an (H) discuss
Frequently Asked Questions about Pediatric Hospice and Pediatric Palliative Care Developed by the New Jersey Hospice and Palliative Care Organization Pediatric Council Items marked with an (H) discuss
HPNA Position Statement The Nurse s Role in Advance Care Planning
 HPNA Position Statement The Nurse s Role in Advance Care Planning Background Advances in medical technology have empowered healthcare providers across settings with the means to prolong life. Tied to this
HPNA Position Statement The Nurse s Role in Advance Care Planning Background Advances in medical technology have empowered healthcare providers across settings with the means to prolong life. Tied to this
INDIANA Advance Directive Planning for Important Health Care Decisions
 INDIANA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Organization
INDIANA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Organization
Put it in Writing. Questions and Answers on Advance QDirectives. www.aha.org July 1998, Revised December 2012, Item No. 166909
 Put it in Writing uestions and nswers on dvance Directives www.aha.org July 1998, Revised December 2012, Item No. 166909 ii Many people today are worried about the medical care they would receive if they
Put it in Writing uestions and nswers on dvance Directives www.aha.org July 1998, Revised December 2012, Item No. 166909 ii Many people today are worried about the medical care they would receive if they
HOSPICE AND PALLIATIVE MEDICINE FELLOWSHIP
 HOSPICE AND PALLIATIVE MEDICINE FELLOWSHIP This one-year ACGME accredited fellowship program is now offering three fellowship positions. The program consists of clinical training, a palliative care seminar
HOSPICE AND PALLIATIVE MEDICINE FELLOWSHIP This one-year ACGME accredited fellowship program is now offering three fellowship positions. The program consists of clinical training, a palliative care seminar
Curriculum Map Incorporating Recommended Competencies for Geriatric Nursing Care/ Clinical Experiences into Baccalaureate Nursing Programs
 Curriculum Map Incorporating Recommended Competencies for Geriatric Nursing Care/ Clinical Experiences into Baccalaureate Nursing Programs List Nursing Courses Topics Attitudes About Aging: Recognize one
Curriculum Map Incorporating Recommended Competencies for Geriatric Nursing Care/ Clinical Experiences into Baccalaureate Nursing Programs List Nursing Courses Topics Attitudes About Aging: Recognize one
DOWNLOAD COVERSHEET:
 DOWNLOAD COVERSHEET: This is a standard advance directive for your state, made available to you as a courtesy by Lifecare Directives, LLC. You should be aware that extensive research has demonstrated that
DOWNLOAD COVERSHEET: This is a standard advance directive for your state, made available to you as a courtesy by Lifecare Directives, LLC. You should be aware that extensive research has demonstrated that
Information for Patients. Advance Health Care Directive Kit A guide to help you express your health care wishes
 Information for Patients Advance Health Care Directive Kit A guide to help you express your health care wishes Table of contents PART I - REQUIRED Selection of a decision maker Who will make health care
Information for Patients Advance Health Care Directive Kit A guide to help you express your health care wishes Table of contents PART I - REQUIRED Selection of a decision maker Who will make health care
NEW JERSEY Advance Directive Planning for Important Health Care Decisions
 NEW JERSEY Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CARINGINFO CaringInfo, a program of the
NEW JERSEY Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CARINGINFO CaringInfo, a program of the
Maine Health Care Advance Directive Form
 Maine Health Care Advance Directive Form You may use this form now to tell your physician and others what medical care you want to receive if you become too sick in the future to tell them what you want.
Maine Health Care Advance Directive Form You may use this form now to tell your physician and others what medical care you want to receive if you become too sick in the future to tell them what you want.
Provincial Hospice Palliative Care Home Based Nurse Practitioner Program: Supporting Patients to Live with Dignity and Comfort at Home
 Provincial Hospice Palliative Care Home Based Nurse Practitioner Program: Supporting Patients to Live with Dignity and Comfort at Home Janet McMullan, RN, BScN, MN, Clinical Program Lead, OACCAC James
Provincial Hospice Palliative Care Home Based Nurse Practitioner Program: Supporting Patients to Live with Dignity and Comfort at Home Janet McMullan, RN, BScN, MN, Clinical Program Lead, OACCAC James
MAINE Advance Directive Planning for Important Health Care Decisions
 MAINE Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Organization
MAINE Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Organization
Maryland Attorney General s Office Douglas F. Gansler Attorney General
 Maryland Attorney General s Office Douglas F. Gansler Attorney General SUMMARY OF MARYLAND HEALTH CARE DECISIONS ACT As Amended Through 2007 I. Informed Consent The Health Care Decisions Act does not affect
Maryland Attorney General s Office Douglas F. Gansler Attorney General SUMMARY OF MARYLAND HEALTH CARE DECISIONS ACT As Amended Through 2007 I. Informed Consent The Health Care Decisions Act does not affect
PAIN MANAGEMENT. Understanding End-of-Life Pain Management. De Anna Looper, RN, CHPN, CHPCA. Carrefour Associates L.L.C.
 PAIN MANAGEMENT Understanding End-of-Life Pain Management De Anna Looper, RN, CHPN, CHPCA Senior Vice President of Clinical Operations Carrefour Associates L.L.C. PAIN MANAGEMENT The effect of uncontrolled
PAIN MANAGEMENT Understanding End-of-Life Pain Management De Anna Looper, RN, CHPN, CHPCA Senior Vice President of Clinical Operations Carrefour Associates L.L.C. PAIN MANAGEMENT The effect of uncontrolled
The Trend of Public Perception of Healthcare in Japan From the 4th Perception Survey of Japanese Healthcare *1
 Field Report The Trend of Public Perception of Healthcare in Japan From the 4th Perception Survey of Japanese Healthcare *1 JMAJ 56(4): 267 274, 13 Narumi EGUCHI* 2 Abstract It is estimated that the population
Field Report The Trend of Public Perception of Healthcare in Japan From the 4th Perception Survey of Japanese Healthcare *1 JMAJ 56(4): 267 274, 13 Narumi EGUCHI* 2 Abstract It is estimated that the population
RESEARCH IN PALLIATIVE CARE: GOALS AND LIMITATIONS
 CAMPUS GROSSHADERN CAMPUS INNENSTADT RESEARCH IN PALLIATIVE CARE: GOALS AND LIMITATIONS Prof. Dr. Claudia Bausewein PhD MSc Research and hospice/palliative care Not new! Emphasis of Cicely Saunders from
CAMPUS GROSSHADERN CAMPUS INNENSTADT RESEARCH IN PALLIATIVE CARE: GOALS AND LIMITATIONS Prof. Dr. Claudia Bausewein PhD MSc Research and hospice/palliative care Not new! Emphasis of Cicely Saunders from
Support for this publication is provided by a grant from e Robert Wood Johnson Foundation, Princeton, New Jersey.
 For more information contact: e National Hospice and Palliative Care Organization 1700 Diagonal Road, Suite 625 Alexandria, VA 22314 Call our HelpLine: 800/658-8898 Visit our Web site: www.caringinfo.org
For more information contact: e National Hospice and Palliative Care Organization 1700 Diagonal Road, Suite 625 Alexandria, VA 22314 Call our HelpLine: 800/658-8898 Visit our Web site: www.caringinfo.org
IDAHO Advance Directive Planning for Important Healthcare Decisions
 IDAHO Advance Directive Planning for Important Healthcare Decisions CaringInfo 1731 King St., Suite 100 Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National (NHPCO),
IDAHO Advance Directive Planning for Important Healthcare Decisions CaringInfo 1731 King St., Suite 100 Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National (NHPCO),
& Care & Choices at the End of Life. Advance Directive. Planning for Important Healthcare Decisions
 compassion & choices Care & Choices at the End of Life. Advance Directive Planning for Important Healthcare Decisions District of Columbia Power of Attorney for Healthcare INFORMATION ABOUT THIS DOCUMENT
compassion & choices Care & Choices at the End of Life. Advance Directive Planning for Important Healthcare Decisions District of Columbia Power of Attorney for Healthcare INFORMATION ABOUT THIS DOCUMENT
National Mental Health Survey of Doctors and Medical Students Executive summary
 National Mental Health Survey of Doctors and Medical Students Executive summary www.beyondblue.org.au 13 22 4636 October 213 Acknowledgements The National Mental Health Survey of Doctors and Medical Students
National Mental Health Survey of Doctors and Medical Students Executive summary www.beyondblue.org.au 13 22 4636 October 213 Acknowledgements The National Mental Health Survey of Doctors and Medical Students
2013 Survey of registered nurses
 We ve earned The Joint Commission s Gold Seal of Approval 2013 Survey of registered nurses Generation Gap Grows as Healthcare Transforms AMN Healthcare, Inc., 2013 12400 High Bluff Drive, San Diego, CA
We ve earned The Joint Commission s Gold Seal of Approval 2013 Survey of registered nurses Generation Gap Grows as Healthcare Transforms AMN Healthcare, Inc., 2013 12400 High Bluff Drive, San Diego, CA
Moving Through Care Settings (Don t Send Me to a Nursing Home)
") Moving Through Care Settings (Don t Send Me to a Nursing Home) NCCNHR Annual Meeting October 23, 2009 Eric Carlson Alfred J. Chiplin, Jr. Gene Coffey 1 At-Home Care Getting More Attention Many federal
Moving Through Care Settings (Don t Send Me to a Nursing Home) NCCNHR Annual Meeting October 23, 2009 Eric Carlson Alfred J. Chiplin, Jr. Gene Coffey 1 At-Home Care Getting More Attention Many federal
Declaring Your Wishes Through an Advance Healthcare Directive A Guide for Mississippi Families
 Declaring Your Wishes Through an Advance Healthcare Directive A Guide for Mississippi Families Advances in medical technology have given us awe-inspiring ability to prolong life despite debilitating diseases
Declaring Your Wishes Through an Advance Healthcare Directive A Guide for Mississippi Families Advances in medical technology have given us awe-inspiring ability to prolong life despite debilitating diseases
voluntary euthanasia: a survey of nurses'
 J7ournal ofmedical Ethics 1999;25:25-30 Conditions required for a law on active voluntary euthanasia: a survey of nurses' opinions in the Australian Capital Territory Betty Kitchener and Anthony F Jorm
J7ournal ofmedical Ethics 1999;25:25-30 Conditions required for a law on active voluntary euthanasia: a survey of nurses' opinions in the Australian Capital Territory Betty Kitchener and Anthony F Jorm
Inquiry into palliative care services and home and community care services in Queensland. Submission to the Health and Community Services Committee
 Inquiry into palliative care services and home and community care services in Queensland Submission to the Health and Community Services Committee August, 2012 1 Introduction The Queensland Nurses Union
Inquiry into palliative care services and home and community care services in Queensland Submission to the Health and Community Services Committee August, 2012 1 Introduction The Queensland Nurses Union
APPENDIX 2 HEALTH CARE POWER OF ATTORNEY
 APPENDIX 2 HEALTH CARE POWER OF ATTNEY A health care power of attorney executed on or after January 1, 2007 must be substantially in the following form (S. C. Code Section 62-5-504 (D): INFMATION ABOUT
APPENDIX 2 HEALTH CARE POWER OF ATTNEY A health care power of attorney executed on or after January 1, 2007 must be substantially in the following form (S. C. Code Section 62-5-504 (D): INFMATION ABOUT
Introduction to Hospice
 Introduction to Hospice Objectives The learner will be able to: Understand general hospice services Discuss ways that hospice services can be accessed Discuss Medicare regulations for hospice services
Introduction to Hospice Objectives The learner will be able to: Understand general hospice services Discuss ways that hospice services can be accessed Discuss Medicare regulations for hospice services
Welcome to the Series on Palliative Care for the Licensed Vocational Nurse.
 Welcome to the Series on Palliative Care for the Licensed Vocational Nurse. My name is Ilene Decker and I am a faculty member and Associate Dean for Academic Affairs at the University of Texas Health Science
Welcome to the Series on Palliative Care for the Licensed Vocational Nurse. My name is Ilene Decker and I am a faculty member and Associate Dean for Academic Affairs at the University of Texas Health Science