SPOUSE INFORMATION (OR GUARANTOR IF PATIENT IS MINOR) EMERGENCY CONTACT (OTHER THAN SPOUSE)
|
|
|
- Maurice Cross
- 8 years ago
- Views:
Transcription
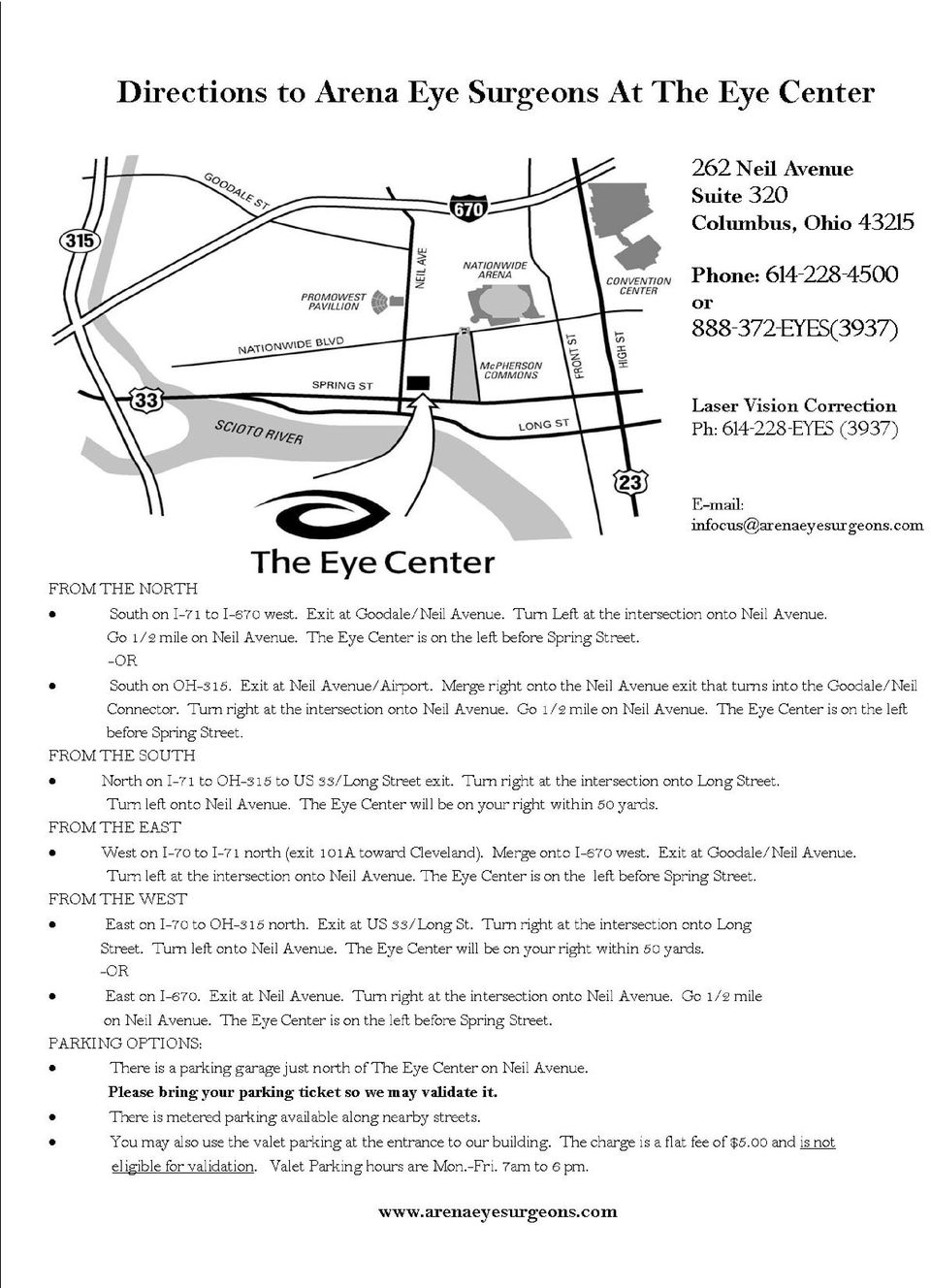
1 OFFICE USE ONLY ARENA EYE SURGEONS PATIENT INFORMATION Acct. No. Doctor Dx Date of Appt. PATIENT INFORMATION PLEASE PRINT Patient Sex: Male Female Marital Status: S M D W Patient Name: FIRST MI LAST Address: Apt. Home Phone: - - City, State, Zip Code: Work Phone: - - Social Security No.: Date of Birth: Cell Phone: - - Address (optional): Occupation: FT / PT Patient Employer: Employer Address: Family Medical Doctor: Who may we thank for referring you to our office? SPOUSE INFORMATION (OR GUARANTOR IF PATIENT IS MINOR) PLEASE PRINT Name: Date of Birth: Social Security No.: Employer: Employer Phone: - - Employer Street Address: City, State, Zip: EMERGENCY CONTACT (OTHER THAN SPOUSE) PLEASE PRINT Name: Phone Number: - - Relationship to Patient: INSURANCE INFORMATION: RECEPTIONIST WILL COPY ALL INSURANCE CARDS PRIMARY Insurance Co.: Subscriber Name: Subscriber Date of Birth: Relationship to Patient: Policy #: Group #: SECONDARY Insurance Co.: Subscriber Name: Subscriber Date of Birth: Relationship to Patient: Policy #: Group #: Treatment received by the ARENA EYE SURGEONS may include, but is not limited to, dilation, laser surgery, and diagnostic procedures. Vision may be temporarily impaired for driving and or operation of mechanical equipment. Should you have any questions concerning this, please feel free to ask the technician. Revised 2/23/2010
 PLEASE PRINT Name: Date of Birth: Social Security No.")
2 ARENA EYE SURGEONS PATIENT HISTORY/MEDICATION FORM Patient Name: DOB: Date: MEDICATION (including over the counter and herbal) STRENGTH DOSAGE FREQUENCY (once a day/twice a day, etc.) Do you have allergies to any medications? (please list below) Medications: Signature: Date: Signature: Date: 3/6/2013
 Do you have allergies to any medications?")
3 ARENA EYE SURGEONS REVIEW OF SYSTEMS FORM Patient Name: Do you have any of the following problems? System Yes/No Date Diagnosed EYE: cataracts, glaucoma, macular degenerations, retina problems, injury or surgery, amblyopia or muscle problems CONSTITUTIONAL (general): fever, weight loss EARS/NOSE/MOUTH/THROAT: dry mouth, hearing loss CARDIOVASCULAR (heart): high blood pressure, high cholesterol, arrhythmia, bypass, congestive failure, heart attack >Pacemaker/Defibrillator/Stent RESPIRATORY (lungs): bronchitis, DOB: Condition/Current Treatment/Surgery Cardiologist Oxygen How many hours asthma, emphysema, MRSA, COPD Sleep Apnea GENITOURINARY: bladder, prostate, Flomax kidneys, dialysis Previously Used D/C GASTROINTESTINAL (stomach): ulcers, heartburn, reflux DERMATOLOGIC (skin): skin disorders, rosacea, MRSA MUSCULOSKELETEL (joints): arthritis, bone problems NEUROLOGICAL (nerves): stroke, MS, Parkinson s, headaches, weakness PSYCHIATRIC: depression, anxiety ENDOCRINE (hormones): thyroid, diabetes >Do you take insulin or oral diabetes meds? Year of diabetes diagnosis: ALLERGIC/IMMUNOLOGIC (allergies/immunity): sinus, seasonal allergies, lupus HEMATOLOGIC/LYMPHATIC (blood/lymph): bleeding tendencies, clots, HIV/AIDS, hepatitis Type: Treatment: Physician: CANCER Type: >Are you allergic to any drugs: List: >Are you allergic to latex: FAMILY HISTORY: Cataracts Glaucoma Macular degeneration High blood pressure Diabetes Family Member SOCIAL HISTORY: Alcohol use Tobacco use Drug use (recreational) Patient s Signature/Date: Tech initials/date: Doctor initials/date: Tech initials/date: Doctor initials/date: 6/1/2010
: bronchitis, DOB: Condition/Current Treatment/Surgery Cardiologist Oxygen How many hours asthma, emphysema, MRSA, COPD Sleep Apnea GENITOURINARY: bladder, prostate, Flomax")
4 262 Neil Ave. Suite 320 Columbus, Ohio Fax ARENA EYE SURGEONS Peter J. Utrata, M.D. John R. Stechschulte, M.D. Robert P. Bennett, M.D. Karl S. Pappa, M.D. Curtin G. Kelley, M.D. Carrie A. Lembach, D.O. Gregory W. DeNaeyer, O.D. 551 W. Central Ave. Suite 101 Delaware, Ohio Fax Our practice offers two types of office eye exams, medical and routine. Insurance companies handle medical eye exams and routine eye exams differently. Please read this form; select the type of examination you expect today and sign below. MEDICAL EYE EXAM Care of eye disease such as cataracts, retinal problems or glaucoma. Evaluation of eye pain, redness, light sensitivity or marked vision changes. ROUTINE EYE EXAM Patient believes she/he has healthy eyes and wants a full eye examination. Patient needs glasses or a change in prescription strength. Patient s insurance pays for an annual or every two year healthy eye exam. IMPORTANT FACTS TO KNOW The measurement for a glasses prescription is called a refraction. Refractions are not covered by Medicare and are to be paid for by the patient at the time of service. Our office does not submit claims to any vision plans. Our ophthalmologists are not providers for any vision insurance plans (i.e.; CVC with United Healthcare, VSP/Vision Service Plan, Cole Vision, Vision One, etc.). Our optometrist is a provider for Eye Med only. Contacts and contact lens fittings are to be paid for by the patient at the time of service. REFERRALS Many insurance companies require the patient to obtain a written referral from his/her primary care physician (PCP). If you have an HMO policy or if a PCP is listed on your insurance card, you need a referral to see our doctors (just as you need for any other specialist you visit). You must have this referral before you see the doctor. If you have not obtained your referral, please use our phone and call your PCP to obtain your referral. The referral can be faxed to our downtown office or our Delaware office PLEASE INDICATE THE TYPE OF EXAM YOU ARE REQUESTING TODAY: Medical Eye Exam - Referral required? Yes No Routine Eye Exam I have my referral. Yes No Self pay Contact Lens Exam Contact Lens Fitting Submit to Eye Med Insurance only PATIENT SIGNATURE: DATE: Medical Office Receptionist will make a copy if requested. Revised 2/1/2010

5 VISUAL ASSESSMENT PATIENT NAME : DOB: VISUAL FUNCTIONING Do you have difficulty, with your glasses, doing the following activities? 1. Reading small print, such as newspaper print, medicine bottles or telephone book? YES NO 2. Reading large-print books? YES NO 3. Reading traffic signs or street signs at a distance? YES NO 4. Difficulty driving at night? YES NO 5. Difficulty driving during the day? YES NO SYMPTOMS Have you been bothered by: 1. Rings or halos around lights? YES NO 2. Glare caused by headlights or bright lights? YES NO 3. Decreased color vision? YES NO Visual Goal 1. Do you dislike wearing glasses? YES NO 2. Do you wish to eliminate the need for glasses? YES NO 3. Do you dislike the idea of wearing reading glasses? YES NO 4. Are you aware that there are implants available to you to help eliminate or decrease the need for glasses after surgery? YES NO SIGNATURE DATE

6 I, (Print Name of Patient), acknowledge that I received a copy of ARENA EYE SURGEONS Notice of Privacy Practices. Signature of Patient or Personal Representative Date I, (Print Name of Patient), acknowledge that I declined a copy of ARENA EYE SURGEONS Notice of Privacy Practices. Signature of Patient or Personal Representative Date Revised 2/1/2010

7 ARENA EYE SURGEONS NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. THE PRIVACY OF YOUR HEALTH INFORMATION IS IMPORTANT TO US. OUR LEGAL DUTY We are required by applicable federal and state law to maintain the privacy of your health information. We are also required to give you this Notice about our privacy practices, our legal duties, and your rights concerning your health information. We must follow the privacy practices that are described in this Notice while it is in effect. This Notice takes effect February 8, 2010, and will remain in effect until we replace it. We reserve the right to change our privacy practices as long as it complies with applicable law. If we make any material revision to this Notice, we will post a copy of the revised Privacy Notice in each of our offices which will specify the date on which the revised Notice is effective. We reserve the right to make the changes in our privacy practices and the new terms of our Notice effective for all health information that we maintain, including health information we created or received before we made the changes. You may request a copy of our Notice at any time. For more information about our privacy practices, or for additional copies of this Notice, please contact us using the information listed at the end of this Notice. USES AND DISCLOSURES OF HEALTH INFORMATION The following categories describe some examples that our practice may use and disclose your medical information. These are some examples and therefore, not every permitted use and disclosure is listed. Treatment: We may use or disclose your health information to a physician or other healthcare provider providing treatment to you. Payment: We may use and disclose your health information to obtain payment for services we provide to you. Healthcare Operations: We may use and disclose your health information about you in connection with our healthcare operations. Healthcare operations include quality assessment and improvement activities, reviewing the competence or qualifications of healthcare professionals, evaluating practitioner and provider performance, conducting training programs, accreditation, certification, licensing or credentialing activities. Your Authorization: In addition to our use of your health information for treatment, payment or healthcare operations, you may give us written authorization to use your health information or to disclose it to anyone for any purpose. If you give us written authorization, you may revoke it in writing at any time. Your revocation will not affect any use or disclosures permitted by your authorization while it was in effect. Unless you give us a written authorization, we cannot use or disclose your health information for any reason except those described in this Notice. Appointment Reminders: We may use and disclose your health information to provide you with appointment reminders (such as voic s or letters). To Your Family and Friends: We must disclose your health information to you, as described in the Patient Rights section of this Notice. We may disclose your health information to a family member, friend or other person to the extent necessary to help with your healthcare or with payment for your healthcare, but only if you agree that we may do so. Person Involved In Care: We may use or disclose health information to notify, or assist in the notification of (including identifying or locating) a family member, your personal representative or another person responsible for your care, of your location, your general condition, or death. If you are present, then prior to use or disclosure of your health information, we will provide you with an opportunity to object to such uses or disclosures. In the event of your incapacity or emergency circumstances, we will disclose health information based on a determination using our professional judgment disclosing only health information that is directly relevant to the person s involvement in your healthcare. We will also use our professional judgment and our experience to make reasonable inferences of your best interest in allowing a person to pick up filled prescriptions, medical supplies, x-rays, or other similar forms of health information. AES NPP, Page 1 of 2

8 Marketing Health-Related Services: We will not use your health information for marketing communications without your written authorization. Required by Law: We may use or disclose your health information when we are required to do so by law. Abuse or Neglect: We may disclose your health information to appropriate authorities if we reasonably believe that you are a possible victim of abuse, neglect or domestic violence or the possible victim of other crimes. We may disclose your health information to the extent necessary to avert a serious threat to your health or safety or the health or safety of others. National Security: We may disclose to military authorities the health information of Armed Forces personnel under certain circumstances. We may disclose to authorized federal officials health information required for lawful intelligence, counterintelligence, and other national security activities. We may disclose to correctional institution or law enforcement official having lawful custody of protected health information of inmate or patient under certain circumstances. PATIENT RIGHTS Access: You have the right to look at or get copies of your health information, with limited exceptions. You may request that we provide copies in a format other than photocopies. We will use the format you request unless we cannot practically and reasonably do so. You must make a request in writing to obtain access to your health information. If you request an alternative format, we may charge a cost-based fee for providing your health information in that format. You may obtain a form to request access by using the contact information listed at the end of this Notice. Disclosure Accounting: You have the right to receive a list of instances in which we or our business associates disclosed your health information for purposes other than treatment, payment, healthcare operations and certain other activities, for the last 6 years or such shorter time as you may specify. If you request this accounting more than once in a 12-month period, we may charge you a reasonable, cost-based fee for responding to these additional requests. Restriction: You have the right to request that we place additional restrictions on our use or disclosure of your health information. We are not required to agree to these additional restrictions (except to the extent required by the Recovery Act for certain cash transactions); but if we do, we will abide by our agreement (except in an emergency). Alternative Communication: You have the right to request that we communicate with you about your health information by alternative means or to alternative locations. You must make your request in writing. Your request must specify the alternative means or location and provide satisfactory explanation how payments will be handled under the alternative means or location you request. Amendment: You have the right to request that we amend your health information. Your request must be in writing and it must explain why the information should be amended. We may deny your request under certain circumstances. Electronic Notice: If you receive this Notice on our Web site or by electronic mail ( ), you have the right to request a paper copy of this Notice. QUESTIONS AND COMPLAINTS If you want more information about our privacy practices or have questions or concerns, please contact us. If you are concerned that we may have violated your privacy rights, or you disagree with a decision we made about access to your health information or in response to a request you made to amend or restrict the use or disclosure of your health information or to have us communicate with you by alternative means or at alternative locations, you may complain to us using the contact information listed at the end of this Notice. You also may submit a written complaint to the U.S. Department of Health and Human Services upon request. We support your right to the privacy of your health information. We will not retaliate in any way if you choose to file a compliant with us or with the U.S. Department of Health and Human Services. Contact Officer: Mary DeLong Telephone: Fax: Address: Arena Eye Surgeons, 262 Neil Avenue, Suite 320, Columbus, OH (Notice amended 6/2/04) (Notice amended 7/10/05) (Notice amended 2/8/2010) AES NPP, Page 2 of 2

9 ARENA EYE SURGEONS Neil Ave. Peter Utrata, MD John Stechschulte, MD 551 W. Central Ave. Suite 320 Robert Bennett, MD Karl Pappa, MD Suite 101 Columbus, Ohio Curtin Kelley, MD Carrie Lembach, DO Delaware, Ohio Kiran Sajja, MD Fax Gregory DeNaeyer, OD Fax Welcome to Arena Eye Surgeons, We trust your first visit with us will meet or exceed your expectations. If any part of your experience with us is not excellent, please contact me. My phone number is and my address is How did you find out about your physician and Arena Eye Surgeons? Check the appropriate box below: Family Member or Friend (Please provide a name so we may send a thank you.) Eye Doctor MD OD Other Type of Physician Health Insurance Plan Arena Eye Surgeons Staff (name) (name) (name) Website Arena Eye Surgeons Website Other Website (Please provide name) Yellow Pages / White Pages Book YellowPages.com Internet Search Engine Publication (name) (name) Community Event/Health Fair Other (Please List) Please bring this completed survey to your appointment. Thank you for choosing Arena Eye Surgeons as your eye health care provider. Mary L. DeLong Mary L. DeLong, MBA Administrator Revised 3/2011

10
Notice of Privacy and Electronic Communication Practices
 Notice of Privacy and Electronic Communication Practices THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION PLEASE REVIEW IT
Notice of Privacy and Electronic Communication Practices THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION PLEASE REVIEW IT
Patient Information. Last First MI (Preferred Name) Male Female Married Single Child. City State Zip Code Emergency Contact/Relation Phone
 Male Female Married Single Child. City State Zip Code Emergency Contact/Relation Phone") LEWIS C. COLE DMD Family and Cosmetic Dentistry 525 ENERGY CENTER BLVD SUITE 1603 NORTHPORT, AL 35473 PHONE 205.344.6900 FAX 205.344.6910 www.lewiscoledentistry.com Patient Name: Patient Information Date:
LEWIS C. COLE DMD Family and Cosmetic Dentistry 525 ENERGY CENTER BLVD SUITE 1603 NORTHPORT, AL 35473 PHONE 205.344.6900 FAX 205.344.6910 www.lewiscoledentistry.com Patient Name: Patient Information Date:
PATIENT REGISTRATION. First Name: Middle Initial: Last Name: Home Phone: Work Phone:
 PATIENT REGISTRATION First Name: Middle Initial: Last Name: Address City, State, Zip: Home Phone: Work Phone: Cell Phone: Birth Date: Age: Sex: Male Female Soc. Sec. #: Occupation: Employer: Marital Status:
PATIENT REGISTRATION First Name: Middle Initial: Last Name: Address City, State, Zip: Home Phone: Work Phone: Cell Phone: Birth Date: Age: Sex: Male Female Soc. Sec. #: Occupation: Employer: Marital Status:
NOTICE ABOUT REFRACTION
 NOTICE ABOUT REFRACTION We have you scheduled for a complete eye exam today. A complete eye exam involves two components: 1. Refraction this portion of the examination determines the best lens correction
NOTICE ABOUT REFRACTION We have you scheduled for a complete eye exam today. A complete eye exam involves two components: 1. Refraction this portion of the examination determines the best lens correction
Date of Birth: / / Age: Gender: M / F SS#: - - Cell Phone: - - Home Phone: - - Email: Address City: State: Zip:
 Paul C. Tisdal, OD Jaclyn A. Munson, OD Welcome to our family of patients! Take a moment and tell us all about you. Sit back, relax, and let us take it from here. Our team is ready to provide customized
Paul C. Tisdal, OD Jaclyn A. Munson, OD Welcome to our family of patients! Take a moment and tell us all about you. Sit back, relax, and let us take it from here. Our team is ready to provide customized
WELCOME TO TRI-COUNTY EYE CLINIC
 WELCOME TO TRI-COUNTY EYE CLINIC Thank you for choosing Tri-County Eye Clinic as the provider for your eye care. You have an appointment at one of the following two locations: 15122 Dedeaux Road, Gulfport,
WELCOME TO TRI-COUNTY EYE CLINIC Thank you for choosing Tri-County Eye Clinic as the provider for your eye care. You have an appointment at one of the following two locations: 15122 Dedeaux Road, Gulfport,
Welcome to Northborough Family Dental
 Date: Patient Information: Welcome to Northborough Family Dental Name D.O.B. SS# Address Apt Town State Zip Marital Status Home Phone Cell# Other Email Employer Work Phone EMERGENCY CONTACT: Name Phone
Date: Patient Information: Welcome to Northborough Family Dental Name D.O.B. SS# Address Apt Town State Zip Marital Status Home Phone Cell# Other Email Employer Work Phone EMERGENCY CONTACT: Name Phone
Insured Party Information (please complete if the insurance is not in your name)
") Price M. Kloess, M.D. / Andrew J. Velazquez, M.D. / J. Randall Pitts, M.D. Holly Young, O.D./ Audrey Richards, O.D./ Brittany M. Mitchell, O.D. Patient Registration and Financial Agreement Patient s Dr
Price M. Kloess, M.D. / Andrew J. Velazquez, M.D. / J. Randall Pitts, M.D. Holly Young, O.D./ Audrey Richards, O.D./ Brittany M. Mitchell, O.D. Patient Registration and Financial Agreement Patient s Dr
Consent for the use of Private Health Information Informed Consent
 Consent for the use of Private Health Information Informed Consent Watertown Dental Care & Dakota Center for Dental Sleep Medicine 600 4 th Street NE, Suite 207 Watertown, SD 57201 Our office operates
Consent for the use of Private Health Information Informed Consent Watertown Dental Care & Dakota Center for Dental Sleep Medicine 600 4 th Street NE, Suite 207 Watertown, SD 57201 Our office operates
Horizon Eye Care, P.A. Patient Information Sheet. For your convenience, please print and complete the pre-registration forms before your visit.
 Patient Information Sheet For your convenience, please print and complete the pre-registration forms before your visit. Section 1: Patient's Legal Name: (First, MI, Last) Parent / Guardian: (If applicable)
Patient Information Sheet For your convenience, please print and complete the pre-registration forms before your visit. Section 1: Patient's Legal Name: (First, MI, Last) Parent / Guardian: (If applicable)
Thank you for making an appointment with our office. We look forward to serving your visual needs.
 Dear New Patient, Thank you for making an appointment with our office. We look forward to serving your visual needs. Enclosed you will find our New Patient Questionnaires. Please complete these and fax
Dear New Patient, Thank you for making an appointment with our office. We look forward to serving your visual needs. Enclosed you will find our New Patient Questionnaires. Please complete these and fax
Lake Oswego Eye Clinic 530 First ST, Suite A Lake Oswego, OR 97068 Office: (503) 636-9608 Fax: (503) 636-9600
 636-9608 Fax: (503) 636-9600") PAYMENT AGREEMENT: We accept most insurance plans as a courtesy. We encourage you to familiarize yourself with your individual plan. Insurance coverage is an agreement between patient and insurance company
PAYMENT AGREEMENT: We accept most insurance plans as a courtesy. We encourage you to familiarize yourself with your individual plan. Insurance coverage is an agreement between patient and insurance company
UH Health Center Dental Office 100 UH Health Center, Building 525 713-227- 6453 (main) / 713-783- 2910 (fax) Patient Information
 / 713-783- 2910 (fax) Patient Information") Name: Address: City, State, Zip: Email: SSN: PeopleSoft Number: Electronic Signboard Health Center Website Email Blast Bus Stop Signage Event Table (Which event: ) Is patient own responsible party? Yes
Name: Address: City, State, Zip: Email: SSN: PeopleSoft Number: Electronic Signboard Health Center Website Email Blast Bus Stop Signage Event Table (Which event: ) Is patient own responsible party? Yes
Patient Checklist. Expect to pay your co-pays and non-covered services on the day of service.
 Welcome to Cedar Run Eye Center. We look forward to your visit with us! Enclosed you will find: Registration Form History Form Patient check list with a map on the back side Patient Name: Date of Appointment:
Welcome to Cedar Run Eye Center. We look forward to your visit with us! Enclosed you will find: Registration Form History Form Patient check list with a map on the back side Patient Name: Date of Appointment:
PATIENT REGISTRATION
 Evan Wolf, MD PhD Jacob Frank, OD PATIENT REGISTRATION Welcome to our office. In order to serve you properly, we will need the following information. (Please Print) Patient First Name Middle Initial Last
Evan Wolf, MD PhD Jacob Frank, OD PATIENT REGISTRATION Welcome to our office. In order to serve you properly, we will need the following information. (Please Print) Patient First Name Middle Initial Last
HISTORY OF PRESENT ILLNESS
 d/b/a Guggino Eye Center 3115 W. Swann Ave., Tampa, FL 33609 (813) 879-7711 13904 N. Dale Mabry Hwy., Suite 200, Tampa, FL 33618 (813) 908-2020 3205 Physicians Way, Sebring, FL 33870 (863) 385-1544 HISTORY
d/b/a Guggino Eye Center 3115 W. Swann Ave., Tampa, FL 33609 (813) 879-7711 13904 N. Dale Mabry Hwy., Suite 200, Tampa, FL 33618 (813) 908-2020 3205 Physicians Way, Sebring, FL 33870 (863) 385-1544 HISTORY
Are you interested in Laser Vision Correction/ LASIK? Yes / No
 Peter J. Cornell, M.D. Stuart B. Stoll, M.D. 450 North Bedford Drive, Suite 101 Beverly Hills, CA 90210 P: (310) 274 9205 F: (310) 274-7229 www.bhlasik.com Name Last First Middle Date of Birth Age_ Sex:
Peter J. Cornell, M.D. Stuart B. Stoll, M.D. 450 North Bedford Drive, Suite 101 Beverly Hills, CA 90210 P: (310) 274 9205 F: (310) 274-7229 www.bhlasik.com Name Last First Middle Date of Birth Age_ Sex:
Welcome to Eye Physicians & Surgeons, PC, Atlanta LASIK Center and Atlanta Eyewear
 Welcome to Eye Physicians & Surgeons, PC, Atlanta LASIK Center and Atlanta Eyewear If you are a new patient to our practice and would like to complete new patient forms before you arrive, please print
Welcome to Eye Physicians & Surgeons, PC, Atlanta LASIK Center and Atlanta Eyewear If you are a new patient to our practice and would like to complete new patient forms before you arrive, please print
Patient Demographic Sheet
 Patient Demographic Sheet Patient Name: Date of Birth: Address: City, State, Zip Code: Home Phone: Cell Phone: Work Phone: E-Mail: Sex: Male Female Marital Status: Married Single Other Occupation: Employer:
Patient Demographic Sheet Patient Name: Date of Birth: Address: City, State, Zip Code: Home Phone: Cell Phone: Work Phone: E-Mail: Sex: Male Female Marital Status: Married Single Other Occupation: Employer:
Welcome! Thank you for choosing our practice for your eye care needs! Please fill out our new patient registration paperwork.
 Welcome! Thank you for choosing our practice for your eye care needs! Please fill out our new patient registration paperwork. So we may eliminate any potential waiting time, please fax the completed forms
Welcome! Thank you for choosing our practice for your eye care needs! Please fill out our new patient registration paperwork. So we may eliminate any potential waiting time, please fax the completed forms
INSURANCE/FINANCIAL DISCLAIMER FOR BRIER CREEK DENTAL
 INSURANCE/FINANCIAL DISCLAIMER FOR BRIER CREEK DENTAL Our office strives to estimate your insurance benefits as accurately as possible. However, your Insurance Policy is a contract between you, your employer
INSURANCE/FINANCIAL DISCLAIMER FOR BRIER CREEK DENTAL Our office strives to estimate your insurance benefits as accurately as possible. However, your Insurance Policy is a contract between you, your employer
TALLAHASSEE EYE CENTER
 TALLAHASSEE EYE CENTER PATIENT INFORMATION Date: Name: Gender: M / F First MI Last Date of Birth: / / Address: City: State: ZIP: Phone Numbers: Home: Cellular: Work: E-Mail: SS#: - - What is the best way
TALLAHASSEE EYE CENTER PATIENT INFORMATION Date: Name: Gender: M / F First MI Last Date of Birth: / / Address: City: State: ZIP: Phone Numbers: Home: Cellular: Work: E-Mail: SS#: - - What is the best way
Medical Insurance and Vision Plans
 Notice of Privacy Practices Methods of Payments No Insurance? No problem! Claremore Eye Associates offers a discount for all non- insurance patients for their vision exam. We also accept all major credit
Notice of Privacy Practices Methods of Payments No Insurance? No problem! Claremore Eye Associates offers a discount for all non- insurance patients for their vision exam. We also accept all major credit
WELCOME TO OUR OFFICE
 WELCOME TO OUR OFFICE WELCOME TO OUR OFFICE Patient Information Insurance Information Today s Date Last First MI Street City State Zip Code Home Phone Work Phone Cell Phone Email Address How do you prefer
WELCOME TO OUR OFFICE WELCOME TO OUR OFFICE Patient Information Insurance Information Today s Date Last First MI Street City State Zip Code Home Phone Work Phone Cell Phone Email Address How do you prefer
Please Print. Patient Name Last First Middle. Address Street Apt # City State Zip. Date of Birth Gender. Home Phone Cell Phone
 Please Print Patient Name Last First Middle Address Street Apt # City State Zip Date of Birth Gender Home Phone Cell Phone Work Phone Social Security# E-mail Occupation Employer Spouse s Name Phone Referred
Please Print Patient Name Last First Middle Address Street Apt # City State Zip Date of Birth Gender Home Phone Cell Phone Work Phone Social Security# E-mail Occupation Employer Spouse s Name Phone Referred
MEDICAL-SURGICAL EYE CARE, P.A.
 MEDICAL-SURGICAL EYE CARE, P.A. DATE PATIENT'S NAME: ADDRESS: CITY/STATE/ZIP: DATE OF BIRTH: MARTIAL STATUS: M S D W HOME PHONE: ( ) SEX: M F AGE: CELLPHONE: ( ) IF CHILD; PARENT OR GUARDIAN NAME: EMERGENCY
MEDICAL-SURGICAL EYE CARE, P.A. DATE PATIENT'S NAME: ADDRESS: CITY/STATE/ZIP: DATE OF BIRTH: MARTIAL STATUS: M S D W HOME PHONE: ( ) SEX: M F AGE: CELLPHONE: ( ) IF CHILD; PARENT OR GUARDIAN NAME: EMERGENCY
Employee s Voluntary Salary Redirection Plan of the City and County of Denver
 Employee s Voluntary Salary Redirection Plan of the City and County of Denver NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
Employee s Voluntary Salary Redirection Plan of the City and County of Denver NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
ORANGE COUNTY EYE INSTITUTE
 ORANGE COUNTY EYE INSTITUTE *Note: It is the patient s responsibility to file insurance claims if we are not contracted with your insurance company. *Note: Be aware that most medical insurance plans do
ORANGE COUNTY EYE INSTITUTE *Note: It is the patient s responsibility to file insurance claims if we are not contracted with your insurance company. *Note: Be aware that most medical insurance plans do
Cutting Edge Eye Care
 Cutting Edge Eye Care The Optos Daytona provides an unequaled 200 degree view of your retina in a single image. This view gives our doctors the opportunity to identify and follow peripheral retinal pathology
Cutting Edge Eye Care The Optos Daytona provides an unequaled 200 degree view of your retina in a single image. This view gives our doctors the opportunity to identify and follow peripheral retinal pathology
THE EYE INSTITUTE. Dear Patient:
 THE EYE INSTITUTE Eye Associates of Wayne P.A. 968 Hamburg Turnpike Wayne, NJ 07470 p. 973-696-0300 f. 973-696-0464 Eye Institute North, LLC 5677 Berkshire Valley Rd. Oak Ridge, NJ 07438 p. 973-208-0600
THE EYE INSTITUTE Eye Associates of Wayne P.A. 968 Hamburg Turnpike Wayne, NJ 07470 p. 973-696-0300 f. 973-696-0464 Eye Institute North, LLC 5677 Berkshire Valley Rd. Oak Ridge, NJ 07438 p. 973-208-0600
Associated Ear, Nose & Throat Specialists, LLC. OCCUPATION: Employer: Work Phone: PHYSICIAN REQUESTING CONSULTATION: TOWN: PHONE:
 Associated Ear, Nose & Throat Specialists, LLC Todd A. Zachs, M.D. Kevin C. Krebsbach, M.D Thomas Hinchey, Au.D., CCC-A Amanda Hessenauer, Au.D. Name: Birth date: SOCIAL SECURITY SEX: M F (IF MINOR) PARENT'S
Associated Ear, Nose & Throat Specialists, LLC Todd A. Zachs, M.D. Kevin C. Krebsbach, M.D Thomas Hinchey, Au.D., CCC-A Amanda Hessenauer, Au.D. Name: Birth date: SOCIAL SECURITY SEX: M F (IF MINOR) PARENT'S
Creekside Physical Therapy and Rehabilitation
 Creekside Physical Therapy and Rehabilitation PATIENT INFORMATION Patient s Name: Social Security #: Age: Sex: M/ F Date of Birth: Email: Home Address: City: State: Zip: Telephone (Hm): Work: Mobile: Employer:
Creekside Physical Therapy and Rehabilitation PATIENT INFORMATION Patient s Name: Social Security #: Age: Sex: M/ F Date of Birth: Email: Home Address: City: State: Zip: Telephone (Hm): Work: Mobile: Employer:
PATIENT REGISTRATION AND HISTORY FORM ~ FAMILY EYE HEALTH ASSOCIATES
 PATIENT REGISTRATION AND HISTORY FORM ~ FAMILY EYE HEALTH ASSOCIATES PATIENT INFORMATION: Name (Last, First, MI) Date: Address: City State Zip Home Phone 2nd Phone Work Cell E-Mail Gender: M F Birthdate
PATIENT REGISTRATION AND HISTORY FORM ~ FAMILY EYE HEALTH ASSOCIATES PATIENT INFORMATION: Name (Last, First, MI) Date: Address: City State Zip Home Phone 2nd Phone Work Cell E-Mail Gender: M F Birthdate
PATIENT DEMOGRAPHIC SHEET
 Patient Information PATIENT DEMOGRAPHIC SHEET Last Name First Name MI of Birth Age Social Security Number Married Widowed Single Other: Marital Status Occupation/Retired Employer English Spanish Mail Phone
Patient Information PATIENT DEMOGRAPHIC SHEET Last Name First Name MI of Birth Age Social Security Number Married Widowed Single Other: Marital Status Occupation/Retired Employer English Spanish Mail Phone
ACKNOWLEDGMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES
 ACKNOWLEDGMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES I acknowledge that I have been provided a copy of Fiorillo Cosmetic and General Dentistry s Notice of Privacy Practices, which has an effective
ACKNOWLEDGMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES I acknowledge that I have been provided a copy of Fiorillo Cosmetic and General Dentistry s Notice of Privacy Practices, which has an effective
Annual Eye Health Exam Eye Care Associates of Princeton DATE :
 Annual Eye Health Exam Eye Care Associates of Princeton DATE : First Name: Last Name: Male/Female (circle) Date of Birth: Age: _ Employer: Occupation: Address: City: State: Zip: Cell Phone Number: May
Annual Eye Health Exam Eye Care Associates of Princeton DATE : First Name: Last Name: Male/Female (circle) Date of Birth: Age: _ Employer: Occupation: Address: City: State: Zip: Cell Phone Number: May
New Patient Information
 New Patient Information Name SSN# - - Date of Birth Male / Female Marital Status Mailing Address City State Zip Home Phone Employer Work Phone How did you hear about our office? Emergency contact Relationship
New Patient Information Name SSN# - - Date of Birth Male / Female Marital Status Mailing Address City State Zip Home Phone Employer Work Phone How did you hear about our office? Emergency contact Relationship
CORONADO EYE ASSOCIATES GLENN B. COOK, M.D., PhD 801 ORANGE AVENUE, STE. 204 - CORONADO, CA 92118 619.437-4406 FAX 619.522-7983
 Dear Please allow us to welcome you to our practice. Our first priority is to provide you with the best care possible. Enclosed is your patient information sheet and medical history questionnaire. Please
Dear Please allow us to welcome you to our practice. Our first priority is to provide you with the best care possible. Enclosed is your patient information sheet and medical history questionnaire. Please
Dear Patient, We look forward to seeing you.
 Dear Patient, Welcome to Mosier Eye Center! We appreciate your selection of our office and we look forward to serving you for all your eye care needs. This packet was created to provide you with some valuable
Dear Patient, Welcome to Mosier Eye Center! We appreciate your selection of our office and we look forward to serving you for all your eye care needs. This packet was created to provide you with some valuable
Western Center Eye Care 2720 Western Center Blvd Ste 316 Fort Worth, TX 76131
 Today s Date Western Center Eye Care WELCOME TO OUR OFFICE Patient s Name (First, Middle, Last): Address: City: State: Zip Code: Email: Main Contact #: Alternate#: Date of Birth: / / Sex: Male Female Primary
Today s Date Western Center Eye Care WELCOME TO OUR OFFICE Patient s Name (First, Middle, Last): Address: City: State: Zip Code: Email: Main Contact #: Alternate#: Date of Birth: / / Sex: Male Female Primary
Mobile Dental Care QUALITY ON-SITE DENTISTRY SINCE 1982
 CONCERNING MEDICAID For Patient: The process for Medicaid to approve the necessary dental treatment and to also fund for that treatment is a slow and confusing procedure. Essentially, Medicaid will make
CONCERNING MEDICAID For Patient: The process for Medicaid to approve the necessary dental treatment and to also fund for that treatment is a slow and confusing procedure. Essentially, Medicaid will make
IMS Allergy & Immunology New Patient Registration Sheet. Personal Information
 Personal Information Today s : Patient First Name: Initial: Last Name: DOB: Age: Social Security #: E-mail: Address: City: State: Zip: Home Phone: Work Phone: Cell Phone: Gender: M F Language: ENGLISH
Personal Information Today s : Patient First Name: Initial: Last Name: DOB: Age: Social Security #: E-mail: Address: City: State: Zip: Home Phone: Work Phone: Cell Phone: Gender: M F Language: ENGLISH
GONZABA MEDICAL GROUP PATIENT REGISTRATION FORM
 GONZABA MEDICAL GROUP PATIENT REGISTRATION FORM DATE: CHART#: GUARANTOR INFORMATION LAST NAME: FIRST NAME: MI: ADDRESS: HOME PHONE: ADDRESS: CITY/STATE: ZIP CODE: **************************************************************************************
GONZABA MEDICAL GROUP PATIENT REGISTRATION FORM DATE: CHART#: GUARANTOR INFORMATION LAST NAME: FIRST NAME: MI: ADDRESS: HOME PHONE: ADDRESS: CITY/STATE: ZIP CODE: **************************************************************************************
Orthodontics on Silver Lake, P.A. Stephanie E. Steckel, D.D.S., M.S. Welcome To Our Office -Please Print-
 HEALTH HISTORY Orthodontics on Silver Lake, P.A. Stephanie E. Steckel, D.D.S., M.S. Welcome To Our Office -Please Print- Date: 20 Date of Birth: Patient s name: First Middle Last Name Patient Prefers to
HEALTH HISTORY Orthodontics on Silver Lake, P.A. Stephanie E. Steckel, D.D.S., M.S. Welcome To Our Office -Please Print- Date: 20 Date of Birth: Patient s name: First Middle Last Name Patient Prefers to
Medicine and Reconstructive Surgery of the Foot and Ankle Board Certified in Foot and Ankle Surgery
 Medicine and Reconstructive Surgery of the Foot and Ankle Board Certified in Foot and Ankle Surgery PATIENT INFORMATION Title First Name MI Last Name Address Apt# City State Zip Code County Home Ph. (
Medicine and Reconstructive Surgery of the Foot and Ankle Board Certified in Foot and Ankle Surgery PATIENT INFORMATION Title First Name MI Last Name Address Apt# City State Zip Code County Home Ph. (
Florida Eye Center Patient Registration Form (Please Print Clearly)
") Florida Eye Center Patient Registration Form (Please Print Clearly) Personal Information Legal Name: Last First MI Suffix Nickname: Social Security: - - Drivers License # Date of Birth: / / Mailing Address:
Florida Eye Center Patient Registration Form (Please Print Clearly) Personal Information Legal Name: Last First MI Suffix Nickname: Social Security: - - Drivers License # Date of Birth: / / Mailing Address:
OMNI DERMATOLOGY, INC. NEW PATIENT INFORMATION RECORD
 OMNI DERMATOLOGY, INC. NEW PATIENT INFORMATION RECORD Name Last: First: MI: Social Security Number: Date of birth: / / Sex: M F Address: Street City State: Zip Code: Contact Numbers: Home Phone: ( ) -
OMNI DERMATOLOGY, INC. NEW PATIENT INFORMATION RECORD Name Last: First: MI: Social Security Number: Date of birth: / / Sex: M F Address: Street City State: Zip Code: Contact Numbers: Home Phone: ( ) -
Retinal Consultants of San Antonio Diseases and Surgery of the Retina and Vitreous www.retinasanantonio. com
 Retinal Consultants of San Antonio Diseases and Surgery of the Retina and Vitreous www.retinasanantonio. com 1 Calvin E. Mein, MD 9480 Huebner Rd, Suite 310 (210) 615-1311 Moises A. Chica, MD San Antonio,
Retinal Consultants of San Antonio Diseases and Surgery of the Retina and Vitreous www.retinasanantonio. com 1 Calvin E. Mein, MD 9480 Huebner Rd, Suite 310 (210) 615-1311 Moises A. Chica, MD San Antonio,
Name Today's Date Sex. Street Address City State Zip Code. Home # Work # Cell # Would you like to receive text confirmations:
 Patient Information 219 Old Hook Road Westwood, NJ 07675 Office: (201) 664-0847 Fax: (201) 664 8890 E-Mail: Mail@2020nj.com Thank you for choosing Valley Eye Associates for you eyecare needs. Please complete
Patient Information 219 Old Hook Road Westwood, NJ 07675 Office: (201) 664-0847 Fax: (201) 664 8890 E-Mail: Mail@2020nj.com Thank you for choosing Valley Eye Associates for you eyecare needs. Please complete
UNIVERSITY OF WISCONSIN MADISON BADGER SPORTS CAMP HEALTH FORM
 UNIVERSITY OF WISCONSIN MADISON BADGER SPORTS CAMP HEALTH FORM Event Name: Dates: Participant Name: Participant cell phone with area code: Custodial Parent/Guardian Name: Phone number: Cell phone: Home
UNIVERSITY OF WISCONSIN MADISON BADGER SPORTS CAMP HEALTH FORM Event Name: Dates: Participant Name: Participant cell phone with area code: Custodial Parent/Guardian Name: Phone number: Cell phone: Home
Life is Beautiful. See it! New Patient. Dr. Mr. Mrs. Ms. First name. Last name. Street address. Home Phone Cell Phone Work Phone
 9201 Sunset Boulevard Suite 709 West Hollywood, CA 90069 New Patient 310. 275. 5533 Fax 310. 275. 5523 info@benjamineye.com www.benjamineye.com Patient Information Title Dr. Mr. Mrs. Ms. Sex M F Patient
9201 Sunset Boulevard Suite 709 West Hollywood, CA 90069 New Patient 310. 275. 5533 Fax 310. 275. 5523 info@benjamineye.com www.benjamineye.com Patient Information Title Dr. Mr. Mrs. Ms. Sex M F Patient
NOTICE OF PRIVACY PRACTICES
 FRANKLIN SQUARE EYE CARE 918 HEMPSTEAD TPKE FRANKLIN SQUARE, NY 11010 TEL #: (516) 354-4242 FAX #: (516) 354-7788 E-mail: franklineyecare@gmail.com OFFICE CONTACT PERSON: SHERIN GEORGE O.D. NOTICE OF PRIVACY
FRANKLIN SQUARE EYE CARE 918 HEMPSTEAD TPKE FRANKLIN SQUARE, NY 11010 TEL #: (516) 354-4242 FAX #: (516) 354-7788 E-mail: franklineyecare@gmail.com OFFICE CONTACT PERSON: SHERIN GEORGE O.D. NOTICE OF PRIVACY
Eye Care of Delaware Patient Health Questionnaire
 Eye Care of Delaware Patient Health Questionnaire Name: Date of birth: Referred by: Eye doctor: Family doctor: Pharmacy name: Phone #: Pharmacy location: Reason for today's visit (signs/symptoms): When
Eye Care of Delaware Patient Health Questionnaire Name: Date of birth: Referred by: Eye doctor: Family doctor: Pharmacy name: Phone #: Pharmacy location: Reason for today's visit (signs/symptoms): When
How do you prefer to be reminded of your dental appointments?
 PATIENT REGISTRATION DATE: ADULT PATIENT CHILD PATIENT Name Address City State Zip Email Landline Cell Phone Do you work? Where? Work Phone Date of Birth Social Security # Single Married Divorced Widowed
PATIENT REGISTRATION DATE: ADULT PATIENT CHILD PATIENT Name Address City State Zip Email Landline Cell Phone Do you work? Where? Work Phone Date of Birth Social Security # Single Married Divorced Widowed
Please allow us to welcome you to our practice. Our first priority is to provide you with the best care possible.
 PAUL L. TREGER, M.D. RANDALL CONRAD, O.D. GLENN B. COOK, M.D., PhD TARA BROWN, M.D. 7877 PARKWAY DRIVE SUITE 100 - LA MESA, CA 91942 619.286.3711 FAX 619.286.2184 Dear Please allow us to welcome you to
PAUL L. TREGER, M.D. RANDALL CONRAD, O.D. GLENN B. COOK, M.D., PhD TARA BROWN, M.D. 7877 PARKWAY DRIVE SUITE 100 - LA MESA, CA 91942 619.286.3711 FAX 619.286.2184 Dear Please allow us to welcome you to
PATIENT REGISTRATION FORM PATIENT INFORMATION
 Siepser Laser Eye Care PATIENT REGISTRATION FORM : PATIENT INFORMATION First Name Middle Initial: Last Name: Birth : Gender: Male Female Marital Status: SSN: Driver s License #: Address: City: State: Zip:
Siepser Laser Eye Care PATIENT REGISTRATION FORM : PATIENT INFORMATION First Name Middle Initial: Last Name: Birth : Gender: Male Female Marital Status: SSN: Driver s License #: Address: City: State: Zip:
Advanced Rheumatology of Houston Offices of Dr. Tamar F Brionez
 Advanced Rheumatology of Houston Offices of Dr. Tamar F Brionez New patient history form Patient name DOB Allergies to Medicines: Current Medications Name Dose Times/day taken Social History Married/single/widowed/divorced
Advanced Rheumatology of Houston Offices of Dr. Tamar F Brionez New patient history form Patient name DOB Allergies to Medicines: Current Medications Name Dose Times/day taken Social History Married/single/widowed/divorced
General Medical Questionnaire
 JONATHAN S LYONS MD, THOMAS H YAU MD, LLC ROBERT P FRIEDLAENDER MD ARUSHA GUPTA MD EYE PHYSICIANS AND SURGEONS 8630 Fenton Street, Suite 514 Silver Spring MD 20910 PATIENT INFORMATION FORM (PLEASE CIRCLE)
JONATHAN S LYONS MD, THOMAS H YAU MD, LLC ROBERT P FRIEDLAENDER MD ARUSHA GUPTA MD EYE PHYSICIANS AND SURGEONS 8630 Fenton Street, Suite 514 Silver Spring MD 20910 PATIENT INFORMATION FORM (PLEASE CIRCLE)
MEDICAL & OCULAR HISTORY QUESTIONAIRRE
 MEDICAL & OCULAR HISTORY QUESTIONAIRRE Name: Date: Age: Preferred Pharmacy Name: Address: 1. Please describe briefly the main reason you are being examined today. 2. Do you have any of the following conditions
MEDICAL & OCULAR HISTORY QUESTIONAIRRE Name: Date: Age: Preferred Pharmacy Name: Address: 1. Please describe briefly the main reason you are being examined today. 2. Do you have any of the following conditions
Dallas Neurosurgical and Spine Associates, P.A Patient Health History
 Dallas Neurosurgical and Spine Associates, P.A Patient Health History DOB: Date: Reason for your visit (Chief complaint): Past Medical History Please check corresponding box if you have ever had any of
Dallas Neurosurgical and Spine Associates, P.A Patient Health History DOB: Date: Reason for your visit (Chief complaint): Past Medical History Please check corresponding box if you have ever had any of
LASIK/PRK Consultation
 LASIK/PRK Consultation How long have you been considering Refractive Surgery (LASIK/PRK)? 6 months 1 Year 2 years As long as I can remember Why are you considering Refractive Surgery? (Please check all
LASIK/PRK Consultation How long have you been considering Refractive Surgery (LASIK/PRK)? 6 months 1 Year 2 years As long as I can remember Why are you considering Refractive Surgery? (Please check all
19235 N Cave Creek Rd #104 Phoenix, AZ 85024 Phone: (602) 485-3414 Fax: (602) 788-0405
 485-3414 Fax: (602) 788-0405") 19235 N Cave Creek Rd #104 Phoenix, AZ 85024 Phone: (602) 485-3414 Fax: (602) 788-0405 Welcome to our practice. We are happy that you selected us as your eye care provider and appreciate the opportunity
19235 N Cave Creek Rd #104 Phoenix, AZ 85024 Phone: (602) 485-3414 Fax: (602) 788-0405 Welcome to our practice. We are happy that you selected us as your eye care provider and appreciate the opportunity
PATIENT REGISTRATION FORM PATIENT INFORMATION
 Siepser Laser Eye Care PATIENT REGISTRATION FORM : PATIENT INFORMATION First Name Middle Initial: Last Name: Birth : Gender: Male Female Marital Status: SSN: Driver s License #: Address: City: State: Zip:
Siepser Laser Eye Care PATIENT REGISTRATION FORM : PATIENT INFORMATION First Name Middle Initial: Last Name: Birth : Gender: Male Female Marital Status: SSN: Driver s License #: Address: City: State: Zip:
WELCOME TO COPPELL VISION CENTER
 WELCOME TO COPPELL VISION CENTER Please Print Name Address Sex: Male Female City/State/Zip Age Home Phone of Birth Alternate Phone SSN# Profession Employed By Responsible Party Address and Phone Number
WELCOME TO COPPELL VISION CENTER Please Print Name Address Sex: Male Female City/State/Zip Age Home Phone of Birth Alternate Phone SSN# Profession Employed By Responsible Party Address and Phone Number
POINCIANA INTERNAL MEDICINE PA. Patient Name: Social Security Number: Date of Birth: / / Sex: M/F (Circle One) Married/Single/Divorced/Widow Address:
 Married/Single/Divorced/Widow Address:") Patient Name: Social Security Number: Date of Birth: / / Sex: M/F (Circle One) Married/Single/Divorced/Widow Address: (Street) (City/State/Zip) Home Phone: ( ) E Mail Address: Would you be interested in
Patient Name: Social Security Number: Date of Birth: / / Sex: M/F (Circle One) Married/Single/Divorced/Widow Address: (Street) (City/State/Zip) Home Phone: ( ) E Mail Address: Would you be interested in
RETINA CARE CENTER, P.C. PATIENT INFORMATION
 RETINA CARE CENTER, P.C. JONATHAN M. BAROFSKY, M.D., F.A.C.S. Parkway Seventy Plaza 1255 Route 70, Suite 31N Lakewood, New Jersey 08701 PHONE (732)905 0004 FAX (732)905 3868 PATIENT INFORMATION Welcome
RETINA CARE CENTER, P.C. JONATHAN M. BAROFSKY, M.D., F.A.C.S. Parkway Seventy Plaza 1255 Route 70, Suite 31N Lakewood, New Jersey 08701 PHONE (732)905 0004 FAX (732)905 3868 PATIENT INFORMATION Welcome
Welcome tokentlands Dental Care
 Patient Information Welcome tokentlands Dental Care Last Name: First Name: MI: Birthdate: Male Female Marital Status: Single Married Other SSN: Address: Apt. No. City: State: Zip: Home Phone: ( ) Work
Patient Information Welcome tokentlands Dental Care Last Name: First Name: MI: Birthdate: Male Female Marital Status: Single Married Other SSN: Address: Apt. No. City: State: Zip: Home Phone: ( ) Work
NEUROSURGERY SERVICES AT APD LOCATED AT UPPER VALLEY MEDICAL GROUP 106 Hanover Street, Lebanon, NH 03766 Phone: 603.448.0447 Fax: 603.448.
 DATE NEUROSURGERY SERVICES AT APD LOCATED AT UPPER VALLEY MEDICAL GROUP 106 Hanover Street, Lebanon, NH 03766 Phone: 603.448.0447 Fax: 603.448.0019 Joseph M. Phillips, M.D., Ph.D. Board Certified in Pain
DATE NEUROSURGERY SERVICES AT APD LOCATED AT UPPER VALLEY MEDICAL GROUP 106 Hanover Street, Lebanon, NH 03766 Phone: 603.448.0447 Fax: 603.448.0019 Joseph M. Phillips, M.D., Ph.D. Board Certified in Pain
PATIENT INFORMATION FORM. Name: Address: City: State: Zip: Social Security Number: Telephone Numbers Home: Age: Sex: M / F Work: Email: Cell:
 PATIENT INFORMATION FORM Name: Address: City: State: Zip: Social Security Number: Telephone Numbers DOB: Home: Age: Sex: M / F Work: Email: Cell: Marital Status: Single Married Spouse s Name: Widowed Divorced
PATIENT INFORMATION FORM Name: Address: City: State: Zip: Social Security Number: Telephone Numbers DOB: Home: Age: Sex: M / F Work: Email: Cell: Marital Status: Single Married Spouse s Name: Widowed Divorced
Patient Information. Name: Soc Security #: Date of Birth: Age: Male / Female. LOCAL Address: Street City State Zip. Phone: Home: Cell / Work:
 Patient Information PERSONAL INFORMATION (Please Print Clearly) Name: Soc Security #: Date of Birth: Age: Male / Female LOCAL Address: Street City State Zip Phone: Home: Cell / Work: Email Address: Out
Patient Information PERSONAL INFORMATION (Please Print Clearly) Name: Soc Security #: Date of Birth: Age: Male / Female LOCAL Address: Street City State Zip Phone: Home: Cell / Work: Email Address: Out
Pulmonary Associates of Richmond
 Pulmonary Associates of Richmond Name: Address One: City: Home Phone#: Work Phone#: Cell Phone#: State: Zip: Sex: Social Security Number: Referring Doctor: of Birth: Employer: Primary Care Doctor: Employment
Pulmonary Associates of Richmond Name: Address One: City: Home Phone#: Work Phone#: Cell Phone#: State: Zip: Sex: Social Security Number: Referring Doctor: of Birth: Employer: Primary Care Doctor: Employment
EAST MS ENDOSCOPIC CENTER, LLC. OPEN ACCESS COLONOSCOPY Patient Questionnaire
 EAST MS ENDOSCOPIC CENTER, LLC OPEN ACCESS COLONOSCOPY Patient Questionnaire PT NAME AGE PHONE NUMBER (Between the hours of 1:00-3:15pm) DATE OF BIRTH 1. Please circle any of the following signs or symptoms
EAST MS ENDOSCOPIC CENTER, LLC OPEN ACCESS COLONOSCOPY Patient Questionnaire PT NAME AGE PHONE NUMBER (Between the hours of 1:00-3:15pm) DATE OF BIRTH 1. Please circle any of the following signs or symptoms
Patient Name: (First) (MI) (Last) (Jr., Sr., etc.) (Preferred Name/Nickname)
 (MI) (Last) (Jr., Sr., etc.) (Preferred Name/Nickname)") Patient Name: (First) (MI) (Last) (Jr., Sr., etc.) (Preferred Name/Nickname) Date of Birth: / / SSN: Gender (circle) M F Address: Apt/Ste: Marital Status (circle) S M D W City: State: Zip Home Ph: Employer
Patient Name: (First) (MI) (Last) (Jr., Sr., etc.) (Preferred Name/Nickname) Date of Birth: / / SSN: Gender (circle) M F Address: Apt/Ste: Marital Status (circle) S M D W City: State: Zip Home Ph: Employer
AUBURN UNIVERSITY PHARMCEUTICAL CARE CENTER New Patient Intake Form. Last Name: First Name: Middle Initial: Date of Birth:
 AUBURN UNIVERSITY PHARMCEUTICAL CARE CENTER New Patient Intake Form Last Name: First Name: Middle Initial: Date of Birth: Insurance Contract Number: Insurance Group Number: Address (Street, City, State,
AUBURN UNIVERSITY PHARMCEUTICAL CARE CENTER New Patient Intake Form Last Name: First Name: Middle Initial: Date of Birth: Insurance Contract Number: Insurance Group Number: Address (Street, City, State,
Roswell Ear, Nose, Throat, & Allergy 342 W. Sherrill Lane Suite A, Roswell, New Mexico 88201 (575)-622-2911 Fax: (575)-622-2598
-622-2911 Fax: (575)-622-2598") Roswell Ear, Nose, Throat, & Allergy 342 W. Sherrill Lane Suite A, Roswell, New Mexico 88201 (575)-622-2911 Fax: (575)-622-2598 Patient Registration Form: (Please Print all Pertinent Information) Last
Roswell Ear, Nose, Throat, & Allergy 342 W. Sherrill Lane Suite A, Roswell, New Mexico 88201 (575)-622-2911 Fax: (575)-622-2598 Patient Registration Form: (Please Print all Pertinent Information) Last
NORTHEAST SPINE & SPORTS MEDICINE PATIENT INTAKE MAILING ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE#: CELL#: WORK PHONE#: S / M / D / W
 NORTHEAST SPINE & SPORTS MEDICINE PATIENT NAME: PATIENT INTAKE SOCIAL SECURITY#: SEX M/F: DATE OF BIRTH: AGE: MAILING ADDRESS: CITY: STATE: ZIP CODE: EMAIL ADDRESS: HOME PHONE#: CELL#: WORK PHONE#: EMPLOYER:
NORTHEAST SPINE & SPORTS MEDICINE PATIENT NAME: PATIENT INTAKE SOCIAL SECURITY#: SEX M/F: DATE OF BIRTH: AGE: MAILING ADDRESS: CITY: STATE: ZIP CODE: EMAIL ADDRESS: HOME PHONE#: CELL#: WORK PHONE#: EMPLOYER:
NEW PATIENT FORMS AARA INFORMATION. Date: Name: Dr. Mr. Mrs. Miss Ms. Birthdate: Height: Weight:
 AARA INFORMATION Due to changes in healthcare privacy and healthcare reform laws, we are now required to gather certain information regarding your race and ethnicity. This information is required as part
AARA INFORMATION Due to changes in healthcare privacy and healthcare reform laws, we are now required to gather certain information regarding your race and ethnicity. This information is required as part
PATIENT/PARENT/GUARDIAN SIGNATURE
 PATIENT REGISTRATION PATIENT S NAME: SEX MALE FEMALE DOB: SOCIAL SECURITY #: CITY/STATE/ZIP: PHONE # GUARANTOR INFORMATION (if responsible party is not the patient) MOTHER S NAME: DOB: SS#: CITY/STATE/ZIP:
PATIENT REGISTRATION PATIENT S NAME: SEX MALE FEMALE DOB: SOCIAL SECURITY #: CITY/STATE/ZIP: PHONE # GUARANTOR INFORMATION (if responsible party is not the patient) MOTHER S NAME: DOB: SS#: CITY/STATE/ZIP:
PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary.
 PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary. Today s : Are you here for an injury that is work-related? YES NO N/A Patient Name (First-Middle-Last)
PATIENT INFORMATION - Please complete and/or verify all information and make changes as necessary. Today s : Are you here for an injury that is work-related? YES NO N/A Patient Name (First-Middle-Last)
P.S. Please remember to bring your completed forms to your office visit!
 Dear Patient: Please print the following forms and complete them as accurately as possible and bring them with you to your office visit. If you have any questions about the forms you can call my office
Dear Patient: Please print the following forms and complete them as accurately as possible and bring them with you to your office visit. If you have any questions about the forms you can call my office
A practice dedicated to excellence in Complete, Comprehensive and Aesthetic Dentistry. Financial Terms
 Financial Terms Thank you for choosing Khanna Dentistry as your dental healthcare provider. We are dedicated to providing the highest quality of care possible. We are also committed to providing our patients
Financial Terms Thank you for choosing Khanna Dentistry as your dental healthcare provider. We are dedicated to providing the highest quality of care possible. We are also committed to providing our patients
1960 Ogden St. Suite 120, Denver, CO 80218, 303-318-3840
 Dear Valued Patient, 1960 Ogden St. Suite 120, Denver, CO 80218, 303-318-3840 Thank you for choosing Denver Medical Associates as your healthcare provider. We strive to provide you with the best possible
Dear Valued Patient, 1960 Ogden St. Suite 120, Denver, CO 80218, 303-318-3840 Thank you for choosing Denver Medical Associates as your healthcare provider. We strive to provide you with the best possible
INSURANCE INFORMATION FINANCIAL AGREEMENT PRIVACY POLICY (HIPAA) LIFETIME INSURANCE AUTHORIZATION
 LIFETIME INSURANCE AUTHORIZATION") PATIENT INFORMATION: DATE: NAME (LAST, FIRST, MI) ADDRESS CITY, STATE, ZIP PHONE ALTERNATE PHONE BIRTHDATE SEX MARITAL STATUS SOCIAL SECURITY RACE/ETHNICITY (please circle): American Indian or Alaskan
PATIENT INFORMATION: DATE: NAME (LAST, FIRST, MI) ADDRESS CITY, STATE, ZIP PHONE ALTERNATE PHONE BIRTHDATE SEX MARITAL STATUS SOCIAL SECURITY RACE/ETHNICITY (please circle): American Indian or Alaskan
New Patient Information Form
 PATIENT INFORMATION New Patient Information Form Patient s Patient s Preferred Name Middle Initial Date of Birth SSN# Primary Language YES NO Email Address Race/Ethnicity Is patient of Hispanic Origin?
PATIENT INFORMATION New Patient Information Form Patient s Patient s Preferred Name Middle Initial Date of Birth SSN# Primary Language YES NO Email Address Race/Ethnicity Is patient of Hispanic Origin?
MEDICATION LIST PATIENT NAME: DATE: Name of Medication Dosage (mg, microgram, etc.) How Many Times a Day
 How Many Times a Day") MEDICATION LIST PATIENT NAME: DATE: Name of Medication Dosage (mg, microgram, etc.) How Many Times a Day PATIENT REGISTRATION CONFIDENTIAL PLEASE COMPLETELY PRINT THE FOLLOWING AND SIGN BELOW PATIENT INFORMATION
MEDICATION LIST PATIENT NAME: DATE: Name of Medication Dosage (mg, microgram, etc.) How Many Times a Day PATIENT REGISTRATION CONFIDENTIAL PLEASE COMPLETELY PRINT THE FOLLOWING AND SIGN BELOW PATIENT INFORMATION
Full name DOB Age Address Email Phone numbers (H) (W) (C) Emergency contact Phone
 (W) (C) Emergency contact Phone") DEMOGRAPHIC INFORMATION Full name DOB Age Address Email Phone numbers (H) (W) (C) Emergency contact Phone CARE INFORMATION Primary care physician: Address Phone Fax Referring physician: Specialty Address
DEMOGRAPHIC INFORMATION Full name DOB Age Address Email Phone numbers (H) (W) (C) Emergency contact Phone CARE INFORMATION Primary care physician: Address Phone Fax Referring physician: Specialty Address
Body Region: Surgery Type: Date:,, Body Region: Surgery Type: Date:,, Body Region: Surgery Type: Date:,, Body Region: Surgery Type: Date:,,
 Medical History Existing or Relevant Previous Conditions Allergies Yes No Dizzy Spells Yes No MRSA Yes No Anemia Yes No Emphysema/Bronchitis Yes No Multiple Sclerosis Yes No Anxiety Yes No Fibromyalgia
Medical History Existing or Relevant Previous Conditions Allergies Yes No Dizzy Spells Yes No MRSA Yes No Anemia Yes No Emphysema/Bronchitis Yes No Multiple Sclerosis Yes No Anxiety Yes No Fibromyalgia
Eger Eye Group, P.C.
 Eger Eye Group, P.C. Last Name: Middle Initial: First Name: Birth Date: Street Address: City/State/Zip: Home Phone: ( ) Work Phone: ( ) Email: Occupation: Employer: Soc. Sec. #: Age: Sex: M F Race: Accompanied
Eger Eye Group, P.C. Last Name: Middle Initial: First Name: Birth Date: Street Address: City/State/Zip: Home Phone: ( ) Work Phone: ( ) Email: Occupation: Employer: Soc. Sec. #: Age: Sex: M F Race: Accompanied
NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only)
") PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
How To Get A Medical Checkup
 NAFISA TEJPAR, M.D., F.A.C.S. 2501 N. Orange Ave, Ste 513 Orlando, FL 32804 (407) 894-1280 APPOINTMENT TIME: (Please be at the office 30 minutes before) Welcome to NAFISA TEJPAR, M.D. PA. We appreciate
NAFISA TEJPAR, M.D., F.A.C.S. 2501 N. Orange Ave, Ste 513 Orlando, FL 32804 (407) 894-1280 APPOINTMENT TIME: (Please be at the office 30 minutes before) Welcome to NAFISA TEJPAR, M.D. PA. We appreciate
Welcome to North Texas Orthopaedic & Spine 955 Garden Park Dr. Ste. 200 Allen Texas 75013. Today s Date: How did you hear of our practice?
 Welcome to North Texas Orthopaedic & Spine 955 Garden Park Dr. Ste. 200 Allen Texas 75013 Name: First Middle Last Today s Date: How did you hear of our practice? Home Address: City: State: Zip: Home Phone:
Welcome to North Texas Orthopaedic & Spine 955 Garden Park Dr. Ste. 200 Allen Texas 75013 Name: First Middle Last Today s Date: How did you hear of our practice? Home Address: City: State: Zip: Home Phone:
Welcome to Dr. Moritis Dental Office
 Welcome to Dr. Moritis Dental Office Patient Information First Last M.I. Address City State Zip Home Phone Work Phone Cell Phone Email Social Security # Birth date Gender M F Marital Status Single Married
Welcome to Dr. Moritis Dental Office Patient Information First Last M.I. Address City State Zip Home Phone Work Phone Cell Phone Email Social Security # Birth date Gender M F Marital Status Single Married
PATIENT INFORMATION. Phone: Cell Phone: _ Work phone: Email Address:
 NEW HAMPSHIRE GASTROENTEROLOGY, INC. 9 Washington Place, Suite 204, Bedford, NH 03110 Office: 603-625-5744 Fax: 603-606-3049 ** Please return this form completed ASAP** PATIENT INFORMATION Name: DOB: DATE:
NEW HAMPSHIRE GASTROENTEROLOGY, INC. 9 Washington Place, Suite 204, Bedford, NH 03110 Office: 603-625-5744 Fax: 603-606-3049 ** Please return this form completed ASAP** PATIENT INFORMATION Name: DOB: DATE:
PATIENT INFORMATION INSURANCE INFORMATION
 (mm/dd/yyyy): Have you been to Physicians Urgent Care before? Yes No Arrival Time: If yes, when? Is this a follow-up to a previous visit: Yes No PATIENT INFORMATION Patient s First Name: Middle Name: Last
(mm/dd/yyyy): Have you been to Physicians Urgent Care before? Yes No Arrival Time: If yes, when? Is this a follow-up to a previous visit: Yes No PATIENT INFORMATION Patient s First Name: Middle Name: Last
Rehabilitation, Sports & Spine Center, P.S. Notice of Privacy Practices. l. Use and Disclosures of Protected Health Information
 Rehabilitation, Sports & Spine Center, P.S. Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
Rehabilitation, Sports & Spine Center, P.S. Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
PRIVACY POLICY (IN ACCORDANCE WITH HIPAA)
") PRIVACY POLICY (IN ACCORDANCE WITH HIPAA) The privacy of your medical information is important to us. We understand that your medical information is personal and we are committed to protecting it. This
PRIVACY POLICY (IN ACCORDANCE WITH HIPAA) The privacy of your medical information is important to us. We understand that your medical information is personal and we are committed to protecting it. This
Guilford Medical Associates, P.A.
 Page 1 Guilford Medical Associates, P.A. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE
Page 1 Guilford Medical Associates, P.A. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE
Please bring the following with you to your appointment: Completed New Patient forms A list of all prescribed medications with dosages and quantity
 Mark E. Hollingshead, M.D. Cataract & Refractive Surgeon Welcome: We look forward to being of assistance to you on your first visit with Hollingshead Eye Center. In order to provide the best possible service,
Mark E. Hollingshead, M.D. Cataract & Refractive Surgeon Welcome: We look forward to being of assistance to you on your first visit with Hollingshead Eye Center. In order to provide the best possible service,
PLEASE COMPLETE AND RETURN
 PLEASE COMPLETE AND RETURN Voluntary Care Network Application Name of Client (Last) (First) (Middle Initial) Street Address Telephone (home) City State Zip Telephone (alternate) Date of Birth US Citizen
PLEASE COMPLETE AND RETURN Voluntary Care Network Application Name of Client (Last) (First) (Middle Initial) Street Address Telephone (home) City State Zip Telephone (alternate) Date of Birth US Citizen
Orthopedic Initial Questionnaire
 Orthopedic Initial Questionnaire Name: Date: Height: Weight: In order to allow the therapist to have a better understanding of the nature of your injury and evaluate your condition fully, please complete
Orthopedic Initial Questionnaire Name: Date: Height: Weight: In order to allow the therapist to have a better understanding of the nature of your injury and evaluate your condition fully, please complete