Anaesthesia and Analgesia
|
|
|
- Stella Lambert
- 8 years ago
- Views:
Transcription
1 Sample chapter from BSAVA Manual of Canine and Feline Anaesthesia and Analgesia 2nd edition Edited by Chris Seymour and Tanya Duke-Novakovski BSAVA

2 7 Patient monitoring and monitoring equipment Yves Moens and Paul Coppens Introduction When performing general anaesthesia, a reversible coma-like state is produced. Most drugs used in anaesthesia have an inherent degree of toxicity and often produce cardiovascular and respiratory side effects. These side effects jeopardize body homeostasis and make anaesthesia a potentially dangerous procedure. In order to limit the risks of general anaesthesia, controllable problems must be prevented. Patientrelated problems can be detected by the pre-anaesthetic examination (see Chapter 2). Checking equipment will help to prevent problems due to technical errors (Figure 7.1; see also Chapters 4, 5 and 6). Furthermore, basic prevention of problems involves maintaining the patient at an appropriate anaesthetic level throughout the procedure. However, even with adequate preparation, it is not possible to eliminate risk because every patient may exhibit individual and unpredictable reactions to anaesthesia. Earliest detection of any adverse reaction by the patient (by closely observing physiological functions during anaesthetic administration) is vital. Therefore, attention should be focused on the monitoring of vital systems, such as the cardiovascular and the respiratory systems, which are responsible for correct delivery of oxygen to the organs. Additionally, other parameters reflecting general homeostasis and the degree of antinociception and unconsciousness should be carefully observed. If deviations from normality outside defined limits occur, analysis of the situation is necessary and corrective measures should be taken. The results of such action must also be evaluated. Monitoring is performed in various ways. Initially, the veterinary surgeon must always make full use of his/her own senses (vision, touch, smell, hearing) to collect clinical information, on which decisions can be made as to whether intervention is necessary. Clinical examination, although very relevant, does have limitations. The information is, in general, more qualitative than quantitative. Moreover, when staff availability is limited, or when the veterinary surgeon monitors more than one patient (or performs some adjustments to equipment), continuous collection of patient parameters will be difficult if not impossible. Therefore, monitoring can be complemented by mechanical and electronic auxiliary equipment. During the last two decades, several new devices have come on to the market and more affordable prices for these have led to their increasing popularity in veterinary anaesthesia. These devices are Anaesthetic machine Check gas source(s): Open cylinder(s) Check quantity Check output pressure Check flowmeter(s) Check vaporizer(s): Off position Quantity Check oxygen bypass Choose and connect a breathing system Check the breathing system; carry out a leak test: 1. Close exhaust valve 2. Obstruct the patient extremity of the breathing system 3. Fill system with oxygen until reservoir bag is under tension (40 cmh 2 O) 4. Check if pressure is kept, otherwise find and fix leak 5. Open exhaust valve If ventilator available: Check function Carry out a leak test Preset the parameters Monitoring equipment Power on Battery state Test Calibration if necessary Specific equipment Intravenous catheter Intubation Fluids Hypothermia prevention Ophthalmic ointment Resuscitation equipment availability Prepare the anaesthesia record 7.1 The preventive approach: pre-anaesthetic equipment check. able to collect information on a continuous basis and can upgrade clinical observation with more sensitive information. The risk of anaesthesia in veterinary medicine remains very high compared with that of human anaesthesia. Healthy dogs and cats run a mortality risk of 0.054% and 0.112%, respectively (Brodbelt et al., 2005). Actual anaesthetic mortality in humans is reported to be as low as 0.05 for every 10,000 patients (Arbous et al., 2001). One should bear in mind that in human medicine (unlike veterinary medicine), anaesthesia is performed by a medical professional specially trained in anaesthesia. 62
. Checking equipment will help to prevent problems due to technical errors (Figure 7.")
3 Monitoring equipment occasionally provides artefactual and wrong information. Hence, the function and limits of these devices (as well the physiological significance of the information they provide) must be very well understood if they are to be used to increase patient safety. Furthermore, this information must be used alongside clinical judgement when evaluating a situation and deciding on possible therapeutic intervention. It is erroneous to think that monitoring may be omitted for some simple or quick procedures, with specific safe drugs or during stable episodes of anaesthesia. Unexpected events often occur during short and simple procedures on apparently healthy patients. Both clinical and technical monitoring must not be limited only to the patient but also include the anaesthetic machine. Monitoring must not concentrate either on one clinical sign or one measured parameter. Simultaneous observation of several parameters (integrated monitoring) is necessary to build a more complete picture of vital system function in the individual animal and the function of the anaesthetic machine. In this way, monitoring is the central tool to pilot anaesthesia with enhanced safety. The main monitor: human senses Veterinary surgeons are used to performing a clinical examination, using their senses, on a daily basis and should adapt this skill to conditions during anaesthesia (Figure 7.2). Moreover, even today, the most appropriate method for assessing the depth of anaesthesia in veterinary practice remains the assessment of clinical signs (Figures 7.3 and 7.4). Sense Observation Information Sight Mucous membrane colour Pale Hypoperfusion, anaemia Pink Normal Red Vasodilation, local congestion Brick red Haemoconcentration Blue Cyanosis Surgical site Tissue colour Cardiovascular and respiratory status Bleeding: colour, intensity Blood vessels: colour, turgescence Thorax, bag of the breathing system, bellows of the ventilator Rate Respiratory rate Amplitude Tidal volume Type Respiratory pattern Eye Position Depth of anaesthesia Lacrimation Pupil size Degree of third eyelid protrusion Movement Spontaneous motor activity Depth of anaesthesia Touch Pulse: femoralis, sublingual, metacarpal, metatarsal arteries Tonus/amplitude Cardiovascular system: heart rate/rhythm, blood pressure Rate/rhythm Autonomous response to noxious stimuli Synchronicity with heart auscultation, ECG Depth of anaesthesia pressure Pulse amplitude: Systolic diastolic pressure difference Capillary refill time Palpebral/corneal reflex Skin temperature Muscle relaxation Relaxation of the jaw Squeeze the bag after closing the exhaust valve Mechanical integrity of the breathing system and respiratory tract time Tonus of the artery Cardiovascular status: peripheral perfusion Depth of anaesthesia Body temperature Muscle tone, depth of anaesthesia Leak Obstruction Pulmonary compliance Thoracic or extrathoracic resistance 7.2 Parameters that can be monitored during anaesthesia using the senses. (continues) 63

4 Sense Observation Information Hearing Smell Abnormal noise Mechanical integrity of the breathing system and respiratory tract Cardiac auscultation: stethoscope, oesophageal stethoscope Rate Rhythm Synchronicity with pulse, ECG Murmur Pulmonary auscultation: stethoscope, oesophageal stethoscope Rate Rhythm Lung sounds Presence of abnormal odour Mechanical integrity of the breathing system and respiratory tract Leak Obstruction Cardiac system: heart rate, rhythm, heart integrity Autonomic responses to noxious stimuli Depth of anaesthesia Respiratory system: rate, rhythm, integrity Autonomic rsponse to noxious stimuli Depth of anaesthesia Leak in the presence of halogenated anaesthetic agent 7.2 (continued) Parameters that can be monitored during anaesthesia using the senses. Parameter Light anaesthesia Adequate anaesthesia Deep anaesthesia Eye position Central Rotated Central Palpebral reflex + Jaw tonicity + Movement Possible Absent Absent Cornea Moist Moist Dry Heart rate Usually increased Usually decreased Respiratory rate Usually increased Usually decreased Haemodynamic and/or respiratory Yes Usually no No variations following surgical stimulation Clinical signs of depth of anaesthesia. Eye position, palpebral reflex and jaw tonicity are the most accurate 7.3 signs to evaluate depth of anaesthesia. Note that heart rate and respiratory rate are influenced by many other factors. These signs are not valid for anaesthesia performed with a dissociative anaesthetic agent. Parameter Light anaesthesia Adequate anaesthesia Deep anaesthesia Eye position Central Central Central Palpebral reflex + + ± Jaw tonicity + + ± Movement Possible Possible Possible/absent Cornea Moist Moist Moist/dry Heart rate Usually increased Usually decreased Respiratory rate Usually increased Usually decreased Haemodynamic and/or respiratory variations Yes Usually no No following surgical stimulation 7.4 Clinical signs of depth of anaesthesia with a dissociative anaesthetic agent. Note that heart rate and respiratory rate are influenced by many other factors. 64
 Parameters that can be monitored during anaesthesia using the senses.")
5 Initially, the person in charge of anaesthesia needs to organize his/her workplace in such a way that the collection of clinical information necessary to assess depth of anaesthesia and the quality of the vital signs is easy: the concept of ergonomics. The aim of this concept is to be able to perform, from one location, a quick and complete assessment of all monitored parameters and machine function (Figure 7.5). The layout of the workplace will help concentration on the perception and integration of measurements from the patient, anaesthetic equipment and monitoring devices. This includes: Clinical parameters, such as eye position, palpebral reflex, jaw tone, mucous membrane colour, capillary refill time, sublingual pulse, chest movement, skin temperature and, during surgery, blood colour and bleeding intensity Indirect clinical parameters, e.g. movement of the reservoir bag Parameters collected from technical/electronic devices, e.g. wave forms and numeric displays on the screen Monitoring of the anaesthetic machine: inlet pressure (when available), flowmeters, vaporizer, breathing system and function of any other accessories like ventilators or syringe pumps. 7.6 The anaesthesia screen. 7.7 (a) Oesophageal stethoscope. (b) Tip of the oesophageal stethoscope. (a) Technical monitors Fluids Patient 7.5 Ergonomics in the workplace. Anaesthetic machine The use of an anaesthesia screen (Figure 7.6), so the patient s head can be seen, and the placement of an oesophageal stethoscope (Figure 7.7), to make cardiac and lung auscultation easier, are strongly recommended. However, the veterinary surgeon remains the main monitor; he/she is the collector of parameters, the central analyser and is responsible for all decisions (i.e. he/she is the pilot on board). The limit of this main monitor is that its quality (and thus safety) is dependent on qualifications, knowledge and experience. A record of anaesthesia, even in a simple form, must be completed. This will: Aid appreciation of trends in observed and measured parameters Act as a reference for future anaesthesia in an individual animal (b) Act as a source for retrospective analysis, allowing further improvement of anaesthesia strategies Represent a medicolegal document, attesting the presence of an active monitoring effort of the patient during anaesthesia. Monitoring of parameters that reflect the integration of several physiological functions Capnometry and capnography Capnometry is the measurement and numerical display of the carbon dioxide concentration in the respiratory gas during the whole respiratory cycle (inspiration and expiration). When a continuous graphical display (screen or paper) is available, the measurement produces typical curves (a capnogram) and the technique (instrument) is often referred to as capnography (capnograph). 65

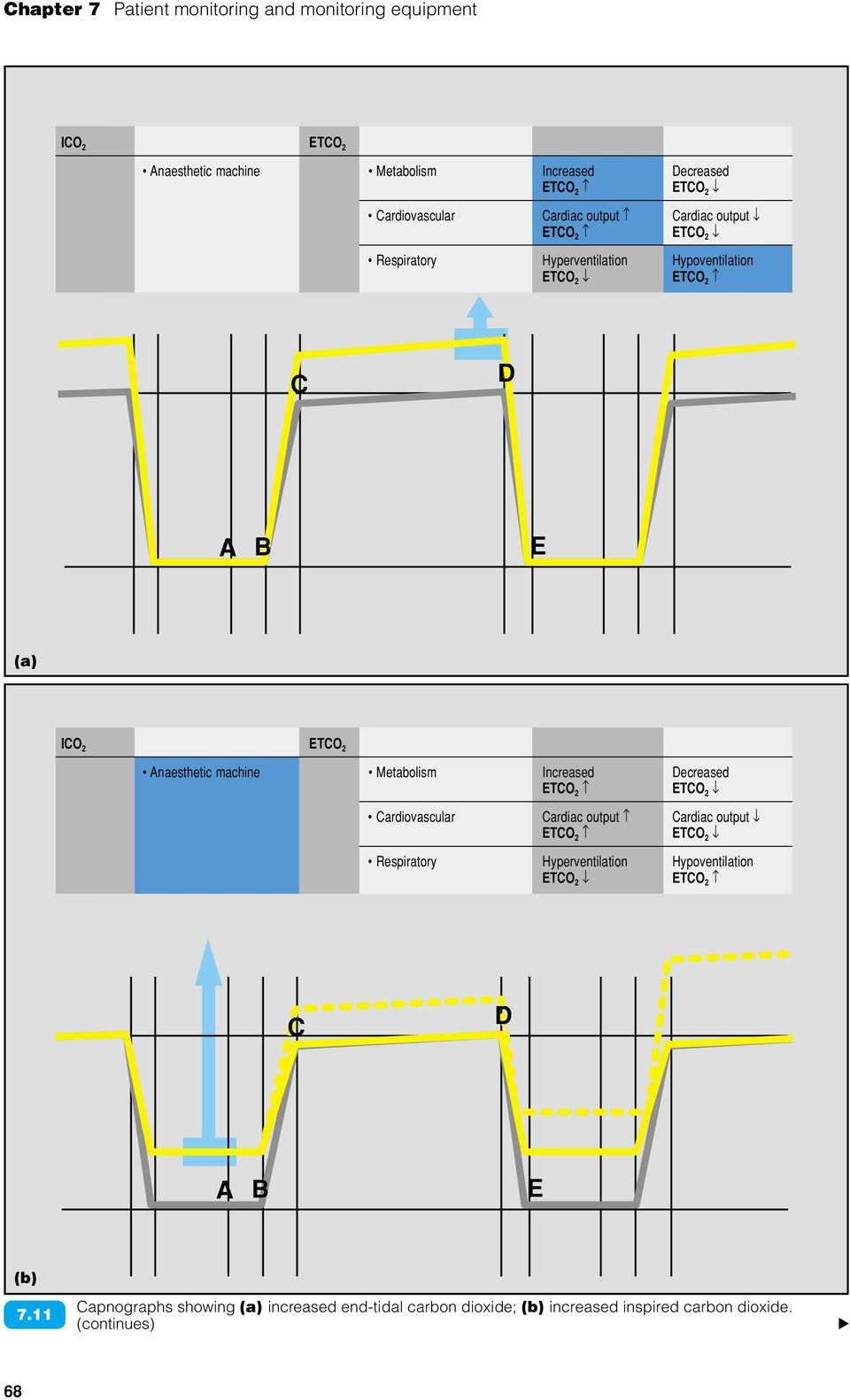
6 The measuring principle relies on absorption of infrared light by carbon dioxide molecules. Capnometers are available as either sidestream or mainstream infrared analysers. Sidestream capnometers require a sampling line connected to the airway and continuously sample the respiratory gases (Figure 7.8a). Samples are then analysed in the measuring chamber of the instrument. With mainstream analysers, miniaturization allows placement of the measuring chamber directly in the airway and the measurement signal is generated here (Figure 7.8b). The capnogram The production of the capnogram is based on the fact that carbon dioxide is produced in cells as a result of metabolism and then carried by the circulation to the lungs, where it is removed by alveolar ventilation. There are four distinct phases of the capnogram (Figure 7.9a): Phase I is the inspiratory baseline. This phase represents the analysis of the gas mixture inspired by the patient for carbon dioxide. The (a) (b) (a) Close-up of a connector for sampling gas 7.8 (sidestream capnograph). (b) Adaptor and sensor of a mainstream capnograph. ICO 2 ETCO 2 Anaesthetic machine Metabolism Increased Decreased ETCO 2 ETCO 2 A B C Cardiovascular Cardiac output Cardiac output ETCO 2 ETCO 2 Respiratory Hyperventilation Hypoventilation ETCO 2 ETCO 2 D E 7.9 (a) The normal capnogram. (b) Cardiogenic oscillations. A B: exhalation of carbon dioxidefree gas contained in deadspace at the beginning of expiration. B C: respiratory upstroke, representing the emptying of connecting airways and the beginning of emptying of alveoli. C D: expiratory (alveolar) plateau, representing emptying of alveoli. D: end-tidal carbon dioxide level the best approximation of alveolar carbon dioxide level. D E: inspiratory downstroke, as the patient begins to inhale fresh gas. E A: continuing inspiration, where carbon dioxide remains at zero. ETCO 2 = End-tidal carbon dioxide; ICO 2 = Inspired carbon dioxide. (a) I II III IV C D A B E (b) 66
.")
7 baseline should have a value of zero, otherwise the patient is rebreathing carbon dioxide Phase II is the expiratory upstroke. This represents arrival at the sampling site of carbon dioxide from the alveoli and the mixing with gas present in the conducting airways. It is usually very steep Phase III is the expiratory (alveolar) plateau, which represents pure alveolar gas (of emptying alveoli). Due to uneven emptying of alveoli, the slope continues to rise gradually during the expiratory pause. The peak of this exhaled carbon dioxide is called the end-tidal carbon dioxide Phase IV is the inspiratory downstroke. This is the beginning of the inhalation and the carbon dioxide curve falls steeply to zero. During anaesthesia, with long expiratory times, phase III can show cardiogenic oscillations caused by movement of the heart and this is considered normal (Figure 7.9b). The capnometer usually displays respiratory rate, the value of end-tidal carbon dioxide and sometimes the value for inspiratory carbon dioxide. If a capnograph is used, the presence of a normal shape of the capnographic curve indicates that the number displayed for end-tidal carbon dioxide is likely to represent a true end-expiratory sample. When grossly normal ventilation/perfusion conditions in the lungs exist, the end-tidal carbon dioxide reflects the partial pressure of carbon dioxide in arterial blood (P a CO 2 ; Figure 7.10). Hence capnometry offers a continuous, non-invasive way to reflect the partial pressure of carbon dioxide in arterial blood, which is directly determined by alveolar ventilation. End-tidal carbon dioxide is displayed as a concentration in volume percent (%) or as a partial pressure (in mmhg or kpa). Concentration can be converted into mmhg with the formula: PCO 2 = (P bar -47) x %CO 2 /100 where P bar is barometric pressure in mmhg. Capnometers can often perform the conversion because of a barometric pressure sensor in the device. End-tidal carbon dioxide concentrations between 5 and 6% (35 45 mmhg; kpa) are considered normal in anaesthetized animals. Interpreting the capnogram The approach for proper interpretation of capnographic information is initially to check if a normal capnographic curve is present and then to note the numerical value of end-tidal carbon dioxide. One must acknowledge the possible contribution of metabolism, circulation and ventilation to the production of this number. When two functions are stable, capnometry monitors closely the third function, e.g. if metabolism and circulation are stable, the capnometer monitors ventilation. Conversely, if metabolism and ventilation are stable, the state of the circulation will be more closely reflected. Additionally, capnography will provide information about airway patency, technical faults and adequacy of gas flow in non-rebreathing systems. Capnography has become standard care for intraoperative monitoring of ventilatory efficiency and thus decreases the need for invasive arterial blood gas analysis. Increased ETCO 2 : Increases in end-tidal carbon dioxide concentrations (Figure 7.11a) may be due to impaired alveolar ventilation (anaesthetic-induced respiratory depression), increased metabolism (malignant hyperthermia or early sepsis), increased cardiac output or the addition of carbon dioxide to the circulatory system as a result of rebreathing carbon dioxide. In the latter case, increased inspired carbon dioxide will be associated with increased end-tidal carbon dioxide (Figure 7.11b). Increased end-tidal carbon dioxide is also observed during laparoscopy due to absorption from the peritoneum of carbon dioxide used to inflate the abdomen. CO 2 MONITOR Capnography: 7.10 the principle. P A CO 2 = Alveolar carbon dioxide; P a CO 2 = Partial pressure of carbon dioxide in arterial blood; P v CO 2 = Partial pressure of carbon dioxide in venous blood. DISPLAY UNIT P A CO 2 P v CO 2 P a CO 2 67

8 ICO 2 ETCO 2 Anaesthetic machine Metabolism Increased Decreased ETCO 2 ETCO 2 Cardiovascular Cardiac output Cardiac output ETCO 2 ETCO 2 Respiratory Hyperventilation Hypoventilation ETCO 2 ETCO 2 C D A B E (a) ICO 2 ETCO 2 Anaesthetic machine Metabolism Increased Decreased ETCO 2 ETCO 2 Cardiovascular Cardiac output Cardiac output ETCO 2 ETCO 2 Respiratory Hyperventilation Hypoventilation ETCO 2 ETCO 2 C D A B E (b) 7.11 Capnographs showing (a) increased end-tidal carbon dioxide; (b) increased inspired carbon dioxide. (continues) 68
9 ICO 2 ETCO 2 Anaesthetic machine Metabolism Increased Decreased ETCO 2 ETCO 2 Cardiovascular Cardiac output Cardiac output ETCO 2 ETCO 2 Respiratory Hyperventilation Hypoventilation ETCO 2 ETCO 2 C D A B E (c) 7.11 (continued) Capnograph showing (c) decreased end-tidal carbon dioxide. Decreased ETCO 2 : Decreased end-tidal carbon dioxide concentrations (Figure 7.11c) may be due to hyperventilation, low cardiac output (low blood volume delivered to the lungs) or pronounced hypothermia. Rapidly falling end-tidal carbon dioxide, in the presence of respiratory movements and absence of hyperventilation, is a good indicator of failing circulation and cardiac arrest. Absent end-tidal carbon dioxide can indicate respiratory arrest (no alveolar ventilation), cardiac arrest (no circulation) or technical problems (see below). Rapid diagnosis of cardiac arrest increases the chance of a successful outcome for cardiopulmonary resuscitation. End-tidal carbon dioxide values during resuscitation and cardiac massage reflect efficiency of lung perfusion, and in human medicine have been considered to have prognostic value for successful restoration of spontaneous circulation. Technical monitoring: Several technical aspects of breathing systems, their function and connection to the patient are also monitored by quantitative (capnometer value) and qualitative analysis (capnogram morphology). The presence of inspired carbon dioxide (rebreathing) (see Figure 7.11b) can be due to soda lime exhaustion; an incompetent expiratory valve on a circle system allowing exhaled carbon dioxide to be re-inhaled (even with normal function of soda lime); insufficient gas flow in a nonrebreathing system. An abnormal capnogram may be due to: A dislodged endotracheal tube A misplaced endotracheal tube (oesophageal intubation) An obstructed endotracheal tube or airway (endotracheal tube cuff hernia; Figure 7.12) C D Capnograph showing 7.12 increased resistance at expiration. A B E 69

10 A leak around the endotracheal tube cuff (Figure 7.13) Disconnection of the endotracheal tube from the breathing system. Capnometry versus capnography: The drawback of a capnometer compared with a capnograph is that the former lacks the capnogram and, therefore, cannot provide a qualitative analysis and precise diagnosis from the morphological changes of exhaled carbon dioxide. When ventilation/perfusion mismatch in the lungs becomes important, the end-tidal carbon dioxide underestimates P a CO 2 due to an increase in alveolar deadspace (e.g. low cardiac output, pulmonary thromboembolism). With sidestream devices, artefactually low end-tidal carbon dioxide is seen: When concomitant aspiration of ambient air occurs anywhere between sampling site and measuring chamber With rapid respiratory rates and very low tidal volumes When sampling at the level of fresh gas delivery in non-rebreathing systems. The sampling line can become obstructed by condensation drops or aspiration of any fluids. With mainstream capnographs, the measuring chamber in the airway adaptor can become dirty or damaged, leading to erroneous end-tidal or inspired carbon dioxide values. Sidestream technology offers other (less important) possibilities like sampling directly from a nostril in non-intubated patients. Mainstream technology can be used only in the presence of an endotracheal tube, but copes better with rapid respiratory rates and very small tidal volumes. Pulse oximetry The pulse oximeter is a device that allows noninvasive measurements of the saturation of haemoglobin with oxygen (S p O 2 ); in addition, it displays heart rate. The principle of measurement is as follows: a probe, which features a transmitter and receiver of red and infrared light, is positioned to transilluminate a pulsatile arteriolar bed. In small animal patients, it is usually placed on the tongue, prepuce or other unpigmented area (Figure 7.14). Computer software analyses the total absorption of the light and detects the pulsating component of the absorption that originates from cyclic arrival of arterial blood in the tissue. The absorption of infrared and red light by the pulsatile component is measured differentially. Because oxyhaemoglobin and reduced haemoglobin absorb more infrared and red light, respectively (Figure 7.15), a ratio is calculated that corresponds to a percentage of haemoglobin saturated with oxygen (Figure 7.16). Because maximal total light absorption corresponds to a pulse, the pulse oximeter also provides a figure for pulse rate. C D Capnograph showing 7.13 leakage at the level of endotracheal tube and/or breathing system. A B E (a) 7.14 Sensor of a pulse oximeter. (a) On the tongue. (b) On a non-pigmented toe. (b) 70
.")
11 Absorption (log scale) Red 660 nm Infrared 940 nm oxyhb reduced Hb Any general cause of poor peripheral perfusion, such as vasoconstriction associated with shock, hypothermia or use of alpha-2 agonists, causes erroneously low values or failure to measure. Local hypoperfusion can also be induced by progressive pressure from the clip holding the probe; changing the position of the clip and the probe every so often temporarily solves the situation. Other factors can also interfere with pulse oximetry readings: 7.15 SpO2 (%) Wavelength Light absorption of reduced haemoglobin and oxyhaemoglobin. Ratio red/infrared light absorption 7.16 Relationship between the ratio of red to infrared light absorption and the saturation of haemoglobin with oxygen (S p O 2 ). The threshold of hypoxaemia occurs at an arterial oxygen tension of 60 mmhg (8 kpa). As shown on the dissociation curve of haemoglobin (Figure 7.17), this threshold corresponds to a saturation of 90%. During anaesthesia, therefore, oxygen saturation must be kept above 90%. When oxygen is supplied (or even in a healthy patient breathing room air), a saturation closer to 100% should be expected. The usual precision of measurement of a pulse oximeter is ± 2%. It is important to note that S p O 2 only indicates that the patient is receiving enough oxygen; S p O 2 can be normal in hypoventilating patients when the inspired oxygen fraction is increased (which normally should be the case during anaesthesia). In these circumstances, S p O 2 gives no information about adequacy of ventilation. Conversely, when a patient hypoventilates whilst breathing room air, S p O 2 will fall. Hb saturation (%) P a O 2 (mmhg) Haemoglobin oxygen dissociation curve. The presence of abnormal haemoglobin will affect measurement. For instance, in the presence of carboxyhaemoglobin S p O 2 will be overestimated Interference from ambient light will reduce the quality of the signal received Motion or shivering, use of electrosurgical equipment and mucosal or skin pigmentation. Some pulse oximeters display a photoplethysmographic waveform. The presence of a regular and distinct waveform similar to an arterial pressure waveform confirms the validity of the displayed S p O 2 values (Figure 7.18). Moreover, this can be supported by a displayed heart rate equivalent to the true heart rate. However, the amplitude of the waveform does not necessarily reflect the quality of the signal because the gain can be automatically adapted. (a) (b) (a) Pulse oximeter: display of S p O 2, heart rate 7.18 and waveform. (b) Display of capnography and pulse oximetry. Capnography and pulse oximetry Capnography and pulse oximetry (see Figure 7.18b) provide complementary information. It has been shown that the proper interpretation of information received by capnography and pulse oximetry, used together, have the potential to prevent 93% of the complications during anaesthesia in human medicine (Tinker, 1989). Blood gas analysis Blood gas analysers measure directly the ph and the partial pressures of oxygen and carbon dioxide in a blood sample. They also calculate derived variables, such as plasma bicarbonate concentration (HCO 3 ), base excess and saturation of haemoglobin with oxygen (S a O 2 ). In traditional analysers, the blood sample is aspirated into a circuit bringing the blood in contact with different electrodes to perform the measurements. These machines are expensive and require careful maintenance. Recently, portable and even handheld 71
 Wavelength Light absorption of reduced haemoglobin and oxyhaemoglobin. Ratio red/infrared light absorption 7.")
12 blood gas analysers have become available, allowing blood gas analysis to be performed in remote locations. These devices use disposable cartridges, which need only a minimal amount of blood to perform the measurement. They measure blood gas parameters but offer the option to measure additional parameters, e.g. electrolytes, glucose and lactate. Blood gas analysis is the gold standard method for evaluation of gas exchange. It provides invaluable information about the oxygenation, ventilation and acid base status of the patient. Interpretation of the values for ph, PCO 2 and HCO 3, coupled to the clinical history of the patient, allows identification of respiratory and metabolic acidosis and alkalosis, as well as ongoing compensatory mechanisms. The detailed interpretation of blood gas measurements can be complex as all the results are interrelated, and interested readers are advised to consult standard textbooks on the subject. Figure 7.19 summarizes basic interpretation of blood gas analysis. If the ability of the lungs to oxygenate blood is to be assessed, sampling of arterial blood is mandatory. The value of P a O 2 (partial pressure of oxygen in arterial blood) on its own is not meaningful to evaluate oxygenation if the inspired oxygen fraction (F i O 2 ) is not known. Classical indices of oxygenation are: The ratio P a O 2 /F i O 2 (normal: >300) The alveolar arterial difference for PO 2 ((A-a)PO 2 ) where P A O 2 = ((P bar -47) x F i O 2 ) 1.2P a CO 2 (normal: 5 10 mmhg if F i O 2 = 0.21, 100 mmhg if F i O 2 = 1.0). The gold standard to evaluate the efficiency of ventilation is P a CO 2. The assessment of venous blood samples does not provide straightforward information about oxygenation, but it does allow satisfactory monitoring of the ability to remove carbon dioxide by ventilation and the acid base status. The classic blood gas machine uses samples of heparinized blood. Failure to use the correct samples causes clotting within the circuit. To obtain accurate results, blood samples should be withdrawn anaerobically (no air bubbles) to avoid actual gas tensions being modified by gas exchange with room air. Analysis is best done promptly, but storing blood samples for less than 1 hour in iced water is acceptable. Taking an arterial blood sample is relatively easy in larger animals, but rather difficult in very small ones. Femoral and dorsal metatarsal arteries are often used. Without careful attention to technique, complications such as haematoma or bruise formation at the site of sampling can occur. In particular, pressure should be applied to the site for several minutes after sample collection to allow the vessel to seal. If it is likely that multiple samples will be required, insertion of an arterial catheter should be considered; this is often done in combination with invasive blood pressure measurement. Blood gas analysis is useful in the management of critically ill patients and patients with ventilatory problems. Specific treatment can be planned from the results of initial blood gas analysis, and the response to this treatment can be monitored by taking further blood gas samples. The necessity of repeated blood sampling in anaesthesia is diminished when noninvasive monitors of oxygenation and ventilation are used simultaneously, e.g. pulse oximetry and capnometry. Cardiovascular monitoring Heart rate indicator Heart rate indicators exist as separate devices but more often heart rate counting is a feature of an electrocardiographic monitoring system. The heart rate is deduced using detection of the QRS complex. The number of complexes is counted over a certain time period and calculated as beats per minute. Algorithms are based on human use and in veterinary patients regularly cause the display of a double heart rate when relatively high T waves are erroneously detected as QRS complexes. The displayed heart rate must be regularly double-checked by clinical examination. There is no information about the pumping function of the heart (see Electrocardiography, below) and consequently such heart rate indicators can give a false feeling of security. Blood pressure Arterial blood pressure Arterial blood pressure is one of the most useful measures of cardiovascular function available to the veterinary surgeon. Two methods of measuring blood pressure can be used: invasive (direct) and non-invasive (indirect). Invasive blood pressure measurement is less straightforward to carry out in practice conditions but, on the other hand, non-invasive blood pressure measurement might not fulfil the expectations of reliability and accuracy. Parameter Normal values Decrease Increase ph Acidaemia Alkalaemia P a CO mmhg Respiratory component: alkalosis Respiratory component: acidosis HCO mmol/l Metabolic component: acidosis Metabolic component: alkalosis P a O 2 If oxygen level in inspired gas (F i O 2 ) = Hypoxaemia: <60 mmhg (8kPa) Due to increased F i O 2 or increased 21%: mmhg ( kpa) atmospheric pressure S a O % Hypoxaemia: < 90 % 7.19 Basic interpretation of blood gas analysis. 72

13 Invasive blood pressure measurement: Invasive blood pressure measurement is considered the gold standard technique. A catheter must be placed in a peripheral artery. In the dog, the dorsal metatarsal artery is most commonly used, but the femoral artery or the palmar artery can also be used. In the cat, the femoral artery is the most common site. The catheter is connected to a pressure transducer via non-compliant tubing filled with heparinized saline. Pure mechanical pressure transducers have been mostly abandoned for electronic ones connected to the monitoring device. The transducer must be zeroed to ambient air at the level of the right atrium. The transducer monitor combination gives a continuous reading of blood pressure and shows the pressure waveform. Systolic and diastolic pressures are taken as the cyclic maximum and minimum pressures, respectively. Mean pressure is automatically calculated. To allow trouble-free continuous monitoring (avoiding clotting in the arterial line), the setup is combined with a pressurized continuous flush system that does not influence the accuracy of the pressure reading (Figure 7.20). Repeated arterial blood sampling (blood gas analysis) is easy when an arterial catheter is in place. Non-invasive blood pressure measurement: There are two methods generally used to measure blood pressure non-invasively: the oscillometric method and the Doppler method. Both methods are based on the occlusion of blood flow to an extremity by the inflation of a cuff and detection of reappearance of blood flow during deflation. Any of the limbs or the tail can be used. The ideal cuff width is usually quoted as 40% of the circumference of the limb. Wider cuffs will lead to underestimation of the true pressure, while narrow cuffs will tend to overestimate. Most cuffs have a mark that should be placed directly over the artery. Using the oscillometric method, returning blood flow is detected by pulsatile pressure changes in the cuff itself. The pressure at which pulses in the cuff appear is taken as systolic blood pressure. As the cuff is further deflated, diastolic and mean blood pressure are measured. Oscillotonometric devices record mean blood pressure as the pressure at which the pulses in the cuff are maximal and diastolic pressure as the pressure below which they disappear. The option of automated function provides non-invasive blood pressure measurements at adjustable time intervals. Heart rate is also usually displayed. Using the Doppler method, placement of an ultrasound probe over an artery distal to the cuff is necessary. The emitted ultrasound is reflected by the moving blood and a frequency shift is converted to an audible signal. The pressure at which blood flow recommences, characterized by a typical whoosh sound, is taken as systolic blood pressure. Diastolic pressure is more difficult to determine. No automatic function is available but leaving the probe in place with a deflated cuff allows one to hear the blood flow continuously, hence turning it into a continuous monitor. Changes in the pitch of the tone suggest changing haemodynamics. The Doppler technique can be applied to any size of animal, including cold-blooded animals, and is relatively inexpensive. It requires more operator experience than automated oscillometric measurement and the noise it produces can be disturbing to some unless headphones are used. Monitor Set-up for 7.20 invasive blood pressure measurement. Pressurized continuous flush system Electronic pressure transducer Catheter in peripheral artery 73

14 Significance of information: There is a wide range in blood pressure encountered in anaesthetized dogs and cats. Ranges commonly seen are between 90 and 120 mmhg for systolic, between 55 and 90 mmhg for diastolic, and between 60 and 120 mm Hg for mean blood pressure. Generally, arterial blood pressure gives an indication of the adequacy of cardiovascular function. The systolic blood pressure is determined by a combination of peripheral vascular resistance, stroke volume and intravascular volume, whereas diastolic blood pressure primarily arises from peripheral vascular resistance. Measurement of systolic and diastolic blood pressures allows estimation of pulse pressure, which is the difference between systolic and diastolic pressures (pulse quality). Mean blood pressure is an important factor in relation to general tissue perfusion. Blood flow to the major organs of the body is autoregulated across a range of mean blood pressures from about 60 mmhg to about 120 mmhg. When mean blood pressure falls below this range, blood flow to the major organs is jeopardized. This results in inadequate oxygen delivery and accumulation of lactic acid, leading to acidosis. On the other hand, it must be realized that a normal mean blood pressure does not necessarily equate to good overall tissue perfusion. If a normal blood pressure is generated by excessive vasoconstriction, perfusion of tissue might be insufficient. Acute hypertension can have deleterious effects on the central nervous system and the lungs. Changes in blood pressure and heart rate can be seen with inadequate anaesthetic depth, anaesthetic agent overdose, hypovolaemia and overhydration (see also Chapters 19 and 29). Analysis of the arterial waveform with invasive blood pressure measurement allows semiqualitative estimation of ventricular contractility, hypovolaemia, cardiac output and the role of peripheral resistance, e.g. a low dichrotic notch indicates vasodilation, steepness of upstroke represents strength of contraction. Invasive blood pressure monitoring is less practical than non-invasive techniques in the clinical setting. It requires more expensive equipment, skills in placement of a catheter (especially in smaller patients) and correct calibration. There is a risk of haematoma formation, particularly after withdrawal of the catheter, and a risk of infection. Individual blood pressure values obtained by noninvasive methods must always be regarded cautiously. Oscillometric blood pressure measurements tend to be less accurate or the measuring devices regularly cease to function during hypotension and peripheral vasoconstriction (especially in small patients <5 kg bodyweight). The Doppler technique, in principle, only indicates systolic pressure; in cats the Doppler technique underestimates true systolic pressure and tends to be more closely related to mean blood pressure. Central venous pressure Central venous pressure (CVP) represents the balance between the filling of the central venous reservoir and the pumping ability of the heart. CVP is measured in the vena cava within the thoracic cavity via a long intravenous catheter. The classical approach is to position the catheter, via the jugular vein, in the thoracic portion of the cranial vena cava. Alternatively, the femoral or saphenous approach can be used to position the catheter in the thoracic portion of the caudal vena cava. CVP can be measured using the technique described for invasive arterial blood pressure. The zero reference point is the level of the right atrium. Landmarks are the manubrium (in lateral recumbency) and the scapulohumeral joint (in patients in dorsal recumbency). Instead of electronic transducers, a cheap saline manometer is often used (Figure 7.21). Set-up for CVP 7.21 measurement. Note that the zero point on the saline manometer is set at the level of the manubrium in the laterally recumbent patient. cm H2O 74

15 A change of CVP over a short time period, in the absence of a changed fluid load suggests changes in cardiac function. A low or falling CVP suggests the presence of hypovolaemia. High or rising CVP can be due to fluid overload or to failing heart function. The administration of a fluid bolus, which is followed by a transient rise in CVP, suggests hypovolaemia but adequate cardiac function. Subsequent fluid therapy can be guided by CVP control. CVP can be a valuable aid in differentiating low arterial blood pressure due to hypovolaemia from low arterial blood pressure due to heart failure. The normal range is quite variable (3 8 cmh 2 O), so single values have limited meaning. Conversely, repetitive measurements and determination of trends provide valuable information. CVP measurement is not a routine procedure during anaesthesia. In many cases, CVP measurement may have already begun before anaesthesia. It is of particular use in critical patients who need extensive and prolonged fluid therapy and/or are being treated for haemodynamic instability. During intermittent positive pressure ventilation (IPPV), CVP is influenced by the elevated intrathoracic pressure, especially when positive end-expiratory pressure is used, and CVP measurements have to be corrected accordingly. Electrocardiography The electrocardiogram (ECG) was the first monitoring to be made compulsory in human medicine and it may be the most frequently used monitor in veterinary anaesthesia. In veterinary practice, the three electrode system is almost exclusively used: the electrical activity of the heart is measured between two electrodes, with the third electrode acting as the ground electrode. They are normally located on left and right forelimbs and the left hindlimb. Perfect electrical contact with the skin is essential to obtain reliable and prolonged ECG tracings. This contact can be achieved with adhesive electrode patches, crocodile clips or transcutaneous needles. In general, electrode gel is recommended to improve electrical contact and is preferred to alcohol; the latter tends to evaporate and the associated loss of electrical contact can be the cause of artefacts. Placing adhesive electrode patches on the skin necessitates shaving, but this can be avoided when they are attached to the pads of the paws. Patches can be reused when fixed with self-adhesive bandage. A normal ECG trace is shown in Figure The three-electrode system is effective for arrhythmia analysis, but in human medicine is considered insufficient for detection of myocardial ischaemia (analysis of the ST segment). When the surgical site does not allow normal electrode placement, a base apex derivation can be used: one electrode is placed dorsal to the base of the heart, another ventrally near the apex and the third peripherally. Transoesophageal ECG, using a special oesophageal probe or stethoscope equipped with ECG electrodes, is also a very convenient method of monitoring cardiac rhythm. The ECG: Provides information limited to electrical activity of the heart. It does not provide any information about pumping function and haemodynamic consequences. An extreme example is electromechanical dissociation, where the ECG remains normal but the heart is not beating Allows quick diagnosis of the type of cardiac arrest (asystole, ventricular fibrillation, electromechanical dissociation) and is the only way to detect and analyse any other arrhythmias. Examples of common ECG abnormalities during anaesthesia are shown in Figure Common causes of artefacts in ECG monitoring are poor electrical contact of the electrodes (insufficient gel, dirty crocodile clips), detachment of electrodes, 50/60 Hz interference, electrical interference from electrosurgical devices and movement of the patient. R 7.22 Normal ECG. P T Q S 75

16 7.23 Abnormal ECGs, with normal ECG trace superimposed in grey. (a) Ventricular extrasystole. (b) Atrioventricular block, second degree. (a) P P (b) Respiratory monitoring Respiratory rate counters One type of respiratory rate monitor uses a connector attached to the end of the endotracheal tube. This connector is equipped with a thermistor, which detects the movement of respiratory gases (expired gas is warmer than inspired gas). These monitors can emit an audible tone synchronous with the detection of movement of gas. They can also display the time in seconds since the last breath, or the respiratory frequency. They produce an alarm in case of apnoea ( apnoea detector ). However, the respiratory rate displayed should not be used as a safe indicator of the efficiency of ventilation, because no information is provided about tidal volume. A normal displayed respiratory rate, and even tachypnoea, can be associated with hypoventilation. In addition, if instrument sensitivity is not properly adjusted, it is possible for these monitors to produce artefactual acoustic signals and display erroneous information. Airway pressure gauges It is highly desirable to have an airway pressure gauge (Figure 7.24) in an anaesthetic breathing system. This is a simple mechanical aneroid (or Bourdon-type) manometer with a scale varying from 10 to +100 cmh 2 O. This instrument helps the performance of a pre-anaesthetic quantitative leak test of the anaesthetic machine and breathing system. The monitoring of the typical pressure cycles of IPPV will serve as a guide during manual ventilation and for adjustment of automatic ventilators. The absence of pressure swings indicates major leaks or disconnection of patient and anaesthetic apparatus. Airway pressure monitoring will detect dangerously high airway pressure, e.g. due to maladjustment of ventilator settings or when the exhaust valve remains inadvertently closed during spontaneous ventilation. If the delivered tidal volume is known, the ratio of tidal volume to airway pressure is an indicator of compliance of the respiratory system when IPPV is applied. Moreover, the level of positive end-expiratory pressure can be checked. 76

17 7.24 Airway pressure gauge. Spirometers A simple method to evaluate the efficiency of ventilation is the use of a mechanical respirometer (Figure 7.25). This instrument measures the volume of expired gases and is often fixed in the expiratory limb of a breathing system. Alternatively, it can be connected directly to an endotracheal tube or facemask. A respirometer indicates tidal volume and thus the minute volume must be calculated using a stopwatch. Some respirometers have a built-in timer and automatically display the minute volume (minute volume (MV) is the product of respiratory rate (RR) per minute and tidal volume (V t ) of the patient (MV = V t x RR/minute)) Spirometer. Electronic spirometers exist in different forms for both research and clinical purposes and are based on different physical principles. However, they are expensive and rarely found in veterinary practice. Some devices do not provide any more information than the mechanical spirometer. Spirometry is reliable and shows whether or not ventilation is within acceptable limits (minute volume ml/kg/minute, tidal volume 7 15 ml/kg). However, acceptable values for ventilation are not necessarily associated with acceptable gas exchange; because the contribution of deadspace volume (about one third in normal circumstances) remains unknown, the alveolar part of the minute volume (which determines P a CO 2 ) remains speculative. In this respect, capnometry and blood gas analysis are most useful. Some spirometers allow advanced monitoring of ventilation because they use physical principles that permit measurement of respiratory flow and airway pressure, calculate compliance of the respiratory system, and provide graphic presentation of the pressure flow and pressure volume relationships in the form of loops. Oxygen analyser The measurement of oxygen concentration in inspired gas (F i O 2 ) is compulsory in human anaesthesia. When several gases are used (oxygen, nitrous oxide, air), monitoring of the inspired oxygen fraction is a basic method to prevent delivery of a hypoxic gas mixture and hypoxaemia. The measurement of F i O 2 also allows safe use of low-flow anaesthesia techniques (see Chapter 5). This measurement is often included in respiratory gas analysis performed by multiparameter anaesthetic monitors and different physical principles are used. A popular simple stand-alone device is based on a chemical reaction in a fuel cell. The lifespan of this relatively costly cell is limited and depends on the amount and time of oxygen measurement. A minimum of 30% oxygen in the inspired gas should be provided during anaesthesia of healthy patients. Temperature monitoring The continuous measurement of body temperature is performed by a thermistor or a thermocouple mounted on an appropriate probe. The probe can be placed in the oesophagus, nasopharynx or rectum. Perioperative monitoring of body temperature is important to detect hypothermia, which commonly develops during anaesthesia. Among other reasons, this is due to depression of hypothalamic thermoregulation and heat loss from surgical exposure of body cavities. Hypothermia leads to reduced cellular metabolism, decreased anaesthetic requirements (danger of overdosage), delayed recovery, bradycardia and increased morbidity. It is important to take preventive measures, such as insulation of the surgical table, use of a circulating warm water mattress, warm blankets and heating pads. However, if not well controlled, there is a potential risk of inducing iatrogenic hyperthermia. Hyperthermia is also seen occasionally during low-flow anaesthesia in a warm environment, and during sepsis and malignant hyperthermia. Inhalational anaesthetic agent monitoring Monitors that continuously measure the concentration of inhaled anaesthetic agents in the breathing system are available. In many of these devices, infrared analysis is used, and is often combined with the measurement of oxygen and carbon dioxide. Measurement allows control of the dosage of volatile agent administered to the patient and correlation of this with its clinical effects. The principle is that alveolar (end-tidal) concentration of an agent reflects its arterial and cerebral concentration; this value can be compared with the documented minimum alveolar concentration (MAC) value of the agent (see Chapter 14). However, a very large number of factors influence MAC value (e.g. individual variation, sedative and analgesic drugs) and measured values are indicative of the dosage of the agent but not of the depth of anaesthesia. Clinical examination remains the key factor in the assessment of anaesthetic depth. 77
 is the product of respiratory rate (RR) per minute and tidal volume (V t ) of the patient (MV")
18 If properly calibrated, these monitors can be used to check the accuracy of the output of vaporizers. In this case, it is imperative that sampling be done at the outlet of the vaporizer and not in the breathing system. Monitoring depth of anaesthesia In clinical veterinary anaesthesia, the most accurate method to assess the depth of anaesthesia is based on collection and interpretation of relevant clinical parameters (see Figure 7.3). The use of neuromuscular-blocking agents as part of a balanced anaesthesia protocol eliminates many of these important clinical parameters (see Chapter 15). In human medicine, this has occasionally led to difficulties in estimation of anaesthetic depth, resulting in awareness during anaesthesia, or undesired recall afterwards. For this reason, there is an increased use in human clinical practice of electronic devices to evaluate depth of anaesthesia. These devices are based on computerized analysis of the electroencephalogram (EEG) (bispectral analysis) or EEG reaction to auditory stimulation (middle latency auditory evoked potentials). In veterinary anaesthesia, this kind of monitoring is reserved for research purposes. Monitoring of the neuromuscular junction For information on monitoring of the neuromuscular junction, see Chapter 15. Additional monitoring When a urinary catheter is in place, the urine output can easily be measured by collecting the urine in a bag (normal 1 2 ml/kg/h). A normal urine output reflects correct cardiovascular status and normal renal perfusion. Renal perfusion can be reduced due to cardiovascular failure, hypovolaemia and shock (see Chapter 23). Urine output is part of the fluid balance evaluation comparing fluid input during anaesthesia (intravenous infusions) and fluid losses (blood, urine, transudates). In some circumstances, the perioperative monitoring of blood glucose concentration (e.g. anaesthesia of diabetic patients and those with insulinoma) or electrolytes, haematocrit and total protein (unstable critical patients with emergency surgery) may be necessary. Guidelines for monitoring strategy in veterinary anaesthesia When organizing and purchasing anaesthetic monitoring equipment, there are several factors to bear in mind: Staff numbers and qualifications Costs versus benefits Case load and nature of those cases The anaesthetic techniques used The need to monitor several cases simultaneously The need for post-anaesthetic monitoring. The choice of which monitoring equipment to buy depends on: The organization of the practice: if nobody is available to monitor anaesthesia, more equipment will be necessary to alert the surgeon, but this method has clear limits. It is far preferable to have a trained person to monitor anaesthesia, rather than rely exclusively on the use of electronic monitors. It cannot be overemphasized that the purchase and use of monitors is of no use if: Clinical monitoring is not mastered Artefactual information cannot be identified The physiological meaning of the information provided is not understood and the right corrective steps cannot consequently be undertaken. Adequate training of staff is therefore of utmost importance, and the practice must be organized in a way that allows someone with adequate training to assess anaesthetized patients on a regular basis The budget: cost of the equipment is a limiting factor. Also, to invest in expensive monitoring equipment which is not properly understood (and whose information cannot be correctly interpreted) will be of no use in either improving quality of anaesthetic management or reducing the incidence of anaesthetic mishaps Patient condition (ASA status): patients with increased anaesthetic risk will require more complete monitoring of their vital functions so that rapid detection of abnormalities is possible and correct assessment and therapeutic decisions can be made quickly The chosen anaesthetic technique: Capnography in non-intubated patients is difficult, whereas pulse oximetry can be used High doses of alpha-2 agonists in intubated patients may increase the likelihood of unreliable pulse oximeter function, but capnography will still be reliable When nitrous oxide is used, or when using low-flow techniques, there is a potential risk of administration of a hypoxic gas mixture. In this case, the use of an oxygen analyser in the breathing system and/or a pulse oximeter is recommended (S p O 2 ) The case load and the types of surgery or diagnostic examinations: it is not obligatory to use all available monitoring equipment for very short and simple procedures on healthy patients. A pulse oximeter in non-intubated patients or a capnograph in intubated patients can suffice. Generally, the greater the disturbance in homeostasis that is anticipated, the greater the number of physiological functions that must be monitored. Invasive surgery (e.g. thoracotomy), 78
. The use of neuromuscular-blocking agents as part of a balanced anaesthesia protocol eliminates many of these important clinical parameters (see Chapter 15).")
19 or surgery associated with specific pathophysiology or problems (e.g. bleeding) will need appropriate monitoring. For practices performing invasive procedures or dealing with emergency cases and postoperative care, capnography, pulse oximetry, ECG, non-invasive blood pressure measurement (with the option of invasive blood pressure measurement) and temperature monitoring are highly desirable. Nevertheless, regular clinical assessment of depth of anaesthesia remains necessary because no technical device can replace this evaluation (Figure 7.26). Conclusion It is clear that monitoring equipment can never replace a suitably qualified person: it has not been proven that monitoring equipment necessarily decreases anaesthetic risk. As complexity increases, the chances for errors to occur due to artefacts and misinterpretations increase accordingly. The preparation and set-up of monitoring equipment can be timeconsuming and the devices are usually expensive; such considerations could lead one to question the true benefits. One important aspect is that the whole concept of monitoring provides continuous information about the patient, and thus becomes a kind of teacher supporting the person in charge of anaesthesia. This teacher demonstrates the physiological consequences of administered drugs and dosages, and of the complex interactions between anaesthesia, disease and surgical manipulation. In this way one can become a better veterinary surgeon, with more insight into what one is actually doing to the patient. In conclusion, when applied appropriately, operated properly, and interpreted correctly, however, monitors afford the patient the best possible outcome (Lawrence, 2005) Multiparametric monitor and anaesthesia screen. The use of normal anaesthetic and monitoring equipment inside a magnetic resonance unit is not possible. The magnetic field attracts all ferrous metal and electronic functions are disturbed. Special monitoring equipment that can remain inside the room is available, but is very expensive. For respiratory gas analysis, including capnography, a simple alternative solution is to sample via a very long line while the monitor is stationed outside the room. For ECG and pulse oximetry, special sensors are necessary. References and further reading Arbous MD, Grobbee DE, van Kleef JW et al. (2001) Mortality associated with anaesthesia: a qualitative analysis to identify risk factors. Anaesthesia 56, Bhavani-Shankar K (a useful, free, website with animated capnographs) Brodbelt D, Brearley J, Young L, Wood J and Pfeiffer D (2005) Anaesthetic-related mortality risks in small animals in the UK. AVA Spring Meeting, Rimini, Italy April 2005 Lawrence JP (2005) Advances and new insights in monitoring. Thoracic Surgery Clinics 15, Tinker JH, Dull DL, Caplan RA, Ward RJ and Cheney FW (1989) Role of monitoring devices in prevention of anesthetic mishaps: a closed claims analysis. Anesthesiology 71,
.")
CRITICAL CARE MONITORING: WHAT, WHEN, AND HOW? Susan G. Hackner, BVSc.MRCVS.DACVIM.DACVECC.
 CRITICAL CARE MONITORING: WHAT, WHEN, AND HOW? Susan G. Hackner, BVSc.MRCVS.DACVIM.DACVECC. A crucial goal in the critical patient is the maintenance and optimization of cellular (and organ) health. Cellular
CRITICAL CARE MONITORING: WHAT, WHEN, AND HOW? Susan G. Hackner, BVSc.MRCVS.DACVIM.DACVECC. A crucial goal in the critical patient is the maintenance and optimization of cellular (and organ) health. Cellular
Reading Assignment: Tasks for the Veterinary Assistant, pages 467-473, Appendix L, O and P
 Patient Monitoring Reading Assignment: Tasks for the Veterinary Assistant, pages 467-473, Appendix L, O and P Patient monitoring during surgery is an extremely important task that is commonly the responsibility
Patient Monitoring Reading Assignment: Tasks for the Veterinary Assistant, pages 467-473, Appendix L, O and P Patient monitoring during surgery is an extremely important task that is commonly the responsibility
Section Two: Arterial Pressure Monitoring
 Section Two: Arterial Pressure Monitoring Indications An arterial line is indicated for blood pressure monitoring for the patient with any medical or surgical condition that compromises cardiac output,
Section Two: Arterial Pressure Monitoring Indications An arterial line is indicated for blood pressure monitoring for the patient with any medical or surgical condition that compromises cardiac output,
RESPONDING TO ANESTHETIC COMPLICATIONS
 RESPONDING TO ANESTHETIC COMPLICATIONS General anesthesia poses minimal risk to most patients when performed by a capable anesthetist using appropriate protocols and proper monitoring. However, it is vitally
RESPONDING TO ANESTHETIC COMPLICATIONS General anesthesia poses minimal risk to most patients when performed by a capable anesthetist using appropriate protocols and proper monitoring. However, it is vitally
Pulmonary Diseases. Lung Disease: Pathophysiology, Medical and Exercise Programming. Overview of Pathophysiology
 Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Oxygenation. Chapter 21. Anatomy and Physiology of Breathing. Anatomy and Physiology of Breathing*
 Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
MONITORING THE ANESTHETIZED PATIENT
 MONITORING THE ANESTHETIZED PATIENT The administration and monitoring of anesthesia for surgical procedures is a complex and multifaceted skill that requires both knowledge and practice. The safety of
MONITORING THE ANESTHETIZED PATIENT The administration and monitoring of anesthesia for surgical procedures is a complex and multifaceted skill that requires both knowledge and practice. The safety of
Indirect Blood Pressure Measurement
 P r o c e d u r e s P r o C A R D I O L O G Y Peer Reviewed Indirect Blood Pressure Measurement Maintenance of appropriate systemic arterial blood pressure is vital for survival. Because many common situations
P r o c e d u r e s P r o C A R D I O L O G Y Peer Reviewed Indirect Blood Pressure Measurement Maintenance of appropriate systemic arterial blood pressure is vital for survival. Because many common situations
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new?
- is anything new?") Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Laerdal Patient Monitor Help Page 1 June 14, 2012, Rev E
 Laerdal Patient Monitor Help Page 1 Using the Laerdal Patient Monitor The Laerdal Patient Monitor software is used to simulate a typical Patient Monitor found in hospitals and ambulances. It is made available
Laerdal Patient Monitor Help Page 1 Using the Laerdal Patient Monitor The Laerdal Patient Monitor software is used to simulate a typical Patient Monitor found in hospitals and ambulances. It is made available
Levels of Critical Care for Adult Patients
 LEVELS OF CARE 1 Levels of Critical Care for Adult Patients STANDARDS AND GUIDELINES LEVELS OF CARE 2 Intensive Care Society 2009 All rights reserved. No reproduction, copy or transmission of this publication
LEVELS OF CARE 1 Levels of Critical Care for Adult Patients STANDARDS AND GUIDELINES LEVELS OF CARE 2 Intensive Care Society 2009 All rights reserved. No reproduction, copy or transmission of this publication
Emergency Fluid Therapy in Companion Animals
 Emergency Fluid Therapy in Companion Animals Paul Pitney BVSc paul.pitney@tafensw.edu.au The administration of appropriate types and quantities of intravenous fluids is the cornerstone of emergency therapy
Emergency Fluid Therapy in Companion Animals Paul Pitney BVSc paul.pitney@tafensw.edu.au The administration of appropriate types and quantities of intravenous fluids is the cornerstone of emergency therapy
Acute heart failure may be de novo or it may be a decompensation of chronic heart failure.
 Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
TRANSPORT OF CRITICALLY ILL PATIENTS
 TRANSPORT OF CRITICALLY ILL PATIENTS Introduction Inter-hospital and intra-hospital transport of critically ill patients places the patient at risk of adverse events and increased morbidity and mortality.
TRANSPORT OF CRITICALLY ILL PATIENTS Introduction Inter-hospital and intra-hospital transport of critically ill patients places the patient at risk of adverse events and increased morbidity and mortality.
How To Treat A Heart Attack
 13 Resuscitation and preparation for anaesthesia and surgery Key Points 13.1 MANAGEMENT OF EMERGENCIES AND CARDIOPULMONARY RESUSCITATION ESSENTIAL HEALTH TECHNOLOGIES The emergency measures that are familiar
13 Resuscitation and preparation for anaesthesia and surgery Key Points 13.1 MANAGEMENT OF EMERGENCIES AND CARDIOPULMONARY RESUSCITATION ESSENTIAL HEALTH TECHNOLOGIES The emergency measures that are familiar
Oxygenation and Oxygen Therapy Michael Billow, D.O.
 Oxygenation and Oxygen Therapy Michael Billow, D.O. The delivery of oxygen to all body tissues is the essence of critical care. Patients in respiratory distress/failure come easily to mind as the ones
Oxygenation and Oxygen Therapy Michael Billow, D.O. The delivery of oxygen to all body tissues is the essence of critical care. Patients in respiratory distress/failure come easily to mind as the ones
3100B Clinical Training Program. 3100B HFOV VIASYS Healthcare
 3100B Clinical Training Program 3100B HFOV VIASYS Healthcare HFOV at Alveolar Level Nieman,, G, SUNY 1999 Who DO We Treat? Only Pathology studied to date has been ARDS Questions about management of adults
3100B Clinical Training Program 3100B HFOV VIASYS Healthcare HFOV at Alveolar Level Nieman,, G, SUNY 1999 Who DO We Treat? Only Pathology studied to date has been ARDS Questions about management of adults
Target groups: Paramedics, nurses, respiratory therapists, physicians, and others who manage respiratory emergencies.
 Overview Estimated scenario time: 10 15 minutes Estimated debriefing time: 10 minutes Target groups: Paramedics, nurses, respiratory therapists, physicians, and others who manage respiratory emergencies.
Overview Estimated scenario time: 10 15 minutes Estimated debriefing time: 10 minutes Target groups: Paramedics, nurses, respiratory therapists, physicians, and others who manage respiratory emergencies.
NORTH WALES CRITICAL CARE NETWORK
 NORTH WALES CRITICAL CARE NETWORK LEVELS OF CRITICAL CARE FOR ADULT PATIENTS Throughout the work of the North Wales Critical Care Network reference to Levels of Care for the critically ill are frequently
NORTH WALES CRITICAL CARE NETWORK LEVELS OF CRITICAL CARE FOR ADULT PATIENTS Throughout the work of the North Wales Critical Care Network reference to Levels of Care for the critically ill are frequently
AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN 82 055 042 852 RECOMMENDATIONS FOR THE POST-ANAESTHESIA RECOVERY ROOM
 Review PS4 (2006) AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN 82 055 042 852 RECOMMENDATIONS FOR THE POST-ANAESTHESIA RECOVERY ROOM 1. INTRODUCTION A well-planned, well-equipped, well-staffed
Review PS4 (2006) AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN 82 055 042 852 RECOMMENDATIONS FOR THE POST-ANAESTHESIA RECOVERY ROOM 1. INTRODUCTION A well-planned, well-equipped, well-staffed
Medical Direction and Practices Board WHITE PAPER
 Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
Section Four: Pulmonary Artery Waveform Interpretation
 Section Four: Pulmonary Artery Waveform Interpretation All hemodynamic pressures and waveforms are generated by pressure changes in the heart caused by myocardial contraction (systole) and relaxation/filling
Section Four: Pulmonary Artery Waveform Interpretation All hemodynamic pressures and waveforms are generated by pressure changes in the heart caused by myocardial contraction (systole) and relaxation/filling
PULMONARY PHYSIOLOGY
 I. Lung volumes PULMONARY PHYSIOLOGY American College of Surgeons SCC Review Course Christopher P. Michetti, MD, FACS and Forrest O. Moore, MD, FACS A. Tidal volume (TV) is the volume of air entering and
I. Lung volumes PULMONARY PHYSIOLOGY American College of Surgeons SCC Review Course Christopher P. Michetti, MD, FACS and Forrest O. Moore, MD, FACS A. Tidal volume (TV) is the volume of air entering and
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
Understanding Anesthetic Delivery Systems Dean Knoll, CVT, VTS (Anes.) Anesthesia Technician Supervisor University of Wisconsin Madison, WI May 2003
 Anesthesia Technician Supervisor University of Wisconsin Madison, WI May 2003") Understanding Anesthetic Delivery Systems Dean Knoll, CVT, VTS (Anes.) Anesthesia Technician Supervisor University of Wisconsin Madison, WI May 2003 Knowing the functions of the anesthetic delivery system
Understanding Anesthetic Delivery Systems Dean Knoll, CVT, VTS (Anes.) Anesthesia Technician Supervisor University of Wisconsin Madison, WI May 2003 Knowing the functions of the anesthetic delivery system
Introduction to Cardiopulmonary Exercise Testing
 Introduction to Cardiopulmonary Exercise Testing 2 nd Edition Andrew M. Luks, MD Robb Glenny, MD H. Thomas Robertson, MD Division of Pulmonary and Critical Care Medicine University of Washington Section
Introduction to Cardiopulmonary Exercise Testing 2 nd Edition Andrew M. Luks, MD Robb Glenny, MD H. Thomas Robertson, MD Division of Pulmonary and Critical Care Medicine University of Washington Section
Ventilation Perfusion Relationships
 Ventilation Perfusion Relationships VENTILATION PERFUSION RATIO Ideally, each alveolus in the lungs would receive the same amount of ventilation and pulmonary capillary blood flow (perfusion). In reality,
Ventilation Perfusion Relationships VENTILATION PERFUSION RATIO Ideally, each alveolus in the lungs would receive the same amount of ventilation and pulmonary capillary blood flow (perfusion). In reality,
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
MEASURING AND RECORDING BLOOD PRESSURE
 MEASURING AND RECORDING BLOOD PRESSURE INTRODUCTION The blood pressure, along with the body temperature, pulse, and respirations, is one of the vital signs. These measurements are used to quickly, easily,
MEASURING AND RECORDING BLOOD PRESSURE INTRODUCTION The blood pressure, along with the body temperature, pulse, and respirations, is one of the vital signs. These measurements are used to quickly, easily,
ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC. BLS Changes
 ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC CPR Chest compressions, Airway, Breathing (C-A-B) BLS Changes New Old Rationale New science indicates the following order:
ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC CPR Chest compressions, Airway, Breathing (C-A-B) BLS Changes New Old Rationale New science indicates the following order:
Guidelines for Standards of Care for Patients with Acute Respiratory Failure on Mechanical Ventilatory Support
 Guidelines for Standards of Care for Patients with Acute Respiratory Failure on Mechanical Ventilatory Support Copyright by the SOCIETY OF CRITICAL CARE MEDICINE These guidelines can also be found in the
Guidelines for Standards of Care for Patients with Acute Respiratory Failure on Mechanical Ventilatory Support Copyright by the SOCIETY OF CRITICAL CARE MEDICINE These guidelines can also be found in the
Hemodynamic Monitoring: Principles to Practice M. L. Cheatham, MD, FACS, FCCM
 SUMMARY HEMODYNAMIC MONITORING: FROM PRINCIPLES TO PRACTICE Michael L. Cheatham, MD, FACS, FCCM Director, Surgical Intensive Care Units Orlando Regional Medical Center Orlando, Florida Fluid-filled catheters
SUMMARY HEMODYNAMIC MONITORING: FROM PRINCIPLES TO PRACTICE Michael L. Cheatham, MD, FACS, FCCM Director, Surgical Intensive Care Units Orlando Regional Medical Center Orlando, Florida Fluid-filled catheters
Edwards FloTrac Sensor & Edwards Vigileo Monitor. Understanding Stroke Volume Variation and Its Clinical Application
 Edwards FloTrac Sensor & Edwards Vigileo Monitor Understanding Stroke Volume Variation and Its Clinical Application 1 Topics System Configuration Pulsus Paradoxes Reversed Pulsus Paradoxus What is Stroke
Edwards FloTrac Sensor & Edwards Vigileo Monitor Understanding Stroke Volume Variation and Its Clinical Application 1 Topics System Configuration Pulsus Paradoxes Reversed Pulsus Paradoxus What is Stroke
MECHINICAL VENTILATION S. Kache, MD
 MECHINICAL VENTILATION S. Kache, MD Spontaneous respiration vs. Mechanical ventilation Natural spontaneous ventilation occurs when the respiratory muscles, diaphragm and intercostal muscles pull on the
MECHINICAL VENTILATION S. Kache, MD Spontaneous respiration vs. Mechanical ventilation Natural spontaneous ventilation occurs when the respiratory muscles, diaphragm and intercostal muscles pull on the
Vtial sign #1: PULSE. Vital Signs: Assessment and Interpretation. Factors that influence pulse rate: Importance of Vital Signs
 Vital Signs: Assessment and Interpretation Elma I. LeDoux, MD, FACP, FACC Associate Professor of Medicine Vtial sign #1: PULSE Reflects heart rate (resting 60-90/min) Should be strong and regular Use 2
Vital Signs: Assessment and Interpretation Elma I. LeDoux, MD, FACP, FACC Associate Professor of Medicine Vtial sign #1: PULSE Reflects heart rate (resting 60-90/min) Should be strong and regular Use 2
Chapter 16. Learning Objectives. Learning Objectives 9/11/2012. Shock. Explain difference between compensated and uncompensated shock
 Chapter 16 Shock Learning Objectives Explain difference between compensated and uncompensated shock Differentiate among 5 causes and types of shock: Hypovolemic Cardiogenic Neurogenic Septic Anaphylactic
Chapter 16 Shock Learning Objectives Explain difference between compensated and uncompensated shock Differentiate among 5 causes and types of shock: Hypovolemic Cardiogenic Neurogenic Septic Anaphylactic
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy
 The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
Artificial Ventilation Theory into practice
 Artificial Ventilation Theory into practice Keith Simpson BVSc MRCVS MIET(Electronics) www.vetronic.co.uk ksimpson@vetronic.co.uk June 13 th 2014 Today we will discuss the administration of IPPV to anaesthetised
Artificial Ventilation Theory into practice Keith Simpson BVSc MRCVS MIET(Electronics) www.vetronic.co.uk ksimpson@vetronic.co.uk June 13 th 2014 Today we will discuss the administration of IPPV to anaesthetised
Cardiac Arrest VF/Pulseless VT Learning Station Checklist
 Cardiac Arrest VF/Pulseless VT Learning Station Checklist VF/VT 00 American Heart Association Adult Cardiac Arrest Shout for Help/Activate Emergency Response Epinephrine every - min Amiodarone Start CPR
Cardiac Arrest VF/Pulseless VT Learning Station Checklist VF/VT 00 American Heart Association Adult Cardiac Arrest Shout for Help/Activate Emergency Response Epinephrine every - min Amiodarone Start CPR
Measuring central venous pressure
 Elaine Cole Senior lecturer ED/Trauma, City University Barts and the London NHS Trust 1 Learning outcomes That the clinician can: Describe the sites of central venous catheterisation Understand why central
Elaine Cole Senior lecturer ED/Trauma, City University Barts and the London NHS Trust 1 Learning outcomes That the clinician can: Describe the sites of central venous catheterisation Understand why central
Recommendations: Other Supportive Therapy of Severe Sepsis*
 Recommendations: Other Supportive Therapy of Severe Sepsis* K. Blood Product Administration 1. Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as myocardial
Recommendations: Other Supportive Therapy of Severe Sepsis* K. Blood Product Administration 1. Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as myocardial
1.4.4 Oxyhemoglobin desaturation
 Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Clinical Monitoring Title: Monitoring of Patients Undergoing Conscious Sedation Policy #: 09 Revised: 05/00 1.0 DESCRIPTION
Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Clinical Monitoring Title: Monitoring of Patients Undergoing Conscious Sedation Policy #: 09 Revised: 05/00 1.0 DESCRIPTION
GRADE 11F: Biology 3. UNIT 11FB.3 9 hours. Human gas exchange system and health. Resources. About this unit. Previous learning.
 GRADE 11F: Biology 3 Human gas exchange system and health UNIT 11FB.3 9 hours About this unit This unit is the third of six units on biology for Grade 11 foundation. The unit is designed to guide your
GRADE 11F: Biology 3 Human gas exchange system and health UNIT 11FB.3 9 hours About this unit This unit is the third of six units on biology for Grade 11 foundation. The unit is designed to guide your
ETCO2 Monitoring: Riding the Wave! Disclosure 4/11/2013
 ETCO2 Monitoring: Riding the Wave! Debbie Fox, MBA, RRT-NPS, FAARC Director, Respiratory Care Wesley Medical Center Disclosure I have no financial conflicts to disclose. I have participated in focus groups
ETCO2 Monitoring: Riding the Wave! Debbie Fox, MBA, RRT-NPS, FAARC Director, Respiratory Care Wesley Medical Center Disclosure I have no financial conflicts to disclose. I have participated in focus groups
A COMPARISON OF THE COST OF INHALATIONAL ANAESTHESIA USING VARIOUS BREATHING SYSTEMS: IMPLICATIONS FOR THE DEVELOPNG WORLD
 A COMPARISON OF THE COST OF INHALATIONAL ANAESTHESIA USING VARIOUS BREATHING SYSTEMS: IMPLICATIONS FOR THE DEVELOPNG WORLD MATTHEW DRAKE, SPECIALITY REGISTRAR, GLOUCESTERSHIRE ROYAL HOSPITAL INTRODUCTION
A COMPARISON OF THE COST OF INHALATIONAL ANAESTHESIA USING VARIOUS BREATHING SYSTEMS: IMPLICATIONS FOR THE DEVELOPNG WORLD MATTHEW DRAKE, SPECIALITY REGISTRAR, GLOUCESTERSHIRE ROYAL HOSPITAL INTRODUCTION
Scope and Standards for Nurse Anesthesia Practice
 Scope and Standards for Nurse Anesthesia Practice Copyright 2013 222 South Prospect Ave. Park Ridge, IL 60068 www.aana.com Scope and Standards for Nurse Anesthesia Practice The AANA Scope and Standards
Scope and Standards for Nurse Anesthesia Practice Copyright 2013 222 South Prospect Ave. Park Ridge, IL 60068 www.aana.com Scope and Standards for Nurse Anesthesia Practice The AANA Scope and Standards
Cerebral blood flow (CBF) is dependent on a number of factors that can broadly be divided into:
 is dependent on a number of factors that can broadly be divided into:") Cerebral Blood Flow and Intracranial Pressure Dr Lisa Hill, SpR Anaesthesia, Royal Oldham Hospital, UK. Email lambpie10@hotmail.com Dr Carl Gwinnutt, Consultant Neuroanaesthetist, Hope Hospital, UK. The
Cerebral Blood Flow and Intracranial Pressure Dr Lisa Hill, SpR Anaesthesia, Royal Oldham Hospital, UK. Email lambpie10@hotmail.com Dr Carl Gwinnutt, Consultant Neuroanaesthetist, Hope Hospital, UK. The
STAGES OF SHOCK. IRREVERSIBLE SHOCK Heart deteriorates until it can no longer pump and death occurs.
 STAGES OF SHOCK SHOCK : A profound disturbance of circulation and metabolism, which leads to inadequate perfusion of all organs which are needed to maintain life. COMPENSATED NONPROGRESSIVE SHOCK 30 sec
STAGES OF SHOCK SHOCK : A profound disturbance of circulation and metabolism, which leads to inadequate perfusion of all organs which are needed to maintain life. COMPENSATED NONPROGRESSIVE SHOCK 30 sec
10 Things Every Paramedic Should Know About Capnography
 10 Things Every Paramedic Should Know About Capnography Capnography is the vital sign of ventilation. By tracking the carbon dioxide in a patient s exhaled breath, capnography enables paramedics to objectively
10 Things Every Paramedic Should Know About Capnography Capnography is the vital sign of ventilation. By tracking the carbon dioxide in a patient s exhaled breath, capnography enables paramedics to objectively
Emergency Medical Services Advanced Level Competency Checklist
 Emergency Services Advanced Level Competency Checklist EMS Service: Current License in State of Nebraska: # (Copy of license kept in file at station) Date of joining EMS Service: EMS Service Member Name:
Emergency Services Advanced Level Competency Checklist EMS Service: Current License in State of Nebraska: # (Copy of license kept in file at station) Date of joining EMS Service: EMS Service Member Name:
404 Section 5 Shock and Resuscitation. Scene Size-up. Primary Assessment. History Taking
 404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
Functions of Blood System. Blood Cells
 Functions of Blood System Transport: to and from tissue cells Nutrients to cells: amino acids, glucose, vitamins, minerals, lipids (as lipoproteins). Oxygen: by red blood corpuscles (oxyhaemoglobin - 4
Functions of Blood System Transport: to and from tissue cells Nutrients to cells: amino acids, glucose, vitamins, minerals, lipids (as lipoproteins). Oxygen: by red blood corpuscles (oxyhaemoglobin - 4
Capnography. McHenry Western Lake County EMS
 Capnography McHenry Western Lake County EMS What is Capnography? Capnography is an objective measurement of exhaled CO2 levels. Capnography measures ventilation. It can be used to: Assist in confirmation
Capnography McHenry Western Lake County EMS What is Capnography? Capnography is an objective measurement of exhaled CO2 levels. Capnography measures ventilation. It can be used to: Assist in confirmation
F.E.E.A. FONDATION EUROPEENNE D'ENSEIGNEMENT EN ANESTHESIOLOGIE FOUNDATION FOR EUROPEAN EDUCATION IN ANAESTHESIOLOGY
 créée sous le Patronage de l'union Européenne Detailed plan of the program of six courses 1. RESPIRATORY 1. ESPIRATORY AND THORAX 1.1 Physics and principles of measurement 1.1.1 Physical laws 1.1.2 Vaporizers
créée sous le Patronage de l'union Européenne Detailed plan of the program of six courses 1. RESPIRATORY 1. ESPIRATORY AND THORAX 1.1 Physics and principles of measurement 1.1.1 Physical laws 1.1.2 Vaporizers
GE Healthcare. Avance Carestation. Innovating with you, shaping exceptional care
 GE Healthcare Avance Carestation Innovating with you, shaping exceptional care Clinician inspired perioperative solutions GE s Avance Carestation was developed using an approach to perioperative solutions
GE Healthcare Avance Carestation Innovating with you, shaping exceptional care Clinician inspired perioperative solutions GE s Avance Carestation was developed using an approach to perioperative solutions
Circulatory System Review
 Circulatory System Review 1. Draw a table to describe the similarities and differences between arteries and veins? Anatomy Direction of blood flow: Oxygen concentration: Arteries Thick, elastic smooth
Circulatory System Review 1. Draw a table to describe the similarities and differences between arteries and veins? Anatomy Direction of blood flow: Oxygen concentration: Arteries Thick, elastic smooth
CH CONSCIOUS SEDATION
 Summary: CH CONSCIOUS SEDATION It is the policy of Carondelet Health that moderate conscious sedation of patients will be undertaken with appropriate evaluation and monitoring. Effective Date: 9/4/04 Revision
Summary: CH CONSCIOUS SEDATION It is the policy of Carondelet Health that moderate conscious sedation of patients will be undertaken with appropriate evaluation and monitoring. Effective Date: 9/4/04 Revision
Arterial pressure monitoring Direct arterial pressure monitoring permits continuous measurement of systolic, diastolic, and mean pressures and allows
 Arterial pressure monitoring Direct arterial pressure monitoring permits continuous measurement of systolic, diastolic, and mean pressures and allows arterial blood sampling. Because direct measurement
Arterial pressure monitoring Direct arterial pressure monitoring permits continuous measurement of systolic, diastolic, and mean pressures and allows arterial blood sampling. Because direct measurement
Evaluation copy. Blood Pressure. Project PROJECT DESIGN REQUIREMENTS
 Blood Pressure Project 9 Blood pressure is a measure of the fluid pressure within the circulatory system. This pressure is required to ensure the delivery of oxygen and nutrients to, and the removal of
Blood Pressure Project 9 Blood pressure is a measure of the fluid pressure within the circulatory system. This pressure is required to ensure the delivery of oxygen and nutrients to, and the removal of
Respiratory failure and Oxygen Therapy
 Respiratory failure and Oxygen Therapy A patient with Hb 15 G % will carry 3X more O2 in his blood than someone with Hb 5G % Give Controlled O2 treatment in acute pulmonary oedema to avoid CO2 retention
Respiratory failure and Oxygen Therapy A patient with Hb 15 G % will carry 3X more O2 in his blood than someone with Hb 5G % Give Controlled O2 treatment in acute pulmonary oedema to avoid CO2 retention
The Anesthesia Ventilator
 The Anesthesia Ventilator Why is the piston replacing the bellows? For many decades, and millions of anesthetics, the bellows anesthesia ventilator has been a safe and effective clinical device. Indeed,
The Anesthesia Ventilator Why is the piston replacing the bellows? For many decades, and millions of anesthetics, the bellows anesthesia ventilator has been a safe and effective clinical device. Indeed,
Scope and Standards for Nurse Anesthesia Practice
 Scope and Standards for Nurse Anesthesia Practice Copyright 2010 222 South Prospect Ave. Park Ridge, IL 60068 www.aana.com Scope and Standards for Nurse Anesthesia Practice The AANA Scope and Standards
Scope and Standards for Nurse Anesthesia Practice Copyright 2010 222 South Prospect Ave. Park Ridge, IL 60068 www.aana.com Scope and Standards for Nurse Anesthesia Practice The AANA Scope and Standards
Paediatric Intensive Care Unit Nursing Procedure: Care of Arterial Lines.
 Paediatric Intensive Care Unit Nursing Procedure: Care of Arterial Lines. Definition: Arterial Line Placement of an indwelling arterial catheter for the purpose of continuous monitoring of intra arterial
Paediatric Intensive Care Unit Nursing Procedure: Care of Arterial Lines. Definition: Arterial Line Placement of an indwelling arterial catheter for the purpose of continuous monitoring of intra arterial
Nursing Education and Research
 Melissa Meloche Meloche, RN RN, MSN MSN, CCRN Nursing Education and Research Describe the purpose p of common clinical equipment found in the Intensive Care Unit and how this equipment could impact a patient
Melissa Meloche Meloche, RN RN, MSN MSN, CCRN Nursing Education and Research Describe the purpose p of common clinical equipment found in the Intensive Care Unit and how this equipment could impact a patient
Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when
 Chapter 4 2 71 Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when they fly. Air medical escorts need to understand what causes hypoxia, why some people are more likely
Chapter 4 2 71 Hypoxia and Oxygenation Hypoxia is a serious threat to patients and escorts alike when they fly. Air medical escorts need to understand what causes hypoxia, why some people are more likely
Sensors / Modules / Monitors. Breath Gas Sensing and Monitoring. For life supporting systems in intensive, emergency and ambulant care
 Sensors / Modules / Monitors Breath Gas Sensing and Monitoring For life supporting systems in intensive, emergency and ambulant care Your competent partner for breath gas sensing and monitoring EnviteC
Sensors / Modules / Monitors Breath Gas Sensing and Monitoring For life supporting systems in intensive, emergency and ambulant care Your competent partner for breath gas sensing and monitoring EnviteC
TRANSPORT OF BLOOD GASES From The Lungs To The Tissues & Back
 TRANSPORT OF BLOOD GASES From The Lungs To The Tissues & Back Dr. Sally Osborne Department of Cellular & Physiological Sciences University of British Columbia Room 3602, D.H Copp Building 604 822-3421
TRANSPORT OF BLOOD GASES From The Lungs To The Tissues & Back Dr. Sally Osborne Department of Cellular & Physiological Sciences University of British Columbia Room 3602, D.H Copp Building 604 822-3421
240- PROBLEM SET INSERTION OF SWAN-GANZ SYSTEMIC VASCULAR RESISTANCE. Blood pressure = f(cardiac output and peripheral resistance)
") 240- PROBLEM SET INSERTION OF SWAN-GANZ 50 kg Pig Rt Jugular 0 cm Rt Atrium 10 cm Rt ventricle 15 cm Wedge 20-25 cm SYSTEMIC VASCULAR RESISTANCE Blood pressure = f(cardiac output and peripheral resistance)
240- PROBLEM SET INSERTION OF SWAN-GANZ 50 kg Pig Rt Jugular 0 cm Rt Atrium 10 cm Rt ventricle 15 cm Wedge 20-25 cm SYSTEMIC VASCULAR RESISTANCE Blood pressure = f(cardiac output and peripheral resistance)
Eileen Whitehead 2010 East Lancashire HC NHS Trust
 Eileen Whitehead 2010 East Lancashire HC NHS Trust 1 Introduction: Arterial blood gas analysis is an essential part of diagnosing and managing a patient s oxygenation status and acid-base balance However,
Eileen Whitehead 2010 East Lancashire HC NHS Trust 1 Introduction: Arterial blood gas analysis is an essential part of diagnosing and managing a patient s oxygenation status and acid-base balance However,
*Reflex withdrawal from a painful stimulus is NOT considered a purposeful response.
 Analgesia and Moderate Sedation This Nebraska Board of Nursing advisory opinion is issued in accordance with Nebraska Revised Statute (NRS) 71-1,132.11(2). As such, this advisory opinion is for informational
Analgesia and Moderate Sedation This Nebraska Board of Nursing advisory opinion is issued in accordance with Nebraska Revised Statute (NRS) 71-1,132.11(2). As such, this advisory opinion is for informational
What, roughly, is the dividing line between the upper and lower respiratory tract? The larynx. What s the difference between the conducting zone and
 What, roughly, is the dividing line between the upper and lower respiratory tract? The larynx. What s the difference between the conducting zone and the respiratory zone? Conducting zone is passageways
What, roughly, is the dividing line between the upper and lower respiratory tract? The larynx. What s the difference between the conducting zone and the respiratory zone? Conducting zone is passageways
NRP 2012 Putting New Resuscitation Guidelines into Practice
 Outreach Education Online Video Library for Healthcare Professionals NRP 2012 Putting New Resuscitation Guidelines into Practice. Jeanette Zaichkin, RN, MN, NNP-BC December 2, 2010 Program Handouts This
Outreach Education Online Video Library for Healthcare Professionals NRP 2012 Putting New Resuscitation Guidelines into Practice. Jeanette Zaichkin, RN, MN, NNP-BC December 2, 2010 Program Handouts This
Enhancements on SCP-ECG protocol for multi vital-sign handling
 Enhancements on SCP-ECG protocol for multi vital-sign handling G. MANDELLOS, G. KOUTELAKIS, G. TRIANTAFYLLOU, M. KOUKIAS, D. LYMPEROPOULOS Wire Communication Lab, Electrical & Computer Engineering Dept.,
Enhancements on SCP-ECG protocol for multi vital-sign handling G. MANDELLOS, G. KOUTELAKIS, G. TRIANTAFYLLOU, M. KOUKIAS, D. LYMPEROPOULOS Wire Communication Lab, Electrical & Computer Engineering Dept.,
Electrocardiography I Laboratory
 Introduction The body relies on the heart to circulate blood throughout the body. The heart is responsible for pumping oxygenated blood from the lungs out to the body through the arteries and also circulating
Introduction The body relies on the heart to circulate blood throughout the body. The heart is responsible for pumping oxygenated blood from the lungs out to the body through the arteries and also circulating
Enables MDA Medical Teams to categorize victims in mass casualty scenarios, in order to be able to triage and treat casualties
 MDA Disposable ALS + BLS Medical Ambulance Equipment Prices shown in CDN. Funds Items Description Picture Mass Casualty ID tag 1000 units = $350 Enables MDA Medical Teams to categorize victims in mass
MDA Disposable ALS + BLS Medical Ambulance Equipment Prices shown in CDN. Funds Items Description Picture Mass Casualty ID tag 1000 units = $350 Enables MDA Medical Teams to categorize victims in mass
Pulse Oximetry. Principles of oximetry
 Pulse Oximetry The principal advantage of optical sensors for medical applications is their intrinsic safety since there is no electrical contact between the patient and the equipment. (An added bonus
Pulse Oximetry The principal advantage of optical sensors for medical applications is their intrinsic safety since there is no electrical contact between the patient and the equipment. (An added bonus
UW MEDICINE PATIENT EDUCATION. Aortic Stenosis. What is heart valve disease? What is aortic stenosis?
 UW MEDICINE PATIENT EDUCATION Aortic Stenosis Causes, symptoms, diagnosis, and treatment This handout describes aortic stenosis, a narrowing of the aortic valve in your heart. It also explains how this
UW MEDICINE PATIENT EDUCATION Aortic Stenosis Causes, symptoms, diagnosis, and treatment This handout describes aortic stenosis, a narrowing of the aortic valve in your heart. It also explains how this
Crash Cart Drugs Drugs used in CPR. Dr. Layla Borham Professor of Clinical Pharmacology Umm Al Qura University
 Crash Cart Drugs Drugs used in CPR Dr. Layla Borham Professor of Clinical Pharmacology Umm Al Qura University Introduction A list of the drugs kept in the crash carts. This list has been approved by the
Crash Cart Drugs Drugs used in CPR Dr. Layla Borham Professor of Clinical Pharmacology Umm Al Qura University Introduction A list of the drugs kept in the crash carts. This list has been approved by the
Cardiovascular Physiology
 Cardiovascular Physiology Heart Physiology for the heart to work properly contraction and relaxation of chambers must be coordinated cardiac muscle tissue differs from smooth and skeletal muscle tissues
Cardiovascular Physiology Heart Physiology for the heart to work properly contraction and relaxation of chambers must be coordinated cardiac muscle tissue differs from smooth and skeletal muscle tissues
Veterinary Clinics and Hospitals
 Anesthetic Gases: Guidelines for Workplace Exposure Veterinary Clinics and Hospitals Inhalation anesthesia in veterinary hospitals is practiced in a manner similar to that in human hospitals. Generally,
Anesthetic Gases: Guidelines for Workplace Exposure Veterinary Clinics and Hospitals Inhalation anesthesia in veterinary hospitals is practiced in a manner similar to that in human hospitals. Generally,
Vascular System The heart can be thought of 2 separate pumps from the right ventricle, blood is pumped at a low pressure to the lungs and then back
 Vascular System The heart can be thought of 2 separate pumps from the right ventricle, blood is pumped at a low pressure to the lungs and then back to the left atria from the left ventricle, blood is pumped
Vascular System The heart can be thought of 2 separate pumps from the right ventricle, blood is pumped at a low pressure to the lungs and then back to the left atria from the left ventricle, blood is pumped
Understanding Hypoventilation and Its Treatment by Susan Agrawal
 www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
ACLS PHARMACOLOGY 2011 Guidelines
 ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
Bier Block (Intravenous Regional Anesthesia)
") Bier Block (Intravenous Regional Anesthesia) History August Bier introduced this block in 1908. Early methods included the use of two separate tourniquets and procaine was the local anesthetic of choice.
Bier Block (Intravenous Regional Anesthesia) History August Bier introduced this block in 1908. Early methods included the use of two separate tourniquets and procaine was the local anesthetic of choice.
Common Ventilator Management Issues
 Common Ventilator Management Issues William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center You have just admitted a 28 year-old
Common Ventilator Management Issues William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center You have just admitted a 28 year-old
Pediatric Airway Management
 Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Exercise, the Electrocardiogram, and Peripheral Circulation
 iworx Physiology Lab Experiment Experiment HH-3 Exercise, the Electrocardiogram, and Peripheral Circulation Note: The lab presented here is intended for evaluation purposes only. iworx users should refer
iworx Physiology Lab Experiment Experiment HH-3 Exercise, the Electrocardiogram, and Peripheral Circulation Note: The lab presented here is intended for evaluation purposes only. iworx users should refer
CHAPTER 1: THE LUNGS AND RESPIRATORY SYSTEM
 CHAPTER 1: THE LUNGS AND RESPIRATORY SYSTEM INTRODUCTION Lung cancer affects a life-sustaining system of the body, the respiratory system. The respiratory system is responsible for one of the essential
CHAPTER 1: THE LUNGS AND RESPIRATORY SYSTEM INTRODUCTION Lung cancer affects a life-sustaining system of the body, the respiratory system. The respiratory system is responsible for one of the essential
The centrepiece of a complete anaesthesia workstation
 The centrepiece of a complete anaesthesia workstation IntelliSave AX700 anaesthesia machine A slim design with rich functionality To develop the first Philips-branded anaesthesia machine, we listened to
The centrepiece of a complete anaesthesia workstation IntelliSave AX700 anaesthesia machine A slim design with rich functionality To develop the first Philips-branded anaesthesia machine, we listened to
Guidelines for the Use of Sedation and General Anesthesia by Dentists
 Guidelines for the Use of Sedation and General Anesthesia by Dentists I. Introduction The administration of local anesthesia, sedation and general anesthesia is an integral part of dental practice. The
Guidelines for the Use of Sedation and General Anesthesia by Dentists I. Introduction The administration of local anesthesia, sedation and general anesthesia is an integral part of dental practice. The
CALIFORNIA EMERGENCY MEDICAL SERVICES (EMS) MECHANICAL CIRCULATORY SUPPORT (MCS) DEVICES BEST PRACTICES GUIDELINE
 MECHANICAL CIRCULATORY SUPPORT (MCS) DEVICES BEST PRACTICES GUIDELINE") CALIFORNIA EMERGENCY MEDICAL SERVICES (EMS) MECHANICAL CIRCULATORY SUPPORT (MCS) DEVICES BEST PRACTICES GUIDELINE Purpose: To provide information and direction regarding the care of patients who have a
CALIFORNIA EMERGENCY MEDICAL SERVICES (EMS) MECHANICAL CIRCULATORY SUPPORT (MCS) DEVICES BEST PRACTICES GUIDELINE Purpose: To provide information and direction regarding the care of patients who have a
PROCEDURAL SEDATION/ANALGESIA NCBON Position Statement for RN Practice
 PROCEDURAL SEDATION/ANALGESIA NCBON Position Statement for RN Practice P.O. BOX 2129 Raleigh, NC 27602 (919) 782-3211 FAX (919) 781-9461 Nurse Aide II Registry (919) 782-7499 www.ncbon.com Issue: Administration
PROCEDURAL SEDATION/ANALGESIA NCBON Position Statement for RN Practice P.O. BOX 2129 Raleigh, NC 27602 (919) 782-3211 FAX (919) 781-9461 Nurse Aide II Registry (919) 782-7499 www.ncbon.com Issue: Administration
Direct Arterial Blood Pressure Monitoring Angel M. Rivera CVT, VTS (ECC) Animal Emergency Center Glendale, WI March 2003
 Animal Emergency Center Glendale, WI March 2003") Direct Arterial Blood Pressure Monitoring Angel M. Rivera CVT, VTS (ECC) Animal Emergency Center Glendale, WI March 2003 Introduction Direct measurement of arterial blood pressure is obtained via a peripheral
Direct Arterial Blood Pressure Monitoring Angel M. Rivera CVT, VTS (ECC) Animal Emergency Center Glendale, WI March 2003 Introduction Direct measurement of arterial blood pressure is obtained via a peripheral
(C) AMBULANCE VICTORIA
 AMBULANCE VICTORIA") The Newborn Baby: Definitions and Contacts Newborn definition 'Newborn' refers to the first min to hours post birth. For the purpose of resuscitation, AV accepts up to the first 24 hours from birth in
The Newborn Baby: Definitions and Contacts Newborn definition 'Newborn' refers to the first min to hours post birth. For the purpose of resuscitation, AV accepts up to the first 24 hours from birth in
Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire
 Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire") Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire Date: RPICC Facility: CMS use only Include the following
Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire Date: RPICC Facility: CMS use only Include the following
CAPNOGRAPHY IN EMS. Scott Temple Lake EMS February 2012
 CAPNOGRAPHY IN EMS Scott Temple Lake EMS February 2012 What is the difference Oxygenation vs. Ventilation Oxygenation vs. Ventilation Oxygenation - the ability of the red blood cells to pick up oxygen
CAPNOGRAPHY IN EMS Scott Temple Lake EMS February 2012 What is the difference Oxygenation vs. Ventilation Oxygenation vs. Ventilation Oxygenation - the ability of the red blood cells to pick up oxygen
The heart then repolarises (or refills) in time for the next stimulus and contraction.
 in time for the next stimulus and contraction.") Atrial Fibrillation BRIEFLY, HOW DOES THE HEART PUMP? The heart has four chambers. The upper chambers are called atria. One chamber is called an atrium, and the lower chambers are called ventricles. In
Atrial Fibrillation BRIEFLY, HOW DOES THE HEART PUMP? The heart has four chambers. The upper chambers are called atria. One chamber is called an atrium, and the lower chambers are called ventricles. In
X-Plain Subclavian Inserted Central Catheter (SICC Line) Reference Summary
 Reference Summary") X-Plain Subclavian Inserted Central Catheter (SICC Line) Reference Summary Introduction A Subclavian Inserted Central Catheter, or subclavian line, is a long thin hollow tube inserted in a vein under the
X-Plain Subclavian Inserted Central Catheter (SICC Line) Reference Summary Introduction A Subclavian Inserted Central Catheter, or subclavian line, is a long thin hollow tube inserted in a vein under the
Edwards FloTrac Sensor & Edwards Vigileo Monitor. Measuring Continuous Cardiac Output with the FloTrac Sensor and Vigileo Monitor
 Edwards FloTrac Sensor & Edwards Vigileo Monitor Measuring Continuous Cardiac Output with the FloTrac Sensor and Vigileo Monitor 1 Topics System Configuration Physiological Principles Pulse pressure relationship
Edwards FloTrac Sensor & Edwards Vigileo Monitor Measuring Continuous Cardiac Output with the FloTrac Sensor and Vigileo Monitor 1 Topics System Configuration Physiological Principles Pulse pressure relationship
Critical Care Therapy and Respiratory Care Section
 Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Special Procedures Title: Transport of Critically Ill Patients Policy #: 05 Revised: 04/00 1.0 DESCRIPTION 1.1 Definition:
Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Special Procedures Title: Transport of Critically Ill Patients Policy #: 05 Revised: 04/00 1.0 DESCRIPTION 1.1 Definition: