MARYLAND MEDICAID (MA) BILLING INSTRUCTIONS HCFA 1500
|
|
|
- Myra Webster
- 8 years ago
- Views:
Transcription
1 MARYLAND MEDICAID (MA) BILLING INSTRUCTIONS HCFA 1500 THIS FORMAT IS USED FOR: DIALYSIS FACILITY PROVIDERS DURABLE MEDICAL EQUIPMENT/DISPOSABLE MEDICAL SUPPLIES EMERGENCY AMBULANCE SERVICES FREE STANDING SURGICAL CENTERS MEDICAL LABORATORY SERVICES MEDICARE/MEDICAL ASSISTANCE CROSSOVER CLAIMS PHYSICAL THERAPY SERVICES PHYSICIAN SERVICES PODIATRY SERVICES PORTABLE X-RAY AND OTHER DIAGNOSTIC SERVICES VISION CARE SERVICES Basic Rules:! Always use the HCFA-1500! Use one claim form for each recipient! Be sure that the information entered on the form is legible! Check for transpositions, especially when entering Provider and Recipient Numbers! Enter information with a Typewriter or Black Ink Before You Begin:! Have you verified through EVS that the recipient is eligible on the date of service?! Is the recipient linked with a Managed Care Organization (MCO)?. If yes, in most instances that organization should be billed.! Is the service or item covered by Medicaid?! Did you obtain preauthorization, if required?! Did you determine if the recipient has other insurance? Revised 12/99 Page 1

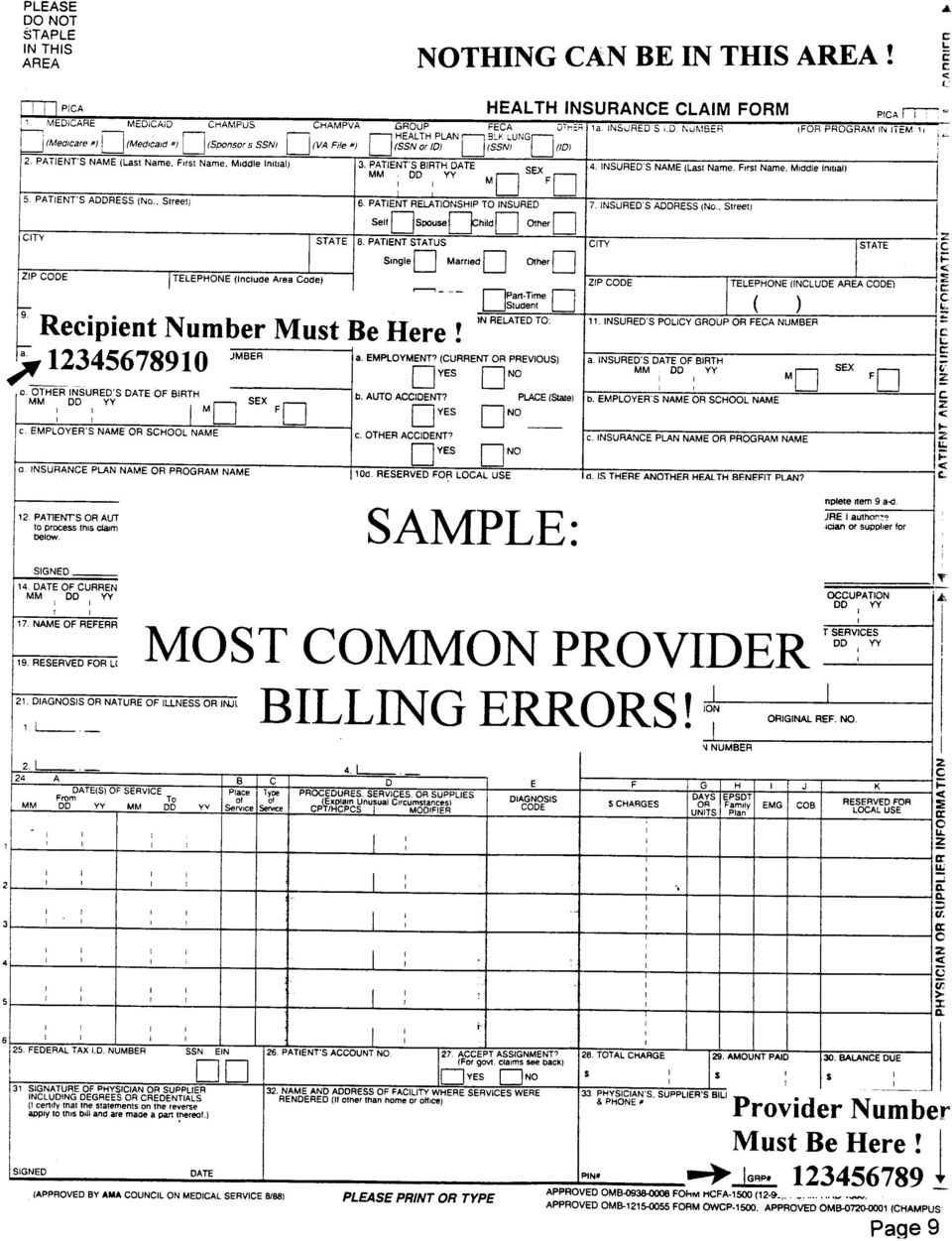
2 PLEASE DO NOT STAPLE IN THIS AREA PICA F HEALTH INSURANCE CLAIM FORM 1. MEDICARE MEDICAID CHAMPUS CHAMPVA GROUP FECA OTHER 1a. INSURED S I.D. NUMBER (FOR PROGRAM IN ITEM 1) HEALTH PLAN BLK LUNG (Medicare #) (Medicaid #) (Sponsor s SSN) (VA File #) (SSN or ID) (SSN) (ID) 2. PATIENT S NAME (Last Name, First Name, Middle Initial) 5. PATIENT S ADDRESS (No., Street) CITY ZIP CODE TELEPHONE (Include Area Code) ( ) 9. OTHER INSURED S NAME (Last Name, First Name, Middle Initial) a. OTHER INSURED S POLICY OR GROUP NUMBER b. OTHER INSURED S DATE OF BIRTH MM DD YY M c. EMPLOYER S NAME OR SCHOOL NAME d. INSURANCE PLAN NAME OR PROGRAM NAME SEX STATE 3. PATIENT S BIRTH DATE MM DD YY M SEX F 6. PATIENT RELATIONSHIP TO INSURED Self Spouse Child Other 8. PATIENT STATUS Single Married Other Employed Full-Time Part-Time Student Student 10. IS PATIENT S CONDITION RELATED TO: a. EMPLOYMENT? (CURRENT OR PREVIOUS) b. AUTO ACCIDENT? c. OTHER ACCIDENT? YES NO YES NO YES NO 10d. RESERVED FOR LOCAL USE PLACE (State) 4. INSURED S NAME (Last Name, First Name, Middle Initial) 7. INSURED S ADDRESS (No., Street) CITY STATE ZIP CODE TELEPHONE (INCLUDE AREA CODE) 11. INSURED S POLICY GROUP OR FECA NUMBER a. INSURED S DATE OF BIRTH MM DD YY b. EMPLOYER S NAME OR SCHOOL NAME c. INSURANCE PLAN NAME OR PROGRAM NAME d. IS THERE ANOTHER HEALTH BENEFIT PLAN? APPROVED OMB ( ) SEX M F PICA CARRIER PATIENT AND INSURED INFORMATION READ BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM. 12. PATIENT S OR AUTHORIZED PERSON S SIGNATURE I authorize the release of any medical or other information necessary to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment below. SIGNED DATE 14. DATE OF CURRENT: MM DD YY ILLNESS (First symptom) OR INJURY (Accident) OR PREGNANCY(LMP) 17. NAME OF REFERRING PHYSICIAN OR OTHER SOURCE 19. RESERVED FOR LOCAL USE 15. IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS. GIVE FIRST DATE MM DD YY 17a. I.D. NUMBER OF REFERRING PHYSICIAN 21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY. (RELATE ITEMS 1,2,3 OR 4 TO ITEM 24E BY LINE) A B C D E DATE(S) OF SERVICE Place Type PROCEDURES, SERVICES, OR SUPPLIES From To DIAGNOSIS of of (Explain Unusual Circumstances) MM DD YY MM DD YY CODE Service Service CPT/HCPCS MODIFIER 25. FEDERAL TAX I.D. NUMBER SSN EIN 26. PATIENT S ACCOUNT NO. 27. ACCEPT ASSIGNMENT? (For govt. claims, see back) YES NO 31. SIGNATURE OF PHYSICIAN OR SUPPLIER INCLUDING DEGREES OR CREDENTIALS (I certify that the statements on the reverse apply to this bill and are made a part thereof.) 32. NAME AND ADDRESS OF FACILITY WHERE SERVICES WERE RENDERED (If other than home or office) YES 13. INSURED S OR AUTHORIZED PERSON S SIGNATURE I authorize payment of medical benefits to the undersigned physician or supplier for services described below. SIGNED NO If yes, return to and complete item 9 a-d. 16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION MM DD YY MM DD YY FROM TO 18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES MM DD YY MM DD YY FROM TO 20. OUTSIDE LAB? $ CHARGES YES NO 22. MEDICAID RESUBMISSION CODE ORIGINAL REF. NO. 23. PRIOR AUTHORIZATION NUMBER F G H I J K DAYS EPSDT RESERVED FOR OR Family $ CHARGES EMG COB LOCAL USE UNITS Plan 28. TOTAL CHARGE 29. AMOUNT PAID 30. BALANCE DUE $ $ $ 33. PHYSICIAN S, SUPPLIER S BILLING NAME, ADDRESS, ZIP CODE & PHONE # PHYSICIAN OR SUPPLIER INFORMATION SIGNED DATE (APPROVED BY AMA COUNCIL ON MEDICAL SERVICE 8/88) PIN# GRP# PLEASE PRINT OR TYPE FORM HCFA-1500 (12-90), FORM RRB-1500, FORM OWCP-1500

3 BECAUSE THIS FORM IS USED BY VARIOUS GOVERNMENT AND PRIVATE HEALTH PROGRAMS, SEE SEPARATE INSTRUCTIONS ISSUED BY APPLICABLE PROGRAMS. NOTICE: Any person who knowingly files a statement of claim containing any misrepresentation or any false, incomplete or misleading information may be guilty of a criminal act punishable under law and may be subject to civil penalties. REFERS TO GOVERNMENT PROGRAMS ONLY MEDICARE AND CHAMPUS PAYMENTS: A patient s signature requests that payment be made and authorizes release of any information necessary to process the claim and certifies that the information provided in Blocks 1 through 12 is true, accurate and complete. In the case of a Medicare claim, the patient s signature authorizes any entity to release to Medicare medical and nonmedical information, including employment status, and whether the person has employer group health insurance, liability, no-fault, worker s compensation or other insurance which is responsible to pay for the services for which the Medicare claim is made. See 42 CFR (a). If item 9 is completed, the patient s signature authorizes release of the information to the health plan or agency shown. In Medicare assigned or CHAMPUS participation cases, the physician agrees to accept the charge determination of the Medicare carrier or CHAMPUS fiscal intermediary as the full charge, and the patient is responsible only for the deductible, coinsurance and noncovered services. Coinsurance and the deductible are based upon the charge determination of the Medicare carrier or CHAMPUS fiscal intermediary if this is less than the charge submitted. CHAMPUS is not a health insurance program but makes payment for health benefits provided through certain affiliations with the Uniformed Services. Information on the patient s sponsor should be provided in those items captioned in Insured ; i.e., items 1a, 4, 6, 7, 9, and 11. BLACK LUNG AND FECA CLAIMS The provider agrees to accept the amount paid by the Government as payment in full. See Black Lung and FECA instructions regarding required procedure and diagnosis coding systems. SIGNATURE OF PHYSICIAN OR SUPPLIER (MEDICARE, CHAMPUS, FECA AND BLACK LUNG) I certify that the services shown on this form were medically indicated and necessary for the health of the patient and were personally furnished by me or were furnished incident to my professional service by my employee under my immediate personal supervision, except as otherwise expressly permitted by Medicare or CHAMPUS regulations. For services to be considered as incident to a physician s professional service, 1) they must be rendered under the physician s immediate personal supervision by his/her employee, 2) they must be an integral, although incidental part of a covered physician s service, 3) they must be of kinds commonly furnished in physician s offices, and 4) the services of nonphysicians must be included on the physician s bills. For CHAMPUS claims, I further certify that I (or any employee) who rendered services am not an active duty member of the Uniformed Services or a civilian employee of the United States Government or a contract employee of the United States Government, either civilian or military (refer to 5 USC 5536). For Black-Lung claims, I further certify that the services performed were for a Black Lung-related disorder. No Part B Medicare benefits may be paid unless this form is received as required by existing law and regulations (42 CFR ). NOTICE: Any one who misrepresents or falsifies essential information to receive payment from Federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable Federal laws. NOTICE TO PATIENT ABOUT THE COLLECTION AND USE OF MEDICARE, CHAMPUS, FECA, AND BLACK LUNG INFORMATION (PRIVACY ACT STATEMENT) We are authorized by HCFA, CHAMPUS and OWCP to ask you for information needed in the administration of the Medicare, CHAMPUS, FECA, and Black Lung programs. Authority to collect information is in section 205(a), 1862, 1872 and 1874 of the Social Security Act as amended, 42 CFR (a) and 424.5(a) (6), and 44 USC 3101;41 CFR 101 et seq and 10 USC 1079 and 1086; 5 USC 8101 et seq; and 30 USC 901 et seq; 38 USC 613; E.O The information we obtain to complete claims under these programs is used to identify you and to determine your eligibility. It is also used to decide if the services and supplies you received are covered by these programs and to insure that proper payment is made. The information may also be given to other providers of services, carriers, intermediaries, medical review boards, health plans, and other organizations or Federal agencies, for the effective administration of Federal provisions that require other third parties payers to pay primary to Federal program, and as otherwise necessary to administer these programs. For example, it may be necessary to disclose information about the benefits you have used to a hospital or doctor. Additional disclosures are made through routine uses for information contained in systems of records. FOR MEDICARE CLAIMS: See the notice modifying system No , titled, Carrier Medicare Claims Record, published in the Federal Register, Vol. 55 No. 177, page 37549, Wed. Sept. 12, 1990, or as updated and republished. FOR OWCP CLAIMS: Department of Labor, Privacy Act of 1974, Republication of Notice of Systems of Records, Federal Register Vol. 55 No. 40, Wed Feb. 28, 1990, See ESA-5, ESA-6, ESA-12, ESA-13, ESA-30, or as updated and republished. FOR CHAMPUS CLAIMS: PRINCIPLE PURPOSE(S): To evaluate eligibility for medical care provided by civilian sources and to issue payment upon establishment of eligibility and determination that the services/supplies received are authorized by law. ROUTINE USE(S): Information from claims and related documents may be given to the Dept. of Veterans Affairs, the Dept. of Health and Human Services and/or the Dept. of Transportation consistent with their statutory administrative responsibilities under CHAMPUS/CHAMPVA; to the Dept. of Justice for representation of the Secretary of Defense in civil actions; to the Internal Revenue Service, private collection agencies, and consumer reporting agencies in connection with recoupment claims; and to Congressional Offices in response to inquiries made at the request of the person to whom a record pertains. Appropriate disclosures may be made to other federal, state, local, foreign government agencies, private business entities, and individual providers of care, on matters relating to entitlement, claims adjudication, fraud, program abuse, utilization review, quality assurance, peer review, program integrity, third-party liability, coordination of benefits, and civil and criminal litigation related to the operation of CHAMPUS. DISCLOSURES: Voluntary; however, failure to provide information will result in delay in payment or may result in denial of claim. With the one exception discussed below, there are no penalties under these programs for refusing to supply information. However, failure to furnish information regarding the medical services rendered or the amount charged would prevent payment of claims under these programs. Failure to furnish any other information, such as name or claim number, would delay payment of the claim. Failure to provide medical information under FECA could be deemed an obstruction. It is mandatory that you tell us if you know that another party is responsible for paying for your treatment. Section 1128B of the Social Security Act and 31 USC provide penalties for withholding this information. You should be aware that P.L , the Computer Matching and Privacy Protection Act of 1988, permits the government to verify information by way of computer matches. MEDICAID PAYMENTS (PROVIDER CERTIFICATION) I hereby agree to keep such records as are necessary to disclose fully the extent of services provided to individuals under the State s Title XIX plan and to furnish information regarding any payments claimed for providing such services as the State Agency or Dept. of Health and Humans Services may request. I further agree to accept, as payment in full, the amount paid by the Medicaid program for those claims submitted for payment under that program, with the exception of authorized deductible, coinsurance, co-payment or similar cost-sharing charge. SIGNATURE OF PHYSICIAN (OR SUPPLIER): I certify that the services listed above were medically indicated and necessary to the health of this patient and were personally furnished by me or my employee under my personal direction. NOTICE: This is to certify that the foregoing information is true, accurate and complete. I understand that payment and satisfaction of this claim will be from Federal and State funds, and that any false claims, statements, or documents, or concealment of a material fact, may be prosecuted under applicable Federal or State laws. Public reporting burden for this collection of information is estimated to average 15 minutes per response, including time for reviewing instructions, searching existing date sources, gathering and maintaining data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing the burden, to HCFA, Office of Financial Management, P.O. Box 26684, Baltimore, MD 21207; and to the Office of Management and Budget, Paperwork Reduction Project (OMB ), Washington, D.C

4 Maryland Medicaid Billing Instructions Step-by-Step Instructions - Use Only HCFA 1500 Block Number Title Action 1 Select a claim type. Show all types of health insurance coverage applicable to this claim by checking the appropriate boxes. 1a Insured=s ID Number Enter the patient=s 10-character Medicare Identification Number from the Medicare Identification Card. 2 Patient=s Name Enter the patient=s name from the Medicaid Identification Card. 3 Patient=s Birth Date Optional Enter the patient=s birth date and use a ΑX to mark the appropriate gender. 4 Insured=s Name Optional If recipient is covered by other insurance, the name of the insured may be placed in this block. If the patient and the insured are the same person, enter ΑSAME. 5 Patient=s Address Optional Enter the patient=s complete mailing & Telephone # address and zip code and the patient=s telephone number. 6 Patient Relationship Optional For patients with third-party health insurance to Insured other than Medicare and Medicaid, mark the appropriate entry with an ΑX. 7 Insured=s Address Optional Enter the insured=s address and telephone & Telephone # number, if applicable. 8 Patient Status No entry required. 9 Other Insured=s No entry required. Name 9a Other Insured=s Enter the patient=s 11-digit MA number as it appears on Policy or Group the MA card. The MA number MUST appear here Number regardless of whether or not a patient has other insurance. The patient=s MA eligibility should be verified on each date of service prior to rendering service by calling the Eligibility Verification System (EVS). EVS also gives information on linkages with Managed Care Organizations (MCOs) Revised 6/99 Page 3

5 Maryland Medicaid Billing Instructions Step-by-Step Instructions - Use Only HCFA 1500 Block Number Title Action 9b Other Insured=s Date No entry required. of Birth 9c Employer=s Name No entry required. or School Name 9d Insurance Plan Name Enter the insured=s group name and group number if or Program Name the patient has health insurance coverage along with Medicare and Medicaid. 10a - 10c Patients Condition Check ΑYes or ΑNo to indicate whether employment, Related To auto liability or other accident involvement applies to any of the services or items provided. 10d Reserved for Local No entry Use 11 Insured=s Policy If the patient has other third party insurance and the Group or FECA claim has been rejected by that insurer, enter the Number appropriate rejection code. Refer to the Maryland Medicaid Value Descriptions (immediately following these instructions) for valid values and their meanings. 11a Insured=s Date of No entry required. Birth 11b Employer=s Name No entry required. or School Name 11c Insurance Plan Name No entry required. or Program Name 11d Is There Another No entry required. Health Benefit Plan? 12 Patient or Authorized No entry required. Person=s Signature 13 Insured=s or No entry required. Authorized Person=s Signature 14 Date of Current No entry required. Illness, Injury, Pregnancy Revised 6/99 Page 4

6 Maryland Medicaid Billing Instructions Step-by-Step Instructions - Use Only HCFA 1500 Block Number Title Action 15 If Patient Has Had No entry required. Same or Similar Illness, Give First Date 16 Dates Patient Unable No entry required. To Work in Current Occupation 17 Name of Referring For services which involve a requesting, referring, Physician or Other ordering, or prescribing practitioner, enter the Source practitioner=s name and degree. (See Addendums for Specific instructions.) 17a I.D. Number of` Enter the MA provider number of the referring Referring Physician provider. (See Addendums for specific instructions) 18 Hospitalization Dates No entry required, Related to Current Services 19 Reserved for Local Enter the MA provider number of the Practitioner Use rendering the service. In some instances, the rendering provider number may be the same as the payee provider number in Block Outside Lab Optional Providers may not bill for laboratory services referred to any other laboratory, practitioner or facility. The laboratory, practitioner or facility must bill MA directly. Medical Laboratory providers are the only exception to this policy. 21 Diagnosis or Enter the 3, 4, or 5 character code from the ICD-9 Nature of related to the procedures, services or supplies listed Illness or in Block 24d. List the primary diagnosis on Line 1 Injury and secondary diagnosis on Line 2. Additional diagnoses are optional and may be listed on lines 3 and Medicaid No entry required. Resubmission Code 23 Prior Authorization For those services which require preauthorization, Number a preauthorization number must be obtained and entered in this block Revised 6/99 Page 5
 17a I.D. Number of` Enter the MA provider number of the referring Referring Physician provider.")
7 Maryland Medicaid Billing Instructions Step-by-Step Instructions - Use Only HCFA 1500 Block Number Title Action 24a Date(s) of Service Enter each separate date of service as a six (6) digit numeric date (e.g. 06/01/99) under the ΑFrom heading. Leave the space under the ΑTo heading blank. Each date of service on which a service was rendered must be listed on a separate line. Ranges of dates are not accepted on this form. 24b Place of Service For each service, enter the appropriate place of service code. Refer to the Maryland Medicaid Value Descriptions (immediately following these instructions) for valid values and their meanings. 24c Type of Service For Physician, Clinic, and Nurse Midwife services only, enter a type of professional code. Refer to the Maryland Medicaid Value Descriptions (immediately following these instructions) for valid values and their meanings. 24d Procedures, Services Enter the five (5) character HCPCS procedure code. or Supplies (For information on use of Modifiers, see Addendum I) 24e Diagnosis Code Enter a single or any combination of diagnosis items (1,2,3,4) from Block 21 above for each line item on the invoice. 24f $ Charges Enter the usual and customary charge. Do not enter the Maryland Medicaid maximum fee unless that amount is your usual and customary charge. If there is more than one unit of service on a line, the charge for that line should be the total for all units. 24g Days or Units Enter the number of units of service for each procedure. The number of units must be for a single visit or day. Multiple, identical services rendered on different days should be billed on separate lines. NOTE: When billing for anesthesia, time is not considered a factor. The units of service for anesthesia may not exceed the number of times a specific procedure was performed on the date given.multiple, identical services for medical,radiological or pathological services, within the CPT code range of through 99999, rendered on the same day must be combined and entered on one line. Revised 7/99 Page 6
 for valid values and their meanings.")
8 Maryland Medicaid Billing Instructions Step-by-Step Instructions - Use Only HCFA 1500 Block Number Title Action 24h EPSDT/Family Plan Enter an ΑE if the service is an Early and Periodic Screening, Diagnosis and Treatment (EPSDT) screen or related to a referral from a screen. Enter an ΑF if the service is known to be related to Family Planning. If neither, leave blank. 24i EMG Enter an ΑX if the service was a medical emergency in an Emergency Room. 24j COB Leave Blank 24k Reserved for Local Leave Blank Use. 25 Federal Tax ID # No entry required. 26 Patient=s Account # No entry required. However, it is recommended that providers place their patient account number or some other information in this field to identify the patient should the patient MA number be incorrect. In that instance, MA will send the information back to you on your Remittance Advice. 27 Accept Assignment? For payment of Medicare coinsurance and/or deductibles, this block must be checked ΑYes. NOTE: Regulations state that providers shall accept payment by the Program as payment in full for covered services rendered and make no additional charge to any recipient for covered services. 28 Total Charges Enter the sum of the charges shown on all lines of Block 24f. 29 Amount Paid Enter the amount of any collections received from any Third Party payor except Medicare. If the patient has third-party insurance and the claim has been rejected, the appropriate rejection code must be entered in Block 11. Collections from patients are not appropriate. 30 Balance Due No entry required. Revised 6/99 Page 7

9 Maryland Medicaid Billing Instructions Step-by-Step Instructions - Use Only HCFA 1500 Block Number Title Action 31 Signature of Physician Optional - A signature is optional, however, or Supplier including a date must be placed in this field in order Degree or Credentials for the claim to be reimbursed. 32 Name and Address If the services were rendered in either a hospital of Facility Where or long term facility, enter the name of the facility Services were followed by the MA provider number associated Rendered with that facility in the lower right corner of this block. NOTE: A list of hospital and long term care facility provider numbers may be found in Addendum O and P of these instructions. 33 Physician=s, Enter the name, street address, city, state and ZIP Suppliers Billing to which claims may be returned. The MA Provider Name, Address, number to which payment is to be made MUST ZIP Code & be entered in the lower right corner of this block Phone # to the IMMEDIATE RIGHT OF THE WORDS GRP. # Errors or omissions of this number will result in non-payment of your claims. NOTE: Please peruse the following page, (Page 9) to assure that you have not made any of the common errors which are made when filing claims to MA. Any of these three errors will result in your claim/claims not being processed. Revised 6/99 Page 8

10
11 MARYLAND MEDICAID VALUE DESCRIPTIONS Field Name Description Value Place of Service Office 11 Patient=s Residence 12 Inpatient Hospital 21 Outpatient Hospital 22 Emergency Room - Hospital 23 Ambulatory Surgical Center 24 Birthing Center 25 Military Treatment Facility 26 Skilled Nursing Facility 31 Nursing Home 32 Custodial Care Facility 33 Hospice 34 Ambulance - Land 41 Ambulance - Air or Water 42 Federally Qualified Health Center 50 Inpatient Psychiatric Facility 51 Psychiatric Facility Partial Hospitalization 52 Community Mental Health Center 53 Intermediate Care Facility/Mentally Retarded 54 Residential Substance Abuse Treatment Center 55 Psychiatric Residential Treatment Center 56 Comprehensive Inpatient Rehabilitation Facility 61 Comprehensive Outpatient Rehabilitation Facility 62 End Stage Renal Disease Treatment Facility 65 State or Local Public Health Clinic 71 Rural Health Clinic 72 Independent Laboratory 81 Other Unlisted Facility 99 Revised 6/99 Page 10

12 MARYLAND MEDICAID VALUE DESCRIPTIONS Field Name Description Value TPL Override Services Not Covered K (Third Party Liability) Coverage Lapsed L Coverage Not In Effect On Service Date M Individual Not Covered N Claims Not Filed Timely Q No Response From Carrier In 90 Days R Other Rejection Reason Not Defined Above S NOTE: Documentation must be attached to claim for values Q, R, or S. Type of Professional Physician (M. D. or D.O.) 01 Registered Nurse (R.N.) 02 Certified Nurse Midwife 03 Certified Psychologist 04 Nurse Practitioner 05 Registered Physician=s Assistant 06 Certified Social Worker 07 Future Use 08 Other 09 Certified Lab Technologist 10 Certified Lab Technician 11 Dentist 12 Podiatrist 13 Nurse Anesthetist 14 Certified Radio Technologist 15 Certified Radio Technician 16 Chiropractor 17 Registered Pulmonary Function Technologist 18 Registered Pulmonary Function Technician 19 Dialysis Technician 20 Revised 6/99 Page 11

13 ADDENDUM A: DIALYSIS FACILITY PROVIDERS ONLY Block 24B - Place of Service Dialysis Facility Providers MUST use Α65" as the place of service for all services provided at the facility. Use the appropriate place of service to describe any site, other than the dialysis facility, where dialysis facility personnel supply services. For example, place of service Α12" would be used to describe any services provided by dialysis facility personnel at the recipient s home. Dialysis Facility Providers cannot bill for ANY service they refer to ANY OTHER provider or that ANY OTHER provider supplies at the facility. That provider must bill MA directly for the service. Refer to ADDENDUM G - MEDICARE/MEDICAL ASSISTANCE CROSSOVER CLAIMS for instructions for billing for Medicare deductible and coinsurance. Revised 6/99 Page 12

14 ADDENDUM B: DMS/DME PROVIDERS (DISPOSABLE MEDICAL SUPPLIES AND DURABLE MEDICAL EQUIPMENT) For disposable medical supplies and durable medical equipment requiring preauthorization, enter the preauthorization approval number given on the computer printout in Block 23 as described in the instructions. It is not necessary to attach the approved Preauthorization Request Form or computer printout to the claim form. One preauthorization number may be assigned for several supplies and/or equipment items if they are requested at the same time for the same recipient. These items should be billed on the same claim form, but listed individually. Use a separate claim form for each different preauthorization approval number. Claims with more than one preauthorization number will be rejected. All information entered on the claim must correspond to the information on the preauthorization computer printout bearing the same approval number. Claims for preauthorized supplies or equipment should be submitted separately from ordinary claims for items with individual procedure codes and fees not requiring preauthorization. When billing for disposable medical supplies, indicate the number of units in Block 24G based on the pricing units stipulated in the Approved List of Items. If the quantity being billed is in terms of packaging units (boxes, packs, bottles, etc.), also indicate the number of individual items contained in the packaging unit. Otherwise, it is assumed that the quantity being billed is the number of individual (single-unit) items. Revised 6/99 Page 13

15 ADDENDUM C: OXYGEN PROVIDERS (OXYGEN AND RELATED RESPIRATORY EQUIPMENT SERVICES) For covered oxygen, oxygen equipment, related respiratory equipment, component replacements, equipment repairs, and tracheostomy items, enter the preauthorization approval number given on the computer printout in Block 23 as described in the instructions. It is not necessary to attach the approved Preauthorization Request Form or computer printout to the claim. One preauthorization number may be assigned for several items if they are requested at the same time for the same recipient. They should be billed on the same claim form, but listed individually. The information entered on the claim must correspond to the information on the preauthorization computer printout bearing the same approval number. Use a separate claim form for each different preauthorization approval number. Claims with more than one preauthorization number will be rejected. Revised 6/99 Page 14

16 ADDENDUM D: EMERGENCY SERVICE TRANSPORTERS ONLY Supplemental Instructions Block 21 - Diagnosis or Nature of Illness or Injury Enter the primary diagnosis in this block. Block 24b - Place of Service Enter the Place of Service Code 41. Block 24d - Procedure Code Enter the five (5) digit HCPCS Procedure Code A0220. Block 24g - Units Reimbursement by the Emergency Service Transporters Program is paid per unit, (or in this case - per trip). Place the Number 1 in Block 24g. Block 24f - Usual and Customary Charge Enter your usual and customary fee in Block 24f. NOTE: Services provided to clients who have Medicare as their primary insurer should be billed to Medicare first. Any coinsurance and/or deductible payable by Medicaid, is covered under COMAR For additional information, refer to Addendum G. Revised 6/99 Page 15

17 ADDENDUM E: FREE-STANDING AMBULATORY SURGICAL CENTERS Reimbursement by the Program is for a facility fee for services provided by a Free- Standing Ambulatory Surgical Center (ASC) in connection with covered surgical procedure. In order to bill the Program the facility must obtain a Maryland Medicaid provider number. The facility fee must be billed separately from the physician bills. Maryland Medicaid uses the list of covered surgical procedures established by Medicare for ambulatory surgical centers - please refer to that list when determining coverage and for the appropriate group. Medicaid does not pay by CPT Code as does Medicare. Instead, eight W-codes are used to identify eight groups of surgical procedures which can be performed in a Free- Standing Medicare Certified ASC as determined by HCFA. These codes and reimbursement rates are as follows: W Group 1 $ W Group 5 $ W Group 2 $ W Group 6 $ W Group 3 $ W Group 7 $ W Group 4 $ W Group 8 $ Use the ΑW-code directly under the CPT/HCPCS area in Block 24D of the HCFA Each W-code (procedure) represents one unit of service. If one covered surgical procedure is furnished to a recipient, payment is at 100 percent of the determined rate for that procedure. However, if more than one covered surgical procedure is provided to a recipient in a single operative session, payment is made at 100 percent of the determined rate for the procedure with the highest reimbursement. Other covered surgical procedures furnished in the same session are reimbursed at 50 percent of the determined rate for each of those procedures. Example: Units Charge W9013 (Group 3) 1 $ W (Group 2) 1 $ W (Group 1) 1 $ NOTES: Χ Χ Χ Use ΑPlace of Service code Α24" in Block 24B COMAR (C)(F) prohibits services performed by a podiatrist as a covered service. Do not bill for a facility fee for procedures performed by a podiatrist. OPTHALMOLOGY CENTER: Procedure codes for cataract surgery (Group 6 and Group 8) include the cost of IOL=s. Do not bill separately for IOL. Revised 6/99 Page 16

18 ADDENDUM F: MEDICAL LABORATORIES ONLY Supplemental Instructions Block 17 - Name of Referring Physician or Other Source: This field is optional, however, if the ordering practitioner is NOT enrolled with the program, Block 17 must include the full name and degree of that practitioner. Refer to Block 17a, ( highlighted area) for clarification. Block 17a - I.D. Number of Referring Physician: To properly identify the ordering practitioner, enter the MA Individual Practitioner ID Number of the ordering practitioner or, in the case of Physician Assistants, the individual practitioner ID number of their supervising physician. If the ordering practitioner is not enrolled with the Program (and, therefore, does not have an individual practitioner number), the laboratory must still include the full name and degree in Block 17, however, must use five zeroes followed by 5100 ( ) instead of the individual practitioner number, AND ATTACH A COPY OF THE SIGNED ORDER. Invoices containing this number in lieu of an individual practitioner ID number may NOT be billed electronically. The group practice number of a physician group or clinic cannot be used as an individual practitioner ID number. If this is done, it will automatically cause the claim to error. It is the responsibility of the medical laboratory provider to verify the individual practitioner number of each and every practitioner from whom orders are accepted. FAILURE TO ENTER THE INDIVIDUAL PRACTITIONER ID NUMBER OF THE ORDERING PRACTITIONER OR ATTACH THE SIGNED ORDER MAY RESULT IN ONE OF THE FOLLOWING: RETURN OF THE CLAIM FOR PROPER COMPLETION, DENIAL OF PAYMENT, OR RECOVERY OF PAYMENTS, IF DISCOVERED AS A RESULT OF POST PAYMENT REVIEW. RECOVERY ALSO EXTENDS TO ANY PAYMENTS MADE FOR ELECTRONIC SUBMISSION THAT REFLECT AS THE INDIVIDUAL PRACTITIONER NUMBER, OR CLAIMS WHICH LACK A VALID NUMBER. Revised 6/99 Page 17

19 ADDENDUM F - Continued Block 24B - Place of Service Medical laboratories MUST use Α81" as the place of service for all medical laboratory services except specimen collection as the ΑMedical Laboratory is where the procedure was performed. Use the appropriate place of service to describe the site of the specimen collection, only if the specimen was collected by the medical laboratory (i.e. code 36415). For example, place of service Α12" would be used to describe any specimen obtained (venipuncture) or procedure performed (bleeding time) at the recipient=s home. Block 24D - Procedures, Services or Supplies The ONLY modifiers required and recognized by the Program for medical laboratory providers are the reference laboratory modifier Α90", the technical component modifier ΑTC, and ΑQW for providers with waived CLIA status. No others are authorized at this time. Block 24F - Charges When billing for referred laboratory tests, the medical laboratory provider MUST BILL THE EXACT AMOUNT PAID to the reference laboratory. No mark up is allowed and any handling fee must be included in the cost of the test. The recipient may not be billed for any charges associated with specimen referral. Block 32 - Name and Address of Facility Where Services Were Rendered Complete only if billing for medical laboratory services referred to another laboratory. Enter the name and MA identification number of the reference laboratory to which the medical laboratory services were referred. The reference laboratory must be enrolled with the MA Program and supply its ID number to the referring laboratory. THE PROGRAM WILL NOT PAY A REFERRING LABORATORY FOR MEDICAL LABORATORY SERVICES REFERRED TO A REFERENCE LABORATORY THAT IS NOT ENROLLED. THE REFERRING LABORATORY ALSO AGREES NOT TO BILL THE RECIPIENT FOR MEDICAL LABORATORY SERVICES REFERRED TO AN UNENROLLED REFERENCE LABORATORY. Revised 6/99 Page 18

20 ADDENDUM G: MEDICARE/MEDICAL ASSISTANCE CROSSOVER CLAIMS When a Maryland Medical Assistance provider bills Medicare Part B for services rendered to a Medical Assistance recipient, and the provider accepts assignment on the claim, Maryland Medical Assistance pays the provider the Medicare coinsurance and/or deductible amount(s) in full less any other third party payments (i.e., Medigap). The payments are generally made automatically for providers using Trailblazers (Blue Cross/Blue Shield, Texas) or Administar Federal (Blue Cross/Blue Shield, Indianapolis) as their Medicare carrier. If not paid automatically within six (6) weeks of receipt of the Medicare payment, it is recommended that the provider bill Αhardcopy. The following explanations of both automatic crossover billing and hardcopy crossover billing may prove useful: Automatic: All billing conditions must be met in accordance with the requirements of the Medicare carrier in order to use the automatic crossover system. An example of these requirements is: When billing Medicare on the form HCFA-1500, place the words ΑMMA (Maryland Medical Assistance) and the recipient=s 11 digit identification number in Block 9a and mark Accept Assignment in Block 27. Hardcopy: Make a copy of the completed form HCFA-1500 used to bill Medicare, or if unavailable, generate a new one. This copy should be an exact copy of the information shown on the Medicare EOMB except for Medicare non-allowed charges. If Medicare has changed your original claim, the HCFA-1500's which you submit to MA must be completed to reflect that change. Make certain that Blocks 1, 9a, and 33 are completed as MA requires. Please make sure to check both Medicare and Medicaid in Block 1 of the HCFA-1500 Form. Failure to appropriately mark both blocks will only delay any payments due. BOTH THE HCFA 1500 AND THE MEDICARE EOMB MUST BE SENT TO MA IN ORDER FOR MA TO REIMBURSE FOR CO-PAYS AND/OR DEDUCTIBLES. They should be sent to the same address as other claims: Maryland Medical Assistance P.O. Box 1935 Baltimore, MD Revised 6/99 Page 19
 weeks of receipt of the Medicare payment, it is recommended that the provider bill Αhardcopy.")
21 Addendum G - Continued Note: Please be sure to advise the Administrative Support/Utilization Review (AS/UR) Section of your Medicare provider number so that claims may be accurately cross-referenced to your Medicaid Provider number. The AS/UR Section maintains a file to cross-reference the Medicare provider number with the appropriate Medicaid provider number. In order for a provider to receive Medicare coinsurance and deductible amounts automatically from Medical Assistance, the Medicare Crossover file must contain the provider=s current Medicare and Medical Assistance provider numbers. Requests to add, change or delete information on the Medicare crossover file must be sent in writing to: Medical Care Operations Administration AS/UR Section P.O. Box 1935 Baltimore, MD Revised 6/99 Page 20
22 ADDENDUM H: PHYSICAL THERAPY BILLING INFORMATION In billing Physical Therapy Services under the MA Physical Therapy Program, please be advised that payment is made on a per visit (office/home) basis rather than on a per treatment basis. That is, regardless of the number of treatments rendered to a patient during a visit, the Program should be billed for either an office or home visit. Exceptions to this are the performance of nerve conduction velocity or latency studies and electromyographies as these items have separate procedure codes for billing purposes. Revised 6/99 Page 21
23 ADDENDUM I: PHYSICIANS= SERVICES PROVIDERS ONLY - MODIFIERS A modifier provides the means by which the reporting physician can indicate that a service or procedure that has been performed has been altered by some circumstance but not changed in its definition or code. When applicable, the modifying circumstance should be identified by the appropriate modifier code, which is a two-digit number suffixed to the procedure code in Block 24D of the HCFA Only one modifier may be used for each procedure code per line on the HCFA MA only recognizes the following four modifiers for Physicians= Services billing: 26 Professional Component Use Modifier Α26" to indicate that you are billing for only the professional component applicable for a radiology (CPT Codes ) service. NOTE: This modifier is not to be used with physician visit/service CPT Codes in the series, except for, procedures when used to report hospital outpatient visits and for immunization administration of vaccines/toxoids or immune globulin covered under the Vaccines for Children Program. Certain procedures (e.g., radiology, electrocardiogram, specific diagnostic services) may be a combination of a physician professional component and a technical component. When the physician component is reported separately, the service must be identified by adding the modifier Α26" to the usual procedure number. The maximum fees listed for radiology services are composed of two parts, a professional component and a technical component. The Program will reimburse a provider for both components (i.e., 100% of the maximum reimbursement) when the technical component is not billed by a health care facility. When a test is performed by a laboratory or another physician, interpretation of the results is not considered a separate billable item. The interpretation is considered to be part of the physician visit. 30 Anesthesia Service The provider who administers the anesthesia must use the modifier Α30" with the applicable surgical or medical procedure code. CPT anesthesia codes are not used by the Program, except for procedure codes 00857, 00955, and Revised 12/00 Page 22
24 ADDENDUM I - Continued Codes for the listing of anesthesia services are the same as those for surgical procedures and are found in the Surgery section (CPT codes ). Anesthesia services are reported by adding the modifier code Α30" to the surgical procedure code. Payment for anesthesia services includes the usual preoperative and postoperative visits, the administration of the anesthetic, the administration of fluids and/or blood and the usual monitoring services. The units of service for anesthesia invoices may not exceed the number of times a specific procedure was performed on the date given. Time is not considered a factor when billing for anesthesia. The maximum reimbursement for anesthesia services is 30% of the listed fee for the surgical procedure. The minimum allowance is $ This modifier should be used only the the anesthesiologist and not by the surgeon. 50 Multiple or Bilateral Procedures Use Modifier Α50 when multiple or bilateral surgical procedures (CPT codes ) are provided at the same operative session. The major procedure should be reported without a modifier. Use the modifier for the second and subsequent procedures. The Program will pay up to the amount listed in the fee schedule for the procedure without the modifier and up to 50% of the amount in the fee schedule for the procedures with the code A50" modifier. NOTE: When a procedure has a code for both a single procedure and for each additional procedure, use the procedure code for the second and subsequent procedures and add the code modifier Α50". When only one procedure code is available, regardless of the number of procedures performed, use the same procedure code with the modifier Α50" to report the second and subsequent procedures of that type. Bilateral Procedures When there is no procedure code to identify bilateral procedures, use the code for a unilateral procedure plus the same code with a modifier Α50" to identify that the service was provided bilaterally. Do not charge separately for component or related procedures which are part of the major procedure. Codes for such procedures are listed for those occasions when they are performed as a Αseparate procedure. Revised 12/00 Page 23
25 ADDENDUM I - Continued 80 Assistant Surgeon Use modifier Α80" with the applicable surgical procedure code (CPT codes ) to indicate the services of a physician acting as surgical assistance. Maximum payment is 20% of the listed fee for the procedure. The minimum allowance is $ THE ASSISTANT SURGEON MUST BE A PHYSICIAN who is an enrolled Medical Assistance provider. This modifier should only be used for the assistant surgeon. Revised 12/00 Page 23-1
26 ADDENDUM J: HEALTHY START PROGRAM - PHYSICIAN OR NURSE MIDWIFE SERVICES Office-based Physicians and certified nurse-midwives interested in providing the following prenatal care services should contact the Maryland Healthy Start Program at (410) Maryland Prenatal Risk Assessment - Plan of Care The Prenatal Risk Assessment - Plan of Care is billed on a standard HCFA 1500 claim form, in conjunction with the initial prenatal visit. The physician or certified nursemidwife will be reimbursed an additional $40. Each Prenatal Risk Assessment Form must be submitted to the patient=s local health department regardless of risk status. One unit of service will be reimbursed for each pregnancy. Procedure Code: W9090. The purpose of the Maryland Prenatal Risk Assessment Form is twofold: (1) to identify prenatal clients who may benefit from community health nursing services and other support services; and (2) to identify prenatal clients at risk for delivering preterm low birthweight babies so that increased surveillance and intervention may be considered. While clinical judgement is necessary in assessing prenatal risk, the physician or certified nurse-midwife may delegate responsibility for completing the Maryland Prenatal Risk Assessment Form to others under his/her supervision, utilizing the clinical record to complete the form. The form should be completely filled out, signed, and the top two (2) copies submitted to the Local Health Department within 10 days of the initial visit. Directions for completion and mailing addresses are on the back of the form. Enriched Maternity Service Enriched Maternity Services must be performed by or under the supervision of a primary prenatal care provider. An Enriched Maternity Service is billed on a standard HCFA-1500 claim form in conjunction with each prenatal and postpartum office visit (up to 60 days after delivery). The physician or certified nurse-midwife will be reimbursed $10 for the provision of Enriched Maternity Service in addition to the standard office visit. Procedure Code W9091. Revised 6/99 Page 24
27 ADDENDUM K: MARYLAND HEALTHY KIDS/EPSDT PROGRAM CERTIFIED PROVIDERS The Maryland Healthy Kids/EPSDT Program is open to all Medical Assistance eligibles under the age of 21 years throughout the State. The Program provides a special package of preventive screening and treatment services through private medical doctors, freestanding clinics, nurse practitioners, Local Health Departments, MCOs, and other eligible Medicaid enrolled providers, such as School Based Health Centers. Healthy Kids/EPSDT Billing Codes The Healthy Kids/EPSDT Program will continue to bill on a standard HCFA-1500 claim form. The provider has the option to bill one of the following procedure codes: W9075 Completed Initial Screen (New Patient) W9077 Completed Periodic Screen W9078 Interperiodic Partial Screen OR , Preventive Medicine, New , Preventive Medicine, Established All claims for Healthy Kids/EPDST services are to be submitted within 60 days from the date of service. This allows the State to track identified referable conditions to ensure that children receive needed health care services. In conjunction with these screen procedure codes, the provider may bill additional codes at certain age intervals. Some of the codes that may be billed when providers utilize objective tests approved by the Healthy Kids Program include: Administration and Medical Interpretation of Developmental Tests (for non-standardized or limited in scope) Standardized Developmental Testing and Interpretation (includes motor, language, social, adaptive and cognitive functioning) Hearing Screen W0609 Vision Screen In addition, other procedures commonly billed in conjunction with a Healthy Kids/EPSDT examination (such as laboratory tests completed in the provider=s office and immunizations) are reimbursed at the current fee schedule. For more information, call Revised 9/99 Page 25
28 Addendum K: Maryland Healthy Kids/EPSDT Program Certified Providers (Continued) On April 1, 1990, services offered by the EPSDT/Healthy Kids Program were expanded to include the following: Audiology & Hearing Aids Case Management Chiropractic Care Dental Care Durable Medical Equipment & Supplies not normally covered under Medicaid Health-related Services in Schools such as phychological testing and mental health Inpatient and Outpatient Alcohol-Drug Treatment Medical Day Care for Medically Fragile Children Nutrition Counseling Occupational Therapy Speech/Language Therapy Vision Care & Eye Glasses These services are in addition to the services already offered to adults including physician=s services, pharmacy, mental health, laboratory, radiology and home health services. A referral for a fee-for-service expanded EPSDT service requires the complete name, degree and nine digit Medical Assistance billing number of the primary care provider in order for the specialty provider to be paid. An optional or universal referral form can be obtained from the Healthy Kids Program to facilitate referrals to specialty providers. If you have questions about expanded EPSDT services, call the Healthy Kids Program Staff Specialist at When making a referral for specialty care for an enrolled MCO eligible recipient, the MCO guidelines for referral must be followed. Revised 6/99 Page 26
29 ADDENDUM L: AUDIOLOGICAL EVALUATION CENTERS AND HEARING AID DEALERS (AUDIOLOGY SERVICES- EPSDT) For audiological diagnostic and hearing aid services requiring preauthorization, enter the preauthorization approval number given on the computer printout in Block 23 as described in the instructions. It is not necessary to attach the approved Preauthorization Request Form, computer printout, or other documents to the claim form. One preauthorization number may be assigned for several items if they are requested at the same time for the same recipient. They should be billed on the same claim form, but listed individually. Use a separate claim form for each different preauthorization approval number. Claims with more than one preauthorization number will be rejected. Information entered on the claim must correspond to the information on the preauthorization computer printout bearing the same approval number. Claims for preauthorized services should be submitted separately from claims for services not requiring preauthorization. Revised 6/99 Page 27
Chapter 5. Billing on the CMS 1500 Claim Form
 Chapter 5 Billing on the CMS 1500 Claim Form This Page Intentionally Left Blank Fee-For-Service Provider Manual April 2012 Billing on the UB-04 Claim Form Chapter: 5 Page: 5-2 INTRODUCTION The CMS 1500
Chapter 5 Billing on the CMS 1500 Claim Form This Page Intentionally Left Blank Fee-For-Service Provider Manual April 2012 Billing on the UB-04 Claim Form Chapter: 5 Page: 5-2 INTRODUCTION The CMS 1500
Chapter 8 Billing on the CMS 1500 Claim Form
 8 Billing on the CMS 1500 Claim form INTRODUCTION The CMS 1500 claim form is used to bill for non-facility services, including professional services, freestanding surgery centers, transportation, durable
8 Billing on the CMS 1500 Claim form INTRODUCTION The CMS 1500 claim form is used to bill for non-facility services, including professional services, freestanding surgery centers, transportation, durable
HOW TO SUBMIT OWCP - 1500 BILLS TO ACS
 HOW TO SUBMIT OWCP - 1500 BILLS TO ACS The services performed by the following providers should be billed on the OWCP-1500 Form: Physicians (MD, DO) Radiologists Independent Laboratories Audiologists/Speech
HOW TO SUBMIT OWCP - 1500 BILLS TO ACS The services performed by the following providers should be billed on the OWCP-1500 Form: Physicians (MD, DO) Radiologists Independent Laboratories Audiologists/Speech
professional billing module
 professional billing module Professional CMS-1500 Billing Module Coding Requirements...2 Evaluation and Management Services...2 Diagnosis...2 Procedures...2 Basic Rules...3 Before You Begin...3 Modifiers...3
professional billing module Professional CMS-1500 Billing Module Coding Requirements...2 Evaluation and Management Services...2 Diagnosis...2 Procedures...2 Basic Rules...3 Before You Begin...3 Modifiers...3
Domestic Accident & Health Division 80 Pine Street, 13 th Floor New York, NY 10005
 Domestic Accident & Health Division 80 Pine Street, 13 th Floor New York, NY 10005 Welcome to the AIG Companies family of customers. We appreciate that you had a choice when placing your insurance and
Domestic Accident & Health Division 80 Pine Street, 13 th Floor New York, NY 10005 Welcome to the AIG Companies family of customers. We appreciate that you had a choice when placing your insurance and
Medicare Coding and Billing Part 2 Sequestration Revalidation Comparative Billing Reports Importance of PQRS CMS 1500 Form Item 14 -
 Medicare Coding and Billing Part 2 Sequestration As of now there are no changes in Sequestration. The Medicare Fee Schedule will change April 1. If you are a non-par doctor, check your MAC website for
Medicare Coding and Billing Part 2 Sequestration As of now there are no changes in Sequestration. The Medicare Fee Schedule will change April 1. If you are a non-par doctor, check your MAC website for
All WRS Users. WRS Revenue Cycle Management Team. Date: 03/14/14. CMS 1500 Version 02/12 Claim Form
 To: From: All WRS Users WRS Revenue Cycle Management Team Date: 03/14/14 Re: CMS 1500 Version 02/12 Claim Form WRS Health presents this document in preview of the new CMS1500 Version 02/12 Claim Form.
To: From: All WRS Users WRS Revenue Cycle Management Team Date: 03/14/14 Re: CMS 1500 Version 02/12 Claim Form WRS Health presents this document in preview of the new CMS1500 Version 02/12 Claim Form.
CMS-1500 PART B MEDICARE ADVANTAGE PLAN BILLING INSTRUCTIONS
 Department of Health and Mental Hygiene Office of Systems, Operations & Pharmacy Medical Care Programs CMS-1500 PART B MEDICARE ADVANTAGE PLAN BILLING INSTRUCTIONS Effective September, 2008 TABLE OF CONTENTS
Department of Health and Mental Hygiene Office of Systems, Operations & Pharmacy Medical Care Programs CMS-1500 PART B MEDICARE ADVANTAGE PLAN BILLING INSTRUCTIONS Effective September, 2008 TABLE OF CONTENTS
MENTAL HEALTH / SUBSTANCE ABUSE TREATMENT CLAIM FORM
 MENTAL HEALTH / SUBSTANCE ABUSE TREATMENT CLAIM FORM DIRECTIONS FOR COMPLETION If you are in treatment with a non-participating ValueOptions provider and your provider has indicated that you will be responsible
MENTAL HEALTH / SUBSTANCE ABUSE TREATMENT CLAIM FORM DIRECTIONS FOR COMPLETION If you are in treatment with a non-participating ValueOptions provider and your provider has indicated that you will be responsible
HEALTH INSURANCE CLAIM FORM APPROVED BY THE BERMUDA HEALTH COUNCIL 10/09
 HEALTH INSURANCE CLAIM FORM APPROVED BY THE BERMUDA HEALTH COUNCIL 10/09 1. NAME OF INSURANCE COMPANY PLEASE PRINT OR TYPE IN UPPERCASE LETTERS 1a. INSURED S CERTIFICATE NUMBER ARGUS BF&M COLONIAL FM GEHI
HEALTH INSURANCE CLAIM FORM APPROVED BY THE BERMUDA HEALTH COUNCIL 10/09 1. NAME OF INSURANCE COMPANY PLEASE PRINT OR TYPE IN UPPERCASE LETTERS 1a. INSURED S CERTIFICATE NUMBER ARGUS BF&M COLONIAL FM GEHI
CLAIMS AND BILLING INSTRUCTIONAL MANUAL
 CLAIMS AND BILLING INSTRUCTIONAL MANUAL 2007 TABLE OF ONTENTS Paper Claims and Block Grant Submission Requirements... 3 State Requirements for Claims Turnaround Time... 12 Claims Appeal Process... 13 Third
CLAIMS AND BILLING INSTRUCTIONAL MANUAL 2007 TABLE OF ONTENTS Paper Claims and Block Grant Submission Requirements... 3 State Requirements for Claims Turnaround Time... 12 Claims Appeal Process... 13 Third
1500 Claims Processing Manual DHMP Health Insurance Claim Form CMS-1500
 DENVER HEALTH MEDICAL PLAN, INC. 1500 Claims Processing Manual DHMP Health Insurance Claim Form CMS-1500 Box 1 Medicare, Medicaid, Group Health Plan or other insurance Information Show the type of health
DENVER HEALTH MEDICAL PLAN, INC. 1500 Claims Processing Manual DHMP Health Insurance Claim Form CMS-1500 Box 1 Medicare, Medicaid, Group Health Plan or other insurance Information Show the type of health
Instructions for Completing the CMS 1500 Claim Form
 Instructions for Completing the CMS 1500 Claim Form The Center of Medicaid and Medicare Services (CMS) form 1500 must be used to bill SFHP for medical services. The form is used by Physicians and Allied
Instructions for Completing the CMS 1500 Claim Form The Center of Medicaid and Medicare Services (CMS) form 1500 must be used to bill SFHP for medical services. The form is used by Physicians and Allied
CMS 1500 Training 101
 CMS 1500 Training 101 HP Enterprise Services Learning Objective Welcome, this training presentation will educate you on how to complete a CMS 1500 claim form; this includes a detailed explanation of all
CMS 1500 Training 101 HP Enterprise Services Learning Objective Welcome, this training presentation will educate you on how to complete a CMS 1500 claim form; this includes a detailed explanation of all
CLAIM FORM REQUIREMENTS
 CLAIM FORM REQUIREMENTS When billing for services, please pay attention to the following points: Submit claims on a current CMS 1500 or UB04 form. Please include the following information: 1. Patient s
CLAIM FORM REQUIREMENTS When billing for services, please pay attention to the following points: Submit claims on a current CMS 1500 or UB04 form. Please include the following information: 1. Patient s
Dental Sleep Medicine
 Dental Sleep Medicine The Patient and Physician Friendly Practice Insurance from A to Pay Dental Sleep Medicine A = Assignment of Benefits A procedure whereby a patient authorizes the administrator of
Dental Sleep Medicine The Patient and Physician Friendly Practice Insurance from A to Pay Dental Sleep Medicine A = Assignment of Benefits A procedure whereby a patient authorizes the administrator of
Tips for Completing the CMS-1500 Claim Form
 Tips for Completing the CMS-1500 Claim Form Member Information (s 1-13) 1 Coverage Optional Show the type of health insurance coverage applicable to this claim by checking the appropriate box (e.g., if
Tips for Completing the CMS-1500 Claim Form Member Information (s 1-13) 1 Coverage Optional Show the type of health insurance coverage applicable to this claim by checking the appropriate box (e.g., if
You must write REHAB at the top center of the claim form!
 CMS 1500 (02/12 INSTRUCTIONS FOR REHABILITATION CENTER SERVICES You must write REHAB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus
CMS 1500 (02/12 INSTRUCTIONS FOR REHABILITATION CENTER SERVICES You must write REHAB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare Champus
To start the pre-approval process, providers must fill out a short online survey, available at: https://www.surveymonkey.com/s/hrszft2.
 Maryland Medicaid EHR Incentive Program Attestation Form for Eligible Providers to Meet Program Requirements Under the Certified Electronic Health Record (CEHRT) Flexibility Rule for Program Year 2014
Maryland Medicaid EHR Incentive Program Attestation Form for Eligible Providers to Meet Program Requirements Under the Certified Electronic Health Record (CEHRT) Flexibility Rule for Program Year 2014
PPO Hospital Care I DRAFT 18973
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.ibx.com or by calling 1-800-ASK-BLUE. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.ibx.com or by calling 1-800-ASK-BLUE. Important Questions
CMS 1500 (02/12) CLAIM FORM INSTRUCTIONS
 CLAIM FORM INSTRUCTIONS") CMS 1500 (02/12) CLAIM FORM INSTRUCTIONS FIELD NUMBER FIELD NAME 1 a INSURED S ID NUMBER INSTRUCTIONS Enter the patient s nine digit Medicaid identification number (SSN) 2 PATIENT S NAME Enter the recipient
CMS 1500 (02/12) CLAIM FORM INSTRUCTIONS FIELD NUMBER FIELD NAME 1 a INSURED S ID NUMBER INSTRUCTIONS Enter the patient s nine digit Medicaid identification number (SSN) 2 PATIENT S NAME Enter the recipient
1. Coverage Indicator Enter an "X" in the appropriate box.
 CMS 1500 Claim Form FIELD NAME INSTRUCTIONS 1. Coverage Indicator Enter an "X" in the appropriate box. 1a. Insured's ID Number Enter the patient's nine-digit Medical Assistance identification number (SSN).
CMS 1500 Claim Form FIELD NAME INSTRUCTIONS 1. Coverage Indicator Enter an "X" in the appropriate box. 1a. Insured's ID Number Enter the patient's nine-digit Medical Assistance identification number (SSN).
SECTION 4. A. Balance Billing Policies. B. Claim Form
 SECTION 4 Participating Physicians, hospitals and ancillary providers shall be entitled to payment for covered services that are provided to a DMC Care member. Payment is made at the established and prevailing
SECTION 4 Participating Physicians, hospitals and ancillary providers shall be entitled to payment for covered services that are provided to a DMC Care member. Payment is made at the established and prevailing
To file a claim: If you have any questions or need additional assistance, please contact our Claim office at 1-800-811-2696.
 The Accident Expense Plus policy is a financial tool that helps cover high deductibles, co-pays and other expenses not covered by your primary major medical plan. This supplemental plan reimburses you
The Accident Expense Plus policy is a financial tool that helps cover high deductibles, co-pays and other expenses not covered by your primary major medical plan. This supplemental plan reimburses you
HCFA-1500 Form Completion. For the RLISYS NSF Electronic Claims Software. 2 Patient Name Patient s name as Last Name, First Name (Example: Doe, John)
") 1 HCFA-1500 Form Completion For the RLISYS NSF Electronic Claims Software 2 Patient Name Patient s name as Last Name, First Name (Example: Doe, John) Do not include a prefix, suffix, or middle initial
1 HCFA-1500 Form Completion For the RLISYS NSF Electronic Claims Software 2 Patient Name Patient s name as Last Name, First Name (Example: Doe, John) Do not include a prefix, suffix, or middle initial
The Healthy Michigan Plan Handbook
 The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). Eligibility for this program will be determined
The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). Eligibility for this program will be determined
The Healthy Michigan Plan Handbook
 The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). The Healthy Michigan Plan provides health
The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). The Healthy Michigan Plan provides health
Administrative Code. Title 23: Medicaid Part 306 Third Party Recovery
 Administrative Code Title 23: Medicaid Part 306 Third Party Recovery Table of Contents Title 23: Division of Medicaid... 1 Part 306: Third Party Recovery... 1 Part 306 Chapter 1: Third Party Recovery...
Administrative Code Title 23: Medicaid Part 306 Third Party Recovery Table of Contents Title 23: Division of Medicaid... 1 Part 306: Third Party Recovery... 1 Part 306 Chapter 1: Third Party Recovery...
United States Fire Insurance Company: International Technological University Coverage Period: beginning on or after 9/7/2014
 or after 9/7/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: PPO This is only a summary. If you want more detail about your coverage and
or after 9/7/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Plan Type: PPO This is only a summary. If you want more detail about your coverage and
How to Bill for a School-Based Clinic
 How to Bill for a School-Based Clinic MDwise.org MDwise is a Hoosier Healthwise/HIP Plan A Hoosier Healthwise/HIP Plan Table of Contents Introduction... 3 The Importance of School-Based Clinics... 3 Covered
How to Bill for a School-Based Clinic MDwise.org MDwise is a Hoosier Healthwise/HIP Plan A Hoosier Healthwise/HIP Plan Table of Contents Introduction... 3 The Importance of School-Based Clinics... 3 Covered
Home Health Services Billing Manual
 Home Health Services Billing Manual F245-424-000 (07-2015) Home Health Services Billing Instructions About Billing Instructions... 1 Where can you find help with L&I billing procedures?... 1 About Labor
Home Health Services Billing Manual F245-424-000 (07-2015) Home Health Services Billing Instructions About Billing Instructions... 1 Where can you find help with L&I billing procedures?... 1 About Labor
CODE AUDITING RULES. SAMPLE Medical Policy Rationale
 CODE AUDITING RULES As part of Coventry Health Care of Missouri, Inc s commitment to improve business processes, we are implemented a new payment policy program that applies to claims processed on August
CODE AUDITING RULES As part of Coventry Health Care of Missouri, Inc s commitment to improve business processes, we are implemented a new payment policy program that applies to claims processed on August
IMPORTANT: WHAT TO KNOW ABOUT FILING YOUR SPECIFIED ILLNESS POLICY CLAIM
 IMPORTANT: WHAT TO KNOW ABOUT FILING YOUR SPECIFIED ILLNESS POLICY CLAIM You can avoid unnecessary processing delays by making sure you provide all of the following: 1. Completed claim forms, including
IMPORTANT: WHAT TO KNOW ABOUT FILING YOUR SPECIFIED ILLNESS POLICY CLAIM You can avoid unnecessary processing delays by making sure you provide all of the following: 1. Completed claim forms, including
You must write AMB at the top center of the claim form!
 CMS 1500 (08/05) INSTRUCTIONS FOR AMBULANCE AND AIR AMBULANCE SERVICES You must write AMB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare
CMS 1500 (08/05) INSTRUCTIONS FOR AMBULANCE AND AIR AMBULANCE SERVICES You must write AMB at the top center of the claim form! Locator # Description Instructions Alerts 1 Medicare / Medicaid / Tricare
CHAPTER 600 PROVIDER QUALIFICATIONS AND PROVIDER REQUIREMENTS 600 CHAPTER OVERVIEW... 600-1 610 AHCCCS PROVIDER QUALIFICATIONS...
 600 CHAPTER OVERVIEW... 600-1 REFERENCES... 600-2 610 AHCCCS PROVIDER QUALIFICATIONS... 610-1 EXHIBIT 610-1 AHCCCS PROVIDER TYPES 620 AHCCCS FFS MINIMUM NETWORK REQUIREMENTS... 620-1 630 MEDICAL RECORD
600 CHAPTER OVERVIEW... 600-1 REFERENCES... 600-2 610 AHCCCS PROVIDER QUALIFICATIONS... 610-1 EXHIBIT 610-1 AHCCCS PROVIDER TYPES 620 AHCCCS FFS MINIMUM NETWORK REQUIREMENTS... 620-1 630 MEDICAL RECORD
MARYLAND MEDICAID CMS-1500 PAPER BILLING INSTRUCTIONS
 MARYLAND MEDICAID CMS-1500 PAPER BILLING INSTRUCTIONS A Comprehensive Guide Focusing on Maryland Medicaid Billing Procedures and Other Useful Information Effective March 2011 Dept. of Health and Mental
MARYLAND MEDICAID CMS-1500 PAPER BILLING INSTRUCTIONS A Comprehensive Guide Focusing on Maryland Medicaid Billing Procedures and Other Useful Information Effective March 2011 Dept. of Health and Mental
US Department of Labor OWCP/FECA P.O. Box 8300 London, KY 40742-8300. DEEOIC P.O. Box 8304 London, KY 40742-8304
 Dear Provider: Thank you for your interest in participating as a provider of medical services for programs administered by the U.S. Department of Labor s Office of Workers Compensation Programs (OWCP).
Dear Provider: Thank you for your interest in participating as a provider of medical services for programs administered by the U.S. Department of Labor s Office of Workers Compensation Programs (OWCP).
The forms must be completed by a qualified person and signed with their occupational title as per its respective form.
 Your ability to work and generate income is your greatest asset. If a disability ever left you unable to work, a combination of increased expenses and loss of income could create financial difficulties.
Your ability to work and generate income is your greatest asset. If a disability ever left you unable to work, a combination of increased expenses and loss of income could create financial difficulties.
NATIONAL PROVIDER IDENTIFIER (NPI) APPLICATION/UPDATE FORM
 APPLICATION/UPDATE FORM") DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES NATIONAL PROVIDER IDENTIFIER (NPI) APPLICATION/UPDATE FORM Form Approved OMB No. 0938-0931 Please PRINT or TYPE all information
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES NATIONAL PROVIDER IDENTIFIER (NPI) APPLICATION/UPDATE FORM Form Approved OMB No. 0938-0931 Please PRINT or TYPE all information
MEDICARE ENROLLMENT APPLICATION
 MEDICARE ENROLLMENT APPLICATION REASSIGNMENT OF MEDICARE BENEFITS CMS-855R SEE PAGE 2 FOR INFORMATION ON WHERE TO MAIL THIS APPLICATION. DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID
MEDICARE ENROLLMENT APPLICATION REASSIGNMENT OF MEDICARE BENEFITS CMS-855R SEE PAGE 2 FOR INFORMATION ON WHERE TO MAIL THIS APPLICATION. DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID
National Uniform Claim Committee
 National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
National Uniform Claim Committee 1500 Health Insurance Claim Form Reference Instruction Manual for 08/05 Version Disclaimer and Notices 2005 American Medical Association This document is published in cooperation
Introduction...2. Definitions...2. Order of Benefit Determination...3
 Introduction...2 Definitions...2 Order of Benefit Determination...3 COB with Medicare...4 When the HMO Is Primary and Medicare Is Secondary... 4 When Medicare Is Primary Payer and the HMO Is Secondary...
Introduction...2 Definitions...2 Order of Benefit Determination...3 COB with Medicare...4 When the HMO Is Primary and Medicare Is Secondary... 4 When Medicare Is Primary Payer and the HMO Is Secondary...
Transamerica Premier Life Insurance Company
 Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Informational Series. Community TM. Glossary of Health Insurance & Medical Terminology. (855) 624-6463 HealthOptions.
 624-6463 HealthOptions.") Informational Series Glossary of Health Insurance & Medical Terminology How to use this glossary This glossary has many commonly used terms, but isn t a full list. These glossary terms and definitions
Informational Series Glossary of Health Insurance & Medical Terminology How to use this glossary This glossary has many commonly used terms, but isn t a full list. These glossary terms and definitions
Section 2. Licensed Nurse Practitioner
 Section 2 Table of Contents 1 General Information... 2 1-1 General Policy... 2 1-2 Fee-For-Service or Managed Care... 2 1-3 Definitions... 2 2 Provider Participation Requirements... 3 2-1 Provider Enrollment...
Section 2 Table of Contents 1 General Information... 2 1-1 General Policy... 2 1-2 Fee-For-Service or Managed Care... 2 1-3 Definitions... 2 2 Provider Participation Requirements... 3 2-1 Provider Enrollment...
If your claim is within the policy s contestability period, we may request additional information.
 Your Cancer Care policy is a limited benefit plan that is designed to supplement the cost of medical procedures and expenses due to the treatment of Cancer. There are three plan options available. Cancer
Your Cancer Care policy is a limited benefit plan that is designed to supplement the cost of medical procedures and expenses due to the treatment of Cancer. There are three plan options available. Cancer
INTRODUCTION. The Workers Compensation Act provides in part as follows:
 INTRODUCTION The Maryland Workers Compensation Commission (Commission) amended COMAR 14.09.03.01 (Guide of Medical and Surgical Fees) on February 12, 2004. AUTHORITY The Workers Compensation Act provides
INTRODUCTION The Maryland Workers Compensation Commission (Commission) amended COMAR 14.09.03.01 (Guide of Medical and Surgical Fees) on February 12, 2004. AUTHORITY The Workers Compensation Act provides
COMBINED INSURANCE COMPANY OF AMERICA INSTRUCTIONS FOR FILING CLAIMS
 COMBINED INSURANCE COMPANY OF AMERICA INSTRUCTIONS FOR FILING CLAIMS GETTING STARTED Follow the Claimant Instructions below to complete the form. Upon completion of the first page you can: Mail OR fax
COMBINED INSURANCE COMPANY OF AMERICA INSTRUCTIONS FOR FILING CLAIMS GETTING STARTED Follow the Claimant Instructions below to complete the form. Upon completion of the first page you can: Mail OR fax
UNITED TEACHER ASSOCIATES INSURANCE COMPANY P.O. Box 26580 Austin, Texas 78755-0580 (800) 880-8824
 880-8824") UNITED TEACHER ASSOCIATES INSURANCE COMPANY P.O. Box 26580 Austin, Texas 78755-0580 (800) 880-8824 OUTLINE OF MEDICARE SUPPLEMENT COVERAGE - COVER PAGE BASIC AND EXTENDED BASIC PLANS The Commissioner of
UNITED TEACHER ASSOCIATES INSURANCE COMPANY P.O. Box 26580 Austin, Texas 78755-0580 (800) 880-8824 OUTLINE OF MEDICARE SUPPLEMENT COVERAGE - COVER PAGE BASIC AND EXTENDED BASIC PLANS The Commissioner of
You also may have purchased the Hospital Cash Rider and/or the Disability Income Benefit Rider. Refer to your policy for detail information.
 Your Emergency Care policy is supplemental insurance to help cover the additional expenses associated with an accidental injury. An Accident is defined as an unforeseen occurrence of an event, which results
Your Emergency Care policy is supplemental insurance to help cover the additional expenses associated with an accidental injury. An Accident is defined as an unforeseen occurrence of an event, which results
Monumental Life Insurance Company
 Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Insurance Claim Filing Instructions PROOF OF LOSS CONSISTS OF THE FOLLOWING: 1. A completed and signed Claim form and Attending Physician s Statement. 2. For Hospital/Intensive Care/Hospital Services Coverage
Michigan Property & Casualty Guaranty Association P.O. Box 531266 Livonia, Michigan 48153-1266 Phone: (248) 482-0381
 482-0381") Michigan Property & Casualty Guaranty Association P.O. Box 531266 Livonia, Michigan 48153-1266 Phone: (248) 482-0381 Dear Claimant: The Michigan Property & Casualty Guaranty Association ("the MPCGA") is
Michigan Property & Casualty Guaranty Association P.O. Box 531266 Livonia, Michigan 48153-1266 Phone: (248) 482-0381 Dear Claimant: The Michigan Property & Casualty Guaranty Association ("the MPCGA") is
Greater Tompkins County Municipal Health Insurance Consortium
 WHO IS COVERED Requires Covered Member to be Enrolled in Both Medicare Parts A & B Type of Coverage Offered Single only Single only MEDICAL NECESSITY Pre-Certification Requirement Not Applicable Not Applicable
WHO IS COVERED Requires Covered Member to be Enrolled in Both Medicare Parts A & B Type of Coverage Offered Single only Single only MEDICAL NECESSITY Pre-Certification Requirement Not Applicable Not Applicable
Your Critical Care policy is supplemental health insurance to help cover the additional expenses associated with a critical illness diagnosis.
 Your Critical Care policy is supplemental health insurance to help cover the additional expenses associated with a critical illness diagnosis. The Critical Care Benefit is a one time lump sum payment.
Your Critical Care policy is supplemental health insurance to help cover the additional expenses associated with a critical illness diagnosis. The Critical Care Benefit is a one time lump sum payment.
Healthy Michigan MEMBER HANDBOOK
 Healthy Michigan MEMBER HANDBOOK 2014 The new name for Healthy 1 TABLE OF CONTENTS WELCOME TO HARBOR HEALTH PLAN.... 2 Who Is Harbor Health Plan?...3 How Do I Reach Member Services?...3 Is There A Website?....
Healthy Michigan MEMBER HANDBOOK 2014 The new name for Healthy 1 TABLE OF CONTENTS WELCOME TO HARBOR HEALTH PLAN.... 2 Who Is Harbor Health Plan?...3 How Do I Reach Member Services?...3 Is There A Website?....
Hospital Confinement/Outpatient Surgery Claim
 FAX this direction If your name has changed, attach a copy of your driver s license or other legal documentation. Hospital Confinement/Outpatient Surgery Claim FAX this form: 1-800-880-9325 Or mail: P.O.
FAX this direction If your name has changed, attach a copy of your driver s license or other legal documentation. Hospital Confinement/Outpatient Surgery Claim FAX this form: 1-800-880-9325 Or mail: P.O.
AMERICAN NATIONAL INSURANCE COMPANY CREDIT INSURANCE DIVISION P. O. BOX 696785 * SAN ANTONIO, TEXAS 78269-6785 800-899-6502
 P. O. BOX 696785 * SAN ANTONIO, TEXAS 78269-6785 DISABILITY CLAIM FORM INSTRUCTIONS Enclosed is a claim form required in order to process disability payments on your loan. It is important that all questions
P. O. BOX 696785 * SAN ANTONIO, TEXAS 78269-6785 DISABILITY CLAIM FORM INSTRUCTIONS Enclosed is a claim form required in order to process disability payments on your loan. It is important that all questions
NJ FamilyCare ABP. Covered by Horizon NJ Health for spontaneous abortions/miscarriages. Abortions & Related Services
 NJ FamilyCare ABP BENEFIT Abortions & Related Services COVERAGE by Horizon NJ Health for spontaneous abortions/miscarriages. by Fee-for-Service for elective/induced abortions. Acupuncture Audiology (see
NJ FamilyCare ABP BENEFIT Abortions & Related Services COVERAGE by Horizon NJ Health for spontaneous abortions/miscarriages. by Fee-for-Service for elective/induced abortions. Acupuncture Audiology (see
3. PATIENT S BIRTHDATE SEX MM DD YY YY 6. PATIENT RELATIONSHIP TO TO INSURED. Self Spouse Child Other
 1 2 3 4 5 6 PLEASE DO NOT STAPLE 1500 IN THIS AREA HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05 HEALTH INSURANCE CLAIM FORM PCA PICA PICA PCA 1. 1. MEDICARE MEDICAID CHAMPUS
1 2 3 4 5 6 PLEASE DO NOT STAPLE 1500 IN THIS AREA HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05 HEALTH INSURANCE CLAIM FORM PCA PICA PICA PCA 1. 1. MEDICARE MEDICAID CHAMPUS
NJ FamilyCare A. Covered by Horizon NJ Health for spontaneous abortions/miscarriages. Abortions & Related Services
 NJ FamilyCare A BENEFIT Abortions & Related Services COVERAGE by Horizon NJ Health for spontaneous abortions/miscarriages. by Fee-for-Service for elective/induced abortions. Acupuncture Audiology (see
NJ FamilyCare A BENEFIT Abortions & Related Services COVERAGE by Horizon NJ Health for spontaneous abortions/miscarriages. by Fee-for-Service for elective/induced abortions. Acupuncture Audiology (see
HOW TO COMPLETE THE HEALTH INSURANCE CLAIM FORM (HCFA-1500) HCFA 1500 Forms Can Be Ordered From The Supply Center 800-549 - 5993
 HCFA 1500 Forms Can Be Ordered From The Supply Center 800-549 - 5993") HOW TO COMPLETE THE HEALTH INSURANCE CLAIM FORM (HCFA-1500) HCFA 1500 Forms Can Be Ordered From The Supply Center 800-549 - 5993 The Health Care Financing Administration Health Insurance Claim Form (HCFA-1500)
HOW TO COMPLETE THE HEALTH INSURANCE CLAIM FORM (HCFA-1500) HCFA 1500 Forms Can Be Ordered From The Supply Center 800-549 - 5993 The Health Care Financing Administration Health Insurance Claim Form (HCFA-1500)
Voluntary Disability Benefits
 Voluntary Disability Benefits Enclosed you will find a disability packet that will provide information to assist you in filing for disability benefits through The Claremont Colleges Voluntary Disability
Voluntary Disability Benefits Enclosed you will find a disability packet that will provide information to assist you in filing for disability benefits through The Claremont Colleges Voluntary Disability
Legacy Medigap SM. Plan A and Plan C. Outline of Medigap insurance coverage and enrollment application for
 2015 Medicare Supplement Coverage offered by Blue Cross Blue Shield of Michigan Legacy Medigap SM Outline of Medigap insurance coverage and enrollment application for Plan A and Plan C LEGM_S_LegacyMedigapBrochure
2015 Medicare Supplement Coverage offered by Blue Cross Blue Shield of Michigan Legacy Medigap SM Outline of Medigap insurance coverage and enrollment application for Plan A and Plan C LEGM_S_LegacyMedigapBrochure
The Hospital Billing Process The purpose of this chapter is to provide an overview of the hospital billing process. The
 3 Section One: Section Title Chapter 5 The Hospital Billing Process The purpose of this chapter is to provide an overview of the hospital billing process. The billing process includes submitting charges
3 Section One: Section Title Chapter 5 The Hospital Billing Process The purpose of this chapter is to provide an overview of the hospital billing process. The billing process includes submitting charges
HANDBOOK FOR ADVANCED PRACTICE NURSES
 HANDBOOK FOR ADVANCED PRACTICE NURSES CHAPTER N 200 Policy and Procedures for Advanced Practice Nurse Services Illinois Department of Public Aid FOREWORD PURPOSE CHAPTER N-200 ADVANCED PRACTICE NURSE SERVICES
HANDBOOK FOR ADVANCED PRACTICE NURSES CHAPTER N 200 Policy and Procedures for Advanced Practice Nurse Services Illinois Department of Public Aid FOREWORD PURPOSE CHAPTER N-200 ADVANCED PRACTICE NURSE SERVICES
Premera Blue Cross Medicare Advantage Provider Reference Manual
 Premera Blue Cross Medicare Advantage Provider Reference Manual Introduction to Premera Blue Cross Medicare Advantage Plans Premera Blue Cross offers Medicare Advantage (MA) plans in King, Pierce, Snohomish,
Premera Blue Cross Medicare Advantage Provider Reference Manual Introduction to Premera Blue Cross Medicare Advantage Plans Premera Blue Cross offers Medicare Advantage (MA) plans in King, Pierce, Snohomish,
Medicare may pay for inpatient hospital, doctor, or ambulance services you receive in Canada or Mexico:
 Medicare Beneficiary Services:1-800-MEDICARE (1-800-633-4227) TTY/ TDD:1-877-486-2048 Thank you for your recent request for the Patient s Request for Medical Payment form (CMS-1490S). Enclosed is the form,
Medicare Beneficiary Services:1-800-MEDICARE (1-800-633-4227) TTY/ TDD:1-877-486-2048 Thank you for your recent request for the Patient s Request for Medical Payment form (CMS-1490S). Enclosed is the form,
State Health Plan: Savings Plan Coverage Period: 01/01/2015-12/31/2015
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.eip.sc.gov or by calling 1-888-260-9430. Important Questions
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.eip.sc.gov or by calling 1-888-260-9430. Important Questions
Glossary of Health Coverage and Medical Terms
 Glossary of Health Coverage and Medical Terms This glossary defines many commonly used terms, but isn t a full list. These glossary terms and definitions are intended to be educational and may be different
Glossary of Health Coverage and Medical Terms This glossary defines many commonly used terms, but isn t a full list. These glossary terms and definitions are intended to be educational and may be different
CHAPTER 27 THE SCOPE OF PROFESSIONAL NURSING PRACTICE AND ARNP AND CNM PROTOCOLS
 I. INTRODUCTION CHAPTER 27 THE SCOPE OF PROFESSIONAL NURSING PRACTICE AND ARNP AND CNM PROTOCOLS Advance registered nurse practitioners (ARNPs) and clinical nurse practitioners (CNPs) have their scope
I. INTRODUCTION CHAPTER 27 THE SCOPE OF PROFESSIONAL NURSING PRACTICE AND ARNP AND CNM PROTOCOLS Advance registered nurse practitioners (ARNPs) and clinical nurse practitioners (CNPs) have their scope
Disability Insurance Claim Packet Instructions. Your Disability Benefit Claim. How To Apply For Benefits
 Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Federally Qualified Health Center Billing (100)
") 1. As a federally qualified health center (FQHC) can we bill for a license medical social worker? The core practitioner must be a licensed or certified clinical social worker (CSW) in your state. Unless
1. As a federally qualified health center (FQHC) can we bill for a license medical social worker? The core practitioner must be a licensed or certified clinical social worker (CSW) in your state. Unless
HCPCS codes should be used to describe outpatient diagnostic laboratory procedures (revenue codes 300 to 319).
.") 6How Do I Bill Tribal Outpatient Hospital Services? Complete the UB-04 form for outpatient hospital services. Refer to How do I complete the UB-04? in the Billing Guidelines section for specific information
6How Do I Bill Tribal Outpatient Hospital Services? Complete the UB-04 form for outpatient hospital services. Refer to How do I complete the UB-04? in the Billing Guidelines section for specific information
DISCHARGE APPLICATION: TOTAL AND PERMANENT DISABILITY IMPORTANT INFORMATION William D. Ford Federal Direct Loan Program
 OMB No. 1845-0065 Fo rm Ap pro ved Exp. Date 6/30/2016 DISCHARGE APPLICATION: TOTAL AND PERMANENT DISABILITY IMPORTANT INFORMATION William D. Ford Federal Direct Loan Program TPD- APP Federal Family Education
OMB No. 1845-0065 Fo rm Ap pro ved Exp. Date 6/30/2016 DISCHARGE APPLICATION: TOTAL AND PERMANENT DISABILITY IMPORTANT INFORMATION William D. Ford Federal Direct Loan Program TPD- APP Federal Family Education
City of Los Angeles Disability Insurance Claim Packet Instructions
 Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
CMS-1500 Billing Guide for PROMISe Audiologists
 CMS-1500 Billing Guide for PROMISe udiologists Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider types
CMS-1500 Billing Guide for PROMISe udiologists Purpose of the document Document format The purpose of this document is to provide a block-by-block reference guide to assist the following provider types
Illustration 1-1. Revised CMS-1500 Claim Form (front)
") Florida Medicaid Provider Reimbursement Handbook, CMS-1500 Illustration 1-1. Revised CMS-1500 Claim Form (front) Incorporated by reference in 59G-4.001, F.A.C. July 2008 1-11 Florida Medicaid Provider
Florida Medicaid Provider Reimbursement Handbook, CMS-1500 Illustration 1-1. Revised CMS-1500 Claim Form (front) Incorporated by reference in 59G-4.001, F.A.C. July 2008 1-11 Florida Medicaid Provider
BlueCross BlueShield of South Carolina Provider Services Voice Response Unit (VRU) Guide
 Guide") BlueCross BlueShield of South Carolina Provider Services Voice Response Unit (VRU) Guide South Carolina: 1-800-868-2510 Columbia/Lexington: 788-8562 Out-of-State: 1-800-334-2583 Eligibility and benefits
BlueCross BlueShield of South Carolina Provider Services Voice Response Unit (VRU) Guide South Carolina: 1-800-868-2510 Columbia/Lexington: 788-8562 Out-of-State: 1-800-334-2583 Eligibility and benefits
Reimbursement and Claims Submission Changes for Nursing Home Provided Non-emergency Transportation for Nursing Home Residents
 Update February 2010 No. 2010-05 Affected Programs: BadgerCare Plus Standard Plan, BadgerCare Plus Benchmark Plan, Medicaid To: Nursing Homes, HMOs and Other Managed Care Programs Reimbursement and Claims
Update February 2010 No. 2010-05 Affected Programs: BadgerCare Plus Standard Plan, BadgerCare Plus Benchmark Plan, Medicaid To: Nursing Homes, HMOs and Other Managed Care Programs Reimbursement and Claims
Virginia Association of Counties Group Self Insurance Risk Pool Disability Insurance Claim Packet Instructions
 Claim Packet Instructions Your Disability Benefit Claim We realize that being disabled is difficult. Even though you are unable to work, your financial obligations do not go away. To help you through these
Claim Packet Instructions Your Disability Benefit Claim We realize that being disabled is difficult. Even though you are unable to work, your financial obligations do not go away. To help you through these
State of Nevada Public Employees Benefits Program (PEBP) Short Term Disability Insurance Claim Packet Instructions
 Short Term Disability Insurance Claim Packet Instructions") Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
The Federal Employees Health Benefits Program and Medicare
 The Federal Employees Health Benefits Program and Medicare This booklet answers questions about how the Federal Employees Health Benefits (FEHB) Program and Medicare work together to provide health benefits
The Federal Employees Health Benefits Program and Medicare This booklet answers questions about how the Federal Employees Health Benefits (FEHB) Program and Medicare work together to provide health benefits
You can see the specialist you choose without permission from this plan.
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.pekininsurance.com or by calling 1-800-322-0160. Important
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.pekininsurance.com or by calling 1-800-322-0160. Important
Traumatlc injury and Claim for Continuation of Pay/Compensation
 Federal Employee's Notice of Traumatlc injury and Claim for Continuation of Pay/Compensation U.S. Department of Labor Employment Standards Administration Office of Workers' Compensation Programs Employee
Federal Employee's Notice of Traumatlc injury and Claim for Continuation of Pay/Compensation U.S. Department of Labor Employment Standards Administration Office of Workers' Compensation Programs Employee
StudentBlue University of Nebraska
 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO What is the overall deductible? This is only a summary. If you want more details about
Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO What is the overall deductible? This is only a summary. If you want more details about
Faculty Group Practice Patient Demographic Form
 Name (Last, First, MI) Faculty Group Practice Patient Demographic Form Today s Date Patient Information Street Address City State Zip Home Phone Work Phone Cell Phone ( ) Preferred ( ) Preferred ( ) Preferred
Name (Last, First, MI) Faculty Group Practice Patient Demographic Form Today s Date Patient Information Street Address City State Zip Home Phone Work Phone Cell Phone ( ) Preferred ( ) Preferred ( ) Preferred
Molina Healthcare of Ohio, Inc. PO Box 22712 Long Beach, CA 90801
 Section 9. Claims As a contracted provider, it is important to understand how the claims process works to avoid delays in processing your claims. The following items are covered in this section for your
Section 9. Claims As a contracted provider, it is important to understand how the claims process works to avoid delays in processing your claims. The following items are covered in this section for your
FUNDAMENTALS OF HEALTH INSURANCE: What Health Insurance Products Are Available?
 http://www.naic.org/ FUNDAMENTALS OF HEALTH INSURANCE: PURPOSE The purpose of this session is to acquaint the participants with the basic principles of health insurance, areas of health insurance regulation
http://www.naic.org/ FUNDAMENTALS OF HEALTH INSURANCE: PURPOSE The purpose of this session is to acquaint the participants with the basic principles of health insurance, areas of health insurance regulation
OFFICE OF GROUP BENEFITS 2014 OFFICE OF GROUP BENEFITS CDHP PLAN FOR STATE OF LOUISIANA EMPLOYEES AND RETIREES PLAN AMENDMENT
 OFFICE OF GROUP BENEFITS 2014 OFFICE OF GROUP BENEFITS CDHP PLAN FOR STATE OF LOUISIANA EMPLOYEES AND RETIREES PLAN AMENDMENT This Amendment is issued by the Plan Administrator for the Plan documents listed
OFFICE OF GROUP BENEFITS 2014 OFFICE OF GROUP BENEFITS CDHP PLAN FOR STATE OF LOUISIANA EMPLOYEES AND RETIREES PLAN AMENDMENT This Amendment is issued by the Plan Administrator for the Plan documents listed
How To Bill Medicaid As An Individual Physician Or Non-Physician Practitioner
 Ohio Department of Job and Family Services Ohio Health Plans Provider Enrollment Application/Time Limited Agreement for Individual Practitioners Submit completed signed application/agreement with required
Ohio Department of Job and Family Services Ohio Health Plans Provider Enrollment Application/Time Limited Agreement for Individual Practitioners Submit completed signed application/agreement with required
MEDICARE CREDIT BALANCE REPORT CERTIFICATION PAGE
 DEPAR ARTMENT OF HEALTH AND HUMAN SERVICES Form Approved OMB No. 0938-0600 MEDICARE CREDIT BALANCE REPORT CERTIFICATION PAGE The Credit Balance Report is required under the authority of sections 1815(a),
DEPAR ARTMENT OF HEALTH AND HUMAN SERVICES Form Approved OMB No. 0938-0600 MEDICARE CREDIT BALANCE REPORT CERTIFICATION PAGE The Credit Balance Report is required under the authority of sections 1815(a),
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY NATIONWIDE SPECIALTY INSURANCE CLAIM FORM
 NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY NATIONWIDE SPECIALTY INSURANCE CLAIM FORM THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY NATIONWIDE SPECIALTY INSURANCE CLAIM FORM THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM
A. CPT Coding System B. CPT Categories, Subcategories, and Headings
 OST 148 MEDICAL CODING, BILLING AND INSURANCE COURSE DESCRIPTION: Prerequisites: None Corequisites: None This course introduces CPT and ICD coding as they apply to medical insurance and billing. Emphasis
OST 148 MEDICAL CODING, BILLING AND INSURANCE COURSE DESCRIPTION: Prerequisites: None Corequisites: None This course introduces CPT and ICD coding as they apply to medical insurance and billing. Emphasis
Disability Insurance Claim Packet Instructions. Your Disability Benefit Claim. The Standard Benefit Administrators. How To Apply For Benefits
 Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Claim Packet Instructions Your Disability Benefit Claim This packet contains the forms necessary to apply for disability benefits. It also addresses common questions about Disability claims. Please save
Florida Medicaid Recipients With Other Medical Insurances. April 2013
 Florida Medicaid Recipients With Other Medical Insurances April 2013 1 Section 1 The Basics 2 What is Third Party Liability? Third Party Liability (TPL) is the obligation of any entity other than Medicaid
Florida Medicaid Recipients With Other Medical Insurances April 2013 1 Section 1 The Basics 2 What is Third Party Liability? Third Party Liability (TPL) is the obligation of any entity other than Medicaid
NJ FamilyCare B. Covered by Horizon NJ Health for spontaneous abortions/miscarriages. Abortions & Related Services
 NJ FamilyCare B BENEFIT Abortions & Related Services COVERAGE by Horizon NJ Health for spontaneous abortions/miscarriages. by Fee-for-Service for elective/induced abortions. Acupuncture Audiology (see
NJ FamilyCare B BENEFIT Abortions & Related Services COVERAGE by Horizon NJ Health for spontaneous abortions/miscarriages. by Fee-for-Service for elective/induced abortions. Acupuncture Audiology (see
First Name MI Last. Street Address (P.O. Boxes cannot be accepted) City State Zip. First Name MI Last
 City State Zip. First Name MI Last") Accident Claim Form Instructions for Filing a Claim LIFESECURE INSURANCE COMPANY ADMINISTRATIVE OFFICE ATTN: Claims Department PO Box 13490, Pensacola, FL 32591-3490 1-888-575-8246 Please have all sections
Accident Claim Form Instructions for Filing a Claim LIFESECURE INSURANCE COMPANY ADMINISTRATIVE OFFICE ATTN: Claims Department PO Box 13490, Pensacola, FL 32591-3490 1-888-575-8246 Please have all sections
HMO Blue Basic Coinsurance Coverage Period: on or after 01/01/2015
 HMO Blue Basic Coinsurance Coverage Period: on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family Plan Type: HMO This is only
HMO Blue Basic Coinsurance Coverage Period: on or after 01/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual and Family Plan Type: HMO This is only
Coverage level: Employee/Retiree Only Plan Type: EPO
 This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan documents at www.dbm.maryland.gov/benefits or by calling 410-767-4775
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan documents at www.dbm.maryland.gov/benefits or by calling 410-767-4775
Claims Procedures. H.2 At a Glance. H.4 Submission Guidelines. H.9 Claims Documentation. H.17 Codes and Modifiers. H.
 H.2 At a Glance H.4 Submission Guidelines H.9 Claims Documentation H.17 Codes and Modifiers H.22 Reimbursement H.25 Denials and Appeals At a Glance pledges to provide accurate and efficient claims processing.
H.2 At a Glance H.4 Submission Guidelines H.9 Claims Documentation H.17 Codes and Modifiers H.22 Reimbursement H.25 Denials and Appeals At a Glance pledges to provide accurate and efficient claims processing.