Maintaining Proper Dental Records
|
|
|
- Brianne McCormick
- 10 years ago
- Views:
Transcription
1 Maintaining Proper Dental Records Wilhemina Leeuw, MS, CDA Continuing Education Units: 2 hours Online Course: Disclaimer: Participants must always be aware of the hazards of using limited knowledge in integrating new techniques or procedures into their practice. Only sound evidence-based dentistry should be used in patient therapy. This course provides dental healthcare professionals with the necessary background and procedures for proper charting and protection. Although this course presents guidelines to minimize legal risks, it is for guidance purposes only and is not intended to be legal in nature. Legal counsel should be sought any time a practice decides to change and/or implement new forms, recordkeeping procedures or privacy safeguards. An attorney will be able to inform and advise on the specific laws, rules and regulations that pertain to specific states and in specific situations. Conflict of Interest Disclosure Statement The author reports no conflicts of interest associated with this work. ADAA This course is part of the home-study library of the American Dental Assistants Association. To learn more about the ADAA and to receive a FREE e-membership visit: ADA CERP The Procter & Gamble Company is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at: 1

2 Overview Maintaining complete and accurate patient records is a sign of quality care and an integral part of our duty to care for the patient. Living in a highly litigious society, all health care professionals face the very real risk of being the target of a malpractice claim. As such, the dental profession must implement processes to minimize the risk of such actions. A properly documented record is the best defense against malpractice litigation, and every member of the dental team is equally responsible for recording pertinent facts about a patient s visit on the chart and protecting vital patient information. This course provides dental healthcare professionals with the necessary background and procedures for proper charting and protection. Although this course presents guidelines to minimize legal risks, it is for guidance purposes only and is not intended to be legal in nature. Legal counsel should be sought any time a practice decides to change and/or implement new forms, recordkeeping procedures or privacy safeguards. An attorney will be able to inform and advise on the specific laws, rules and regulations that pertain to specific states and in specific situations. Learning Objectives Upon completion of this course, the dental professional should be able to: Understand the importance of and the reasons for properly documenting and maintaining patient records. Differentiate between types of data that should be included or excluded from the complete record. Explain ownership of the physical dental records, radiographs and information found in patient charts. Avoid potential charting errors by learning to use objective and legible entries to properly document pertinent patient information. Enumerate important criteria when recording treatment procedures. Demonstrate how to properly revise an incorrect entry. Explain the difference between a correction and an alteration of an entry in the patient chart. Understand contributory actions and their necessary documentation. Discuss the risks involved if documentation is inaccurate. Gain a better understanding of dental malpractice, Standard of Care and the importance of communicating with patients. Suggest ways to improve record documentation in the practice setting. Understand the HIPAA privacy and security rules. Course Contents Glossary Categories of Records The Need to Maintain Good Dental Records Ownership of the Dental Record Components of the Clinical Record The Registration Form Acknowledgement of HIPAA Practices The Medical/Health History Form The Dental History Form The Informed Consent Form Clinical Progress Notes Additional Components of the Patient Record Steps in Documentation Other Important Documentation Documenting in the Clinical Record Dental Records and the Computer Retention of Records Dental Malpractice HIPAA HIPAA Intent HIPAA Compliance Standard Transactions Privacy Rule Compliance Business Associates Security Rule Compliance Summary Appendices Course Test Preview References About the Author 2

3 Glossary allege to assert without proof alteration a change or revision breach of contract failure to act as required by a contract (for example, failure of a patient to pay a reasonable fee for services provided is a breach of contract) chart a portion of the complete patient record; the chart receives documentation including dates and reasons for visits, treatments rendered, radiographs, instructions provided, medications prescribed, laboratory prescriptions and results, referral information, telephone support provided, and recare recommended clinical pertaining to the disease and treatment of the patient conceal to hide, to prevent disclosure confidential information to be kept secret contract a written or oral agreement between two or more parties that is enforceable by law (for example, a contract to deliver the Standard of Care is implied and initiated when a dentist assumes responsibility for examining and treating a patient) defendant a person, company, etc., against whom a claim or charge is brought in a court expert witness a person with knowledge not normally possessed by the average person concerning the topic on which he is to testify in a court of law forensic odontologist a dentist who studies teeth and their bite mark patterns to make identifications and diagnosis HIPAA acronym for Health Insurance Portability and Accountability Act of 1996 informed consent voluntary agreement by a person in the possession of sufficient information to make an intelligent choice informed refusal voluntary denial of recommended services or treatments by a person in the possession of sufficient information to make an intelligent choice litigation engaging in legal proceedings malpractice negligence and/or misconduct on the part of a professional Notice of Privacy Practices required under HIPAA; written notification informing patients of the office s policies related to the use and disclosure of their protected health information objective factual information; not influenced by opinion obliterate to destroy completely, leaving no trace PHI stands for protected health information plaintiff a person who files a lawsuit against another person, group, or business precedent a judicial decision that may be used as a standard in subsequent similar cases Privacy Contact required under HIPAA; the designated individual in the office responsible for providing information, receiving complaints, and handling the administration of patients rights Privacy Officer required under HIPAA; the designated individual in the office responsible for developing and implementing the policies and procedures necessary for HIPAA compliance Privacy Rule; HIPAA national standard to protect patient records and other personal health information; applies to all dental offices professional liability insurance also known as malpractice insurance; insurance covering the insured against losses arising from injury or damage to another person promulgate to make known, proclaim or teach publicly records the patient record is comprised of the clinical chart, treatment forms, financial transactions, radiographs, and study models scrutiny a searching examination or investigation 3

4 Security Rule; HIPAA national standard to protect and ensure the confidentiality, integrity, and security of electronic protected health information Standard of Care legal duty of a dentist to exercise a degree of skill and care that would be exhibited by other prudent dentists statute of limitations amount of time during which a lawsuit may be filed subjective information that is influenced by personal feeling or opinion subpoena a written order to appear and testify in court with a stated penalty for failure to comply Categories of Records There are many different types of records in the dental office. How a record is stored and used depends on its type. Generally, records can be categorized as vital, important, useful, and unimportant. Vital records are essential documents that cannot be replaced and, therefore, highly protected. The patient record falls within this category along with office deed and mortgage paperwork. These documents should be maintained in fireproof cabinets for utmost safety. If the office has electronic records, these must be backed up often for document safety and integrity. Important records are valuable to the operation of the office. Examples of these documents will include accounting information, inventory records, and federal regulatory paperwork. These documents must be kept for 5 7 years. Useful records are harder to define as each office may decide differently on what it and is not important. Examples of these may include employment application, petty cash receipts, and bank reconciliations. When an office decides that it is considered a useful document, these are usually stored for 1 3 years. Unimportant paperwork will consist of outdated memos and announcements, and meeting reminders. Common sense dictates when these items should be disposed. The Need to Maintain Good Dental Records A dental record is a combination of any written, oral, diagnostic artifact, or other transmission of information that identifies the patient and relates to his or her health care. Components of the patient record may include the patient chart, radiographs and dental casts, and certain documentation required by law. The primary goal of keeping good dental records is to maintain continuity of care. Diligent and complete documentation and standardized charting procedures are essential. The patient record documents all patient visits and the treatment that occurred, including examinations, diagnoses, treatment options, correspondence, and chosen treatment courses with financial arrangements. The record documents treatment history and offers a basic measurement for evaluating the quality of care provided. In addition, the record provides a means of communication between the treating dentist and any other health care provider called upon to contribute to the care of a patient. Keeping adequate records entails charting enough information to allow another provider even one who has no prior knowledge of or experience with the patient to know the patient s total dental history while in that practice. Clinical entries are often too abridged and abbreviated to cover the clinical treatment properly. Dentistry as a culture has historically erred towards brevity, which is often turned against the office in legal matters concerning neglect. The patient record will be used supplementally as verification. Third-party carriers may request information concerning treatment to determine adequate, eligible services before making payment. The Internal Revenue Service may use it in an audit to verify treatment services. A forensic odontologist may need vital documentation or radiographs to identify otherwise unrecognizable. Also, because dental records are considered legal documents each component will help protect the interests of the dental team and/or the patient by establishing the details of the care that was rendered. In malpractice cases, an expert witness usually helps the court decide if a dentist did or 4

5 did not perform in accordance with the accepted norms, guidelines and degrees of competence that can be reasonably expected from a dental professional. Referred to as Standard of Care, this legal duty requires the dentist to exercise the degree of skill and care that would be exhibited by other prudent dentists faced with the same patient-care situation. Dental associations and state dental boards promulgate standards and recommendations that typically determine the Standard of Care. When considered in a broad sense, errors may be actions of commission, oversight, or completion and any one of these can be brought into question when examining Standard of Care as a legal duty. The Health Insurance Portability and Accountability Act (HIPAA) of 1994 requires all dental offices as covered entities to maintain the security and privacy of all patient records and electronic transactions. Civil and criminal penalties can be charged to any person or dental office that does not follow the law. Each dental office must give a copy of their privacy practices to each patient and in return, the patient or guardian signs a receipt to be kept in the patient record to acknowledge that they have received it. Finally, poorly maintained records convey a poor overall impression. A practice failing at basic record keeping suggests additional problems office wide. This factor would be used by attorneys and judges involved in a malpractice case, leading to a negative impact during the investigation phase. Ownership of the Dental Record The dentist owns the physical record(s) pertaining to the patient and is the legal guardian of the chart and records. In the situation where a dentist is an employee of a group practice, ownership usually lies with the practice. The ownership in this case depends on the contract negotiated between the individual dentist and the practice. Ultimately, the state s dental laws dictate dental record ownership. Patients do not have the right to possess their original record, but the patient does have the right to see, review, inspect, request and obtain a copy of their record components. The dental professional is advised to become familiar with the laws of his/her particular state governing patient record ownership. Upon request, a patient must be able to gain access to their records within a reasonable time frame. When asked by the patient, or patient s guardian, to copy any portion of the patient dental record, offices may charge a reasonable fee for the labor, supplies, and postage incurred. The dental office is to refer to applicable state laws, as this fee is often defined within the state s privacy laws. A practice cannot refuse to release any portion of a patient s record because of an outstanding financial account, especially if another dentist is requesting the information or the patient is transferring to another practice for care. At all cost, any interruption in patient care should be avoided. Radiographs are a vital part of a patient s clinical record, and only a licensed dentist can interpret them. When radiographs are obtained, the patient is paying for the interpretation of the radiograph(s) and not the actual film itself. Therefore, in most states dentists typically maintain ownership of patient radiographs. (Consult the state s laws to verify ownership regulations). However, patients have the right to obtain copies of their radiographs. Original records are never to be released, including radiographs, to any party. No matter how formal a request for the originals may seem, only copies should be sent. The one exception to this rule is Subpoena Ducus Tecum, which requires that the dentist or representative present original records to a court of law. In such an event, copies of the original records must be kept in the dental office. Due to the confidential nature of the dental record, permission must be received before sending any patient information. Under HIPAA, this refers to an acknowledgment or authorization form. A HIPAA regulation that went into effect in 2013 will further regulate the restrictions of patient treatment information that has been paid in full by the patient out of pocket. A general release form to authorize the release of the patient record will include basic elements: Patient name and identification Identity and address of the owning office A description of the information being released 5

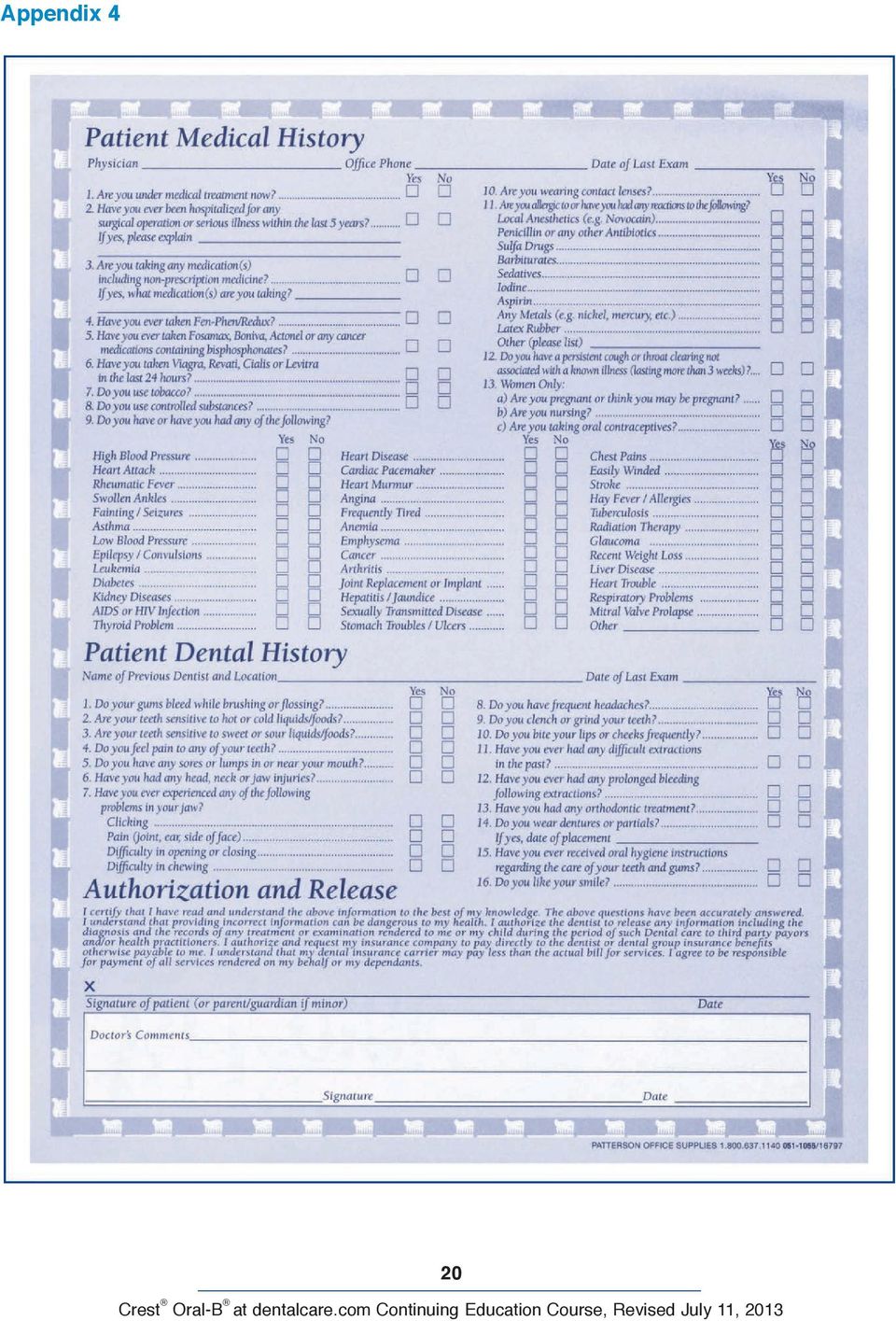
6 Basic statement that details to release of the information Patient signature to verify release The form used must be valid, signed, and on hand before any information is released to the patient, the patient s representative or another provider. Verify the signature on the form with the one on file (either on the Medical History Form or the Patient Registration Form). Document on the original record the date as well, as where and to whom the copies were sent. If mailing the records, they should be delivered via certified mail so a return receipt request can be obtained. This can be added to the patient record to provide proof of delivery and that the record was delivered safely to the destination. Members of the dental team should never send anything out of the office without the dentist s knowledge and approval no matter how formal the request. Components of the Clinical Record Some offices maintain a personal information sheet, or tickler file. This file contains bits of conversational information about the patient s interests, latest trips or hobbies, but such information should be kept to a minimum. The vast majority of the information in dental documentation should be clinical in nature. Financial information should not be kept in the clinical chart. Ledger cards, insurance benefit breakdowns, insurance claims, and payments vouchers are not part of the patient s clinical record and should not be included in or on the front cover of the clinical chart. Financial information must be recorded, tracked, and kept with the other accounts receivables for the office. The paperwork of the records must be kept in a file folder. The outside cover of the chart should only display the patient s name and/or the account number. Because the patient chart contains confidential information, notations of medical conditions, treatment plan, or correspondence should not be written on the outside folder where others can see. All medical notations belong inside the record and, if the record is electronic, computer screens must be directed for only authorized personnel to see. If the chart must be flagged, use an abstract system (such as color- or symbol-coding) so that only the dental healthcare workers know its relevance. The Registration Form This form will contain the patient s full name and demographic information as well as their employment and insurance information. Omissions on this form can complicate account collections and impede the ability for expected patient communications and recare. This form contains vital information such as a social security number and must be protected. This form will need to be reviewed and updated whenever the patient changes residence, obtains new contact phone numbers, changes employment or their current employment changes their insurance carrier. Appendix 1 is an example of a registration form. Acknowledgement of HIPAA Practices All patients, or their legal representative, must sign a form verifying their receipt of the office s HIPAA practices. This form is required as part of the HIPAA Act and must be kept in the patient s records for 6 years. This written policy must inform the patient that the office will not disclose PHI for any purposes other than treatment, diagnosis, and billing. Appendix 2 and Appendix 3 are examples of a HIPAA statement and a form to acknowledge the receipt of the HIPAA statement. The Medical/Health History Form The Medical History Form is of primary importance. This form provides necessary information that will aid the dental team in providing safe and quality care. Failure on the part of the office to update a Medical History Form or obtain proper medical information from a patient constitutes malpractice. Because this history may take exra time to complete for a new patient, this form can be mailed to the patient before the appointment so they can take time to complete it accurately, or they should be asked to arrive approximately 10 minutes early to begin the new patient record forms. With patient diversity increasing, it may be necessary to provide a health history in a different language. The University of Pacific Dental School in California ( 6

7 Professional_Services_and_Resources/Dental_ Practice_Documents.html) and MetLife Dental has free downloadable forms in 39 languages. Medical history questions are included to help the dental team professionals evaluate the patient s health and identify possible treatment risks (see Appendix 4.) A patient s medical history contains essential information for protecting the patient and the treating dentist. The dentist should review and discuss the information on the completed form with the patient to ensure that the information was understood and complete. All questions must be answered and the form must be signed by the patient or the patient s guardian. The dentist must either sign or initial the form to show that he/she reviewed it with the patient at every visit. It has been recommended that a new Medical History Form be completed approximately every 3 years. Each form must have an identifier on it (either the patient s name or account number). If there are no changes, a notation is made to that effect. It is the dentist s responsibility to discern applicable new medications for treatment and the assessment of using an anesthesia that contains epinephrine. There have been numerous cases of malpractice where the patient was prescribed a medication that was clearly contraindicated by the patient s current medical condition. A complete list of medications must be obtained at each visit and questions as to reason of use need to be discussed. It is difficult to know every medication and the reason it is being prescribed. If the dental team has questions, they should not hesitate to contact the patient s physician for answers. The Dental History Form Dental offices often make an error in choosing not to complete a Dental History Form (see Appendix 4) for each new patient. As dental records are not required to be transferred between dentists, each dentist should obtain a dental history from the patient. This document should include information offered by the patient about current fears and concerns, as well as any recalled previous restorations, extractions, orthodontic treatment, oral habits and patient reactions to treatment, including anesthesia methods. Along with an oral history, dental offices are also beginning to use an intraoral camera to document the condition of the oral cavity at the patient s first appointment. The name(s) of previous dentists should be noted if the patient offers them. Once this baseline Dental History Form is completed, the patient should sign the form. This form should never be altered and should be kept in the clinical notes as a reference to previous treatments. The Informed Consent Form Before beginning any dental treatment, it is prudent to obtain a signed Informed Consent Form from the patient. Appendix 5 shows an example of a Treatment Plan Estimate that aids in the informed consent process. It is especially recommended for treatment that requires the use of anesthesia, is risky or invasive. Informed consent is given by competent adults when they are given sufficient knowledge (in understandable terms) about a specific procedure, including the benefits, risks (if any) and expected outcomes. The informed consent process also involves allowing the patient to ask questions about recommended treatments and available treatment options. For patients who are minors or mentally compromised, an adult guardian must sign on their behalf. Clinical situations when written consent is required include: use of general anesthesia; new drugs being prescribed; experimental treatments or clinical testing; minors being treated in a public program; treatment that is expected to last more than one year. Consent for treatment can also be given verbally. For example, when a patient makes an appointment for an examination and prophylaxis, the consent to treatment is implied. This type of consent is very popular in dentistry but is not as reliable in a court of law as an Informed Consent Form. Informed Refusal Forms should be obtained when a patient refuses a recommended treatment plan or necessary component of treatment (for example, refusal of diagnostic radiographs that are necessary to provide a susceptible 7

8 Standard of Care). It should also be noted if any educational brochures or materials are given to the patient. This informed refusal must be documented as it protects the office against the allegation of not fully disclosing the consequences of refusing or receiving treatment. The patient s reason for refusal should be documented on the signed form. Clinical Progress Notes This portion of the record offers a historical account of all treatment services. Basic charting procedures are employed to document diagnostic, preventive, and restorative treatment. Entries should include detailed information such as: preoperative vital signs, the procedure performed on the tooth/teeth numbers and surfaces, type and amount of anesthesia, dental materials used and how the patient tolerated the procedure. Additional entries can include details of telephone conversations, missed appointments, and home care instructions. More details about these entries are discussed later in the course. This information is always managed in a chronological format beginning with the first date of service to the latest contact made with the patient. These entries must use dental terminology and references that dental professionals can understand. This is important to show consistency should the records come into question, or when they have been transferred to a new dentist of record. See Appendix 6. Additional Components of the Patient Record Depending on the office preferences, additional forms may be included in the patient record. periodontal screening - used for adult patients that are showing signs of gingiva and bone recession treatment plan used to explain and prioritize work that needs to be completed signature on file allows the office to submit information for insurance claim processing; having this form on file eliminates the need for the patient to sign every form for the patient or family correspondence log used to document any written or oral correspondence with that patient, or treatment that concerns that patient As patients receive comprehensive dental treatment according to the Standard of Care, peripheral components also become a part of the complete patient record. These components include the previously mentioned, and purposefully separate financial records, all of the patient s radiographs, intraoral and extra-oral photographs, and any study models created for patient treatment. When a patient remains with the practice for several years, radiographs will accumulate. All radiographs are documentations of growth and treatment and they must be maintained. As space in the clinical chart may become limited, the office may keep these radiographs in a separate location in the office. These will often be filed by name or numbered and crossreferenced for easy retrieval. Study models may also be created for a variety of purposes and should also be kept as part of the record. As these larger components will not fit into a standard clinical chart, these are boxed and kept in a separate office location and cross-referenced by number or alpha order for easy retrieval. As they are created, the models are labeled with the patient s name and date. Reference should be made in the chart as to the location of any models. Steps in Documentation The patient chart is a legal representation of dental services. Information noted must be accurate, comprehensive, concise and current. During routine appointments, data entered includes all conditions present and dental treatment provided. Dental SOAP notes are written to improve communication among the entire team treating the patient by standardizing evaluation entries made in the dental charts. Each letter in SOAP is a specific heading in the notes: S refers to subjective, the purpose of the patient s dental visit. This is not meant for subjective statements from the dental team member. This section includes the description of symptoms in the patient s own words including: pain, what triggers the discomfort, what causes the discomfort to disappear, and the duration of 8

9 symptoms. This patient history will help when writing the objective statement. O refers to objective, unbiased observations by the dental team. Included under this heading would be things that can actually be felt, heard, measured, seen, smelled and touched. A refers to assessment, the diagnosis of the patient s condition done by the dentist. The diagnosis may be clear or there may be several diagnostic possibilities. P refers to the plan or proposed treatment, and is decided upon by the patient and the dentist. The plan may include radiographs, medications prescribed, dental procedures, patient referral to specialists and patient follow-up care instructions. A SOAP notation is usually not as detailed as a progress report and the usage of abbreviations is standard. Abbreviations will vary slightly from one practice to another, so it is important to use notations commonly used within the practice. Everyone within the practice should use the same abbreviations for continuity. Including detailed information in the clinical chart whenever patient contact is made ensures the dental team provides the best care possible and reduces questions concerning the treatment provided. The following information should always be recorded with any patient contact. Many offices use abbreviations when making entries. This is a common practice but should not ultimately decrease the quality or necessary amount of information to make a complete sequence of events. The following detailed list of information should be included in each clinical entry: Date This entry is always started with the full date in a month/day/year format of each patient visit. Reason for the visit Document the chief dental complaint, as well as any other concerns of the patient or guardian. This is the S of the SOAP documentation. Listening to the patient is part of the Standard of Care; documenting these discussions supports the delivery of quality dental care. Radiographs and other diagnostic tools Describe all radiographs taken. Include all other diagnostics used; for example, study casts, pulp test findings and photographs. Examination Provide a complete account of the oral cavity and document the findings. Oral exam is not descriptive enough as most dentists examine more than just the teeth. The charting should specify the tongue, lips, cheeks, palate and other soft tissues examined with the findings detailed. Include oral cancer screenings and periodontal probings, noting tooth mobility patterns and any abnormal conditions present. This is the O of the SOAP documentation. Document all diagnoses and discoveries stated by the dentist. All positive and negative results of treatment found during the examination must be noted. This is the A of the SOAP documentation. Treatment rendered According to the steps already done, a treatment plan will be created. This plan will be discussed with the patient. This is the P of the SOAP notes. As procedures are completed, each step should be dissected as much as possible during documentation. When a tooth is restored, simply noting #3 MOD is insufficient. Include details on whether anesthetic was used (include the type, quantity in number of carpules and applicable epinephrine ratio). If nitrous oxide was administered, note the concentration and duration of administration, including the patient s reaction. Note the type of restorative material used, including the type of base, liner or varnish if used and noting a shade if a tooth colored material was used. Document how the patient tolerated the procedure and describe any other incidents that were pertinent to the procedure. To illustrate an extraction appointment, simply noting Tooth #17 Ext. is insufficient. Notations should include applicable information such as ease of extraction (regular, dento-disection, surgical), gingival tissue flap required, bone recontouring on buccal or lingual, kind and number of sutures placed and whether there is need for removal. Always include notation on bleeding and coagulation. Instructions Outline any instructions given to the patient. Preoperative instructions may include 9

10 what the patient is to do prior to a particular dental appointment, such as refraining from eating 6 8 hours prior to a surgical procedure in which general anesthesia will be used. Never overestimate the ability of the patient to understand instructions, no matter how simple they may seem. Instructions are to be delivered verbally and in writing, and documented in the chart. If a pamphlet is provided, note it in the chart as supportive to home care instructions. Even simple directions on brushing and flossing should be cited, as should any instructions for a phone follow-up or a recare visit. Prescriptions Always document the full name of the drug prescribed, dosage amount, strength, duration, administration and amount of refills, if any. If a prescription is called in, this information must be entered in the patient s clinical chart. Discuss, inform, and document about any possible side effects to show that the patient was made aware of any ill effects. Laboratory Reports Always keep copies of the instructions given to the dental laboratory concerning the fabrication of patient appliances. This information will be used as reference to know chosen tooth shades and special instructions. Results Document when patients are satisfied or happy with a certain outcome. Conversely, document if the patient is dissatisfied with the treatment rendered, and note any steps taken to alleviate patient concerns or discomfort. Referral Simply noting a patient was referred out is insufficient. Instead, reference the consulting specialist by name and cite the reason for the referral. Usually, when a general dentist refers a patient to a specialist, the referring dentist is not held accountable for any negligence on the part of the specialist, provided the referrer has no control over and provides no direction on the mode of treatment used by the specialist. Followup with the specialist, and include all reports from consulting specialists in the patient chart. Telephone calls As a general rule, all telephone calls regarding patient care or financial transactions should be entered into the patient record. As conversations take place, the dental healthcare worker must take accurate, objective notes. These notes must be entered as soon as possible into the patient record as information can be lost or forgotten. Always give patients the opportunity to explain their concerns; never dismiss their questions. Caution must be exercised when discussing protected health information over the telephone. To maintain confidentiality, the patient, parent or legal guardian must be verified and addressed directly. Quotation marks ( ) are used as much as possible when making a documentation of an actual conversation. Identify the person being quoted by name should this person be a guardian, legal representative, medical doctor or insurance representative. Always hold telephone conversations out of earshot of other patients to maintain privacy. Recare/Recall Document when and why the patient is returning for treatment. If the patient fails to return for regularly scheduled prophylaxis or continuing treatment as instructed, it must be noted in their chart. In the event of a claim against the dentist, evidence of non-compliance from the patient may be labeled as contributory negligence by a court. This establishes that the patient has contributed to the alleged injuries and must likely accept some of the responsibility for an unsatisfactory treatment outcome. Other Important Documentation There is much debate among attorneys and dentists regarding who should make the entries in the dental record components. Each member of the dental team is responsible for portions of the documentation. The business assistant will document telephone calls; prescription changes; and canceled, changed, and failed appointments. The clinical assistant and/or hygienist will enter the patient s comments, concerns, and disposition; vital signs; medical history notations; exposed radiographs and other diagnostic tools used; details of treatment performed; instructions given to the patient; and any other notes relevant to the patient s time in the dental chair. All entries must be initialed and/or signed by the responsible dental team member. Charting of the actual treatment rendered is ultimately the responsibility of the dentist. When a dentist decides not to make their own entries, it should be dictated what to write. 10

11 Regardless of whether the entry is dictated or not, and which dental team member composed the entry, the dentist must review the contents of all entries for accuracy and then sign and/or initial them. Documenting in the Clinical Record The dental healthcare professional must always think before making a permanent entry in a patient s financial or clinical record, especially if the documentation is complex in nature. All hand written entries should be made in permanent, preferably black ink. Preliminary notes may be written on a separate sheet and arranged for organization, then transcribed into the proper record component. The separate sheet must then be destroyed according to HIPAA regulations if it contains obvious patient identified information. It is best to document while the patient is still in the office, because as time passes, memory of the treatment or conversation may be forgotten. A dental record is the single most important source of evidence in a liability claim. Most attorneys contend that if an occurrence is not cited in the chart, it never happened, and juries are not inclined to trust the memories of the dental team. As noted previously in the SOAP notes, all entries from the dental team must remain objective in nature. Only enter what happened and do not include subjective information or opinions. Limit all comments to necessary information about the patient s treatment, and avoid making unnecessary negative comments. The patient can request copies of their complete record at any time and, should the record appear in a court case, disparaging remarks could alienate the judge or jury. For example, do not write, Patient seemed angry. A better choice of words would be, Patient said, I am tired of dealing with this sensitive tooth. Part of the legal duty to the patient is to maintain a neat, legible patient record to provide continuity of care. Accurate and legible records discourage litigation. Illegible and incomplete entries can compromise the defense of the dentist. Consistency is also very important. If abbreviations are used they must be standard or universal. Otherwise, charted abbreviations are open to interpretation by attorneys, and the definitions they suggest may not be in the best interest of the dental practice. When a mistake is realized, it becomes necessary to make a correction to an entry in the patient clinical chart. When handled properly, corrections do not compromise the integrity of the patient record. The following steps are to be followed in a correction: A single line is drawn through the incorrect entry with an ink pen. The date and initials of the team member(s) are included for verification. Write the correct entry on the next available line in the chart. Maintain the current spacing in the chart for legibility and uniformity. The new entry must be dated and initialed. The important factor in making a change is that the original entry can still be read. An entry should never be obliterated. Markers or correction fluid should never be used in any part of an entry. A correction becomes an alteration when the author, in hindsight, makes a correction to try to enhance or add to the original entry to his or her own benefit. An alteration of any component of the record also may be defined as damaging, destroying, concealing, or obscuring a record, whether knowingly; willfully; or neither. The dental team must avoid leaving empty lines between entries; it may be too tempting to add something at a later date that could be construed as an alteration. The team must also avoid squeezing in words or phrases, which may invite suspicion and damage credibility, even if done without malice. If an addition needs to be entered at a later date, the entry should be made as others are chronologically entered and then referred to the date of the visit in question. If a court suspects an alteration of the record, expert document examiners may be called upon to study the entries. These professionals can discern if an entry was made at a later date, even if the same author and pen was used. They look at factors such as the dryness of the ink (which identifies entries that were made at different times), the pressure used while writing, differences in surfaces where the entry was written and the slant and speed of writing. 11

12 Dental Records and the Computer Computers are now an integral part of most dental offices. When utilized properly, computerized dental record software in a window or tabbed-typed format can aid in efficiency. Record components can be printed accurately and efficiently to aid in patient education and obtaining proper consent. Issues of chart space for all paper documents and radiographs can be resolved with digital, computerized documents. Easily stored within the office computer, the need for separate storage space and cross referencing is not an issue. Transfer and copying to and from other dental professionals is also streamlined. According to the American Dental Association, dental offices that rely on computers and paperless dental records must perform daily backups of system data. It is important to employ a reliable backup system for all patient records. Automated electronic backup of information can be used to protect information every day and the office/dentist will receive automatic alerts every time the process is completed. It is best if data and application backups can be at offsite locations, protected from fire, flood, and violent impact. Additionally, HIPAA security requirements include provisions concerning backup. Electronic communications for patient-care purposes must meet HIPAA standards. Confidentiality remains a primary concern, and certain steps must be taken to ensure that patient information is neither shared nor accessible to unauthorized parties. Also, the authenticity of the original record must be maintained with electronic transmissions. The dental office must make sure that their utilized dental software package provides confidentiality and the ability to retain the integrity of the original records. When selecting a computerized charting program, the inability to change entries at a later date must be considered. Once an entry is made, the only way to change that entry should be to amend it in the form of an addition; once entered, an existing entry should be inalterable. Retention of Records Regardless of any particular state s laws regarding record retention, it is recommended that all dental records, including radiographs, be kept indefinitely. If space is a concern, consider alternative methods of storage. Old, inactive record components can be committed to microfilm or microfiche or scanned into electronic documents. Some companies specialize in record retention; they can help with storage or the creation of scans, microfilms or microfiches from paper records. If a practice opts to employ a company to properly and legally dispose of old, inactive charts, these companies should furnish a Certificate of Destruction. Dental Malpractice All practitioners are open to the possibility of claims that question the quality of their work. Dental malpractice is the common term used to describe professional negligence involving a dentist. Positive and effective patient communication is the key to reducing the risk of malpractice claims and a vital tool for preventing errors. Dental professionals must not guarantee results or make promises about treatment outcome. Also, patients tend to not file claims against people they like, so developing a good relationship with patients may actually help protect against litigation. Everyone on the dental team is responsible for the quality of the patient relationship. Cases have been reported in which patients decided not to file a claim against the dentist simply because they liked a staff member or felt that the dental team was polite. Patients do not expect their dentists to be perfect, but they do expect them to show compassion and honesty rather than indifference. Most medical and dental malpractice claims arise from an unfavorable interaction with the dentist and not necessarily from a poor treatment outcome. As reported in RDH Magazine, the ADA questioned several major malpractice carriers concerning frequent areas of complaint. The number one record keeping error they identified was the absence of a treatment plan, and the number two error was a failure to update medical history forms. An interesting fact, also included, was that one of the top reasons that malpractice cases are lost by a practice is that someone in the practice went back and altered the chart a serious error in judgment as this can be detected by professional analysts. If any team member is notified that they are involved in a lawsuit, they must immediately inform 12

13 the dentist. The patient must not be contacted in any way. The patient record must not be altered no matter what. If anything is remembered that a staff member believes would be important to add, an addendum can be created on a separate sheet of paper. Again, copies of any record component must never be sent to anyone without first informing the dentist and verifying there is a signed Release of Information form in the chart. The dentist must be aware of all copies of the patient records that are transferred or sent out, regardless of the reason. Documentation of conversations with attorneys and/or the malpractice insurer should be maintained in a file separate from the clinical chart, as should any lawsuit correspondence or letters from attorneys and/or the malpractice insurance company. It is important to be aware if a malpractice suit is filed, members of the team other than the dentist may also be named. Although most malpractice policies carried by the dentist have limited coverage of team members, it is imperative for all clinical team members to carry individual liability coverage. The statute of limitations for filing a lawsuit varies from state to state. Each dental practice should know the limitations enforced in their state. Generally, plaintiffs must file within 5 years of the last date of service or within 3 years of the date of discovery. As a point of reference, it takes approximately 7 years to settle a claim. HIPAA The rules and regulations of the federal Health Insurance Portability and Accountability Act (HIPAA) apply to health care providers (including dentists) who submit claims electronically to health plans, and to health care clearinghouses for which the U.S. Department of Health and Human Services has established a standard. As stated in the title, it focuses on portability and accountability. The portability provision is meant to guarantee that an employee can still receive health insurance coverage should they change jobs. The accountability section states who is responsible for specific healthcare activities. This act was designed to improve portability and continuity of health insurance coverage in both group and individual markets; to combat waste, fraud, and abuse in health insurance and health care delivery; to promote the use of medical saving accounts; to improve access to long-term care services and coverage; and to simplify the administration of health insurance. Administrative simplification was created to make the business practices behind the healthcare easier by the development of standards for transaction code sets, privacy of protected health information (PHI), and national provider identifiers. HIPAA Intent The intent of HIPAA is to protect patient privacy and provide security of health records without impeding patient care. It was not intended to discourage smaller dental practices from utilizing electronic transactions. Because violation penalties can be significant, dental offices must understand how to protect the privacy and security of PHI. Dental team members also should familiarize themselves with state privacy regulations. Federal HIPAA privacy and security regulations usually preempt state law, unless state laws require greater patient protection than HIPAA. The implementation of HIPAA has been an opportunity for many entrepreneurs to present the dental office with costly consultations and forms for compliance. The purchase of these services and materials is not necessary to comply with HIPAA. The American Dental Association has a compact and reasonable publication designed to ensure compliance. The ADA s HIPAA Privacy and Security Kits ( org/productguide/p/1070/practice-management/ HIPAA-Privacy-Documentation-Kit-for-Healthcare- Providers)%20or%20by%20telephone%20 at% ) can be ordered from the American Dental Association. As the best way to ensure compliance, every U.S. dental office should have a copy of the Health Insurance Portability and Accountability Act, familiarize team members with its rules, and be certain that all staff members know how it is implemented in their practice setting. HIPAA Compliance Regardless of whether an office is paper only, the office must comply with both HIPAA s Privacy 13

14 Rule and its Security Rule. If a billing service is used that converts the paper forms to electronic versions for processing, the dentist must have an agreement with that service to protect the patient health information. A signed Participating Provider Agreement must be obtained with an insurance company that must be HIPAAcompliant. Penalties for noncompliance may range from monetary fines to jail time. Due to the confidentiality of medical information and the dentist-patient relationship, all requests for medical consultation information on patients should be made in writing, with the patient s signature authorizing the release of the information. In some cases, the release form may be sent to the physician with the patient or through the mail. In other cases, to save time, the form may be sent by facsimile (fax) and returned in this manner. The electronic transmission of PHI is covered by HIPAA and the dental practice must have a one-time consent form signed by the patient for the transmission of this information, in addition to the release that must be signed for the physician to release information to the dental practice. When sharing patient information between dental and medical professionals, it is best to adopt a minimum necessary policy. This means that only the information pertinent and necessary for patient treatment should be shared and secondary information should remain confidential. Standard Transactions Standard electronic transactions covered by HIPAA include: claims or equivalent encounters; claim attachments; claim status inquiries; eligibility inquiries; payment or remittance advice; coordination or explanation of benefits; first report of injury for Worker s Compensation; enrollment or disenrollment in a health plan; and notice of premium payment. Privacy Rule Compliance In order to be HIPAA-compliant, dental offices must: adopt a written privacy policy; designate a Privacy Officer; designate a Privacy Contact person (often the same person who serves as Privacy Officer); develop the required forms (the American Dental Association and other sources offer these materials); display the office s Notice of Privacy Practices; provide copies of the Notice of Privacy Practices to patients; make a good faith effort to receive written acknowledgement from patients that they received the office s Notice of Privacy Practices; protect patient privacy by taking reasonable precautions to prevent against inadvertent disclosure; protect patient privacy by adhering to the minimum necessary rule when using and disclosing patient information; train staff in privacy policy and practices; enter into business associate agreements, if necessary (see below); and implement the necessary physical and technical safeguards to protect patient information. Patient clinical records are often pulled from the filing cabinet or retrieved from the computer database and reviewed before the patient arrives. These files should be protected from the view of other patients as they move through the office. This information must only be displayed where authorized personnel have viewing access. Computer monitors should never be directed toward the patient s view in the treatment room or the business office areas. The daily schedule should not be on display in the treatment area nor should it be left up on the screen. Just as with the patient s record, appointments times should not be on public display. This is an often overlooked aspect of protecting patient s privacy. Business Associates HIPAA allows for the dental office to designate business associates (BA) to aid in the care of the patient. The BA is a person or entity that, on behalf of the office, performs or assists in the performance of a function or activity involving the use or disclosure of PHI. HIPAA considers a BA to be any third party that a health care provider shares PHI with so that the associates may complete the services for 14

15 which they have been hired. Further, any role of a third party with access to PHI must be clearly documented. In 2013, a HIPAA regulation went into effect that further regulates any entity that is considered a BA to the dental office. The following are not considered to be Business Associates: a member of the staff such as an employed dental associate, assistant, receptionist or hygienist; the U.S. Postal Service; or a janitorial service. Examples of a BA include: dental/medical labs attorney accountant billing service answering service computer support staff Security Rule Compliance The HIPAA Security Rule defines highly-detailed standards for the integrity, availability and confidentiality of electronic protected health information (EPHI), and addresses both external and internal security issues. assess potential risks and vulnerabilities; protect against threats to information security or integrity, and guard against unauthorized use or disclosure; implement and maintain security measures that are appropriate to their needs, capabilities, and circumstances; and ensure compliance with these safeguards by all staff. The Security Rule comprises three separate standards. Administrative Safeguards: This first standard, which makes up half of the complete standard, limits information access to appropriate parties and guards information from all others. The office policy must include documented policies and procedures for day-to-day operations; address the conduct and access of workforce members to EPHI; and describe the selection, development, and use of security controls. Physical Safeguards: Physical safeguards prevent unauthorized individuals from gaining access to EPHI. Technical Safeguards: This third standard involves using technology to protect and control access to EPHI. For information on the various components of each of these Security Rule standards, visit securityrule/index. A HIPAA rule went into effect March 26, 2013 and covered entities, including covered dental practices, will have an additional 180 days, or until September 23, 2013 to comply with applicable requirements. The regulations: enhance HIPAA enforcement expand many HIPAA requirements to business associates such as contractors and subcontractors that receive protected health information expand individuals rights to receive electronic copies of their health information and to restrict disclosures to a health plan concerning treatment for which the provider has been paid out of pocket in full modify rules that apply to marketing and fundraising communications and the sale of protected health information expand the definition of health information to include genetic information clarify when data breaches must be reported to the HHS Office for Civil Rights Much has changed in health care since HIPAA was enacted over fifteen years ago, HHS Secretary Kathleen Sebelius said in a news release. The new rule will help protect patient privacy and safeguard patients health information in an ever expanding digital age. Summary Referred to as Standard of Care, the legal duty of a dentist requires exercising the degree of skill and care that would be exhibited by other prudent dentists faced with the same patientcare situation. Primarily, the goal of keeping good dental records is to maintain continuity of care. Diligent and complete documentation and charting procedures are essential to fulfilling the Standard of Care. Secondly, because dental records are considered legal documents they help protect the interest of the dentist and/or the 15

16 patient by establishing the details of the services rendered. Patients today are better educated and more assertive than ever before, and dentists must be equipped to protect themselves against malpractice claims. Every record component must be handled as if it could be summoned to a court room and scrutinized by an attorney, judge or jury. Complete, accurate, objective and honest entries in a patient record is the only way to defend against any clinical and/or legal problems that might arise. Most medical and dental malpractice claims arise from an unfavorable interaction with the dentist and not from a poor treatment outcome. By implementing the suggestions mentioned in this course, dental healthcare professionals can minimize the legal risks associated with the delivery of dental care to promote greater understanding for patients of their rights and privileges to their complete record. 16

17 Appendix 1 17

18 Appendix 2 18

19 Appendix 3 19

20 Appendix 4 20
21 Appendix 5 21
22 Appendix 6 22
23 Course Test Preview To receive Continuing Education credit for this course, you must complete the online test. Please go to: 1. The Standard of Care includes. a. listening to the patient s complaints b. giving the patient an appointment the same day they call c. taking the patient home because they missed the bus d. All of the above. 2. A patient walks into the office and demands his/her radiographs. The protocol is to. a. give them to the patient since they own them b. obtain a release and give them a copy of the radiographs c. tell them they cannot have them because they belong to the dentist d. None of the above. 3. The belongs in the patient s clinical dental record. a. ledger card b. insurance payment vouchers c. laboratory report d. All of the above. 4. It is known for a fact that Patient X never showed up for dental appointments, even after receiving a confirmation call. The protocol is to. a. pull the chart and document if she fails to show b. pull the chart only if they show this time c. document in the chart that the patient is a chronic no show and that the dentist can t stand this behavior d. book an additional patient during this appointment time 5. is NOT a safeguard of the HIPAA Security Rule. a. Technical safeguards b. Physical safeguards c. Practice safeguards d. Administrative safeguards 6. It is important to maintain complete dental records because. a. it will help maintain continuity of care if the patient decides to leave your practice b. it provides a means of communication between the dentist and any other health care provider for proper patient care c. the records are a legal document and may be needed in a lawsuit d. All of the above. 7. If needed, dental entries should be corrected by. a. a thick black line covering the incorrect information b. in red marker c. with correction fluid d. with a thin line through the incorrect information 23
24 8. To ensure that the dental record is kept in proper order. a. only the dentist should write in it b. only one person should be responsible for proper documentation c. everyone is equally responsible for proper documentation d. all entries should be made in the same color 9. It is best to document patient treatment in the patient s dental record. a. at the end of the day when there are no distractions b. immediately following treatment before patient dismissal c. as billing is processed d. in pencil for easy correction 10. The is a component of the patient dental record. a. clinical chart b. patient s radiographs c. periodontal screening d. All of the above. 11. The outside cover of the chart should only display the patient s name and/or the account number. All medical notations belong inside the chart for only authorized dental team members to see. a. The first statement is true. The second statement is false. b. The first statement is false. The second statement is true. c. Both statements are true. d. Both statements are false. 12. Patient Y has not received treatment since their last recare appointment 6 months ago. The dental team must. a. inquire about their medical history b. make no changes to the medical history unless an issue is mentioned c. ask the patient to update the medical history, inquire about the changes and record findings about the updated history d. take a whole new medical history every 6 months 13. The owner of the patient record is. a. HIPAA b. the patient or guardian c. the courts d. the dentist 14. An attorney requests original records because he s representing a patient of record. The protocol is to. a. send the originals as requested and keep copies b. call the patient to ask if originals are necessary c. send copies regardless of the demand d. ask the attorney if this is due to formal complaint against the dentist 24
25 15. Dental offices that submit insurance claims on paper do not need to be concerned with the HIPAA regulations. The dental practice must have a one-time consent form signed by the patient for the electronic transmission of personal information. a. The first statement is true. The second statement is false. b. The first statement is false. The second statement is true. c. Both statements are true. d. Both statements are false. References 1. ADA Council on Dental Practice (2010) Dental Records. (Accessed February 2013.) 2. ADA Council on Dental Practice (2003) Emergency Planning & Disaster Recovery in the Dental Office. (Accessed March 2013.) 3. ADA Legal Adviser - April HIPAA 20 Questions: Answers to Your Inquires About The Privacy Regulation. (Accessed June 2003.) 4. Bird, D. L. & Robinson, D. S. (2012.) Torres & Ehrlich s Modern Dental Assisting., 10th ed. St. Louis: Saunders Elsevier. 5. Coleman H. & Stannard D. (2006) For The Record. Clinical Risk. The Royal Society of Medicine Press, (12) Finkbeiner, B.L. and Finkbeiner, C.A. (2010) Practice Management for the Dental Team, 7th. ed. St. Louis: Mosby Elsevier. 7. FreshPatients.com. August 6, (Accessed Jan. 10, 2010.) 8. Gaylor, L. J. (2012) The Administrative Dental Assistant, 3rd ed. St. Louis: Saunders Elsevier. 9. Glasscoe-Watterson, D. (July 2009) Documentation Dilemma, RDH. Pg HIPAAdvisory: the HIPAA Security Rule Overview. (Accessed February 2013.) 11. HIPAA Security Rule FAQ. (Accessed July 2005.) Knowledge based clinical dental records management systems. 12. Palmer, Craig, New HIPAA rules issued. ADA News. January 28, Weil, S. HIPAA Security Rule. (Accessed August 2005.) About the Author Wilhemina Leeuw, MS, CDA Wilhemina Leeuw is a Clinical Assistant Professor of Dental Education at Indiana University Purdue University, Fort Wayne. A DANB Certified Dental Assistant since 1985, she worked in private practice over twelve years before beginning her teaching career in the Dental Assisting Program at IPFW. She is very active in her local and Indiana state dental assisting organizations. Prof. Leeuw s educational background includes dental assisting - both clinical and office management, and she received her Master s degree in Organizational Leadership and Supervision. She is also the Continuing Education Coordinator for the American Dental Assistants Association. 25
ACKNOWLEDGEMENT OF RECEIPT OF WESTERN DENTAL S NOTICE OF PRIVACY PRACTICE
 ACKNOWLEDGEMENT OF RECEIPT OF WESTERN DENTAL S NOTICE OF PRIVACY PRACTICE By signing this document, I acknowledge that I have received a copy of Western Dental s Joint Notice of Privacy Practices. Name
ACKNOWLEDGEMENT OF RECEIPT OF WESTERN DENTAL S NOTICE OF PRIVACY PRACTICE By signing this document, I acknowledge that I have received a copy of Western Dental s Joint Notice of Privacy Practices. Name
HIPAA Notice of Privacy Practices
 HIPAA Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Notice
HIPAA Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Notice
Salt Lake Community College Employee Health Care Benefits Plan Notice of Privacy Practices
 THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. Date: June 1, 2014 Salt Lake Community College
THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. Date: June 1, 2014 Salt Lake Community College
ELECTRONIC HEALTH RECORDS
 ELECTRONIC HEALTH RECORDS Understanding and Using Computerized Medical Records CHAPTER TEN LESSON ONE Privacy and Security of Health Records Understanding HIPAA HIPAA: acronym for Health Insurance Portability
ELECTRONIC HEALTH RECORDS Understanding and Using Computerized Medical Records CHAPTER TEN LESSON ONE Privacy and Security of Health Records Understanding HIPAA HIPAA: acronym for Health Insurance Portability
Chapter 10: The Dental Record
 Chapter 10: The Dental Record Protecting health information is the right thing to do, and it is also good risk management. 78 The recording of accurate patient information is essential to dentistry. The
Chapter 10: The Dental Record Protecting health information is the right thing to do, and it is also good risk management. 78 The recording of accurate patient information is essential to dentistry. The
HIPAA Omnibus Notice of Privacy Practices Effective Date: March 03, 2012 Revised on: July 1, 2015
 HIPAA Omnibus Notice of Privacy Practices Effective Date: March 03, 2012 Revised on: July 1, 2015 Mobile Physician Group PC 231 High Street Suite 1, Mount Holly, NJ 08060 1-855-MPG-DOCS THIS NOTICE DESCRIBES
HIPAA Omnibus Notice of Privacy Practices Effective Date: March 03, 2012 Revised on: July 1, 2015 Mobile Physician Group PC 231 High Street Suite 1, Mount Holly, NJ 08060 1-855-MPG-DOCS THIS NOTICE DESCRIBES
HIPAA Notice of Privacy Practices - Sample Notice. Disclaimer: Template Notice of Privacy Practices (45 C.F.R. 164.520)
") HIPAA Notice of Privacy Practices - Sample Notice Disclaimer: Template Notice of Privacy Practices (45 C.F.R. 164.520) The information provided in this document does not constitute, and is no substitute
HIPAA Notice of Privacy Practices - Sample Notice Disclaimer: Template Notice of Privacy Practices (45 C.F.R. 164.520) The information provided in this document does not constitute, and is no substitute
NOTICE OF HEALTH INFORMATION PRIVACY PRACTICES (HIPAA)
") NOTICE OF HEALTH INFORMATION PRIVACY PRACTICES (HIPAA) THIS NOTICE OF PRIVACY PRACTICES DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
NOTICE OF HEALTH INFORMATION PRIVACY PRACTICES (HIPAA) THIS NOTICE OF PRIVACY PRACTICES DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
SCHOOL DISTRICT OF BLACK RIVER FALLS HIPAA PRIVACY AND SECURITY POLICY
 SCHOOL DISTRICT OF BLACK RIVER FALLS HIPAA PRIVACY AND SECURITY POLICY School Board Policy 523.5 The School District of Black River Falls ( District ) is committed to compliance with the health information
SCHOOL DISTRICT OF BLACK RIVER FALLS HIPAA PRIVACY AND SECURITY POLICY School Board Policy 523.5 The School District of Black River Falls ( District ) is committed to compliance with the health information
NOTICE OF PRIVACY PRACTICES Walter Chiropractic Clinic, 5219 Peters Creek Rd Ste 5, Roanoke VA 24019
 Effective Date: 5/18/15 NOTICE OF PRIVACY PRACTICES Walter Chiropractic Clinic, 5219 Peters Creek Rd Ste 5, Roanoke VA 24019 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED
Effective Date: 5/18/15 NOTICE OF PRIVACY PRACTICES Walter Chiropractic Clinic, 5219 Peters Creek Rd Ste 5, Roanoke VA 24019 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED
HIPAA POLICIES & PROCEDURES AND ADMINISTRATIVE FORMS TABLE OF CONTENTS
 HIPAA POLICIES & PROCEDURES AND ADMINISTRATIVE FORMS TABLE OF CONTENTS 1. HIPAA Privacy Policies & Procedures Overview (Policy & Procedure) 2. HIPAA Privacy Officer (Policy & Procedure) 3. Notice of Privacy
HIPAA POLICIES & PROCEDURES AND ADMINISTRATIVE FORMS TABLE OF CONTENTS 1. HIPAA Privacy Policies & Procedures Overview (Policy & Procedure) 2. HIPAA Privacy Officer (Policy & Procedure) 3. Notice of Privacy
GONZABA MEDICAL GROUP PATIENT REGISTRATION FORM
 GONZABA MEDICAL GROUP PATIENT REGISTRATION FORM DATE: CHART#: GUARANTOR INFORMATION LAST NAME: FIRST NAME: MI: ADDRESS: HOME PHONE: ADDRESS: CITY/STATE: ZIP CODE: **************************************************************************************
GONZABA MEDICAL GROUP PATIENT REGISTRATION FORM DATE: CHART#: GUARANTOR INFORMATION LAST NAME: FIRST NAME: MI: ADDRESS: HOME PHONE: ADDRESS: CITY/STATE: ZIP CODE: **************************************************************************************
APPENDIX 1: Frequently Asked Questions
 APPENDIX 1: Frequently Asked Questions Practice Name Q: What is the HIPAA Privacy Rule? A: The HIPAA Privacy Rule controls the use and disclosure of what is known as Protected Health Information (PHI).
APPENDIX 1: Frequently Asked Questions Practice Name Q: What is the HIPAA Privacy Rule? A: The HIPAA Privacy Rule controls the use and disclosure of what is known as Protected Health Information (PHI).
Sarasota Personal Medicine 1250 S. Tamiami Trail, Suite 202 Sarasota, FL 34239 Phone 941.954.9990 Fax 941.954.9995
 Sarasota Personal Medicine 1250 S. Tamiami Trail, Suite 202 Sarasota, FL 34239 Phone 941.954.9990 Fax 941.954.9995 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY
Sarasota Personal Medicine 1250 S. Tamiami Trail, Suite 202 Sarasota, FL 34239 Phone 941.954.9990 Fax 941.954.9995 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY
Notice of Privacy Practices. Human Resources Division Employees Benefits Section
 Notice of Privacy Practices Human Resources Division Employees Benefits Section THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
Notice of Privacy Practices Human Resources Division Employees Benefits Section THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
IF YOU HAVE ANY QUESTIONS ABOUT THIS NOTICE OR IF YOU NEED MORE INFORMATION, PLEASE CONTACT OUR PRIVACY OFFICER:
 NOTICE OF PRIVACY PRACTICES COMPLETE EYE CARE THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED OR DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
NOTICE OF PRIVACY PRACTICES COMPLETE EYE CARE THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED OR DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Harris County - Texas HIPAA Notice of Privacy Practices
 Harris County - Texas HIPAA Notice of Privacy Practices Effective Date: September 23, 2013. THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
Harris County - Texas HIPAA Notice of Privacy Practices Effective Date: September 23, 2013. THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
POLICY STATEMENT 5.17
 POLICY STATEMENT 5.17 DENTAL RECORDS 1 (Including ADA Guidelines for Dental Records) 1. Introduction 1.1 Dentists have a professional and a legal obligation to maintain clinically relevant, accurate and
POLICY STATEMENT 5.17 DENTAL RECORDS 1 (Including ADA Guidelines for Dental Records) 1. Introduction 1.1 Dentists have a professional and a legal obligation to maintain clinically relevant, accurate and
Northwest Cardiology Associates 400 W. Northwest Hwy Barrington, IL 60010 847.382.4600 Fax 847.382.1771. HIPAA Notice of Privacy Practices ( Notice )
") Northwest Cardiology Associates 400 W. Northwest Hwy Barrington, IL 60010 847.382.4600 Fax 847.382.1771 HIPAA Notice of Privacy Practices ( Notice ) THIS NOTICE DESCRIBES HOW INFORMATION ABOUT YOU MAY
Northwest Cardiology Associates 400 W. Northwest Hwy Barrington, IL 60010 847.382.4600 Fax 847.382.1771 HIPAA Notice of Privacy Practices ( Notice ) THIS NOTICE DESCRIBES HOW INFORMATION ABOUT YOU MAY
DISCLAIMER HEALTH INFORMATION PRIVACY POLICIES & PROCEDURES
 DISCLAIMER This web site is provided for information and education purposes only. No doctor/patient relationship is established by your use of this site. No diagnosis or treatment is being provided. The
DISCLAIMER This web site is provided for information and education purposes only. No doctor/patient relationship is established by your use of this site. No diagnosis or treatment is being provided. The
Jerry M. Ruhl Ph.D. Clinical Psychologist (Texas #34359) 5200 Montrose Blvd. Houston, TX 77006
 5200 Montrose Blvd. Houston, TX 77006") Jerry M. Ruhl Ph.D. Clinical Psychologist (Texas #34359) 5200 Montrose Blvd. Houston, TX 77006 CELL (937) 684-7746 PLEASE USE THIS NUMBER TO SCHEDULE OR CHANGE APPOINTMENTS INFORMED CONSENT FOR TREATMENT
Jerry M. Ruhl Ph.D. Clinical Psychologist (Texas #34359) 5200 Montrose Blvd. Houston, TX 77006 CELL (937) 684-7746 PLEASE USE THIS NUMBER TO SCHEDULE OR CHANGE APPOINTMENTS INFORMED CONSENT FOR TREATMENT
HIPAA NOTICE OF PRIVACY PRACTICES
 HIPAA NOTICE OF PRIVACY PRACTICES Human Resources Department 16000 N. Civic Center Plaza Surprise, AZ 85374 Ph: 623-222-3532 // Fax: 623-222-3501 TTY: 623-222-1002 Purpose of This Notice This Notice describes
HIPAA NOTICE OF PRIVACY PRACTICES Human Resources Department 16000 N. Civic Center Plaza Surprise, AZ 85374 Ph: 623-222-3532 // Fax: 623-222-3501 TTY: 623-222-1002 Purpose of This Notice This Notice describes
UNITED CEREBRAL PALSY OF NORTHWEST MISSOURI NOTICE OF PRIVACY PRACTICES EFFECTIVE DATE: OCTOBER 22, 2014
 UNITED CEREBRAL PALSY OF NORTHWEST MISSOURI NOTICE OF PRIVACY PRACTICES EFFECTIVE DATE: OCTOBER 22, 2014 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
UNITED CEREBRAL PALSY OF NORTHWEST MISSOURI NOTICE OF PRIVACY PRACTICES EFFECTIVE DATE: OCTOBER 22, 2014 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
DALLAS ALLERGY & ASTHMA CENTER
 DALLAS ALLERGY & ASTHMA CENTER Gary N. Gross, MD Michael E. Ruff, MD 5499 Glen Lakes Dr., Suite 100 Dallas, TX 75231 Dania A. Wierzbicki, MD Phone: (214) 691-1330 Jane Zepeda, PA-C FAX: (214) 691-6405
DALLAS ALLERGY & ASTHMA CENTER Gary N. Gross, MD Michael E. Ruff, MD 5499 Glen Lakes Dr., Suite 100 Dallas, TX 75231 Dania A. Wierzbicki, MD Phone: (214) 691-1330 Jane Zepeda, PA-C FAX: (214) 691-6405
AVE MARIA UNIVERSITY HIPAA PRIVACY NOTICE
 AVE MARIA UNIVERSITY HIPAA PRIVACY NOTICE This Notice of Privacy Practices describes the legal obligations of Ave Maria University, Inc. (the plan ) and your legal rights regarding your protected health
AVE MARIA UNIVERSITY HIPAA PRIVACY NOTICE This Notice of Privacy Practices describes the legal obligations of Ave Maria University, Inc. (the plan ) and your legal rights regarding your protected health
Notice of Privacy Practices
 Notice of Privacy Practices Effective September 20, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
Notice of Privacy Practices Effective September 20, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
HIPAA Policies and Procedures
 HIPAA Policies and Procedures William T. Chen, MD, Inc. General Rule 164.502 A Covered Entity may not use or disclose PHI except as permitted or required by the privacy regulations. Permitted Disclosures:
HIPAA Policies and Procedures William T. Chen, MD, Inc. General Rule 164.502 A Covered Entity may not use or disclose PHI except as permitted or required by the privacy regulations. Permitted Disclosures:
NOTICE OF PRIVACY PRACTICES
 Effective Date: September 23, 2013 THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. OUR PLEDGE
Effective Date: September 23, 2013 THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. OUR PLEDGE
NOTICE OF PRIVACY PRACTICES ILLINOIS EYE CENTER
 NOTICE OF PRIVACY PRACTICES ILLINOIS EYE CENTER THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED OR DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
NOTICE OF PRIVACY PRACTICES ILLINOIS EYE CENTER THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED OR DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
NOTICE OF PRIVACY PRACTICES FOR OUR PATIENTS POTOMAC PHYSICIAN ASSOCIATES, P.C.
 NOTICE OF PRIVACY PRACTICES FOR OUR PATIENTS POTOMAC PHYSICIAN ASSOCIATES, P.C. THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED OR DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
NOTICE OF PRIVACY PRACTICES FOR OUR PATIENTS POTOMAC PHYSICIAN ASSOCIATES, P.C. THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED OR DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
HIPAA Notice of Privacy Practices
 HIPAA Notice of Privacy Practices Hilton-Diminick Orthodontic Associates, P.C. This notice describes how medical information about you may be used and disclosed and how you can get access to this information.
HIPAA Notice of Privacy Practices Hilton-Diminick Orthodontic Associates, P.C. This notice describes how medical information about you may be used and disclosed and how you can get access to this information.
WELCOME TO PCCMA. We look forward to being of service to you and helping you to be healthier in the future.
 Phone: 717-234-2561 Franklyn J. Myers, III, M.D., F.C.C.P. Alexis B. Aaronson, M.S.N, C.R.N.P. Michele M. Knepper, C.R.N.P. WELCOME TO PCCMA Welcome to our practice. We are specialists in the treatment
Phone: 717-234-2561 Franklyn J. Myers, III, M.D., F.C.C.P. Alexis B. Aaronson, M.S.N, C.R.N.P. Michele M. Knepper, C.R.N.P. WELCOME TO PCCMA Welcome to our practice. We are specialists in the treatment
USES AND DISCLOSURES OF HEALTH INFORMATION
 HIPAA Privacy Policy NOTICE OF PRIVACY PRACTICES This notice describes how health information about you may be used and disclosed. Please review carefully. The privacy of your health information is important
HIPAA Privacy Policy NOTICE OF PRIVACY PRACTICES This notice describes how health information about you may be used and disclosed. Please review carefully. The privacy of your health information is important
Self-study instructions for Risk management: a practical guide for dentists
 Self-study instructions for Risk management: a practical guide for dentists 1. Read the attached document, Risk management: a practical guide for dentists. 2. Answer the questions in the quiz by circling
Self-study instructions for Risk management: a practical guide for dentists 1. Read the attached document, Risk management: a practical guide for dentists. 2. Answer the questions in the quiz by circling
HIPAA Notice of Privacy Practices
 HIPAA Notice of Privacy Practices Date of Last Revision: 09/20/2013 Effective Date: Immediately THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
HIPAA Notice of Privacy Practices Date of Last Revision: 09/20/2013 Effective Date: Immediately THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
Health Insurance Portability and Accountability Policy 1.8.4
 Health Insurance Portability and Accountability Policy 1.8.4 Appendix C Uses and Disclosures of PHI Procedures This Appendix covers procedures related to Uses and Disclosures of PHI. Disclosures to Law
Health Insurance Portability and Accountability Policy 1.8.4 Appendix C Uses and Disclosures of PHI Procedures This Appendix covers procedures related to Uses and Disclosures of PHI. Disclosures to Law
HIPAA Privacy Policies & Procedures
 HIPAA Privacy Policies & Procedures This sample HIPAA Privacy Policies & Procedures document will help you with your HIPAA Privacy compliance efforts. This document addresses the basics of HIPAA Privacy
HIPAA Privacy Policies & Procedures This sample HIPAA Privacy Policies & Procedures document will help you with your HIPAA Privacy compliance efforts. This document addresses the basics of HIPAA Privacy
a) Each facility shall have a medical record system that retrieves information regarding individual residents.
 Each facility shall have a medical record system that retrieves information regarding individual residents.") TITLE 77: PUBLIC HEALTH CHAPTER I: DEPARTMENT OF PUBLIC HEALTH SUBCHAPTER c: LONG-TERM CARE FACILITIES PART 300 SKILLED NURSING AND INTERMEDIATE CARE FACILITIES CODE SECTION 300.1810 RESIDENT RECORD REQUIREMENTS
TITLE 77: PUBLIC HEALTH CHAPTER I: DEPARTMENT OF PUBLIC HEALTH SUBCHAPTER c: LONG-TERM CARE FACILITIES PART 300 SKILLED NURSING AND INTERMEDIATE CARE FACILITIES CODE SECTION 300.1810 RESIDENT RECORD REQUIREMENTS
Parsonage Vandenack Williams LLC Attorneys at Law
 MEDICAL RECORDS ACCESS GUIDE NEBRASKA Parsonage Vandenack Williams LLC Attorneys at Law Parsonage Vandenack Williams LLC 2008 For more information, contact [email protected] TABLE OF CONTENTS RESPONDING
MEDICAL RECORDS ACCESS GUIDE NEBRASKA Parsonage Vandenack Williams LLC Attorneys at Law Parsonage Vandenack Williams LLC 2008 For more information, contact [email protected] TABLE OF CONTENTS RESPONDING
PRIVACY PRACTICES OUR PRIVACY OBLIGATIONS
 PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. General Information To comply
PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. General Information To comply
VALPARAISO UNIVERSITY NOTICE OF PRIVACY PRACTICES. Health, Dental and Vision Benefits Health Care Reimbursement Account
 VALPARAISO UNIVERSITY NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
VALPARAISO UNIVERSITY NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
We ask that you contact our Privacy Officer in the event you have any questions or concerns regarding this Code or its implementation.
 PRIVACY AND ANTI-SPAM CODE FOR OUR DENTAL OFFICE Please refer to Appendix A for a glossary of defined terms. INTRODUCTION The Personal Health Information Act (PHIA) came into effect on December 11, 1997,
PRIVACY AND ANTI-SPAM CODE FOR OUR DENTAL OFFICE Please refer to Appendix A for a glossary of defined terms. INTRODUCTION The Personal Health Information Act (PHIA) came into effect on December 11, 1997,
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES Effective Date: Immediately This information is made available to all patients THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU
NOTICE OF PRIVACY PRACTICES Effective Date: Immediately This information is made available to all patients THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU
Cardiology Consultants of Atlanta, P.C. 2801 N. Decatur Rd. Suite 395, Decatur GA, 30033 (404) 298-2220 phone (678) 904-5336 fax
 298-2220 phone (678) 904-5336 fax") OFFICE POLICIES AND PROCEDURES Thank you for choosing Cardiology Consultants of Atlanta for your cardiovascular care. We realize that you have a choice in medical providers and are pleased that you have
OFFICE POLICIES AND PROCEDURES Thank you for choosing Cardiology Consultants of Atlanta for your cardiovascular care. We realize that you have a choice in medical providers and are pleased that you have
Floyd Healthcare Management, Inc. Notice of Privacy Practices
 Floyd Healthcare Management, Inc. Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
Floyd Healthcare Management, Inc. Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
NOTICE OF PRIVACY PRACTICES for the HARVARD UNIVERSITY MEDICAL, DENTAL, VISION AND MEDICAL REIMBURSEMENT PLANS
 NOTICE OF PRIVACY PRACTICES for the HARVARD UNIVERSITY MEDICAL, DENTAL, VISION AND MEDICAL REIMBURSEMENT PLANS THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW
NOTICE OF PRIVACY PRACTICES for the HARVARD UNIVERSITY MEDICAL, DENTAL, VISION AND MEDICAL REIMBURSEMENT PLANS THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW
The Health and Benefit Trust Fund of the International Union of Operating Engineers Local Union No. 94-94A-94B, AFL-CIO. Notice of Privacy Practices
 The Health and Benefit Trust Fund of the International Union of Operating Section 1: Purpose of This Notice Notice of Privacy Practices Effective as of September 23, 2013 THIS NOTICE DESCRIBES HOW MEDICAL
The Health and Benefit Trust Fund of the International Union of Operating Section 1: Purpose of This Notice Notice of Privacy Practices Effective as of September 23, 2013 THIS NOTICE DESCRIBES HOW MEDICAL
HIPAA BUSINESS ASSOCIATE AGREEMENT
 HIPAA BUSINESS ASSOCIATE AGREEMENT This HIPAA Business Associate Agreement ("BA AGREEMENT") supplements and is made a part of any and all agreements entered into by and between The Regents of the University
HIPAA BUSINESS ASSOCIATE AGREEMENT This HIPAA Business Associate Agreement ("BA AGREEMENT") supplements and is made a part of any and all agreements entered into by and between The Regents of the University
EXHIBIT C BUSINESS ASSOCIATE AGREEMENT
 EXHIBIT C BUSINESS ASSOCIATE AGREEMENT THIS AGREEMENT is made and entered into by and between ( Covered Entity ) and KHIN ( Business Associate ). This Agreement is effective as of, 20 ( Effective Date
EXHIBIT C BUSINESS ASSOCIATE AGREEMENT THIS AGREEMENT is made and entered into by and between ( Covered Entity ) and KHIN ( Business Associate ). This Agreement is effective as of, 20 ( Effective Date
Notice of Privacy Practices
 SHANNON LERACH, Ph.D. Licensed Clinical Psychologist PSY23705 243 N. Highway 101, Suite 16, Solana Beach, CA 92075 Telephone: (619) 817.5320 Fax: (858) 481.1674 Notice of Privacy Practices This Notice
SHANNON LERACH, Ph.D. Licensed Clinical Psychologist PSY23705 243 N. Highway 101, Suite 16, Solana Beach, CA 92075 Telephone: (619) 817.5320 Fax: (858) 481.1674 Notice of Privacy Practices This Notice
NOTICE OF PRIVACY PRACTICES
 GLOUCESTER COUNTY PUBLIC SCHOOLS EMPLOYEE HEALTH CARE PLAN, GLOUCESTER COUNTY PUBLIC SCHOOLS EMPLOYEE DENTAL CARE PLAN, GLOUCESTER COUNTY PUBLIC SCHOOLS EMPLOYEE FLEXIBLE BENEFITS PLAN 1 NOTICE OF PRIVACY
GLOUCESTER COUNTY PUBLIC SCHOOLS EMPLOYEE HEALTH CARE PLAN, GLOUCESTER COUNTY PUBLIC SCHOOLS EMPLOYEE DENTAL CARE PLAN, GLOUCESTER COUNTY PUBLIC SCHOOLS EMPLOYEE FLEXIBLE BENEFITS PLAN 1 NOTICE OF PRIVACY
HEALTH INSURANCE PORTABILITY & ACCOUNTABILITY ACT OF 1996 HIPAA
 TRAINING MANUAL HEALTH INSURANCE PORTABILITY & ACCOUNTABILITY ACT OF 1996 HIPAA Table of Contents INTRODUCTION 3 What is HIPAA? Privacy Security Transactions and Code Sets What is covered ADMINISTRATIVE
TRAINING MANUAL HEALTH INSURANCE PORTABILITY & ACCOUNTABILITY ACT OF 1996 HIPAA Table of Contents INTRODUCTION 3 What is HIPAA? Privacy Security Transactions and Code Sets What is covered ADMINISTRATIVE
Keeps a physician up to date on all laws and regulations affecting medical practice.
 Dear Doctor: Thank you for the inquiry you made to the Cooperative of American Physicians, Inc. (CAP). The accompanying document that addresses your professional liability question is published by the
Dear Doctor: Thank you for the inquiry you made to the Cooperative of American Physicians, Inc. (CAP). The accompanying document that addresses your professional liability question is published by the
NOTICE OF PRIVACY PRACTICES
 THE PHYSICIAN PRACTICE, P.A. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
THE PHYSICIAN PRACTICE, P.A. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
Metropolitan Living, LLC 151 W. Burnsville Parkway, Suite 101 Burnsville, MN 55337 Ph: (952) 564-3030 Fax: (651) 925-0031
 564-3030 Fax: (651) 925-0031") The Health Insurance Portability and Accountability Act (HIPAA) and Client Privacy Statement This notice describes how your medical information may be used and disclosed and how you can get access to this
The Health Insurance Portability and Accountability Act (HIPAA) and Client Privacy Statement This notice describes how your medical information may be used and disclosed and how you can get access to this
A A E S C. Albuquerque Ambulatory Eye Surgery Center NOTICE OF PRIVACY PRACTICES
 A A E S C Albuquerque Ambulatory Eye Surgery Center NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
A A E S C Albuquerque Ambulatory Eye Surgery Center NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA): FACT SHEET FOR NEUROPSYCHOLOGISTS Division 40, American Psychological Association
: FACT SHEET FOR NEUROPSYCHOLOGISTS Division 40, American Psychological Association") HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA): FACT SHEET FOR NEUROPSYCHOLOGISTS Division 40, American Psychological Association DISCLAIMER This general information fact sheet is made available
HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA): FACT SHEET FOR NEUROPSYCHOLOGISTS Division 40, American Psychological Association DISCLAIMER This general information fact sheet is made available
EAST ALABAMA HEALTH CARE AUTHORITY d/b/a EAST ALABAMA MEDICAL CENTER EAST ALABAMA MEDICAL CENTER SKILLED NURSING FACILITY EMERGENCY MEDICAL SERVICES
 EAST ALABAMA HEALTH CARE AUTHORITY d/b/a EAST ALABAMA MEDICAL CENTER EAST ALABAMA MEDICAL CENTER SKILLED NURSING FACILITY EMERGENCY MEDICAL SERVICES (334) 749-3411 www.eamc.org THIS NOTICE DESCRIBES HOW
EAST ALABAMA HEALTH CARE AUTHORITY d/b/a EAST ALABAMA MEDICAL CENTER EAST ALABAMA MEDICAL CENTER SKILLED NURSING FACILITY EMERGENCY MEDICAL SERVICES (334) 749-3411 www.eamc.org THIS NOTICE DESCRIBES HOW
Notice of Privacy Practices
 Notice of Privacy Practices This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review it carefully. This Notice of
Notice of Privacy Practices This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review it carefully. This Notice of
River Valley Therapy & Sports Medicine, Inc. Notice of Privacy Practices
 River Valley Therapy & Sports Medicine, Inc. Notice of Privacy Practices This notice describes how medical information about you may be used and disclosed and how you can get access to this information.
River Valley Therapy & Sports Medicine, Inc. Notice of Privacy Practices This notice describes how medical information about you may be used and disclosed and how you can get access to this information.
Connecticut Pipe Trades Health Fund Privacy Notice. 2013 Restatement
 Connecticut Pipe Trades Health Fund Privacy Notice 2013 Restatement Section 1: Purpose of This Notice and Effective Date THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED
Connecticut Pipe Trades Health Fund Privacy Notice 2013 Restatement Section 1: Purpose of This Notice and Effective Date THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED
The dental profession s peer review program is a process to resolve disputes between a
 HOW THE DENTAL PEER REVIEW SYSTEM WORKS AND WHAT YOU EXPECT FROM IT Introduction The dental profession s peer review program is a process to resolve disputes between a patient and a dentist or a third
HOW THE DENTAL PEER REVIEW SYSTEM WORKS AND WHAT YOU EXPECT FROM IT Introduction The dental profession s peer review program is a process to resolve disputes between a patient and a dentist or a third
Notice of Privacy Practices
 Notice of Privacy Practices THIS NOTICE OF PRIVACY PRACTICES DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Notice of Privacy Practices THIS NOTICE OF PRIVACY PRACTICES DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Notice of Privacy Practices
 Notice of Privacy Practices This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review it carefully. This practice uses
Notice of Privacy Practices This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review it carefully. This practice uses
HIPAA Notice of Privacy Practices
 This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review this notice carefully. This practice is required by law to
This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review this notice carefully. This practice is required by law to
Privacy Notice. The Plan s duties with respect to health information about you
 Privacy Notice Please carefully review this notice. It describes how medical information about you may be used and disclosed and how you can get access to this information. The Health Insurance Portability
Privacy Notice Please carefully review this notice. It describes how medical information about you may be used and disclosed and how you can get access to this information. The Health Insurance Portability
Effective Date: March 23, 2016
 AIG COMPANIES Effective Date: March 23, 2016 HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
AIG COMPANIES Effective Date: March 23, 2016 HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
HIPAA NOTICE OF PRIVACY PRACTICES
 HIPAA NOTICE OF PRIVACY PRACTICES Marden Rehabilitation Associates, Inc. Marden Rehabilitation Associates of Ohio, Inc. Marden Rehabilitation Associates of West Virginia Health Care Plus Preferred Care
HIPAA NOTICE OF PRIVACY PRACTICES Marden Rehabilitation Associates, Inc. Marden Rehabilitation Associates of Ohio, Inc. Marden Rehabilitation Associates of West Virginia Health Care Plus Preferred Care
HIPAA. HIPAA and Group Health Plans
 HIPAA HIPAA and Group Health Plans CareFirst BlueCross BlueShield is the business name of CareFirst of Maryland, Inc. and is an independent licensee of the Blue Cross and Blue Shield Association. Registered
HIPAA HIPAA and Group Health Plans CareFirst BlueCross BlueShield is the business name of CareFirst of Maryland, Inc. and is an independent licensee of the Blue Cross and Blue Shield Association. Registered
Birkam Health Center Ferris State University NOTICE OF PRIVACY PRACTICES
 Birkam Health Center Ferris State University NOTICE OF PRIVACY PRACTICES Effective Date of Notice: October 1, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
Birkam Health Center Ferris State University NOTICE OF PRIVACY PRACTICES Effective Date of Notice: October 1, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
SOUTHLAKE DERMATOLOGY 1170 N. Carroll Ave. Southlake, TX 76092 www.southlakedermatology.com Main 817-251-6500 Fax 817-442-0550
 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. EFFECTIVE September 15, 2014 This Notice of
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. EFFECTIVE September 15, 2014 This Notice of
Privacy Notice Document (HIPAA)
") Privacy Notice Document (HIPAA) THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Privacy
Privacy Notice Document (HIPAA) THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Privacy
PRIVACY NOTICE. In certain situations, we may also disclose patient information to another provider or health plan for their health care operations.
 1 PRIVACY NOTICE THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Privacy Notice is being
1 PRIVACY NOTICE THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Privacy Notice is being
Eye Clinic of Bellevue, LTD. P.S. Privacy Policy EYE CLINIC OF BELLEVUE LTD PS NOTICE OF INFORMATION PRACTICES
 Eye Clinic of Bellevue, LTD. P.S. Privacy Policy EYE CLINIC OF BELLEVUE LTD PS NOTICE OF INFORMATION PRACTICES Date of Last Revision: 4/8/03 Effective Date: Immediately This information is made available
Eye Clinic of Bellevue, LTD. P.S. Privacy Policy EYE CLINIC OF BELLEVUE LTD PS NOTICE OF INFORMATION PRACTICES Date of Last Revision: 4/8/03 Effective Date: Immediately This information is made available
Schindler Elevator Corporation
 -4539 Telephone: (973) 397-6500 Mail Address: P.O. Box 1935 Morristown, NJ 07962-1935 NOTICE OF PRIVACY PRACTICES FOR PROTECTED HEALTH INFORMATION THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU
-4539 Telephone: (973) 397-6500 Mail Address: P.O. Box 1935 Morristown, NJ 07962-1935 NOTICE OF PRIVACY PRACTICES FOR PROTECTED HEALTH INFORMATION THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU
NOTICE OF PRIVACY PRACTICES Allergy Treatment Center of New Jersey, P.C. Effective Date: April 14, 2003
 Allergy Treatment Center of New Jersey, P.C. 388 Pompton Avenue 415 Avenel Street Cedar Grove, NJ 07009 Avenel, NJ 07001 (973) 857 9890 (732) 636-7030 NOTICE OF PRIVACY PRACTICES Allergy Treatment Center
Allergy Treatment Center of New Jersey, P.C. 388 Pompton Avenue 415 Avenel Street Cedar Grove, NJ 07009 Avenel, NJ 07001 (973) 857 9890 (732) 636-7030 NOTICE OF PRIVACY PRACTICES Allergy Treatment Center
HIPAA PRIVACY NOTICE PLEASE REVIEW IT CAREFULLY
 HIPAA PRIVACY NOTICE THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN OBTAIN ACCESS TO THIS INFORMATION. INTRODUCTION PLEASE REVIEW IT CAREFULLY Moriarty
HIPAA PRIVACY NOTICE THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN OBTAIN ACCESS TO THIS INFORMATION. INTRODUCTION PLEASE REVIEW IT CAREFULLY Moriarty
GENOA, a QoL HEALTHCARE COMPANY, LLC WEBSITE PRIVACY POLICY
 GENOA, a QoL HEALTHCARE COMPANY, LLC WEBSITE PRIVACY POLICY PLEASE READ THIS WEBSITE PRIVACY POLICY CAREFULLY BEFORE USING THIS WEBSITE, OR SUBMITTING ANY PROTECTED HEALTH INFORMATION OR PERSONALLY IDENTIFIABLE
GENOA, a QoL HEALTHCARE COMPANY, LLC WEBSITE PRIVACY POLICY PLEASE READ THIS WEBSITE PRIVACY POLICY CAREFULLY BEFORE USING THIS WEBSITE, OR SUBMITTING ANY PROTECTED HEALTH INFORMATION OR PERSONALLY IDENTIFIABLE
CBIA Service Corporation Privacy and Security Notice
 July 1, 2012 CBIA Service Corporation Privacy and Security Notice THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE
July 1, 2012 CBIA Service Corporation Privacy and Security Notice THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE