Are patients preferences for shifting services from medical specialists to general practitioners related to the type of medical intervention?
|
|
|
- Eunice Montgomery
- 8 years ago
- Views:
Transcription
1 Postprint Version Journal website Pubmed link DOI Are patients preferences for shifting services from medical specialists to general practitioners related to the type of medical intervention? Leti van Bodegom-Vos PhD Senior Researcher/Implementation Fellow, Netherlands Institute for Health Services Research (NIVEL), Utrecht and Department of Medical Decision Making, Leiden University Medical Centre, The Netherlands Judith D de Jong PhD Programme Coordinator Peter Spreeuwenberg MSc Statistician Netherlands Institute for Health Services Research (NIVEL), Utrecht, The Netherlands Emile C Curfs Professor, School of Management, Open University, Heerlen and VGZ, Eindhoven, The Netherlands Peter P Groenewegen Director, Netherlands Institute for Health Services Research (NIVEL), Utrecht and Professor, Department of Sociology and Department of Human Geography, Utrecht University, The Netherlands ABSTRACT Background To improve the feasibility of shifting medical specialist to general practitioner (GP) services in patient-centred health care systems, it is important to know how this substitution is valued by patients. However, insight into patients preferences is lacking. Aim This study aims to fill this gap by assessing whether patients preferences for substitution are related to the type of medical intervention. Methods Questionnaires were sent to 1000 members of thedutch Insurants Panel (potential patients). Panel members were asked about their preferences for and use of medical specialist and GP services regarding 11 medical interventions. Six hundred and ninety-four members (69%) responded. We used multilevel multinomial regression to analyse the data. Results Preferences were significantly related to medical intervention type. GP services were preferred for follow-up treatments (e.g. removing stitches) and non-complex invasive treatments (e.g. removal of lumps), and medical specialist services were preferred for complex invasive treatments (e.g. injection therapy for varicose veins), non-invasive treatments (e.g. start of insulin therapy) and diagnostic examinations (e.g. abdominal ultrasound).
, Utrecht and Department of Medical Decision Making, Leiden University")
2 Age, effort required to visit a GP, perceived health status and previous treatment experiences also influenced preferences but did not confound the effects of medical intervention type. Conclusion This study provides strong indications that patients preferences for substitution are influenced by the type of medical intervention. Therefore it seems important that health policy makers, purchasers and practitioners take the preferences of (potential) patients into account. How this fits with quality in primary care What do we know? Substitution for medical specialist services by primary care is increasingly considered an instrument to improve quality and efficiency of care delivery. To effectively substitute medical specialist services in patientcentred health care systems it is important to take patient preferences into account alongside technical feasibility criteria, but insight into patients preferences is lacking. What does this paper add? This study provides strong indications that patients preferences for substitution are influenced by the type of medical intervention. According to patients, follow-up treatment and non-complex invasive treatment are more acceptable for substitution than complex invasive treatment, non-invasive treatment and diagnostic examinations. INTRODUCTION In the Netherlands and other countries with a strong primary care system, such as theukand Scandinavian countries, general practitioners (GPs) provide first contact and ongoing care for most health care problems. They decide whether or not to refer patients to medical specialists in hospitals ( gatekeeper function). This is regarded as cost-effective compared with health systems in which patients can access specialist services directly. To further improve the quality and efficiency of the health care system, health policies in many countries stimulate shifting medical specialist services delivered in hospitals to GPs. 1 Research suggests that this substitution offers cost benefits, 2 4 while quality of care and health outcomes seem to be unaffected if the transferred service does not demand competencies beyond those of the average GP. 1,5 Besides this, care by GPs is associated with improved access (proximity) and convenience for patients. 1,5 To stimulate substitution, the Dutch government included several incentives for substitution in the reform of the Dutch health insurance system in First, they introduced additional payments for specific services in primary care that substituted for medical specialist services. 6 Previous research has shown that additional payments for specific services in primary care indeed stimulate substitution. 7,8 Second, the Dutch government introduced a regulated market for health insurance, which emphasises cost-effective health care purchasing by insurers in order to attract patients. 6,9 For example, insurers can purchase care delivered by GPs instead of by medical specialists. To achieve this, they in turn have to spur on health care providers to provide high-quality health care which is produced as efficiently as possible. At the same time, insurers need to take into account their insurants preferences for the source of health care delivery, since insurants have a free choice of insurer and can change insurer every year. 9

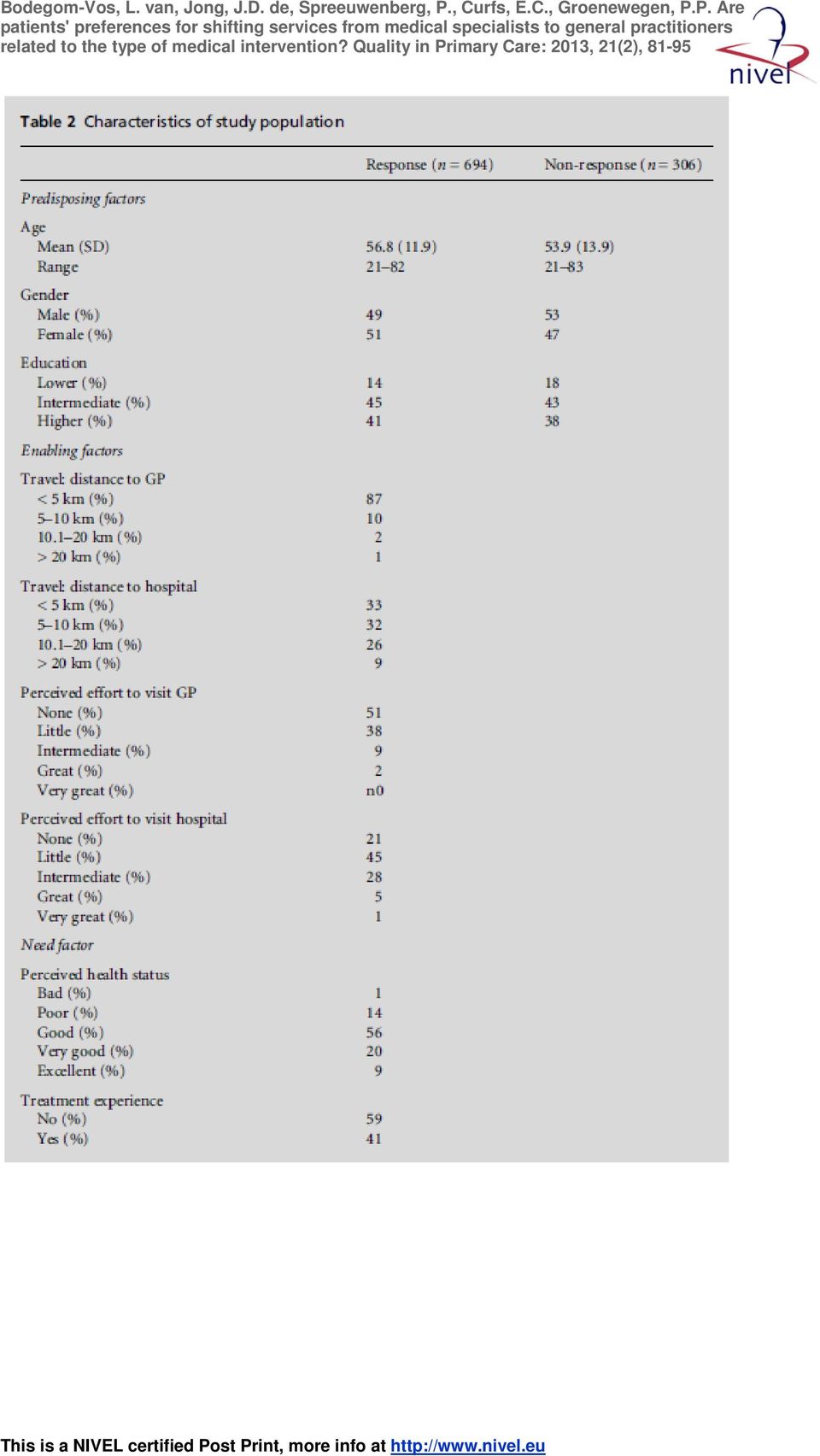
3 However, to date it is unclear how shifting medical specialist services to GPs is valued by patients. Previous research that assessed patients preferences for different provider types (e.g. medical specialist versus nurse practitioner) showed that patients base their provider choice mainly on providers expertise, and less on convenience 10 and the location of care. 13 The importance of waiting time for patients preferences for provider type varies in different studies. 10,13 Furthermore, it was shown that patients preferences for different provider types are influenced by age, 12 education 12 and previous experiences with the medical intervention. 12,14 Previous studies show slight differences between patients preferences for health care provider types by type of medical intervention. For example, while surgical patients mainly base their provider choice on care delivery characteristics such as provider experience and specialisation, 13 chronically ill patients base their provider choice on the continuity of care. 15 Accordingly, we expect that patients preferences for health care provider types, and thus for substitution, may be affected by medical intervention type (e.g. minor surgery, follow-up treatment and diagnostics). When this is true, health care policy makers, insurers and practitioners should take patients preferences into account next to quality, efficiency and technical feasibility as criteria to effectively shift medical specialist services to GPs. The aim of this study was to assess whether patients preferences for service delivery by medical specialists or GPswere related to the type of medical intervention (e.g. diagnostics or minor surgery). METHODS Data collection We conducted an online survey among members of the Dutch Insurants Panel. The Insurants Panel consists of approximately 10,000 insurants of one of the biggest Dutch health insurers (market share = 26%). 16 Compared with the Dutch population, older people (aged between 40 and 80 years), people with a bad to moderate selfreported health status and people who have been insured with the same health insurer for over 10 years are over-represented. 17 The aim of the panel is to gather information on people s experiences with and expectations of health care in general and their health insurer in particular. Members for the panel were recruited through an announcement in the health insurer s magazine. Compliance with privacy regulations was approved by the Dutch Data Protection Authority (number ). According to Dutch legislation, neither obtaining informed consent nor approval by a medical ethics committee was obligatory for this study. In February 2008, all panel members filled in a questionnaire on several background variables (age, gender and educational level). In June 2008, questionnaires were sent to 500 men and 500 women of the Insurants Panel who had agreed to complete Internet questionnaires. We used stratified random sampling to select these panel members and to create a subgroup that showed the same distribution regarding age as the whole Insurants Panel. After oneweek, a reminderwas sent to 512 panel members who had not responded, and again after one week a second reminder was sent to 339 panel members.

4 Conceptual model To assess the effect of medical intervention type on patients preferences for type of health care provider, we constructed a conceptual model. In this model, the patients preference for health care provider type is the dependent variable. The independent variable is represented by the medical intervention type. Andersen s Behavioural Model of Health Services Utilisation 18 was used to determine which covariates had to be included in our model to correct for confounding. Originally, the purpose of Andersen s framework was to discover inequities in health care utilisation, 18 but it has also been used to analyse choices of type of health care utilisation, 19 and choices for using conventional or complementary (alternative) medical services. 20 The framework portrays the process of choosing health care as a complex of three interrelated sets of predisposing (sociocultural characteristics of individuals), enabling (logistical aspects of obtaining care) and need factors. 21 The survey included questions on all variables of our conceptual model:. Preferences for health care provider type regarding 11 different medical interventions (Table 1). There were three options: (1) treatment by a GP, (2) treatment by a medical specialist and (3) no preference. According to the purchasing department of the insurer, these 11 medical interventions were eligible for substitution.. Predisposing factors: age (continuous variable), gender and educational level (highest level of education was categorised into three levels, lower, intermediate and higher, according to the classification of Statistics Netherlands). [TABLE 1]. Enabling factors: travel distance four-level categorical variable (< 5, 5 10, or > 20 km, perceived effort needed to visit a GP or medical specialist five-level categorical variable (none, little, intermediate, great or very great). Health insurance was not included as an enabling factor because the study population consists of insured patients of one health insurer, and all medical interventions included in this study were covered.. Need factor: perceived health status five-level categorical variable (poor, fair, good, very good or excellent)]. Perceived health status was used as a proxy for need because of its relation to use of health services. 16 In addition, we included treatment experience use of health care services for one of the medical interventions in the past 12 months (dichotomous variable indicating whether or not a respondent had one of the medical interventions in the past 12 months) as a covariate in our analysis, assuming that previous experiences could influence patients preferences. In addition, all panel members were asked why they preferred being treated or examined by a GP or medical specialist. The respondents could choose from 12 reasons. These reasons were similar for both health care providers. The complete questionnaire used in this study is shown in Supplementary file 1. Data analysis We used descriptive statistics to describe the survey results. To analyse the effect of medical intervention type on preferences for health care provider type, we first categorised the medical interventions into five groups using dummy variables:

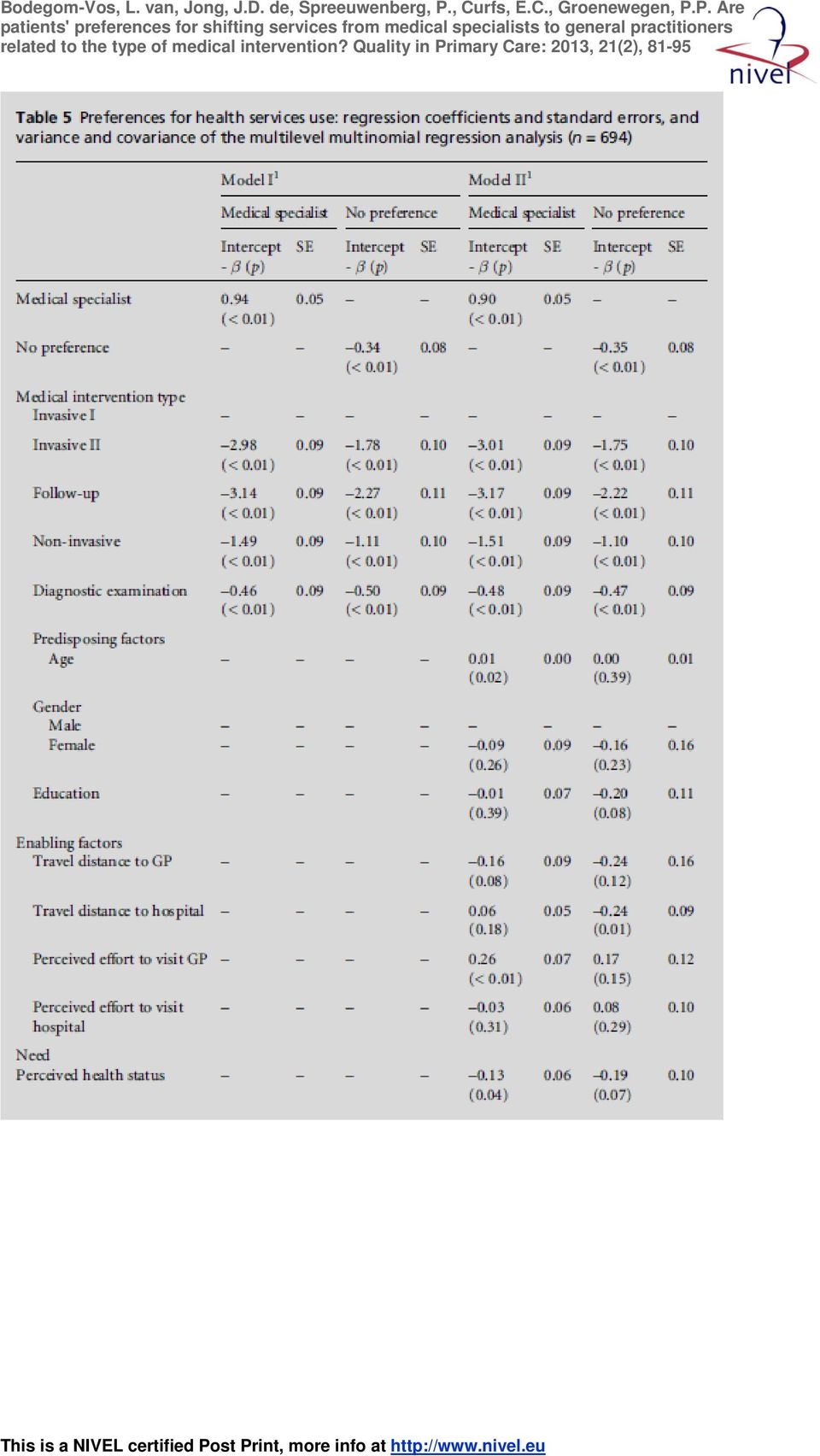
5 complex invasive treatment (invasive I), non-complex invasive treatment (invasive II), follow-up treatment (follow-up), non-invasive treatment (non-invasive) and diagnostic examinations (Table 1). Categorisation was based on substantive considerations and a first analysis of the medical interventions. Next, we conducted multilevel multinomial regression analyses comparing three responses: (1) preference for GP, (2) preference for medical specialist and (3) no preference. The GP preference was regarded as a reference group. In the multilevel analyses, two levels were distinguished: 11 medical interventions (level 1) within individual respondents (level 2). By analysing the data with multilevel models, we took into account this hierarchical data structure; the preferences of a given individual for each of the medical interventions are supposed to be correlated. 22,23 Two models were tested using MLwiN 2.0 (see Supplementary file 2, available online only, for model specifications). In the first model, the influence of the type of medical intervention on preferences for health care provider type was assessed. In the second model, the covariates were added to the model to correct for confounding. The level 2 variance and the covariance between the dependent variables were inspected. RESULTS The questionnaire was returned by 694 members of the Insurants Panel (response rate 69.4%). All 694 respondents filled in all questions about their preferences for health care provider type regarding the 11 medical interventions. Respondents were similar to non-respondents in terms of age, gender and educational level (Table 2). Table 3 shows the unadjusted preferences for health care provider type. For complex invasive treatments, non-invasive treatment and diagnostic examinations, respondents more often preferred treatment or examination by a medical specialist than by a GP. Respondents more often preferred to visit a GP for follow-up treatment and non-complex invasive treatments. Table 4 shows the five most common reasons to prefer utilisation of GP or medical specialist services. GP services were preferred because of better accessibility (52% of respondents), shorter access times (50%) and more comfort (28%) in comparison with medical specialist services. Reasons for preferences for medical specialist services included better skills of a medical specialist (82% of respondents), a lower perceived risk of treatment by a medical specialist (43%) and more confidence in medical specialists (31%) compared with GP services. The results of the multilevel multinomial regression analysis are presented in Table 5. The preference for health care provider type was significantly related to medical intervention type. The regression coefficients confirm the pattern in Table 3. In order of preference for GP services compared with GP preference in cases of complex invasive treatment, medical specialist services are preferred slightly less often for the examples of diagnostic examination (Model I: ß = 0.45, p < 0.01; Model II: ß = 0.48, p < 0.01), less so for the examples of non-invasive treatment (Model I: ß = 1.49, p < 0.01; Model II: ß = 1.51, p < 0.01), even less so for the examples of less complex invasive care (Model I: ß = 2.98, p < 0.01; Model II: ß = 3.01, p < 0.01), and least for follow-up care (Model I: ß = 3.11, p < 0.01; Model II: ß = 3.17, p < 0.01). The preference for GP services compared with no preference shows the same pattern.
 within individual respondents (level 2).")
6 Comparison of model 1 and model 2 showed that covariates did not confound the effect of type of medical intervention on respondents preferences. [TABLE 2, TABLE 3, TABLE 4] Instead, they provided additional information about the respondents preferences. It appeared that older respondents (ß = 0.01, p = 0.02), respondents for whom the effort to visit a GP is relatively great (ß = 0.26, p < 0.01) and respondents with treatment experience (ß = 0.47, p < 0.01) more often preferred medical specialist services. Respondents with a better perceived health status (ß = 0.13, p = 0.04) preferred GP services more frequently. The bottomrows of Table 5 show the variance in the responses at the level of the respondents and the covariance between the responses. Multilevel analysis allowed us to analyse variance and covariance. In a traditional analysis we would have analysed the responses for each of the 11 interventions separately. [TABLE 5] This is inefficient and does not take into account that a respondent s preference in the case of one of the interventions might be related to their preference in the case of the other interventions. This relationship between preferences, elicited for the 11 different interventions, is expressed by the variance at the level of the respondents (level 2 variance intable 5).The variance between respondents who have no preference is much higher ( X 2 = 2.84, p < 0.01) than that between respondents who prefer medical specialist services ( X 2 = 0.88, p < 0.01). This means that that stating no preference is more of a general pattern of reacting to the questions about their preferences rather than being influenced by the specific medical interventions. Conversely, the specific preferences for either GPs or medical specialists depended more on the specific medical interventions. The use of multinomial multilevel analysis allowed us to analyse the three options for preferences, no preference, preference for GP or preference for medical specialist, simultaneously. Again, this is a more efficient analysis and it takes into account the fact that these preferences might be mutually related. This is expressed by the covariance. The covariance shows that respondents who more frequently prefer medical specialist services also frequently have no preference rather than preference for a GP. DISCUSSION This study provides strong indications that patients preferences for substitution are influenced by medical intervention type. Additional findings suggest that patients age, the effort needed to visit a GP, perceived health status and previous treatment experiences also influence preferences for substitution but do not confound the effects of medical intervention type on patients preferences. These additional findings are in line with previous studies 12 and utilisation patterns of health services. Rodriguez et al 24 found, for example, that having fair or poor health increases the chance of visiting a medical specialist, and that longer travel times to hospitals (i.e. a greater effort) had a significant negative effect on the probability of seeing a medical specialist. Being older increases the chance of having fair or poor health due to having an increased chance of (multiple) illness. This is probably not completely
 more often preferred medical specialist services. Respondents with a better perceived health status (ß = 0.13, p = 0.04) preferred GP services more frequently.")
7 captured by self-rated health. Therefore it seems plausible that older people more often prefer treatment by a medical specialist. Our study has some limitations. First, due to the limited number of treatment examples per medical intervention type, the results cannot be generalised to all treatments. Second, the medical interventions included in this survey were not all applicable to male and female respondents (e.g. male sterilisations). However, the statistical model adjusted for gender. Although these limitations prevent us from applying our results to every type of diagnostic examination, complex invasive, noncomplex invasive, non-invasive and follow-up treatment, our study does give clear indications that patients do not always prefer substitution. A third limitation of our study is that, compared with the Dutch population overall, older people (aged years) and people with a bad to moderate selfreported health status were over-represented in the panel used. However, these groups use health care services more frequently, which makes their preferences more relevant. We therefore do not think that the overrepresentation of these groups has led to distortions in the results, and it does not influence the relevance of the results. Another limitation is that we performed our study among a sample of panel members instead of patients. These panel members are not typical of all patients. This may have led to selection bias. Our study is, to our knowledge, the first to quantitatively investigate patients preferences for health care providers regarding several types of medical interventions. Previous studies have focused on patients preferences for one type of medical intervention (e.g. follow-up care for breast cancer patients 12 ) or for one patient group (e.g. dermatology services 10 ). Despite the limitations, our study provides useful findings for health care policies aiming to shift services from medical specialists to GPs in patient-centred health care systems. The results of this study show health policy makers, purchasers and practitioners strong indications that shifting follow-up treatment and noncomplex invasive treatment from medical specialists togps has the largest support among(potential)patients. However, health care policy makers, purchasers and practitioners have to be aware that patients may be resistant to changes in the organisation of health care. Patients tend to prefer what they know best or have experienced previously. 12,25 However, acceptance by the public is not enough to effectively implement substitution of care. To ensure that patients get the opportunity to act according to their preferences, they must be adequately informed and the health care system must allow it. Patients have to learn, in turn, to express their preferences and act as autonomous health care users. Furthermore, health care policy makers and purchasers have to be aware of the risk that the quality of services may change when medical specialist services are substituted with primary care services. A change in quality could go either way, improving or decreasing quality. A risk to quality is, for example, that GPs will not be sufficiently skilled to undertake the work previously done by medical specialists. 1 It is therefore important to first assess whether GPs are equipped and skilled to provide these treatments, or otherwise start educational interventions to address this before shifting services. Another concern in the literature is that transfer will lead to increases in total health care expenditure at a macro level. 26 Although previous research showed that reductions in costs were

8 achieved through lower salaries or reimbursements in primary care 2 4 and reduced time and travel costs for patients, 1,5 these can be offset by rises in costs generated through increases in the volume of care and loss of economies of scale. 1 More important probably is that the capacity that is freed in medical specialist care by shifting services to primary care might be quickly filled by higher demand for other services. The extent to which this happens depends on the incentives in the system. Specifically, for the interventions that were used as examples in our survey there is as far as we know no literature about improved quality when comparing medical specialists and GPs. In general, research about disease management 27 and bundled payments for the treatment of chronic disease 28,29 shows some evidence of improved care. However, this is related to programmes, rather than separate interventions, and the evidence is still not very strong. Therefore, first of all, medical specialist services that can be substituted by GPs should be chosen carefully. Second, purchasing should be part of an integral policy that focuses on broader care programmes into which separate interventions fit, and that as far as possible takes cross-over effects of substitution into account. CONCLUSION This study demonstrated that patients preferences for substitution are influenced by medical intervention type. These findings provide strong indications that health policy makers, purchasers and practitioners in patient-centred health care systems should take patients preferences into account next to quality, efficiency and technical feasibility as criteria for effectively substituting medical specialist services with GP services. REFERENCES 1 Sibbald B, McDonald R, Roland M. Shifting care from hospitals to the community: a review of the evidence on quality and efficiency. Journal of Health Services Research & Policy 2007;12(2): World Health Organization. Advisory Support to Primary Health Care Evaluation Model: Estonia PHC Evaluation Project. World Health Organization: Geneva, Health Council of the Netherlands. European primary care, publication no. 2004/20E Ros CC, Groenewegen PP, Delnoij DM. All rights reserved, or can we just copy? Cost sharing arrangements and characteristics of health care systems. Health Policy 2000;52(1): Roland M, Mead N, Sibbald B et al. Outpatient Services and Primary Care. A scoping review of research into strategies for improving outpatient effectiveness and efficiency. National Primary Care Research and Development Centre, Manchester: Minister of Health, Welfare and Sport. Substitution of Care [in Dutch]. Document number CZ/FBI Minister of Health, Welfare and Sport: The Hague, 12 September Groenewegen PP. Subsitution of primary care and specialist care: a regional analysis in Denmark. Social Science & Medicine 1991;33(4): Krasnik A, Groenewegen PP, Pedersen PA et al. Changing remuneration systems: effects on activity in general practice. British Medical Journal 1990;300: Custers T, Onyebuchi AA, Klazinga NS. Is there a business case for quality in the Netherlands? A critical analysis of the recent reforms of the health care system. Health Policy 2007;82: Coast J, Salisbury C, de Berker D et al. Preferences for aspects of a dermatology consultation. Epidemiology and Health Services Research 2006;155:

9 11 Gerard K, Lattimer V. Preferences of patients for emergency services available during GP surgery hours: a discrete choice experiment. Family Practice 2005;22: Kimman ML, Dellaert BGC, Boersman LJ, Lambin P, Dirksen CD. Follow-up after treatment for breast cancer: one strategy fits all? An investigation of patient preferences using a discrete choice experiment. Acta Oncologica 2010;49: Schwappach DL, Strasmann TJ. Does location matter? A study of the public0s preferences for surgical care provision. Journal of Evaluation in Clinical Practice 2007; 13: Scott A. Identifying and analysing dominant preferences in discrete choice experiments: an application in health care. Journal of Economic Psychology 2002;23: Berendsen AJ, De Jong GM, Meyboom-de Jong B, Dekker JH, Schuling J. Transition of care: experiences and preferences of patients across the primary/secondary interface a qualitative study. BMC Health Services Research 2009;9: Hoeymans N, Melse JM, Schoemaker CG. Health and Determinants: part of the report of public health status and forecasts 2010 [in Dutch]. National Institute for Public Health and the Environment: Bilthoven, Hendriks M, Delnoij DMJ, Groenewegen PP. VGZ Insurance Panel: Background characteristics 2006 [in Dutch]. Netherlands Institute for Health Services Research: Utrecht, Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? Journal of Health and Social Behavior 1995;36: Thind A, Mohani A, Banerjee K, Hagigi F. Where to deliver? Analysis of choice of delivery location from a national survey in India. BMC Public Health 2008;8(29). 20 Sirois FM, Gick ML. An investigation of the health beliefs and motivations of complementary medicine clients. Social Science & Medicine 2002;55: Kelner M, Wellman B. Health care and consumer choice: medical and alternative therapies. Social Science&Medicine 1997;45: Leyland AH, Groenewegen PP. Multilevel modelling and public health policy. Scandinavian Journal of Public Health 2003;31: Snijders TAB, Bosker RJ. Multilevel Analysis. An introduction to basic and advanced multilevel modeling. Sage: London, Rodriquez M, Stoyanova A. The effect of private insurance access on the choice of GP/specialist and public/ private provider in Spain. Health Economics 2004;13: Salked G, Ryan M, Short L. The veil of experience: do consumers prefer what they know best? Health Economics 2000;9: Sibbald B, Pickard S, McLeod H et al. Moving specialist care into the community: an initial evaluation. Journal of Health Services Research & Policy 2008;13: Gress S, Baan CA, Calnan M et al. Co-ordination and management of chronic conditions in Europe: the role of primary care position paper of the European Forum for Primary Care. Quality in Primary Care 2009;17: de Bakker DH, Struijs JN, Baan CB et al. Early results from adoption of bundled payment for diabetes care in the Netherlands show improvement in care coordination. Health Affairs (Millwood) 2012;31: Struijs JN, de Jong-van Til JT, Lemmens LC, Drewes HW, de Bruin SR, Baan CA. Three Years of Bundled Payment for Diabetes Care in the Netherlands: Impact on health care delivery process and the quality of care. RIVM: Bilthoven, FUNDING This work was supported by the Dutch health care insurer VGZ. ETHICAL APPROVAL According to Dutch legislation, neither obtaining informed consent nor approval by a medical ethics committee was obligatory for this study. PEER REVIEW Not commissioned; externally peer reviewed. CONFLICTS OF INTEREST Leti van Bodegom-Vos, Judith de Jong, Peter Spreeuwenberg and Peter Groenewegen declare that they have no conflicts of interest. Emile Curfs is an employee of VGZ (not involved in decisions about policy and health care purchasing of VGZ), the funder of this research.

10 TABLES

11
12

13
14

Integrating care by bundled payments
 Integrating care by bundled payments Lessons from the Netherlands JN Struijs 1 18 Background Integrated care for diabetes is introduced in Netherlands since decades. The fragmentary funding hampered the
Integrating care by bundled payments Lessons from the Netherlands JN Struijs 1 18 Background Integrated care for diabetes is introduced in Netherlands since decades. The fragmentary funding hampered the
Annicka G. M. van der Plas. Kris C. Vissers. Anneke L. Francke. Gé A. Donker. Wim J. J. Jansen. Luc Deliens. Bregje D. Onwuteaka-Philipsen
 CHAPTER 8. INVOLVEMENT OF A CASE MANAGER IN PALLIATIVE CARE REDUCES HOSPITALISATIONS AT THE END OF LIFE IN CANCER PATIENTS; A MORTALITY FOLLOW-BACK STUDY IN PRIMARY CARE. Annicka G. M. van der Plas Kris
CHAPTER 8. INVOLVEMENT OF A CASE MANAGER IN PALLIATIVE CARE REDUCES HOSPITALISATIONS AT THE END OF LIFE IN CANCER PATIENTS; A MORTALITY FOLLOW-BACK STUDY IN PRIMARY CARE. Annicka G. M. van der Plas Kris
THE ORGANISATION AND FINANCING OF HEALTH CARE SYSTEM IN LATVIA
 THE ORGANISATION AND FINANCING OF HEALTH CARE SYSTEM IN LATVIA Eriks Mikitis Ministry of Health of the Republic of Latvia Department of Health Care Director General facts, financial resources Ministry
THE ORGANISATION AND FINANCING OF HEALTH CARE SYSTEM IN LATVIA Eriks Mikitis Ministry of Health of the Republic of Latvia Department of Health Care Director General facts, financial resources Ministry
Use of health care services by ethnic minorities in The Netherlands: do patterns differ?
 Postprint Version 1.0 Journal website http://eurpub.oxfordjournals.org Pubmed link http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=retrieve&dop t=abstractplus&list_uids=16641158&itool=iconabstr&query_hl=1&itool=pubm
Postprint Version 1.0 Journal website http://eurpub.oxfordjournals.org Pubmed link http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=retrieve&dop t=abstractplus&list_uids=16641158&itool=iconabstr&query_hl=1&itool=pubm
REGULATIONS FOR THE POSTGRADUATE CERTIFICATE IN PUBLIC HEALTH (PCPH) (Subject to approval)
 (Subject to approval)") 512 REGULATIONS FOR THE POSTGRADUATE CERTIFICATE IN PUBLIC HEALTH (PCPH) (Subject to approval) (See also General Regulations) M.113 Admission requirements To be eligible for admission to the programme
512 REGULATIONS FOR THE POSTGRADUATE CERTIFICATE IN PUBLIC HEALTH (PCPH) (Subject to approval) (See also General Regulations) M.113 Admission requirements To be eligible for admission to the programme
THE CORRELATION BETWEEN PHYSICAL HEALTH AND MENTAL HEALTH
 HENK SWINKELS (STATISTICS NETHERLANDS) BRUCE JONAS (US NATIONAL CENTER FOR HEALTH STATISTICS) JAAP VAN DEN BERG (STATISTICS NETHERLANDS) THE CORRELATION BETWEEN PHYSICAL HEALTH AND MENTAL HEALTH IN THE
HENK SWINKELS (STATISTICS NETHERLANDS) BRUCE JONAS (US NATIONAL CENTER FOR HEALTH STATISTICS) JAAP VAN DEN BERG (STATISTICS NETHERLANDS) THE CORRELATION BETWEEN PHYSICAL HEALTH AND MENTAL HEALTH IN THE
UMEÅ INTERNATIONAL SCHOOL
 UMEÅ INTERNATIONAL SCHOOL OF PUBLIC HEALTH Master Programme in Public Health - Programme and Courses Academic year 2015-2016 Public Health and Clinical Medicine Umeå International School of Public Health
UMEÅ INTERNATIONAL SCHOOL OF PUBLIC HEALTH Master Programme in Public Health - Programme and Courses Academic year 2015-2016 Public Health and Clinical Medicine Umeå International School of Public Health
TAKING PART IN CANCER TREATMENT RESEARCH STUDIES
 For more infomation about Cancer Clinical Trials at Upstate Cancer Center please call Upstate Connect 1.800.464.8668 TAKING PART IN CANCER TREATMENT RESEARCH STUDIES Information provided by: National Cancer
For more infomation about Cancer Clinical Trials at Upstate Cancer Center please call Upstate Connect 1.800.464.8668 TAKING PART IN CANCER TREATMENT RESEARCH STUDIES Information provided by: National Cancer
Evaluation of a Primary Care Dermatology Service: final report
 Evaluation of a Primary Care Dermatology Service: final report Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R&D (NCCSDO) December 2005 prepared by Chris Salisbury*
Evaluation of a Primary Care Dermatology Service: final report Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R&D (NCCSDO) December 2005 prepared by Chris Salisbury*
Study Design and Statistical Analysis
 Study Design and Statistical Analysis Anny H Xiang, PhD Department of Preventive Medicine University of Southern California Outline Designing Clinical Research Studies Statistical Data Analysis Designing
Study Design and Statistical Analysis Anny H Xiang, PhD Department of Preventive Medicine University of Southern California Outline Designing Clinical Research Studies Statistical Data Analysis Designing
National Cancer Institute
 National Cancer Institute Taking Part in Cancer Treatment Research Studies U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health Taking Part in Cancer Treatment Research Studies If
National Cancer Institute Taking Part in Cancer Treatment Research Studies U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health Taking Part in Cancer Treatment Research Studies If
Education, occupation, organisation: the dynamics of new occupations in health care
 Education, occupation, organisation: the dynamics of new occupations in health care Peter P. Groenewegen NIVEL Netherlands Institute for Health Services Research Overview The research domain of new occupations
Education, occupation, organisation: the dynamics of new occupations in health care Peter P. Groenewegen NIVEL Netherlands Institute for Health Services Research Overview The research domain of new occupations
Quality of care from the perspective of elderly people: the QUOTE-Elderly instrument
 Age and Ageing 2000; 29: 173 178 2000, British Geriatrics Society Quality of care from the perspective of elderly people: the QUOTE-Elderly instrument HERMAN J. SIXMA, CRÉTIEN VAN CAMPEN, JAN J. KERSSENS,
Age and Ageing 2000; 29: 173 178 2000, British Geriatrics Society Quality of care from the perspective of elderly people: the QUOTE-Elderly instrument HERMAN J. SIXMA, CRÉTIEN VAN CAMPEN, JAN J. KERSSENS,
Clinical Trials: Questions and Answers
 Clinical Trials: Questions and Answers Key Points Clinical trials are research studies that test how well new medical approaches work in people (see Question 1). Every clinical trial has a protocol, which
Clinical Trials: Questions and Answers Key Points Clinical trials are research studies that test how well new medical approaches work in people (see Question 1). Every clinical trial has a protocol, which
Can a tulip become a rose?
 Can a tulip become a rose? The Dutch route of guided self-regulation towards a community based integrated health care system. Niek Klazinga, Diana Delnoij, Isik Kulu-Glasgow Department of Social Medicine
Can a tulip become a rose? The Dutch route of guided self-regulation towards a community based integrated health care system. Niek Klazinga, Diana Delnoij, Isik Kulu-Glasgow Department of Social Medicine
Do nurse practitioners working in primary care provide equivalent care to doctors?
 August 2008 SUPPORT Summary of a systematic review Do nurse practitioners working in primary care provide equivalent care to doctors? Nurse practitioners are nurses who have undergone further training,
August 2008 SUPPORT Summary of a systematic review Do nurse practitioners working in primary care provide equivalent care to doctors? Nurse practitioners are nurses who have undergone further training,
Costing statement: Depression: the treatment and management of depression in adults. (update) and
 and") Costing statement: Depression: the treatment and management of depression in adults (update) and Depression in adults with a chronic physical health problem: treatment and management Summary It has not
Costing statement: Depression: the treatment and management of depression in adults (update) and Depression in adults with a chronic physical health problem: treatment and management Summary It has not
Key words: primary care, gatekeeper, coordination of care, self-referrals, health policy
 Primary Care Physicians in Israel: Self-Perception of Their Role in the Healthcare System and Policy Makers' and Patients' Perception of Them as Gatekeepers Hava Tabenkin MD MSc LLB 1, Revital Gross 2,
Primary Care Physicians in Israel: Self-Perception of Their Role in the Healthcare System and Policy Makers' and Patients' Perception of Them as Gatekeepers Hava Tabenkin MD MSc LLB 1, Revital Gross 2,
Conducting research on road traffic injuries where do I start? Research design, ethics and consent.
 Conducting research on road traffic injuries where do I start? Research design, ethics and consent. Rebecca Ivers, Director, Injury Division, The George Institute Associate Professor, Sydney School of
Conducting research on road traffic injuries where do I start? Research design, ethics and consent. Rebecca Ivers, Director, Injury Division, The George Institute Associate Professor, Sydney School of
Stamped Envelopes and Their Impact on Response Rates
 First Mailings versus Follow-up Mailings: Do the same strategies have the same effects? Emily McFarlane, Joe Murphy, Murrey G. Olmsted RTI International 1 Abstract A number of studies have shown that stamped
First Mailings versus Follow-up Mailings: Do the same strategies have the same effects? Emily McFarlane, Joe Murphy, Murrey G. Olmsted RTI International 1 Abstract A number of studies have shown that stamped
WEEK 10 SUPPLY SIDE REFORM AND REIMBURSEMENT. Activity- based funding versus block grants
 WEEK 10 SUPPLY SIDE REFORM AND REIMBURSEMENT Activity- based funding versus block grants The cost containment thesis was outlined in the previous lecture. In this lecture we examine proffered solutions.
WEEK 10 SUPPLY SIDE REFORM AND REIMBURSEMENT Activity- based funding versus block grants The cost containment thesis was outlined in the previous lecture. In this lecture we examine proffered solutions.
Code of Conduct. Property of UKAPA 20/11/2009 1
 Code of Conduct A Physician Assistant (now associate) (PA) is defined as someone who is: a new healthcare professional who, while not a doctor, works to the medical model, with the attitudes, skills and
Code of Conduct A Physician Assistant (now associate) (PA) is defined as someone who is: a new healthcare professional who, while not a doctor, works to the medical model, with the attitudes, skills and
Physical therapy for patients dying at home of chronic obstructive pulmonary disease A Qualitative Study
 Physical therapy for patients dying at home of chronic obstructive pulmonary disease A Qualitative Study D.M. Keesenberg, Pt, student Science for physical therapy Physical therapy practice Zwanenzijde,
Physical therapy for patients dying at home of chronic obstructive pulmonary disease A Qualitative Study D.M. Keesenberg, Pt, student Science for physical therapy Physical therapy practice Zwanenzijde,
CHAPTER 3. Research methodology
 39 CHAPTER 3 Research methodology 3.1 INTRODUCTION In this chapter the research methodology used in the study is described. The geographical area where the study was conducted, the study design and the
39 CHAPTER 3 Research methodology 3.1 INTRODUCTION In this chapter the research methodology used in the study is described. The geographical area where the study was conducted, the study design and the
Quality in and Equality of Access to Healthcare Services
 Quality in and Equality of Access to Healthcare Services Executive Summary European Commission Directorate-General for Employment, Social Affairs and Equal Opportunities Manuscript completed in March 2008
Quality in and Equality of Access to Healthcare Services Executive Summary European Commission Directorate-General for Employment, Social Affairs and Equal Opportunities Manuscript completed in March 2008
T3.1. Independent Living Applications Portfolio. Henk Herman Nap: h.h.nap@smart-homes.nl. Ad van Berlo: a.vberlo@smart-homes.nl
 T3.1 Independent Living Applications Portfolio Henk Herman Nap: h.h.nap@smart-homes.nl Ad van Berlo: a.vberlo@smart-homes.nl Richard Pasmans: r.pasmans@smart-homes.nl 2013 Roll-out with 7000 users in real
T3.1 Independent Living Applications Portfolio Henk Herman Nap: h.h.nap@smart-homes.nl Ad van Berlo: a.vberlo@smart-homes.nl Richard Pasmans: r.pasmans@smart-homes.nl 2013 Roll-out with 7000 users in real
NATIONAL INFORMATION BOARD. WORK STREAM 1.2 ROADMAP Enable me to make the right health and care choices
 NATIONAL INFORMATION BOARD Personalised Health and Care 2020 WORK STREAM 1.2 ROADMAP Enable me to make the right health and care choices Providing citizens with access to an assessed set of NHS and social
NATIONAL INFORMATION BOARD Personalised Health and Care 2020 WORK STREAM 1.2 ROADMAP Enable me to make the right health and care choices Providing citizens with access to an assessed set of NHS and social
The Regional Growth Fund. Detailed methodology
 The Regional Growth Fund Detailed methodology MAY 2012 2 The Regional Growth Fund Detailed methodology 1 This document outlines the methods used in our examination. Scope 2 This National Audit Office report
The Regional Growth Fund Detailed methodology MAY 2012 2 The Regional Growth Fund Detailed methodology 1 This document outlines the methods used in our examination. Scope 2 This National Audit Office report
Caring for people with multiple chronic conditions in the Netherlands: policy and practices
 Innovating care for people with multiple chronic conditions in Europe Caring for people with multiple chronic conditions in the Netherlands: policy and practices Mieke Rijken a, Simone R. de Bruin b, Sanne
Innovating care for people with multiple chronic conditions in Europe Caring for people with multiple chronic conditions in the Netherlands: policy and practices Mieke Rijken a, Simone R. de Bruin b, Sanne
Bachelor of Science in Social Work, 210 credits (SGSOC)
") PROGRAMME SYLLABUS 1 (8) Reg. no S2012/206 School of Social Work Bachelor of Science in Social Work, 210 (SGSOC) The syllabus for the Bachelor of Science programme in Social Work was approved by the Board
PROGRAMME SYLLABUS 1 (8) Reg. no S2012/206 School of Social Work Bachelor of Science in Social Work, 210 (SGSOC) The syllabus for the Bachelor of Science programme in Social Work was approved by the Board
Master of Science. Public Health Nutrition
 Department of Clinical Sciences and Nutrition Master of Science in Public Health Nutrition Full-Time and Part-Time Taught Modular Masters Programme Module Descriptor Outlines 1 Short Module Descriptors
Department of Clinical Sciences and Nutrition Master of Science in Public Health Nutrition Full-Time and Part-Time Taught Modular Masters Programme Module Descriptor Outlines 1 Short Module Descriptors
The impact and future of QOF in the UK
 The impact and future of QOF in the UK Dr Stephen Campbell On behalf of the Quality Theme, National Primary Care Research and Development Centre, University of Manchester, UK October 2009 Declaration of
The impact and future of QOF in the UK Dr Stephen Campbell On behalf of the Quality Theme, National Primary Care Research and Development Centre, University of Manchester, UK October 2009 Declaration of
PUBLIC HEALTH NUTRITION Master of Science (M.Sc.)
") MODULE HANDBOOK PUBLIC HEALTH NUTRITION Master of Science (M.Sc.) Module Nutritional and Health Politics Credit Points: 10 Degree Programme: MSc Public Health Nutrition ID: OE-MS-GEE Faculty: Nursing and
MODULE HANDBOOK PUBLIC HEALTH NUTRITION Master of Science (M.Sc.) Module Nutritional and Health Politics Credit Points: 10 Degree Programme: MSc Public Health Nutrition ID: OE-MS-GEE Faculty: Nursing and
University of Queensland. Monash University. Southern Health Victoria
 Michele Foster 1 Michele Haynes 1 Martin O Flaherty 1 Geoff Mitchell 1 Elizabeth Skinner 2 Terry Haines 2,3 1 University of Queensland 2 Monash University 3 Southern Health Victoria Emphasis on multidisciplinary
Michele Foster 1 Michele Haynes 1 Martin O Flaherty 1 Geoff Mitchell 1 Elizabeth Skinner 2 Terry Haines 2,3 1 University of Queensland 2 Monash University 3 Southern Health Victoria Emphasis on multidisciplinary
Primary health care in the Netherlands: current situation and trends
 Primary health care in the Netherlands: current situation and trends Prof. Peter P. Groenewegen NIVEL Netherlands Institute for Health Services Research and Utrecht University Contents of my presentation
Primary health care in the Netherlands: current situation and trends Prof. Peter P. Groenewegen NIVEL Netherlands Institute for Health Services Research and Utrecht University Contents of my presentation
Direct Access to Physical Therapy for Patients With Low Back Pain in the Netherlands: Prevalence and Predictors
 Postprint Version Journal website Pubmed link DOI 1.0 http://ptjournal.apta.org/content/early/2013/12/18/ptj.20120330.long http://www.ncbi.nlm.nih.gov/pubmed/?term=24092899 10.2522/ptj.20120330 Direct
Postprint Version Journal website Pubmed link DOI 1.0 http://ptjournal.apta.org/content/early/2013/12/18/ptj.20120330.long http://www.ncbi.nlm.nih.gov/pubmed/?term=24092899 10.2522/ptj.20120330 Direct
Ask Us About Clinical Trials
 Ask Us About Clinical Trials Clinical Trials and You. Our specialists and researchers are at the forefront of their fields and are leading the way in developing new therapies and procedures for diagnosing
Ask Us About Clinical Trials Clinical Trials and You. Our specialists and researchers are at the forefront of their fields and are leading the way in developing new therapies and procedures for diagnosing
Curriculum for to the PhD Program in Pharmacy Administration
 Curriculum for to the PhD Program in Pharmacy Administration Course Hours Course Title BSE 5113 3 Principles of Epidemiology BSE 5163 3 Biostatistics Methods I* BSE 5173 3 Biostatistics Methods II* BSE
Curriculum for to the PhD Program in Pharmacy Administration Course Hours Course Title BSE 5113 3 Principles of Epidemiology BSE 5163 3 Biostatistics Methods I* BSE 5173 3 Biostatistics Methods II* BSE
Key Priority Area 1: Key Direction for Change
 Key Priority Areas Key Priority Area 1: Improving access and reducing inequity Key Direction for Change Primary health care is delivered through an integrated service system which provides more uniform
Key Priority Areas Key Priority Area 1: Improving access and reducing inequity Key Direction for Change Primary health care is delivered through an integrated service system which provides more uniform
Are You Buying Private Medical Insurance? Take a look at this guide before you decide
 Are You Buying Private Medical Insurance? Take a look at this guide before you decide 2012 ARE YOU BUYING PRIVATE MEDICAL INSURANCE? 3 Contents 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. About this guide 4 Understanding
Are You Buying Private Medical Insurance? Take a look at this guide before you decide 2012 ARE YOU BUYING PRIVATE MEDICAL INSURANCE? 3 Contents 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. About this guide 4 Understanding
Commissioning Policy: Defining the boundaries between NHS and Private Healthcare April 2013 Reference : NHSCB/CP/12
 Commissioning Policy: Defining the boundaries between NHS and Private Healthcare April 2013 Reference : NHSCB/CP/12 NHS Commissioning Board Commissioning Policy: Defining the Boundaries between NHS and
Commissioning Policy: Defining the boundaries between NHS and Private Healthcare April 2013 Reference : NHSCB/CP/12 NHS Commissioning Board Commissioning Policy: Defining the Boundaries between NHS and
Mental Health Professionals Attitudes Towards People Who Are Deaf
 Journal of Community & Applied Social Psychology J. Community Appl. Soc. Psychol., 13: 314 319 (2003) Published online 8 June 2003 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/casp.725
Journal of Community & Applied Social Psychology J. Community Appl. Soc. Psychol., 13: 314 319 (2003) Published online 8 June 2003 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/casp.725
Consultation Response Medical profiling and online medicine: the ethics of 'personalised' healthcare in a consumer age Nuffield Council on Bioethics
 Consultation Response Medical profiling and online medicine: the ethics of 'personalised' healthcare in a consumer age Nuffield Council on Bioethics Response by the Genetic Interest Group Question 1: Health
Consultation Response Medical profiling and online medicine: the ethics of 'personalised' healthcare in a consumer age Nuffield Council on Bioethics Response by the Genetic Interest Group Question 1: Health
Health Promotion, Prevention, Medical care, Rehabilitation under the CBR Matrix heading of "Health
 Health Promotion, Prevention, Medical care, Rehabilitation under the CBR Matrix heading of "Health Dr Deepthi N Shanbhag Assistant Professor Department of Community Health St. John s Medical College Bangalore
Health Promotion, Prevention, Medical care, Rehabilitation under the CBR Matrix heading of "Health Dr Deepthi N Shanbhag Assistant Professor Department of Community Health St. John s Medical College Bangalore
How To Compare Social Preferences Of The General Public With The National Health Service
 Social Science & Medicine 64 (2007) 2499 2503 www.elsevier.com/locate/socscimed Do NHS clinicians and members of the public share the same views about reducing inequalities in health? Aki Tsuchiya a,,
Social Science & Medicine 64 (2007) 2499 2503 www.elsevier.com/locate/socscimed Do NHS clinicians and members of the public share the same views about reducing inequalities in health? Aki Tsuchiya a,,
Center for Medicare and Medicaid Innovation
 Center for Medicare and Medicaid Innovation Summary: Establishes within the Centers for Medicare and Medicaid Services (CMS) a Center for Medicare & Medicaid Innovation (CMI). The purpose of the Center
Center for Medicare and Medicaid Innovation Summary: Establishes within the Centers for Medicare and Medicaid Services (CMS) a Center for Medicare & Medicaid Innovation (CMI). The purpose of the Center
Pharmacoeconomic, Epidemiology, and Pharmaceutical Policy and Outcomes Research (PEPPOR) Graduate Program
 Graduate Program") Pharmacoeconomic, Epidemiology, and Pharmaceutical Policy and Outcomes Research (PEPPOR) Graduate Program Front from left: 2010 Graduates Rupali Nail, PhD & Pallavi Jaiswal, MS; Back from left: PEPPOR
Pharmacoeconomic, Epidemiology, and Pharmaceutical Policy and Outcomes Research (PEPPOR) Graduate Program Front from left: 2010 Graduates Rupali Nail, PhD & Pallavi Jaiswal, MS; Back from left: PEPPOR
Questionnaire. Nurses
 Questionnaire Nurses 2 Nurse Questionnaire This form is to be used if you are already a member of the MDU and your day-to-day duties change. In order to ensure we have your accurate work circumstances,
Questionnaire Nurses 2 Nurse Questionnaire This form is to be used if you are already a member of the MDU and your day-to-day duties change. In order to ensure we have your accurate work circumstances,
Integrating care by bundled payments in the Netherlands
 Integrating care by bundled payments in the Netherlands Jeroen N Struijs, PhD National Institute of Public Health and the Environment (RIVM), Department of Quality of Care and Health Economics 1 Content
Integrating care by bundled payments in the Netherlands Jeroen N Struijs, PhD National Institute of Public Health and the Environment (RIVM), Department of Quality of Care and Health Economics 1 Content
Commission on the Future of Health and Social Care in England. The UK private health market
 Commission on the Future of Health and Social Care in England The UK private health market The NHS may dominate the provision of health care in England, but that still leaves the country with a significant
Commission on the Future of Health and Social Care in England The UK private health market The NHS may dominate the provision of health care in England, but that still leaves the country with a significant
INDIGENOUS CHRONIC DISEASE PACKAGE CARE COORDINATION AND SUPPLEMENTARY SERVICES PROGRAM GUIDELINES
 CLOSING THE GAP tackling disease INDIGENOUS CHRONIC DISEASE PACKAGE CARE COORDINATION AND SUPPLEMENTARY SERVICES PROGRAM GUIDELINES November 2012 CONTENTS 1. Introduction... 3 Program Context... 3 Service
CLOSING THE GAP tackling disease INDIGENOUS CHRONIC DISEASE PACKAGE CARE COORDINATION AND SUPPLEMENTARY SERVICES PROGRAM GUIDELINES November 2012 CONTENTS 1. Introduction... 3 Program Context... 3 Service
CASE STUDY. Sunderland dermatology and minor surgery service
 CASE STUDY Sunderland dermatology and minor surgery service October 2014 Specialists in out-ofhospital settings As part of the drive to keep patients out of hospital and better integrate services across
CASE STUDY Sunderland dermatology and minor surgery service October 2014 Specialists in out-ofhospital settings As part of the drive to keep patients out of hospital and better integrate services across
Are you buying private medical insurance? Take a look at this guide before you decide 2008
 Are you buying private medical insurance? Take a look at this guide before you decide 2008 2 Private medical insurance Private medical insurance 3 Contents 1 About this guide 4 2 What is private medical
Are you buying private medical insurance? Take a look at this guide before you decide 2008 2 Private medical insurance Private medical insurance 3 Contents 1 About this guide 4 2 What is private medical
The research was carried out by: Carol Borrill, Michael West, Jeremy Dawson Aston Business School, Aston University.
 The research was carried out by: Carol Borrill, Michael West, Jeremy Dawson Aston Business School, Aston University. David Shapiro, Anne Rees, Ann Richards University of Leeds. Simon Garrod, Jean Carletta
The research was carried out by: Carol Borrill, Michael West, Jeremy Dawson Aston Business School, Aston University. David Shapiro, Anne Rees, Ann Richards University of Leeds. Simon Garrod, Jean Carletta
Six Month Pilot Analysis: Improving Rehabilitation for Men with Prostate Cancer in North East London
 Six Month Pilot Analysis: Improving Rehabilitation for Men with Prostate Cancer in North East London June 2015 Helen Whitney (Physiotherapist and Prostate Cancer Project Lead) Thufayel Islam (Prostate
Six Month Pilot Analysis: Improving Rehabilitation for Men with Prostate Cancer in North East London June 2015 Helen Whitney (Physiotherapist and Prostate Cancer Project Lead) Thufayel Islam (Prostate
Data Analysis: Analyzing Data - Inferential Statistics
 WHAT IT IS Return to Table of ontents WHEN TO USE IT Inferential statistics deal with drawing conclusions and, in some cases, making predictions about the properties of a population based on information
WHAT IT IS Return to Table of ontents WHEN TO USE IT Inferential statistics deal with drawing conclusions and, in some cases, making predictions about the properties of a population based on information
Executive Summary. 1. What is the temporal relationship between problem gambling and other co-occurring disorders?
 Executive Summary The issue of ascertaining the temporal relationship between problem gambling and cooccurring disorders is an important one. By understanding the connection between problem gambling and
Executive Summary The issue of ascertaining the temporal relationship between problem gambling and cooccurring disorders is an important one. By understanding the connection between problem gambling and
PHEPA II INTERIM COUNTRY REPORT - SLOVENIA
 PHEPA II INTERIM COUNTRY REPORT - SLOVENIA Istanbul, 8. 9. October 2007 Dr. Marko Kolšek Department of Family Medicine Medical faculty University of Ljubljana, Slovenia Current policies and activities:
PHEPA II INTERIM COUNTRY REPORT - SLOVENIA Istanbul, 8. 9. October 2007 Dr. Marko Kolšek Department of Family Medicine Medical faculty University of Ljubljana, Slovenia Current policies and activities:
Standards of proficiency. Operating department practitioners
 Standards of proficiency Operating department practitioners Contents Foreword 1 Introduction 3 Standards of proficiency 7 Foreword We are pleased to present the Health and Care Professions Council s standards
Standards of proficiency Operating department practitioners Contents Foreword 1 Introduction 3 Standards of proficiency 7 Foreword We are pleased to present the Health and Care Professions Council s standards
Office ID Location: City State Date / / PRIMARY CARE SURVEY
 A. Organizational Characteristics PRIMARY CARE SURVEY We want to learn more about the general features of your office. A1. What health-related services does your office provide (check all that apply)?
A. Organizational Characteristics PRIMARY CARE SURVEY We want to learn more about the general features of your office. A1. What health-related services does your office provide (check all that apply)?
Service delivery interventions
 Service delivery interventions S A S H A S H E P P E R D D E P A R T M E N T O F P U B L I C H E A L T H, U N I V E R S I T Y O F O X F O R D CO- C O O R D I N A T I N G E D I T O R C O C H R A N E E P
Service delivery interventions S A S H A S H E P P E R D D E P A R T M E N T O F P U B L I C H E A L T H, U N I V E R S I T Y O F O X F O R D CO- C O O R D I N A T I N G E D I T O R C O C H R A N E E P
Graduate Curriculum Guide Course Descriptions: Core and DNP
 Graduate Curriculum Guide Course Descriptions: Core and DNP APN Core Courses (35 credits total) N502 Theoretical Foundations of Nursing Practice (3 credits) Theoretical Foundations of Nursing Practice
Graduate Curriculum Guide Course Descriptions: Core and DNP APN Core Courses (35 credits total) N502 Theoretical Foundations of Nursing Practice (3 credits) Theoretical Foundations of Nursing Practice
The Trend of Public Perception of Healthcare in Japan From the 4th Perception Survey of Japanese Healthcare *1
 Field Report The Trend of Public Perception of Healthcare in Japan From the 4th Perception Survey of Japanese Healthcare *1 JMAJ 56(4): 267 274, 13 Narumi EGUCHI* 2 Abstract It is estimated that the population
Field Report The Trend of Public Perception of Healthcare in Japan From the 4th Perception Survey of Japanese Healthcare *1 JMAJ 56(4): 267 274, 13 Narumi EGUCHI* 2 Abstract It is estimated that the population
Summary of health effects
 Review of Findings on Chronic Disease Self- Management Program (CDSMP) Outcomes: Physical, Emotional & Health-Related Quality of Life, Healthcare Utilization and Costs Summary of health effects The major
Review of Findings on Chronic Disease Self- Management Program (CDSMP) Outcomes: Physical, Emotional & Health-Related Quality of Life, Healthcare Utilization and Costs Summary of health effects The major
Employee Benefit Trends Study Australia
 Employee Benefit Trends Study Australia The easy and effective way to differentiate your business Contents About us 1 Global expertise 1 1. Latest trends in employee benefits 2 2. Key issues 3 3. The rest
Employee Benefit Trends Study Australia The easy and effective way to differentiate your business Contents About us 1 Global expertise 1 1. Latest trends in employee benefits 2 2. Key issues 3 3. The rest
Frede Olesen. Frede Olesen
 Former GP Professor, dr. med. sci. Research unit for General Practice, Aarhus University (Chaiman for the Danish Cancer Society untill 01.06.2015) Some of my first observations 1976-85 Variation in use
Former GP Professor, dr. med. sci. Research unit for General Practice, Aarhus University (Chaiman for the Danish Cancer Society untill 01.06.2015) Some of my first observations 1976-85 Variation in use
Patients expectations of private osteopathic care in the UK: a national survey of patients
 Patients expectations of private osteopathic care in the UK: a national survey of patients C.M. Janine Leach, Anne Mandy, Vinette Cross, Carol A. Fawkes, Ann P. Moore IICAOR London 2012 Acknowledgements
Patients expectations of private osteopathic care in the UK: a national survey of patients C.M. Janine Leach, Anne Mandy, Vinette Cross, Carol A. Fawkes, Ann P. Moore IICAOR London 2012 Acknowledgements
The family physician system reform in small cities in I.R. Iran
 Evaluating Impact: Turning Promises into Evidence The family physician system reform in small cities in I.R. Iran Masoud Abolhallaj, Abbas Vosoogh, Arash Rashidian, Alireza Delavari Cairo, January 2008
Evaluating Impact: Turning Promises into Evidence The family physician system reform in small cities in I.R. Iran Masoud Abolhallaj, Abbas Vosoogh, Arash Rashidian, Alireza Delavari Cairo, January 2008
Appendix 10. The Speaker of the House of Representatives of the States General PO Box 20018 2500 EA THE HAGUE DE/2008/8871
 Appendix 10 The Speaker of the House of Representatives of the States General PO Box 20018 2500 EA THE HAGUE The Hague Our reference DE/2008/8871 Subject Policy response to Sardes report, TalentForce and
Appendix 10 The Speaker of the House of Representatives of the States General PO Box 20018 2500 EA THE HAGUE The Hague Our reference DE/2008/8871 Subject Policy response to Sardes report, TalentForce and
Attitudes of nursing staff towards involvement in medical end-of-life decisions: a national survey study
 Postprint Version 1.0 Journal website Pubmed link DOI http://www.sciencedirect.com/science/article/pii/s0738399113003935 http://www.ncbi.nlm.nih.gov/pubmed/24268920 10.1016/j.pec.2013.09.018 Attitudes
Postprint Version 1.0 Journal website Pubmed link DOI http://www.sciencedirect.com/science/article/pii/s0738399113003935 http://www.ncbi.nlm.nih.gov/pubmed/24268920 10.1016/j.pec.2013.09.018 Attitudes
Standards for specialist education and practice
 Standards for specialist education and practice This document is now the UKCC s exclusive reference document specifying standards for specialist practice. Any previous documentation, as detailed below,
Standards for specialist education and practice This document is now the UKCC s exclusive reference document specifying standards for specialist practice. Any previous documentation, as detailed below,
ANALYSIS FOR OUTCOMES BETTER USE OF DATA TO IMPROVE OUTCOMES
 Chair Cabinet Committee on State Sector Reform and Expenditure Control ANALYSIS FOR OUTCOMES BETTER USE OF DATA TO IMPROVE OUTCOMES Purpose 1. This paper reports back on business case work to develop a
Chair Cabinet Committee on State Sector Reform and Expenditure Control ANALYSIS FOR OUTCOMES BETTER USE OF DATA TO IMPROVE OUTCOMES Purpose 1. This paper reports back on business case work to develop a
A cross-sectional study to assess the long-term health status of patients with lower respiratory tract infections, including Q fever
 Postprint Version Journal website 1.0 http://journals.cambridge.org/action/displayabstract?frompage=online&aid=9204 662&fileId=S0950268814000417 Pubmed link http://www.ncbi.nlm.nih.gov/pubmed/?term=24625631
Postprint Version Journal website 1.0 http://journals.cambridge.org/action/displayabstract?frompage=online&aid=9204 662&fileId=S0950268814000417 Pubmed link http://www.ncbi.nlm.nih.gov/pubmed/?term=24625631
Standards of proficiency. Arts therapists
 Standards of proficiency Arts therapists Contents Foreword 1 Introduction 3 Standards of proficiency 7 Foreword We are pleased to present the Health and Care Professions Council s standards of proficiency
Standards of proficiency Arts therapists Contents Foreword 1 Introduction 3 Standards of proficiency 7 Foreword We are pleased to present the Health and Care Professions Council s standards of proficiency
Are you buying private medical insurance? Take a look at this guide before you decide 2008
 Are you buying private medical insurance? Take a look at this guide before you decide 2008 2 Private medical insurance Private medical insurance 3 Contents 1. About this guide 4 2. What is private medical
Are you buying private medical insurance? Take a look at this guide before you decide 2008 2 Private medical insurance Private medical insurance 3 Contents 1. About this guide 4 2. What is private medical
Alcohol treatment in England 2012-13
 Alcohol treatment in England 2012-13 October 2013 About Public Health England Public Health England s mission is to protect and improve the nation s health and to address inequalities through working with
Alcohol treatment in England 2012-13 October 2013 About Public Health England Public Health England s mission is to protect and improve the nation s health and to address inequalities through working with
An Assessment of the Effect of Misreporting of Phone Line Information on Key Weighted RDD Estimates
 An Assessment of the Effect of Misreporting of Phone Line Information on Key Weighted RDD Estimates Ashley Bowers 1, Jeffrey Gonzalez 2 1 University of Michigan 2 Bureau of Labor Statistics Abstract Random-digit
An Assessment of the Effect of Misreporting of Phone Line Information on Key Weighted RDD Estimates Ashley Bowers 1, Jeffrey Gonzalez 2 1 University of Michigan 2 Bureau of Labor Statistics Abstract Random-digit
Personal Insurance. Do I need Trauma cover? a safety. to help get you back on track
 Personal Insurance Do I need Trauma cover? a safety to help get you back on track Being able to focus on your recovery after suffering a traumatic event is going to be your primary concern. Having trauma
Personal Insurance Do I need Trauma cover? a safety to help get you back on track Being able to focus on your recovery after suffering a traumatic event is going to be your primary concern. Having trauma
Research Agenda for General Practice / Family Medicine and Primary Health Care in Europe Summary EGPRN
 Research Agenda for General Practice / Family Medicine and Primary Health Care in Europe Summary EGPRN EUROPEAN GENERAL PRACTICE RESEARCH NETWO RK EGPRN is a network organisation within WONCA Region Europe
Research Agenda for General Practice / Family Medicine and Primary Health Care in Europe Summary EGPRN EUROPEAN GENERAL PRACTICE RESEARCH NETWO RK EGPRN is a network organisation within WONCA Region Europe
Telehealth for carers communication skills: Research report
 Telehealth for carers communication skills: Research report Professor Leanne Togher Dr Emma Power Rachael Rietdijk 6 March 2015 Research report #: 073-0315-R01 This research report was prepared by Professor
Telehealth for carers communication skills: Research report Professor Leanne Togher Dr Emma Power Rachael Rietdijk 6 March 2015 Research report #: 073-0315-R01 This research report was prepared by Professor
About the consultation
 Hearing Aid Council and Health Professions Council consultation on standards of proficiency and the threshold level of qualification for entry to the Hearing Aid Audiologists/Dispensers part of the Register.
Hearing Aid Council and Health Professions Council consultation on standards of proficiency and the threshold level of qualification for entry to the Hearing Aid Audiologists/Dispensers part of the Register.
(Resolutions, recommendations and opinions) RECOMMENDATIONS COUNCIL
 RECOMMENDATIONS COUNCIL") 3.7.2009 Official Journal of the European Union C 151/1 I (Resolutions, recommendations and opinions) RECOMMENDATIONS COUNCIL COUNCIL RECOMMENDATION of 9 June 2009 on patient safety, including the prevention
3.7.2009 Official Journal of the European Union C 151/1 I (Resolutions, recommendations and opinions) RECOMMENDATIONS COUNCIL COUNCIL RECOMMENDATION of 9 June 2009 on patient safety, including the prevention
Title Older people s participation and engagement in falls prevention interventions: Comparing rates and settings
 Title Older people s participation and engagement in falls prevention interventions: Comparing rates and settings Keywords: patient adherence; falls, accidental; intervention studies; patient participation;
Title Older people s participation and engagement in falls prevention interventions: Comparing rates and settings Keywords: patient adherence; falls, accidental; intervention studies; patient participation;
Barriers & Incentives to Obtaining a Bachelor of Science Degree in Nursing
 Southern Adventist Univeristy KnowledgeExchange@Southern Graduate Research Projects Nursing 4-2011 Barriers & Incentives to Obtaining a Bachelor of Science Degree in Nursing Tiffany Boring Brianna Burnette
Southern Adventist Univeristy KnowledgeExchange@Southern Graduate Research Projects Nursing 4-2011 Barriers & Incentives to Obtaining a Bachelor of Science Degree in Nursing Tiffany Boring Brianna Burnette
Family Focused Therapy for Bipolar Disorder (Clinical Case Series) Participant Information Sheet
 Participant Information Sheet") Family Focused Therapy for Bipolar Disorder (Clinical Case Series) Participant Information Sheet Study Title: Family Focused Therapy for Bipolar Disorder: A Clinical Case Series) We would like to invite
Family Focused Therapy for Bipolar Disorder (Clinical Case Series) Participant Information Sheet Study Title: Family Focused Therapy for Bipolar Disorder: A Clinical Case Series) We would like to invite
What you will study on the MPH Master of Public Health (online)
") Public Health Foundations Core This module builds upon the nine core competencies of Public Health Practice set out by the Faculty of Public Health UK. The English NHS will form the central empirical case
Public Health Foundations Core This module builds upon the nine core competencies of Public Health Practice set out by the Faculty of Public Health UK. The English NHS will form the central empirical case
JSNA Factsheet Template Tower Hamlets Joint Strategic Needs Assessment 2010 2011
 JSNA Factsheet Template Tower Hamlets Joint Strategic Needs Assessment 2010 2011. Executive Summary This fact sheet considers breast cancer, with a particular emphasis on breast screening and raising awareness
JSNA Factsheet Template Tower Hamlets Joint Strategic Needs Assessment 2010 2011. Executive Summary This fact sheet considers breast cancer, with a particular emphasis on breast screening and raising awareness
James E. Bartlett, II is Assistant Professor, Department of Business Education and Office Administration, Ball State University, Muncie, Indiana.
 Organizational Research: Determining Appropriate Sample Size in Survey Research James E. Bartlett, II Joe W. Kotrlik Chadwick C. Higgins The determination of sample size is a common task for many organizational
Organizational Research: Determining Appropriate Sample Size in Survey Research James E. Bartlett, II Joe W. Kotrlik Chadwick C. Higgins The determination of sample size is a common task for many organizational
Your local specialist mental health services
 Your local specialist mental health services Primary Care Liaison Service B&NES Primary Care Mental Health Liaison service is a short-term support service to help people with mental health difficulties
Your local specialist mental health services Primary Care Liaison Service B&NES Primary Care Mental Health Liaison service is a short-term support service to help people with mental health difficulties
THE EUROPEAN DEFINITION OF GENERAL PRACTICE / FAMILY MEDICINE
 Network organisation within WONCA Region Europe - ESGP/FM European Academy of Teachers in General Practice (Network within WONCA Europe) THE EUROPEAN DEFINITION OF GENERAL PRACTICE / FAMILY MEDICINE SHORT
Network organisation within WONCA Region Europe - ESGP/FM European Academy of Teachers in General Practice (Network within WONCA Europe) THE EUROPEAN DEFINITION OF GENERAL PRACTICE / FAMILY MEDICINE SHORT
Quality and critical appraisal of clinical practice guidelines a relevant topic for health care?
 Quality and critical appraisal of clinical practice guidelines a relevant topic for health care? Françoise Cluzeau, PhD St George s Hospital Medical School, London on behalf of the AGREE Collaboration
Quality and critical appraisal of clinical practice guidelines a relevant topic for health care? Françoise Cluzeau, PhD St George s Hospital Medical School, London on behalf of the AGREE Collaboration
The National Health Plan for Young Australians An action plan to protect and promote the health of children and young people
 The National Health Plan for Young Australians An action plan to protect and promote the health of children and young people Copyright 1997 ISBN 0 642 27200 X This work is copyright. It may be reproduced
The National Health Plan for Young Australians An action plan to protect and promote the health of children and young people Copyright 1997 ISBN 0 642 27200 X This work is copyright. It may be reproduced
Travel Distance to Healthcare Centers is Associated with Advanced Colon Cancer at Presentation
 Travel Distance to Healthcare Centers is Associated with Advanced Colon Cancer at Presentation Yan Xing, MD, PhD, Ryaz B. Chagpar, MD, MS, Y Nancy You MD, MHSc, Yi Ju Chiang, MSPH, Barry W. Feig, MD, George
Travel Distance to Healthcare Centers is Associated with Advanced Colon Cancer at Presentation Yan Xing, MD, PhD, Ryaz B. Chagpar, MD, MS, Y Nancy You MD, MHSc, Yi Ju Chiang, MSPH, Barry W. Feig, MD, George
Perceptions of Adding Nurse Practitioners to Primary Care Teams
 Quality in Primary Care (2015) 23 (2): 122-126 2015 Insight Medical Publishing Group Short Communication Interprofessional Research Article Collaboration: Co-workers' Perceptions of Adding Nurse Practitioners
Quality in Primary Care (2015) 23 (2): 122-126 2015 Insight Medical Publishing Group Short Communication Interprofessional Research Article Collaboration: Co-workers' Perceptions of Adding Nurse Practitioners
CHILDREN, YOUTH AND WOMEN S HEALTH SERVICE JOB AND PERSON SPECIFICATION
 CHILDREN, YOUTH AND WOMEN S HEALTH SERVICE JOB AND PERSON SPECIFICATION POSITION DETAILS Position Title: Senior Clinical Psychologist Classification: PO2 Position No: WC0469 Cost Centre: 02811 Reports
CHILDREN, YOUTH AND WOMEN S HEALTH SERVICE JOB AND PERSON SPECIFICATION POSITION DETAILS Position Title: Senior Clinical Psychologist Classification: PO2 Position No: WC0469 Cost Centre: 02811 Reports
Nursing Knowledge for Your Benefit
 Nursing Knowledge for Your Benefit Policy of the Icelandic Nurses Association on Nursing and Health Care 2011-2020 About this Policy The present Policy of the Icelandic Nurses Association (INA) was developed
Nursing Knowledge for Your Benefit Policy of the Icelandic Nurses Association on Nursing and Health Care 2011-2020 About this Policy The present Policy of the Icelandic Nurses Association (INA) was developed
HEALTH INSURANCE REFORM IN THE NETHERLANDS
 HEALTH INSURANCE REFORM IN THE NETHERLANDS STEFAN GREß*, MARAL MANOUGUIAN** AND JÜRGEN WASEM*** At the beginning of 2006 the Dutch government introduced a fundamental reform of the health insurance system.
HEALTH INSURANCE REFORM IN THE NETHERLANDS STEFAN GREß*, MARAL MANOUGUIAN** AND JÜRGEN WASEM*** At the beginning of 2006 the Dutch government introduced a fundamental reform of the health insurance system.
Inquiry into the out-of-pocket costs in Australian healthcare
 Submission to the Senate Standing Committee on Community Affairs - References Committee Inquiry into the out-of-pocket costs in Australian healthcare May 2014 Out-of-pocket costs in Australian healthcare
Submission to the Senate Standing Committee on Community Affairs - References Committee Inquiry into the out-of-pocket costs in Australian healthcare May 2014 Out-of-pocket costs in Australian healthcare
Standards of proficiency. Occupational therapists
 Standards of proficiency Occupational therapists Contents Foreword 1 Introduction 3 Standards of proficiency 7 Foreword We are pleased to present the Health and Care Professions Council s standards of
Standards of proficiency Occupational therapists Contents Foreword 1 Introduction 3 Standards of proficiency 7 Foreword We are pleased to present the Health and Care Professions Council s standards of
JOB DESCRIPTION. Advanced Nurse Practitioner Professional Lead
 JOB DESCRIPTION JOB TITLE: RESPONSIBLE TO: LOCATION(S): JOB PROFILE: Advanced Nurse Practitioner Advanced Nurse Practitioner Professional Lead North Bristol Trust Southmead Hospital This role is to work
JOB DESCRIPTION JOB TITLE: RESPONSIBLE TO: LOCATION(S): JOB PROFILE: Advanced Nurse Practitioner Advanced Nurse Practitioner Professional Lead North Bristol Trust Southmead Hospital This role is to work