North Carolina Story Collection Campaign on the Health Care Coverage Gap
|
|
|
- Madeleine Beasley
- 8 years ago
- Views:
Transcription
1 TOOLKIT North Carolina Story Collection Campaign on the Health Care Coverage Gap North Carolina Community Health Center Association 4917 Waters Edge Drive, Suite 165 Raleigh, NC Updated 11/10/15

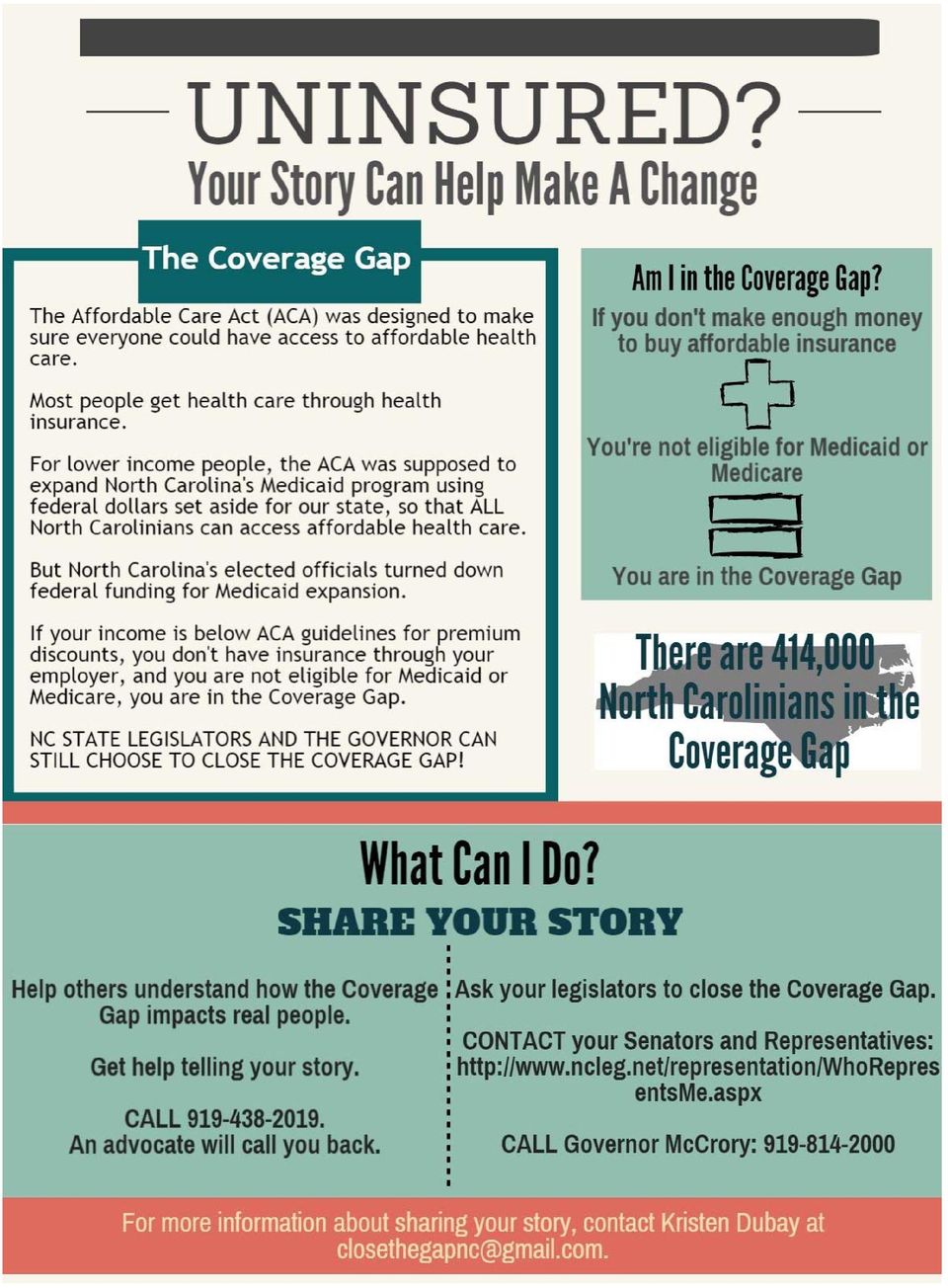
2 Thank You Thank you for your willingness to support North Carolinians who fall in the Health Insurance Coverage Gap. This toolkit is designed to provide support for people across the state interacting with those in the Coverage Gap, so you can direct them to engaging on this issue. The focus of this particular engagement action is sharing his/her story so it can be highlighted in media or through contact with policy makers so they understand why closing the Coverage Gap in North Carolina is so important. This toolkit is meant to help you connect individuals you identify in the coverage gap with our organization and others working to Close the Coverage Gap. We hope this project will empower those in the Coverage Gap and help them to feel their concerns are heard. This toolkit is provided to help you feel more comfortable making this connection. CONTENTS: 1. Flyer about the Health Insurance Coverage Gap and Sharing Consumer Stories explains what the Coverage Gap is and how to share a story. 2. Draft script for asking a consumer if they are willing to participate in the Story Collection Project. 3. An authorization form this is a separate consent form specifically for the story collection effort. Scan it and send it to closethegapnc@gmail.com or fax it to Someone on the story collection team will follow up with the consumer. 4. A follow up letter for the consumer to thank them and to provide information about who is leading this project. 5. A request for individuals to share their pictures if they don t feel comfortable sharing their entire story. 6. A quick story form to gather information from individuals who don t have time to complete an interview. THANK YOU for helping us identify individuals in the Coverage Gap. We could not succeed with this project without your assistance. Sincerely,

3 Making the Ask Will you share your story? AFTER IDENTIFYING A PATIENT IS IN THE COVERAGE GAP, THIS IS ONE WAY TO ASK A CONSUMER IF HE/SHE WOULD BE WILLING TO PARTICIPATE IN THE STORY COLLECTION PROJECT: Mr. Smith, I m really sorry you don t qualify for subsidies on the federal marketplace. You are what we call the health insurance Coverage Gap. You don t have access to employer sponsored insurance, you don t qualify for Medicaid or Medicare, and your income is too low to get affordable coverage through HealthCare.gov. The federal government set aside funding for North Carolina to offer subsidies or Medicaid to people like you in the Coverage Gap but so far our state leaders have chosen not to do so. Advocates around the state are looking for personal Coverage Gap stories like to show how people and communities are impacted. Would you be interested in sharing your experience with advocates working on this issue? WAIT FOR THE ANSWER. IF YES: Thank you so much for your willingness. Signing this authorization form allows me to share your contact information with the NC Community Health Center Association, which is leading the Story Collection project. They may choose to use your story in a story booklet or connect you with other advocates working on this issue. However, we (or our colleagues at the NCCHCA) will be sure to double check with you first before your story is publicly shared. We want to make sure you are completely comfortable with how your story is used. IF NO: I understand. Health issues are very personal. If you change your mind, feel free to let me know. Another option is to share your photo. The advocates are collecting photos of individuals in the coverage gap to draw attention to the vast number of impacted. You can text a photo (or selfie) to (919) or send it via to closethegapnc@gmail.com. Please remember you can always come to our community health center for your primary care needs. We will do all we can to help. Thank you so much.

4
5 AUTHORIZATION AND RELEASE FOR USES AND DISCLOSURES OF PROTECTED HEALTH INFORMATION (PHI) AND RELEASE OF RIGHTS AUTHORIZATION AND RELEASE FOR USES AND DISCLOSURES OF PROTECTED HEALTH INFORMATION (PHI) AND RELEASE OF RIGHTS Section A: This section must be completed for all Authorizations I authorize Community Health Center (CHC),, and the North Carolina Community Health Center Association (NCCHCA) to use or disclose the specific Information about me described below, for the Purpose(s) described below. Patient name: Birth Date: Phone Number: Patient Address: E mail address: Information To Be Used Or Disclosed My name and any photograph or video in which I may appear. Protected health information about me (as defined in the Federal Health Insurance Portability and Accountability Act (HIPAA)). This may include information about my access to care, the care I have received, my clinical outcomes, my health conditions, my income, and my insurance status. Any other information I may share during an interview. Purpose(s) For The Use Or Disclosure I acknowledge and agree that the CHC or NCCHCA may use and disclose all or any part of the Information described above, including protected health information: for marketing, educational, policy advocacy, and public relations purposes; and in press releases, print and online publications, public service announcements, and other materials ( Materials ), any or all of which may be printed, transmitted, broadcast, posted online, or otherwise published in any type of media. Release of Rights I hereby grant to NCCHCA any and all rights I may have with regard to any Materials, including any copyright in them. On behalf of myself and any family member about whom I may share information, and to the fullest extent permitted by law, I waive all rights and release any claim based upon or relating to the use or disclosure of the Information as set forth above. This waiver of rights and release of claims shall include, but not necessarily be limited to: Claims against the CHC, NCCHCA, NCCHCA's members, and any of their agents, employees, directors, officers, successors and assigns; Claims for invasion of any right to privacy, violation of any right of publicity, violation of any law regarding protected health information, or any similar matter; and Claims that may have been unknown or unforeseenonthedateisignedthisauthorization. I understand that: 1. I may refuse to sign this authorization and that this authorization is strictly voluntary. 2. My treatment, payment, enrollment or eligibility for benefits may not be conditioned on signing this authorization. 3. I may revoke this authorization at any time in writing, but if I do, it will not have any effect on any Materials published or actions taken by the PCC or NCCHCA before the organization received the revocation. (To revoke this authorization, please contact NCCHCA at (919) or contact your CHC directly.) 4. Unless I choose to revoke this authorization, it remains in effect and will not expire until the CHC or NCCHCA decide to no longer publish or use any Information. 5. Once released, my information may no longer be protected by federal privacy regulations and may be re disclosed. 6. I understand that I may see and obtain a copy of the information described on this form or a copy of this form, if I ask for it. 7. This authorization is given without any promise that I will receive compensation. Section B: Signature I have read the above and authorize the disclosure of the protected health information as stated. Signature of Patient/Guardian/Patient Representative: Date: Print Name of Patient/Patient Representative Relationship or scope of your legal authority to act on the patient s behalf:

6 The Story Collection Project Closing the Coverage Gap in NC Hello! Thank you for being willing to share your health care experiences with us. We believe sharing stories of real people who cannot access needed health care services will be a powerful way to show how increasing access to insurance coverage can positively impact the lives of more than 400,000 North Carolinians. By giving your contact information to one of our health center colleagues, you are giving them permission to share it with us. A number of organizations across the state are working to encourage our state leaders to increase access to insurance coverage for those in the coverage gap population, meaning they make less than 100% of the federal poverty level and do not qualify for insurance through an employer, the Affordable Care Act, Medicaid, or Medicare. Next, you can call (919) and leave a message with information about your health care coverage story. If we don t hear from you directly, one of the organizations connected with this work, most likely the NC Community Health Center Association, will contact you to learn more about your experiences. Below is the contact information for our organization and our address. Feel free to call us directly, otherwise, you can expect a call from us soon. Thank you for your participation! Kristen Dubay NC Community Health Center Association, closethegapnc@gmail.com To get help telling the story of your struggle to access affordable health care coverage, call (919)

7 Don t want to share your story but still want to help? Share your picture! We are compiling photos showing faces of those in the coverage gap. If you would be willing to share a picture of yourself, consider taking one of these two actions: A) Take a selfie or have a friend take your picture and it to us at closethegapnc@gmail.com or text it to us at (919) B) If you are unable to or text your picture, give us a call at (919) , leave a message with your name and contact information, and we will call you back with details about collecting your picture for this project. Thank you for your participation! NC Community Health Center Association, To get help telling the story of your struggle to access affordable health care coverage, call (919)
 If you are unable to email or text your picture, give us a call at (919)438 2019, leave a message with your name and contact information, and we will call you back with details about collecting")
8 Don t have time for an interview but still want to tell your story? Complete this quick story form! Name: Age: Community of Residence: Occupation: Phone: Address or 1. How long have you been uninsured? 2. How do you access the health care you need? What care are you UNABLE to access? 3. How does your lack of health insurance impact your life? 1. If you could communicate with NC legislators about expanding insurance coverage, what would you tell them? 5. Being uninsured keeps me from. Thank you for your participation! Kristen Dubay NC Community Health Center Association, closethegapnc@gmail.com To get help telling the story of your struggle to access affordable health care coverage, call (919)

University of Mississippi Medical Center Office of Integrity and Compliance
 Office of Integrity and Effective Date: 2005 By: Committee 1.0 PURPOSE The purpose of this policy is to guide (UMMC) employees, who are involved with research, in obtaining an authorization for the use
Office of Integrity and Effective Date: 2005 By: Committee 1.0 PURPOSE The purpose of this policy is to guide (UMMC) employees, who are involved with research, in obtaining an authorization for the use
HIPAA (The Health Insurance Portability and Accountability Act)
") Section 16. HIPAA Requirements and Information HIPAA (The Health Insurance Portability and Accountability Act) Molina Healthcare s Commitment to Patient Privacy Protecting the privacy of members personal
Section 16. HIPAA Requirements and Information HIPAA (The Health Insurance Portability and Accountability Act) Molina Healthcare s Commitment to Patient Privacy Protecting the privacy of members personal
Releasing Information
 Releasing Information There are 3 kinds of release situations now: our original Release of Information and it s uses under Colorado Law and Professional Ethical Standards; HPAA s Consent to release information
Releasing Information There are 3 kinds of release situations now: our original Release of Information and it s uses under Colorado Law and Professional Ethical Standards; HPAA s Consent to release information
Kathleen Long, Ph.D. 510 A Pollock Street New Bern, NC 28562 Phone: (252) 636-2286 Fax: (252) 636-5677
 636-2286 Fax: (252) 636-5677") Kathleen Long, Ph.D. 510 A Pollock Street New Bern, NC 28562 Phone: (252) 636-2286 Fax: (252) 636-5677 Welcome! Please take a minute to complete the following information. Your name: Phone Number: Address:
Kathleen Long, Ph.D. 510 A Pollock Street New Bern, NC 28562 Phone: (252) 636-2286 Fax: (252) 636-5677 Welcome! Please take a minute to complete the following information. Your name: Phone Number: Address:
SDC-League Health Fund
 SDC-League Health Fund 1501 Broadway, 17 th Floor New York, NY 10036 Tel: 212-869-8129 Fax: 212-302-6195 E-mail: health@sdcweb.org NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION
SDC-League Health Fund 1501 Broadway, 17 th Floor New York, NY 10036 Tel: 212-869-8129 Fax: 212-302-6195 E-mail: health@sdcweb.org NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION
Mendel Psychological Associates
 PSYCHOLOGIST- PATIENT SERVICES AGREEMENT This document is an agreement between therapist: and client:. Welcome to our practice. This document (the Agreement) contains important information about professional
PSYCHOLOGIST- PATIENT SERVICES AGREEMENT This document is an agreement between therapist: and client:. Welcome to our practice. This document (the Agreement) contains important information about professional
Southern Counseling and Psychological Services LLC 104B E. Linda Vista, Roswell, NM 88201 (575) 420-1853 Fax (575) 624-8889
 420-1853 Fax (575) 624-8889") Southern Counseling and Psychological Services LLC 104B E. Linda Vista, Roswell, NM 88201 (575) 420-1853 Fax (575) 624-8889 PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT Welcome to my practice. This document
Southern Counseling and Psychological Services LLC 104B E. Linda Vista, Roswell, NM 88201 (575) 420-1853 Fax (575) 624-8889 PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT Welcome to my practice. This document
REGISTRATION FORM (Please print)
") REGISTRATION FORM (Please print) PATIENT INFORMATION Patient s last name: First: Middle: Mr. Mrs. Miss Ms. Marital status (circle one) Single / Mar / Div / Sep / Wid Is this your legal name? If not so,
REGISTRATION FORM (Please print) PATIENT INFORMATION Patient s last name: First: Middle: Mr. Mrs. Miss Ms. Marital status (circle one) Single / Mar / Div / Sep / Wid Is this your legal name? If not so,
PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT
 The Bethesda Group Psychological Services, LLC Old Georgetown Office Park 7988 Old Georgetown Road, 8A Bethesda, Maryland 20814 Phone 301.718.4544 Fax 301.718.4545 info@thebethesdagroup.com PSYCHOTHERAPIST-PATIENT
The Bethesda Group Psychological Services, LLC Old Georgetown Office Park 7988 Old Georgetown Road, 8A Bethesda, Maryland 20814 Phone 301.718.4544 Fax 301.718.4545 info@thebethesdagroup.com PSYCHOTHERAPIST-PATIENT
Integrative Psycho-Therapy and Assessment Services, P.L.L.C. PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT
 Integrative Psycho-Therapy and Assessment Services, P.L.L.C. PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT Welcome to my practice. This document (the Agreement) contains important information about my professional
Integrative Psycho-Therapy and Assessment Services, P.L.L.C. PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT Welcome to my practice. This document (the Agreement) contains important information about my professional
How To Complete The Kcdcoastal Health Cooperative'S Authorization To Disclose Protected Health Information Form
 Authorization to Use and Disclose Protected Health Information Form Under the HIPAA Privacy Rule, an individual may authorize the release of his or her protected health information (PHI) to a specific
Authorization to Use and Disclose Protected Health Information Form Under the HIPAA Privacy Rule, an individual may authorize the release of his or her protected health information (PHI) to a specific
Michael S. McLane, Psy.D. Licensed Psychologist. Informed Consent to Treatment / Evaluation I,, who was born on and who resides at
 Michael S. McLane, Psy.D. Licensed Psychologist 12830 Hillcrest Road Suite D233 Dallas, TX 75230 Ph: (972) 620-1225 Fax: (972) 620-4393 Informed Consent to Treatment / Evaluation I,, who was born on and
Michael S. McLane, Psy.D. Licensed Psychologist 12830 Hillcrest Road Suite D233 Dallas, TX 75230 Ph: (972) 620-1225 Fax: (972) 620-4393 Informed Consent to Treatment / Evaluation I,, who was born on and
Leonard M. Bohanon, PhD Psychologist
 2203 Timberloch Pl., Suite 100 PERSONAL DATA RECORD Client Name: Date of Birth Address: City/State/Zip: Home Phone: Cell Phone: SSN: Work Phone: Other Phone: TXDL: Employer/School: Referred to Our Office
2203 Timberloch Pl., Suite 100 PERSONAL DATA RECORD Client Name: Date of Birth Address: City/State/Zip: Home Phone: Cell Phone: SSN: Work Phone: Other Phone: TXDL: Employer/School: Referred to Our Office
Policies for Easter Seals South Carolina Therapy Services
 Policies for Easter Seals South Carolina Therapy Services It is our goal to serve you and your child with excellence. Please carefully read through the following policies. 1. During or prior to your initial
Policies for Easter Seals South Carolina Therapy Services It is our goal to serve you and your child with excellence. Please carefully read through the following policies. 1. During or prior to your initial
Deborah Issokson, Psy.D.
 Deborah Issokson, Psy.D. Licensed Psychologist HEALTHCARE PRIVACY AND SECURITY POLICIES PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT Welcome to my practice. This document (the Agreement) contains important
Deborah Issokson, Psy.D. Licensed Psychologist HEALTHCARE PRIVACY AND SECURITY POLICIES PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT Welcome to my practice. This document (the Agreement) contains important
WELCOME TO MY PRACTICE Thank you for choosing me as your therapist. I am looking forward to our work together and providing you with assistance.
 Lorie Jenddryka, MS, LCPC, CH 800 E. Northwest Highway, Suite 500 Palatine, IL 60074 (847) 794-8836 WELCOME TO MY PRACTICE Thank you for choosing me as your therapist. I am looking forward to our work
Lorie Jenddryka, MS, LCPC, CH 800 E. Northwest Highway, Suite 500 Palatine, IL 60074 (847) 794-8836 WELCOME TO MY PRACTICE Thank you for choosing me as your therapist. I am looking forward to our work
Worker s Compensation Intake Form
 Worker s Compensation Intake Form Patient Information: Name Home Phone Address Work Phone Social Security No. Date of Birth Sex Male Female Height Weight lbs Occupation Marital Status Employer No of Children
Worker s Compensation Intake Form Patient Information: Name Home Phone Address Work Phone Social Security No. Date of Birth Sex Male Female Height Weight lbs Occupation Marital Status Employer No of Children
RACHEL LACY, PSY.D., PC 1805 Herrington Road, Building 2 Lawrenceville, GA 30043. PSYCHOTHERAPIST- PATIENT AGREEMENT (Revision 01/12)
") RACHEL LACY, PSY.D., PC 1805 Herrington Road, Building 2 Lawrenceville, GA 30043 1 PSYCHOTHERAPIST- PATIENT AGREEMENT (Revision 01/12) Welcome to my practice. This agreement contains important information
RACHEL LACY, PSY.D., PC 1805 Herrington Road, Building 2 Lawrenceville, GA 30043 1 PSYCHOTHERAPIST- PATIENT AGREEMENT (Revision 01/12) Welcome to my practice. This agreement contains important information
APPENDIX 1: Frequently Asked Questions
 APPENDIX 1: Frequently Asked Questions Practice Name Q: What is the HIPAA Privacy Rule? A: The HIPAA Privacy Rule controls the use and disclosure of what is known as Protected Health Information (PHI).
APPENDIX 1: Frequently Asked Questions Practice Name Q: What is the HIPAA Privacy Rule? A: The HIPAA Privacy Rule controls the use and disclosure of what is known as Protected Health Information (PHI).
PSYCHOTHERAPIST-CLIENT SERVICES AGREEMENT
 PSYCHOTHERAPIST-CLIENT SERVICES AGREEMENT Welcome to my practice. This document (the Agreement) contains important information about my professional services and business policies. It also contains summary
PSYCHOTHERAPIST-CLIENT SERVICES AGREEMENT Welcome to my practice. This document (the Agreement) contains important information about my professional services and business policies. It also contains summary
FAQ on Remote Identity Proofing, Remote Identity Proofing Failures and Application Inconsistencies (Federally-facilitated Marketplace)
") FAQ on Remote Identity Proofing, Remote Identity Proofing Failures and Application Inconsistencies (Federally-facilitated Marketplace) Updated May 21, 2014 This document outlines information on identity
FAQ on Remote Identity Proofing, Remote Identity Proofing Failures and Application Inconsistencies (Federally-facilitated Marketplace) Updated May 21, 2014 This document outlines information on identity
www.attorneygeneral.gov
 Required fields are marked with an asterisk* Your information: Are you a veteran? Yes No Are you on active duty? Yes No Age Group: Under 18 18-34 35-59 60-64 65 and older Mr. Mrs. Address* Ms. Dr. Name*
Required fields are marked with an asterisk* Your information: Are you a veteran? Yes No Are you on active duty? Yes No Age Group: Under 18 18-34 35-59 60-64 65 and older Mr. Mrs. Address* Ms. Dr. Name*
Ann Dunnewold, Ph.D., 2012
 1 Ann Dunnewold, Ph.D. 8140 Walnut Hill Lane, Suite 100 Dallas, TX 75231 (214) 343-1353 PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT Welcome to my practice. This document (the Agreement) contains important
1 Ann Dunnewold, Ph.D. 8140 Walnut Hill Lane, Suite 100 Dallas, TX 75231 (214) 343-1353 PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT Welcome to my practice. This document (the Agreement) contains important
I. Individual (Name and information of person whose protected health information is being disclosed): Jane Doe 05-10-1962
: Jane Doe 05-10-1962") Instructions for Completing Standard Authorization Form To Complete Form go to Page 4 of 5 Use this form to authorize Blue Cross Blue Shield of Texas to disclose your protected health information (PHI)
Instructions for Completing Standard Authorization Form To Complete Form go to Page 4 of 5 Use this form to authorize Blue Cross Blue Shield of Texas to disclose your protected health information (PHI)
Notice of Privacy Practices
 LiveWell Group 7781 Cooper Road 2 nd floor Suite 5 Cincinnati OH, 45242 Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET
LiveWell Group 7781 Cooper Road 2 nd floor Suite 5 Cincinnati OH, 45242 Notice of Privacy Practices THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET
MEDICAL BENEFITS CLASS ACTION SETTLEMENT NOTICE OF INTENT TO SUE
 MEDICAL BENEFITS CLASS ACTION SETTLEMENT NOTICE OF INTENT TO SUE Complete this form if you are a MEDICAL BENEFITS SETTLEMENT CLASS MEMBER seeking to exercise a BACK END LITIGATION OPTION. In addition to
MEDICAL BENEFITS CLASS ACTION SETTLEMENT NOTICE OF INTENT TO SUE Complete this form if you are a MEDICAL BENEFITS SETTLEMENT CLASS MEMBER seeking to exercise a BACK END LITIGATION OPTION. In addition to
Dale C. Godby, Ph.D., ABPP, CGP 6330 LBJ Suite 150 Dallas, Texas 75240 972-233-0648
 Dale C. Godby, Ph.D., ABPP, CGP 6330 LBJ Suite 150 Dallas, Texas 75240 972-233-0648 Problems in love and work, as well as troubling symptoms like depression and anxiety, often lead people to seek therapy.
Dale C. Godby, Ph.D., ABPP, CGP 6330 LBJ Suite 150 Dallas, Texas 75240 972-233-0648 Problems in love and work, as well as troubling symptoms like depression and anxiety, often lead people to seek therapy.
HIPAA INFORMATION FOR METLIFE GROUP DENTAL and/or VISION INSURANCE CUSTOMERS
 HIPAA INFORMATION FOR METLIFE GROUP DENTAL and/or VISION INSURANCE CUSTOMERS Dear Group Dental and/or Vision Customer : This letter relates to privacy requirements contained in federal regulations under
HIPAA INFORMATION FOR METLIFE GROUP DENTAL and/or VISION INSURANCE CUSTOMERS Dear Group Dental and/or Vision Customer : This letter relates to privacy requirements contained in federal regulations under
Jennifer L. Trotter, Ph.D.
 Jennifer L. Trotter, Ph.D. Telephone: 248-880-4966 - Email: JenniferLTrotter@gmail.com Licensed Clinical Psychologist Address: 25882 Orchard Lake Road - Suite L-4 - Farmington Hills, MI 48336 OUTPATIENT
Jennifer L. Trotter, Ph.D. Telephone: 248-880-4966 - Email: JenniferLTrotter@gmail.com Licensed Clinical Psychologist Address: 25882 Orchard Lake Road - Suite L-4 - Farmington Hills, MI 48336 OUTPATIENT
HIPAA COMPLIANCE INFORMATION. HIPAA Policy
 HIPAA COMPLIANCE INFORMATION HIPAA Policy Use of Protected Health Information for Research Policy University of North Texas Health Science Center at Fort Worth Applicability: All University of North Texas
HIPAA COMPLIANCE INFORMATION HIPAA Policy Use of Protected Health Information for Research Policy University of North Texas Health Science Center at Fort Worth Applicability: All University of North Texas
You and Healthcare Reform. You and your benefits through The Distirct. You and Insurance Marketplaces (Exchanges)
") You and Healthcare Reform The Patient Protection and Affordable Care Act (PPACA, also known as Healthcare Reform) is a set of laws that affect healthcare coverage in the United States. While there is a
You and Healthcare Reform The Patient Protection and Affordable Care Act (PPACA, also known as Healthcare Reform) is a set of laws that affect healthcare coverage in the United States. While there is a
The HIPAA Privacy Rule: Overview and Impact
 The HIPAA Privacy Rule: Overview and Impact DISCLAIMER: This information is provided as is without any express or implied warranty. It is provided for educational purposes only and does not constitute
The HIPAA Privacy Rule: Overview and Impact DISCLAIMER: This information is provided as is without any express or implied warranty. It is provided for educational purposes only and does not constitute
HIPAA Compliance And Participation in the National Oncologic Pet Registry Project
 HIPAA Compliance And Participation in the National Oncologic Pet Registry Project Your facility has indicated its willingness to participate in the National Oncologic PET Registry Project (NOPR) sponsored
HIPAA Compliance And Participation in the National Oncologic Pet Registry Project Your facility has indicated its willingness to participate in the National Oncologic PET Registry Project (NOPR) sponsored
PATIENT RECORDS PRIVACY POLICIES AND PROCEDURES FOR HIPAA COMPLIANCE (4/03)
") PATIENT RECORDS PRIVACY POLICIES AND PROCEDURES FOR HIPAA COMPLIANCE (4/03) Use and Disclosure of PHI: Protected Health Information ( PHI ) may not be used or disclosed in violation of the Health Insurance
PATIENT RECORDS PRIVACY POLICIES AND PROCEDURES FOR HIPAA COMPLIANCE (4/03) Use and Disclosure of PHI: Protected Health Information ( PHI ) may not be used or disclosed in violation of the Health Insurance
Personal Information - Protecting And Balancing It At Hulse QM
 Hulse/QM Healthcare Advocacy Program Notice of Privacy Practices THIS NOTICE DESCRIBES HOW PERSONAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE
Hulse/QM Healthcare Advocacy Program Notice of Privacy Practices THIS NOTICE DESCRIBES HOW PERSONAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE
BUSINESS ASSOCIATE AGREEMENT FOR ATTORNEYS
 BUSINESS ASSOCIATE AGREEMENT FOR ATTORNEYS This Business Associate Agreement (this Agreement ), is made as of the day of, 20 (the Effective Date ), by and between ( Business Associate ) and ( Covered Entity
BUSINESS ASSOCIATE AGREEMENT FOR ATTORNEYS This Business Associate Agreement (this Agreement ), is made as of the day of, 20 (the Effective Date ), by and between ( Business Associate ) and ( Covered Entity
NOTICE OF PRIVACY PRACTICES
 THE PHYSICIAN PRACTICE, P.A. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
THE PHYSICIAN PRACTICE, P.A. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
DETAILED NOTICE OF PRIVACY AND SECURITY PRACTICES OF THE Trustees of the Stevens Institute of Technology Health & Welfare Plan
 DETAILED NOTICE OF PRIVACY AND SECURITY PRACTICES OF THE Trustees of the Stevens Institute of Technology Health & Welfare Plan THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED
DETAILED NOTICE OF PRIVACY AND SECURITY PRACTICES OF THE Trustees of the Stevens Institute of Technology Health & Welfare Plan THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED
THE HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA) EMPLOYEE TRAINING MANUAL
 EMPLOYEE TRAINING MANUAL") THE HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA) EMPLOYEE TRAINING MANUAL What is HIPAA? Comprehensive federal legislation regarding health insurance which is comprised of four key areas:
THE HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA) EMPLOYEE TRAINING MANUAL What is HIPAA? Comprehensive federal legislation regarding health insurance which is comprised of four key areas:
Sincerely, Donated Dental Services (DDS) Program Coordinator
 Program Coordinator") DONATED DENTAL SERVICES (DDS) Dear Applicant: In response to your request for more information regarding how to apply for donated dental care, we are pleased to provide the following information and application
DONATED DENTAL SERVICES (DDS) Dear Applicant: In response to your request for more information regarding how to apply for donated dental care, we are pleased to provide the following information and application
INDIVIDUALS WITH DISABILITIES EDUCATION ACT NOTICE OF PROCEDURAL SAFEGUARDS
 INDIVIDUALS WITH DISABILITIES EDUCATION ACT NOTICE OF PROCEDURAL SAFEGUARDS Tennessee Department of Education Division of Special Education Department of Education February 11, 2008; Publication Authorization
INDIVIDUALS WITH DISABILITIES EDUCATION ACT NOTICE OF PROCEDURAL SAFEGUARDS Tennessee Department of Education Division of Special Education Department of Education February 11, 2008; Publication Authorization
Health Insurance Portability and Accountability Policy 1.8.4
 Health Insurance Portability and Accountability Policy 1.8.4 Appendix C Uses and Disclosures of PHI Procedures This Appendix covers procedures related to Uses and Disclosures of PHI. Disclosures to Law
Health Insurance Portability and Accountability Policy 1.8.4 Appendix C Uses and Disclosures of PHI Procedures This Appendix covers procedures related to Uses and Disclosures of PHI. Disclosures to Law
REQUEST FOR INDEPENDENT EXTERNAL REVIEW OF A HEALTH INSURANCE GRIEVANCE THROUGH THE OFFICE OF PATIENT PROTECTION
 The Commonwealth of Massachusetts Health Policy Commission Office of Patient Protection 50 Milk Street, 8 th Floor Boston, MA 02109 (800)436-7757 (phone) (617)624-5046 (fax) REQUEST FOR INDEPENDENT EXTERNAL
The Commonwealth of Massachusetts Health Policy Commission Office of Patient Protection 50 Milk Street, 8 th Floor Boston, MA 02109 (800)436-7757 (phone) (617)624-5046 (fax) REQUEST FOR INDEPENDENT EXTERNAL
Doctors Weight Loss Center of Cary Patient Information Form (please print)
") Doctors Weight Loss Center of Cary Patient Information Form (please print) Patient Name: Date: City: State: Zip Code: Home Phone: Cell Phone: Marital Status: Date of Birth: Email: Your Primary Care Provider:
Doctors Weight Loss Center of Cary Patient Information Form (please print) Patient Name: Date: City: State: Zip Code: Home Phone: Cell Phone: Marital Status: Date of Birth: Email: Your Primary Care Provider:
HOSPICE INFORMED CONSENT
 HOSPICE INFORMED CONSENT PATIENT NAME: INSTRUCTIONS: This form is used to acknowledge receipt of our Orientation Booklet and confirm your understanding and agreement with its contents. Your signature below
HOSPICE INFORMED CONSENT PATIENT NAME: INSTRUCTIONS: This form is used to acknowledge receipt of our Orientation Booklet and confirm your understanding and agreement with its contents. Your signature below
2015 Annual Patient Paperwork Update for Existing Patients
 2015 Annual Patient Paperwork Update for Existing Patients DATE: ͺͺͺͺ ŚĞĐŬ WƌĞĨĞƌƌĞĚ ůŝŷŝđ &ƚ tăljŷğ 'ƌğğŷǁžžě
2015 Annual Patient Paperwork Update for Existing Patients DATE: ͺͺͺͺ ŚĞĐŬ WƌĞĨĞƌƌĞĚ ůŝŷŝđ &ƚ tăljŷğ 'ƌğğŷǁžžě
Maryland Insurance Administration
 Maryland Insurance Administration Today s Date: COMPLAINT FORM Life and Health Insurance Please use this form to submit a complaint about an insurance company The Maryland Insurance Administration (MIA)
Maryland Insurance Administration Today s Date: COMPLAINT FORM Life and Health Insurance Please use this form to submit a complaint about an insurance company The Maryland Insurance Administration (MIA)
DURABLE POWER OF ATTORNEY FOR HEALTH CARE
 ELDER LAW & DISABILITY RIGHTS SECTION DURABLE POWER OF ATTORNEY FOR HEALTH CARE I,, am of sound mind, and I (Print or type your full name) voluntarily make this designation. APPOINTMENT OF PATIENT ADVOCATE
ELDER LAW & DISABILITY RIGHTS SECTION DURABLE POWER OF ATTORNEY FOR HEALTH CARE I,, am of sound mind, and I (Print or type your full name) voluntarily make this designation. APPOINTMENT OF PATIENT ADVOCATE
How To Get A Life Insurance Policy In Gorgonia
 Employee Enrollment Application For 51+ Employee s Georgia You, the employee, must complete this application. You are solely responsible for its accuracy and completeness. To avoid the possibility of delay,
Employee Enrollment Application For 51+ Employee s Georgia You, the employee, must complete this application. You are solely responsible for its accuracy and completeness. To avoid the possibility of delay,
PATIENT INTAKE FORM PATIENT INFORMATION. Name Soc. Sec. # Last Name First Name Initial Address. City State Zip. Home Phone Work/Mobile Phone
 PATIENT INTAKE FORM PATIENT INFORMATION Name Soc. Sec. # Last Name First Name Initial Address City State Zip Home Phone Work/Mobile Phone Sex M F Age Birth date Single Married Widowed Separated Divorced
PATIENT INTAKE FORM PATIENT INFORMATION Name Soc. Sec. # Last Name First Name Initial Address City State Zip Home Phone Work/Mobile Phone Sex M F Age Birth date Single Married Widowed Separated Divorced
Genworth Life Insurance Company Genworth Life Insurance Company of New York NOTICE OF PRIVACY PRACTICES
 Genworth Life Insurance Company Genworth Life Insurance Company of New York NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
Genworth Life Insurance Company Genworth Life Insurance Company of New York NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
Blood & Marrow Transplant Group of Georgia Patient Demographic Form PLEASE FILL OUT FRONT AND BACK OF THIS FORM
 Blood & Marrow Transplant Group of Georgia Patient Demographic Form ***Please complete entire form---do not leave any blanks*** BLOOD MARROW TRANSPLANT GROUP OF GEORGIA DEMOGRAPHIC FORM H. Kent Holland,
Blood & Marrow Transplant Group of Georgia Patient Demographic Form ***Please complete entire form---do not leave any blanks*** BLOOD MARROW TRANSPLANT GROUP OF GEORGIA DEMOGRAPHIC FORM H. Kent Holland,
Personal Injury Intake Form
 Personal Injury Intake Form Patient Information: Name Home Phone Address Work Phone Cell Phone Date of Birth Social Security # Sex Male Female Height Weight lbs Occupation Marital Status Employer No of
Personal Injury Intake Form Patient Information: Name Home Phone Address Work Phone Cell Phone Date of Birth Social Security # Sex Male Female Height Weight lbs Occupation Marital Status Employer No of
Long-Term Disability Income Benefit. Employee s Statement
 Long-Term Disability Income Benefit Employee s Statement Employee s Statement Long Term Disability Income Benefits This guide explains how to apply for Long Term Disability benefits. It contains the form
Long-Term Disability Income Benefit Employee s Statement Employee s Statement Long Term Disability Income Benefits This guide explains how to apply for Long Term Disability benefits. It contains the form
Ph. 540.370.4344 Fx. 540.370.4345 Email: dclcsw@dclcsw.com
 Personal Information Client Name(s): Date: Client Address: E-mail: Home Phone Number: OK to call at work? Y N Work Phone Number: Mobile Phone Number: Date of Birth: Age: Sex: M F Ethnicity: Social Security
Personal Information Client Name(s): Date: Client Address: E-mail: Home Phone Number: OK to call at work? Y N Work Phone Number: Mobile Phone Number: Date of Birth: Age: Sex: M F Ethnicity: Social Security
Chicago Homeless Management Information System (HMIS) Privacy Packet
 Privacy Packet") Chicago Homeless Management Information System (HMIS) Privacy Packet Table of Contents Standard Agency Privacy Practices Notice... 3 Chicago Standard HMIS Privacy Posting... 6 Client Consent Form for Data
Chicago Homeless Management Information System (HMIS) Privacy Packet Table of Contents Standard Agency Privacy Practices Notice... 3 Chicago Standard HMIS Privacy Posting... 6 Client Consent Form for Data
HIPAA POLICIES & PROCEDURES AND ADMINISTRATIVE FORMS TABLE OF CONTENTS
 HIPAA POLICIES & PROCEDURES AND ADMINISTRATIVE FORMS TABLE OF CONTENTS 1. HIPAA Privacy Policies & Procedures Overview (Policy & Procedure) 2. HIPAA Privacy Officer (Policy & Procedure) 3. Notice of Privacy
HIPAA POLICIES & PROCEDURES AND ADMINISTRATIVE FORMS TABLE OF CONTENTS 1. HIPAA Privacy Policies & Procedures Overview (Policy & Procedure) 2. HIPAA Privacy Officer (Policy & Procedure) 3. Notice of Privacy
Notice of Privacy Practices. Human Resources Division Employees Benefits Section
 Notice of Privacy Practices Human Resources Division Employees Benefits Section THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
Notice of Privacy Practices Human Resources Division Employees Benefits Section THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
NOTICE OF PRIVACY PRACTICES Murdoch Developmental Center. Effective Date: April 14, 2003
 NOTICE OF PRIVACY PRACTICES Murdoch Developmental Center Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS
NOTICE OF PRIVACY PRACTICES Murdoch Developmental Center Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS
HIPAA Medical Billing Requirements For Research
 The Health Insurance Portability and Accountability Act (HIPAA) Excerpted from the UTC IRB Policy June 2008 Table of Contents PART V: The Health Insurance Portability and Accountability Act (HIPAA)...
The Health Insurance Portability and Accountability Act (HIPAA) Excerpted from the UTC IRB Policy June 2008 Table of Contents PART V: The Health Insurance Portability and Accountability Act (HIPAA)...
INDIVIDUAL HIPAA RIGHTS (Health Insurance Portability and Accountability Act)
") INDIVIDUAL HIPAA RIGHTS (Health Insurance Portability and Accountability Act) All staff with access to protected health information will follow the procedures below: Alternate Communications: The district
INDIVIDUAL HIPAA RIGHTS (Health Insurance Portability and Accountability Act) All staff with access to protected health information will follow the procedures below: Alternate Communications: The district
INTERMEDIARY AND PRODUCER COMPENSATION NOTICE
 INTERMEDIARY AND PRODUCER COMPENSATION NOTICE MetLife enters into arrangements concerning the sale, servicing and/or renewal of MetLife group insurance and certain other group-related products ( Products
INTERMEDIARY AND PRODUCER COMPENSATION NOTICE MetLife enters into arrangements concerning the sale, servicing and/or renewal of MetLife group insurance and certain other group-related products ( Products
Michael S. McLane, Psy.D. Licensed Psychologist. Informed Consent to Treatment / Evaluation of a Minor Child. who was born on and who resides at
 Michael S. McLane, Psy.D. Licensed Psychologist 12830 Hillcrest Road Suite D233 Dallas, TX 75230 Ph: (972) 620-1225 Fax: (972) 620-4393 Informed Consent to Treatment / Evaluation of a Minor Child I am
Michael S. McLane, Psy.D. Licensed Psychologist 12830 Hillcrest Road Suite D233 Dallas, TX 75230 Ph: (972) 620-1225 Fax: (972) 620-4393 Informed Consent to Treatment / Evaluation of a Minor Child I am
CLIENT INFORMATION FORM
 Please take a moment to complete this form. We will consider it, along with your group s experience, enrollment data, and any other applicable information, when setting up your account with Delta Dental.
Please take a moment to complete this form. We will consider it, along with your group s experience, enrollment data, and any other applicable information, when setting up your account with Delta Dental.
A Consumer s Guide to Internal Appeals and External Reviews
 A Consumer s Guide to Internal Appeals and External Reviews The Iowa Insurance Division, Consumer Advocate Bureau http://www.insuranceca.iowa.gov June 2012 Table of Contents Introduction Page 3 Chapter
A Consumer s Guide to Internal Appeals and External Reviews The Iowa Insurance Division, Consumer Advocate Bureau http://www.insuranceca.iowa.gov June 2012 Table of Contents Introduction Page 3 Chapter
A PSYCHOLOGICAL SERVICE DR. PAMELA REBECK
 A PSYCHOLOGICAL SERVICE DR. PAMELA REBECK PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT AND INFORMED CONSENT Welcome to my practice. This document (the Agreement) contains important information about my professional
A PSYCHOLOGICAL SERVICE DR. PAMELA REBECK PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT AND INFORMED CONSENT Welcome to my practice. This document (the Agreement) contains important information about my professional
Patient Bill of Rights and Responsibilities
 Patient Bill of Rights and Responsibilities The patient or the patient s legal representative has the right to be informed of the patient s rights and responsibilities as a patient through effective means
Patient Bill of Rights and Responsibilities The patient or the patient s legal representative has the right to be informed of the patient s rights and responsibilities as a patient through effective means
BUSINESS ASSOCIATE AGREEMENT
 BUSINESS ASSOCIATE AGREEMENT Express Scripts, Inc. and one or more of its subsidiaries ( ESI ), and Sponsor or one of its affiliates ( Sponsor ), are parties to an agreement ( PBM Agreement ) whereby ESI
BUSINESS ASSOCIATE AGREEMENT Express Scripts, Inc. and one or more of its subsidiaries ( ESI ), and Sponsor or one of its affiliates ( Sponsor ), are parties to an agreement ( PBM Agreement ) whereby ESI
HIPAA (Health Insurance Portability and Accountability Act of 1996) Stetson University HIPAA Training
 Stetson University HIPAA Training") HIPAA (Health Insurance Portability and Accountability Act of 1996) Stetson University HIPAA Training Objectives of this Training l To help you understand: l What HIPAA privacy rule is l Why it is important
HIPAA (Health Insurance Portability and Accountability Act of 1996) Stetson University HIPAA Training Objectives of this Training l To help you understand: l What HIPAA privacy rule is l Why it is important
PSYCHOTHERAPY CONTRACT
 Aaron J. Dodini, Ph.D. Licensed Clinical Psychologist Licensed Marriage & Family Therapist PSYCHOTHERAPY CONTRACT Welcome to my practice. This document contains important information about my professional
Aaron J. Dodini, Ph.D. Licensed Clinical Psychologist Licensed Marriage & Family Therapist PSYCHOTHERAPY CONTRACT Welcome to my practice. This document contains important information about my professional
IDAHO STATE UNIVERSITY POLICIES AND PROCEDURES (ISUPP) HIPAA Privacy Use and Disclosure of Psychotherapy Notes 10130
 HIPAA Privacy Use and Disclosure of Psychotherapy Notes 10130") IDAHO STATE UNIVERSITY POLICIES AND PROCEDURES (ISUPP) HIPAA Privacy Use and Disclosure of Psychotherapy Notes 10130 POLICY INFORMATION Major Functional Area (MFA): MFA X - Office of General Counsel &
IDAHO STATE UNIVERSITY POLICIES AND PROCEDURES (ISUPP) HIPAA Privacy Use and Disclosure of Psychotherapy Notes 10130 POLICY INFORMATION Major Functional Area (MFA): MFA X - Office of General Counsel &
Metropolitan Living, LLC 151 W. Burnsville Parkway, Suite 101 Burnsville, MN 55337 Ph: (952) 564-3030 Fax: (651) 925-0031
 564-3030 Fax: (651) 925-0031") The Health Insurance Portability and Accountability Act (HIPAA) and Client Privacy Statement This notice describes how your medical information may be used and disclosed and how you can get access to this
The Health Insurance Portability and Accountability Act (HIPAA) and Client Privacy Statement This notice describes how your medical information may be used and disclosed and how you can get access to this
IDAHO Advance Directive Planning for Important Healthcare Decisions
 IDAHO Advance Directive Planning for Important Healthcare Decisions CaringInfo 1731 King St., Suite 100 Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National (NHPCO),
IDAHO Advance Directive Planning for Important Healthcare Decisions CaringInfo 1731 King St., Suite 100 Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National (NHPCO),
Counseling Intake Form (Each person attending therapy should complete a form)
") Counseling Intake Form (Each person attending therapy should complete a form) Name Male Female Mailing Address Date of Birth Home Phone Work Email How would you like to be contacted? Home Work Email Okay
Counseling Intake Form (Each person attending therapy should complete a form) Name Male Female Mailing Address Date of Birth Home Phone Work Email How would you like to be contacted? Home Work Email Okay
BILLING INFORMATION AND ASSIGNMENT OF BENEFITS
 BILLING INFORMATION AND ASSIGNMENT OF BENEFITS Facility: Northpoint Radiation Center Pro Physicians Clinic PA Physician: Timothy D. Nichols, M.D. PA, Board Certified Radiation Oncology Wilhelm J. Lubbe,
BILLING INFORMATION AND ASSIGNMENT OF BENEFITS Facility: Northpoint Radiation Center Pro Physicians Clinic PA Physician: Timothy D. Nichols, M.D. PA, Board Certified Radiation Oncology Wilhelm J. Lubbe,
California Life Settlement Qualification Form
 PERSONAL INFORMATION California Life Settlement Qualification Form First Insured Name: SS # Current Address: City: State: Zip: Date of Birth: Driver s License Number: State: Expiration: Second Insured
PERSONAL INFORMATION California Life Settlement Qualification Form First Insured Name: SS # Current Address: City: State: Zip: Date of Birth: Driver s License Number: State: Expiration: Second Insured
Who to call for an emergency: Name: Relationship: Home Phone: ( ) - Work Phone: ( ) - Cell Phone: ( ) -
 - Work Phone: ( ) - Cell Phone: ( ) -") 4425 Ponce de Leon Blvd., Suite 115 Email:info@ Dr. Mercedes Gonzalez, Pediatric Dermatologist Patient Information: Patient Name: Social Security Number: / / Date of Birth: / / Sex: M / F (Circle one)
4425 Ponce de Leon Blvd., Suite 115 Email:info@ Dr. Mercedes Gonzalez, Pediatric Dermatologist Patient Information: Patient Name: Social Security Number: / / Date of Birth: / / Sex: M / F (Circle one)
SUPPORT PATH PROGRAM INTAKE FORM PHONE: 1-855-769-7284 FAX: 1-855-298-8700
 SUPPORT PATH PROGRAM INTAKE FORM PHONE: 1-855-769-7284 FAX: 1-855-298-8700 1 REQUESTED SERVICE(S) (REQUIRED) CHECK ALL BOXES THAT APPLY Benefits Investigation Prior Authorization and Appeals Support Patient
SUPPORT PATH PROGRAM INTAKE FORM PHONE: 1-855-769-7284 FAX: 1-855-298-8700 1 REQUESTED SERVICE(S) (REQUIRED) CHECK ALL BOXES THAT APPLY Benefits Investigation Prior Authorization and Appeals Support Patient
JANET PURCELL, PH.D. 1818 N.E. IRVING STREET PORTLAND, OR 97232 PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT
 JANET PURCELL, PH.D. 1818 N.E. IRVING STREET PORTLAND, OR 97232 PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT This document contains important information about my professional and business policies. It also
JANET PURCELL, PH.D. 1818 N.E. IRVING STREET PORTLAND, OR 97232 PSYCHOTHERAPIST-PATIENT SERVICES AGREEMENT This document contains important information about my professional and business policies. It also
These are just some of the eligibility requirements meeting these criteria does not guarantee acceptance.
 BARACLUDE PATIENT ASSISTANCE PROGRAM The Baraclude Patient Assistance Program is designed to provide free medication to qualifying patients who do not have prescription drug coverage and are having a hard
BARACLUDE PATIENT ASSISTANCE PROGRAM The Baraclude Patient Assistance Program is designed to provide free medication to qualifying patients who do not have prescription drug coverage and are having a hard
ATTORNEY-CLIENT WORKERS COMPENSTATION FEE CONTRACT AND AUTHORIZATION TO REPRESENT
 STATE OF GEORGIA ATTORNEY-CLIENT WORKERS COMPENSTATION FEE CONTRACT AND AUTHORIZATION TO REPRESENT I,, with a Social Security Number of the undersigned, do hereby retain the Ramos Law Firm, LLC, located
STATE OF GEORGIA ATTORNEY-CLIENT WORKERS COMPENSTATION FEE CONTRACT AND AUTHORIZATION TO REPRESENT I,, with a Social Security Number of the undersigned, do hereby retain the Ramos Law Firm, LLC, located
Conroe Physician Associates. Patient Consent Form. I fully understand that this is given in advance of any specific diagnosis or treatment.
 Conroe Physician Associates Patient Consent Form Please Read and Sign I, undersigned, hereby consent to the following: Administration and performance of all treatments Administration of any needed anesthetics
Conroe Physician Associates Patient Consent Form Please Read and Sign I, undersigned, hereby consent to the following: Administration and performance of all treatments Administration of any needed anesthetics
Dear Friend: God bless you. Rev. Dr. Howard S. Russell President and CEO
 Dear Friend: If you have been ill, I am sorry to hear of your medical need. I want you to know that all of us here at the Christian Healthcare Ministries office are praying for your recovery. We will especially
Dear Friend: If you have been ill, I am sorry to hear of your medical need. I want you to know that all of us here at the Christian Healthcare Ministries office are praying for your recovery. We will especially
AMAZING BIKE CAMP JUNE 22 26, 2015
 AMAZING BIKE CAMP JUNE 22 26, 2015 REGISTRATION FORM The Children s Institute of Pittsburgh partners with icanshine (formerly Lose the Training Wheels) to offer this unique camp that teaches children with
AMAZING BIKE CAMP JUNE 22 26, 2015 REGISTRATION FORM The Children s Institute of Pittsburgh partners with icanshine (formerly Lose the Training Wheels) to offer this unique camp that teaches children with
Notice of Privacy Practices
 SHANNON LERACH, Ph.D. Licensed Clinical Psychologist PSY23705 243 N. Highway 101, Suite 16, Solana Beach, CA 92075 Telephone: (619) 817.5320 Fax: (858) 481.1674 Notice of Privacy Practices This Notice
SHANNON LERACH, Ph.D. Licensed Clinical Psychologist PSY23705 243 N. Highway 101, Suite 16, Solana Beach, CA 92075 Telephone: (619) 817.5320 Fax: (858) 481.1674 Notice of Privacy Practices This Notice
MEDICAL LIEN CONTRACT. Date Patient Name Patient Date of Birth Date of Loss
 MEDICAL LIEN CONTRACT Date Patient Name Patient Date of Birth Date of Loss Payment to Provider: I, ( Patient ), hereby authorize and direct you ( Attorney ), to pay directly to ( Provider ) AND/OR TO ANY
MEDICAL LIEN CONTRACT Date Patient Name Patient Date of Birth Date of Loss Payment to Provider: I, ( Patient ), hereby authorize and direct you ( Attorney ), to pay directly to ( Provider ) AND/OR TO ANY
JEWISH FAMILY SERVICE NOTICE OF PRIVACY PRACTICES
 Jewish Family Service takes pride in treating our clients and each other with respect and dignity. Protecting your health information is very important to us. We want you to have a clear understanding
Jewish Family Service takes pride in treating our clients and each other with respect and dignity. Protecting your health information is very important to us. We want you to have a clear understanding
Student Board of Directors Application Packet
 Dear Student, Thank you for your interest in participating in the Student Board of Directors Program at the Federal Reserve Bank of Kansas City, Denver Branch. Please complete this application packet,
Dear Student, Thank you for your interest in participating in the Student Board of Directors Program at the Federal Reserve Bank of Kansas City, Denver Branch. Please complete this application packet,
Population Health Management Program Notice of Privacy Practices from Piedmont WellStar HealthPlans, Inc.
 Population Health Management Program Notice of Privacy Practices from Piedmont WellStar HealthPlans, Inc. Piedmont WellStar HealthPlans, Inc. (PWHP) provides population health management services to its
Population Health Management Program Notice of Privacy Practices from Piedmont WellStar HealthPlans, Inc. Piedmont WellStar HealthPlans, Inc. (PWHP) provides population health management services to its
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES The Pain Treatment Center, Inc. d/b/a Stone Road Surgery Center THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
NOTICE OF PRIVACY PRACTICES The Pain Treatment Center, Inc. d/b/a Stone Road Surgery Center THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
High School last attended: Month: Day: Year: Yes, I graduated No, I did not graduate. Program of study at WCC: Expected graduation date: 1. 2. 3.
 Financial Aid Office General Scholarship Application Instructions: Complete this application and return the completed application to the Financial Aid Office. An incomplete application will not be considered.
Financial Aid Office General Scholarship Application Instructions: Complete this application and return the completed application to the Financial Aid Office. An incomplete application will not be considered.
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY NATIONWIDE SPECIALTY INSURANCE CLAIM FORM
 NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY NATIONWIDE SPECIALTY INSURANCE CLAIM FORM THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY NATIONWIDE SPECIALTY INSURANCE CLAIM FORM THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM
The Health and Benefit Trust Fund of the International Union of Operating Engineers Local Union No. 94-94A-94B, AFL-CIO. Notice of Privacy Practices
 The Health and Benefit Trust Fund of the International Union of Operating Section 1: Purpose of This Notice Notice of Privacy Practices Effective as of September 23, 2013 THIS NOTICE DESCRIBES HOW MEDICAL
The Health and Benefit Trust Fund of the International Union of Operating Section 1: Purpose of This Notice Notice of Privacy Practices Effective as of September 23, 2013 THIS NOTICE DESCRIBES HOW MEDICAL
HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA): FACT SHEET FOR NEUROPSYCHOLOGISTS Division 40, American Psychological Association
: FACT SHEET FOR NEUROPSYCHOLOGISTS Division 40, American Psychological Association") HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA): FACT SHEET FOR NEUROPSYCHOLOGISTS Division 40, American Psychological Association DISCLAIMER This general information fact sheet is made available
HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA): FACT SHEET FOR NEUROPSYCHOLOGISTS Division 40, American Psychological Association DISCLAIMER This general information fact sheet is made available
Nichol A. Moses, Psy.D., NCSP
 PATIENT INFORMATION SHEET It is our hope to provide the highest quality of service. Below you will find a patient information sheet which provides our office with useful information that is helpful to
PATIENT INFORMATION SHEET It is our hope to provide the highest quality of service. Below you will find a patient information sheet which provides our office with useful information that is helpful to
Salt Lake Community College Employee Health Care Benefits Plan Notice of Privacy Practices
 THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. Date: June 1, 2014 Salt Lake Community College
THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. Date: June 1, 2014 Salt Lake Community College
This is your copy of our privacy notice so please take it home with you and read it carefully.
 Main 2219 E. Seventh Street South Charlotte 7000 Shannon Willow Rd Charlotte, NC 28226 Charlotte 2607 E. Seventh Street Suite 200 Monroe 1315 E. Sunset Drive Suite 201 Monroe, NC 28112 North Charlotte
Main 2219 E. Seventh Street South Charlotte 7000 Shannon Willow Rd Charlotte, NC 28226 Charlotte 2607 E. Seventh Street Suite 200 Monroe 1315 E. Sunset Drive Suite 201 Monroe, NC 28112 North Charlotte
Betsy Mencher, Ph.D. Licensed Clinical Psychologist 1350 Connecticut Avenue, NW Suite 602 Washington, DC 20036
 Betsy Mencher, Ph.D. Licensed Clinical Psychologist 1350 Connecticut Avenue, NW Suite 602 Washington, DC 20036 PSYCHOLOGIST-CLIENT SERVICES AGREEMENT Welcome to my practice. This document (the Agreement)
Betsy Mencher, Ph.D. Licensed Clinical Psychologist 1350 Connecticut Avenue, NW Suite 602 Washington, DC 20036 PSYCHOLOGIST-CLIENT SERVICES AGREEMENT Welcome to my practice. This document (the Agreement)
acknowledgment of health center privacy policy, privacy practices, and privacy procedures PATIENT PRIVACY
 LAST NAME FIRST NAME OF BIRTH 001 acknowledgment of health center privacy policy, privacy practices, and privacy procedures PATIENT PRIVACY! HOPE s PRIVACY ACKNOWLEDGMENT PAGE 1 OF 1 HOPE s Statement of
LAST NAME FIRST NAME OF BIRTH 001 acknowledgment of health center privacy policy, privacy practices, and privacy procedures PATIENT PRIVACY! HOPE s PRIVACY ACKNOWLEDGMENT PAGE 1 OF 1 HOPE s Statement of
HIPAA NOTICE OF PRIVACY PRACTICES
 HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW YOUR MEDICAL INFORMATION MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This HIPAA Notice
HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW YOUR MEDICAL INFORMATION MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This HIPAA Notice