Innovations in CBT for Treatment Resistant OCD and BDD. James M. Claiborn Ph.D. ABPP ACT Riverview Psychiatric Center Augusta Maine
|
|
|
- Marsha Johns
- 8 years ago
- Views:
Transcription
1 Innovations in CBT for Treatment Resistant OCD and BDD James M. Claiborn Ph.D. ABPP ACT Riverview Psychiatric Center Augusta Maine

2 Characteristics of Individuals with Treatment Resistant OCD and BDD Little or no response to standard treatment. Frequently described as having over-valued ideas or as delusional. Likely to refuse to engage in exposure based treatment. Their obsessions are generally seen as realistic and compulsions seen as reasonable efforts.

3 Over-Valued Ideas Generally seen as poor prognostic indicators Assumed to be more resistant to change Commonly seen in BDD and in OCD with poor insight or in forms of OCD seen as most treatment resistant such as hoarding

4 Definitions DSM defines an over-valued idea as An unreasonable and sustained belief that is maintained with less than delusional intensity The person is able to acknowledge the possibility that the belief may or may not be true The belief is not one that is ordinarily accepted by other members of the persons subculture Most sources use this as shorthand for poor insight and place it on a continuum with delusional certainty

5 Definitions DSM defines a delusion as a false belief based on incorrect inference about external reality that is firmly sustained despite what almost everyone else believes and despite what constitutes incontrovertible and obvious proof or evidence to the contrary. The difference between over-valued ideas and delusions is based on how firmly the belief is held

6 Delusions? Delusions are actually held with varying degrees of conviction which may fluctuate over time and are not fixed The definition from DSM does not accurately distinguish between delusions and over-valued ideas There is no qualitative distinction between beliefs we call delusions and other beliefs All differences are in degree

7 Quality vs Quantity The standard definitions and traditional thinking about delusions holds that there is a qualitative difference between the thinking of people who have delusions and those who don't This distinction does not stand up to closer examination

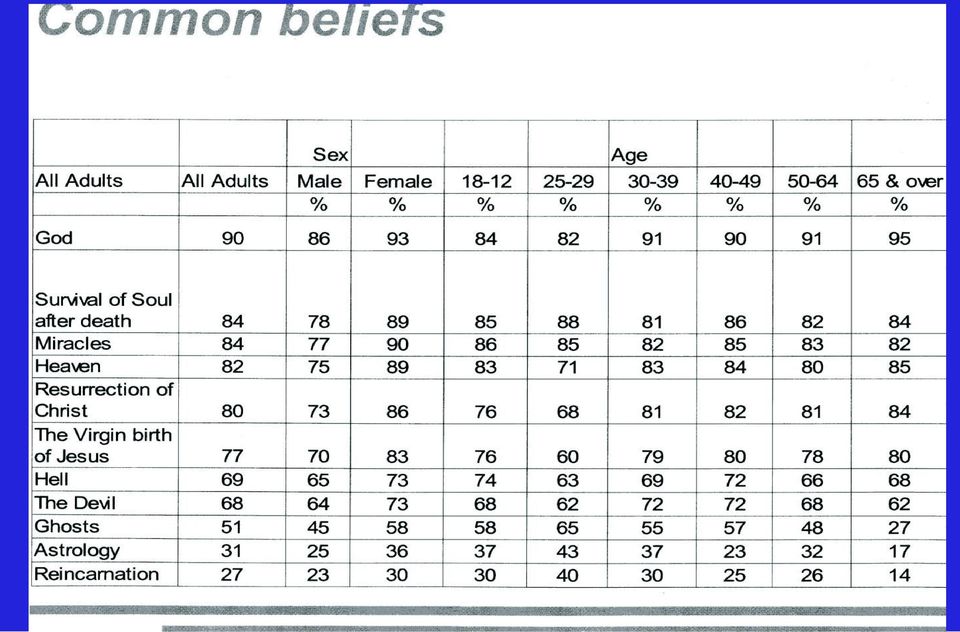
8 Normal Delusions? A survey of 60,000 British adults found 50% believed in thought transference 25% believed in ghosts 25% believed in reincarnation Interview using the Peters Delusional Inventory 272 healthy adults 20 psychotic inpatients 10% of the healthy population scored above the mean for the deluded patients

9 An Alternative Understanding The individual patient (and everyone else in the world) is attempting to make sense of their own experience. It is likely that they hear the voice and try to explain why they hear the voice. They may come up with an explanation that we think is strange but it makes sense to them.

10
11 Ideas of Reference Ideas of reference include the thought that others are talking about the individual and it is only a small step to the belief that they know what others are thinking about the them** Ideas of reference are typically described as a psychotic feature or a form of delusional belief They are extremely common in people with BDD

12 Schizotypy Schizotypal personality disorder is a predictor of poor treatment response (Jenike et al) This personality disorder or trait includes aberrant perceptions and beliefs Schizotypal patients may simply have what we would otherwise describe as delusions or overvalued ideas that impact compliance with treatment or interfere with belief change as a component of therapy**

13 Thought Action Fusion Thought action fusion can occur in moral or causal reasoning. Moral thought action fusion is the belief that a thought is the moral equivalent of an action If I think of doing something bad that is as bad as doing it Causal thought action fusion is the belief that thinking about possible events changes their probability If I think of something that can go wrong it is more likely to happen. Thought action fusion is seen as a key feature of OCD. How is it different from a delusion?

14 How Delusions Work Delusions are present in ¾ of people diagnosed with schizophrenia, ½ of people with BDD and an unknown percentage of people with OCD. They also appear in an estimated 5-10% of the general population. Individuals who develop such beliefs appear to jump to conclusions based on minimal evidence and ignore contradictory information.

15 Hallucinations Hallucinations are defined as a sensory experience that doesn't correspond to an external environmental event Hallucinations are not listed in the diagnostic criteria for OCD or BDD While there is no good data, a substantial number of people with BDD report hearing others commenting on their appearance. Is this a hallucinatory experience?

16 The Truth About Hallucinations Most people including most mental health professionals describe hallucinations as a sign of mental illness. Because of this belief and the typical reaction to talking about hallucinations, patients often deny they experience them. If hallucinations are acknowledged most mental health professionals believe discussion of them is contraindicated

17 Hallucinations in the General Population The incidence of psychotic symptoms in the general population is about 100 times greater than the incidence of psychotic disorders The experience of hallucinations at one point in time is not a good predictor of later hallucinations Hanssen et al 2005

18 You Heard What? In a survey of 375 college students 71% reported some brief, occasional experiences of voices while awake. In another study of 586 college students 30-40% reported hearing voices, and almost ½ reported it happened at least once a month Reports of hallucinations were not related to measures of psychopathology

19 Explanation of Hallucinations Functional brain imaging data shows speech areas of the brain are active when people are having auditory hallucinations. EMG data supports the conclusion that people are sub-vocalizing when they hear voices. The content is essentially the same as typical intrusive thoughts. Hallucinations may be explained as sub-vocalized intrusive thoughts which are misperceived as being from an external source.

20 Medical Model and Tradition The medical model and traditional way of understanding hallucinations and delusions include: That they are the result of brain dysfunction or disease That these experiences are qualitatively different from normal experience That it is futile or perhaps even harmful to engage in discussion of them That it is best to explain that they are the result of the patients illness

21 Effects of Confrontation To some extent the caution about discussing delusions is supported by the fact that confronting them is most likely to lead to strengthening conviction. Arguing with the patient that their beliefs are false or that what they experience is not real will not only not convince them it will probably be experienced as invalidating and damage the therapy relationship.
22 The European Model of Over- Valued Ideas Most American sources seem to use intensity of conviction as the defining variable. The European model includes the idea that over valued ideas are characterized by: preoccupation, being more ego syntonic, development is comprehensible, and associated with a high degree of affect??
23 Application of these Distinctions If we view the distinctions suggested in the European model and allow for the fact that delusions are not held with absolute conviction it may suggest that we can understand beliefs as falling on several continua and that this more complex model can lead to implications for interventions.
24 Where do Delusions Come From? Beliefs arise from a search for meaning. Delusional beliefs may arise from attempts to explain experiences that are anomalous and which are emotionally important. They arise as a result of an attempt to find meaning and are influenced by both environment and preexisting beliefs.
25 Personal Importance Principle Obsessions attach to concerns that are of central importance to the individual. For example the patient who holds strong religious beliefs is most bothered by intrusive thoughts that conflict with religious values. Similarly?? delusions attach to central concepts about beliefs about the self and the world.
26 Why do Delusions Persist? Obsessions seem to persist because people avoid situations which could produce disconfirming information and compulsions produce negative reinforcement which strengthens the belief in the obsession. In delusional beliefs the same mechanisms are in place. Compulsions and other safety behaviors prevent disconfirmation
27 Why Treatment Resistance Over valued ideas and delusions are more resistant to treatment in part because they tend to be held with greater conviction but in addition they may have a stronger affective component. This stronger affective component means that addressing them at all is likely to be perceived as threatening. Due to being more ego syntonic conflicting arguments are more likely to be experienced as personal attacks.
28 Hallucinations and Treatment Resistance In effect the problem with hallucinations is not the presence but the reaction to them. In BDD the reported hallucinations are often confirming of the beliefs about appearance and others reaction to it. If the mental health professional is seen as not believing in the experience it is another event that can be interpreted as attacking or demeaning to the patient.
29 Discussion of Beliefs in Therapy Since most people with OCD will admit their beliefs or fears are exaggerated or irrational they are more likely to be willing to discuss or question them or consider a therapy task that would test them. More centrally held beliefs are more likely to be OFF LIMITS and an attempt to question or test them is likely to be threatening to the individual.
30 What does Cognitive Therapy Offer? The traditional view is that delusional patients need to be treated with medication. In fact approximately 60% of patients will still have psychotic symptoms when fully compliant with medication. A body of evidence has been accumulated that cognitive behavioral therapy produces a clinically important benefit in otherwise drug resistant psychotic patients.
31 Engagement in Therapy When the patient is able to question the beliefs or meaning of experiences it is easier to engage in a collaborative therapy approach. Both parties can engage in an effort to reduce dysfunction and distress beginning with a shared conceptualization of the problem. In working with a delusional patient this engagement is impeded.
32 Enhancing Engagement Early establishment of goals Sharing of the cognitive model Therapist presentation: Knowledgeable, Trustworthy, Likable, Confident Expectations for therapy Therapists work hard and patients get better vs. Patients work hard and therapists get better Patience
33 Can You Tell Me About Them? If we inquire in an empathetic way the patient may be able to describe the experience with voices. This includes many characteristics Number, Identity, Social position, Gender, Volume, Power, Knowledge, Occurrence, Content, Beliefs about origin and mechanism
34 An Alternative Understanding The individual patient (and everyone else in the world) is attempting to make sense of their own experience. It is likely that they hear the voice and try to explain why they hear the voice. They may come up with an explanation that we think is strange but it makes sense to them.
35 What is it Like If given a chance and an accepting response many people with voices will describe their experience. We tend to shut this down when we respond to the presence as a symptom of an illness and an indication that more medication is all that is needed to take it away. Consider how you would feel if you reported an experience and others said that is just a sign you are sick.??
36 The Message to Give Patients You are not crazy, the problems you have are understandable. Either your concerns are real or you believe them to be real. (Both explain how you feel) How you interpret events affects how you feel. It is important to evaluate beliefs by testing them and this involves changing your behavior. What you pay attention to and how you pay attention can affect how you feel and what you believe.
37 Normalization Engaging the patient in the collaborative production of an explanatory normalizing rationale /model of symptom emergence is the first crucial step in developing a relationship with the patient (Kingdon and Turkington)
38 How Can We Engage the Delusional Patient? Empathy warmth and genuineness are central to building any therapeutic relationship but are especially critical with individuals with psychotic symptoms. Word perfect accuracy contributes to avoiding invalidating experiences. Instead of invalidating or denying delusional beliefs engage in evaluating them collaboratively by gathering evidence and developing alternative explanations.
39 More on Engagement Be willing to agree to disagree. When the patient is distressed it may be useful to engage in tactical withdrawal. Allow the illogical or psychotic logic to flow over you. Eventually it becomes comprehensible Teach a cognitive model, emotional responses are the result of interpretation of events, not the events themselves. Events can include intrusive thoughts, images, obsessions or hallucinations.
40 Examining Antecedents It is important to look at events leading to development of symptoms in the context of how they could be interpreted to support the conclusions embedded in delusions or lead to experiences such as hallucinations in context so they may lead to development of alternative explanations.
41 Anna's Belief that She is Ugly When asked about evidence that she was ugly a BDD patient reported that her father had told her she was when she was a child. This was seen as irrefutable evidence of a fact. A cognitive restructured alternative was that this was evidence only that her father said this not that it was a fact. This alternative clicked and led to a dramatic shift in the patients self image.
42 What Can We Do? If we begin by simply listening to the patient and trying to understand their experience we can begin to build a helping relationship. This alone may have considerable impact on their mental status. We can work toward an open dialogue about the experience of the voice and how to deal with it.
43 What is the Real Problem with Psychotic Symptoms The actual beliefs and explanations of experience are not a problem in and of themselves. The problem is the distress associated with the experience or belief or the interference with function that follows from the beliefs. With this in mind the goal of therapy is not necessarily to change the belief but rather to change the effects of the belief, reduce distress and interference.
44 What are safety behaviors and why are they a problem? Safety behaviors are things someone does to get relief where they believe that if they did not do them some disastrous consequence would follow. A classic example is the panic patient who takes a Xanax and believes it saves his life. The problem is that such behaviors actually reinforce the belief in the danger of the symptom and the magical belief that the coping response was all important in preventing a disaster. This perpetuates the disorder and distress associated with the symptom
45 Joining in the patients conceptualization In order to work with patients who have delusional beliefs we need to first join with them in conceptualization. This includes accepting that they are reporting their experience as they understand it and their beliefs represent their efforts to make sense of those experiences.
46 Working with Delusions Begin with an individual formulation that accounts for the patients beliefs and associated distress. What evidence is the person using as the basis for their beliefs? How do these ideas build on the persons ideas about self, others and the world? How do these thoughts make sense of previous life experiences?
47 Problematic Beliefs Supported by Mental Health Professionals There are some beliefs about symptoms which may contribute to treatment resistance and which are supported by popular conceptualizations or other mental health professionals who have interacted with the patient. Depression is anger turned inward and expressed only by a compulsion. If not expressed the anger would lead to aggressive behavior
48 Continuing Work with Delusions Is the individual reacting to puzzling, confusing or otherwise ambiguous experiences? How is the person reasoning about experiences? Recognize known biases Bias for confirmatory information Tendency to jump to conclusions All or nothing thinking Feed back this formulation to the patient In effect the reasoning of the client is unpacked and treated as understandable in a normalizing and empathetic manner.
49 Therapy Process Develop alternative interpretations of anomalous or other distressing experiences. Review evidence supporting interpretation and alternative explanations of experience Develop the ability to become an observer and evaluate thoughts rather than simply accepting them.
50 Working from the Outside In The effect of confrontation of delusions is typically to lead to greater entrenchment. Therapeutic efforts may be more acceptable if you begin with less central beliefs. Using the approach of working with more peripheral beliefs first and working with toward more central ones is less likely to be met with resistance and may lead to acceptance of the process of developing alternatives.
51 Peripheral Questions In discussing any delusional or overvalued idea it is best to explore the belief beginning with more peripheral elements and by examining details and possible inconsistencies. With the use of Socratic questioning and with the understanding that beliefs are rarely held with absolute conviction an approach that is both accepting and mildly skeptical is likely to lead to reevaluation of the belief.
52 No Safety Behavior Please! There are a number of techniques that have been found helpful in dealing with hallucinations but they must be used in context. Both Therapist and patients need to understand that the use of these methods is a way to be more comfortable as the voices can be unpleasant or annoying but that it is not necessary to get rid of the voices.
53 Behavioral Experiments Often confused with exposure exercises. Determine a specific thought or belief to be tested. Determine what information is needed to conduct this test. Set up an experiment to gather this data. Establish in advance what a particular outcome will mean.
54 Outcome of Behavioral Experiment How does the outcome relate to the automatic thought? How much do you believe the thought now? To what extent were predictions confirmed or disconfirmed? What is a realistic view given the results of the experiment? What next?
55 Use of Classic Cognitive Interventions Becoming aware of automatic thoughts Which thoughts to address Identifying when they are occurring and learning to catch them Worst case scenario Recounting events Affect shifts Use of a DTR
56 Critical Role of Therapist Acceptance In any effort to use cognitive restructuring or other cognitive approaches to belief change the attitude of the therapist plays a critical role. Because the beliefs we describe as over valued or delusional are typically held with strong affect any indication of a non accepting attitude by the therapist is likely to be damaging to the already fragile working alliance.
57 Work on Values If overvalued ideas are more of a problem because of firmly held values than because of their content then work focused on those values has the potential to lead to important change. Example A person who values perfection may be treatment resistant since the goal of treatment seems to be to accept imperfection. The effect and desirability of seeking perfection can be examined and the reconsidered.
58 The Role of Mindfulness Mindfulness as a special kind of attention without judgment or evaluation Since it is not the intrusive thought but the evaluation or judgment that is the source of distress a mindful response to the intrusions leads to reduction of distress Mindfulness can be viewed as a skill which can be developed with practice. This may begin with practice of mindful attention to non distressing stimuli
59 Wells and Attention Training Based in Wells SREF model Successfully used in case studies with panic and hallucinations Attention Training Technique Application to excess attention to detail in OCD or BDD
60 Schema Focused Therapy Based in the work of J. Young Early maladaptive schema serve as prototypes for automatic thoughts Delusions may emerge as a result of invalidation of personal schema and may serve to protect against loss of self-esteem or other threat Schema are responded to in one of 3 fundamental ways. Overcompensation, Confirmation/ Surrender, or Avoidance
61 Steps in Schema Work Rationale: Use of prejudice model Identification of schema using Socratic questioning and downward arrow Use of historical testing Use of responsibility pie Use of continua to evaluate schema Review of advantages/disadvantages of a schema or belief Development and testing of alternative schema
62 Motivational Interviewing First developed for work with substance abuse clients where treatment resistance is often extreme Therapists are taught to roll with the resistance and enhance ambivalence Adopted for treatment of hoarding (a particularly difficult form of OCD) by Frost and Steketee
CBT Treatment. Obsessive Compulsive Disorder
 CBT Treatment Obsessive Compulsive Disorder 1 OCD DEFINITION AND DIAGNOSIS NORMAL WORRIES & COMPULSIONS DYSFUNCTIONAL/ABNORMAL OBSESSIONS DSM IV DIAGNOSIS 2 OCD DIAGNOSIS DSM IV & ICD 10 A significant
CBT Treatment Obsessive Compulsive Disorder 1 OCD DEFINITION AND DIAGNOSIS NORMAL WORRIES & COMPULSIONS DYSFUNCTIONAL/ABNORMAL OBSESSIONS DSM IV DIAGNOSIS 2 OCD DIAGNOSIS DSM IV & ICD 10 A significant
Issues in OCD Resistance: Co-Morbidity and Merged Vs Unmerged OCD Page 1 Jonathan Grayson, Ph.D.
 Issues in OCD Resistance: Co-Morbidity and Merged Vs Unmerged OCD Page 1 Jonathan Grayson, Ph.D. I. Introduction A. Treatment resistance comes in many forms, which all of us have been addressing over the
Issues in OCD Resistance: Co-Morbidity and Merged Vs Unmerged OCD Page 1 Jonathan Grayson, Ph.D. I. Introduction A. Treatment resistance comes in many forms, which all of us have been addressing over the
The Priory Group. What is obsessive-compulsive disorder?
 The Priory Group What is obsessive-compulsive disorder? by Dr David Veale Dr Veale is a Consultant Psychiatrist at the Priory Hospital North London and the coauthor of Overcoming Obsessive Compulsive Disorder
The Priory Group What is obsessive-compulsive disorder? by Dr David Veale Dr Veale is a Consultant Psychiatrist at the Priory Hospital North London and the coauthor of Overcoming Obsessive Compulsive Disorder
Psychotic Disorders. 1995-2013, The Patient Education Institute, Inc. www.x-plain.com mhff0101 Last reviewed: 01/10/2013 1
 Psychotic Disorders Introduction Psychotic disorders are severe mental disorders that cause abnormal thinking and perceptions. These disorders cause people to lose touch with reality. As a result, people
Psychotic Disorders Introduction Psychotic disorders are severe mental disorders that cause abnormal thinking and perceptions. These disorders cause people to lose touch with reality. As a result, people
How To Treat An Addiction With Cognitive Behavioral Therapy
 Cognitive Behavioral Therapy Part 1 An Overview Cognitive Behavioral Therapy (CBT) is a general classification of psycho therapy, based on social learning theory, which emphasizes how our thinking interacts
Cognitive Behavioral Therapy Part 1 An Overview Cognitive Behavioral Therapy (CBT) is a general classification of psycho therapy, based on social learning theory, which emphasizes how our thinking interacts
Delusions are false beliefs that are not part of their real-life. The person keeps on believing his delusions even when other people prove that the be
 Schizophrenia Schizophrenia is a chronic, severe, and disabling brain disorder which affects the whole person s day-to-day actions, for example, thinking, feeling and behavior. It usually starts between
Schizophrenia Schizophrenia is a chronic, severe, and disabling brain disorder which affects the whole person s day-to-day actions, for example, thinking, feeling and behavior. It usually starts between
Taming the OCD Monster Tips & Tricks for Living Sanely with OCD
 Taming the OCD Monster Tips & Tricks for Living Sanely with OCD January 13, 2016 FAA Family Resource Meeting Presented by: Gwennyth Palafox, Ph.D. What is Obsessive Compulsive Disorder (OCD)? Is an anxiety
Taming the OCD Monster Tips & Tricks for Living Sanely with OCD January 13, 2016 FAA Family Resource Meeting Presented by: Gwennyth Palafox, Ph.D. What is Obsessive Compulsive Disorder (OCD)? Is an anxiety
Borderline Personality Disorder and Treatment Options
 Borderline Personality Disorder and Treatment Options MELISSA BUDZINSKI, LCSW VICE PRESIDENT, CLINICAL SERVICES 2014 Horizon Mental Health Management, LLC. All rights reserved. Objectives Define Borderline
Borderline Personality Disorder and Treatment Options MELISSA BUDZINSKI, LCSW VICE PRESIDENT, CLINICAL SERVICES 2014 Horizon Mental Health Management, LLC. All rights reserved. Objectives Define Borderline
Personality Difficulties
 Personality Difficulties The essential features of a personality disorder are impairments in personality (self and interpersonal) functioning and the presence of pathological personality traits. There
Personality Difficulties The essential features of a personality disorder are impairments in personality (self and interpersonal) functioning and the presence of pathological personality traits. There
USVH Disease of the Week #1: Posttraumatic Stress Disorder (PTSD)
") USVH Disease of the Week #1: Posttraumatic Stress Disorder (PTSD) Effects of Traumatic Experiences A National Center for PTSD Fact Sheet By: Eve B. Carlson, Ph.D. and Josef Ruzek, Ph.D. When people find
USVH Disease of the Week #1: Posttraumatic Stress Disorder (PTSD) Effects of Traumatic Experiences A National Center for PTSD Fact Sheet By: Eve B. Carlson, Ph.D. and Josef Ruzek, Ph.D. When people find
Dual Diagnosis Dr. Ian Paylor Senior Lecturer in Applied Social Science Lancaster University
 Dual Diagnosis Dr. Ian Paylor Senior Lecturer in Applied Social Science Lancaster University Dual diagnosis has become a critical issue for both drug and mental health services. The complexity of problems
Dual Diagnosis Dr. Ian Paylor Senior Lecturer in Applied Social Science Lancaster University Dual diagnosis has become a critical issue for both drug and mental health services. The complexity of problems
Obsessive Compulsive Disorder (OCD)
") Obsessive Compulsive Disorder (OCD) Introduction Obsessive compulsive disorder, or OCD, is a type of anxiety disorder. OCD causes repeated upsetting thoughts called obsessions. To try and get rid of these
Obsessive Compulsive Disorder (OCD) Introduction Obsessive compulsive disorder, or OCD, is a type of anxiety disorder. OCD causes repeated upsetting thoughts called obsessions. To try and get rid of these
PTSD Ehlers and Clark model
 Problem-specific competences describe the knowledge and skills needed when applying CBT principles to specific conditions. They are not a stand-alone description of competences, and should be read as part
Problem-specific competences describe the knowledge and skills needed when applying CBT principles to specific conditions. They are not a stand-alone description of competences, and should be read as part
Schizoaffective Disorder
 FACT SHEET 10 What Is? Schizoaffective disorder is a psychiatric disorder that affects about 0.5 percent of the population (one person in every two hundred). Similar to schizophrenia, this disorder is
FACT SHEET 10 What Is? Schizoaffective disorder is a psychiatric disorder that affects about 0.5 percent of the population (one person in every two hundred). Similar to schizophrenia, this disorder is
Unit 4: Personality, Psychological Disorders, and Treatment
 Unit 4: Personality, Psychological Disorders, and Treatment Learning Objective 1 (pp. 131-132): Personality, The Trait Approach 1. How do psychologists generally view personality? 2. What is the focus
Unit 4: Personality, Psychological Disorders, and Treatment Learning Objective 1 (pp. 131-132): Personality, The Trait Approach 1. How do psychologists generally view personality? 2. What is the focus
Cognitive Behavioral Treatment Interventions for Compulsive Hoarding
 Cognitive Behavioral Treatment Interventions for Compulsive Hoarding Thinking Outside our Box(es): A Housing, Service, Clinical and Enforcement Team Approach to Hoarding December, 2007 Christiana Bratiotis,
Cognitive Behavioral Treatment Interventions for Compulsive Hoarding Thinking Outside our Box(es): A Housing, Service, Clinical and Enforcement Team Approach to Hoarding December, 2007 Christiana Bratiotis,
Obsessive Compulsive Disorder What you need to know to help your patients
 Obsessive Compulsive Disorder What you need to know to help your patients By Renae M. Reinardy, PsyD, LP, and Jon E. Grant, MD Obsessive compulsive disorder (OCD) is a condition that affects millions of
Obsessive Compulsive Disorder What you need to know to help your patients By Renae M. Reinardy, PsyD, LP, and Jon E. Grant, MD Obsessive compulsive disorder (OCD) is a condition that affects millions of
These core elements are included in three increasingly detailed levels of definition:
 A Definition of Motivational Interviewing The definition of Motivational Interviewing (MI) has evolved and been refined since the original publications on its utility as an approach to behavior change.
A Definition of Motivational Interviewing The definition of Motivational Interviewing (MI) has evolved and been refined since the original publications on its utility as an approach to behavior change.
Making sense of cognitive behaviour therapy (CBT)
") Making sense of cognitive behaviour therapy (CBT) Making sense of cognitive behaviour therapy What is cognitive behaviour therapy? 4 How does negative thinking start? 6 What type of problems can CBT help
Making sense of cognitive behaviour therapy (CBT) Making sense of cognitive behaviour therapy What is cognitive behaviour therapy? 4 How does negative thinking start? 6 What type of problems can CBT help
Licensing Exam Practice Questions
 Licensing Exam Practice Questions Everyone has a different study style but the best way to study for this exam is to test your self on the art of the multiple choice question. The exam will have 170 multiple
Licensing Exam Practice Questions Everyone has a different study style but the best way to study for this exam is to test your self on the art of the multiple choice question. The exam will have 170 multiple
Anxiety and Education Impact, Recognition & Management Strategies
 Anxiety and Education Impact, Recognition & Management Strategies Dr Amanda Gamble Centre for Emotional Health (formerly MUARU) Macquarie University, Sydney. WHY SHOULD I BE CONCERNED? 1 Prevalence of
Anxiety and Education Impact, Recognition & Management Strategies Dr Amanda Gamble Centre for Emotional Health (formerly MUARU) Macquarie University, Sydney. WHY SHOULD I BE CONCERNED? 1 Prevalence of
Mental Health Role Plays
 Mental Health Role Plays Goals: To discuss various mental health issues and mental illnesses. To discuss stigma, support and treatment options surrounding mental health issues and mental illnesses. Requirements:
Mental Health Role Plays Goals: To discuss various mental health issues and mental illnesses. To discuss stigma, support and treatment options surrounding mental health issues and mental illnesses. Requirements:
Mental Health Needs Assessment Personality Disorder Prevalence and models of care
 Mental Health Needs Assessment Personality Disorder Prevalence and models of care Introduction and definitions Personality disorders are a complex group of conditions identified through how an individual
Mental Health Needs Assessment Personality Disorder Prevalence and models of care Introduction and definitions Personality disorders are a complex group of conditions identified through how an individual
Treatments for OCD: Cognitive- Behavioural Therapy
 Source: CAMH (Centre for Addiction and Mental Health) www.camh.net Treatments for OCD: Cognitive- Behavioural Therapy Obsessive-Compulsuve Disorder: An Information Guide On this page: Cognitive-Behavioural
Source: CAMH (Centre for Addiction and Mental Health) www.camh.net Treatments for OCD: Cognitive- Behavioural Therapy Obsessive-Compulsuve Disorder: An Information Guide On this page: Cognitive-Behavioural
Mental Health Ombudsman Training Manual. Advocacy and the Adult Home Resident. Module V: Substance Abuse and Common Mental Health Disorders
 Mental Health Ombudsman Training Manual Advocacy and the Adult Home Resident Module V: Substance Abuse and Common Mental Health Disorders S WEHRY 2004 Goals Increase personal comfort and confidence Increase
Mental Health Ombudsman Training Manual Advocacy and the Adult Home Resident Module V: Substance Abuse and Common Mental Health Disorders S WEHRY 2004 Goals Increase personal comfort and confidence Increase
Suicidal. Caring For The Person Who Is. Why might a person be suicidal?
 Caring For The Person Who Is Suicidal For further information see also the following MIND Essentials resource Conducting a suicide risk assessment. Suicidal thoughts and behaviours are not unique to mental
Caring For The Person Who Is Suicidal For further information see also the following MIND Essentials resource Conducting a suicide risk assessment. Suicidal thoughts and behaviours are not unique to mental
Ninon Yale Clinical Nurse Specialist Trauma Program McGill University Health Centre Sept. 27, 2012
 Ninon Yale Clinical Nurse Specialist Trauma Program McGill University Health Centre Sept. 27, 2012 Suicide in Québec Québec is the Canadian province with the highest suicide rate Affects all age groups
Ninon Yale Clinical Nurse Specialist Trauma Program McGill University Health Centre Sept. 27, 2012 Suicide in Québec Québec is the Canadian province with the highest suicide rate Affects all age groups
What is a personality disorder?
 What is a personality disorder? What is a personality disorder? Everyone has personality traits that characterise them. These are the usual ways that a person thinks and behaves, which make each of us
What is a personality disorder? What is a personality disorder? Everyone has personality traits that characterise them. These are the usual ways that a person thinks and behaves, which make each of us
Abnormal Psychology PSY-350-TE
 Abnormal Psychology PSY-350-TE This TECEP tests the material usually taught in a one-semester course in abnormal psychology. It focuses on the causes of abnormality, the different forms of abnormal behavior,
Abnormal Psychology PSY-350-TE This TECEP tests the material usually taught in a one-semester course in abnormal psychology. It focuses on the causes of abnormality, the different forms of abnormal behavior,
Verbal Communication II
 Verbal Communication II Course Health Science Unit II Communication Essential Question How does the communication process affect health care delivery? TEKS 130.204 (c) 2A, 2B, 3B, 3C Prior Student Learning
Verbal Communication II Course Health Science Unit II Communication Essential Question How does the communication process affect health care delivery? TEKS 130.204 (c) 2A, 2B, 3B, 3C Prior Student Learning
Symptoms of mania can include: 3
 Bipolar Disorder This factsheet gives information on bipolar disorder. It explains the symptoms of bipolar disorder, treatments and ways to manage symptoms. It also covers what treatment the National Institute
Bipolar Disorder This factsheet gives information on bipolar disorder. It explains the symptoms of bipolar disorder, treatments and ways to manage symptoms. It also covers what treatment the National Institute
COGNITIVE BEHAVIORAL THERAPY Arron Beck "Cog B" Evidence Based Therapy (CBT) The Focus on Faulty Thinking patterns Automatic Thoughts
 The Focus on Faulty Thinking patterns Automatic Thoughts") COGNITIVE BEHAVIORAL THERAPY Arron Beck "Cog B" Evidence Based Therapy (CBT) The Focus on Faulty Thinking patterns Automatic Thoughts People respond to situations based on how these situations are consciously
COGNITIVE BEHAVIORAL THERAPY Arron Beck "Cog B" Evidence Based Therapy (CBT) The Focus on Faulty Thinking patterns Automatic Thoughts People respond to situations based on how these situations are consciously
CROSS EXAMINATION OF AN EXPERT WITNESS IN A CHILD SEXUAL ABUSE CASE. Mark Montgomery
 CROSS EXAMINATION OF AN EXPERT WITNESS IN A CHILD SEXUAL ABUSE CASE Mark Montgomery Post Office Box 161 Durham, NC 27702 (919) 680-6249 mark.montgomery@mindspring.com Opinion Testimony by a Pediatrician/Nurse/Counselor/Social
CROSS EXAMINATION OF AN EXPERT WITNESS IN A CHILD SEXUAL ABUSE CASE Mark Montgomery Post Office Box 161 Durham, NC 27702 (919) 680-6249 mark.montgomery@mindspring.com Opinion Testimony by a Pediatrician/Nurse/Counselor/Social
Developing a Therapeutic Relationship with Clients with Personality Disorders. The Therapeutic Relationship. The Therapeutic Relationship 7/31/15&
 Developing a Therapeutic Relationship with Clients with Personality Disorders Jim Seckman, MAC, CACII, CCS The Therapeutic Relationship The therapeutic relationship, also called the therapeutic alliance,
Developing a Therapeutic Relationship with Clients with Personality Disorders Jim Seckman, MAC, CACII, CCS The Therapeutic Relationship The therapeutic relationship, also called the therapeutic alliance,
PhD. IN (Psychological and Educational Counseling)
") PhD. IN (Psychological and Educational Counseling) I. GENERAL RULES CONDITIONS: Plan Number 2012 1. This plan conforms to the regulations of the general frame of the programs of graduate studies. 2. Areas
PhD. IN (Psychological and Educational Counseling) I. GENERAL RULES CONDITIONS: Plan Number 2012 1. This plan conforms to the regulations of the general frame of the programs of graduate studies. 2. Areas
Case Formulation in Cognitive-Behavioral Therapy. What is Case Formulation? Rationale 12/2/2009
 Case Formulation in Cognitive-Behavioral Therapy What is Case Formulation? A set of hypotheses regarding what variables serve as causes, triggers, or maintaining factors for a person s problems Description
Case Formulation in Cognitive-Behavioral Therapy What is Case Formulation? A set of hypotheses regarding what variables serve as causes, triggers, or maintaining factors for a person s problems Description
Get Help Now. Call us 1-877-855-3470
 Get Help Now. Call us 1-877-855-3470 1 The Purpose of an Intervention The principle behind an intervention is that those with an addiction may never choose to seek treatment on their own accord. The goal
Get Help Now. Call us 1-877-855-3470 1 The Purpose of an Intervention The principle behind an intervention is that those with an addiction may never choose to seek treatment on their own accord. The goal
Brief Strategic Family Therapy for Adolescent Drug Abuse
 Brief Strategic Family Therapy for Adolescent Drug Abuse Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Chapter One: Brief Strategic Family Therapy-An
Brief Strategic Family Therapy for Adolescent Drug Abuse Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Chapter One: Brief Strategic Family Therapy-An
When a Parent Has Mental Illness Helping Children Cope
 When a Parent Has Mental Illness Helping Children Cope World Fellowship for Schizophrenia and Allied Disorders 124 Merton Street, Suite 507 Toronto, Ontario, M4S 2Z2, Canada Email: info@world-schizophrenia.org
When a Parent Has Mental Illness Helping Children Cope World Fellowship for Schizophrenia and Allied Disorders 124 Merton Street, Suite 507 Toronto, Ontario, M4S 2Z2, Canada Email: info@world-schizophrenia.org
The Meaning of Mental Disorder and Impairment from a Young Person s Perspective. Professor Peter Hill London
 The Meaning of Mental Disorder and Impairment from a Young Person s Perspective Professor Peter Hill London Professor Peter Hill: Disclosures Advisory Lecturer Medice x x Flynn x x Janssen-Cilag x x Lilly
The Meaning of Mental Disorder and Impairment from a Young Person s Perspective Professor Peter Hill London Professor Peter Hill: Disclosures Advisory Lecturer Medice x x Flynn x x Janssen-Cilag x x Lilly
How To Treat A Mental Illness At Riveredge Hospital
 ABOUT US n Riveredge Hospital maintains the treatment philosophy of Trauma Informed Care. n Our commitment to providing the highest quality of care includes offering Animal Assisted Therapy, and Expressive
ABOUT US n Riveredge Hospital maintains the treatment philosophy of Trauma Informed Care. n Our commitment to providing the highest quality of care includes offering Animal Assisted Therapy, and Expressive
OBSESSIVE-COMPULSIVE AND RELATED DISORDERS
 OBSESSIVE-COMPULSIVE AND RELATED DISORDERS According to the American Psychiatric Association (APA), the publisher of the DSM-5, the major change for obsessivecompulsive disorder is the fact that it and
OBSESSIVE-COMPULSIVE AND RELATED DISORDERS According to the American Psychiatric Association (APA), the publisher of the DSM-5, the major change for obsessivecompulsive disorder is the fact that it and
CLASS OBJECTIVE: What is Obsessive-Compulsive Disorder? What is OCD?
 CLASS OBJECTIVE: What is Obsessive-Compulsive Disorder? Chapter 4-Anxiety Disorders What is OCD? Obsessive-compulsive disorder is an anxiety disorder that involves unwanted, What Did you see? The obsessions
CLASS OBJECTIVE: What is Obsessive-Compulsive Disorder? Chapter 4-Anxiety Disorders What is OCD? Obsessive-compulsive disorder is an anxiety disorder that involves unwanted, What Did you see? The obsessions
Reality in the Eyes of Descartes and Berkeley. By: Nada Shokry 5/21/2013 AUC - Philosophy
 Reality in the Eyes of Descartes and Berkeley By: Nada Shokry 5/21/2013 AUC - Philosophy Shokry, 2 One person's craziness is another person's reality. Tim Burton This quote best describes what one finds
Reality in the Eyes of Descartes and Berkeley By: Nada Shokry 5/21/2013 AUC - Philosophy Shokry, 2 One person's craziness is another person's reality. Tim Burton This quote best describes what one finds
Cognitive triad: negative view of future, world, and self. Cognitive distortions-faulty information processing Core irrational beliefs which create a
 Cognitive triad: negative view of future, world, and self. Cognitive distortions-faulty information processing Core irrational beliefs which create a psychological vulnerability to depression. Typically
Cognitive triad: negative view of future, world, and self. Cognitive distortions-faulty information processing Core irrational beliefs which create a psychological vulnerability to depression. Typically
Healing the Invisible Wound. Recovery and Rehabilitation from a Post Traumatic. Stress Injury. By Dr. Amy Menna
 Healing the Invisible Wound Recovery and Rehabilitation from a Post Traumatic Stress Injury By Dr. Amy Menna Post Traumatic Stress Disorder can affect anyone. It is a term used to describe a reaction to
Healing the Invisible Wound Recovery and Rehabilitation from a Post Traumatic Stress Injury By Dr. Amy Menna Post Traumatic Stress Disorder can affect anyone. It is a term used to describe a reaction to
Conceptual Models of Substance Use
 Conceptual Models of Substance Use Different causal factors emphasized Different interventions based on conceptual models 1 Developing a Conceptual Model What is the nature of the disorder? Why causes
Conceptual Models of Substance Use Different causal factors emphasized Different interventions based on conceptual models 1 Developing a Conceptual Model What is the nature of the disorder? Why causes
Treatment of Chronic Pain: Our Approach
 Treatment of Chronic Pain: Our Approach Today s webinar was coordinated by the National Association of Community Health Centers, a partner with the SAMHSA-HRSA Center for Integrated Health Solutions SAMHSA
Treatment of Chronic Pain: Our Approach Today s webinar was coordinated by the National Association of Community Health Centers, a partner with the SAMHSA-HRSA Center for Integrated Health Solutions SAMHSA
Mental Health Awareness. Haley Berry and Nic Roberts Nottinghamshire Mind Network
 Mental Health Awareness 2015 Haley Berry and Nic Roberts Nottinghamshire Mind Network The aim of this training:! to provide you with a basic understanding of mental health and mental illness. What do you
Mental Health Awareness 2015 Haley Berry and Nic Roberts Nottinghamshire Mind Network The aim of this training:! to provide you with a basic understanding of mental health and mental illness. What do you
Specific Phobias. Anxiety Disorders Association of America
 Specific Phobias Everyone thinks that once I ve driven on the highway, I ve conquered it. They just don t understand... I don t understand. It s a day-in and day-out struggle. What is a phobia? We all
Specific Phobias Everyone thinks that once I ve driven on the highway, I ve conquered it. They just don t understand... I don t understand. It s a day-in and day-out struggle. What is a phobia? We all
[KQ 804] FEBRUARY 2007 Sub. Code: 9105
![[KQ 804] FEBRUARY 2007 Sub. Code: 9105](/thumbs/26/8053833.jpg "[KQ 804] FEBRUARY 2007 Sub. Code: 9105") [KQ 804] FEBRUARY 2007 Sub. Code: 9105 (Revised Regulations) Theory : Two hours and forty minutes Q.P. Code: 419105 Maximum : 100 marks Theory : 80 marks M.C.Q. : Twenty minutes M.C.Q. : 20 marks 1. A
[KQ 804] FEBRUARY 2007 Sub. Code: 9105 (Revised Regulations) Theory : Two hours and forty minutes Q.P. Code: 419105 Maximum : 100 marks Theory : 80 marks M.C.Q. : Twenty minutes M.C.Q. : 20 marks 1. A
Chapter 13 & 14 Quiz. Name: Date:
 Name: Date: Chapter 13 & 14 Quiz 1. Regarding the difference between normal and abnormal behavior, which of the following statements is TRUE? A) Abnormal behavior is unusual, whereas normal behavior is
Name: Date: Chapter 13 & 14 Quiz 1. Regarding the difference between normal and abnormal behavior, which of the following statements is TRUE? A) Abnormal behavior is unusual, whereas normal behavior is
Children s Community Health Plan INTENSIVE IN-HOME MENTAL HEALTH / SUBSTANCE ABUSE SERVICES ASSESSMENT AND RECOVERY / TREATMENT PLAN ATTACHMENT
 Children s Community Health Plan INTENSIVE IN-HOME MENTAL HEALTH / SUBSTANCE ABUSE SERVICES ASSESSMENT AND RECOVERY / TREATMENT PLAN ATTACHMENT Please fax with CCHP prior authorization form to 608-252-0853
Children s Community Health Plan INTENSIVE IN-HOME MENTAL HEALTH / SUBSTANCE ABUSE SERVICES ASSESSMENT AND RECOVERY / TREATMENT PLAN ATTACHMENT Please fax with CCHP prior authorization form to 608-252-0853
Glossary Of Terms Related To The Psychological Evaluation Pain
 Glossary Of Terms Related To The Psychological Evaluation Pain Excerpted From The BHI 2 Manual By Daniel Bruns and John Mark Disorbio 2003 by Pearson Assessments. All rights reserved. Addiction: A chronic
Glossary Of Terms Related To The Psychological Evaluation Pain Excerpted From The BHI 2 Manual By Daniel Bruns and John Mark Disorbio 2003 by Pearson Assessments. All rights reserved. Addiction: A chronic
Parents recording social workers - A guidance note for parents and professionals
 Parents recording social workers - A guidance note for parents and professionals The Transparency Project December 2015 www.transparencyproject.org.uk info@transparencyproject.org.uk (Charity Registration
Parents recording social workers - A guidance note for parents and professionals The Transparency Project December 2015 www.transparencyproject.org.uk info@transparencyproject.org.uk (Charity Registration
Objectives Participants will be able to: Conflict of Interest Disclosure. Author s Conflicts of Interest: E. Bernhofer, No Conflict of Interest
 September 19, 2015 ASPMN 25th National Conference Esther I. Bernhofer, PhD, RN-BC Senior Nurse Researcher Pain Education Specialist Office of Nursing Research and Innovation Cleveland Clinic Conflict of
September 19, 2015 ASPMN 25th National Conference Esther I. Bernhofer, PhD, RN-BC Senior Nurse Researcher Pain Education Specialist Office of Nursing Research and Innovation Cleveland Clinic Conflict of
Motivational Interviewing Strategies and Techniques: Rationales and Examples
 Motivational Interviewing Strategies and Techniques: Rationales and Examples ASKING PERMISSION Rationale: Communicates respect for clients. Also, clients are more likely to discuss changing when asked,
Motivational Interviewing Strategies and Techniques: Rationales and Examples ASKING PERMISSION Rationale: Communicates respect for clients. Also, clients are more likely to discuss changing when asked,
Presently, there are no means of preventing bipolar disorder. However, there are ways of preventing future episodes: 1
 What is bipolar disorder? There are two main types of bipolar illness: bipolar I and bipolar II. In bipolar I, the symptoms include at least one lifetime episode of mania a period of unusually elevated
What is bipolar disorder? There are two main types of bipolar illness: bipolar I and bipolar II. In bipolar I, the symptoms include at least one lifetime episode of mania a period of unusually elevated
Intervention Strategies to Engage Students and Parents Struggling with School Anxiety School Refusal Patrick McGrath Ph.D Jackie Rhew MA, CADC, LPC
 Intervention Strategies to Engage Students and Parents Struggling with School Anxiety School Refusal Patrick McGrath Ph.D Jackie Rhew MA, CADC, LPC School Anxiety / School Refusal Program Alexian Brothers
Intervention Strategies to Engage Students and Parents Struggling with School Anxiety School Refusal Patrick McGrath Ph.D Jackie Rhew MA, CADC, LPC School Anxiety / School Refusal Program Alexian Brothers
What is an intervention?
 (Adapted from the Mayo Clinic, 2014) It's challenging to help a loved one struggling with any type of addiction. Sometimes a direct, heart-to-heart conversation can start the road to recovery. But when
(Adapted from the Mayo Clinic, 2014) It's challenging to help a loved one struggling with any type of addiction. Sometimes a direct, heart-to-heart conversation can start the road to recovery. But when
Is Faith Delusion? Andrew Sims
 Is Faith Delusion? Andrew Sims Fixed points You must be mad to believe that By mid-20th Century mutual distrust between the Church and Psychiatry Bilingual psychiatrists need... to become fluent in
Is Faith Delusion? Andrew Sims Fixed points You must be mad to believe that By mid-20th Century mutual distrust between the Church and Psychiatry Bilingual psychiatrists need... to become fluent in
GUIDE TO PATIENT COUNSELLING
 Guide To Patient Counselling page - 1 - GUIDE TO PATIENT COUNSELLING Communication is the transfer of information meaningful to those involved. It is the process in which messages are generated and sent
Guide To Patient Counselling page - 1 - GUIDE TO PATIENT COUNSELLING Communication is the transfer of information meaningful to those involved. It is the process in which messages are generated and sent
DSM-5: A Comprehensive Overview
 1) The original DSM was published in a) 1942 b) 1952 c) 1962 d) 1972 DSM-5: A Comprehensive Overview 2) The DSM provides all the following EXCEPT a) Guidelines for the treatment of identified disorders
1) The original DSM was published in a) 1942 b) 1952 c) 1962 d) 1972 DSM-5: A Comprehensive Overview 2) The DSM provides all the following EXCEPT a) Guidelines for the treatment of identified disorders
MANAGING DEPRESSIVE SYMPTOMS IN SUBSTANCE ABUSE CLIENTS DURING EARLY RECOVERY
 MANAGING DEPRESSIVE SYMPTOMS IN SUBSTANCE ABUSE CLIENTS DURING EARLY RECOVERY Presented by: William L. Mock, Ph.D., LISW,LICDC, SAP Professional Training Associates Inc North Ridgeville, Ohio 1 (216) 299-9506
MANAGING DEPRESSIVE SYMPTOMS IN SUBSTANCE ABUSE CLIENTS DURING EARLY RECOVERY Presented by: William L. Mock, Ph.D., LISW,LICDC, SAP Professional Training Associates Inc North Ridgeville, Ohio 1 (216) 299-9506
WORKERS COMPENSATION PROTOCOLS WHEN PRIMARY INJURY IS PSYCHIATRIC/PSYCHOLOGICAL
 WORKERS COMPENSATION PROTOCOLS WHEN PRIMARY INJURY IS PSYCHIATRIC/PSYCHOLOGICAL General Guidelines for Treatment of Compensable Injuries Patient must have a diagnosed mental illness as defined by DSM-5
WORKERS COMPENSATION PROTOCOLS WHEN PRIMARY INJURY IS PSYCHIATRIC/PSYCHOLOGICAL General Guidelines for Treatment of Compensable Injuries Patient must have a diagnosed mental illness as defined by DSM-5
Are you ever afraid to be around the person when he or she is drinking or using drugs because of the possibility of verbal or physical abuse?
 COMMON TERMS: Denial: The "hallmark" of the disease. All family members and close friends are affected by the actions of the Chemically Dependent Person. The refusal to admit the truth is a part of the
COMMON TERMS: Denial: The "hallmark" of the disease. All family members and close friends are affected by the actions of the Chemically Dependent Person. The refusal to admit the truth is a part of the
TRANSACTIONAL ANALYSIS
 TRANSACTIONAL ANALYSIS Developed by Eric Berne during the 1950 s, Transactional Analysis (TA) is a simple method of describing our experiences of life in a way that makes both sense and brings a smile
TRANSACTIONAL ANALYSIS Developed by Eric Berne during the 1950 s, Transactional Analysis (TA) is a simple method of describing our experiences of life in a way that makes both sense and brings a smile
Sue/Sue/Sue Understanding Abnormal Behavior, 9 th edition 2010 Cengage Learning CHAPTER EIGHT. Personality Disorders
 Sue/Sue/Sue Understanding Abnormal Behavior, 9 th edition 2010 Cengage Learning CHAPTER EIGHT Personality Disorders PERSONALITY DISORDERS Personality Disorder: Sue/Sue/Sue Understanding Abnormal Behavior,
Sue/Sue/Sue Understanding Abnormal Behavior, 9 th edition 2010 Cengage Learning CHAPTER EIGHT Personality Disorders PERSONALITY DISORDERS Personality Disorder: Sue/Sue/Sue Understanding Abnormal Behavior,
Talking Points. DOMESTIC VIOLENCE, ABUSE and CHILD CUSTODY
 Talking Points DOMESTIC VIOLENCE, ABUSE and CHILD CUSTODY These talking points were designed for domestic violence advocates and other allies of protective mothers to speak with administrative judges in
Talking Points DOMESTIC VIOLENCE, ABUSE and CHILD CUSTODY These talking points were designed for domestic violence advocates and other allies of protective mothers to speak with administrative judges in
Substance Abuse Treatment: Group Therapy
 Substance Abuse Treatment: Group Therapy Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Chapter 1 This natural propensity in humans makes group therapy
Substance Abuse Treatment: Group Therapy Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Chapter 1 This natural propensity in humans makes group therapy
What are Cognitive and/or Behavioural Psychotherapies?
 What are Cognitive and/or Behavioural Psychotherapies? Paper prepared for a UKCP/BACP mapping psychotherapy exercise Katy Grazebrook, Anne Garland and the Board of BABCP July 2005 Overview Cognitive and
What are Cognitive and/or Behavioural Psychotherapies? Paper prepared for a UKCP/BACP mapping psychotherapy exercise Katy Grazebrook, Anne Garland and the Board of BABCP July 2005 Overview Cognitive and
ASSESSMENT AND MANAGEMENT OF PSYCHOSIS IN PERSONS WITH DEMENTIA
 ASSESSMENT AND MANAGEMENT OF PSYCHOSIS IN PERSONS WITH DEMENTIA Overview: Psychosis is a common clinical feature of dementia. Hallucinations and delusions are the two most common types of psychotic symptoms
ASSESSMENT AND MANAGEMENT OF PSYCHOSIS IN PERSONS WITH DEMENTIA Overview: Psychosis is a common clinical feature of dementia. Hallucinations and delusions are the two most common types of psychotic symptoms
Schizophrenia. This factsheet provides a basic description of schizophrenia, its symptoms and the treatments and support options available.
 This factsheet provides a basic description of schizophrenia, its symptoms and the treatments and support options available. What is schizophrenia? Schizophrenia is a commonly misunderstood condition,
This factsheet provides a basic description of schizophrenia, its symptoms and the treatments and support options available. What is schizophrenia? Schizophrenia is a commonly misunderstood condition,
Personality Disorders
 Personality Disorders Source: Linda Lebelle, Focus Adolescent Services A Personality Disorder is identified by a pervasive pattern of experience and behaviour that is abnormal with respect to any of the
Personality Disorders Source: Linda Lebelle, Focus Adolescent Services A Personality Disorder is identified by a pervasive pattern of experience and behaviour that is abnormal with respect to any of the
Harm Reduction Strategies to Address Anxiety and Trauma. Presented by Jodi K. Brightheart, MSW
 Harm Reduction Strategies to Address Anxiety and Trauma Presented by Jodi K. Brightheart, MSW What would you diagnose a client with the following symptoms? Frantic efforts to avoid being abandoned by friends
Harm Reduction Strategies to Address Anxiety and Trauma Presented by Jodi K. Brightheart, MSW What would you diagnose a client with the following symptoms? Frantic efforts to avoid being abandoned by friends
Chapter 13. Prejudice: Causes and Cures
 Chapter 13 Prejudice: Causes and Cures Prejudice Prejudice is ubiquitous; it affects all of us -- majority group members as well as minority group members. Prejudice Prejudice is dangerous, fostering negative
Chapter 13 Prejudice: Causes and Cures Prejudice Prejudice is ubiquitous; it affects all of us -- majority group members as well as minority group members. Prejudice Prejudice is dangerous, fostering negative
Criteria to Identify Abnormal Behavior
 Criteria to Identify Abnormal Behavior Unusualness Social deviance Emotional distress Maladaptive behavior Dangerousness Faulty perceptions or interpretations of reality Hallucinations Delusions Copyright
Criteria to Identify Abnormal Behavior Unusualness Social deviance Emotional distress Maladaptive behavior Dangerousness Faulty perceptions or interpretations of reality Hallucinations Delusions Copyright
Addiction is a Brain Disease
 Addiction is a Brain Disease By ALAN I. LESHNER, MD A core concept evolving with scientific advances over the past decade is that drug addiction is a brain disease that develops over time as a result of
Addiction is a Brain Disease By ALAN I. LESHNER, MD A core concept evolving with scientific advances over the past decade is that drug addiction is a brain disease that develops over time as a result of
Chapter 14. Psychological Disorders
 Chapter 14 Psychological Disorders We ve Come a Long Way Trepanning Ancient priests or medicine men cut holes into the skills of living persons, to release the demons. What is Abnormality Psychopathology
Chapter 14 Psychological Disorders We ve Come a Long Way Trepanning Ancient priests or medicine men cut holes into the skills of living persons, to release the demons. What is Abnormality Psychopathology
Education Day Schedule with Topics and Objectives: 12 to 1 brunch and keynote. Session 1-1:00 to 2:00PM
 Education Day Schedule with Topics and 12 to 1 brunch and keynote Session 1-1:00 to 2:00PM Eating Disorders: Myths vs. Realities Presented by Elizabeth Mariutto, PsyD, Lindner Center of HOPE, Staff Psychologist
Education Day Schedule with Topics and 12 to 1 brunch and keynote Session 1-1:00 to 2:00PM Eating Disorders: Myths vs. Realities Presented by Elizabeth Mariutto, PsyD, Lindner Center of HOPE, Staff Psychologist
SPECIALIST ARTICLE A BRIEF GUIDE TO PSYCHOLOGICAL THERAPIES
 SPECIALIST ARTICLE A BRIEF GUIDE TO PSYCHOLOGICAL THERAPIES Psychological therapies are increasingly viewed as an important part of both mental and physical healthcare, and there is a growing demand for
SPECIALIST ARTICLE A BRIEF GUIDE TO PSYCHOLOGICAL THERAPIES Psychological therapies are increasingly viewed as an important part of both mental and physical healthcare, and there is a growing demand for
OCD and disordered eating: When OCD masquerades as eating disorders
 OCD and disordered eating: When OCD masquerades as eating disorders Brigette A. Erwin, PhD Director, OCD Program Anxiety and Agoraphobia Treatment Center Bala Cynwyd, PA A presentation conducted at the
OCD and disordered eating: When OCD masquerades as eating disorders Brigette A. Erwin, PhD Director, OCD Program Anxiety and Agoraphobia Treatment Center Bala Cynwyd, PA A presentation conducted at the
A Review of Conduct Disorder. William U Borst. Troy State University at Phenix City
 A Review of 1 Running head: A REVIEW OF CONDUCT DISORDER A Review of Conduct Disorder William U Borst Troy State University at Phenix City A Review of 2 Abstract Conduct disorders are a complicated set
A Review of 1 Running head: A REVIEW OF CONDUCT DISORDER A Review of Conduct Disorder William U Borst Troy State University at Phenix City A Review of 2 Abstract Conduct disorders are a complicated set
Foundation Skills for Substance Abuse Counseling. Geoff Wilson, LCSW, CADC The Ridge Behavioral Health System
 Foundation Skills for Substance Abuse Counseling Geoff Wilson, LCSW, CADC The Ridge Behavioral Health System The Take Home!! What do you want to leave with today? Agenda TAP 21: Addiction Counseling Competencies:
Foundation Skills for Substance Abuse Counseling Geoff Wilson, LCSW, CADC The Ridge Behavioral Health System The Take Home!! What do you want to leave with today? Agenda TAP 21: Addiction Counseling Competencies:
Acceptance and Commitment Therapy with Treatment Resistant PTSD Clients. Michael P. Twohig, Ph.D. Associate Professor of Psychology
 Acceptance and Commitment Therapy with Treatment Resistant PTSD Clients Michael P. Twohig, Ph.D. Associate Professor of Psychology C B T How did ACT develop? 1 2 3 Rule Governed Behavior Verbal humans
Acceptance and Commitment Therapy with Treatment Resistant PTSD Clients Michael P. Twohig, Ph.D. Associate Professor of Psychology C B T How did ACT develop? 1 2 3 Rule Governed Behavior Verbal humans
Insecure Attachment and Reactive Attachment Disorder
 Attachment Disorders Insecure Attachment and Reactive Attachment Disorder When infants and young children have a loving caregiver consistently responding to their needs, they build a secure attachment.
Attachment Disorders Insecure Attachment and Reactive Attachment Disorder When infants and young children have a loving caregiver consistently responding to their needs, they build a secure attachment.
A Guide to Cognitive- Behavioural Therapy (CBT)
") A Guide to Cognitive- Behavioural Therapy (CBT) Cognitive-behavioural Therapy (CBT) aims to help you to change the way that you think, feel and behave. It is used as a treatment for various mental health
A Guide to Cognitive- Behavioural Therapy (CBT) Cognitive-behavioural Therapy (CBT) aims to help you to change the way that you think, feel and behave. It is used as a treatment for various mental health
SUBSTANCE ABUSE & DEPRESSION: WHAT YOU SHOULD KNOW
 SUBSTANCE ABUSE & DEPRESSION: WHAT YOU SHOULD KNOW TABLE OF CONTENTS What is Depression? 4 Symptoms of Depression 6 Substance Abuse as a Coping Mechanism 8 Which Occurs First? 10 Substance Abuse and the
SUBSTANCE ABUSE & DEPRESSION: WHAT YOU SHOULD KNOW TABLE OF CONTENTS What is Depression? 4 Symptoms of Depression 6 Substance Abuse as a Coping Mechanism 8 Which Occurs First? 10 Substance Abuse and the
Personality Disorders
 Personality Disorders Chapter 11 Personality Disorders: An Overview The Nature of Personality and Personality Disorders Enduring and relatively stable predispositions (i.e., ways of relating and thinking)
Personality Disorders Chapter 11 Personality Disorders: An Overview The Nature of Personality and Personality Disorders Enduring and relatively stable predispositions (i.e., ways of relating and thinking)
Identification and Treatment Manual
 Therapeutic Identification of Depression in Young People Identification and Treatment Manual The TIDY project The Academic Unit of Child and Adolescent Psychiatry, Imperial College London & Lonsdale Medical
Therapeutic Identification of Depression in Young People Identification and Treatment Manual The TIDY project The Academic Unit of Child and Adolescent Psychiatry, Imperial College London & Lonsdale Medical
For the Support Person
 For the Support Welcome to this self-care guide and thank you for agreeing to act as a Support. Your involvement is an important part of the support for the person in recovery. You may be a relative, mental
For the Support Welcome to this self-care guide and thank you for agreeing to act as a Support. Your involvement is an important part of the support for the person in recovery. You may be a relative, mental
Co-dependency. Fact Sheet on co-dependency from Mental Health America:
 Co-dependency Fact Sheet on co-dependency from Mental Health America: Co-dependency is a learned behavior that can be passed down from one generation to another. It is an emotional and behavioral condition
Co-dependency Fact Sheet on co-dependency from Mental Health America: Co-dependency is a learned behavior that can be passed down from one generation to another. It is an emotional and behavioral condition
RAK Medical and Health Sciences University. RAK College of Nursing RN-BSN Bridge Program Ethical Issues in Mental Health Nursing
 RAK Medical and Health Sciences University RAK College of Nursing RN-BSN Bridge Program Ethical Issues in Mental Health Nursing Mrs.Vimala Edwin MSc N,PGDHM Lecturer RAK College of Nursing Learning objectives
RAK Medical and Health Sciences University RAK College of Nursing RN-BSN Bridge Program Ethical Issues in Mental Health Nursing Mrs.Vimala Edwin MSc N,PGDHM Lecturer RAK College of Nursing Learning objectives
The Emotional Bank Account
 The Emotional Bank Account We all know what a bank account is. It is where we put our money, make deposits, save for the future, and make withdrawals when we need to. An Emotional Bank Account is a metaphor
The Emotional Bank Account We all know what a bank account is. It is where we put our money, make deposits, save for the future, and make withdrawals when we need to. An Emotional Bank Account is a metaphor
 DEPARTMENT OF COUNSELING AND EDUCATIONAL PSYCHOLOGY COLLEGE OF EDUCATION 6300 Ocean drive, Unit 5834 Corpus Christi, Texas- 78412-5834 Facilitating Change: Combining Motivational Interviewing and Dialectical
DEPARTMENT OF COUNSELING AND EDUCATIONAL PSYCHOLOGY COLLEGE OF EDUCATION 6300 Ocean drive, Unit 5834 Corpus Christi, Texas- 78412-5834 Facilitating Change: Combining Motivational Interviewing and Dialectical
Rogers Memorial Hospital (Wisconsin).
.") Bradley C. Riemann, Ph.D. Clinical Director, OCD Center and CBT Services Rogers Memorial Hospital The Use of Exposure and Ritual Prevention with OCD: Key Concepts and New Directions OCD Center Rogers Memorial
Bradley C. Riemann, Ph.D. Clinical Director, OCD Center and CBT Services Rogers Memorial Hospital The Use of Exposure and Ritual Prevention with OCD: Key Concepts and New Directions OCD Center Rogers Memorial
The Goal of Correctional Counseling
 41140_CH03_Pass2.qxd 8/9/07 12:21 PM Page 45 Jones and Bartlett Publishers. NOT FOR SALE OR DISTRIBUTION The Goal of Correctional Counseling 3 The goal of correctional counseling is usually based on two
41140_CH03_Pass2.qxd 8/9/07 12:21 PM Page 45 Jones and Bartlett Publishers. NOT FOR SALE OR DISTRIBUTION The Goal of Correctional Counseling 3 The goal of correctional counseling is usually based on two
Clinical Science I CRN 25305
 Clinical Science I CRN 25305 (formerly, Intervention Science I) Course Syllabus Winter 2012 Tuesdays 2:00 4:50 pm in 295 Straub (clinic group room) Instructors: Karyn L. Angell, Ph.D. Stephenie Frank,
Clinical Science I CRN 25305 (formerly, Intervention Science I) Course Syllabus Winter 2012 Tuesdays 2:00 4:50 pm in 295 Straub (clinic group room) Instructors: Karyn L. Angell, Ph.D. Stephenie Frank,
Minnesota Co-occurring Mental Health & Substance Disorders Competencies:
 Minnesota Co-occurring Mental Health & Substance Disorders Competencies: This document was developed by the Minnesota Department of Human Services over the course of a series of public input meetings held
Minnesota Co-occurring Mental Health & Substance Disorders Competencies: This document was developed by the Minnesota Department of Human Services over the course of a series of public input meetings held
Physical Symptoms Mood Symptoms Behavioral Symptoms
 Prescription drugs are the 3 rd most commonly abused drugs amongst teens in Nebraska, and the same statistic holds true on a national level. The rise in prescription drug abuse is becoming increasingly
Prescription drugs are the 3 rd most commonly abused drugs amongst teens in Nebraska, and the same statistic holds true on a national level. The rise in prescription drug abuse is becoming increasingly