Sir Muir Gray, Director,
|
|
|
- Andrew Preston
- 8 years ago
- Views:
Transcription
1 Incorporating Specialty Nurses and Advanced Nurse Practice into Multidisciplinary i li Heart Failure Team Abdiqani Qasim, MScN, FNP, ACNP Head, General Nursing Training, Unit

2 Knowledge is the enemy of disease The application of what we know will have a bigger impact on health and disease than any single drug or technology likely to be introduced in the next decade. Sir Muir Gray, Director, NHS National Knowledge Service

3 Simple hand washing to prevent transmission of disease Elevation HOB to prevent VAP

4 CHF Population Salt & Fluid restriction Daily weight Activity i monitoring i demand d & Supply Medication Sign and symptoms to watch Important of follow up appointments When to call help

5
6 Advanced dn Nursing Practice Advanced Nursing Practice (ANP) is an umbrella term. It describes an advanced d level l of nursing practice that t maximizes the use of in-depth nursing knowledge & skill in meeting the health needs of clients. In this way, ANP extends the boundaries of nursing's scope of practice & contributes to nursing knowledge & the development & advancement of the profession (CNA 1999)

7 Acute Care Nurse Practitioner ACNP The Acute Care Nurse Practitioner is an academic title used to describe an RN who has completed education at a graduate level, in an ACNP program, with a focus on a sub-specialty specialty (NPAO 2002)

8 Advanced Practice Nurse APN An ACNP is an advanced practice nurse who works collaboratively with members of the health care team, not only to provide individual patient care, but also to improve practice, using evidence based research to develop, implement & evaluate care Canadian Association of Advanced Practice Nurses (CAAPN) 2003

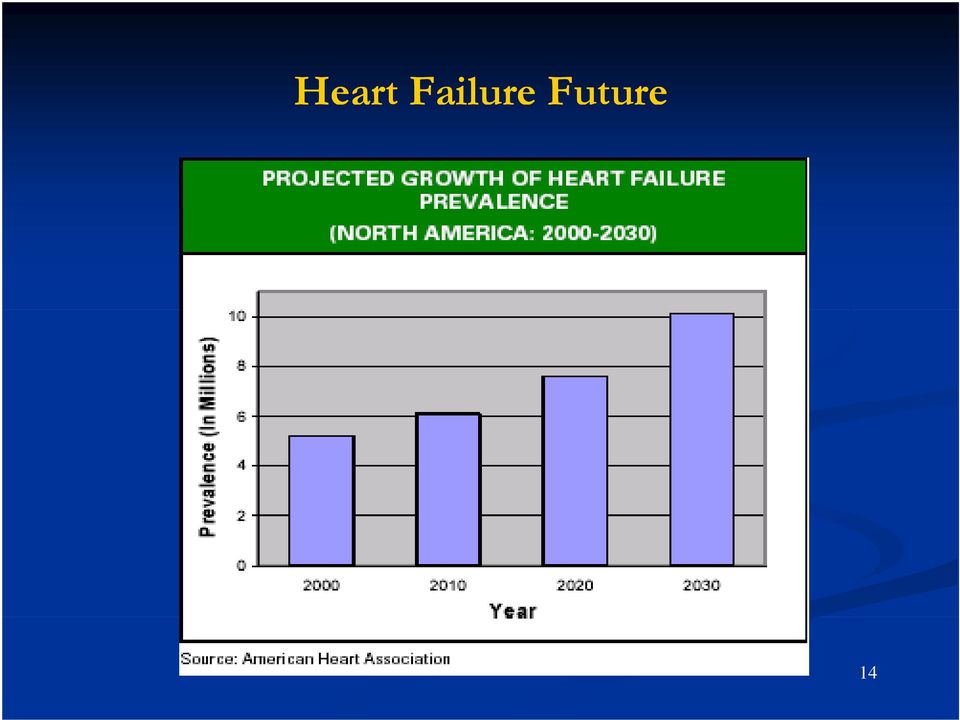
9 Background Heart failure (HF) is a syndrome of shortness of breath and fatigue. It occurs when forward flow of blood out of the heart is impeded. This is the only cardiovascular condition that continues to increase in prevalence and incidence. It is a major healthcare problem, not only for the patient, but also for significant others and the community at large.

10 Background HF is a leading cause of hospitalization and death world wide, and its prevalence continues to increase. The clinical care of patients with HF encompasses a continuum from the treatment of acute episodes requiring ii hospitalization to chronic management in the outpatient office setting.

11 Heart Failure Impact
12 Barriers sto Effective ectve Heart Failure Management age e Rich et al, Journal of Cardiac Failure Vol. 5 No. 1 March 1999

13 Evidences
14 Heart Failure Future 14
15 Lothian Managed Clinical Network (Heart Failure) Rehabilitation General practitioner Specialist HF nurses District nurse Patient Cardiologist Specialist/EP Volunteer support workers Geriatrician/care of the elderly elderly Social Services Pharmacist Palliative Care team Dietitian

16 Cycles of Heart Failure Care Home Hospitalisation GP Clinic OP clinic

17 Role of APN Incorporating specialty nurses and NPs into multidisciplinary heart failure teams enhances the efforts of cardiologists and improves patient access to medical care and education. Nurses working within such a framework develop significant expertise in the narrowly focused area of heart failure management to implement, coordinate, and monitor all aspects of heart failure care.

18 Role of APN They are able to: Monitor hemodynamic status, Titrate medications, Review results of laboratory testing, and Triage calls from patients, which may prevent repeat hospital admissions. Nurses may transplantation, support. also assist end-of-life with care, end-stage strategies of or mechanical circulatory

19 Case Study The following case studies demonstrate the role NPs play in acute and chronic heart failure care Mrs. KN is a 68-year-old woman admitted with progressive dyspnea, abdominal bloating, and cough. When severe orthopnea developed, she presented to the emergency room.

20 Case Study History of Present Illness Bt Beta blockers for lft left ventricular ti dysfunction, discontinued d several months prior to admission, were restarted 1 week prior to admission after a nuclear study suggested a decrease in left ventricular ejection fraction (LVEF).

21 Case Study Past Medical History 1999: non-hodgkin's lymphoma treated with adriamycin 2000: tricuspid valve repair 2000: cardiomyopathy (presumed adriamycin-induced), induced), initial LVEF 20% 2001: LVEF improved to 50% with medical therapy 2005: implantable cardioverter-defibrillator defibrillator for nonsustained ventricular tachycardia
22 Case Study Admission Medications Mrs. KN currently takes: Furosemide Potassium Simvastatin Lisinopril, and Carvedilol.
23 Case Study Plan of Care/Clinical Course Mrs. KN was admitted d to an acute care floor rb by the general cardiology service with a presumed heart failure exacerbation. The attending cardiologist i requested a formal consultation by the heart failure service. The acute care nurse practitioner (ACNP) proceeded with a thorough history and physical exam: Vital signs: blood pressure (BP) 102/70 mm Hg, heart rate 92 bpm, SaO2 96% General demeanour: no distress; pleasant and cooperative Chest: clear lungs
24 Case Study Cardiovascular: heart rhythm regular, II/VI holosystolic murmur, laterally displaced point of maximal impulse,, jugular jg venous distension (~ right atrial pressure about 14 cm H20) Abdomen: soft, active bowel sounds, right upper quadrant tenderness, liver edge at the costal margin, overall liver height 8 cm Extremities: no edema, slightly cool Admission laboratory results and diagnostic tests: B-type natriuretic peptide 1287 pg/ml, all other labs normal; Electrocardiogram: normal sinus rhythm
25 Case Study The ACNP discussed Mrs. KN's case with the attending physician, and it was mutually agreed that the patient needed intravenous (IV) diuretics and monitoring of diuretic response. The beta blocker was discontinued, given her volume- overloaded dd state. Mrs. KN was given furosemide 40 mg IV. Over the next 2 hours, the symptoms improved as she started to diurese. However, she had a reported decrease in BP to 85/60 mm Hg. Sheremained asymptomaticand ti and alert.
26 Case Study The BP was confirmed with a manual sphygmomanometer in both arms. The ACNP discontinued her lisinopril and discussed plans with the attending physician for transfer to the intensive care unit and invasive hemodynamic monitoring i should Mrs. KN's BP continue to decline. Over the next hour, KN's BPfellto78/56 mm Hg. Echocardiogram was ordered: LVEF was again 20% with moderately severe mitral regurgitation and evidence of pulmonary hypertension.
27 Case Study The ACNP discussed Mrs. KN's hypotension and ventricular function with the attending physician, patient, and the family. KN underwent pulmonary artery catheter placement. Her hemodynamic status showed: Mean right atrial pressure: 25 mm Hg Mean pulmonary capillary wedge pressure: 31 mm Hg Pulmonary artery pressures: 38/56 mm Hg Cardiac output: 2.8 L/min; cardiac index: 1.4 L/min/m2 Mixed venous saturation: 40%
28 Case Study Mrs. KN was transferred to the coronary care unit with an indwelling pulmonary artery catheter. Milrinone 0.3 mcg/kg/min and a continuous furosemide drip were started. Care was managed by an intensive care unit fellow and the attending physician. The ACNP resumed care after KN had stabilized and transferred from the intensive care unit to the acute care floor.
29 Case Study She had lost 5kg of body weight. Orthopnea symptoms had completely resolved and BP had stabilized. KN was slowly weaned off milrinone and transitioned to an oral diuretic regimen, and lisinopril i was restarted rt The ACNP provided discharge planning, which consisted of patient and family education about heart failure self-management, including follow-up appointments, what to monitor at home, and when to call if changes in symptoms occur.
30 Case Study The ACNP provided discharge documentation mandated by the Joint Commission for Accreditation of Hospital and the Centers for Mdi Medicare Services Assessment of LV function; Recommendation for treatment with angiotensin converting enzyme (ACE) inhibitors in the event that LVEF drops below 40%; and Discharge instructions on medications, Weighing g daily at home, Maintaining activity, Restricting sodium, and when to call about worsening symptoms. Plans for resuming the beta blocker would occur in the outpatient setting
31 Case Study Summary This is an example of how an ACNP functions as part of a team to provide consultative services to ageneral cardiologist for someone hospitalized with heart failure. The ACNP was able to adequately assess volume and perfusion status of a patient with acutely decompensated heart failure, and then make a collaborative plan with the attending physician.
32 Case Study Understanding hemodynamic compromise, using evidence-based medicines, monitoring response to therapy, and adjusting the plan of care for deterioration in clinical status are all within the scope of an ACNP. In this case, the ACNP was able to collaborate with others to intensify care when needed, then to resume care and prepare the patient and family for discharge.
33 Case Study 2: Mr. P's Cardiomyopathy y and Heart Failure Mr. P, a 28-year-old male, was hospitalized with new- onset heart failure, which was diagnosed as idiopathic dilated cardiomyopathy. The left ventricular ejection fraction was 18%. The heart failure and transplant team started a comprehensive workup for cardiac transplantation in case Mr. P failed medical therapy.
34 Case Study 2: Mr. P's condition stabilized. He was given diuretics and started on an angiotensin converting enzyme inhibitor and discharged home. The outpatient plan was for close follow-up and titration of prognosis-altering medications as tolerated.
35 Case Study 2: The heart failure nurse practitioner (HF NP) saw Mr. P for his first outpatient visit. Hospital records gave a clear history and plan for outpatient management
36 HF NP Assessment (Post Discharge) Mr. P had done well since his hospitalization. He kept records of his vital signs: His systolic blood pressure (BP) ranged from mm Hg, Heart rate was in the 80s, and His weight only fluctuated 2 lbs in the last 5 days.
37 HF NP Assessment (Post Discharge) He was clearly less short of breath than before his admission, and no longer noted orthopnea. He had no chest pain, light-headedness headedness, or syncope. He was eating and sleeping well, and was tolerating slow walks with his wife and new baby. He was trying to adhere to a low-salt, fluid-restricted diet, but it was "tough."
38 Discharge Medications Mr. P was currently taking: Lisinopril 5 mg daily, Furosemide 40 mg twice a day, Digoxin 0.25 mg daily, potassium 20 meq twice a day, and a multivitamin daily. Physical Examination Vital signs: BP 106/64 mm Hg, Heart rate 83 bpm, Weight 84 kg, SaO2 95% General: No distress Chest: clear lungs
39 Discharge Medications Cardiovascular: regular rate and rhythm; no extrasystoles; II/VI systolic murmur left of sternum and radiating to axilla; neck veins not distended; no edema; peripheral pulses intact Abdomen: normal exam Extremities: normal pulses
40 Assessment Mr. P had an idiopathic dilated cardiomyopathy with new-onset heart failure symptoms. He was diagnosed and stabilized in the hospital setting. He was currently in Stage C and had New York Heart Association Class II symptoms. He was tolerating his new medications without problem, was euvolemic (ie, not retaining fluid), and had a stable blood pressure in clinic and at home.
41 Plan of Care/Clinical Course A regimen of Carvedilol mg twice daily was prescribed. Mr. P was given samples, and the medication name and dose were added to his written list from the hospital.
42 Plan of Care/Clinical Course He was instructed to continue self-monitoring and to call the HF NP if he had worsening dyspnea, weight gain, or other symptoms. He was also instructed that, although beta blockers provide morbidity and mortality benefits, they would take time to work.
43 Plan of Care/Clinical Course Mr. P was instructed that he will need close follow-up for titrations every 2 weeks, as tolerated. He was commended d on keeping records rd and bringing them to the clinic appointment. Suggestions on how to flavour food while avoiding salt were provided. The HF NP completed the appointment by answering any remaining questions.
44 Plan of Care/Clinical Course The long-term plan of medical therapy was reiterated. Transplantation would be considered if his condition deteriorated. The risk of sudden death had been discussed in the hospital, and it was agreed to wait until medications had been appropriately titrated before assessing the need for a prophylactic p internal cardiac defibrillator.
45 Summary This case demonstrates how an outpatient HF NP provided care to a patient recently discharged with acutely decompensated heart failure. An outpatient HF NP's role includes: Knowledge about the hospital course, Assessing toleration to medications, Evaluating volume and perfusion status, Offering further patient self-management education, and Initiating prognosis-altering medications.
46 Summary Other considerations of outpatient management include managing co morbidities of heart failure and assessing the need for other therapies based on the stage of heart failure
47 Conclusion Newer models of care are needed to accommodate the needs of the growing population of heart failure patients and the wide range of treatments available. Recent discussions centered on narrowing the gap between the need for and supply of heart failure specialists fail to fully acknowledge the role specialized nurses now have in improving the delivery of heart failure care. Nurses can function as "heart failure specialists," complementing and augmenting the vital role of heart failure cardiologists.
48 Conclusion When studied in the context of multidisciplinary teams, often led by cardiologists, nurse specialists have been shown to contribute significantly to improving outcomes. While the need for a fully recognized ed heart failure subspecialty within cardiology is clear, national organizations are now planning for a cardiovascular specialty within nursing. Future crises in heart failure management may be mitigated in part by more uniformly adopting nurse specialists to perform many of the core cognitive functions of integrated disease management.
49 Conclusion Concerns are mounting regarding g the limited availability of heart failure specialists. Specialized providers are in greater demand db because of a growing number of cases of heart failure and the advancement of technology that has made complicated treatment strategies possible. While many solutions are being explored to bridge the gap between the number of qualified specialists and projected needs, the role nurses play has received limited analysis.
50 Conclusion Strategies using the expertise provided by specialized nurses have generally shown improved heart failure outcomes. Nurse specialists should not be overlooked as part of the solution for providing care to those afflicted with heart failure.
51 Pathogenesis Primary damage myocyte loss overload Necrosis apoptosis Stretch Pump dysfunction Neurohumoral activation Ventricular remodeling SNS RAAS, AVP Edema, tachycardia vasoconstriction, congestion CHF
Procedure for Inotrope Administration in the home
 Procedure for Inotrope Administration in the home Purpose This purpose of this procedure is to define the care used when administering inotropic agents intravenously in the home This includes: A. Practice
Procedure for Inotrope Administration in the home Purpose This purpose of this procedure is to define the care used when administering inotropic agents intravenously in the home This includes: A. Practice
Advanced Heart Failure & Transplantation Fellowship Program
 Advanced Heart Failure & Transplantation Fellowship Program Curriculum I. Patient Care When on the inpatient Heart Failure and Transplant Cardiology service, the cardiology fellow will hold primary responsibility
Advanced Heart Failure & Transplantation Fellowship Program Curriculum I. Patient Care When on the inpatient Heart Failure and Transplant Cardiology service, the cardiology fellow will hold primary responsibility
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
CORONARY ARTERY BYPASS GRAFT & HEART VALVE SURGERY
 CORONARY ARTERY BYPASS GRAFT & HEART VALVE SURGERY www.cpmc.org/learning i learning about your health What to Expect During Your Hospital Stay 1 Our Team: Our cardiac surgery specialty team includes nurses,
CORONARY ARTERY BYPASS GRAFT & HEART VALVE SURGERY www.cpmc.org/learning i learning about your health What to Expect During Your Hospital Stay 1 Our Team: Our cardiac surgery specialty team includes nurses,
1 Congestive Heart Failure & its Pharmacological Management
 Harvard-MIT Division of Health Sciences and Technology HST.151: Principles of Pharmocology Instructor: Prof. Keith Baker 1 Congestive Heart Failure & its Pharmacological Management Keith Baker, M.D., Ph.D.
Harvard-MIT Division of Health Sciences and Technology HST.151: Principles of Pharmocology Instructor: Prof. Keith Baker 1 Congestive Heart Failure & its Pharmacological Management Keith Baker, M.D., Ph.D.
Successful Heart Failure Management Nurse/NP Run Clinics
 Dagmar Knot RN BScN CCCN Transplant Coordination Team Leader Organ Transplant Center KFSHRC Riyadh, KSA Heart Failure Nurses Role, responsibilities & education Successful Heart Failure Management Nurse/NP
Dagmar Knot RN BScN CCCN Transplant Coordination Team Leader Organ Transplant Center KFSHRC Riyadh, KSA Heart Failure Nurses Role, responsibilities & education Successful Heart Failure Management Nurse/NP
Pulmonary Artery Hypertension
 Pulmonary Artery Hypertension Janet M. Pinson, RN, MSN, ACNP Maureen P. Flattery, RN, MS, ANP Virginia Commonwealth University Health System Richmond, VA Pulmonary artery hypertension (PAH) is defined
Pulmonary Artery Hypertension Janet M. Pinson, RN, MSN, ACNP Maureen P. Flattery, RN, MS, ANP Virginia Commonwealth University Health System Richmond, VA Pulmonary artery hypertension (PAH) is defined
Atrial Fibrillation Management Across the Spectrum of Illness
 Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
The heart then repolarises (or refills) in time for the next stimulus and contraction.
 in time for the next stimulus and contraction.") Atrial Fibrillation BRIEFLY, HOW DOES THE HEART PUMP? The heart has four chambers. The upper chambers are called atria. One chamber is called an atrium, and the lower chambers are called ventricles. In
Atrial Fibrillation BRIEFLY, HOW DOES THE HEART PUMP? The heart has four chambers. The upper chambers are called atria. One chamber is called an atrium, and the lower chambers are called ventricles. In
The new Heart Failure pathway
 The new Heart Failure pathway An integrated and seamless Strategy Dr Sunil Balani Definition of Heart Failure The inability of the heart to pump blood at a rate commensurate with the requirements of metabolising
The new Heart Failure pathway An integrated and seamless Strategy Dr Sunil Balani Definition of Heart Failure The inability of the heart to pump blood at a rate commensurate with the requirements of metabolising
Universitätsklinik für Kardiologie. Test. Thomas M. Suter Akute Herzinsuffizienz Diagnostik und Therapie thomas.suter@insel.ch 1
 Test Thomas M. Suter Akute Herzinsuffizienz Diagnostik und Therapie thomas.suter@insel.ch 1 Heart Failure - Definition European Heart Journal (2008) 29, 2388 2442 Akute Herzinsuffizienz Diagnostik und
Test Thomas M. Suter Akute Herzinsuffizienz Diagnostik und Therapie thomas.suter@insel.ch 1 Heart Failure - Definition European Heart Journal (2008) 29, 2388 2442 Akute Herzinsuffizienz Diagnostik und
Quiz 5 Heart Failure scores (n=163)
") Quiz 5 Heart Failure summary statistics The correct answers to questions are indicated by *. Students were awarded 2 points for question #3 for either selecting spironolactone or eplerenone. However, the
Quiz 5 Heart Failure summary statistics The correct answers to questions are indicated by *. Students were awarded 2 points for question #3 for either selecting spironolactone or eplerenone. However, the
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL
 Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
CONGESTIVE HEART FAILURE PATIENT TEACHING
 CONGESTIVE HEART FAILURE PATIENT TEACHING What is Heart Failure? Congestive Heart Failure occurs when the heart loses its ability to pump enough blood to meet the body s needs. Because the heart is not
CONGESTIVE HEART FAILURE PATIENT TEACHING What is Heart Failure? Congestive Heart Failure occurs when the heart loses its ability to pump enough blood to meet the body s needs. Because the heart is not
Heart Attack: What You Need to Know
 A WorkLife4You Guide Heart Attack: What You Need to Know What is a Heart Attack? The heart works 24 hours a day, pumping oxygen and nutrient-rich blood to the body. Blood is supplied to the heart through
A WorkLife4You Guide Heart Attack: What You Need to Know What is a Heart Attack? The heart works 24 hours a day, pumping oxygen and nutrient-rich blood to the body. Blood is supplied to the heart through
SPECIALTY : CARDIOLOGY CLINICAL PROBLEM: HEART FAILURE
 SPECIALTY : CARDIOLOGY CLINICAL PROBLEM: HEART FAILURE Summary Heart failure has a worse prognosis than many cancers with an annual mortality of 40% in the first year following diagnosis and 10% thereafter.
SPECIALTY : CARDIOLOGY CLINICAL PROBLEM: HEART FAILURE Summary Heart failure has a worse prognosis than many cancers with an annual mortality of 40% in the first year following diagnosis and 10% thereafter.
Inpatient Heart Failure Management: Risks & Benefits
 Inpatient Heart Failure Management: Risks & Benefits Dr. Kenneth L. Baughman Professor of Medicine Harvard Medical School Director, Advanced Heart Disease Section Brigham & Women's Hospital Harvard Medical
Inpatient Heart Failure Management: Risks & Benefits Dr. Kenneth L. Baughman Professor of Medicine Harvard Medical School Director, Advanced Heart Disease Section Brigham & Women's Hospital Harvard Medical
Heart Failure: Diagnosis and Treatment
 Heart Failure: Diagnosis and Treatment Approximately 5 million people about 2 percent of the U.S. population are affected by heart failure. Diabetes affects 20.8 million Americans and 65 million Americans
Heart Failure: Diagnosis and Treatment Approximately 5 million people about 2 percent of the U.S. population are affected by heart failure. Diabetes affects 20.8 million Americans and 65 million Americans
Tackling the Semantic Interoperability challenge
 European Patient Summaries: What is next? Tackling the Semantic Interoperability challenge Dipak Kalra Cross-border health care The context for sharing health summaries Also useful for within-border health
European Patient Summaries: What is next? Tackling the Semantic Interoperability challenge Dipak Kalra Cross-border health care The context for sharing health summaries Also useful for within-border health
Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations.
 INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
Program Evaluation: RCH Heart Function Clinic February 2, 2011 - May 1, 2012. Charline Hooper, Margaret Meloche, Rita Sobolyeva
 Program Evaluation: RCH Heart Function Clinic February 2, 2011 - May 1, 2012 Charline Hooper, Margaret Meloche, Rita Sobolyeva 1 Evaluation Planning Team Charline Hooper, Nurse Practitioner, RCH Cardiac
Program Evaluation: RCH Heart Function Clinic February 2, 2011 - May 1, 2012 Charline Hooper, Margaret Meloche, Rita Sobolyeva 1 Evaluation Planning Team Charline Hooper, Nurse Practitioner, RCH Cardiac
2/20/2015. Cardiac Evaluation of Potential Solid Organ Transplant Recipients. Issues Specific to Transplantation. Kidney Transplantation.
 DISCLOSURES I have no relevant financial relationships to disclose. Cardiac Evaluation of Potential Solid Organ Transplant Recipients Michele Hamilton, MD Director, Heart Failure Program Cedars Sinai Heart
DISCLOSURES I have no relevant financial relationships to disclose. Cardiac Evaluation of Potential Solid Organ Transplant Recipients Michele Hamilton, MD Director, Heart Failure Program Cedars Sinai Heart
Cardiovascular System & Its Diseases. Lecture #4 Heart Failure & Cardiac Arrhythmias
 Cardiovascular System & Its Diseases Lecture #4 Heart Failure & Cardiac Arrhythmias Dr. Derek Bowie, Department of Pharmacology & Therapeutics, Room 1317, McIntyre Bldg, McGill University derek.bowie@mcgill.ca
Cardiovascular System & Its Diseases Lecture #4 Heart Failure & Cardiac Arrhythmias Dr. Derek Bowie, Department of Pharmacology & Therapeutics, Room 1317, McIntyre Bldg, McGill University derek.bowie@mcgill.ca
Treating AF: The Newest Recommendations. CardioCase presentation. Ethel s Case. Wayne Warnica, MD, FACC, FACP, FRCPC
 Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
SYMPTOMS Heart failure symptoms may vary and can be hard to detect. Symptoms may include:
 Heart Failure Heart failure is a condition in which the heart has trouble pumping blood. This means your heart does not pump blood efficiently for your body to work well. In some cases of heart failure,
Heart Failure Heart failure is a condition in which the heart has trouble pumping blood. This means your heart does not pump blood efficiently for your body to work well. In some cases of heart failure,
Supportive Cardiology: Living with Advanced Heart Failure A GUIDE FOR PATIENTS AND FAMILIES
 Supportive Cardiology: Living with Advanced Heart Failure A GUIDE FOR PATIENTS AND FAMILIES Table of contents Contact information...1 Advanced heart failure care at North York General Hospital...2 What
Supportive Cardiology: Living with Advanced Heart Failure A GUIDE FOR PATIENTS AND FAMILIES Table of contents Contact information...1 Advanced heart failure care at North York General Hospital...2 What
PAH. Salman Bin AbdulAziz University College Of Pharmacy 22/01/35
 Salman Bin AbdulAziz University College Of Pharmacy PAH Therapeutics II PHCL 430 Ahmed A AlAmer PharmD R.W. is a 38-year-old obese woman who presents with increasing symptoms of fatigue and shortness of
Salman Bin AbdulAziz University College Of Pharmacy PAH Therapeutics II PHCL 430 Ahmed A AlAmer PharmD R.W. is a 38-year-old obese woman who presents with increasing symptoms of fatigue and shortness of
Heart Failure Outpatient Clinical Pathway
 Heart Failure Outpatient Clinical Pathway PHASE 1: PHASE 2: PHASE 3: PHASE 4: Initial Consult and Treatment Optimization of Therapy Reassessment and Further Optimization Maintenance I. Provider II. Consults
Heart Failure Outpatient Clinical Pathway PHASE 1: PHASE 2: PHASE 3: PHASE 4: Initial Consult and Treatment Optimization of Therapy Reassessment and Further Optimization Maintenance I. Provider II. Consults
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis
 Population in Connecticut Survey Analysis") Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
Performance Measurement for the Medicare and Medicaid Eligible (MME) Population in Connecticut Survey Analysis Methodology: 8 respondents The measures are incorporated into one of four sections: Highly
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF)
 MANAGEMENT of Atrial Fibrillation (AF)") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
CARDIOLOGIST What does a cardiologist do? A cardiologist is a doctor who specializes in caring for your heart and blood vessel health.
 YOUR TREATMENT TEAM CARDIOLOGIST What does a cardiologist do? A cardiologist is a doctor who specializes in caring for your heart and blood vessel health. To become a cardiologist, a doctor completes additional
YOUR TREATMENT TEAM CARDIOLOGIST What does a cardiologist do? A cardiologist is a doctor who specializes in caring for your heart and blood vessel health. To become a cardiologist, a doctor completes additional
She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary. Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart
 revealed during pregnancy by a New York Heart") Case #1 (year 1992): She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart Association (NYHA) functional class
Case #1 (year 1992): She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart Association (NYHA) functional class
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
Congestive Heart Failure Management Program
 Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
HYPERTROPHIC CARDIOMYOPATHY
 HYPERTROPHIC CARDIOMYOPATHY Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy (HCM) is the second most common form of heart muscle disease, is usually genetically transmitted,
HYPERTROPHIC CARDIOMYOPATHY Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy (HCM) is the second most common form of heart muscle disease, is usually genetically transmitted,
Kidney Disease WHAT IS KIDNEY DISEASE? TESTS TO DETECT OR DIAGNOSE KIDNEY DISEASE TREATMENT STRATEGIES FOR KIDNEY DISEASE
 Kidney Disease WHAT IS KIDNEY DISEASE? Kidney disease is when your kidneys are damaged and not functioning as they should. When kidney disease is not going away it is called chronic kidney disease or CKD.
Kidney Disease WHAT IS KIDNEY DISEASE? Kidney disease is when your kidneys are damaged and not functioning as they should. When kidney disease is not going away it is called chronic kidney disease or CKD.
CorCap Cardiac Support Device Patient Information Booklet
 What is Heart Failure? CorCap Cardiac Support Device Patient Information Booklet Heart failure is a condition in which the heart is unable to pump enough blood to meet the needs of the body. To compensate
What is Heart Failure? CorCap Cardiac Support Device Patient Information Booklet Heart failure is a condition in which the heart is unable to pump enough blood to meet the needs of the body. To compensate
KINDRED HEALTHCARE. Billing & Coding for SNF Physician Visits. KINDRED HEALTHCARE Continue the Care
 KINDRED HEALTHCARE Billing & Coding for SNF Physician Visits KINDRED HEALTHCARE Continue the Care 1 SNF CPT Codes Initial Care Services 99304 99305 99306 Subsequent Care Services 99307 99308 99309 99310
KINDRED HEALTHCARE Billing & Coding for SNF Physician Visits KINDRED HEALTHCARE Continue the Care 1 SNF CPT Codes Initial Care Services 99304 99305 99306 Subsequent Care Services 99307 99308 99309 99310
How To Treat Dilated Cardiomyopathy
 DILATED CARDIOMYOPATHY Dilated or congestive cardiomyopathy (DCM) is diagnosed when the heart is enlarged (dilated) and the pumping chambers contract poorly (usually left side worse than right). A diagram
DILATED CARDIOMYOPATHY Dilated or congestive cardiomyopathy (DCM) is diagnosed when the heart is enlarged (dilated) and the pumping chambers contract poorly (usually left side worse than right). A diagram
Concept Series Paper on Disease Management
 Concept Series Paper on Disease Management Disease management is the concept of reducing health care costs and improving quality of life for individuals with chronic conditions by preventing or minimizing
Concept Series Paper on Disease Management Disease management is the concept of reducing health care costs and improving quality of life for individuals with chronic conditions by preventing or minimizing
Heart failure is estimated to affect 4 to 5 million Americans,
 Team Management of Patients With Heart Failure A Statement for Healthcare Professionals From the Cardiovascular Nursing Council of the American Heart Association Kathleen L. Grady, PhD, RN; Kathleen Dracup,
Team Management of Patients With Heart Failure A Statement for Healthcare Professionals From the Cardiovascular Nursing Council of the American Heart Association Kathleen L. Grady, PhD, RN; Kathleen Dracup,
Congestive Heart Failure
 Healthy People 2010 Conference Health Education on the Internet Welcome Mr. System Administrator Congestive Heart Failure What is congestive heart failure? How does it occur? What are the symptoms? How
Healthy People 2010 Conference Health Education on the Internet Welcome Mr. System Administrator Congestive Heart Failure What is congestive heart failure? How does it occur? What are the symptoms? How
CARDIAC CARE. Giving you every advantage
 CARDIAC CARE Giving you every advantage Getting to the heart of the matter The Cardiovascular Program at Northwest Hospital & Medical Center is dedicated to the management of cardiovascular disease. The
CARDIAC CARE Giving you every advantage Getting to the heart of the matter The Cardiovascular Program at Northwest Hospital & Medical Center is dedicated to the management of cardiovascular disease. The
Berkshire Medical Center Heart Failure Program
 Berkshire Medical Center Heart Failure Program Reducing Readmissions A Multi Disciplinary Approach 1 Project Goals To improve the overall care of Berkshire County Heart Failure Patients Reduce 30 day readmission
Berkshire Medical Center Heart Failure Program Reducing Readmissions A Multi Disciplinary Approach 1 Project Goals To improve the overall care of Berkshire County Heart Failure Patients Reduce 30 day readmission
Educational Goals & Objectives
 Educational Goals & Objectives The Cardiology rotation will provide the resident with an understanding of cardiovascular physiology and its broad systemic manifestations. The resident will have the opportunity
Educational Goals & Objectives The Cardiology rotation will provide the resident with an understanding of cardiovascular physiology and its broad systemic manifestations. The resident will have the opportunity
UW MEDICINE PATIENT EDUCATION. Aortic Stenosis. What is heart valve disease? What is aortic stenosis?
 UW MEDICINE PATIENT EDUCATION Aortic Stenosis Causes, symptoms, diagnosis, and treatment This handout describes aortic stenosis, a narrowing of the aortic valve in your heart. It also explains how this
UW MEDICINE PATIENT EDUCATION Aortic Stenosis Causes, symptoms, diagnosis, and treatment This handout describes aortic stenosis, a narrowing of the aortic valve in your heart. It also explains how this
Heart Failure Clinical Pathway
 Patient & Family Guide 2016 Heart Failure Clinical Pathway www.nshealth.ca Heart Failure Clinical Pathway Your hospital stay will follow a written care plan called a Clinical Pathway. The pathway is a
Patient & Family Guide 2016 Heart Failure Clinical Pathway www.nshealth.ca Heart Failure Clinical Pathway Your hospital stay will follow a written care plan called a Clinical Pathway. The pathway is a
Telehealth and the Homebound Heart Failure Patient
 Telehealth and the Homebound Heart Failure Patient By Karen Malin Garfield, RN, BSN 104 HEART 2010 The Official Guide to a Strong Heart and Healthy Lifestyle PTS Article Heart2010_Suncrest.indd 1 Health
Telehealth and the Homebound Heart Failure Patient By Karen Malin Garfield, RN, BSN 104 HEART 2010 The Official Guide to a Strong Heart and Healthy Lifestyle PTS Article Heart2010_Suncrest.indd 1 Health
4/7/2015. Cardiac Rehabilitation: From the other side of the glass door. Chicago, circa 1999. Objectives. No disclosures, no conflicts
 Cardiac Rehabilitation: From the other side of the glass door No disclosures, no conflicts Charles X. Kim, MD, FACC, ABVM Objectives 1. Illustrate common CV benefits of CV rehab in real world practice.
Cardiac Rehabilitation: From the other side of the glass door No disclosures, no conflicts Charles X. Kim, MD, FACC, ABVM Objectives 1. Illustrate common CV benefits of CV rehab in real world practice.
KIH Cardiac Rehabilitation Program
 KIH Cardiac Rehabilitation Program For any further information Contact: +92-51-2870361-3, 2271154 Feedback@kih.com.pk What is Cardiac Rehabilitation Cardiac rehabilitation describes all measures used to
KIH Cardiac Rehabilitation Program For any further information Contact: +92-51-2870361-3, 2271154 Feedback@kih.com.pk What is Cardiac Rehabilitation Cardiac rehabilitation describes all measures used to
Quiz 4 Arrhythmias summary statistics and question answers
 1 Quiz 4 Arrhythmias summary statistics and question answers The correct answers to questions are indicated by *. All students were awarded 2 points for question #2 due to no appropriate responses for
1 Quiz 4 Arrhythmias summary statistics and question answers The correct answers to questions are indicated by *. All students were awarded 2 points for question #2 due to no appropriate responses for
5. Management of rheumatic heart disease
 5. Management of rheumatic heart disease The fundamental goal in the long-term management of RHD is to prevent ARF recurrences, and therefore, prevent the progression of RHD, and in many cases allow for
5. Management of rheumatic heart disease The fundamental goal in the long-term management of RHD is to prevent ARF recurrences, and therefore, prevent the progression of RHD, and in many cases allow for
Community health care services Alternatives to acute admission & Facilitated discharge options. Directory
 Community health care services Alternatives to acute admission & Facilitated discharge options Directory Introduction The purpose of this directory is to provide primary and secondary health and social
Community health care services Alternatives to acute admission & Facilitated discharge options Directory Introduction The purpose of this directory is to provide primary and secondary health and social
HEART FAILURE ROBERT SOUFER, M.D.
 CHAPTER 14 HEART FAILURE ROBERT SOUFER, M.D. The heart s primary function is to pump blood to all parts of the body, bringing nutrients and oxygen to the tissues and removing waste products. When the body
CHAPTER 14 HEART FAILURE ROBERT SOUFER, M.D. The heart s primary function is to pump blood to all parts of the body, bringing nutrients and oxygen to the tissues and removing waste products. When the body
LIVING WELL WITH HEART FAILURE
 JOHN MUIR HEALTH How Does a Healthy Heart Work? What is Heart Failure (HF)? Summary of How Heart Failure Develops How is Heart Failure Diagnosed? Ejection Fraction and Its Importance Is There a Cure for
JOHN MUIR HEALTH How Does a Healthy Heart Work? What is Heart Failure (HF)? Summary of How Heart Failure Develops How is Heart Failure Diagnosed? Ejection Fraction and Its Importance Is There a Cure for
HEART CENTER. Touching Lives
 HEART CENTER Touching Lives with INNOVATIVE TOOLS and an EXPERIENCED TEAM THE HEART MATTERS If you or someone you love is faced with a heart problem, you want to put your trust in experienced professionals
HEART CENTER Touching Lives with INNOVATIVE TOOLS and an EXPERIENCED TEAM THE HEART MATTERS If you or someone you love is faced with a heart problem, you want to put your trust in experienced professionals
Exchange solutes and water with cells of the body
 Chapter 8 Heart and Blood Vessels Three Types of Blood Vessels Transport Blood Arteries Carry blood away from the heart Transport blood under high pressure Capillaries Exchange solutes and water with cells
Chapter 8 Heart and Blood Vessels Three Types of Blood Vessels Transport Blood Arteries Carry blood away from the heart Transport blood under high pressure Capillaries Exchange solutes and water with cells
Atrial Fibrillation (AF) March, 2013
 March, 2013") Atrial Fibrillation (AF) March, 2013 This handout is meant to help with discussions about the condition, and it is not a complete discussion of AF. We hope it will complement your appointment with one
Atrial Fibrillation (AF) March, 2013 This handout is meant to help with discussions about the condition, and it is not a complete discussion of AF. We hope it will complement your appointment with one
BG MEDICINE. Corporate Presentation February 2013
 BG MEDICINE Corporate Presentation February 2013 CONFIDENTIAL Oct 9, 2007 Forward-Looking Statements This presentation contains forward-looking statements regarding future events or the future financial
BG MEDICINE Corporate Presentation February 2013 CONFIDENTIAL Oct 9, 2007 Forward-Looking Statements This presentation contains forward-looking statements regarding future events or the future financial
Heart Failure: Nursing Assessment and Care
 Heart Failure: Nursing Assessment and Care Objectives 1. Understand the complexities of CHF and the care needs of a patient with CHF. 2. Employ critical components of diseases management into the care
Heart Failure: Nursing Assessment and Care Objectives 1. Understand the complexities of CHF and the care needs of a patient with CHF. 2. Employ critical components of diseases management into the care
Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI)
") Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI) Highlights from Prescribing Information - the link to the full text PI is as follows: http://www.pharma.us.novartis.com/product/pi/pdf/gilenya.pdf
Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI) Highlights from Prescribing Information - the link to the full text PI is as follows: http://www.pharma.us.novartis.com/product/pi/pdf/gilenya.pdf
Population Health Management Program
 Population Health Management Program Program (formerly Disease Management) is dedicated to improving our members health and quality of life. Our Population Health Management Programs aim to improve care
Population Health Management Program Program (formerly Disease Management) is dedicated to improving our members health and quality of life. Our Population Health Management Programs aim to improve care
MINISTRY OF HEALTH AND LONG-TERM CARE Primary Health Care Team FACT SHEET
 Title: Date: April 2008 MINISTRY OF HEALTH AND LONG-TERM CARE Primary Health Care Team FACT SHEET HEART FAILURE MANAGEMENT INCENTIVE Eligible Patient Enrolment Models (PEMs): Family Health Networks (FHNs)
Title: Date: April 2008 MINISTRY OF HEALTH AND LONG-TERM CARE Primary Health Care Team FACT SHEET HEART FAILURE MANAGEMENT INCENTIVE Eligible Patient Enrolment Models (PEMs): Family Health Networks (FHNs)
Overview. Geriatric Overview. Chapter 26. Geriatrics 9/11/2012
 Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
1p36 and the Heart. John Lynn Jefferies, MD, MPH, FACC, FAHA
 1p36 and the Heart John Lynn Jefferies, MD, MPH, FACC, FAHA Director, Advanced Heart Failure and Cardiomyopathy Services Associate Professor, Pediatric Cardiology and Adult Cardiovascular Diseases Associate
1p36 and the Heart John Lynn Jefferies, MD, MPH, FACC, FAHA Director, Advanced Heart Failure and Cardiomyopathy Services Associate Professor, Pediatric Cardiology and Adult Cardiovascular Diseases Associate
getemed Medizin- und Informationstechnik AG
 getemed Medizin- und Informationstechnik AG Oderstraße 77 14513 Teltow Germany Ambulatory Monitoring of Physiological Parameters Robert Downes ehealth Conference, Berlin April 19, 2007 Contents Introduction
getemed Medizin- und Informationstechnik AG Oderstraße 77 14513 Teltow Germany Ambulatory Monitoring of Physiological Parameters Robert Downes ehealth Conference, Berlin April 19, 2007 Contents Introduction
The science of medicine. The compassion to heal.
 A PATIENT S GUIDE TO ELECTROPHYSIOLOGY STUDIES OF THE HEART The science of medicine. The compassion to heal. This teaching booklet is designed to introduce you to electrophysiology studies of the heart.
A PATIENT S GUIDE TO ELECTROPHYSIOLOGY STUDIES OF THE HEART The science of medicine. The compassion to heal. This teaching booklet is designed to introduce you to electrophysiology studies of the heart.
IN-HOME QUALITY IMPROVEMENT BEST PRACTICE: PHYSICIAN RELATIONSHIPS NURSE TRACK
 IN-HOME QUALITY IMPROVEMENT BEST PRACTICE: PHYSICIAN RELATIONSHIPS NURSE TRACK Best Practice Intervention Packages were designed for use by any In-Home Provider Agency to support reducing avoidable hospitalizations
IN-HOME QUALITY IMPROVEMENT BEST PRACTICE: PHYSICIAN RELATIONSHIPS NURSE TRACK Best Practice Intervention Packages were designed for use by any In-Home Provider Agency to support reducing avoidable hospitalizations
2013 ACO Quality Measures
 ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
Appendix L: HQO Year 1 Implementation Priorities
 Appendix L: HQO Year 1 Implementation Priorities Chronic Obstructive Pulmonary Disease (Source: COPD Chairs) Non-Invasive Positive Pressure Ventilation Early Ambulation If possible, seek patient preferences
Appendix L: HQO Year 1 Implementation Priorities Chronic Obstructive Pulmonary Disease (Source: COPD Chairs) Non-Invasive Positive Pressure Ventilation Early Ambulation If possible, seek patient preferences
Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions?
 Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions? AFSHAN HAMEED, MD, FACOG, FACC Associate Clinical Professor Maternal Fetal Medicine and Cardiology University
Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions? AFSHAN HAMEED, MD, FACOG, FACC Associate Clinical Professor Maternal Fetal Medicine and Cardiology University
Automatic External Defibrillators
 Last Review Date: May 27, 2016 Number: MG.MM.DM.10dC2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: May 27, 2016 Number: MG.MM.DM.10dC2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
PULMONARY HYPERTENSION. Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana
 PULMONARY HYPERTENSION Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana What is Pulmonary Hypertension? What is normal? Pulmonary artery systolic pressure
PULMONARY HYPERTENSION Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana What is Pulmonary Hypertension? What is normal? Pulmonary artery systolic pressure
Christopher M. Wright, MD, MBA Pioneer Cardiovascular Consultants Tempe, Arizona
 Christopher M. Wright, MD, MBA Pioneer Cardiovascular Consultants Tempe, Arizona Areas to be covered Historical, current, and future treatments for various cardiovascular disease: Atherosclerosis (Coronary
Christopher M. Wright, MD, MBA Pioneer Cardiovascular Consultants Tempe, Arizona Areas to be covered Historical, current, and future treatments for various cardiovascular disease: Atherosclerosis (Coronary
Geriatric Cardiology: Challenges and Strategies
 Geriatric Cardiology: Challenges and Strategies No financial disclosures Geriatrics -- No Specific Age 'you know it when you see it' Functional Status Polypharmacy Impaired Renal Function Diagnostic Testing:
Geriatric Cardiology: Challenges and Strategies No financial disclosures Geriatrics -- No Specific Age 'you know it when you see it' Functional Status Polypharmacy Impaired Renal Function Diagnostic Testing:
ADULT HYPERTENSION PROTOCOL STANFORD COORDINATED CARE
 I. PURPOSE To establish guidelines for the monitoring of antihypertensive therapy in adult patients and to define the roles and responsibilities of the collaborating clinical pharmacist and pharmacy resident.
I. PURPOSE To establish guidelines for the monitoring of antihypertensive therapy in adult patients and to define the roles and responsibilities of the collaborating clinical pharmacist and pharmacy resident.
Atrial Fibrillation The High Risk Obese Patient
 Atrial Fibrillation The High Risk Obese Patient Frederick Schaller, D.O.,F.A.C.O.I. Professor and Vice Dean Touro University Nevada A 56 year old male with a history of hypertension and chronic stable
Atrial Fibrillation The High Risk Obese Patient Frederick Schaller, D.O.,F.A.C.O.I. Professor and Vice Dean Touro University Nevada A 56 year old male with a history of hypertension and chronic stable
HEART HEALTH WEEK 3 SUPPLEMENT. A Beginner s Guide to Cardiovascular Disease HEART FAILURE. Relatively mild, symptoms with intense exercise
 WEEK 3 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease HEART FAILURE Heart failure can be defined as the failing (insufficiency) of the heart as a mechanical pump due to either acute
WEEK 3 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease HEART FAILURE Heart failure can be defined as the failing (insufficiency) of the heart as a mechanical pump due to either acute
The CCU is an environment that requires a high level of comfort with electronic monitoring and support equipment including electrocardiograms,
 Cardiovascular Nursing: Leadership in the Fight Against America s Number One Killer Written and prepared by the Preventative Cardiovascular Nurses Association A ccording to the American Heart Association
Cardiovascular Nursing: Leadership in the Fight Against America s Number One Killer Written and prepared by the Preventative Cardiovascular Nurses Association A ccording to the American Heart Association
Cardiology Fact Sheet. ACVIM Fact Sheet: Myxomatous Mitral Valve Degeneration
 Cardiology Fact Sheet ACVIM Fact Sheet: Myxomatous Mitral Valve Degeneration Overview Myxomatous mitral valve degeneration (MMVD) is the most common acquired type of heart disease and new murmurs in older
Cardiology Fact Sheet ACVIM Fact Sheet: Myxomatous Mitral Valve Degeneration Overview Myxomatous mitral valve degeneration (MMVD) is the most common acquired type of heart disease and new murmurs in older
Pathophysiology: Heart Failure. Objectives. Heart Failure. Mat Maurer, MD Associate Professor of Clinical Medicine
 Pathophysiology: Heart Failure Mat Maurer, MD Associate Professor of Clinical Medicine Objectives At the conclusion of this seminar, learners will be able to: 1. Define heart failure as a clinical syndrome
Pathophysiology: Heart Failure Mat Maurer, MD Associate Professor of Clinical Medicine Objectives At the conclusion of this seminar, learners will be able to: 1. Define heart failure as a clinical syndrome
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY. Guidelines for Use of Intravenous Isoproterenol
 ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Isoproterenol Major Indications Status Asthmaticus As a last resort for
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Isoproterenol Major Indications Status Asthmaticus As a last resort for
Heart Disease: Diagnosis & Treatment
 How I Treat Cardiology Peer Reviewed Heart Disease: Diagnosis & Treatment Amara Estrada, DVM, DACVIM (Cardiology) University of Florida Background Clinical heart disease is the stage of disease when a
How I Treat Cardiology Peer Reviewed Heart Disease: Diagnosis & Treatment Amara Estrada, DVM, DACVIM (Cardiology) University of Florida Background Clinical heart disease is the stage of disease when a
HISTORY. Questions: 1. What diagnosis is suggested by this history? 2. How do you explain her symptoms during pregnancy?
 HISTORY 33-year-old woman. CHIEF COMPLAINT: months duration. Dyspnea, fatigue and nocturnal wheezing of six PRESENT ILLNESS: At ages 5 and 9, she had migratory arthritis. At age 29, in the third trimester
HISTORY 33-year-old woman. CHIEF COMPLAINT: months duration. Dyspnea, fatigue and nocturnal wheezing of six PRESENT ILLNESS: At ages 5 and 9, she had migratory arthritis. At age 29, in the third trimester
How should we treat atrial fibrillation in heart failure
 Advances in Cardiac Arrhhythmias and Great Innovations in Cardiology Torino, 23/24 Ottobre 2015 How should we treat atrial fibrillation in heart failure Matteo Anselmino Dipartimento Scienze Mediche Città
Advances in Cardiac Arrhhythmias and Great Innovations in Cardiology Torino, 23/24 Ottobre 2015 How should we treat atrial fibrillation in heart failure Matteo Anselmino Dipartimento Scienze Mediche Città
CARDIO/PULMONARY MEDICINE FOR PRIMARY CARE. Las Vegas, Nevada Bellagio March 4 6, 2016. Participating Faculty
 CARDIO/PULMONARY MEDICINE FOR PRIMARY CARE Las Vegas, Nevada Bellagio March 4 6, 2016 Participating Faculty Friday, March 4th: 7:30 am - 8:00 am Registration and Hot Breakfast 8:00 am - 9:00 am Pulmonary
CARDIO/PULMONARY MEDICINE FOR PRIMARY CARE Las Vegas, Nevada Bellagio March 4 6, 2016 Participating Faculty Friday, March 4th: 7:30 am - 8:00 am Registration and Hot Breakfast 8:00 am - 9:00 am Pulmonary
Acquired, Drug-Induced Long QT Syndrome
 Acquired, Drug-Induced Long QT Syndrome A Guide for Patients and Health Care Providers Sudden Arrhythmia Death Syndromes (SADS) Foundation 508 E. South Temple, Suite 202 Salt Lake City, Utah 84102 800-STOP
Acquired, Drug-Induced Long QT Syndrome A Guide for Patients and Health Care Providers Sudden Arrhythmia Death Syndromes (SADS) Foundation 508 E. South Temple, Suite 202 Salt Lake City, Utah 84102 800-STOP
TACO vs. TRALI: Recognition, Differentiation, and Investigation of Pulmonary Transfusion Reactions
 TACO vs. TRALI: Recognition, Differentiation, and Investigation of Pulmonary Transfusion Reactions Shealynn Harris, M.D. Assistant Medical Director American Red Cross Blood Services Southern Region Case
TACO vs. TRALI: Recognition, Differentiation, and Investigation of Pulmonary Transfusion Reactions Shealynn Harris, M.D. Assistant Medical Director American Red Cross Blood Services Southern Region Case
Remote Monitoring of Cardiac Implantable Electrical Devices (CIEDs)
") Remote Monitoring of Cardiac Implantable Electrical Devices (CIEDs) Changing the face of enhanced self-management and improved coordinated healthcare K Fan, CKC Tsui, KL Au, RTC Ng, CYS Chung, KW Lai,
Remote Monitoring of Cardiac Implantable Electrical Devices (CIEDs) Changing the face of enhanced self-management and improved coordinated healthcare K Fan, CKC Tsui, KL Au, RTC Ng, CYS Chung, KW Lai,
Cardiac Rehabilitation at AUBMC
 Cardiac Rehabilitation at AUBMC Clinical Protocols and The Role of The Advanced Practice Nurse Presentation by: Mohamad Issa, MSN, BSN, BC- RN, AUBMC CCU OUTLINE Background on cardiovascular diseases History
Cardiac Rehabilitation at AUBMC Clinical Protocols and The Role of The Advanced Practice Nurse Presentation by: Mohamad Issa, MSN, BSN, BC- RN, AUBMC CCU OUTLINE Background on cardiovascular diseases History
MISSING DATA ANALYSIS AMONG PATIENTS IN THE PINNACLE REGISTRY
 MISSING DATA ANALYSIS AMONG PATIENTS IN THE PINNACLE REGISTRY In order to improve the efficiency of PINNACLE Registry data analytics, a missing data analysis has been conducted on PINNACLE Registry data
MISSING DATA ANALYSIS AMONG PATIENTS IN THE PINNACLE REGISTRY In order to improve the efficiency of PINNACLE Registry data analytics, a missing data analysis has been conducted on PINNACLE Registry data
3/2/2010 Post CABG R h e bili a i tat on Ahmed Elkerdany Professor o f oof C ardiac Cardiac Surgery Ain Shams University 1
 Post CABG Rehabilitation i Ahmed Elkerdany Professor of Cardiac Surgery Ain Shams University 1 Definition Cardiac rehabilitation services are comprehensive, long-term programs involving : medical evaluation.
Post CABG Rehabilitation i Ahmed Elkerdany Professor of Cardiac Surgery Ain Shams University 1 Definition Cardiac rehabilitation services are comprehensive, long-term programs involving : medical evaluation.
Atrial Fibrillation An update on diagnosis and management
 Dr Arvind Vasudeva Consultant Cardiologist Atrial Fibrillation An update on diagnosis and management Atrial fibrillation (AF) remains the commonest disturbance of cardiac rhythm seen in clinical practice.
Dr Arvind Vasudeva Consultant Cardiologist Atrial Fibrillation An update on diagnosis and management Atrial fibrillation (AF) remains the commonest disturbance of cardiac rhythm seen in clinical practice.
Multidisciplinary care for people with chronic heart failure. Principles and recommendations for best practice
 Multidisciplinary care for people with chronic heart failure Principles and recommendations for best practice 2010 National Heart Foundation of Australia. All rights reserved. This work is copyright. No
Multidisciplinary care for people with chronic heart failure Principles and recommendations for best practice 2010 National Heart Foundation of Australia. All rights reserved. This work is copyright. No
ACLS PHARMACOLOGY 2011 Guidelines
 ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
HEART & VASCULAR SERVICES. Heart & Vascular Services www.mhsystem.org
 HEART & VASCULAR SERVICES Heart & Vascular Services www.mhsystem.org Heart Services Testing Before Your Procedure If you are scheduled for a procedure in the catheterization lab, there will be blood work
HEART & VASCULAR SERVICES Heart & Vascular Services www.mhsystem.org Heart Services Testing Before Your Procedure If you are scheduled for a procedure in the catheterization lab, there will be blood work
What Are Arrhythmias?
 What Are Arrhythmias? Many people have questions about what the word arrhythmia means, and arrhythmias can be a difficult subject to understand. The text below should give you a better understanding of
What Are Arrhythmias? Many people have questions about what the word arrhythmia means, and arrhythmias can be a difficult subject to understand. The text below should give you a better understanding of
National Learning Objectives for COPD Educators
 National Learning Objectives for COPD Educators National Learning Objectives for COPD Educators The COPD Educator will be able to achieve the following objectives. Performance objectives, denoted by the
National Learning Objectives for COPD Educators National Learning Objectives for COPD Educators The COPD Educator will be able to achieve the following objectives. Performance objectives, denoted by the
Cardiology ICD-10-CM Coding Tip Sheet Overview of Key Chapter Updates for Cardiology
 Cardiology ICD-10-CM Coding Tip Sheet Overview of Key Chapter Updates for Cardiology Chapter 4: Endocrine, Nutritional, and Metabolic Diseases (E00-E89) The diabetes mellitus codes are combination codes
Cardiology ICD-10-CM Coding Tip Sheet Overview of Key Chapter Updates for Cardiology Chapter 4: Endocrine, Nutritional, and Metabolic Diseases (E00-E89) The diabetes mellitus codes are combination codes