Terapia del paziente non candidato a trapianto
|
|
|
- Jocelin Quinn
- 8 years ago
- Views:
Transcription
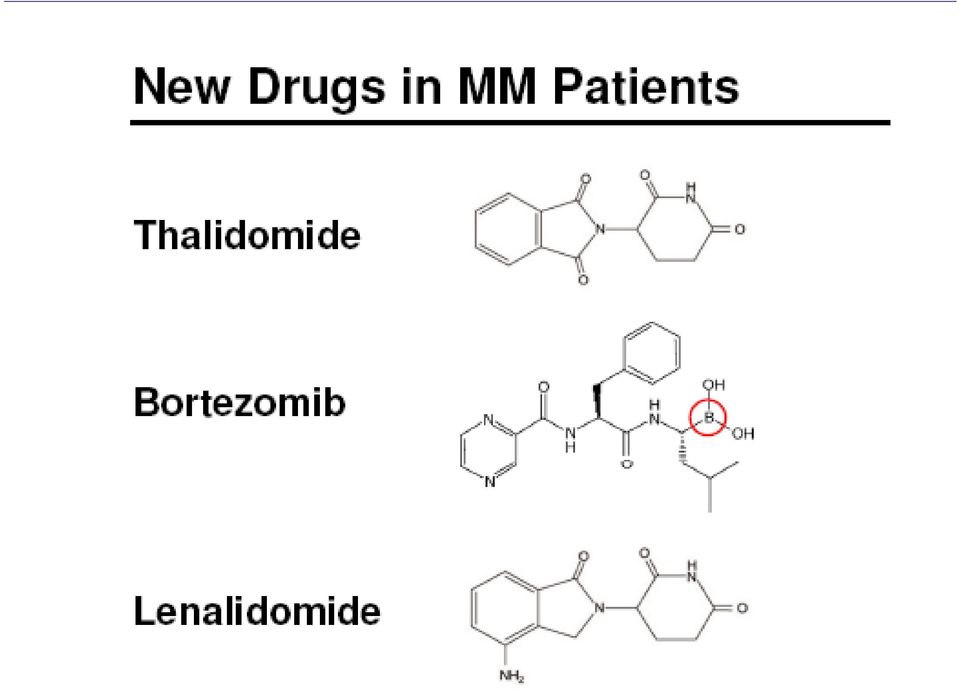
1 Gammapatie monoclonali e mieloma multiplo Varese, 14 novembre 2011 Terapia del paziente non candidato a trapianto Luca Baldini UO Ematologia 1-CTMO 1 Università degli studi di Milano Fondazione IRCCS Cà Granda OM Policlinico, Milano

2 Elderly patients with MM MM is predominantly a disease of the elderly In the US, two-thirds of pts is 65 years old ASL TORINO: people Median age at diagnosis: 69.4 years years 36% 31% years 33% years Regione Piemonte, Assessorato Sanità 2006,15

3 Major milestones in Multiple Myeloma Therapy Other CCT regimens = MP ASCT Single vs double ASCT Bortezomib Melph-Pdn HDMelphalan Thal Lenalidomide Quality of response PF survival Overall survival LB UNIMI

4
5 LESSON FROM NEW AGENTS IN MM Role of CR New toxicities Different subsets of elderly pts

6 LESSON FROM NEW AGENTS IN MM Role of CR Different subsets of elderly pts New toxicities

7 What disease response is best? Depth of response Time to progression Treatment initiation MR PR VGPR ncr CR scr icr mcr Time Depth of response is related to TTP Niesvizky et al. Br J Haematol 2008; 143(1): 46-53; Harousseau et al. Blood 2009; 114(15): Chanan-Khan et al. J Clin Oncol 2010; 28(15):
: 46-53; Harousseau et al.")
8 CR correlates with survival International MyelomaWorking Group criteria (2009) Retrospective analysis of three randomized studies from GIMEMA and HOVON (n=1175; median age: 72 yrs) MP (n=332), MPT (n=332), VMP (n=257), or VMPT-VT VT (n=254) CR CR (195) VGPR (212) VGPR PR PFS PR (397) OS p<0.001 p<0.001 Median follow-up: 29 months Gay et al. Blood 2011; 117(11):
 OS p<0.001 p<0.001 Median follow-up: 29 months Gay et al.")
9 CR associata a miglior PFS e OS anche nei pazienti >75 anni CR VGPR PR 3y PFS 79% 24% 23% 3y OS 88% 65% 57% 3y PFS 3y OS Gay et al. ASH Gay et 2010 al. Blood (Abs )

10 La miglior qualità della risposta è associata a miglior QoL Progressive disease Stable disease Partial response Complete response Study details n=292 newly diagnosed MM Prospective comparison: Continuous prednisone + VMCP Intermittent prednisone + VMCP Collection of quality of life data using EORTC QLQ-C Quality of life score 100 Ludwig et al. IMW 2007; (Abs 1103)

11 LESSON FROM NEW AGENTS IN MM Role of CR New toxicities Different subsets of elderly pts

12 Summary Table of Selected Therapy-Related Adverse Effects Peripheral Neuropathy Thalidomide [1] Lenalidomide [2] Bortezomib [3] (50%): grade 3-4: 5-8%; may be irreversible DVT More with dex (4-15%) More with dex (7%) Myelosuppression Hypotension Neutropenia Neutropenia (21%), thrombocytopenia (10%) anemia (20-30%); grade 3-4: 4-8%; painful, usuallyreversible Thrombocytopenia (20%) Fatigue, weakness (70%) (38%) Sedation Rash (30%) GI Disturbance Constipation (50%) Constipation (39%) diarrhea (29%) Nausea and vomiting, diarrhea (8%) 1. Thalidomide [package insert]. 2. Lenalidomide [package insert]. 3. Bortezomib [package insert]. 4. Orlowski RZ, et al. J Clin Oncol. 2007;25: L. Baldini -UniMI
 1. Thalidomide [package insert]. 2. Lenalidomide [package insert]. 3. Bortezomib [package insert]. 4. Orlowski RZ, et al. J Clin Oncol. 2007;25:3892-3901.")
13 LESSON FROM NEW AGENTS IN MM Role of CR New toxicities Different subsets of elderly pts

14 10-Yr Relative Survival (%) Improvements in Survival by Age Period Estimates of 10-Yr Survival by Major Age Groups in Defined Calendar Periods Age, yrs Years < Improvements in survival for elderly patients expected with longer follow-up of ongoing trials Brenner H, et al. Blood. 2008;111:

15
16 Management of elderly patients The NCCN guidelines on treating older adults with cancer recommend using Comprehensive Geriatric Assesment tools to asses the patient s likely tolerance of treatment by formally assessing: - comorbidities, - functional status - geriatric syndromes - polypharmacy,nutrition - socioeconomic status and personal preferences Toxicity Comorbidities Depth of response Niesvizky R et al. Oncology 24:3; March 2010

17 Len + High- or Low-Dose Dex (E4A03 trial) Low-dose Dex = 40 mg/day PO, on Days 1, 8, 15, 22 High-dose Dex = 40 mg/day PO, on Days 1-4, 9-12, High Dose Low Dose P Value Best overall response, % VGPR, % OVERALL SURVIVAL Rajkumar SV, et al. Lancet Oncol. 2010;11:29-37.

18

19 Nel paziente > 75 aa,, il raggiungimento della miglior risposta possibile è auspicabile, ma altri parametri devono essere considerati TTNT (time to next treatment): è il tempo dall inizio di un trattamento all inizio del successivo TFI (treatment free interval): è il tempo dalla fine di un trattamento all inizio del successivo QoL TWiST (time without symptoms disease or toxicity related) LB UNIMI
")

20 Terapia con nuovi agenti a dose ridotta o terapia convenzionale Terapia con nuovi agenti a dose piena

21 Expanding treatment options in front-line therapy for elderly myeloma pts MP/CTX + novel agents MPT (GIMEMA, IFM, NMSG, HOVON, Turkish study group) CTD (MRC Myeloma IX) VMP (VISTA, PETHEMA, GIMEMA) VMPT-VT (GIMEMA) VMP-VT/VP (PETHEMA) MPR-R (GIMEMA) Dex + novel agents Bortezomib/Dex-based (UPFRONT study) Thal/Dex-based (ECOG, Celgene 003, CEMSG, MRC Myeloma IX) Len/Dex (ECOG, SWOG others) Len/Bortezomib/Dex (DFCI)
22 CONVENTIONAL THERAPY MP, Dex,, VAD or VAD-like regimens ORR ~ 50% CR < 5% Median DFS: 18 mos Median OS: 3 yrs LB MM
23 Farmaci concessi dal SSN in Italia per la terapia di prima linea del paziente non ASCT candidabile MP, HCTX, VAD MP+Thalidomide (MPT) Frontline therapy in elderly pts (FDA, EMEA,AIFA march 2009) MP+Bortezomib (MPV) Frontline therapy in elderly pts (FDA and EMEA 2008, AIFA july 2009) L. Baldini -UniMI
24 ALKILATING + NOVEL AGENTS without maintenance
25 MP vs MPT Studies Patient Characteristics and MPT Regimens GIMEMA [1,2] IFM [3] IFM [4] NMSG [5] HOVON [6] Patients, n (MPT) 331 (167) 447 (125) 232 (113) 362 (182) 301 (152) Age, yrs Median (mean) 72 Range N/A WHO grade 3/4, % MPT regimen Cycles, n Until plateau Until plateau M dosing 4 mg/m 2 Days mg/kg Days mg/kg Days mg/kg Days mg/kg Days 1-5 Thal dosing, mg/day 100 Up to Up to Maintenance Palumbo A, et al. Lancet. 2006; 367: Palumbo A, et al. Blood. 2008;112: Facon T, et al. Lancet. 2007;370: Hulin C, et al. JCO 2009, 27: Waage A, et al. Blood 2010, 116: Wijermans P, et al. JCO 2010, 28:
26 Summary of MPT phase III trials in the upfront setting Regimen GIMEMA Thal/MP MP IFM Thal/MP MP MEL 100 n. Pts (median FU) 129 (18) 126 (15) ( 1 5 ) (51) CR (%) CR+VGPR (%) PFS (mos) OS (mos) Reference Palumbo et al. Blood 2008; 112: Facon, et al. Lancet 2007; 370: IFM Thal/MP MP NMSG Thal/MP MP (47) (42) Hulin, et al. JCO 2009; 27: Waage A et al. Blood (9): HOVON Thal/MP MP 165 (nr) 168 (nr) Wijermans P, et al. JCO 2010, 28:
27 Toxicities of THAL combined with melphalan in phase III trials Toxicity grade 3-4 (%) MPT (n=167) Palumbo et al. (GIMEMA) MPT (n=124) Facon et al (IFM) MPT (n=113) Hulin et al. (IFM) - Infections n./a. - Neutropenia DVT Neuropathy Thal Discontinuation / Treatment withdrawal (%) 46.5* 45* 53* * Due to adverse events LB UNIMI
28 Valutazione del rischio trombotico in pazienti trattati con talidomide Fattori di rischio individuali Fattori di rischio associati alla terapia Pregressa trombosi Trombofilia ereditaria Obesità CVC Comorbidità (diabete, infezioni..) Interventi chirurgici Desametasone ad alte dosi Doxorubicina Polichemioterapia Fattori di rischio associati al mieloma Trombosi nel MM: ~5% LB UNIMI
29 Aspirina Profilassi antitrombotica in pazienti trattati con IMiD Se 1 1 FR individuali o associati al mieloma Eparina a basso peso molecolare Se 2 2 FR individuali o associati al mieloma Se talidomide + HD dexa, doxorubicina, poli-ct Palumbo et al, Leukemia 2008; Palumbo et al, EHA 2008 LB UNIMI
30
31 CTD vs MP : MRC Myeloma IX Phase III, Study in Elderly Patients with Newly Diagnosed MM RANDOMIZATION 849 pts (median age 73 yrs; ; 57-89) 100 P<.001 CTD CTX 500 mg po,, days 1,8,and 15; THAL mg/day; Dex 20 mg/day days 1-41 and q 4 wk RANDOMIZATION MP Response, % CTD (n = 426) MP (n = 423) PR VGPR CR Thal +Thal 100 mg/day No differences in terms of OS and PFS (36 and 12 mos) Correlation with quality of response and cytogenetic profile) VTE 16% vs 4.5% Morgan et al. Blood, 2011
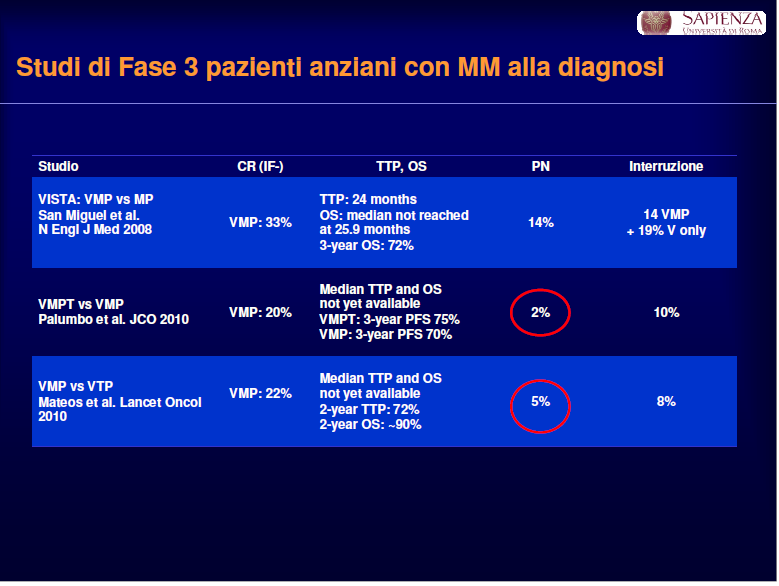
32 VISTA - Velcade as Initial Standard Therapy in newly diagnose multiple myeloma (> 65 yrs or not transplant eligible): Assessment with melphalan and prednisone 54 weeks 682 pts Bort 1.3 mg/m 2 IV on Days 1, 4, 8, 11, 22, 25, 29, 32 during first four 6-week cycles + MP* (n = 344) Bort 1.3 mg/m 2 IV on Days 1, 8, 22, 29 for five 6-week cycles + MP* (n = 344) Melphalan (9 mg/sm) and Prednisone (60 mg/sm) on days 1-4 for nine 6-week cycles (n = 338) DOSE/INTENSITY OF BORTEZOMIB: 52 doses/54 wks Primary end point: TTP San Miguel J, NEJM 2008; 359:906 LB Unimi
33 VISTA: response rates and TTP Responses Time to progression p < % PR VGPR CR 39% Event-free patients (%) Median TTP MPV: 24 months MP: 16.6 months HR 0.48; p < Time (months) San Miguel JF, et al. N Engl J Med. 2008;359:
34 VISTA: overall survival 3-year OS rates: MPV 68.5%, MP 54.0% Surviving patients (%) Median follow-up: 36.7 months Median OS MPV: not reached (109 deaths) MP: 43.1 months (148 deaths) HR (95% CI ); p = Time (months) Mateos MV, et al. J Clin Oncol. 2010;28:
35 VISTA - Adverse events VMP (N=340) MP (N=337) AE, % Grade 3 Grade 4 Grade 3 Grade 4 Neutropenia Thrombocytopenia Anemia GI <1 Peripheral sensory neuropathy 13 <1 0 0 Fatigue Asthenia 6 <1 3 0 Pneumonia Herpes zoster Overall rate of peripheral sensory neuropathy with VMP was 44%, including 14% grade 1, 17% grade 2 At data cut-off 74% of peripheral neuropathy (PN) events had resolved to baseline (56%) or decreased by at least one toxicity grade (18%) in a median of 2 months Herpes zoster was more frequent with VMP (13% vs 4%); rate with VMP only 3% among patients receiving antiviral prophylaxis Rate of DVT was low and similar with VMP vs MP (1% vs 2%) LB UNIMI
36 Raccomandazioni per la gestione della neuropatia da Bortezomib Segni e sintomi di PN Grado 1 (parestesie e/o perdita dei riflessi senza dolore nè deficit funzionali) Azione Se bisettimanale passare a monosettimanale; se monosettimanale ridurre di un livello Grado 2 (non interferisce con lo svolgimento delle normali attività quotidiane) Grado 3 e 4 (disabilitante) Se bisettimanale passare a monosettimanale; se monosettimanale ridurre di un livello o sospendere temporaneamente. Se migliora riprendere monosettimanale con dose ridotta a 1 mg/m 2 Sospendere definitivamente La presenza di dolore neuropatico innalza di 1 grado Riduzione dose livello 1 =: 1 mg/sm; livello 2= 0.7 mg/sm Delforge et al, Lancet Oncol 2010

37 Bortezomib planned dose: 67.6 mg/sm sm; administreded dose: 38.5 mg/sm Bortezomib planned dose: 36.4 mg/sm sm; administreded dose: na Bortezomib planned dose: 46.8 mg/sm sm; administreded dose: 40 mg/smn
38
39 MM-015: phase 3 trial of MPR vs MP for longterm control in newly diagnosed MM R A N D O M I Z A T I O N 51 centres in Europe, Australia, and Israel (N = 459) MPR-R Melphalan 0.18 mg/kg, days 1 4 Prednisone 2 mg/kg, days 1 4 Lenalidomide 10 mg/day p.o., days 1 21 MPR Cycles (28-day) 1 9 Melphalan 0.18 mg/kg, days 1 4 Prednisone 2 mg/kg, days 1 4 Lenalidomide 10 mg/day p.o., days 1 21 MPSecondary comparison Melphalan MPR-R 0.18 vsmg/kg, MPR days 1 4 Prednisone Addition of 2 MPR mg/kg, arm days per 1 4 PlaceboEMEA days advice 1 21 Cycles 10+ Lenalidomide continued 10 mg/day days 1 21 Placebo Placebo P R O G R E S S I O N Len (25 mg/day) ± Dex Double-blind treatment phase Stratification by age ( 75 vs > 75 years) and ISS stage (1, 2, or 3) Open-label extension and follow-up phase Palumbo A, et al. Blood. 2010;116:[abstract 622]. Updated data presented at ASH 2010.
40 MM-015: response rates significantly higher with MPR vs MP Best overall response* MPR (n = 153) ORR ( PR) (%) CR ** (%) 13 4 VGPR*** (%) Median time to first response (months) 2 3 MP (n = 154) *As measured using EBMT criteria. 1 **Immunofixation negative with or without bone marrow confirmation. ***VGPR: > 90% reduction in M protein. Palumbo A, et al. Blood. 2010;116:[abstract 622]. 1. Bladé J, et al. Br J Haematol. 1998;102:
41 MM-015: MPR vs MP progressionfree survival 100 Patients (%) MPR MP Median PFS 14 months 13 months Time (months) Median follow-up 25 months p = *Analysis based on data up to May Palumbo A, et al. Blood. 2010;116:[abstract 622]. Updated data presented at ASH 2010.
42 Treatment Initial 9 cycles MPR MP Discontinuation rate (%) years of age > 75 years of age Cumulative dose intensity (%) years of age > 75 years of age Discontinuation due to AEs or withdrawal of consent Cumulative dose intensity of melphalan and lenalidomide/placebo
43 DEX + NOVEL AGENTS
44 Lenalidomide + High (RD) vs Low-Dose Dex (Rd) in Elderly Patients with Newly Diagnosed MM: ECOG (E4A03 phase III study) Four 28-day cycles 445 pts Median age 66 yrs (51-88) RD Arm A Lenalidomide 25 mg/day orally on Days Dexamethasone 40 mg orally on Days 1-4, 9-12, (Dex tot 480) (n = 223) Rd Arm B Lenalidomide 25 mg/day orally on Days Dexamethasone 40 mg orally on Days 1, 8, 15, 22 (Dex tot 160) (n = 222) CR/PR < PR ASCT or RD/Rd Rd or no further therapy CR/PR 4 cycles thal + dex LB MM UniMi
45 Phase III ECOG Trial: RD vs Rd After 4 induction cycles: VGPR 51% with RD vs 40% with Rd PR 81% with RD vs 70% with Rd PFS: months (P P =.08. log-rank; P =.04 Pepe-Fleming) OS: 75% at 3 years Although initial findings suggested better OS with Rd; OS at 3 years identical for both treatment arms (P P =.46. log-rank rank; ; P =.01 Pepe-Fleming) Rajkumar SV, et al. Lancet Oncol. 2009
46 Novel agents in combination as primary treatment (without maintenance) Study n Median age, years VGPR, % PR, % PFS or TTP (mos) Median MPT 1 IFM MPT 2,3 MPT vs MP MPV 4,5 VISTA TTP: 24 MPR 6 MPR Rd 7 ECOG-E4A03 65 years CTDa 8,9 MRC Myeloma IX NA Facon T, et al. Lancet. 2007;370: Palumbo A, et al. Lancet. 2006;367: Palumbo A, et al. Blood. 2008;112: San Miguel JF, et al. N Engl J Med. 2008;359: Mateos MV, et al. Blood. 2009;114:[abstract 3859]. 6. Palumbo A, et al. Blood. 2009;114:[abstract 613]. 7. Rajkumar SV, et al. Lancet Oncol Morgan GJ, et al. Blood. 2007;110:[abstract 3593]. 9. Owen RG, et al. Presented at IMW 2009 [abstract 547].
47 Outcomes from randomized phase 3 trials in elderly NDMM Regimen Median age CR rate % Median PS Median OS, mos Stop rate, % MPT (5 studies) VMP (VISTA) na nr 34 VMP (Palumbo( Palumbo) nr 17 Rd (Rajkumar) nr 19 VMPT (Palumbo) nr nr 23 MPR-R (Palumbo) nr nr 13 CTDa (Morgan) NA
48 Novel agents as primary treatment: safety Grade 3 or 4 adverse events, % IFM MPT VISTA MPV GIMEMA MPR ECOG Rd Neutropenia Thrombocytopenia Anaemia Neuropathy DVT Infection Herpes zoster NR NR Moreau P, et al. Blood Rev. 2008;22: Rajkumar SV, et al. Lancet Oncol. [Epub ahead of print 2009 Oct 21.]
49 OPEN QUESTIONS ABOUT NEW AGENTS IN MM Role of CR Different subsets of elderly pts New toxicities Fixed doses or continuos therapy Identification of the best synergistic effect New-new agents
50 Approach to MM cells control Progression free Survival MM cells TARGET OF EFFICACY Improvement Citostatici convenzionali of quality of response Improvement or ofifn/dex OS Continuous terapy (continuous ther. vs ther. at relapse) Nuovi farmaci ± CT Overall Survival time
51 Phase III Study of Bortezomib, Melphalan, Prednisone (VMP) ± Thalidomide (VMPT) in elderly patients with Newly Diagnosed MM: GIMEMA Trial Newly diagnosed symptomatic MM 65 yr or <65 yr and not transplanteligible (N=393) R A N D O M I Z A T I O N VMP Bortezomib 1.3 mg/m2 IV days 1,8,15,22* Melphalan 9 mg/m2 and prednisone 60 mg/m2 days 1 4 VMPT Bortezomib 1.3 mg/m2 IV days 1,8,15,22* Melphalan 9 mg/m2 and prednisone 60 mg/m2 days 1 4 Thalidomide 50 mg/d continuously NO MAINTENANCE MAINTENANCE Bortezomib 1.3 mg/m2 IV days 1,15 Thalidomide 50 mg/day 9 5-wk cycles in both arms Until relapse *61 VMP patients and 70 VMPT patients were treated with biweekly infusions of bortezomib Palumbo A, et al. J Clin Oncol. 2010;28:
52 GIMEMA (MPVT-VT vs MPV): efficacy Response MPVT-VT (n = 250) Patients (%) MPV (n = 253) p value CR < VGPR PR OS at 3 years Palumbo A, et al. J Clin Oncol. 2010;28:
53 GIMEMA (MPVT-VT vs MPV): PFS and TTNT Progression-free survival Median follow-up: 32 months Time to next therapy 41% reduced risk of progression 48% reduced risk of progression 3-year PFS Median PFS 3-year TTNT Median TTNT 1.00 MPVT MPV 51% 37.2 months 32% 27.4 months 1.00 MPVT MPV 70% Not reached 51% 37.6 months Patients (%) HR 0.59 p < Time (months) Patients (%) HR 0.52 p < Time (months) Palumbo A, et al. J Clin Oncol. 2010;28:
54 PETHEMA/GEM study phase 3 trial of MPV and VTP in elderly patients with previously untreated MM Untreated MM; age > 65 years (N = 253) R A N D O M I Z A T I O N MPV (n = 130) Bortezomib 1.3 mg/m 2 for one 6-week cycle, days 1, 4, 8, 11, 22, 25, 29, 32; then for five 5-week cycles, days 1, 8, 15, 22 Melphalan 9 mg/m 2 and Prednisone 60 mg/m 2, days 1 4 of each cycle VTP (n = 130) Bortezomib as above, continuous Thalidomide 100 mg/day, Prednisone as above Maintenance Bortezomib 1.3 mg/m 2, days 1, 4, 8, 11 every 3 months Prednisone 50 mg every other day Maintenance Bortezomib 1.3 mg/m 2, days 1, 4, 8, 11 every 3 months Thalidomide 50 mg/day Maximum 6 cycles Up 3 years Mateos MV, et al. Lancet Oncology. 2010;11:
55 VMP vs VTP VT vs VP in Elderly Newly Diagnosed Myeloma Patients: Responses Outcome Following Induction, % VMP VTP After a median follow-up (n = of 130) 32 months from (n = 130) first randomization ORR CR (if negative) CR (if median positive) PFS for all patients 12 was 31 months 10 PR MR median TTP was 35 months 10 6 SD 8 11 Outcome 3-year Following OS was 70% VT VP Maintenance Therapy, % (n = 91) (n = 87) CR/nCRno significant differences between the MPV and CR (if negative) CR VTP (if positive) groups in PFS (p = ) and 3-year OS 16 (p = PR 0.3) MR 2 1 Overall CR rate (if negative) increased from 23% following induction to 42% after maintenance Mateos MV, et al. Lancet Oncol. 2010;11:
56 Toxicity of Maintenance in Elderly MM Patients Grade 3/4 adverse events significantly increased in VMPT VT vs VMP arms (Neutropenia (P =.02); Cardiologic (P =.04); Deep vein thrombosis/pulmonary embolism (P =.05) More patients in VMPT VT vs VMP arm discontinued treatment due to adverse events: 21% vs 16% Palumbo A, et al. J Clin Oncol. 2010;28: MPV treatment produced more haematological adverse events than VTPV (particularly grade 3 or worse neutropenia and thrombocytopenia) VTP was associated with severe cardiac complications (11 patients (8%) compared with none in those receiving MPV) Rate of infections was higher with MPV than with VTP Mateos MV, et al. Lancet Oncology. 2010;11:
57 MM-015: phase 3 trial of MPR vs MP for longterm control in newly diagnosed MM R A N D O M I Z A T I O N 51 centres in Europe, Australia, and Israel (N = 459) MPR-R Melphalan 0.18 mg/kg, days 1 4 Prednisone 2 mg/kg, days 1 4 Lenalidomide 10 mg/day p.o., days 1 21 MPR Cycles (28-day) 1 9 Melphalan 0.18 mg/kg, days 1 4 Prednisone 2 mg/kg, days 1 4 Lenalidomide 10 mg/day p.o., days 1 21 MPSecondary comparison Melphalan MPR-R 0.18 vsmg/kg, MPR days 1 4 Prednisone Addition of 2 MPR mg/kg, arm days per 1 4 PlaceboEMEA days advice 1 21 Cycles 10+ Lenalidomide continued 10 mg/day days 1 21 Placebo Placebo P R O G R E S S I O N Len (25 mg/day) ± Dex Double-blind treatment phase Stratification by age ( 75 vs > 75 years) and ISS stage (1, 2, or 3) Open-label extension and follow-up phase Palumbo A, et al. Blood. 2010;116:[abstract 622]. Updated data presented at ASH 2010.
58 MM-015: response rates significantly higher with MPR-R vs MP Best overall response* MPR-R (n = 152) MP (n = 154) p value (MPR-R vs MP) ORR ( PR) (%) < CR ** (%) 16 4 < VGPR*** (%) < Median time to first response (months) 2 3 < *As measured using EBMT criteria. 1 **Immunofixation negative with or without bone marrow confirmation. ***VGPR: > 90% reduction in M protein. Palumbo A, et al. Blood. 2010;116:[abstract 622]. 1. Bladé J, et al. Br J Haematol. 1998;102:
59 MM-015: MPR-R significantly improved progression-free survival Patients (%) Time (months) Median follow-up 25 months *Analysis based on data up to May MPR MP p < 10-7 Median PFS low incidence of adverse events MPR-R during lenalidomide continuous treatment but p = months 14 months 13 months maintenance 25 therapy should performed only in clinical trials! Palumbo A, et al. Blood. 2010;116:[abstract 622]. Updated data presented at ASH 2010.
60 COSA è CAMBIATO CON LE NUOVE ASSOCIAZIONI? La THAL e il Bortezomib si potenziano in associazione con MP Il patner ideale per la Len non sembra essere MP ma il Dex/dex La scelta dell uno vs l altro l dipende da considerazioni specifiche sul singolo paziente (PS/comorbidit comorbidità,, rischio genetico, PNP all esordio etc) Le dosi dei nuovi agenti devono essere aggiustate in relazione all et età Non ci sono dati a favore che l utilizzo l contemporaneo dei nuovi agenti possa comportare ad un miglioramento della risposta in grado di incisìdere sulla OS rispetto ad un uso sequenziale volto ad ottenere il massimo da ogni singolo agente Mantenimento/Extended therapy migliora la qualità della risposta e la PFS. Non ci sono dati a favore di un incremento della OS (soprattutto vs un trattamento alla recidiva). Il mantenimento con Bortezomib o Thal aumentano la tossicità.. MPR-R: R: secondo tumore?
61 VULNERABILITY OF ELDERLY PATIENTS Frailty grade Description Fraility: weakness, regularly poor or occasionally endurance, weight loss, low physical activity, Patients not, slow regularly gait active speed beyond Very fit Moderately fit Active, energetic patients, who exercise routinely walking Comorbidity: At concurrent presence of 2 least 2 comorbidities in US: medically diagnosed diseases. Vulnerable Mildly frail Moderately frail Severely frail Patients who can perform limited activities but yet do not need help from other people yrs: : 35% in M and 45% in F Patients who need help for household tasks (shopping, walking several blocks, managing their finances, and medications) - 80 yrs: : 53% in M and 70% in F Disability: difficulty in activities essential to independent living (personal care, household tasks) Patients who need partial help for their personal care (dressing, bathing, toileting, eating) Patients completely dependent on other people for their personal care Palumbo et al, Blood 2011
62 Report of European Myeloma Network (EMN) on personalized therapy in MM according to age and vulnerability Palumbo et al, Blood oct 2011
63

64 CR, PFS and OS CR and PFS QoL

65
66 PROPOSAL OF THERAPEUTIC ALGORITHM FOR PTS NOT CANDIDATE FOR ASCT > 75 yrs or frail < 75 yrs or fit Specific complications Low-dose MPT Low-dose Bz ± MP MP Low-dose Dex Low dose Len/Dex CDT Ctx-Pdn NO MPT MPV CTD Rd MPR-R R? Renal: Bz-based YES Thrombophilic status, cardiovascular events: Bz-based Poor genetic risk: Bz-based History of PN: Len-based
67 Future Directions (Continued)? Tuning of tested combinations Newer combinations. Novel agent sequences (second generation PIs, HDAC inhibitors, other small molecules, 3rd generation IMiDs, MoAbs)? Tailored approach to therapy: Identify groups of pts in whom combinations are required versus pts in whom doublets and/or sequences should be used Use of GEP, Proteomics Risk adaptation
68
69 In the Absence of Data Quality of Life Response CLINICAL TRIALS!!!!!! and Risk Based Therapy
70 IMWG response criteria Durie et al., Leukemia 2006 scr: : CR più normale rapporto FLC,, assenza di cellule clonali midollari all analisi analisi citofluorimetrica ed immunoistochimica CR: : IF negativa nel siero e nelle urine, scomparsa di localizzazioni tessutali da plasmacitoma e <5% di plasmacellule midollari VGPR: : negatività all elettroforesi o riduzione di della CM sierica 90% e BJ proteinuria <100 mg/24h PR: riduzione della CM sierica 50% e della BJ 90% o < 200 mg/24h; nei MM non secernenti, riduzione 50% del rapporto FLC e della plasmocitosi midollare 50% (partendo da un infiltrato iniziale 30%; nei plasmacitomi solitari, riduzione 50% delle dimensioni SD: se non soddisfatti i criteri della CR, VGPR, PR e della progressione sione (non criterio di risposta; utile per calcolare TTP) LB UNIMI


71 IMiDs, bortezomib Dex Bortezomib Hsp90 inh HDAC inh Alkylators Anthracyclines Mitochondria Caspase-8 Cytochrome-c Caspase 9 Smac NFκB Transcriptional changes Caspase-3 PARP Proteasome Aggresome TUMOR CELL DEATH TUMOR CELL DEATH The Future: Synergistic anti-mm activity Proteasome Inhibitor/IMiD-based Novel Agent Combos
Cure versus control: Which is the best strategy?
 Cure versus control: Which is the best strategy? Barcelona 8-9-2012 Mario Boccadoro DIVISIONE UNIVERSITARIA DI EMATOLOGIA AZIENDA OSPEDALIERA SAN GIOVANNI TORINO, ITALY MULTIPLE MYELOMA Cure versus control
Cure versus control: Which is the best strategy? Barcelona 8-9-2012 Mario Boccadoro DIVISIONE UNIVERSITARIA DI EMATOLOGIA AZIENDA OSPEDALIERA SAN GIOVANNI TORINO, ITALY MULTIPLE MYELOMA Cure versus control
Multiple Myeloma: Novel Agents. Robert A. Kyle, M.D. Germany June 28, 2008. Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida
 Multiple Myeloma: Novel Agents Robert A. Kyle, M.D. Germany June 28, 2008 Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Multiple Myeloma Untreated Initial Therapy Transplant eligible Multiple
Multiple Myeloma: Novel Agents Robert A. Kyle, M.D. Germany June 28, 2008 Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Multiple Myeloma Untreated Initial Therapy Transplant eligible Multiple
Treatment results with Bortezomib in multiple myeloma
 Treatment results with Bortezomib in multiple myeloma Prof. Dr. Orhan Sezer Hamburg University Medical Center Circulating proteasome levels are an independent prognostic factor in MM 1.0 Probability of
Treatment results with Bortezomib in multiple myeloma Prof. Dr. Orhan Sezer Hamburg University Medical Center Circulating proteasome levels are an independent prognostic factor in MM 1.0 Probability of
Modern Induction Therapy for Transplant-ineligible Multiple Myeloma Patients: Literature of Review
 Modern Induction Therapy for Transplant-ineligible Multiple Myeloma Patients: Literature of Review Dr. Kalita Lohit kumar 1, Dr. Gogoi Pabitra Kamar 2, Dr. Sarma Umesh Ch. 3 1 MS, Assistant Professor,
Modern Induction Therapy for Transplant-ineligible Multiple Myeloma Patients: Literature of Review Dr. Kalita Lohit kumar 1, Dr. Gogoi Pabitra Kamar 2, Dr. Sarma Umesh Ch. 3 1 MS, Assistant Professor,
STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA
 STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA Sundar Jagannath MD Professor of Medicine St. Vincent s Comprehensive Cancer Center New York, NY Where is transplant today in the management of Myeloma? Autologous
STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA Sundar Jagannath MD Professor of Medicine St. Vincent s Comprehensive Cancer Center New York, NY Where is transplant today in the management of Myeloma? Autologous
Multiple Myeloma Therapy Doublet, Triplet, and beyond October 2013 The IV. International Eurasian Congress of Hematology Rafat Abonour, M.D.
 Multiple Myeloma Therapy Doublet, Triplet, and beyond October 2013 The IV. International Eurasian Congress of Hematology Rafat Abonour, M.D. Multiple Myeloma Facts Second most prevalent hematologic neoplasm,
Multiple Myeloma Therapy Doublet, Triplet, and beyond October 2013 The IV. International Eurasian Congress of Hematology Rafat Abonour, M.D. Multiple Myeloma Facts Second most prevalent hematologic neoplasm,
pan-canadian Oncology Drug Review Final Clinical Guidance Report Bortezomib (Velcade) for Multiple Myeloma March 25, 2013
 for Multiple Myeloma March 25, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Bortezomib (Velcade) for Multiple Myeloma March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Final Clinical Guidance Report Bortezomib (Velcade) for Multiple Myeloma March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
Current Multiple Myeloma Treatment Adapted From the NCCN Guidelines
 Current Multiple Myeloma Treatment Adapted From the NCCN Guidelines Diagnosis Survival 3-5 yrs Survival
Current Multiple Myeloma Treatment Adapted From the NCCN Guidelines Diagnosis Survival 3-5 yrs Survival
Bendamustine for the fourth-line treatment of multiple myeloma
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Bendamustine for the fourth-line treatment of multiple myeloma Contents Summary 1 Background 2 Epidemiology 3 Cost 6 References 7 Summary There is no standard
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Bendamustine for the fourth-line treatment of multiple myeloma Contents Summary 1 Background 2 Epidemiology 3 Cost 6 References 7 Summary There is no standard
NATIONAL CANCER DRUG FUND PRIORITISATION SCORES
 NATIONAL CANCER DRUG FUND PRIORITISATION SCORES Drug Indication Regimen (where appropriate) BORTEZOMIB In combination with dexamethasone (VD), or with dexamethasone and thalidomide (VTD), is indicated
NATIONAL CANCER DRUG FUND PRIORITISATION SCORES Drug Indication Regimen (where appropriate) BORTEZOMIB In combination with dexamethasone (VD), or with dexamethasone and thalidomide (VTD), is indicated
Treating myeloma. Dr Rachel Hall Royal Bournemouth Hospital
 Treating myeloma Dr Rachel Hall Royal Bournemouth Hospital Treatment overview When to treat? Aim of treatment Which treatment? Monitoring response to treatment Prevention of complications What happens
Treating myeloma Dr Rachel Hall Royal Bournemouth Hospital Treatment overview When to treat? Aim of treatment Which treatment? Monitoring response to treatment Prevention of complications What happens
ONCOLOGIA: esperienze cliniche a confronto. Il carcinoma mammario metastatico
 ONCOLOGIA: esperienze cliniche a confronto. Il carcinoma mammario metastatico Sequenza ottimale del trattamento Maria Teresa Scognamiglio U.O.C. Clinica Oncologica Chieti-Ortona Chieti 12 novembre 213
ONCOLOGIA: esperienze cliniche a confronto. Il carcinoma mammario metastatico Sequenza ottimale del trattamento Maria Teresa Scognamiglio U.O.C. Clinica Oncologica Chieti-Ortona Chieti 12 novembre 213
Multiple Myeloma. Solving a growing puzzle
 Multiple Myeloma Solving a growing puzzle Disclosures Financial I wish. I eat too much. I did ask who the audience would be. Nurses and Doctors Goals 1. Understand the incidence, symptoms, and pathophysiology
Multiple Myeloma Solving a growing puzzle Disclosures Financial I wish. I eat too much. I did ask who the audience would be. Nurses and Doctors Goals 1. Understand the incidence, symptoms, and pathophysiology
REVLIMID and IMNOVID for Multiple Myeloma
 REVLIMID and IMNOVID for Multiple Myeloma What is Multiple Myeloma? Multiple myeloma (MM) is a persistent and life-threatening blood cancer that is characterised by tumour proliferation and immune suppression.
REVLIMID and IMNOVID for Multiple Myeloma What is Multiple Myeloma? Multiple myeloma (MM) is a persistent and life-threatening blood cancer that is characterised by tumour proliferation and immune suppression.
FastTest. You ve read the book... ... now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. Please refer back to relevant sections
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. Please refer back to relevant sections
ORIGINAL ARTICLE. European Journal of Haematology ISSN 0902-4441
 European Journal of Haematology ISSN 0902-4441 ORIGINAL ARTICLE Lenalidomide in combination with dexamethasone at first relapse in comparison with its use as later salvage therapy in relapsed or refractory
European Journal of Haematology ISSN 0902-4441 ORIGINAL ARTICLE Lenalidomide in combination with dexamethasone at first relapse in comparison with its use as later salvage therapy in relapsed or refractory
Review of health-related quality of life data in multiple myeloma patients treated with novel agents
 OPEN Leukemia (2013) 27, 1959 1969 & 2013 Macmillan Publishers Limited All rights reserved 0887-6924/13 www.nature.com/leu REVIEW Review of health-related quality of life data in multiple myeloma patients
OPEN Leukemia (2013) 27, 1959 1969 & 2013 Macmillan Publishers Limited All rights reserved 0887-6924/13 www.nature.com/leu REVIEW Review of health-related quality of life data in multiple myeloma patients
Future strategies for myeloma: An overview of novel treatments In development
 Future strategies for myeloma: An overview of novel treatments In development Dr. Matthew Streetly Guys and St. Thomas NHS Trust How far have we come? Melphalan and prednisolone VAD Autologous SCT Thalidomide
Future strategies for myeloma: An overview of novel treatments In development Dr. Matthew Streetly Guys and St. Thomas NHS Trust How far have we come? Melphalan and prednisolone VAD Autologous SCT Thalidomide
Background. t 1/2 of 3.7 4.7 days allows once-daily dosing (1.5 mg) with consistent serum concentration 2,3 No interaction with CYP3A4 inhibitors 4
 with consistent serum concentration 2,3 No interaction with CYP3A4 inhibitors 4") Abstract No. 4501 Tivozanib versus sorafenib as initial targeted therapy for patients with advanced renal cell carcinoma: Results from a Phase III randomized, open-label, multicenter trial R. Motzer, D.
Abstract No. 4501 Tivozanib versus sorafenib as initial targeted therapy for patients with advanced renal cell carcinoma: Results from a Phase III randomized, open-label, multicenter trial R. Motzer, D.
Pro Cure in Multiple Myeloma. Nicolaus Kröger Dept. of Stem Cell Transplantation University Hospital Hamburg Hamburg, Germany
 Pro Cure in Multiple Myeloma Nicolaus Kröger Dept. of Stem Cell Transplantation University Hospital Hamburg Hamburg, Germany Pro Cure in Multiple Myeloma Several hematological malignancies can be cured
Pro Cure in Multiple Myeloma Nicolaus Kröger Dept. of Stem Cell Transplantation University Hospital Hamburg Hamburg, Germany Pro Cure in Multiple Myeloma Several hematological malignancies can be cured
Advances In Chemotherapy For Hormone Refractory Prostate Cancer. TAX 327 study results & SWOG 99-16 study results presented at ASCO 2004
 Ronald de Wit Rotterdam Cancer Institute The Netherlands Advances In Chemotherapy For Hormone Refractory Prostate Cancer TAX 327 study results & SWOG 99-16 study results presented at Slide 1 Prostate Cancer
Ronald de Wit Rotterdam Cancer Institute The Netherlands Advances In Chemotherapy For Hormone Refractory Prostate Cancer TAX 327 study results & SWOG 99-16 study results presented at Slide 1 Prostate Cancer
Shaji Kumar, M.D. Multiple Myeloma: Multiple myeloma (MM) is the second most common hematological
 is the second most common hematological") An update on the management of multiple myeloma and amyloidosis Shaji Kumar, M.D. Multiple Myeloma: Multiple myeloma (MM) is the second most common hematological malignancy in this country affecting nearly
An update on the management of multiple myeloma and amyloidosis Shaji Kumar, M.D. Multiple Myeloma: Multiple myeloma (MM) is the second most common hematological malignancy in this country affecting nearly
The Blood Cancer Twice As Likely To Affect African Americans: Multiple Myeloma
 The Blood Cancer Twice As Likely To Affect African Americans: Multiple Myeloma 11 th Annual National Leadership Summit on Health Disparities Innovation Towards Reducing Disparities Congressional Black
The Blood Cancer Twice As Likely To Affect African Americans: Multiple Myeloma 11 th Annual National Leadership Summit on Health Disparities Innovation Towards Reducing Disparities Congressional Black
Maintenance therapy in in Metastatic NSCLC. Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai
 Maintenance therapy in in Metastatic NSCLC Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai Definition of Maintenance therapy The U.S. National Cancer Institute s
Maintenance therapy in in Metastatic NSCLC Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai Definition of Maintenance therapy The U.S. National Cancer Institute s
How to treat elderly patients with multiple myeloma: combination of therapy or sequencing
 MULTIPLE MYELOMA How to treat elderly patients with multiple myeloma: combination of therapy or sequencing Antonio Palumbo 1 and Francesca Gay 1 1 Divisione di Ematologia dell Università di Torino, Azienda
MULTIPLE MYELOMA How to treat elderly patients with multiple myeloma: combination of therapy or sequencing Antonio Palumbo 1 and Francesca Gay 1 1 Divisione di Ematologia dell Università di Torino, Azienda
What's new for the treatment of multiple myeloma and related disorders in 2010? Angela Dispenzieri, M.D.
 What's new for the treatment of multiple myeloma and related disorders in 2010? Angela Dispenzieri, M.D. The progress being made for the treatment of multiple myeloma has resulted in a significant prolongation
What's new for the treatment of multiple myeloma and related disorders in 2010? Angela Dispenzieri, M.D. The progress being made for the treatment of multiple myeloma has resulted in a significant prolongation
FEIST- WEILLER CANCER CENTER MULTIPLE MYELOMA GUIDELINES. Updated December, 2011. Authors: Nebu Koshy, MD. Binu Nair, MD. Gerhard Hildebrandt, MD
 FEIST- WEILLER CANCER CENTER MULTIPLE MYELOMA GUIDELINES Updated December, 2011 Authors: Nebu Koshy, MD Binu Nair, MD Gerhard Hildebrandt, MD Reinhold Munker, MD Glenn Mills, MD Mandatory initial tests
FEIST- WEILLER CANCER CENTER MULTIPLE MYELOMA GUIDELINES Updated December, 2011 Authors: Nebu Koshy, MD Binu Nair, MD Gerhard Hildebrandt, MD Reinhold Munker, MD Glenn Mills, MD Mandatory initial tests
LEUCEMIA MIELOIDE ACUTA. A.M. Carella U.O.C. Ematologia IRCCS AOU San Martino IST, Genova
 LEUCEMIA MIELOIDE ACUTA A.M. Carella U.O.C. Ematologia IRCCS AOU San Martino IST, Genova Impact of mutational analysis in AML C. Thiede Optimal acute myeloid leukemia therapy in 2012 H. Dombret Acquired
LEUCEMIA MIELOIDE ACUTA A.M. Carella U.O.C. Ematologia IRCCS AOU San Martino IST, Genova Impact of mutational analysis in AML C. Thiede Optimal acute myeloid leukemia therapy in 2012 H. Dombret Acquired
MULTIPLE MYELOMA Treatment Overview
 MULTIPLE MYELOMA Treatment Overview ABOUT THE MULTIPLE MYELOMA RESEARCH FOUNDATION After being diagnosed with multiple myeloma in 1998, Kathy Giusti and her sister Karen Andrews, a successful corporate
MULTIPLE MYELOMA Treatment Overview ABOUT THE MULTIPLE MYELOMA RESEARCH FOUNDATION After being diagnosed with multiple myeloma in 1998, Kathy Giusti and her sister Karen Andrews, a successful corporate
MULTIPLE MYELOMA Review & Update for Primary Care. Dr. Joseph Mignone 21st Century Oncology
 MULTIPLE MYELOMA Review & Update for Primary Care Dr. Joseph Mignone 21st Century Oncology OVERVIEW Identify the diagnostic criteria for multiple myeloma Compare first & second line therapies, using data
MULTIPLE MYELOMA Review & Update for Primary Care Dr. Joseph Mignone 21st Century Oncology OVERVIEW Identify the diagnostic criteria for multiple myeloma Compare first & second line therapies, using data
AUTOLOGOUS STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA: IS IT STILL THE RIGHT CHOICE?
 AUTOLOGOUS STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA: IS IT STILL THE RIGHT CHOICE? *Patrizia Tosi Hematology Unit, Department of Oncology and Hematology, Infermi Hospital, Rimini, Italy *Correspondence
AUTOLOGOUS STEM CELL TRANSPLANTATION IN MULTIPLE MYELOMA: IS IT STILL THE RIGHT CHOICE? *Patrizia Tosi Hematology Unit, Department of Oncology and Hematology, Infermi Hospital, Rimini, Italy *Correspondence
Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003)
 in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003)") Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003) Reeder CB et al. Proc ASCO 2010;Abstract 8037. Introduction > Patients (pts) with low-grade
Lenalidomide (LEN) in Patients with Transformed Lymphoma: Results From a Large International Phase II Study (NHL-003) Reeder CB et al. Proc ASCO 2010;Abstract 8037. Introduction > Patients (pts) with low-grade
2014; 5(3): 248-252. doi: 10.7150/jca.8541 Research Paper
: 248-252. doi: 10.7150/jca.8541 Research Paper") 248 Ivyspring International Publisher Journal of Cancer 2014; 5(3): 248-252. doi: 10.7150/jca.8541 Research Paper Partial Response at Completion of Bortezomib- Thalidomide-Dexamethasone (VTd) Induction
248 Ivyspring International Publisher Journal of Cancer 2014; 5(3): 248-252. doi: 10.7150/jca.8541 Research Paper Partial Response at Completion of Bortezomib- Thalidomide-Dexamethasone (VTd) Induction
lenalidomide, 5mg, 10mg, 15mg and 25mg hard capsules (Revlimid ) SMC No. (441/08) Celgene Limited
 SMC No. (441/08) Celgene Limited") Resubmission: lenalidomide, 5mg, 10mg, 15mg and 25mg hard capsules (Revlimid ) SMC No. (441/08) Celgene Limited 07 March 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Resubmission: lenalidomide, 5mg, 10mg, 15mg and 25mg hard capsules (Revlimid ) SMC No. (441/08) Celgene Limited 07 March 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the
New Treatment Options for Breast Cancer
 New Treatment Options for Breast Cancer Brandon Vakiner, PharmD., BCOP Clinical Pharmacy Specialist - Oncology The University of Iowa Hospitals and Clinics Assistant Professor (Clinical) University of
New Treatment Options for Breast Cancer Brandon Vakiner, PharmD., BCOP Clinical Pharmacy Specialist - Oncology The University of Iowa Hospitals and Clinics Assistant Professor (Clinical) University of
Multiple. Powerful thinking advances the cure
 Multiple Myeloma Treatment OVERVIEW Powerful thinking advances the cure Powerful thinking advances the cure About the Multiple Myeloma Research Foundation The Multiple Myeloma Research Foundation (MMRF)
Multiple Myeloma Treatment OVERVIEW Powerful thinking advances the cure Powerful thinking advances the cure About the Multiple Myeloma Research Foundation The Multiple Myeloma Research Foundation (MMRF)
In ELOQUENT-2, Empliciti was evaluated in patients who had received one to three prior
 - First and only immunostimulatory antibody approved in the European Union for multiple myeloma - Accelerated assessment and approval based on long-term data from ELOQUENT-2, which evaluated Empliciti
- First and only immunostimulatory antibody approved in the European Union for multiple myeloma - Accelerated assessment and approval based on long-term data from ELOQUENT-2, which evaluated Empliciti
Verso un interruzione dei farmaci nella leucemia mieloide cronica
 Verso un interruzione dei farmaci nella leucemia mieloide cronica Giuseppe Saglio Rational to try to discontinue therapy Quality of life Long-term side effects of therapy still unknown Cost Terms and definitions
Verso un interruzione dei farmaci nella leucemia mieloide cronica Giuseppe Saglio Rational to try to discontinue therapy Quality of life Long-term side effects of therapy still unknown Cost Terms and definitions
La personalizzazione terapeutica: quanto influisce l età
 La personalizzazione terapeutica: quanto influisce l età PierFranco Conte University of Padova Department of Surgery, Oncology and Gastroenterology IOV Istituto Oncologico Veneto I.R.C.C.S. Breast Cancer
La personalizzazione terapeutica: quanto influisce l età PierFranco Conte University of Padova Department of Surgery, Oncology and Gastroenterology IOV Istituto Oncologico Veneto I.R.C.C.S. Breast Cancer
Integrating novel agents into multiple myeloma treatment current status in Switzerland and treatment recommendations
 current status in Switzerland and treatment recommendations Christian Taverna a, Mario Bargetzi b, Daniel Betticher c, Jürg Gmür d, Michael Gregor e, Dominik Heim f, Urs Hess g, Nicolas Ketterer h, Erika
current status in Switzerland and treatment recommendations Christian Taverna a, Mario Bargetzi b, Daniel Betticher c, Jürg Gmür d, Michael Gregor e, Dominik Heim f, Urs Hess g, Nicolas Ketterer h, Erika
Long-term Results of Response to Therapy, Time to Progression, and Survival With Lenalidomide Plus Dexamethasone in Newly Diagnosed Myeloma
 ORIGINAL ARTICLE LONG-TERM RESULTS OF REV-DEX THERAPY FOR NEWLY DIAGNOSED MYELOMA Long-term Results of Response to Therapy, Time to Progression, and Survival With Lenalidomide Plus Dexamethasone in Newly
ORIGINAL ARTICLE LONG-TERM RESULTS OF REV-DEX THERAPY FOR NEWLY DIAGNOSED MYELOMA Long-term Results of Response to Therapy, Time to Progression, and Survival With Lenalidomide Plus Dexamethasone in Newly
MULTIPLE MYELOMA. Version Date: February, 2015
 MULTIPLE MYELOMA Version Date: February, 2015 The recommendations contained in this guideline are a consensus of the Alberta Provincial Hematology Tumour Team synthesis of currently accepted approaches
MULTIPLE MYELOMA Version Date: February, 2015 The recommendations contained in this guideline are a consensus of the Alberta Provincial Hematology Tumour Team synthesis of currently accepted approaches
Multiple Myeloma. Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida CP1123175-1
 Multiple Myeloma 8 th Annual Living with Myeloma Conference New Developments in Multiple Myeloma Treatment Scottsdale, AZ March 22, 2014 Robert A. Kyle, MD Scottsdale, Arizona Rochester, Minnesota Jacksonville,
Multiple Myeloma 8 th Annual Living with Myeloma Conference New Developments in Multiple Myeloma Treatment Scottsdale, AZ March 22, 2014 Robert A. Kyle, MD Scottsdale, Arizona Rochester, Minnesota Jacksonville,
FARYDAK (Panobinostat) for the Treatment of Patients With Previously Treated Multiple Myeloma
 for the Treatment of Patients With Previously Treated Multiple Myeloma") CI-1 FARYDAK (Panobinostat) for the Treatment of Patients With Previously Treated Multiple Myeloma Oncologic Drugs Advisory Committee Meeting November 6, 2014 CI-2 FARYDAK (Panobinostat) for the Treatment
CI-1 FARYDAK (Panobinostat) for the Treatment of Patients With Previously Treated Multiple Myeloma Oncologic Drugs Advisory Committee Meeting November 6, 2014 CI-2 FARYDAK (Panobinostat) for the Treatment
What is the Optimal Front-Line Treatment for mrcc? Michael B. Atkins, MD Deputy Director, Georgetown-Lombardi Comprehensive Cancer Center
 What is the Optimal Front-Line Treatment for mrcc? Michael B. Atkins, MD Deputy Director, Georgetown-Lombardi Comprehensive Cancer Center The Case for Immunotherapy in mrcc 1. Achieves patient s goal 2.
What is the Optimal Front-Line Treatment for mrcc? Michael B. Atkins, MD Deputy Director, Georgetown-Lombardi Comprehensive Cancer Center The Case for Immunotherapy in mrcc 1. Achieves patient s goal 2.
What is the optimal sequence of anti-her2 therapy in metastatic breast cancer?
 What is the optimal sequence of anti-her2 therapy in metastatic breast cancer? David Miles Mount Vernon Cancer Centre Northwood Middlesex UKBCM mee)ng: London 2013 Herceptin plus a taxoid extends survival
What is the optimal sequence of anti-her2 therapy in metastatic breast cancer? David Miles Mount Vernon Cancer Centre Northwood Middlesex UKBCM mee)ng: London 2013 Herceptin plus a taxoid extends survival
New Targets and Treatments for Follicular Lymphoma. Disclosures
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Disclosures Consulting fees from:
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Disclosures Consulting fees from:
MULTIPLE MYELOMA TREATMENT OVERVIEW
 MULTIPLE MYELOMA TREATMENT OVERVIEW Sponsored by: This activity is supported by independent educational grants from Genentech BioOncology, Merck & Co., Inc., Millennium Pharmaceuticals, Inc., and Novartis
MULTIPLE MYELOMA TREATMENT OVERVIEW Sponsored by: This activity is supported by independent educational grants from Genentech BioOncology, Merck & Co., Inc., Millennium Pharmaceuticals, Inc., and Novartis
UNDERSTANDING MULTIPLE MYELOMA AND LABORATORY VALUES Benjamin Parsons, DO bmparson@gundersenhealth.org Gundersen Health System Center for Cancer and
 UNDERSTANDING MULTIPLE MYELOMA AND LABORATORY VALUES Benjamin Parsons, DO bmparson@gundersenhealth.org Gundersen Health System Center for Cancer and Blood Disorders La Crosse, WI UNDERSTANDING MULTIPLE
UNDERSTANDING MULTIPLE MYELOMA AND LABORATORY VALUES Benjamin Parsons, DO bmparson@gundersenhealth.org Gundersen Health System Center for Cancer and Blood Disorders La Crosse, WI UNDERSTANDING MULTIPLE
Prior Authorization Guideline
 Prior Authorization Guideline Guideline: PS Inj - Velcade Therapeutic Class: Antineoplastic Agents Therapeutic Sub-Class: Antineoplastic Client: PS Inj Approval Date: 10/2/2004 Revision Date: 5/22/2007
Prior Authorization Guideline Guideline: PS Inj - Velcade Therapeutic Class: Antineoplastic Agents Therapeutic Sub-Class: Antineoplastic Client: PS Inj Approval Date: 10/2/2004 Revision Date: 5/22/2007
Momentum in Multiple Myeloma Treatment
 WHITE PAPER Momentum in Multiple Myeloma Treatment Dr. Harish P. Dave, MD, MBA Dr. Ben Manderman, MD Quintiles examines promising new approaches to more effective multiple myeloma treatments. HIGH RESPONSE
WHITE PAPER Momentum in Multiple Myeloma Treatment Dr. Harish P. Dave, MD, MBA Dr. Ben Manderman, MD Quintiles examines promising new approaches to more effective multiple myeloma treatments. HIGH RESPONSE
IF AT FIRST YOU DON T SUCCEED: TRIAL, TRIAL AGAIN
 + IF AT FIRST YOU DON T SUCCEED: TRIAL, TRIAL AGAIN Rena Buckstein MD FRCPC Head Hematology Site Group Sunnybrook Odette Cancer Center (OCC) Head of Hematology Clinical Trials Group at OCC + Outline Start
+ IF AT FIRST YOU DON T SUCCEED: TRIAL, TRIAL AGAIN Rena Buckstein MD FRCPC Head Hematology Site Group Sunnybrook Odette Cancer Center (OCC) Head of Hematology Clinical Trials Group at OCC + Outline Start
Multiple Myeloma in HUSM. Dr Azlan Husin HUSM
 Multiple Myeloma in HUSM Dr Azlan Husin HUSM Outline Overview Presenting features Progress in myeloma Global HUSM Multiple myeloma is a neoplastic plasma-cell disorder that is characterized by clonal proliferation
Multiple Myeloma in HUSM Dr Azlan Husin HUSM Outline Overview Presenting features Progress in myeloma Global HUSM Multiple myeloma is a neoplastic plasma-cell disorder that is characterized by clonal proliferation
Henk Lokhorst, Torben Plesner, Peter Gimsing, Hareth Nahi, Steen Lisby, Paul Richardson
 DRTUMUMB, a CD38 Monoclonal ntibody Study in dvanced Multiple Myeloma an Open-Label, Dose Escalation Followed by Open-Label Extension in a Single-rm Phase I/II Study bstract #S576 Henk Lokhorst, Torben
DRTUMUMB, a CD38 Monoclonal ntibody Study in dvanced Multiple Myeloma an Open-Label, Dose Escalation Followed by Open-Label Extension in a Single-rm Phase I/II Study bstract #S576 Henk Lokhorst, Torben
Clinical Trial Design. Sponsored by Center for Cancer Research National Cancer Institute
 Clinical Trial Design Sponsored by Center for Cancer Research National Cancer Institute Overview Clinical research is research conducted on human beings (or on material of human origin such as tissues,
Clinical Trial Design Sponsored by Center for Cancer Research National Cancer Institute Overview Clinical research is research conducted on human beings (or on material of human origin such as tissues,
Understanding Revlimid
 Understanding Revlimid International Myeloma Foundation 12650 Riverside Drive, Suite 206 North Hollywood, CA 91607 USA Telephone: 800-452-CURE (2873) (USA & Canada) 818-487-7455 Fax: 818-487-7454 TheIMF@myeloma.org
Understanding Revlimid International Myeloma Foundation 12650 Riverside Drive, Suite 206 North Hollywood, CA 91607 USA Telephone: 800-452-CURE (2873) (USA & Canada) 818-487-7455 Fax: 818-487-7454 TheIMF@myeloma.org
Multiple Myeloma Overview. Treatment and challenges.
 Multiple Myeloma Overview. Treatment and challenges. Ade Olujohungbe Dip.Haem ( Lond) MD FRCP FRCPath. Associate Professor of Hematology. Cancercare Manitoba Disclosure of Potential for Conflict of Interest
Multiple Myeloma Overview. Treatment and challenges. Ade Olujohungbe Dip.Haem ( Lond) MD FRCP FRCPath. Associate Professor of Hematology. Cancercare Manitoba Disclosure of Potential for Conflict of Interest
Front Line Treatment of Elderly Multiple Myeloma in the Era of Novel Agents
 Front Line Treatment of Elderly Multiple Myeloma in the Era of Novel Agents The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
Front Line Treatment of Elderly Multiple Myeloma in the Era of Novel Agents The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
Multiple Myeloma: Overview and Therapeutic Approaches
 Multiple Myeloma: Overview and Therapeutic Approaches Presented as a Live Webinar Wednesday, August 14, 2013 and Wednesday, September 11, 2013 Planned and conducted by ASHP Advantage and supported by educational
Multiple Myeloma: Overview and Therapeutic Approaches Presented as a Live Webinar Wednesday, August 14, 2013 and Wednesday, September 11, 2013 Planned and conducted by ASHP Advantage and supported by educational
Focus on the Treatment of Multiple Myeloma
 Focus on the Treatment of Multiple Myeloma PRINTER-FRIENDLY VERSION AT CLINICALONCOLOGY.COM SHAJI KUMAR, MD Associate Professor of Medicine Division of Hematology Mayo Clinic Rochester, Minnesota S. VINCENT
Focus on the Treatment of Multiple Myeloma PRINTER-FRIENDLY VERSION AT CLINICALONCOLOGY.COM SHAJI KUMAR, MD Associate Professor of Medicine Division of Hematology Mayo Clinic Rochester, Minnesota S. VINCENT
Pharmacoeconomic Analyses and Oncology Pharmacy: Optimizing Multiple Myeloma Value for Patients and Plans
 Pharmacoeconomic Analyses and Oncology Pharmacy: Optimizing Multiple Myeloma Value for Patients and Plans C. Daniel Mullins, PhD Professor Pharmaceutical Health Services Research Department University
Pharmacoeconomic Analyses and Oncology Pharmacy: Optimizing Multiple Myeloma Value for Patients and Plans C. Daniel Mullins, PhD Professor Pharmaceutical Health Services Research Department University
January 2013 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW. Summary. Contents
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/paclitaxel for cancer Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/ paclitaxel for
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/paclitaxel for cancer Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/ paclitaxel for
A Clinical Primer. for Managed Care Stakeholders
 reviews therapy Diagnosing, Staging, and Treating Multiple Myeloma: A Clinical Primer for Managed Care Stakeholders by Ralph V. Boccia, MD, FACP, Medical Director, Center for Cancer and Blood Disorders
reviews therapy Diagnosing, Staging, and Treating Multiple Myeloma: A Clinical Primer for Managed Care Stakeholders by Ralph V. Boccia, MD, FACP, Medical Director, Center for Cancer and Blood Disorders
FIFTEEN YEARS OF SINGLE CENTER EXPERIENCE WITH STEM CELL TRANSPLANTATION FOR MULTIPLE MYELOMA: A RETROSPECTIVE ANALYSIS
 ORIGINAL ARTICLE FIFTEEN YEARS OF SINGLE CENTER EXPERIENCE WITH STEM CELL TRANSPLANTATION FOR MULTIPLE MYELOMA: A RETROSPECTIVE ANALYSIS Jakub Radocha, Vladimír Maisnar, Alžběta Zavřelová, Melanie Cermanová,
ORIGINAL ARTICLE FIFTEEN YEARS OF SINGLE CENTER EXPERIENCE WITH STEM CELL TRANSPLANTATION FOR MULTIPLE MYELOMA: A RETROSPECTIVE ANALYSIS Jakub Radocha, Vladimír Maisnar, Alžběta Zavřelová, Melanie Cermanová,
Should we use Docetaxel in hormone- naïve prostate cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
 Should we use Docetaxel in hormone- naïve prostate cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards/honorarium from: Amgen, Astellas,
Should we use Docetaxel in hormone- naïve prostate cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards/honorarium from: Amgen, Astellas,
Multicenter, Randomized Trial in Newly Diagnosed Multiple Myeloma Patients Older Than 65 Years (GEM05>65)
") Multicenter, Randomized Trial in Newly Diagnosed Multiple Myeloma Patients Older Than 65 Years (GEM05>65) MV Mateos, A Oriol, J Martínez, MT Cibeira, R de Paz, MJ Terol, J García-Laraña, E Bengoechea,
Multicenter, Randomized Trial in Newly Diagnosed Multiple Myeloma Patients Older Than 65 Years (GEM05>65) MV Mateos, A Oriol, J Martínez, MT Cibeira, R de Paz, MJ Terol, J García-Laraña, E Bengoechea,
RELAPSED/REFRACTORY MULTIPLE MYELOMA: THE CURRENT STATE OF PLAY
 RELAPSED/REFRACTORY MULTIPLE MYELOMA: THE CURRENT STATE OF PLAY *María-Victoria Mateos, Enrique M. Ocio, Verónica González, Julio Dávila University Hospital of Salamanca/IBSAL, Salamanca, Spain *Correspondence
RELAPSED/REFRACTORY MULTIPLE MYELOMA: THE CURRENT STATE OF PLAY *María-Victoria Mateos, Enrique M. Ocio, Verónica González, Julio Dávila University Hospital of Salamanca/IBSAL, Salamanca, Spain *Correspondence
Effects of bortezomib on the prognosis of the newlydiagnosed multiple myeloma patients with renal impairment
 African Journal of Pharmacy and Pharmacology Vol. 6(11), pp. 793-797, 22 March, 2012 Available online at http://www.academicjournals.org/ajpp DOI: 10.5897/AJPP11.530 ISSN 1996-0816 2012 Academic Journals
African Journal of Pharmacy and Pharmacology Vol. 6(11), pp. 793-797, 22 March, 2012 Available online at http://www.academicjournals.org/ajpp DOI: 10.5897/AJPP11.530 ISSN 1996-0816 2012 Academic Journals
OI PARP ΑΝΑΣΤΟΛΕΙΣ ΣΤΟΝ ΚΑΡΚΙΝΟ ΤΟΥ ΜΑΣΤΟΥ ΝΙΚΟΛΑΙΔΗ ΑΔΑΜΑΝΤΙΑ ΠΑΘΟΛΟΓΟΣ-ΟΓΚΟΛΟΓΟΣ Β ΟΓΚΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΝΟΣ. ΜΗΤΕΡΑ
 OI PARP ΑΝΑΣΤΟΛΕΙΣ ΣΤΟΝ ΚΑΡΚΙΝΟ ΤΟΥ ΜΑΣΤΟΥ ΝΙΚΟΛΑΙΔΗ ΑΔΑΜΑΝΤΙΑ ΠΑΘΟΛΟΓΟΣ-ΟΓΚΟΛΟΓΟΣ Β ΟΓΚΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΝΟΣ. ΜΗΤΕΡΑ Study Overview Inhibition of poly(adenosine diphosphate [ADP]-ribose) polymerase
OI PARP ΑΝΑΣΤΟΛΕΙΣ ΣΤΟΝ ΚΑΡΚΙΝΟ ΤΟΥ ΜΑΣΤΟΥ ΝΙΚΟΛΑΙΔΗ ΑΔΑΜΑΝΤΙΑ ΠΑΘΟΛΟΓΟΣ-ΟΓΚΟΛΟΓΟΣ Β ΟΓΚΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΝΟΣ. ΜΗΤΕΡΑ Study Overview Inhibition of poly(adenosine diphosphate [ADP]-ribose) polymerase
Long Term Low Dose Maintenance Chemotherapy in the Treatment of Acute Myeloid Leukemia
 Long Term Low Dose Chemotherapy in the Treatment of Acute Myeloid Leukemia Murat TOMBULO LU*, Seçkin ÇA IRGAN* * Department of Hematology, Faculty of Medicine, Ege University, zmir, TURKEY ABSTRACT In
Long Term Low Dose Chemotherapy in the Treatment of Acute Myeloid Leukemia Murat TOMBULO LU*, Seçkin ÇA IRGAN* * Department of Hematology, Faculty of Medicine, Ege University, zmir, TURKEY ABSTRACT In
Multiple Myeloma and Amyloidosis: Optimism for Heretofore Incurable Diseases
 Multiple Myeloma and Amyloidosis: Optimism for Heretofore Incurable Diseases Robert Vescio, MD Director Multiple Myeloma & Bone Metastases Program Samuel Oschin Comprehensive Cancer Center Cedars-Sinai
Multiple Myeloma and Amyloidosis: Optimism for Heretofore Incurable Diseases Robert Vescio, MD Director Multiple Myeloma & Bone Metastases Program Samuel Oschin Comprehensive Cancer Center Cedars-Sinai
Clinical Spotlight in Breast Cancer
 2015 European Oncology Congress in Vienna Clinical Spotlight in Breast Cancer Reference Slide Deck Abstract #1815 Impact of Palbociclib Plus Fulvestrant on Global QOL, Functioning, and Symptoms Compared
2015 European Oncology Congress in Vienna Clinical Spotlight in Breast Cancer Reference Slide Deck Abstract #1815 Impact of Palbociclib Plus Fulvestrant on Global QOL, Functioning, and Symptoms Compared
Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases
 Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases R. Shraddha, P.N. Pandit Radium Institute, Patna Medical College and Hospital, Patna, India Abstract NHL is a highly
Role of taxanes in the treatment of advanced NHL patients: A randomized study of 87 cases R. Shraddha, P.N. Pandit Radium Institute, Patna Medical College and Hospital, Patna, India Abstract NHL is a highly
Evolving Management of Multiple Myeloma: 2015. Todd M. Zimmerman, M.D. Associate Professor of Medicine Section of Hematology/Oncology
 Evolving Management of Multiple Myeloma: 2015 Todd M. Zimmerman, M.D. Associate Professor of Medicine Section of Hematology/Oncology MULTIPLE MYELOMA Estimated 24,050 cases and 11,090 deaths in 2014 [1]
Evolving Management of Multiple Myeloma: 2015 Todd M. Zimmerman, M.D. Associate Professor of Medicine Section of Hematology/Oncology MULTIPLE MYELOMA Estimated 24,050 cases and 11,090 deaths in 2014 [1]
Multiple Myeloma Workshop- Tandem 2014
 Multiple Myeloma Workshop- Tandem 2014 1) Review of Plasma Cell Disorders Asymptomatic (smoldering) myeloma M-protein in serum at myeloma levels (>3g/dL); and/or 10% or more clonal plasma cells in bone
Multiple Myeloma Workshop- Tandem 2014 1) Review of Plasma Cell Disorders Asymptomatic (smoldering) myeloma M-protein in serum at myeloma levels (>3g/dL); and/or 10% or more clonal plasma cells in bone
Outline. Question 1. Question 2. What is Multiple Myeloma? Andrew Eisenberger, MD
 Outline A Disease Overview June 3, 2013 Andrew Eisenberger, MD Assistant Professor of Medicine Hematology/Oncology Columbia Presbyterian Medical Center Introduction Epidemiology/Risk Factors Clinical Features/Diagnostic
Outline A Disease Overview June 3, 2013 Andrew Eisenberger, MD Assistant Professor of Medicine Hematology/Oncology Columbia Presbyterian Medical Center Introduction Epidemiology/Risk Factors Clinical Features/Diagnostic
Bendamustine with rituximab for the first-line treatment of advanced indolent non-hodgkin's and mantle cell lymphoma
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Bendamustine with rituximab for the first-line treatment of advanced indolent non-hodgkin's and mantle cell lymphoma Bendamustine with rituximab for the first-line
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Bendamustine with rituximab for the first-line treatment of advanced indolent non-hodgkin's and mantle cell lymphoma Bendamustine with rituximab for the first-line
NATIONAL CANCER INSTITUTE. Lenalidomide or Observation in Treating Patients With Asymptomatic High-Risk Smoldering Multiple Myeloma
 NATIONAL CANCER INSTITUTE Lenalidomide or Observation in Treating Patients With Asymptomatic High-Risk Smoldering Multiple Myeloma Basic Trial Information Phase Type Status Age Sponsor Protocol IDs Phase
NATIONAL CANCER INSTITUTE Lenalidomide or Observation in Treating Patients With Asymptomatic High-Risk Smoldering Multiple Myeloma Basic Trial Information Phase Type Status Age Sponsor Protocol IDs Phase
Therapie des Patienten mit rezidiviertem Multiplem Myelom
 DGHO 2014, Hamburg Therapie des Patienten mit rezidiviertem Multiplem Myelom Martin Gramatzki Division for Stem Cell Transplantation and Immunotherapy, Department of Medicine II, University of Kiel, Kiel,
DGHO 2014, Hamburg Therapie des Patienten mit rezidiviertem Multiplem Myelom Martin Gramatzki Division for Stem Cell Transplantation and Immunotherapy, Department of Medicine II, University of Kiel, Kiel,
NOUVEAUTES THERAPEUTIQUES DANS LES TUMEURS NEUROENDOCRINES DIGESTIVES (Radiothérapie vectorisée et loco-régionale exclue) Philippe RUSZNIEWSKI
 Philippe RUSZNIEWSKI") NOUVEAUTES THERAPEUTIQUES DANS LES TUMEURS NEUROENDOCRINES DIGESTIVES (Radiothérapie vectorisée et loco-régionale exclue) Réunion APRAMEN, Paris, 2 février 2013 Philippe RUSZNIEWSKI Pôle des Maladies de
NOUVEAUTES THERAPEUTIQUES DANS LES TUMEURS NEUROENDOCRINES DIGESTIVES (Radiothérapie vectorisée et loco-régionale exclue) Réunion APRAMEN, Paris, 2 février 2013 Philippe RUSZNIEWSKI Pôle des Maladies de
Cancer Treatments Subcommittee of PTAC Meeting held 18 September 2015. (minutes for web publishing)
") Cancer Treatments Subcommittee of PTAC Meeting held 18 September 2015 (minutes for web publishing) Cancer Treatments Subcommittee minutes are published in accordance with the Terms of Reference for the
Cancer Treatments Subcommittee of PTAC Meeting held 18 September 2015 (minutes for web publishing) Cancer Treatments Subcommittee minutes are published in accordance with the Terms of Reference for the
Antiangiogenic Therapy In Breast Cancer
 Antiangiogenic Therapy In Breast Cancer Michele De Laurentiis UOC Oncologia Medica Senologica Istituto Nazionale Tumori Fondazione Pascale Napoli, Italia Judah Folkman 1971 Bevacizumab in MBC Ø Biologic
Antiangiogenic Therapy In Breast Cancer Michele De Laurentiis UOC Oncologia Medica Senologica Istituto Nazionale Tumori Fondazione Pascale Napoli, Italia Judah Folkman 1971 Bevacizumab in MBC Ø Biologic
Acute Myeloid Leukemia
 Acute Myeloid Leukemia Upfront Therapy in Newly Diagnosed Elderly AML Patients: Is Decitabine (DAC) the new standard? Raoul Tibes, MD, PhD Senior Associate Consultant, Mayo Clinic Arizona Associate Director,
Acute Myeloid Leukemia Upfront Therapy in Newly Diagnosed Elderly AML Patients: Is Decitabine (DAC) the new standard? Raoul Tibes, MD, PhD Senior Associate Consultant, Mayo Clinic Arizona Associate Director,
Stem Cell Transplantation for Multiple Myeloma: Current and Future Status
 CONTROVERSIES AND UPDATES IN MULTIPLE MYELOMA Stem Cell Transplantation for Multiple Myeloma: Current and Future Status Sergio Giralt 1 1 Memorial Sloan Kettering Cancer Center, New York, NY High-dose
CONTROVERSIES AND UPDATES IN MULTIPLE MYELOMA Stem Cell Transplantation for Multiple Myeloma: Current and Future Status Sergio Giralt 1 1 Memorial Sloan Kettering Cancer Center, New York, NY High-dose
Frequency of NHL Subtypes in Adults
 Chemotherapy Options Stephanie A. Gregory, M.D. The Elodia Kehm Professor of Medicine Director, Section of Hematology Rush University Medical Center Chicago, Illinois Frequency of NHL Subtypes in Adults
Chemotherapy Options Stephanie A. Gregory, M.D. The Elodia Kehm Professor of Medicine Director, Section of Hematology Rush University Medical Center Chicago, Illinois Frequency of NHL Subtypes in Adults
DARATUMUMAB, A CD38 MONOCLONAL ANTIBODY IN PATIENTS WITH MULTIPLE MYELOMA - DATA FROM A DOSE- ESCALATION PHASE I/II STUDY
 DARATUMUMAB, A CD38 MONOCLONAL ANTIBODY IN PATIENTS WITH MULTIPLE MYELOMA - DATA FROM A DOSE- ESCALATION PHASE I/II STUDY Torben Plesner, Henk Lokhorst, Peter Gimsing, Hareth Nahi, Steen Lisby, Paul Richardson
DARATUMUMAB, A CD38 MONOCLONAL ANTIBODY IN PATIENTS WITH MULTIPLE MYELOMA - DATA FROM A DOSE- ESCALATION PHASE I/II STUDY Torben Plesner, Henk Lokhorst, Peter Gimsing, Hareth Nahi, Steen Lisby, Paul Richardson
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
If several different trials are mentioned in one publication, the data of each should be extracted in a separate data extraction form.
 General Remarks This template of a data extraction form is intended to help you to start developing your own data extraction form, it certainly has to be adapted to your specific question. Delete unnecessary
General Remarks This template of a data extraction form is intended to help you to start developing your own data extraction form, it certainly has to be adapted to your specific question. Delete unnecessary
Prior Authorization Guideline
 Prior Authorization Guideline Guideline: PS Inj - Alimta Therapeutic Class: Antineoplastic Agents Therapeutic Sub-Class: Antifolates Client: PS Inj Approval Date: 8/2/2004 Revision Date: 12/5/2006 I. BENEFIT
Prior Authorization Guideline Guideline: PS Inj - Alimta Therapeutic Class: Antineoplastic Agents Therapeutic Sub-Class: Antifolates Client: PS Inj Approval Date: 8/2/2004 Revision Date: 12/5/2006 I. BENEFIT
Health Disparities in Multiple Myeloma. Kenneth R. Bridges, M.D. Senior Medical Director Onyx Pharmaceuticals, Inc.
 Health Disparities in Multiple Myeloma Kenneth R. Bridges, M.D. Senior Medical Director Onyx Pharmaceuticals, Inc. Multiple Myeloma Overview Multiple myeloma (MM) is a type of blood cancer that develops
Health Disparities in Multiple Myeloma Kenneth R. Bridges, M.D. Senior Medical Director Onyx Pharmaceuticals, Inc. Multiple Myeloma Overview Multiple myeloma (MM) is a type of blood cancer that develops
Laura Biganzoli Oncologia Medica Nuovo Ospedale di Prato Istituto Toscano Tumori
 EFFECT: A randomized phase II study to evaluate the EFficacy and impact on Function of two different doses of nabpaclitaxel in elderly patients with advanced breast cancer Laura Biganzoli Oncologia Medica
EFFECT: A randomized phase II study to evaluate the EFficacy and impact on Function of two different doses of nabpaclitaxel in elderly patients with advanced breast cancer Laura Biganzoli Oncologia Medica
Are CAR T-Cells the Solution for Chemotherapy Refractory Diffuse Large B-Cell Lymphoma? Umar Farooq, MD University of Iowa Hospitals and Clinics
 Are CAR T-Cells the Solution for Chemotherapy Refractory Diffuse Large B-Cell Lymphoma? Umar Farooq, MD University of Iowa Hospitals and Clinics Disclosure(s) I do not intend to discuss an off-label use
Are CAR T-Cells the Solution for Chemotherapy Refractory Diffuse Large B-Cell Lymphoma? Umar Farooq, MD University of Iowa Hospitals and Clinics Disclosure(s) I do not intend to discuss an off-label use
Personalized, Targeted Treatment Options Offer Hope of Multiple Myeloma as a Chronic Disease
 /publications/targeted-therapy-news/2012/november-2012/personalized-targeted-treatment-options- Offer-Hope-of-Multiple-Myeloma-as-a-Chronic-Disease Personalized, Targeted Treatment Options Offer Hope of
/publications/targeted-therapy-news/2012/november-2012/personalized-targeted-treatment-options- Offer-Hope-of-Multiple-Myeloma-as-a-Chronic-Disease Personalized, Targeted Treatment Options Offer Hope of
IMMUNOMEDICS, INC. February 2016. Advanced Antibody-Based Therapeutics. Oncology Autoimmune Diseases
 IMMUNOMEDICS, INC. Advanced Antibody-Based Therapeutics Oncology Autoimmune Diseases February 2016 Forward-Looking Statements This presentation, in addition to historical information, contains certain
IMMUNOMEDICS, INC. Advanced Antibody-Based Therapeutics Oncology Autoimmune Diseases February 2016 Forward-Looking Statements This presentation, in addition to historical information, contains certain
CI-1. DACOGEN (decitabine) United States Food and Drug Administration Oncologic Drugs Advisory Committee February 9, 2012 NDA #21790/S-010
 United States Food and Drug Administration Oncologic Drugs Advisory Committee February 9, 2012 NDA #21790/S-010") CI-1 DACOGEN (decitabine) United States Food and Drug Administration Oncologic Drugs Advisory Committee February 9, 2012 NDA #21790/S-010 CI-2 Introduction Alton Kremer, MD, PhD Senior Vice President,
CI-1 DACOGEN (decitabine) United States Food and Drug Administration Oncologic Drugs Advisory Committee February 9, 2012 NDA #21790/S-010 CI-2 Introduction Alton Kremer, MD, PhD Senior Vice President,
Approccio multidisciplinare nel carcinoma della vescica. D. Amoroso Dip. di Oncologia Medica Ospedale Versilia Lido di Camaiore (LU)
") Approccio multidisciplinare nel carcinoma della vescica D. Amoroso Dip. di Oncologia Medica Ospedale Versilia Lido di Camaiore (LU) Disclosures Advisory Role, Honoraria: ü Roche ü Italfarmaco Outline v
Approccio multidisciplinare nel carcinoma della vescica D. Amoroso Dip. di Oncologia Medica Ospedale Versilia Lido di Camaiore (LU) Disclosures Advisory Role, Honoraria: ü Roche ü Italfarmaco Outline v
Achieving Complete Response in Multiple Myeloma: Do We Need to Change the Definition?
 內 科 學 誌 2011:22:266-277 Achieving Complete Response in Multiple Myeloma: Do We Need to Change the Definition? Wen-Chi Yang, and Sheng-Fung Lin Hematology-Oncology Division, Department of Internal Medicine,
內 科 學 誌 2011:22:266-277 Achieving Complete Response in Multiple Myeloma: Do We Need to Change the Definition? Wen-Chi Yang, and Sheng-Fung Lin Hematology-Oncology Division, Department of Internal Medicine,
Multiple Myeloma Making Sense of the Report Forms. Parameswaran Hari Medical College of Wisconsin Milwaukee
 Hodgkin CML MDS/Other Leuk CLL Neuroblastoma Multiple Myeloma Making Sense of the Report Forms Parameswaran Hari Medical College of Wisconsin Milwaukee Indications for Blood and Marrow Transplantation
Hodgkin CML MDS/Other Leuk CLL Neuroblastoma Multiple Myeloma Making Sense of the Report Forms Parameswaran Hari Medical College of Wisconsin Milwaukee Indications for Blood and Marrow Transplantation
Low dose capecitabine is effective and relatively nontoxic in breast cancer treatment.
 1 Low dose capecitabine is effective and relatively nontoxic in breast cancer treatment. John T. Carpenter, M.D. University of Alabama at Birmingham NP 2508 1720 Second Avenue South Birmingham, AL 35294-3300
1 Low dose capecitabine is effective and relatively nontoxic in breast cancer treatment. John T. Carpenter, M.D. University of Alabama at Birmingham NP 2508 1720 Second Avenue South Birmingham, AL 35294-3300
Bortezomib, melphalan, prednisone, and thalidomide for relapsed multiple myeloma
 CLINICAL TRIALS AND OBSERVATIONS Bortezomib, melphalan, prednisone, and thalidomide for relapsed multiple myeloma Antonio Palumbo, 1 Maria Teresa Ambrosini, 1 Giulia Benevolo, 2 Patrizia Pregno, 2 Norbert
CLINICAL TRIALS AND OBSERVATIONS Bortezomib, melphalan, prednisone, and thalidomide for relapsed multiple myeloma Antonio Palumbo, 1 Maria Teresa Ambrosini, 1 Giulia Benevolo, 2 Patrizia Pregno, 2 Norbert