A New Biomarker in Prostate Cancer Care: Oncotype Dx. David M Albala, MD Chief of Urology Crouse Hospital Syracuse, NY
|
|
|
- Nicholas McDonald
- 8 years ago
- Views:
Transcription

1 A New Biomarker in Prostate Cancer Care: Oncotype Dx David M Albala, MD Chief of Urology Crouse Hospital Syracuse, NY
2 Learning Objectives Review the current challenges in the prediction and prognosis of prostate cancer Review current means for predicting prostate cancer aggressiveness Review current available diagnostic tests via genetic signatures Understand and interpret the results and clinical relevance of these predictive systems
3 Clinical Staging Alone Not Adequate for Prognosis +DRE (digital rectal exam) +PSA (prostate specific antigen) +Gleason Score +Clinical Stage 80% predictive diagnostic accuracy
4 Prostatic Adenocarcinoma Morphologic resemblance to normal prostate Degree of invasiveness Score = most + 2nd most Gleason Grading ISUP 2 : Grading biopsies: Most + highest remaining grade present Grades 1&2 should not be used (most upgraded or found to be benign on RP) Score ranges from Gleason DF. Urologic Pathology: The Prostate, ISUP: Amer J Surg Pathol, 2005.
5 The Current Treatment Paradigm Shift Early PSA Era Screen & Treat Everybody Today Don t Screen and Don t Treat Anyone The Challenge and Goal is to Balance: Age and health of the patient Risk of having aggressive cancer Biologic potential of the tumor Patient and family desire
6 Clinical Need in Localized Prostate Cancer Over-diagnosis and over-treatment Limited confidence in existing risk stratification Low-risk disease can be safely managed with AS AS under-utilized despite guidelines
7 Percentage (%) Percentage (%) Current State of Low Risk Prostate Cancer Incidence/Risk 1-7 % Newly Diagnosed Low Risk % Lifetime Risk of Progression and Death 46% Low Risk 3% 100 Surveillance Outcomes: n = 3,762; PCSS 99.4% 9 WW, watchful waiting; AS, active surveillance. 1. Cooperberg, MR et al. J Clin Oncol; 23: , 2. Adapted from Cooperberg MR, et al. BJU Int; (3): ; 3. Cooperberg MR et al. J Clin Oncol. 2010;28(7): ; 4. Boorjian 2008; 5. Wilt TJ, et al. N Engl J Med. 2012;367(3):203-13; 6. Damber 2008; 7. Ploussard 2011; 8. Cooperberg, MR et al. Western AUA Poster 09-40, 9. Glass AS, et al. J Natl Cancer Inst 2012(45): % Treatment 1-8 Low Risk % Immediate Treatment % AS/WW 37 %
8 Clear Need and Opportunity to Improve Prostate Cancer Management Driver of over treatment is limited accuracy of low risk classification based on measures available today Despite low (3%) risk of disease progression 1 and modest treatment benefit 2, >90% 3 of low risk men receive immediate treatment We desperately need the ability to predict which patient has a localized cancer that is going to metastasize and cause suffering and death, and which patient has a cancer that is destined to stay in the patient's prostate for the remainder of his life. -American Cancer Society 4 1. Boorjian SA, et al. Urol Oncol 2008; 2. Wilt TJ, et al. N Engl J Med. 2012; 3. Cooperberg MR et al. J Clin Oncol 2010; 4. Otis W. Brawley, MD, American Cancer Society
9 Treatment Decisions in Prostate Cancer Currently urologists use prostate cancer risk to help guide treatment decisions What risk group is your cancer? Very low risk Low risk Intermediate risk High risk
 Anxiety Patient, family, doctors Economic/Professional Doctors get trained & paid to treat, not watch Legal Failure to diagnose or")
10 What are the Barriers to Adopting Surveillance Uncertainties in clinical tools to predict True biologic potential at diagnosis True biologic progression after initiating surveillance ( when to pull the trigger ) Anxiety Patient, family, doctors Economic/Professional Doctors get trained & paid to treat, not watch Legal Failure to diagnose or cure
11 NCCN Pathway for Very Low Risk CAP RISK GROUP EXPECTED PATIENT SURVIVAL 20 y INITIAL THERAPY Active surveillance g PSA no more often than every 6 mo unless clinically indicated DRE no more often than every 12 mo unless clinically indicated Repeat prostate biopsy no more often than every 12 mo unless clinically indicated EBRT or brachytherapy Very low T1c Gleason score 6 PSA < 10 ng/ml Fewer than 3 prostate biopsy cores positive, 50% cancer in each core PSA density < 0.15 ng/ml/g y < 10 y Radical prostatectomy (RP) ± pelvic lymph node dissection (PLND) if predicted probability of lymph node metastasis 2% Active surveillance g PSA no more often than every 6 mo unless clinically indicated DRE no more often than every 12 mo unless clinically indicated Repeat prostate biopsy no more often than every 12 mo unless clinically indicated Observation g Active surveillance involves actively monitoring the course of disease with the expectation to intervene with potentially curative therapy if the cancer progresses. See Principles of Active Surveillance and Observation (PROS-C). NCCN Clinical Practice Guidelines in Oncology, Prostate Cancer v National Comprehensive Cancer Network, 2015
12 NCCN Pathway for Low Risk CAP RISK GROUP EXPECTE D PATIENT SURVIVAL 10 y INITIAL THERAPY Active surveillance g PSA no more often than every 6 mo unless clinically indicated DRE no more often than every 12 mo unless clinically indicated Repeat prostate biopsy no more often than every 12 mo unless clinically indicated EBRT or brachytherapy Low T1-T2a Gleason score 6 PSA < 10 ng/ml RP + PLND if predicted probability of lymph node metastasis 2% < 10 y Observation g Active surveillance involves actively monitoring the course of disease with the expectation to intervene with potentially curative therapy if the cancer progresses. See Principles of Active Surveillance and Observation (PROS-C). NCCN Clinical Practice Guidelines in Oncology, Prostate Cancer v National Comprehensive Cancer Network, 2015
13 NCCN Pathway for Intermediate Risk CAP NCCN Clinical Practice Guidelines in Oncology, Prostate Cancer v National Comprehensive Cancer Network, 2013 NCCN is a registered trademark of the National Comprehensive Cancer Network, which does not endorse any product or therapy.
14 NCCN Clinical Practice Guidelines in Oncology, Prostate Cancer v National Comprehensive Cancer Network, NCCN Guidelines Describe Use of Molecular Diagnostics for Initial Prostate Cancer Diagnosis INITIAL PROSTATE CANCER DIAGNOSIS DRE PSA Gleason primary and secondary grade Life expectancy 5 y and asymptomatic Life expectancy > 5 y or asymptomatic b Preferred treatment for any therapy is approved clinical trial. INITIAL CLINICAL ASSESSMENT STAGING WORKUP No further workup or treatment until symptomatic, except in high- or very-high-risk groups Bone scan if any of these: T1 and PSA > 20 T2 and PSA > 10 Gleason score 8 T3, T4 Symptomatic Pelvic CT or MRI if any of these: T3, T4 T1-T2 and nomogram indicated probability of lymph node involvement > 10% All others: no additional imaging Suspiciou s nodes Consider biopsy RISK GROUP Clinically Localized: Very low T1c Gleason score 6 PSA < 10 ng/ml Fewer than 3 prostate biopsy cores positive, 50% cancer in each core PSA density < 0.15 ng/ml/g Low T1-T2a Gleason score 6 PSA < 10 ng/ml Intermediate d T2b-T2c or Gleason score 7 or PSA ng/ml b Men with clinically localized disease could consider use of a tumor-based molecular assay to stratify better risk of adverse pathology at radical prostatectomy or chance of biochemical recurrence or disease-specific mortality after radical prostatectomy.
15 Ideal Prognostic Test Easily obtained specimen Accurately stratifies risk by meaningful endpoints Prostate specific survival Recurrence Provides significant independent information Provides actionable information

16 Landscape of PCa Genomic Analyses

17 The Promise of Genomics Unfavorable Biology Intermediate Risk Clinical Risk Groups Very Low Low Intermediate Favorable Biology Very Low Risk INDIVIDUAL RISK
 to help guide initial treatment decisions at the time of biopsy WHO is the test for?")
18 The Oncotype DX Prostate Cancer Assay WHAT is the test? A tumor gene expression assay which produces a Genomic Prostate Score (GPS) to help guide initial treatment decisions at the time of biopsy WHO is the test for? Men with low to low-intermediate risk prostate cancer (GS 3+3, low volume 3+4) WHY do the test? To improve risk stratification by incorporating individual underlying tumor biology To identify appropriate patients for Active Surveillance (AS) or immediate treatment HOW are the results reported? Favorable Pathology: freedom from high-grade (dominant pattern 4 or any pattern 5) and/or non-organ-confined disease

19 Gene Selection for the Oncotype DX GPS Assay 727 candidate genes in dominant Gleason samples 374 genes predict outcome (dominant) 288 genes predictive regardless of sampled Gleason pattern 288 Genes Consistent performance in biopsies Predict PC death, adv. path, BCR Value beyond existing measures Represent key pathways Analytical performance 727 candidate genes in highest Gleason samples 367 genes predict outcome (highest) PC, prostate cancer; BCR, biochemical recurrence. Final 17 GPS Genes

20 GPS Incorporates Multiple Biologic Pathways Predictive of Prostate Cancer Aggressiveness The combination of multiple pathways is more predictive than any single pathway Genes Associated with Worse Outcome Stromal Response BGN COL1A1 SFRP4 Proliferation TPX2 Genes Associated with Better Outcome Androgen Signaling AZGP1 FAM13C KLK2 SRD5A2 Cellular Organization FLNC GSN GSTM2 TPM2 Reference Genes ARF1 ATP5E CLTC GPS1 PGK1 Genes were selected for performance in biopsies and prediction of PC death, adverse pathology, and BCR Klein, Cooperberg et al, Euro Urol (2014).
21 Clinical Development, Validation and Utility Prostatectomy Cancer Feasibility Studies (n=104) Prostatectomy Study (n=441) Endpoints: Clinical Recurrence, Biochemical Recurrence, Prostate Cancer Death, Adverse Pathology at RP Biopsy Development Study #1 (n=167) Endpoint: Prediction of Adverse Pathology at RP Selection of Final Gene List & Algorithm Standardization and Validation of Analytical Methods Clinical Validation Study #1 (n=395) Endpoint: Prediction of Adverse Pathology at RP Clinical Validation Study #2 (n=402) Endpoints: Biochemical Recurrence (n=402), Prediction of Adverse Pathology at RP (n=382), Metastasis (n=402) Clinical Utility Study #1: Decision Impact (n=158) Objectives: To validate GPS as a predictor of adverse pathology in a contemporary clinically low risk patient cohort To determine whether GPS adds independent predictive information beyond standard clinical and pathologic data Clinical Utility Study #2: Chart Pull (n=200) Klein, Cooperberg et al, Euro Urol (2014).
22 Contemporary Patient Population in UCSF Validation Study Clinical Characteristics of Patients Age at Diagnosis Race Mean Range Caucasian African American Other 58.3 years (91%) 13 ( 3%) 23 ( 6%) PSA 0-4 >4-10 > (21%) 262 (66%) 50 (13%) Clinical T-stage Central Biopsy Gleason Score Endpoint Grade/Stage at RP Klein, Cooperberg et al, Euro Urol (2014). T1c T2a T2b/c High Grade pt3 High Grade and/or pt3 228 (58%) 118 (30%) 49 (12%) 301 (76%) 94 (24%) 70 (18%) 87 (22%) 123 (31%)
23 Interpretation of Genomic Prostate Score NCCN Risk Group Likelihood of Favorable Pathology Very Low 80% Low 70% Intermediate 60% Tosoian et al, J Urol 190:1218, 2013
24 Likelihood of Favorable Pathology (%) Successful Validation of GPS: Improved Risk Discrimination with Addition of GPS to NCCN NCCN Very Low = 84% NCCN Low = 75% NCCN Low-Intermediate = 56% Low Very Low Multivariate Analysis NCCN p-value = GPS p-value = Low-Intermediate Very Low Low Low-Intermediate GPS Cooperberg et al, AUA 2013
25 Combining Biologic & Clinical Information Refines Risk Stratification for Individual Patients Population-Based Clinical Risk Assessment VERY LOW RISK 10% (N=37) LOW RISK LOW-INTERMEDIATE 49% (N=191) 41% RISK (N=160) More Individualized Biologic and Clinical Risk Assessment VERY LOW RISK LOW RISK LOW-INTERMEDIATE RISK 26% (N=100) 31% (N=119) 44% (N=169) GPS=8 84% GPS Provides Biologic Risk Information GPS=25 75% GPS=51 57% UCSF GPS Validation Study NCCN Risk Classification Precisely Adds Predicted 35% Enables Identified 10% of more men more identifies patients which accurate in the with in a patient s risk patients accurate Intermediate NCCN the NCCN assessment Low-risk have tumor identification Very risk biology Low- group by who combining consistent with biological their and of had 10% risk a group refines larger more indolent Very aggressive who population Low-risk the had and NCCN clinical clinical risk risk population-based of biology, 49% more patients aggressive Low-risk and predicted who likelihood can to be biology, with likelihood factors group consistent pathology clinical more 41% of favorable confidently with Lowrisk disease of favorable Intermediate risk pathology Risk consistent assessment choose pathology consistent active consistent with with with Very Low a more Low-risk surveillance with and Intermediate personalized risk risk assessment disease 100% 30% Likelihood of Favorable Pathology Cooperberg et al, AUA 2013
26 CPDR Validation Study Clinical Characteristics Representative of a Contemporary Patient Population Age at Diagnosis Clinical Characteristics of Patients Mean Range Race Caucasian African-American Other PSA < Clinical T-Stage T1 T2 Biopsy Gleason Score NCCN Risk Group Very Low Low Intermediate 61 years (76%) 82 (20%) 15 ( 4%) 92 (23%) 273 (68%) 37 ( 9%) 276 (69%) 126 (31%) 295 (73%) 94 (23%) 13 ( 3%) 43 (11%) 210 (54%) 139 (36%) Distribution of baseline characteristics was representative of a contemporarily managed population of men with prostate cancer Cullen J, et al. Eur Urol
27 GP S GPS Predicts AP and BCR Across Different Racial Groups Tumor aggressiveness, as measured by GPS, was similar between races Caucasian African-American Other Event Race Variable N OR 95% CI P-value Adverse Pathology Caucasian Race N GPS Median Caucasian African American 82 Other African- American GPS per 20 units GPS per 20 units ( ) < ( ) Event Race Variable N HR 95% CI P-value BCR GPS was predictive of outcome in both Caucasian and African- American men Caucasian African- American GPS per 20 units GPS per 20 units (2.00, 4.33) < (1.02, 11.74) Cullen J, et al. Eur Urol
28 Validation Studies Adds independent predictive information beyond standard clinical and pathological measures Predicted multiple clinically relevant endpoints (AP, BCR) Tumor aggressiveness was similar between white and black men
29 Clinical Utility Study #1: Confidence and Utility Confidence (N=158) Utility (N=158) Strongly Agree 25% Extremely Useful 21% Agree 36% Useful 35% Somewhat Agree 24% Somewhat Useful 22% Neither Agree nor Disagree 7% Neither 6% Somewhat Disagree 2% Somewhat Not Useful 7% Disagree 6% Not Useful 9% Strongly Disagree Not at All Useful In 85% of patients, physicians indicated increased confidence in their treatment recommendations In 78% of patients, physicians found the GPS useful in making treatment recommendations Badani et al, SUO 2014
30
31 GPS Case Study 59 year-old patient PSA: 5.2 Gleason Score: 3+3=6 Number of cores positive/collected: 3/12 >50% tumor involvement in any core: No Stage: T1c PSA Density: 0.13 Life Expectancy: 25 yrs. Initial Clinical Risk (NCCN): Low Pre GPS Recommendation: Undecided GPS RESULTS GPS of 10: NCCN Very Low Likelihood of favorable pathology: 83% Post GPS Recommendation: AS and patient agreed.
32 General Conclusions Current tests harness the power of biology and genomics to provide a more precise and accurate assessment of risk based on individual tumor biology Validated in large studies and can be used along with established clinical and pathological parameters to define prediction and prognosis of PCa behavior for each patient. Further collection of data and introducing new assays to search different pathways and signatures of individual cancers may lead to significant breakthrough in personalized oncology approach.

33 Active Surveillance v. 2.0 Current Paradigm Genomic Based Paradigm Initial Bx & Risk Categorization Comorbidity & Life Expectancy Patient desire No change Re-biopsy to improve accuracy of risk classification Periodic re-evaluation for change in risk categorization Reduce burden of determining eligibility - Substitute a biomarker for a 2nd biopsy Improve patient selection - Favorable score: Increase confidence that AS is safe - Unfavorable score: Increase acceptance that RX is warranted Change intensity of monitoring - Favorable score Less intense - Unfavorable score More intense Serial biologic monitoring Intervention Change in risk categorization Worry over PSA Patient desire Help decide when to pull the trigger for RX
34
Gleason Score. Oncotype DX GPS. identified for. about surveillance. time to get sophisticated
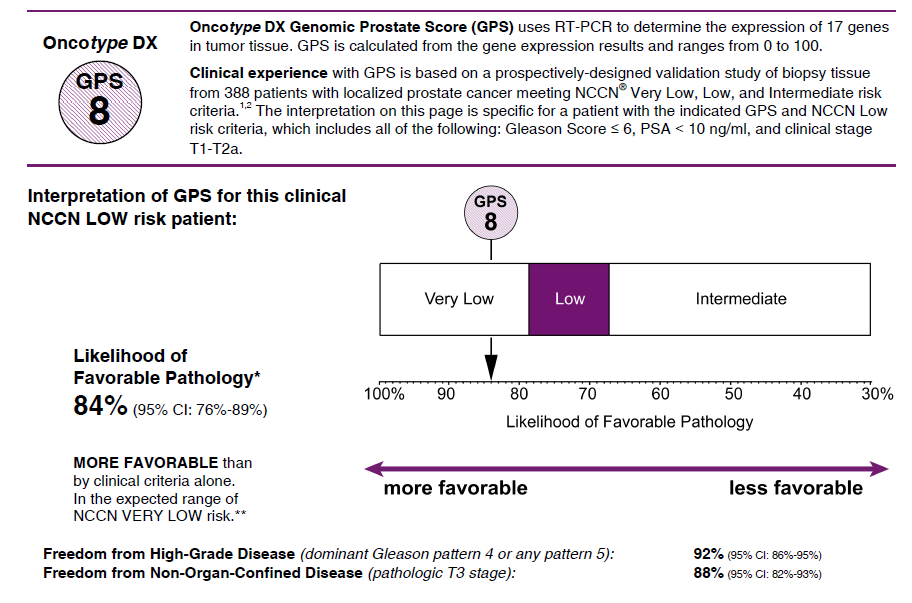
 patient: MARK SMITH PSA 6.2 Gleason Score 6 Oncotype DX GPS 8 identified for active surveillance time to get sophisticated about surveillance Accurate prediction of prostate cancer risk is needed at the
patient: MARK SMITH PSA 6.2 Gleason Score 6 Oncotype DX GPS 8 identified for active surveillance time to get sophisticated about surveillance Accurate prediction of prostate cancer risk is needed at the
Prostate Cancer 2014
 Prostate Cancer 2014 Eric A. Klein, M.D. Chairman Glickman Urological and Kidney Institute Professor of Surgery Cleveland Clinic Lerner College of Medicine Incidence rates, US Men Mortality Rates, US Men
Prostate Cancer 2014 Eric A. Klein, M.D. Chairman Glickman Urological and Kidney Institute Professor of Surgery Cleveland Clinic Lerner College of Medicine Incidence rates, US Men Mortality Rates, US Men
Local Coverage Determination (LCD): MolDX: Genomic Health Oncotype DX Prostate Cancer Assay (L36153)
: MolDX: Genomic Health Oncotype DX Prostate Cancer Assay (L36153)") Local Coverage Determination (LCD): MolDX: Genomic Health Oncotype DX Prostate Cancer Assay (L36153) Contractor Information Contractor Name Palmetto GBA LCD Information Document Information LCD ID L36153
Local Coverage Determination (LCD): MolDX: Genomic Health Oncotype DX Prostate Cancer Assay (L36153) Contractor Information Contractor Name Palmetto GBA LCD Information Document Information LCD ID L36153
MolDX: Genomic Health Oncotype DX Prostate Cancer Assay
 MolDX: Genomic Health Oncotype DX Prostate Cancer Assay Noridian Healthcare Solutions, LLC Close Please Note: This is a Proposed LCD. Proposed LCDs are works in progress and not necessarily a reflection
MolDX: Genomic Health Oncotype DX Prostate Cancer Assay Noridian Healthcare Solutions, LLC Close Please Note: This is a Proposed LCD. Proposed LCDs are works in progress and not necessarily a reflection
Beyond the PSA: Genomic Testing in Localized Prostate Cancer
 Beyond the PSA: Genomic Testing in Localized Prostate Cancer Kelvin A. Moses, MD, PhD Vanderbilt University Medical Center Wednesday, December 2, 2015 5:00 p.m. ET/2:00 p.m. PT About ZERO ZERO s mission
Beyond the PSA: Genomic Testing in Localized Prostate Cancer Kelvin A. Moses, MD, PhD Vanderbilt University Medical Center Wednesday, December 2, 2015 5:00 p.m. ET/2:00 p.m. PT About ZERO ZERO s mission
STATE OF MICHIGAN DEPARTMENT OF INSURANCE AND FINANCIAL SERVICES Before the Director of Insurance and Financial Services
 STATE OF MICHIGAN DEPARTMENT OF INSURANCE AND FINANCIAL SERVICES Before the Director of Insurance and Financial Services In the matter of: Petitioner, v Blue Care Network of Michigan, Respondent. File
STATE OF MICHIGAN DEPARTMENT OF INSURANCE AND FINANCIAL SERVICES Before the Director of Insurance and Financial Services In the matter of: Petitioner, v Blue Care Network of Michigan, Respondent. File
Historical Basis for Concern
 Androgens After : Are We Ready? Mohit Khera, MD, MBA Assistant Professor of Urology Division of Male Reproductive Medicine and Surgery Scott Department of Urology Baylor College of Medicine Historical
Androgens After : Are We Ready? Mohit Khera, MD, MBA Assistant Professor of Urology Division of Male Reproductive Medicine and Surgery Scott Department of Urology Baylor College of Medicine Historical
Analysis of Prostate Cancer at Easter Connecticut Health Network Using Cancer Registry Data
 The 2014 Cancer Program Annual Public Reporting of Outcomes/Annual Site Analysis Statistical Data from 2013 More than 70 percent of all newly diagnosed cancer patients are treated in the more than 1,500
The 2014 Cancer Program Annual Public Reporting of Outcomes/Annual Site Analysis Statistical Data from 2013 More than 70 percent of all newly diagnosed cancer patients are treated in the more than 1,500
Jurisdiction Virginia
 PROPOSED/DRAFT Local Coverage Determination (LCD): MolDX: Prolaris Prostate Cancer Genomic Assay (DL35629) Please note: This is a Proposed/Draft policy. Proposed/Draft LCDs are works in progress that are
PROPOSED/DRAFT Local Coverage Determination (LCD): MolDX: Prolaris Prostate Cancer Genomic Assay (DL35629) Please note: This is a Proposed/Draft policy. Proposed/Draft LCDs are works in progress that are
Newly Diagnosed Prostate Cancer: Understanding Your Risk
 Newly Diagnosed Prostate Cancer: Understanding Your Risk When the urologist calls with the life-changing news that your prostate biopsy is positive for prostate cancer, an office appointment is made to
Newly Diagnosed Prostate Cancer: Understanding Your Risk When the urologist calls with the life-changing news that your prostate biopsy is positive for prostate cancer, an office appointment is made to
Update on Prostate Cancer: Screening, Diagnosis, and Treatment Making Sense of the Noise and Directions Forward
 Update on Prostate Cancer: Screening, Diagnosis, and Treatment Making Sense of the Noise and Directions Forward 33 rd Annual Internal Medicine Update December 5, 2015 Ryan C. Hedgepeth, MD, MS Chief of
Update on Prostate Cancer: Screening, Diagnosis, and Treatment Making Sense of the Noise and Directions Forward 33 rd Annual Internal Medicine Update December 5, 2015 Ryan C. Hedgepeth, MD, MS Chief of
Robert Bristow MD PhD FRCPC
 Robert Bristow MD PhD FRCPC Clinician-Scientist and Professor, Radiation Oncology and Medical Biophysics, University of Toronto and Ontario Cancer Institute/ (UHN) Head, PMH-CFCRI Prostate Cancer Research
Robert Bristow MD PhD FRCPC Clinician-Scientist and Professor, Radiation Oncology and Medical Biophysics, University of Toronto and Ontario Cancer Institute/ (UHN) Head, PMH-CFCRI Prostate Cancer Research
Prostate Cancer Screening. Dr. J. McCracken, Urologist
 Prostate Cancer Screening Dr. J. McCracken, Urologist USPSTF Lifetime risk for diagnosis currently estimated at 15.9% Llifetime risk of dying of prostate cancer is 2.8% Seventy percent of deaths due to
Prostate Cancer Screening Dr. J. McCracken, Urologist USPSTF Lifetime risk for diagnosis currently estimated at 15.9% Llifetime risk of dying of prostate cancer is 2.8% Seventy percent of deaths due to
The 4Kscore blood test for risk of aggressive prostate cancer
 The 4Kscore blood test for risk of aggressive prostate cancer Prostate cancer tests When to use the 4Kscore Test? Screening Prior to 1 st biopsy Prior to negative previous biopsy Prognosis in Gleason 6
The 4Kscore blood test for risk of aggressive prostate cancer Prostate cancer tests When to use the 4Kscore Test? Screening Prior to 1 st biopsy Prior to negative previous biopsy Prognosis in Gleason 6
4/8/13. Pre-test Audience Response. Prostate Cancer 2012. Screening and Treatment of Prostate Cancer: The 2013 Perspective
 Pre-test Audience Response Screening and Treatment of Prostate Cancer: The 2013 Perspective 1. I do not offer routine PSA screening, and the USPSTF D recommendation will not change my practice. 2. In light
Pre-test Audience Response Screening and Treatment of Prostate Cancer: The 2013 Perspective 1. I do not offer routine PSA screening, and the USPSTF D recommendation will not change my practice. 2. In light
Does my patient need more therapy after prostate cancer surgery?
 Does my patient need more therapy after prostate cancer surgery? Contact the GenomeDx Patient Care Team at: 1.888.792.1601 (toll-free) or e-mail: client.service@genomedx.com Prostate Cancer Classifier
Does my patient need more therapy after prostate cancer surgery? Contact the GenomeDx Patient Care Team at: 1.888.792.1601 (toll-free) or e-mail: client.service@genomedx.com Prostate Cancer Classifier
The PSA Controversy: Defining It, Discussing It, and Coping With It
 The PSA Controversy: Defining It, Discussing It, and Coping With It 11 TH ANNUAL SYMPOSIUM ON MEN S HEALTH June 12, 2013 The PSA Controversy Defining It, Discussing It and Coping With It As of May 2012,
The PSA Controversy: Defining It, Discussing It, and Coping With It 11 TH ANNUAL SYMPOSIUM ON MEN S HEALTH June 12, 2013 The PSA Controversy Defining It, Discussing It and Coping With It As of May 2012,
Advances in Diagnostic and Molecular Testing in Prostate Cancer
 Advances in Diagnostic and Molecular Testing in Prostate Cancer Ashley E. Ross MD PhD Assistant Professor Urology, Oncology, Pathology Johns Hopkins School of Medicine September 24, 2015 1 Disclosures
Advances in Diagnostic and Molecular Testing in Prostate Cancer Ashley E. Ross MD PhD Assistant Professor Urology, Oncology, Pathology Johns Hopkins School of Medicine September 24, 2015 1 Disclosures
Prostate cancer. Christopher Eden. The Royal Surrey County Hospital, Guildford & The Hampshire Clinic, Old Basing.
 Prostate cancer Christopher Eden The Royal Surrey County Hospital, Guildford & The Hampshire Clinic, Old Basing. Screening Screening men for PCa (prostate cancer) using PSA (Prostate Specific Antigen blood
Prostate cancer Christopher Eden The Royal Surrey County Hospital, Guildford & The Hampshire Clinic, Old Basing. Screening Screening men for PCa (prostate cancer) using PSA (Prostate Specific Antigen blood
Gene Expression Profiling and Protein Biomarkers for Prostate Cancer Management
 MEDICAL POLICY POLICY RELATED POLICIES POLICY GUIDELINES DESCRIPTION SCOPE BENEFIT APPLICATION RATIONALE REFERENCES CODING APPENDIX HISTORY Gene Expression Profiling and Protein Biomarkers for Prostate
MEDICAL POLICY POLICY RELATED POLICIES POLICY GUIDELINES DESCRIPTION SCOPE BENEFIT APPLICATION RATIONALE REFERENCES CODING APPENDIX HISTORY Gene Expression Profiling and Protein Biomarkers for Prostate
The 4Kscore blood test for risk of aggressive prostate cancer
 The 4Kscore blood test for risk of aggressive prostate cancer Early detection of aggressive prostate cancer Challenges Serum PSA has a high false positive rate Over 1 million prostate biopsies performed
The 4Kscore blood test for risk of aggressive prostate cancer Early detection of aggressive prostate cancer Challenges Serum PSA has a high false positive rate Over 1 million prostate biopsies performed
7. Prostate cancer in PSA relapse
 7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
PROSTATE CANCER. Get the facts, know your options. Samay Jain, MD, Assistant Professor,The University of Toledo Chief, Division of Urologic Oncology
 PROSTATE CANCER Get the facts, know your options Samay Jain, MD, Assistant Professor,The University of Toledo Chief, Division of Urologic Oncology i What is the Prostate? Unfortunately, you have prostate
PROSTATE CANCER Get the facts, know your options Samay Jain, MD, Assistant Professor,The University of Toledo Chief, Division of Urologic Oncology i What is the Prostate? Unfortunately, you have prostate
Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical
 Summary. 111 Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical recurrence (BCR) is the first sign of recurrent
Summary. 111 Detection and staging of recurrent prostate cancer is still one of the important clinical problems in prostate cancer. A rise in PSA or biochemical recurrence (BCR) is the first sign of recurrent
Biomarkers for Prostate Cancer. Eric Wallen, MD Department of Urology
 Biomarkers for Prostate Cancer Eric Wallen, MD Department of Urology Disclosure MDxHealth Scientific Advisor 55-year-old man: Poor Guy Risk of prostate cancer? 1 in 6 Risk of prostate cancer death? 1 in
Biomarkers for Prostate Cancer Eric Wallen, MD Department of Urology Disclosure MDxHealth Scientific Advisor 55-year-old man: Poor Guy Risk of prostate cancer? 1 in 6 Risk of prostate cancer death? 1 in
An Introduction to PROSTATE CANCER
 An Introduction to PROSTATE CANCER Being diagnosed with prostate cancer can be a life-altering experience. It requires making some very difficult decisions about treatments that can affect not only the
An Introduction to PROSTATE CANCER Being diagnosed with prostate cancer can be a life-altering experience. It requires making some very difficult decisions about treatments that can affect not only the
Us TOO University Presents: Understanding Diagnostic Testing
 Us TOO University Presents: Understanding Diagnostic Testing for Prostate Cancer Patients Today s speaker is Manish Bhandari, MD Program moderator is Pam Barrett, Us TOO International Made possible by
Us TOO University Presents: Understanding Diagnostic Testing for Prostate Cancer Patients Today s speaker is Manish Bhandari, MD Program moderator is Pam Barrett, Us TOO International Made possible by
Description of Procedure or Service. gene_based_tests_for_screening_detection_or_management_of_prostate_cancer 4/2009 8/2015 8/2016 8/2015
 Corporate Medical Policy Gene-Based Tests for Screening, Detection, and/or Management File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_based_tests_for_screening_detection_or_management_of_prostate_cancer
Corporate Medical Policy Gene-Based Tests for Screening, Detection, and/or Management File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_based_tests_for_screening_detection_or_management_of_prostate_cancer
Prostate Cancer Screening in Taiwan: a must
 Prostate Cancer Screening in Taiwan: a must 吳 俊 德 基 隆 長 庚 醫 院 台 灣 醫 學 會 105 th What is the PSA test? The blood level of PSA is often elevated in men with prostate cancer, and the PSA test was originally
Prostate Cancer Screening in Taiwan: a must 吳 俊 德 基 隆 長 庚 醫 院 台 灣 醫 學 會 105 th What is the PSA test? The blood level of PSA is often elevated in men with prostate cancer, and the PSA test was originally
PCa Commentary. Volume 73 January-February 2012 PSA AND TREATMENT DECISIONS:
 1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 73 January-February 2012 CONTENTS PSA SCREENING & BASIC SCIENCE PSA AND TREATMENT 1 DECISIONS
1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 73 January-February 2012 CONTENTS PSA SCREENING & BASIC SCIENCE PSA AND TREATMENT 1 DECISIONS
Prostate cancer is the most common cause of death from cancer in men over age 75. Prostate cancer is rarely found in men younger than 40.
 A.D.A.M. Medical Encyclopedia. Prostate cancer Cancer - prostate; Biopsy - prostate; Prostate biopsy; Gleason score Last reviewed: October 2, 2013. Prostate cancer is cancer that starts in the prostate
A.D.A.M. Medical Encyclopedia. Prostate cancer Cancer - prostate; Biopsy - prostate; Prostate biopsy; Gleason score Last reviewed: October 2, 2013. Prostate cancer is cancer that starts in the prostate
2010 SITE REPORT St. Joseph Hospital PROSTATE CANCER
 2010 SITE REPORT St. Joseph Hospital PROSTATE CANCER Humboldt County is located on the Redwood Coast of Northern California. U.S census data for 2010 reports county population at 134,623, an increase of
2010 SITE REPORT St. Joseph Hospital PROSTATE CANCER Humboldt County is located on the Redwood Coast of Northern California. U.S census data for 2010 reports county population at 134,623, an increase of
SRO Tutorial: Prostate Cancer Treatment Options
 SRO Tutorial: Prostate Cancer Treatment Options May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible,
SRO Tutorial: Prostate Cancer Treatment Options May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible,
PSA Screening for Prostate Cancer Information for Care Providers
 All men should know they are having a PSA test and be informed of the implications prior to testing. This booklet was created to help primary care providers offer men information about the risks and benefits
All men should know they are having a PSA test and be informed of the implications prior to testing. This booklet was created to help primary care providers offer men information about the risks and benefits
ACCEPTED MANUSCRIPT. Understanding the performance of active surveillance selection criteria in diverse urology practices
 Understanding the performance of active surveillance selection criteria in diverse urology practices Scott R. Hawken BS*,1, Paul R. Womble MD*,1, Lindsey A. Herrel MD 1, Zaojun Ye MS 1, Susan M. Linsell
Understanding the performance of active surveillance selection criteria in diverse urology practices Scott R. Hawken BS*,1, Paul R. Womble MD*,1, Lindsey A. Herrel MD 1, Zaojun Ye MS 1, Susan M. Linsell
Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC)
") Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC) FDA Presentation ODAC Meeting September 14, 2011 1 Review Team Paul G. Kluetz,
Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC) FDA Presentation ODAC Meeting September 14, 2011 1 Review Team Paul G. Kluetz,
TO SCREEN OR NOT TO SCREEN: THE PROSTATE CANCER
 TO SCREEN OR NOT TO SCREEN: THE PROSTATE CANCER DILEMMA Thomas J Stormont MD January 2012 http://www.youtube.com/watch?v=8jd 7bAHVp0A&feature=related related INTRODUCTION A government health panel (the
TO SCREEN OR NOT TO SCREEN: THE PROSTATE CANCER DILEMMA Thomas J Stormont MD January 2012 http://www.youtube.com/watch?v=8jd 7bAHVp0A&feature=related related INTRODUCTION A government health panel (the
Use of Androgen Deprivation Therapy (ADT) in Localized Prostate Cancer
 in Localized Prostate Cancer") Use of Androgen Deprivation Therapy (ADT) in Localized Prostate Cancer Adam R. Kuykendal, MD; Laura H. Hendrix, MS; Ramzi G. Salloum, PhD; Paul A. Godley, MD, PhD; Ronald C. Chen, MD, MPH No conflicts
Use of Androgen Deprivation Therapy (ADT) in Localized Prostate Cancer Adam R. Kuykendal, MD; Laura H. Hendrix, MS; Ramzi G. Salloum, PhD; Paul A. Godley, MD, PhD; Ronald C. Chen, MD, MPH No conflicts
Individual Prediction
 Individual Prediction Michael W. Kattan, Ph.D. Professor of Medicine, Epidemiology and Biostatistics, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University Chairman, Department
Individual Prediction Michael W. Kattan, Ph.D. Professor of Medicine, Epidemiology and Biostatistics, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University Chairman, Department
Implementation Date: April 2015 Clinical Operations
 National Imaging Associates, Inc. Clinical guideline PROSTATE CANCER Original Date: March 2011 Page 1 of 5 Radiation Oncology Last Review Date: March 2015 Guideline Number: NIA_CG_124 Last Revised Date:
National Imaging Associates, Inc. Clinical guideline PROSTATE CANCER Original Date: March 2011 Page 1 of 5 Radiation Oncology Last Review Date: March 2015 Guideline Number: NIA_CG_124 Last Revised Date:
Thomas A. Kollmorgen, M.D. Oregon Urology Institute
 Thomas A. Kollmorgen, M.D. Oregon Urology Institute None 240,000 new diagnosis per year, and an estimated 28,100 deaths (2012) 2 nd leading cause of death from cancer in U.S.A. Approximately 1 in 6 men
Thomas A. Kollmorgen, M.D. Oregon Urology Institute None 240,000 new diagnosis per year, and an estimated 28,100 deaths (2012) 2 nd leading cause of death from cancer in U.S.A. Approximately 1 in 6 men
Oncology Annual Report: Prostate Cancer 2005 Update By: John Konefal, MD, Radiation Oncology
 Oncology Annual Report: Prostate Cancer 25 Update By: John Konefal, MD, Radiation Oncology Prostate cancer is the most common cancer in men, with 232,9 new cases projected to be diagnosed in the U.S. in
Oncology Annual Report: Prostate Cancer 25 Update By: John Konefal, MD, Radiation Oncology Prostate cancer is the most common cancer in men, with 232,9 new cases projected to be diagnosed in the U.S. in
These rare variants often act aggressively and may respond differently to therapy than the more common prostate adenocarcinoma.
 Prostate Cancer OVERVIEW Prostate cancer is the second most common cancer diagnosed among American men, accounting for nearly 200,000 new cancer cases in the United States each year. Greater than 65% of
Prostate Cancer OVERVIEW Prostate cancer is the second most common cancer diagnosed among American men, accounting for nearly 200,000 new cancer cases in the United States each year. Greater than 65% of
Understanding the. Controversies of. testosterone replacement. therapy in hypogonadal men with prostate cancer. controversies surrounding
 Controversies of testosterone replacement therapy in hypogonadal men with prostate cancer Samuel Deem, DO CULTURA CREATIVE (RF) / ALAMY Understanding the controversies surrounding testosterone replacement
Controversies of testosterone replacement therapy in hypogonadal men with prostate cancer Samuel Deem, DO CULTURA CREATIVE (RF) / ALAMY Understanding the controversies surrounding testosterone replacement
Cancer in Primary Care: Prostate Cancer Screening. How and How often? Should we and in which patients?
 Cancer in Primary Care: Prostate Cancer Screening How and How often? Should we and in which patients? PLCO trial (Prostate, Lung, Colorectal and Ovarian) Results In the screening group, rates of compliance
Cancer in Primary Care: Prostate Cancer Screening How and How often? Should we and in which patients? PLCO trial (Prostate, Lung, Colorectal and Ovarian) Results In the screening group, rates of compliance
Prostate-Specific Antigen Based Screening: Controversy and Guidelines
 Prostate-Specific Antigen Based Screening: Controversy and Guidelines Eric H. Kim and Gerald L. Andriole Institutional Address: Washington University School of Medicine 4960 Children's Place Campus Box
Prostate-Specific Antigen Based Screening: Controversy and Guidelines Eric H. Kim and Gerald L. Andriole Institutional Address: Washington University School of Medicine 4960 Children's Place Campus Box
PROSTATE CANCER 101 WHAT IS PROSTATE CANCER?
 PROSTATE CANCER 101 WHAT IS PROSTATE CANCER? Prostate cancer is cancer that begins in the prostate. The prostate is a walnut-shaped gland in the male reproductive system located below the bladder and in
PROSTATE CANCER 101 WHAT IS PROSTATE CANCER? Prostate cancer is cancer that begins in the prostate. The prostate is a walnut-shaped gland in the male reproductive system located below the bladder and in
Prostate Cancer. Treatments as unique as you are
 Prostate Cancer Treatments as unique as you are UCLA Prostate Cancer Program Prostate cancer is the second most common cancer among men. The UCLA Prostate Cancer Program brings together the elements essential
Prostate Cancer Treatments as unique as you are UCLA Prostate Cancer Program Prostate cancer is the second most common cancer among men. The UCLA Prostate Cancer Program brings together the elements essential
Early Prostate Cancer: Questions and Answers. Key Points
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Early Prostate Cancer:
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Early Prostate Cancer:
PSA screening in asymptomatic men the debate continues www.bpac.org.nz keyword: psa
 PSA screening in asymptomatic men the debate continues www.bpac.org.nz keyword: psa Key messages: PSA is present in the benign and malignant prostate There is currently no national screening programme
PSA screening in asymptomatic men the debate continues www.bpac.org.nz keyword: psa Key messages: PSA is present in the benign and malignant prostate There is currently no national screening programme
HAVE YOU BEEN NEWLY DIAGNOSED with DCIS?
 HAVE YOU BEEN NEWLY DIAGNOSED with DCIS? Jen D. Mother and volunteer. Diagnosed with DCIS breast cancer in 2012. An educational guide prepared by Genomic Health This guide is designed to educate women
HAVE YOU BEEN NEWLY DIAGNOSED with DCIS? Jen D. Mother and volunteer. Diagnosed with DCIS breast cancer in 2012. An educational guide prepared by Genomic Health This guide is designed to educate women
NCCN Prostate Cancer Guidelines Update. James L. Mohler, MD Roswell Park Cancer Institute
 NCCN Prostate Cancer Guidelines Update James L. Mohler, MD Roswell Park Cancer Institute Every 2.5 Minutes an American is Diagnosed with Prostate Cancer Every 15 Minutes an American Dies of Prostate Cancer
NCCN Prostate Cancer Guidelines Update James L. Mohler, MD Roswell Park Cancer Institute Every 2.5 Minutes an American is Diagnosed with Prostate Cancer Every 15 Minutes an American Dies of Prostate Cancer
Prostatectomy, pelvic lymphadenect. Med age 63 years Mean followup 53 months No other cancer related therapy before recurrence. Negative.
 Adjuvante und Salvage Radiotherapie Ludwig Plasswilm Klinik für Radio-Onkologie, KSSG CANCER CONTROL WITH RADICAL PROSTATECTOMY ALONE IN 1,000 CONSECUTIVE PATIENTS 1983 1998 Clinical stage T1 and T2 Mean
Adjuvante und Salvage Radiotherapie Ludwig Plasswilm Klinik für Radio-Onkologie, KSSG CANCER CONTROL WITH RADICAL PROSTATECTOMY ALONE IN 1,000 CONSECUTIVE PATIENTS 1983 1998 Clinical stage T1 and T2 Mean
Saturation Biopsy for Diagnosis and Staging of Prostate Cancer. Original Policy Date
 MP 7.01.101 Saturation Biopsy for Diagnosis and Staging of Prostate Cancer Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date /12/2013 Return to Medical Policy
MP 7.01.101 Saturation Biopsy for Diagnosis and Staging of Prostate Cancer Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date /12/2013 Return to Medical Policy
Cancer research in the Midland Region the prostate and bowel cancer projects
 Cancer research in the Midland Region the prostate and bowel cancer projects Ross Lawrenson Waikato Clinical School University of Auckland MoH/HRC Cancer Research agenda Lung cancer Palliative care Prostate
Cancer research in the Midland Region the prostate and bowel cancer projects Ross Lawrenson Waikato Clinical School University of Auckland MoH/HRC Cancer Research agenda Lung cancer Palliative care Prostate
Predominance of ERG negative high grade prostate cancers in African American men
 982 Predominance of ERG negative high grade prostate cancers in African American men JAMES FARRELL 1,2, DENISE YOUNG 1, YONGMEI CHEN 1, JENNIFER CULLEN 1, INGER L. ROSNER 1,2, JACOB KAGAN 3, SUDHIR SRIVASTAVA
982 Predominance of ERG negative high grade prostate cancers in African American men JAMES FARRELL 1,2, DENISE YOUNG 1, YONGMEI CHEN 1, JENNIFER CULLEN 1, INGER L. ROSNER 1,2, JACOB KAGAN 3, SUDHIR SRIVASTAVA
The Business of Prostate Cancer Care: A Clinician-Researcher s Perspective
 The Business of Prostate Cancer Care: A Clinician-Researcher s Perspective David F. Penson, MD, MPH Departments of Urology and Preventive Medicine Keck School of Medicine University of Southern California
The Business of Prostate Cancer Care: A Clinician-Researcher s Perspective David F. Penson, MD, MPH Departments of Urology and Preventive Medicine Keck School of Medicine University of Southern California
Prostate Cancer What Are the Outcomes of Radical Prostatectomy for High-risk Prostate Cancer?
 Prostate Cancer What Are the Outcomes of Radical Prostatectomy for High-risk Prostate Cancer? Stacy Loeb, Edward M. Schaeffer, Bruce J. Trock, Jonathan I. Epstein, Elizabeth B. Humphreys, and Patrick C.
Prostate Cancer What Are the Outcomes of Radical Prostatectomy for High-risk Prostate Cancer? Stacy Loeb, Edward M. Schaeffer, Bruce J. Trock, Jonathan I. Epstein, Elizabeth B. Humphreys, and Patrick C.
DIAGNOSIS OF PROSTATE CANCER
 DIAGNOSIS OF PROSTATE CANCER Determining the presence of prostate cancer generally involves a series of tests and exams. Before starting the testing process, the physician will ask questions about the
DIAGNOSIS OF PROSTATE CANCER Determining the presence of prostate cancer generally involves a series of tests and exams. Before starting the testing process, the physician will ask questions about the
Report with statistical data from 2007
 2008 Cancer Program Annual Report with statistical data from 2007 Lake Cumberland Regional Hospital 305 Langdon Streett Somerset, KY 42503 Telephone: 606-679-7441 Fax: 606-678-9919 Cancer Committee Mullai,
2008 Cancer Program Annual Report with statistical data from 2007 Lake Cumberland Regional Hospital 305 Langdon Streett Somerset, KY 42503 Telephone: 606-679-7441 Fax: 606-678-9919 Cancer Committee Mullai,
Genomic Basis of Prostate Cancer Health Disparity Among African-American
 AD AWARD NUMBER: W81XWH-12-1-0259 TITLE: Men Genomic Basis of Prostate Cancer Health Disparity Among African-American PRINCIPAL INVESTIGATOR: Harry Ostrer, M.D. RECIPIENT: Albert Einstein College of Medicine
AD AWARD NUMBER: W81XWH-12-1-0259 TITLE: Men Genomic Basis of Prostate Cancer Health Disparity Among African-American PRINCIPAL INVESTIGATOR: Harry Ostrer, M.D. RECIPIENT: Albert Einstein College of Medicine
PROSTATE CANCER. Normal-risk men: No family history of prostate cancer No history of prior screening Not African-American
 PROSTATE CANCER 1. Guidelines for Screening Risk Factors Normal-risk men: No family history of prostate cancer No history of prior screening Not African-American High-risk men: Family history of prostate
PROSTATE CANCER 1. Guidelines for Screening Risk Factors Normal-risk men: No family history of prostate cancer No history of prior screening Not African-American High-risk men: Family history of prostate
Secondary Cancer and Relapse Rates Following Radical Prostatectomy for Prostate-Confined Cancer
 Copyright E 2007 Journal of Insurance Medicine J Insur Med 2007;39:242 250 MORTALITY Secondary Cancer and Relapse Rates Following Radical Prostatectomy for Prostate-Confined Cancer David Wesley, MD; Hugh
Copyright E 2007 Journal of Insurance Medicine J Insur Med 2007;39:242 250 MORTALITY Secondary Cancer and Relapse Rates Following Radical Prostatectomy for Prostate-Confined Cancer David Wesley, MD; Hugh
CMScript. Member of a medical scheme? Know your guaranteed benefits! Issue 7 of 2014
 Background CMScript Member of a medical scheme? Know your guaranteed benefits! Issue 7 of 2014 Prostate cancer is second only to lung cancer as the leading cause of cancer-related deaths in men. It is
Background CMScript Member of a medical scheme? Know your guaranteed benefits! Issue 7 of 2014 Prostate cancer is second only to lung cancer as the leading cause of cancer-related deaths in men. It is
PSA Screening and the USPSTF Understanding the Controversy
 PSA Screening and the USPSTF Understanding the Controversy Peter C. Albertsen Division of Urology University of Connecticut Farmington, CT, USA USPSTF Final Report 1 Four Key Questions 1. Does PSA based
PSA Screening and the USPSTF Understanding the Controversy Peter C. Albertsen Division of Urology University of Connecticut Farmington, CT, USA USPSTF Final Report 1 Four Key Questions 1. Does PSA based
Guidelines for Cancer Prevention, Early detection & Screening. Prostate Cancer
 Guidelines for Cancer Prevention, Early detection & Screening Prostate Cancer Intervention Comments & Recommendations For primary prevention, it has been suggested that diets low in meat & other fatty
Guidelines for Cancer Prevention, Early detection & Screening Prostate Cancer Intervention Comments & Recommendations For primary prevention, it has been suggested that diets low in meat & other fatty
Published Ahead of Print on June 17, 2013 as 10.1200/JCO.2012.47.0302. J Clin Oncol 31. 2013 by American Society of Clinical Oncology INTRODUCTION
 Published Ahead of Print on June 17, 2013 as 10.1200/JCO.2012.47.0302 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2012.47.0302 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E
Published Ahead of Print on June 17, 2013 as 10.1200/JCO.2012.47.0302 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2012.47.0302 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E
Screening for Prostate Cancer
 Screening for Prostate Cancer It is now clear that screening for Prostate Cancer discovers the disease at an earlier and more curable stage. It is not yet clear whether this translates into reduced mortality
Screening for Prostate Cancer It is now clear that screening for Prostate Cancer discovers the disease at an earlier and more curable stage. It is not yet clear whether this translates into reduced mortality
Prostate Cancer In-Depth
 Prostate Cancer In-Depth Introduction Prostate cancer is the most common visceral malignancy among American men. In the year 2003, there are expected to be 220,000 new cases and nearly 29,000 deaths in
Prostate Cancer In-Depth Introduction Prostate cancer is the most common visceral malignancy among American men. In the year 2003, there are expected to be 220,000 new cases and nearly 29,000 deaths in
An Empirical Evaluation of Guidelines on Prostate-specific Antigen Velocity in Prostate Cancer Detection
 DOI: 10.1093/jnci/djr028 ARTICLE JNCI djr028 MA JOURNAL NAME Art. No. CE Code The Author 2011. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
DOI: 10.1093/jnci/djr028 ARTICLE JNCI djr028 MA JOURNAL NAME Art. No. CE Code The Author 2011. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Modeling Drivers of Cost and Benefit for Policy Development in Cancer
 Modeling Drivers of Cost and Benefit for Policy Development in Cancer Harms? Benefits? Costs? Ruth Etzioni Fred Hutchinson Cancer Research Center Seattle, Washington The USPSTF recommends against routine
Modeling Drivers of Cost and Benefit for Policy Development in Cancer Harms? Benefits? Costs? Ruth Etzioni Fred Hutchinson Cancer Research Center Seattle, Washington The USPSTF recommends against routine
Medical Policy Manual. Topic: Gene Expression Analysis for Prostate Cancer Management. Date of Origin: January 2014
 Medical Policy Manual Topic: Gene Expression Analysis for Prostate Cancer Management Date of Origin: January 2014 Section: Genetic Testing Last Reviewed Date: February 2015 Policy No: 71 Effective Date:
Medical Policy Manual Topic: Gene Expression Analysis for Prostate Cancer Management Date of Origin: January 2014 Section: Genetic Testing Last Reviewed Date: February 2015 Policy No: 71 Effective Date:
SIGNPOSTS. Along the Pathway of Prostate Cancer. Understanding Diagnostic Tests and Procedures to Monitor Prostate Cancer
 SIGNPOSTS Along the Pathway of Prostate Cancer Understanding Diagnostic Tests and Procedures to Monitor Prostate Cancer Your journey is unique like you. Signposts along the pathway can show you where you
SIGNPOSTS Along the Pathway of Prostate Cancer Understanding Diagnostic Tests and Procedures to Monitor Prostate Cancer Your journey is unique like you. Signposts along the pathway can show you where you
MEDICAL POLICY SUBJECT: PROSTATE CANCER SCREENING, DETECTION AND MONITORING
 MEDICAL POLICY PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
DECISION AID TOOL PROSTATE CANCER SCREENING WITH PSA TESTING
 DECISION AID TOOL PROSTATE CANCER SCREENING WITH PSA TESTING This booklet is what is often called a decision aid. The goals of a decision aid are to help people better understand their medical choices
DECISION AID TOOL PROSTATE CANCER SCREENING WITH PSA TESTING This booklet is what is often called a decision aid. The goals of a decision aid are to help people better understand their medical choices
PSA Testing 101. Stanley H. Weiss, MD. Professor, UMDNJ-New Jersey Medical School. Director & PI, Essex County Cancer Coalition. weiss@umdnj.
 PSA Testing 101 Stanley H. Weiss, MD Professor, UMDNJ-New Jersey Medical School Director & PI, Essex County Cancer Coalition weiss@umdnj.edu September 23, 2010 Screening: 3 tests for PCa A good screening
PSA Testing 101 Stanley H. Weiss, MD Professor, UMDNJ-New Jersey Medical School Director & PI, Essex County Cancer Coalition weiss@umdnj.edu September 23, 2010 Screening: 3 tests for PCa A good screening
Health Policy Advisory Committee on Technology
 Health Policy Advisory Committee on Technology Technology Brief Molecular testing for prostate cancer prognosis November 2014 State of Queensland (Queensland Department of Health) 2014 This work is licensed
Health Policy Advisory Committee on Technology Technology Brief Molecular testing for prostate cancer prognosis November 2014 State of Queensland (Queensland Department of Health) 2014 This work is licensed
Prostate cancer is the second most
 Treatment Options for Localized Prostate Cancer RAVINDER MOHAN, MD, PhD, and PAUL F. SCHELLHAMMER, MD Eastern Virginia Medical School, Norfolk, Virginia In the United States, more than 90 percent of prostate
Treatment Options for Localized Prostate Cancer RAVINDER MOHAN, MD, PhD, and PAUL F. SCHELLHAMMER, MD Eastern Virginia Medical School, Norfolk, Virginia In the United States, more than 90 percent of prostate
Gene Expression Analysis for Prostate Cancer
 Original Issue Date (Created): 10/1/2014 Most Recent Review Date (Revised): 6/2/2015 Effective Date: 8/1/2015 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT VARIATIONS DISCLAIMER
Original Issue Date (Created): 10/1/2014 Most Recent Review Date (Revised): 6/2/2015 Effective Date: 8/1/2015 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT VARIATIONS DISCLAIMER
Prostate cancer volume at biopsy vs. findings at Prostatectomy
 Prostate cancer volume at biopsy vs. findings at Prostatectomy May 2005 By Shelly Smits, RHIT, CCS, CTR Ian Thompson, MD Data Source: Cancer registry data of prostate cancer treated with prostatectomy
Prostate cancer volume at biopsy vs. findings at Prostatectomy May 2005 By Shelly Smits, RHIT, CCS, CTR Ian Thompson, MD Data Source: Cancer registry data of prostate cancer treated with prostatectomy
Prostate Cancer Screening: Are We There Yet? March 2010 Andrew M.D. Wolf, MD University of Virginia School of Medicine
 Prostate Cancer Screening: Are We There Yet? March 2010 Andrew M.D. Wolf, MD University of Virginia School of Medicine Case #1 A 55 yo white man with well-controlled hypertension presents for his annual
Prostate Cancer Screening: Are We There Yet? March 2010 Andrew M.D. Wolf, MD University of Virginia School of Medicine Case #1 A 55 yo white man with well-controlled hypertension presents for his annual
HEALTH NEWS PROSTATE CANCER THE PROSTATE
 HEALTH NEWS PROSTATE CANCER THE PROSTATE Prostate comes from the Greek meaning to stand in front of ; this is very different than prostrate which means to lie down flat. The prostate is a walnut-sized
HEALTH NEWS PROSTATE CANCER THE PROSTATE Prostate comes from the Greek meaning to stand in front of ; this is very different than prostrate which means to lie down flat. The prostate is a walnut-sized
SIOG Guidelines Update 2014 Prostate Cancer. Dr Helen Boyle Centre Léon Bérard SIOG meeting 25 October 2014,Lisbon
 SIOG Guidelines Update 2014 Prostate Cancer Dr Helen Boyle Centre Léon Bérard SIOG meeting 25 October 2014,Lisbon Droz JP, Aapro M, Balducci L, Boyle H, Van den Broeck T, Cathcart P, Dickinson L, Efstathiou
SIOG Guidelines Update 2014 Prostate Cancer Dr Helen Boyle Centre Léon Bérard SIOG meeting 25 October 2014,Lisbon Droz JP, Aapro M, Balducci L, Boyle H, Van den Broeck T, Cathcart P, Dickinson L, Efstathiou
Controversites: Screening for Prostate Cancer in Older Adults
 Controversites: Screening for Prostate Cancer in Older Adults William Dale, MD, PhD University of Chicago Sections of Geriatrics & Palliative Medicine and Hematology/Oncology Director, Specialized Oncology
Controversites: Screening for Prostate Cancer in Older Adults William Dale, MD, PhD University of Chicago Sections of Geriatrics & Palliative Medicine and Hematology/Oncology Director, Specialized Oncology
NCCN Prostate Cancer Early Detection Guideline
 NCCN Prostate Cancer Early Detection Guideline Joan McClure Senior Vice President National Comprehensive Cancer Network African American Prostate Cancer Disparity Summit September 22, 2006 Washington,
NCCN Prostate Cancer Early Detection Guideline Joan McClure Senior Vice President National Comprehensive Cancer Network African American Prostate Cancer Disparity Summit September 22, 2006 Washington,
Questions to ask my doctor: About prostate cancer
 Questions to ask my doctor: About prostate cancer Being diagnosed with prostate cancer can be scary and stressful. You probably have a lot of questions and concerns. Learning about the disease, how it
Questions to ask my doctor: About prostate cancer Being diagnosed with prostate cancer can be scary and stressful. You probably have a lot of questions and concerns. Learning about the disease, how it
Prostate cancer screening: clinical applications and challenges
 Urologic Oncology: Seminars and Original Investigations 22 (2004) 353 357 Seminar article Prostate cancer screening: clinical applications and challenges Otis W. Brawley, M.D.* Winship Cancer Institute,
Urologic Oncology: Seminars and Original Investigations 22 (2004) 353 357 Seminar article Prostate cancer screening: clinical applications and challenges Otis W. Brawley, M.D.* Winship Cancer Institute,
Advances In Chemotherapy For Hormone Refractory Prostate Cancer. TAX 327 study results & SWOG 99-16 study results presented at ASCO 2004
 Ronald de Wit Rotterdam Cancer Institute The Netherlands Advances In Chemotherapy For Hormone Refractory Prostate Cancer TAX 327 study results & SWOG 99-16 study results presented at Slide 1 Prostate Cancer
Ronald de Wit Rotterdam Cancer Institute The Netherlands Advances In Chemotherapy For Hormone Refractory Prostate Cancer TAX 327 study results & SWOG 99-16 study results presented at Slide 1 Prostate Cancer
Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer
 Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer David Josephson, MD FACS Fellowship Director, Urologic Oncology and Robotic Surgery Program Staging Most important in risk assessment and
Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer David Josephson, MD FACS Fellowship Director, Urologic Oncology and Robotic Surgery Program Staging Most important in risk assessment and
The PLCO Trial Not a comparison of Screening vs no Screening
 PSA Screening: Science, Politics and Uncertainty David F. Penson, MD, MPH Hamilton and Howd Chair of Urologic Oncology Professor and Chair, Department of Urologic Surgery Director, Center for Surgical
PSA Screening: Science, Politics and Uncertainty David F. Penson, MD, MPH Hamilton and Howd Chair of Urologic Oncology Professor and Chair, Department of Urologic Surgery Director, Center for Surgical
Saturation Biopsy vs. 3D Spatial Biopsy vs. Free Hand Ultrasound biopsy for Targeted Prostate Cancer Therapies
 Saturation Biopsy vs. 3D Spatial Biopsy vs. Free Hand Ultrasound biopsy for Targeted Prostate Cancer Therapies John F. Ward, MD Assistant Professor University of Texas M. D. Anderson Cancer Center Ablation
Saturation Biopsy vs. 3D Spatial Biopsy vs. Free Hand Ultrasound biopsy for Targeted Prostate Cancer Therapies John F. Ward, MD Assistant Professor University of Texas M. D. Anderson Cancer Center Ablation
Active surveillance strategy for patients with localised prostate cancer
 PHD THESIS DANISH MEDICAL JOURNAL Active surveillance strategy for patients with localised prostate cancer Criteria for progression Frederik Birkebæk Thomsen This review has been accepted as a thesis together
PHD THESIS DANISH MEDICAL JOURNAL Active surveillance strategy for patients with localised prostate cancer Criteria for progression Frederik Birkebæk Thomsen This review has been accepted as a thesis together
Targeted Therapy What the Surgeon Needs to Know
 Targeted Therapy What the Surgeon Needs to Know AATS Focus in Thoracic Surgery 2014 David R. Jones, M.D. Professor & Chief, Thoracic Surgery Memorial Sloan Kettering Cancer Center I have no disclosures
Targeted Therapy What the Surgeon Needs to Know AATS Focus in Thoracic Surgery 2014 David R. Jones, M.D. Professor & Chief, Thoracic Surgery Memorial Sloan Kettering Cancer Center I have no disclosures
Key Messages for Healthcare Providers
 Cancer Care Ontario: Prostate Cancer Screening with the Prostate- Specific Antigen (PSA) Test Key Messages for Healthcare Providers Considerations for men at average risk Avoid prostate-specific antigen
Cancer Care Ontario: Prostate Cancer Screening with the Prostate- Specific Antigen (PSA) Test Key Messages for Healthcare Providers Considerations for men at average risk Avoid prostate-specific antigen
In 2006 approximately 234,000 men were diagnosed with
 Long-Term Survival in Men With High Grade Prostate Cancer: A Comparison Between Conservative Treatment, Radiation Therapy and Radical Prostatectomy A Propensity Scoring Approach Ashutosh Tewari,*, George
Long-Term Survival in Men With High Grade Prostate Cancer: A Comparison Between Conservative Treatment, Radiation Therapy and Radical Prostatectomy A Propensity Scoring Approach Ashutosh Tewari,*, George
Prostate Cancer Treatment: What s Best for You?
 Prostate Cancer Treatment: What s Best for You? Prostate Cancer: Radiation Therapy Approaches I. Choices There is really a variety of options in prostate cancer management overall and in radiation therapy.
Prostate Cancer Treatment: What s Best for You? Prostate Cancer: Radiation Therapy Approaches I. Choices There is really a variety of options in prostate cancer management overall and in radiation therapy.
Use Of Testosterone In Men With Prostate Cancer. Traditional view: T is dangerous for PCa
 Use Of Testosterone In Men With Prostate Cancer Abraham Morgentaler, MD, FACS Director, Men s s Health Boston Associate Clinical Professor of Urology Harvard Medical School Boston, USA Traditional view:
Use Of Testosterone In Men With Prostate Cancer Abraham Morgentaler, MD, FACS Director, Men s s Health Boston Associate Clinical Professor of Urology Harvard Medical School Boston, USA Traditional view:
Establishing a Cohort of African-American Men to Validate a Method for using Serial PSA Measures to Detect Aggressive Prostate Cancers
 Establishing a Cohort of African-American Men to Validate a Method for using Serial PSA Measures to Detect Aggressive Prostate Cancers James R. Hebert, Sc.D., Cancer Prevention and Control Program, University
Establishing a Cohort of African-American Men to Validate a Method for using Serial PSA Measures to Detect Aggressive Prostate Cancers James R. Hebert, Sc.D., Cancer Prevention and Control Program, University
Department of Urology, Erasmus MC, 3015 CE Rotterdam, The Netherlands
 Advances in Urology Volume 2012, Article ID 612707, 6 pages doi:10.1155/2012/612707 Research Article The Role of Adjuvant Hormonal Treatment after Surgery for Localized High-Risk Prostate Cancer: Results
Advances in Urology Volume 2012, Article ID 612707, 6 pages doi:10.1155/2012/612707 Research Article The Role of Adjuvant Hormonal Treatment after Surgery for Localized High-Risk Prostate Cancer: Results
Bard: Prostate Cancer Treatment. Bard: Pelvic Organ Prolapse. Prostate Cancer. An overview of. Treatment. Prolapse. Information and Answers
 Bard: Prostate Cancer Treatment Bard: Pelvic Organ Prolapse Prostate Cancer An overview of Pelvic Treatment Organ Prolapse Information and Answers A Brief Overview Prostate Anatomy The prostate gland,
Bard: Prostate Cancer Treatment Bard: Pelvic Organ Prolapse Prostate Cancer An overview of Pelvic Treatment Organ Prolapse Information and Answers A Brief Overview Prostate Anatomy The prostate gland,