Delta College Corporate Services BPSC (on assignment at Dow) Payroll /Orientation Information
|
|
|
- Robert Moore
- 10 years ago
- Views:
Transcription
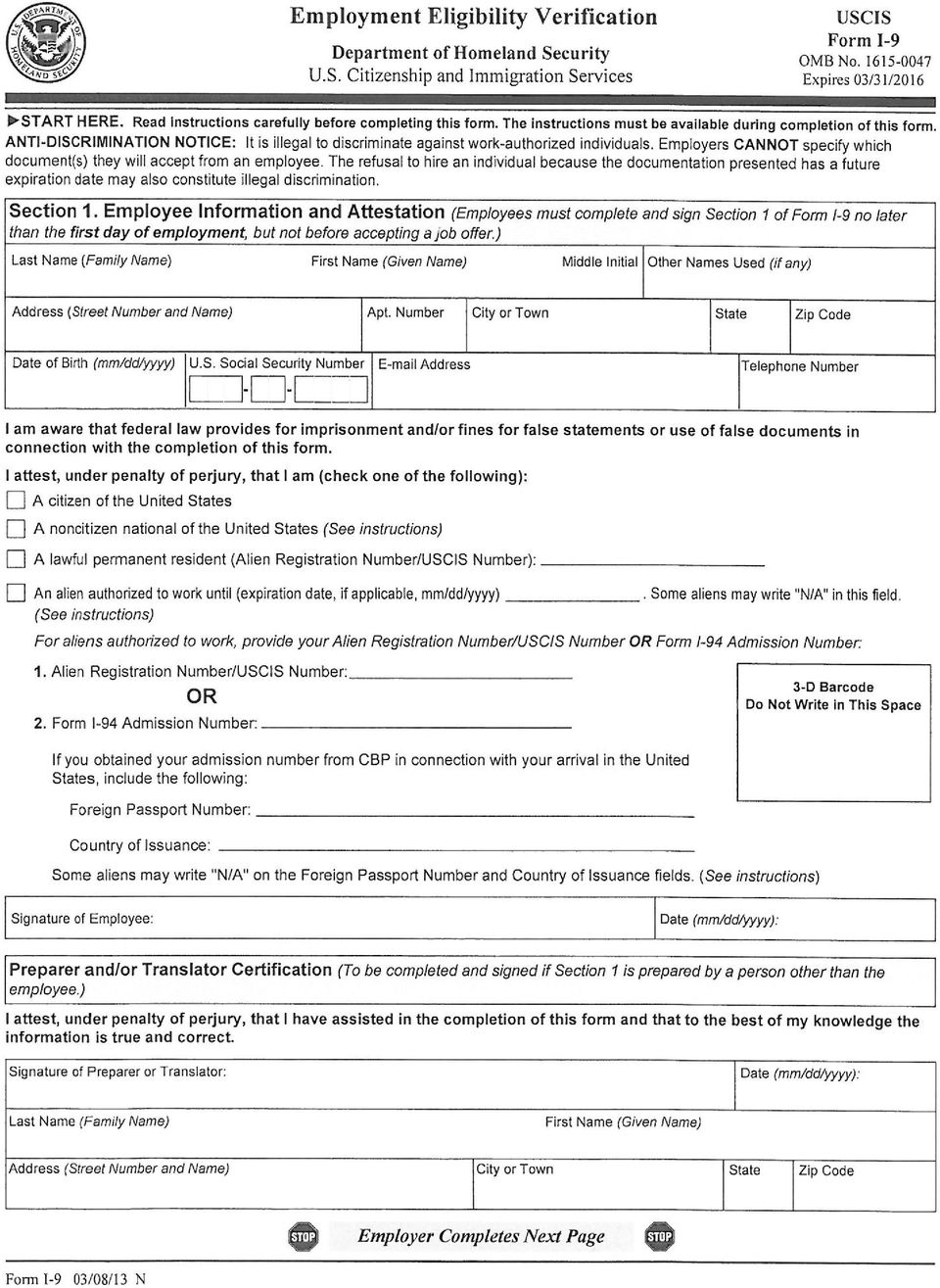
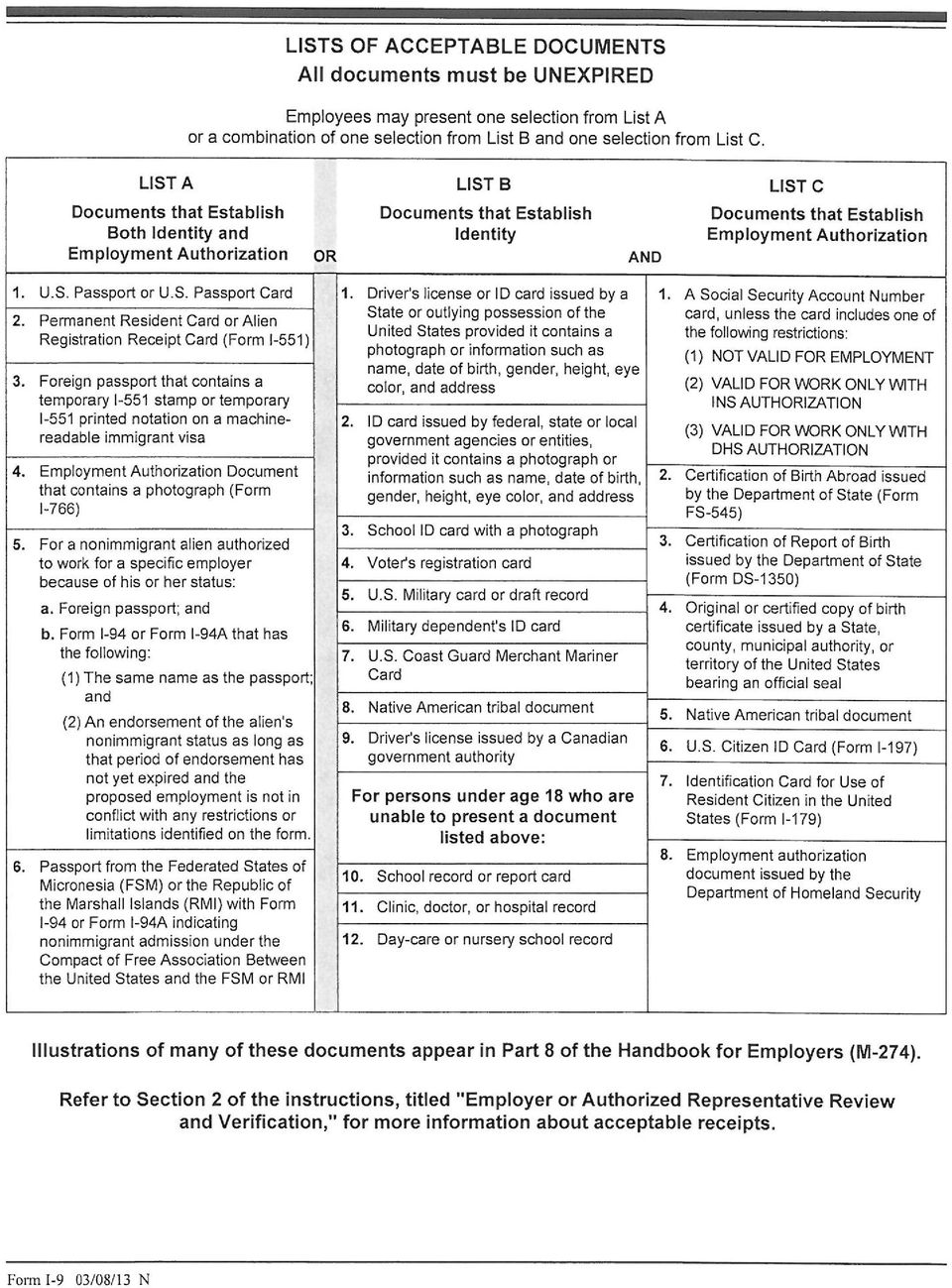
1 Delta College Corporate Services BPSC (on assignment at Dow) Payroll /Orientation Information The following forms must be completed and returned to the Human Resources Office, J101, in order to be placed on payroll. A signed copy of this page must be submitted to Human Resources, by signing you have acknowledged receipt of the policies listed below. Questions should be directed to the department responsible for providing you with payroll packet, or Human Resources at (989) Employee Name: Home Phone #: Address: ETHNICITY:(please circle one) (1-Not Hispanic or Latino) (2-Hispanic or Latino) Date of Hire: GENDER: (please circle one) (1-Female) (2- Male) RACE: (please circle one or more): (African American) (American Indian or Alaskan Native) (Asian) (Caucasian) (Native Hawaiian or Other Pacific Island) 1 Emergency Information 5 6 W-4 Form - Federal W-4 Form - Michigan SW-4 Form (City of Saginaw Residents Only) Employment Eligibility Verification Form (I-9) (identification required - refer to form for options) Form must be completed within 3 business days of the date employment begins. Original documentation must be presented. Michigan Public School Employees Retirement System - New Employees will receive their Member ID in a personalized Welcome Letter. This letter will direct you to login to the miaccount where you can nominate a beneficiary. You should receive your Member ID personalized Welcome Letter approximately two weeks after your first pay period. MPSERS website 7 Direct Deposit - OPTIONAL FORM Employees not selecting direct deposit must pick up their checks at the Cashier s Office. 8 Drug Free Work Place Act 10 Hepatitis B Vaccination Acknowledgement and Release Form Required for Category A Employees only Health / Dental Enrollment Forms (Employee self pay option available) Benefits Summary and Health/Dental rates All new employees are required to review each of the items listed below Family Medical Leave Act Employees Rights and Responsibilities HIPAA(Health Insurances Portability and Accountability Act) Notice Regarding Medicare and Your Prescription Drug Coverage Injury/Accident Reporting Regulations and Rules of Conduct Health Insurance Marketplace Coverage Options Required Training Modules: Bloodborne Pathogens, Copyright pt1 Provisions, Copyright pt6 Guidelines, Sexual Harassment, Diversity, FFERPA, Hazard Communications, Title IX-Higher Ed and SaVE act. Delta College s Vision, Mission and Values Tobacco Free Campus Delta College Emergency Procedures Additional Information Electronic Resources-For access to Delta's electronic resources go through the signup process at You must have completed and returned your payroll paperwork prior to sign up. Tax Sheltered Annuities Program Participation Details Payroll dates - employees are paid biweekly on Fridays for the previous 2 weeks (7 days in arrears) By signing this form, you are verifying that you have completed the payroll forms and have received information related to the topics listed above. Employee Signature: Date:
 (1-Not Hispanic or Latino) (2-Hispanic or Latino) Date of Hire: GENDER: (please circle one) (1-Female) (2- Male) RACE: (please")
2 DELTA COLLEGE EMERGENCY INFORMATION Name: Position: Full-Time Part-Time Faculty Staff IN CASE OF AN EMERGENCY NOTIFY First Choice Name: Address: Day Phone: Evening Phone: Relationship: Second Choice Name: Address: Day Phone: Evening Phone: Relationship: Do you have any health and/or medication information you want the College to know in the event of emergency situations: Additional Comments:

3 Form W-4 (2015) Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial situation changes. Exemption from withholding. If you are exempt, complete only lines 1, 2, 3, 4, and 7 and sign the form to validate it. Your exemption for 2015 expires February 16, See Pub. 505, Tax Withholding and Estimated Tax. Note. If another person can claim you as a dependent on his or her tax return, you cannot claim exemption from withholding if your income exceeds $1,050 and includes more than $350 of unearned income (for example, interest and dividends). Exceptions. An employee may be able to claim exemption from withholding even if the employee is a dependent, if the employee: Is age 65 or older, Is blind, or Will claim adjustments to income; tax credits; or itemized deductions, on his or her tax return. The exceptions do not apply to supplemental wages greater than $1,000,000. Basic instructions. If you are not exempt, complete the Personal Allowances Worksheet below. The worksheets on page 2 further adjust your withholding allowances based on itemized deductions, certain credits, adjustments to income, or two-earners/multiple jobs situations. Complete all worksheets that apply. However, you may claim fewer (or zero) allowances. For regular wages, withholding must be based on allowances you claimed and may not be a flat amount or percentage of wages. Head of household. Generally, you can claim head of household filing status on your tax return only if you are unmarried and pay more than 50% of the costs of keeping up a home for yourself and your dependent(s) or other qualifying individuals. See Pub. 501, Exemptions, Standard Deduction, and Filing Information, for information. Tax credits. You can take projected tax credits into account in figuring your allowable number of withholding allowances. Credits for child or dependent care expenses and the child tax credit may be claimed using the Personal Allowances Worksheet below. See Pub. 505 for information on converting your other credits into withholding allowances. Nonwage income. If you have a large amount of nonwage income, such as interest or dividends, consider making estimated tax payments using Form 1040-ES, Estimated Tax for Individuals. Otherwise, you may owe additional tax. If you have pension or annuity income, see Pub. 505 to find out if you should adjust your withholding on Form W-4 or W-4P. Two earners or multiple jobs. If you have a working spouse or more than one job, figure the total number of allowances you are entitled to claim on all jobs using worksheets from only one Form W-4. Your withholding usually will be most accurate when all allowances are claimed on the Form W-4 for the highest paying job and zero allowances are claimed on the others. See Pub. 505 for details. Nonresident alien. If you are a nonresident alien, see Notice 1392, Supplemental Form W-4 Instructions for Nonresident Aliens, before completing this form. Check your withholding. After your Form W-4 takes effect, use Pub. 505 to see how the amount you are having withheld compares to your projected total tax for See Pub. 505, especially if your earnings exceed $130,000 (Single) or $180,000 (Married). Future developments. Information about any future developments affecting Form W-4 (such as legislation enacted after we release it) will be posted at Personal Allowances Worksheet (Keep for your records.) A Enter 1 for yourself if no one else can claim you as a dependent A You are single and have only one job; or B Enter 1 if: { You are married, have only one job, and your spouse does not work; or... B Your wages from a second job or your spouse s wages (or the total of both) are $1,500 or less. C Enter 1 for your spouse. But, you may choose to enter -0- if you are married and have either a working spouse or more than one job. (Entering -0- may help you avoid having too little tax withheld.) C D Enter number of dependents (other than your spouse or yourself) you will claim on your tax return D E Enter 1 if you will file as head of household on your tax return (see conditions under Head of household above).. E F Enter 1 if you have at least $2,000 of child or dependent care expenses for which you plan to claim a credit... F (Note. Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.) G Child Tax Credit (including additional child tax credit). See Pub. 972, Child Tax Credit, for more information. If your total income will be less than $65,000 ($100,000 if married), enter 2 for each eligible child; then less 1 if you have two to four eligible children or less 2 if you have five or more eligible children. If your total income will be between $65,000 and $84,000 ($100,000 and $119,000 if married), enter 1 for each eligible child... G H Add lines A through G and enter total here. (Note. This may be different from the number of exemptions you claim on your tax return.) H { If you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions For accuracy, and Adjustments Worksheet on page 2. complete all If you are single and have more than one job or are married and you and your spouse both work and the combined worksheets earnings from all jobs exceed $50,000 ($20,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 to that apply. avoid having too little tax withheld. If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below. Separate here and give Form W-4 to your employer. Keep the top part for your records. Employee's Withholding Allowance Certificate Form W-4 Department of the Treasury Whether you are entitled to claim a certain number of allowances or exemption from withholding is Internal Revenue Service subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS. 1 Your first name and middle initial Last name OMB No Your social security number Home address (number and street or rural route) 3 Single Married Married, but withhold at higher Single rate. Note. If married, but legally separated, or spouse is a nonresident alien, check the Single box. City or town, state, and ZIP code 4 If your last name differs from that shown on your social security card, check here. You must call for a replacement card. 5 Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2) 5 6 Additional amount, if any, you want withheld from each paycheck $ 7 I claim exemption from withholding for 2015, and I certify that I meet both of the following conditions for exemption. Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and This year I expect a refund of all federal income tax withheld because I expect to have no tax liability. If you meet both conditions, write Exempt here Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete. Employee s signature (This form is not valid unless you sign it.) Date 8 Employer s name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.) 9 Office code (optional) 10 Employer identification number (EIN) For Privacy Act and Paperwork Reduction Act Notice, see page 2. Cat. No Q Form W-4 (2015)

4 Form W-4 (2015) Page 2 Deductions and Adjustments Worksheet Note. Use this worksheet only if you plan to itemize deductions or claim certain credits or adjustments to income. 1 Enter an estimate of your 2015 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state and local taxes, medical expenses in excess of 10% (7.5% if either you or your spouse was born before January 2, 1951) of your income, and miscellaneous deductions. For 2015, you may have to reduce your itemized deductions if your income is over $309,900 and you are married filing jointly or are a qualifying widow(er); $284,050 if you are head of household; $258,250 if you are single and not head of household or a qualifying widow(er); or $154,950 if you are married filing separately. See Pub. 505 for details $ $12,600 if married filing jointly or qualifying widow(er) 2 Enter: { $9,250 if head of household } $ $6,300 if single or married filing separately 3 Subtract line 2 from line 1. If zero or less, enter $ 4 Enter an estimate of your 2015 adjustments to income and any additional standard deduction (see Pub. 505) 4 $ 5 Add lines 3 and 4 and enter the total. (Include any amount for credits from the Converting Credits to Withholding Allowances for 2015 Form W-4 worksheet in Pub. 505.) $ 6 Enter an estimate of your 2015 nonwage income (such as dividends or interest) $ 7 Subtract line 6 from line 5. If zero or less, enter $ 8 Divide the amount on line 7 by $4,000 and enter the result here. Drop any fraction Enter the number from the Personal Allowances Worksheet, line H, page Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet, also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1 10 Two-Earners/Multiple Jobs Worksheet (See Two earners or multiple jobs on page 1.) Note. Use this worksheet only if the instructions under line H on page 1 direct you here. 1 Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet) 1 2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if you are married filing jointly and wages from the highest paying job are $65,000 or less, do not enter more than If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter -0- ) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet Note. If line 1 is less than line 2, enter -0- on Form W-4, line 5, page 1. Complete lines 4 through 9 below to figure the additional withholding amount necessary to avoid a year-end tax bill. 4 Enter the number from line 2 of this worksheet Enter the number from line 1 of this worksheet Subtract line 5 from line Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here $ 8 Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed.. 8 $ 9 Divide line 8 by the number of pay periods remaining in For example, divide by 25 if you are paid every two weeks and you complete this form on a date in January when there are 25 pay periods remaining in Enter the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck 9 $ Table 1 Table 2 Married Filing Jointly All Others Married Filing Jointly All Others If wages from LOWEST paying job are Enter on line 2 above $0 - $6, ,001-13, ,001-24, ,001-26, ,001-34, ,001-44, ,001-50, ,001-65, ,001-75, ,001-80, , , , , , , , , , , ,001 and over 15 If wages from LOWEST paying job are Enter on line 2 above $0 - $8, ,001-17, ,001-26, ,001-34, ,001-44, ,001-75, ,001-85, , , , , , , ,001 and over 10 Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this form to carry out the Internal Revenue laws of the United States. Internal Revenue Code sections 3402(f)(2) and 6109 and their regulations require you to provide this information; your employer uses it to determine your federal income tax withholding. Failure to provide a properly completed form will result in your being treated as a single person who claims no withholding allowances; providing fraudulent information may subject you to penalties. Routine uses of this information include giving it to the Department of Justice for civil and criminal litigation; to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws; and to the Department of Health and Human Services for use in the National Directory of New Hires. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. If wages from HIGHEST paying job are Enter on line 7 above $0 - $75,000 $600 75, ,000 1, , ,000 1, , ,000 1, , ,000 1, ,001 and over 1,580 If wages from HIGHEST paying job are Enter on line 7 above $0 - $38,000 $600 38,001-83,000 1,000 83, ,000 1, , ,000 1, ,001 and over 1,580 You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by Code section The average time and expenses required to complete and file this form will vary depending on individual circumstances. For estimated averages, see the instructions for your income tax return. If you have suggestions for making this form simpler, we would be happy to hear from you. See the instructions for your income tax return.
; $284,050 if you are head of household;")
5 MI-W4 (Rev ) EMPLOYEE'S MICHIGAN WITHHOLDING EXEMPTION CERTIFICATE STATE OF MICHIGAN - DEPARTMENT OF TREASURY This certificate is for Michigan income tax withholding purposes only. You must file a revised form within 10 days if your exemptions decrease or your residency status changes from nonresident to resident. Read instructions below before completing this form. 1. Social Security Number 2. Date of Birth Issued under P.A. 281 of Type or Print Your First Name, Middle Initial and Last Name 4. Driver's License Number or State ID Home Address (No., Street, P.O. Box or Rural Route) 5. Are you a new employee? City or Town State ZIP Code Yes No If Yes, enter date of hire Enter the number of personal and dependent exemptions you are claiming Additional amount you want deducted from each pay (if employer agrees) I claim exemption from withholding because (does not apply to nonresident members of flow-through entities - see instructions): a. A Michigan income tax liability is not expected this year. b. Wages are exempt from withholding. Explain: c. Permanent home (domicile) is located in the following Renaissance Zone: EMPLOYEE: If you fail or refuse to file this form, your employer must withhold Michigan income tax from your wages without allowance for any exemptions. Keep a copy of this form for your records. INSTRUCTIONS TO EMPLOYER: Employers must report all new hires to the State of Michigan. Keep a copy of this certificate with your records. If the employee claims 10 or more personal and dependent exemptions or claims a status exempting the employee from withholding, you must file their original MI-W4 form with the Michigan Department of Treasury. Mail to: New Hire Operations Center, P.O. Box 85010; Lansing, MI You must submit a Michigan withholding exemption certificate (form MI-W4) to your employer on or before the date that employment begins. If you fail or refuse to submit this certificate, your employer must withhold tax from your compensation without allowance for any exemptions. Your employer is required to notify the Michigan Department of Treasury if you have claimed 10 or more personal and dependent exemptions or claimed a status which exempts you from withholding. You MUST file a new MI-W4 within 10 days if your residency status changes or if your exemptions decrease because: a) your spouse, for whom you have been claiming an exemption, is divorced or legally separated from you or claims his/her own exemption(s) on a separate certificate, or b) a dependent must be dropped for federal purposes. Line 5: If you check "Yes," enter your date of hire (mo/day/year). Line 6: Personal and dependent exemptions. The total number of exemptions you claim on the MI-W4 may not exceed the number of exemptions you are entitled to claim when you file your Michigan individual income tax return. If you are married and you and your spouse are both employed, you both may not claim the same exemptions with each of your employers. 6. $.00 Under penalty of perjury, I certify that the number of withholding exemptions claimed on this certificate does not exceed the number to which I am entitled. If claiming exemption from withholding, I certify that I anticipate that I will not incur a Michigan income tax liability for this year. 9. Employee's Signature Date Employer: Complete lines 10 and 11 before sending to the Michigan Department of Treasury. 10. Employer's Name, Address, Phone No. and Name of Contact Person INSTRUCTIONS TO EMPLOYEE Federal Employer Identification Number If you hold more than one job, you may not claim the same exemptions with more than one employer. If you claim the same exemptions at more than one job, your tax will be under withheld. Line 7: You may designate additional withholding if you expect to owe more than the amount withheld. Line 8: You may claim exemption from Michigan income tax withholding ONLY if you do not anticipate a Michigan income tax liability for the current year because all of the following exist: a) your employment is less than full time, b) your personal and dependent exemption allowance exceeds your annual compensation, c) you claimed exemption from federal withholding, d) you did not incur a Michigan income tax liability for the previous year. You may also claim exemption if your permanent home (domicile) is located in a Renaissance Zone or you are a non-resident spouse of military personnel stationed in Michigan. Members of flow-through entities may not claim exemption from nonresident flow-through withholding. For more information on Renaissance Zones call (517) Full-time students that do not satisfy all of the above requirements cannot claim exempt status. Visit the Treasury Web site at:
 5. Are you a new employee? City or Town State ZIP Code Yes No If Yes, enter date of hire.... 6. 7. 8.")
6 Form SW-4 Instructions - revised 1/05/10 Purpose: Complete form SW-4 so your employer can withhold the correct amount of city income taxes from your pay. Dependents: To qualify as your dependent (line 4 below), a person (a) Must receive more than one-half of his or her support from you for the year, and (b) Must have less than $ gross income during the year (except your child who is a student or who is under 19 years of age, and (c) Must not be claimed as an exemption by such person s husband or wife, and (d) Must be a citizen or resident of the United States, and (e) Must have your home as his/her principal residence and be a member of your household for the entire year, or Must be related to you as follows: Your son or daughter, grandchild, step-son/daughter, son/daughter-in-law, father, mother, grandparent, step-father/mother, father/mother-in-law, brother, sister, stepbrother/sister, half brother/sister, brother/sister-in-law, uncle, aunt, nephew, or niece (but only if related by blood). Changes in exemptions: You must file a new certificate within 10 days if the number of exemptions previously claimed by you decreases for any of the following reasons: (a) Your wife/husband for whom you have been claiming exemption is divorced or legally separated, or claims her/his own exemption on a separate certificate. (b) The support of a dependent for whom you claimed exemption is taken over by someone else. (c) You find that a dependent for whom you claimed exemption will receive $ or more income of his/her own during the year (except your child who is a student and who is under 19 years of age). Other Decreases: Such as the death of a wife, husband, or a dependent, do not affect your withholding until the next year, but require the filing of a new certificate by December 1 of the year in which they occur. Change of Residence: You must file a new certificate within 10 days after you change your residence from or to a taxing city. Employee: File this form with your employer. Otherwise your employer must withhold City of Saginaw income tax from your earnings without exemptions. Employer: Keep this certificate with your record. If the information submitted by the employee is not believed to be true, correct and complete the City of Saginaw must be advised. FORM SW-4 EMPLOYEE S WITHHOLDING CERTIFICATE FOR CITY OF SAGINAW INCOME TAX City Resident or Non-City Resident Your Social Security Number: Full Name: (First, Middle and Last Name) Home Address: (Number & Street) City: State: Zip Code: Main place of employment: City: Under Print name of each city where you work for this employer 25% 40% 60% 80% 100% and circle closest % of total earnings in each. This is for withholding purposes only. City: Under 25% 40% 60% 80% 100% 1. Exemptions for yourself: 2. Exemptions for your spouse: 3. Enter Total number of boxes checked in 1& 2: Yourself age 65 or over Blind Yourself age 65 or over Blind 4. Other Exemptions: Number of exemptions Number of exemptions 5. Enter total number of Other Exemptions in box 4 below: for your children for your other dependents 6. Add the number of exemptions which you have claimed in box 3 & 5 and write the total below: Employer s Name and Address: 7. Write the additional amounts you want withheld from each paycheck, if any: I certify that the information submitted on this certificate is true, correct and complete to the best of my knowledge and belief. SIGNATURE: DATE:
 Must have your home as his/her principal residence and be a member of your household for the entire year, or Must be related to you as follows: Your")
7
8
9
10

11
12 DIRECT DEPOSIT Revised July 2014 Direct deposit advices are delivered to employees online via MyDelta. For questions about direct deposits contact payroll at Employee Name Employee ID or SSN Employee Phone Number NEW/ADDITIONAL DEPOSIT MAY TAKE UP TO ONE MONTH TO GO INTO EFFECT (Payroll use only) Bank/Credit Union Name Deposit code Address City, State Bank Routing Number Contact your Institution for this number Type of account for Deposit Checking Savings Account Number Dollar Amount $ Enter Total Check to have your entire check deposited or enter a specific dollar amount to have a portion of you check deposited CHANGE MAY TAKE UP TO ONE MONTH TO GO INTO EFFECT This is for changing the dollar amount or account number only at your current bank/credit union. If you want your deposit to go to another Institution, you must cancel your existing direct deposit (CANCEL section below) and then fill out the New/Additional Deposit section (above). Bank/Credit Union Name Type of account for Deposit Checking Savings Change Account Number to (Payroll use only) Deposit code Change Dollar Amount to $ Enter Total Check to have your entire check deposited or enter a specific dollar amount to have a portion of you check deposited CANCEL REQUIRES FIVE (5) DAYS ADVANCE NOTICE Please cancel my existing Direct Deposit to Institution Name Account Number AUTHORIZATION * I authorize Delta College and the financial institution listed to deposit my pay automatically to my account each payday. Adjusting entries to correct errors are also authorized. This authority will remain in effect until I have cancelled it in writing. * I understand that if I am setting up a new direct deposit or changing account numbers or banking institutions, that I will receive a printed paycheck in the interim until my direct deposit is officially established. Paychecks are available for pickup at the Cashier s Office. SIGNATURE DATE

13 DELTA COLLEGE POSITION STATEMENT ON DRUG-FREE WORK PLACE ACT OF 1988 By signing below, this indicates that I acknowledge receipt of the Delta College Position Statement on the Drug-Free Workplace Act of Print Name Human Resources Office Employee Signature Received by Date Date INTRODUCTION Under the Drug-Free Work Place Act of 1988 effective March 18, 1989, all Federal grant recipients are required to publish a statement, notifying employees that the unlawful manufacture, distributions, dispensation, possession, or use of a controlled substance is prohibited in the work place, specifying the sanctions that will take place against violators of their policy. The following is the position statement of Delta College pursuant to the requirements of such act. DRUG-FREE WORK PLACE ACT OF 1988 STATEMENT No member of the college community shall manufacture, possess, distribute or use any prohibited drug in either the refines or crude form, except: (1) Controlled substance for personal usage must be under a current prescription of a licensed physician. (2) Those specifically authorized to Delta College by federal or state authorizing agencies for educational purposes, nor shall any member of the college community possess property, which is used, or intended for use, as a container for any controlled substances. Such policy is specifically applicable to college employees during the course of their employment or at their work place. Employees who admit to violating such policy or are found to be in violation by a judicial process of the state or Delta College shall be suspended from employment. Employees who are certified to medically dependent (hereafter dependent employees) by a licensed physician will be considered to have a health problem and eligible for medical leave provided they participate in a recognized medically supervised program of treatment for chemical dependency under the following conditions:

14 (a) Dependent employees will first obtain Delta s written consent to participate in a specified treatment program. (b) Dependent employees who voluntarily enroll in such a recognized program may use personal and/or vacation time, if medical leave is not available, or may apply to borrow sick leave. Otherwise, such employees will be considered to be on an approved leave of absence (without pay) for the period of the rehabilitation program. (c) During the period of enrollment in the program, such employees will comply with all medical decisions made by the treating or supervising physician of the program under the above conditions after being given the opportunity to participate, will be subject to disciplinary action including suspension for a stated period of time, or termination of employment (d) A dependent employee will be given only one opportunity for rehabilitation. If after returning to work it is determined by Delta that such employee has again violated any of Delta's rules and regulations related to possession or use of illegal drugs, or that such employee has been convicted of a drug related violation in the workplace, such employee will be subject to immediate discharge. (e) Dependent employees who do not participate in a rehabilitation program under the above conditions after being given the opportunity to participate, will be subject to disciplinary action including suspension for a stated period of time, or termination of employment. All employees are notified that as a condition of employment each employee shall abide by the terms of this statement and must further notify Delta College of any criminal drug statute conviction for a violation occurring in the workplace no later than five (5) days after receiving such conviction. Upon such notification, if funded under a Federal Grant, The Human Resources Office of the college must notify the granting agency within (10) days. Delta College has established and is making a good faith effort to maintain a drug-free workplace through the implementation of a drug-free awareness program to inform and educate employees about: (1) The dangers of drug abuse in the workplace, (2) The policy of maintaining a drug-free workplace; (3) Any available drug counseling, rehabilitation, and employee assistance program; and (4) The penalties that may be imposed upon employees from drug violations occurring in the workplace. Employees should make a copy of this policy for their own records.
 During the period of enrollment in the program, such employees will comply with all medical decisions made by the treating or supervising physician of the program under the above conditions after")
15 DELTA COLLEGE EMPLOYEES ACKNOWLEDGEMENT AND RELEASE FORM HEPATITIS B VACCINATION Only complete if you are a Category A Employee Please check with your supervisor for clarification if you are unsure whether or not your position is considered Category A. The following jobs have been identified as requiring procedures or tasks which involve exposure or reasonably anticipated exposure to blood or other potentially hazardous material: Public Safety Dental Assisting - Faculty, Staff & Students Exploratory Teaching - Faculty, Staff & Students Fire Science Technology Faculty, Staff & Students Nursing LPN - Faculty, Staff & Students Phlebotomy - Faculty, Staff & Students Respiratory Care - Faculty, Staff & Students Lifeguards Coaches Dental Hygiene - Faculty, Staff & Students Facilities Management Staff Multimedia Learning Lab (MLL) Technicians Nursing RN - Faculty, Staff & Students Designated Ctr Personnel -Planetarium, Saginaw & Midland Surgical Technology - Faculty, Staff & Students Operations Assistants Science courses with microbiology components and/or involving human specimen collection - Faculty, Staff & Students involved in BIO 102 and BIO 203 I understand that due to my occupational exposure to blood or other potentially infectious materials I may be at risk of acquiring hepatitis B virus (HBV) infection. I have been given the opportunity to be vaccinated with hepatitis B vaccine, at no charge to me. IF YOU CHOOSE TO DECLINE. If I decline the vaccination at this time, I understand that I continue to be at risk of acquiring hepatitis B, a serious disease. If in the future I still have occupational exposure risk and want to be vaccinated, I can receive the vaccine series at no charge to me. MAKE YOUR DECISION, CHECK ONE OF THE FOLLOWING: I have ALREADY RECEIVED the hepatitis B vaccine and decline the vaccination provided by Delta College. I WOULD LIKE TO RECEIVE the hepatitis B vaccine series provided by Delta College. I DECLINE the vaccine and release Delta College from liability should I become infected. EMPLOYEE S NAME (print): EMPLOYEE S SIGNATURE: DATE: DEPARTMENT/DIVISION: PHONE:

16 BLUE CROSS/BLUE SHIELD AND DELTA DENTAL ENROLLMENT/CHANGE FORM CORPORATE SERVICES DOW BPSC EMPLOYEE GROUP Section I - Select action to be taken: Enrollment: Birth of Child Marriage/Divorce New Hire Dependent Change Separation: Retirement Resignation Other Dependent Change Effective date of action: (New hires are effective the first of the month following date of hire.) Section II Enrollment (check box to enroll) Blue Cross/Blue Shield Community Blue PPO #1 PPO #15 Delta Dental of Michigan Dental Eligible for health benefits but elect to not participate. Decline Health Section III Employee Subscriber Name: Address: Social Security No: City/State/Zip: Phone: Marital Status: Sex: Date of Hire: Date of Birth: Section IV - List all person(s) to be added or removed from coverage. Spouse Name (Last, First, MI) Social Security # Birth Date M/F Check One Add Remove Dep. 1 Dep. 2 Dep. 3 Dep. 4 If you are adding/removing a spouse and/or dependents, a copy of your marriage license and dependent(s) birth certificate are needed for adding and divorce decree for removing. (COPY ONLY) is required. Any changes in covered family members, if due to birth of a child, marriage, divorce, death, dependent obtains own coverage or no longer meets eligibility, must be communicated to the Human Resources within 30 days of the effective date to ensure dependents are removed and/or added to coverage without a delay and to avoid being liable for insurance claims and college health and dental premiums paid. COBRA NOTIFICATION ADDRESS: Complete only if you are discontinuing coverage for a covered member. You can enroll or change your Flexible Spending if you have a change of status. Refer to the Flexible Spending Summary Plan Description for eligibility Flexible Spending Summary Plan Description You must make a new election within 30 days of your qualified change in family status for it to be effective for the remainder of the year. Employee Signature: Date: HUMAN RESOURCES OFFICE USE ONLY Benefit Datatel Processed COBRA Transfer Benefit Effective/Separation Date Processed From: To: Health Dental Dep Chg / 1095C PREL / PBVN
 to be added")
17 Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, jobprotected leave to eligible employees for the following reasons: For incapacity due to pregnancy, prenatal medical care or child birth; To care for the employee s child after birth, or placement for adoption or foster care; To care for the employee s spouse, son or daughter, or parent, who has a serious health condition; or For a serious health condition that makes the employee unable to perform the employee s job. Military Family Leave Entitlements Eligible employees with a spouse, son, daughter, or parent on active duty or call to active duty status in the National Guard or Reserves in support of a contingency operation may use their 12-week leave entitlement to address certain qualifying exigencies. Qualifying exigencies may include attending certain military events, arranging for alternative childcare, addressing certain financial and legal arrangements, attending certain counseling sessions, and attending post-deployment reintegration briefings. FMLA also includes a special leave entitlement that permits eligible employees to take up to 26 weeks of leave to care for a covered servicemember during a single 12-month period. A covered servicemember is a current member of the Armed Forces, including a member of the National Guard or Reserves, who has a serious injury or illness incurred in the line of duty on active duty that may render the servicemember medically unfit to perform his or her duties for which the servicemember is undergoing medical treatment, recuperation, or therapy; or is in outpatient status; or is on the temporary disability retired list. Benefits and Protections During FMLA leave, the employer must maintain the employee s health coverage under any group health plan on the same terms as if the employee had continued to work. Upon return from FMLA leave, most employees must be restored to their original or equivalent positions with equivalent pay, benefits, and other employment terms. Use of FMLA leave cannot result in the loss of any employment benefit that accrued prior to the start of an employee s leave. Eligibility Requirements Employees are eligible if they have worked for a covered employer for at least one year, for 1,250 hours over the previous 12 months, and if at least 50 employees are employed by the employer within 75 miles. Definition of Serious Health Condition A serious health condition is an illness, injury, impairment, or physical or mental condition that involves either an overnight stay in a medical care facility, or continuing treatment by a health care provider for a condition that either prevents the employee from performing the functions of the employee s job, or prevents the qualified family member from participating in school or other daily activities. Subject to certain conditions, the continuing treatment requirement may be met by a period of incapacity of more than 3 consecutive calendar days combined with at least two visits to a health care provider or one visit and a regimen of continuing treatment, or incapacity due to pregnancy, or incapacity due to a chronic condition. Other conditions may meet the definition of continuing treatment. EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT Use of Leave An employee does not need to use this leave entitlement in one block. Leave can be taken intermittently or on a reduced leave schedule when medically necessary. Employees must make reasonable efforts to schedule leave for planned medical treatment so as not to unduly disrupt the employer s operations. Leave due to qualifying exigencies may also be taken on an intermittent basis. Substitution of Paid Leave for Unpaid Leave Employees may choose or employers may require use of accrued paid leave while taking FMLA leave. In order to use paid leave for FMLA leave, employees must comply with the employer s normal paid leave policies. Employee Responsibilities Employees must provide 30 days advance notice of the need to take FMLA leave when the need is foreseeable. When 30 days notice is not possible, the employee must provide notice as soon as practicable and generally must comply with an employer s normal call-in procedures. Employees must provide sufficient information for the employer to determine if the leave may qualify for FMLA protection and the anticipated timing and duration of the leave. Sufficient information may include that the employee is unable to perform job functions, the family member is unable to perform daily activities, the need for hospitalization or continuing treatment by a health care provider, or circumstances supporting the need for military family leave. Employees also must inform the employer if the requested leave is for a reason for which FMLA leave was previously taken or certified. Employees also may be required to provide a certification and periodic recertification supporting the need for leave. Employer Responsibilities Covered employers must inform employees requesting leave whether they are eligible under FMLA. If they are, the notice must specify any additional information required as well as the employees rights and responsibilities. If they are not eligible, the employer must provide a reason for the ineligibility. Covered employers must inform employees if leave will be designated as FMLA-protected and the amount of leave counted against the employee s leave entitlement. If the employer determines that the leave is not FMLAprotected, the employer must notify the employee. Unlawful Acts by Employers FMLA makes it unlawful for any employer to: Interfere with, restrain, or deny the exercise of any right provided under FMLA; Discharge or discriminate against any person for opposing any practice made unlawful by FMLA or for involvement in any proceeding under or relating to FMLA. Enforcement An employee may file a complaint with the U.S. Department of Labor or may bring a private lawsuit against an employer. FMLA does not affect any Federal or State law prohibiting discrimination, or supersede any State or local law or collective bargaining agreement which provides greater family or medical leave rights. FMLA section 109 (29 U.S.C. 2619) requires FMLA covered employers to post the text of this notice. Regulations 29 C.F.R (a) may require additional disclosures. For additional information: US-WAGE ( ) TTY: U.S. Department of Labor Employment Standards Administration Wage and Hour Division WHD Publication 1420 Revised January 2009

18 HIPAA NOTICE THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. If you have any questions about this Notice, please contact: Delta College HIPAA Privacy Officer 1961 Delta Road University Center, MI (989) NOTICE EFFECTIVE DATE: APRIL 14, 2004 THIS NOTICE GIVES YOU INFORMATION REQUIRED BY LAW about the duties and privacy practices of the Delta College Group Health Plans (the Plans ) to protect the privacy of your medical information. The Delta College Group Health Plans consist of the following components: Blue Cross/Blue Shield Medical Plans Delta Dental Plan Blue Cross/Blue Shield Vision Plans Flexible Spending Plan Health Care Expense Reimbursement Account The Plans provide health and/or dental benefits to you as described in your summary plan descriptions. The Plans receive and maintain your medical information in the course of providing these health benefits to you. The Plans may hire business associates to help provide these benefits to you. These business associates also receive and maintain your medical information in the course of assisting the Plans. The Plans are sponsored by Delta College (the Plan Sponsor ). The Plans are all subject to the same federal privacy law, and are part of an Organized Health Care Arrangement ( OHCA ) that follows the same privacy policies and procedures. This notice applies to the Flexible Spending Plan Health Care Expense Reimbursement Account. Blue Cross/Blue Shield of Michigan and Delta Dental each issued a Notice of Privacy Practices for their plans, which describes how they may use and disclose health information in connection with the coverage they provide for the Delta College Group Health Plans. Our purpose for providing you with this notice is to tell you how the Plans and the third parties that assist in plan administration will use and disclose health information about you. The description of the uses and disclosures of medical information applies to the Plans and to the entities that perform services for the Plans or perform the functions of the Plans.

19 The Plans are required to follow the terms of this notice until it is replaced. The Plans reserve the right to change the terms of this notice at any time. If the Plans make changes to this notice, the Plans will revise it and send a new notice to all subscribers covered by the Plans at that time. The Plans reserve the right to make the new changes apply to all of your medical information maintained by the Plans before and after the effective date of the new notice. For ease of reference, this Notice will use the word Plan to mean each of the Plans identified above. PURPOSES FOR WHICH THE PLAN MAY USE OR DISCLOSE YOUR MEDICAL INFORMATION WITHOUT YOUR CONSENT OR AUTHORIZATION The Plan may use and disclose your medical information for the following purposes: Health Care Providers Treatment Purposes. The Plan may disclose your medical information to your health care providers, at their request, for your treatment by them. For example, the Plan may disclose to your primary care physician the name of a specialist who is treating you so that they may coordinate your care. Payment. The Plan may use or disclose your medical information to determine eligibility for plan benefits, to facilitate payment for the treatment and services you receive from health care providers, to determine benefit responsibility under the Plan, or to coordinate plan coverage. For example, the Plan may tell your health care provider about your medical history to determine whether a particular treatment is experimental, investigational, or medically necessary or to determine whether the Plan will cover the treatment. Health Care Operations. The Plan may use or disclose your medical information as necessary to operate the Plan, including plan management and administrative activities. For example, the Plan may (i) conduct quality assessment and improvement activities, (ii) underwriting, premium rating, or other activities relating to the creation, renewal or replacement of a contract of health insurance, (iii) authorize business associates to perform data aggregation services, (iv) engage in care coordination or case management, and (v) manage, plan or develop the Plan s business. As required by law. The Plan must allow the U.S. Department of Health and Human Services to audit the Plan s records. The Plan may also disclose your medical information as authorized by and to the extent necessary as required by federal, state or local law, including compliance with workers compensation or other similar laws. To Business Associates. The Plan may disclose your medical information to business associates the Plan hires to assist the Plan. Each business associate of the Plan must agree in writing to ensure the continuing confidentiality and security of your medical information. To Plan Sponsor. The Plan may disclose to the Plan Sponsor, in summary form, claims history and other similar information. Such summary information does not disclose your name or other distinguishing characteristics. The Plan may also disclose to the Plan Sponsor the fact that you are enrolled in, or disenrolled from the Plan. The Plan may disclose your

20 medical information to the Plan Sponsor for plan administrative functions that the Plan Sponsor provides to the Plan if the Plan Sponsor agrees in writing to ensure the continuing confidentiality and security of your medical information. The Plan Sponsor must also agree not to use or disclose your medical information for employment-related activities. To Plans in the OHCA. Your medical information may be shared, used and disclosed among the Plans sponsored by Delta College and their business associates for purposes of facilitating and coordinating health care treatment, payments and operations, including the health care operations of the Organized Health Care Arrangement ( OHCA ). The Plan may also use and disclose your medical information as follows: To comply with legal proceedings, such as a court or administrative order or subpoena; To law enforcement officials for limited law enforcement purposes; To a family member, friend or other person, for the purpose of helping you with your health care or with payment for your health care, if you are in a situation such as a medical emergency and you cannot give your agreement to the Plan; To your personal representatives appointed by you or designated by applicable law; For research purposes in limited circumstances; To a coroner, medical examiner, or funeral director about a deceased person; To an organ procurement organization in limited circumstances; To avert a serious threat to your health or safety or the health or safety of others; To a governmental agency authorized to oversee the health care system or government programs; To federal officials for lawful intelligence, counterintelligence and other national security purposes; To public health authorities for public health purposes; To appropriate military authorities, if you are a member of the armed forces. USES AND DISCLOSURES WITH YOUR PERMISSION The Plan will not use or disclose your medical information for any other purposes unless you give the Plan your written authorization to do so. If you give the Plan written authorization to use or disclose your medical information for a purpose that is not described in this notice, then, in most cases, you may revoke it in writing at any time. Your revocation will be effective for all your medical information the Plan maintains, unless the Plan has taken action in reliance on your authorization. YOUR RIGHTS You have certain rights with respect to your health information. To exercise these rights, you or your personal representative must make your request, in writing, directed to the Delta College HIPAA Privacy Officer. The HIPAA Privacy Officer will give you the necessary information and forms for you to complete and return to the HIPAA Privacy Officer. In some cases, the Plan may charge you a nominal, cost-based fee to carry out your request.
.")
21 You have the right to: Request restrictions on certain uses and disclosures of your health information; however the Plan is not required to agree to a requested restriction; Receive confidential communications of your health information. You may request that the Plan communicates with you about your health information by alternative means or at an alternative location; Inspect and obtain a copy of your health information, except with regard to psychotherapy notes or information compiled in reasonable anticipation of certain civil, criminal or administrative proceedings; Request an amendment to your health information that the Plan has created, except with regard to those portions of your health information that you are precluded from inspecting and copying as set forth above; Obtain an accounting of certain disclosures of your health information; and Receive a paper copy of this notice in addition to any electronic copy you may receive. COMPLAINTS If you believe your privacy rights have been violated by the Plan, you have the right to complain to the Plan or to the Secretary of the U.S. Department of Health and Human Services. You may file a complaint to the Plan, in writing, directed to the Delta College HIPAA Privacy Officer. You will not be penalized or retaliated against if you choose to file a complaint. Delta College HIPAA Privacy Officer 1961 Delta Road University Center, MI (989)
22 Important Notice from Delta College About Your Prescription Drug Coverage and Medicare Please read this notice carefully and keep it where you can find it. This notice has information about your current prescription drug coverage with Delta College and about your options under Medicare s prescription drug coverage. This information can help you decide whether or not you want to join a Medicare drug plan. If you are considering joining, you should compare your current coverage, including which drugs are covered at what cost, with the coverage and costs of the plans offering Medicare prescription drug coverage in your area. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice. There are two important things you need to know about your current coverage and Medicare s prescription drug coverage: 1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get this coverage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like an HMO or PPO) that offers prescription drug coverage. All Medicare drug plans provide at least a standard level of coverage set by Medicare. Some plans may also offer more coverage for a higher monthly premium. 2. Delta College has determined that the prescription drug coverage offered by the Delta College Health Plan is, on average for all plan participants, expected to pay out as much as standard Medicare prescription drug coverage pays and is therefore considered Creditable Coverage. Because your existing coverage is Creditable Coverage, you can keep this coverage and not pay a higher premium (a penalty) if you later decide to join a Medicare drug plan. When Can You Join A Medicare Drug Plan? You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15 th through December 7 th. However, if you lose your current creditable prescription drug coverage, through no fault of your own, you will also be eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan. What Happens to Your Current Coverage If You Decide to Join A Medicare Drug Plan? If you do decide to enroll in a Medicare prescription drug plan and drop your Delta College prescription drug coverage, be aware that you and your dependents may not be able to get the coverage back. When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan? You should also know that if you drop or lose your current coverage with Delta College and don t join a Medicare drug plan within 63 continuous days after your current coverage ends, you may pay a higher premium (a penalty) to join a Medicare drug plan later. If you go 63 continuous days or longer without creditable prescription drug coverage, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have that coverage. For example, if you go nineteen months without
23 creditable coverage, your premium may consistently be at least 19% higher than the Medicare base beneficiary premium. You may have to pay this higher premium (a penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join. For More Information About This Notice Or Your Current Prescription Drug Coverage Contact the person listed below for further information. NOTE: You ll get this notice each year. You will also get it before the next period you can join a Medicare drug plan, and if this coverage through Delta College changes. You also may request a copy of this notice at any time. For More Information About Your Options Under Medicare Prescription Drug Coverage More detailed information about Medicare plans that offer prescription drug coverage is in the Medicare & You handbook. You ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans. For more information about Medicare prescription drug coverage: Visit Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the Medicare & You handbook for their telephone number) for personalized help Call MEDICARE ( ). TTY users should call If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about this extra help, visit Social Security on the web at or call them at (TTY ). Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare drug plans, you may be required to provide a copy of this notice when you join to show whether or not you have maintained creditable coverage and, therefore, whether or not you are required to pay a higher premium (a penalty) Date: October 14, 2015 Entity: Delta College Contact: Shannon Mehl Address: 1961 Delta Road University Center, MI Phone: (989)
24 INJURY/ACCIDENT REPORTING PROCEDURE If an employee sustains a personal injury or occupational disease, which arises out of and in the course of employment, the employee must file a work-related claim of injury or illness. 1. All injuries/illnesses must be reported to Public Safety (Ext. 9111) within 24 hours of the injury/illness. 2. Injuries/illnesses requiring treatment must be done within 28 days at Covenant Occupational Health Services. If treatment requires first aid only, the officer on duty shall administer first aid. If the employee needs to be transported to Covenant, Public Safety will assist with transportation or call an ambulance. 3. If at the time of the injury/illness you need to seek treatment, authorization must be given by Public Safety or the Human Resources Office (Ext. 9106) prior to receiving treatment. Employees electing to seek their own treatment will be responsible for all payments incurred. 4. If treatment is needed other than at the time of the injury, the employee must contact the Human Resources Office (9106 or 9107) for authorization to seek treatment at Covenant Occupational Health Services. 5. All employees seeking treatment due to a work related injury or illness will be drug and alcohol tested at the time of the visit. 6. The employee will be responsible for providing the Human Resources Office with a copy of their physician's statement. Human Resources will complete the appropriate forms to be forwarded to our Workers' Compensation Company. Any bills the employee receives as a result of the work-related injury/illness must be sent to the Human Resources Office. Any lost time as a result of a work-related injury or illness will be reported as sick leave, if available. Injuries/illnesses occurring off campus, which are work-related (i.e., at a College off campus facility or center, College sponsored trip, or approved off campus work assignment) shall be reported by phone as per instructions mentioned above.
25 REGULATIONS AND RULES OF CONDUCT Delta College has adopted rules consistent with its goals and operations and enforces them with appropriate due process. 1. General Responsibility: Delta College has the responsibility to adopt and enforce rules which are consistent with Delta College goals and operations and to establish due process procedures in disciplinary cases. 2. Authority to Establish Standards of Conduct: Standards of conduct are established by rules of the College, as adopted by the Board of Trustees, and made known through College publications or by notices distributed or prominently posted on College Bulletin Boards; and by the law of the United States, State of Michigan, and County of Bay (public laws). Except in the case of interim or emergency type rules as granted by Michigan Public Act No. 26 of 1970, such regulations will be established and amended with the advice of the College Senate, but final authority is through either the Delta College Board of Trustees or the laws of the United States, State of Michigan, or County of Bay. 3. Individual Responsibility: An individual having an institutional relationship to Delta College (members of the Community College) is automatically placed under the rules of the College. "Institutional relationship to the College" means any connection of employment, enrollment, or service existing between any person and Delta College. As used herein, this phraseology is intended to prevent the application of these rules to purely personal or social relationships between or among students, faculty members, administration, or staff members, outside of the College proper. Therefore, it is important for all members of the College Community to familiarize themselves with the rules and regulations affecting them. 4. Effect of Violating Rules: A member of the College Community violating any of the rules of the College, or a public law, on campus, or off campus at a Delta College sponsored activity, is subject to disciplinary action by Delta College that is appropriate to the nature of the offense. Such disciplinary action will be taken in accordance with the procedures governing cases of violation as outlined in the Delta College Judicial Process. 5. Reports of Violations: Reporting of violations will be within the province of all members of the College Community, because they have a common responsibility to maintain an orderly and efficient community for their mutual benefit. Violations may fall in one of several categories: (1) Minor offenses which are dealt with by reprimand; (2) Violations by students which are to be reported to the Vice President of Student Services; (3) Violations by faculty or staff members which are to be reported to the College President; and (4) Civil or criminal violations which are to be reported to the Office of Public Safety. 6. Severance Provision: If any of the foregoing rules or any part of such rule will be adjudged invalid by a court of competent jurisdiction, then such adjudication will not affect the validity of these rules as a whole or any provision or part of any such rule not so adjudged invalid. Rules and Regulations: 1. Physical Force: No member of the College Community will use physical force, threaten physical force, or use intimidation against any person engaged in an activity properly undertaken as part of an institutional relationship of the College except as permitted under normal law enforcement procedures. 2. Disruption: No member of the College Community will interfere with a College function by depriving any person of needed safety, quiet or other physical conditions of work or study. 3. Interference: No member of the College Community will interfere with the free movement of any person engaged in an activity properly undertaken as part of an institutional relationship to the College. 4. Compliance: In keeping with the system of voluntary compliance that underlies the reasonable instructions given by an appropriate College official to cease specified conduct, if such conduct threatens disruption or interference with: a. The rights of others b. College discipline c. College functions d. Order in the College Community 5. Identification: No member of the College Community will refuse to provide identification when requested to do so by an identified employee of the College.
26 6. Forbidden Occupation: No member of the College Community will, subsequent to reasonable notice to leave given by the College President, or an authorized designee, continue occupation of any College facility or property which is under the direct control or responsibility of the College, especially if such occupation interferes with a College function or is a risk of injury to a person or property. 7. Facility Entry and Usage: No member of the College Community will gain or attempt to gain unauthorized entry to or make unauthorized use of the College facilities or property. 8. Property: No member of the College Community will damage, deface, destroy, steal, or misappropriate the property of the College or of any member of the College community or of any visitor to the College campus. 9. Unauthorized Use of College Credit, Property, Etc.: No unauthorized member of the College Community will use the College telephones, postal machines and meters, duplicating machines, motorized vehicles, computers, or other equipment where the unauthorized use of any such instrumentalities results in the incurring of charges by the College. This provision will be deemed to also include College billing, charging and credit card numbers utilized for communications or transportation purposes. Further it will be a violation of this section for any member of the College Community who has not been issued a key by the College to possess or use College keys for any purpose whatsoever. 10. Counterfeiting, Altering and Copying: a. No member of the College Community, with intent to injure or defraud, will falsely make, forge, manufacture, print, reproduce, copy, tamper with, or alter any writing, document, record, or identification used or maintained by the College or by members of the College Community. b. No member of the College Community will knowingly posses, display, or cause or permit to be displayed any writing, record, document, or identification form used or maintained by the College or by members of the College Community, knowing the same to be fictitious, altered, forged, counterfeited, or made without proper authority. 11. Confidentiality of College Records: No person will inspect, investigate, or use College files (i.e., Counseling, Financial Aid, Placement, Registrar) without proper College authorization. 12. Firearms and Other Dangerous Material: The possession or use of firearms, firecrackers, explosives, toxic or dangerous chemicals, or other lethal weapons, equipment or material is not permitted on College property at any time except: a. When specifically authorized by the College for educational purposes, or b. When firearms used for recreational purposes and transported through the campus meet the regulations of the Office of Public Safety. 13. Alcoholic Beverages: No member of the College Community will possess or consume beer, wine, or other alcoholic beverages on College property, or any property which is under the direct control or responsibility of the College, excluding college housing, in which case regulation of such will be the responsibility of Food and Conference Services. This rule may be suspended from time to time by authorization of the President's Office. 14. Tobacco Free Campus Policy Philosophy. Effective August 1, 2007, Delta College became a tobocco free campus. 15. Drugs: No member of the College Community will possess, distribute, or use any prohibited drug in either the refined or crude form, nor will any member of the College community possess property which is used, or intended for use, as a container for any controlled substance except: a. Controlled substances for personal usage, and these must be under a current prescription of a licensed physician; b. Those specifically authorized to Delta College by Federal or State authorizing agencies for educational purposes. 16. Selling, Soliciting, and Distributing: Any person who wishes to distribute, solicit, or sell information, materials, goods, or services not within normal College activities and routine, must have the written permission of the Vice President of Student Services or Vice President of Finance and Business or their designee. 17. Private Business Ventures: Delta College facilities such as offices, computers, copiers, etc., are not to be used for private business ventures. Also, Delta College's name is not to be associated in any way (such as use of letterhead or return address) with private business ventures. 18. Animals: People may not bring animals on campus or into College buildings. Leader dogs and animals used for educational purposes are exceptions; however, all animals must remain under the control of their owners and be properly licensed and medically treated as required by law. 19. Federal, State, Local Laws: Violations of Federal, State, or local laws on campus, or off campus in connection with College sponsored activities, will constitute violations of College rules.
27 REQUIRED TRAINING MODULES All employees are required to view the: Bloodborne Pathogens, Copyright pt1 Provisions, Copyright pt6 Guidelines, Sexual Harassment, Diversity, FERPA, Hazard Communications, Title IX Higher Ed and SaVE Act modules. Delta College employees have access to training modules at the following link : Username: delta You can create a UID (Personal ID) by clicking Create New Account. Your User ID should simply be your First Name, Middle Initial and Last Name. Additional instructions for accessing the Global Compliance Network are available on the FAQ tab at the following link: After you review each module, click the submit button at the bottom and this will register you on the completion report that Human Resources will run to verify all modules were reviewed. If you have any questions or difficulties accessing these resources, please the Human Resources Office at
28 Notice of Employee Eligibility to Participate in 403(b) Retirement Plan All employees, excluding student workers, are eligible to participate in the Delta College 403(b) Retirement Plan immediately upon hire. Eligible employees may elect to make pre-tax salary reduction contributions to the 403(b) plan up to the maximum allowed by the IRS each tax year. Each participating employee chooses among the available investment options offered by the approved investment vendors under the plan. Employee contributions and the related investment earnings are tax deferred until withdrawn from the plan. Employees may enroll in the 403(b) plan by contacting one or more of the Delta College approved 403(b) vendors at any time throughout the year to speak to a representative. A list of approved vendors and representatives is available at After establishing a 403(b) account and making investment and beneficiary choices with a vendor representative, a completed Salary Reduction Agreement must be submitted to the Delta College Finance Office to begin making bi-weekly payroll deduction contributions to a 403(b) account. The Salary Reduction Agreement is available. This form may also be used to stop deductions or to make changes to the deduction amount. We ask that employees limit making changes to their salary reduction to 4 times per year. Links to the Plan Document and Adoption Agreement for the Delta College 403(b) Retirement Plan as amended 01/01/09 are as follows: Plan Document: Adoption Agreement: Please contact Jeanne Doyle at extension 9390 or [email protected] with any questions.
 PART A: General Information When key parts of the health care law take effect in 2014, there will be a new way to buy health insurance: the Health Insurance Marketplace.")
29 New Health Insurance Marketplace Coverage Options and Your Health Coverage Form Approved OMB No (expires ) PART A: General Information When key parts of the health care law take effect in 2014, there will be a new way to buy health insurance: the Health Insurance Marketplace. To assist you as you evaluate options for you and your family, this notice provides some basic information about the new Marketplace and employment based health coverage offered by your employer. What is the Health Insurance Marketplace? The Marketplace is designed to help you find health insurance that meets your needs and fits your budget. The Marketplace offers "one-stop shopping" to find and compare private health insurance options. You may also be eligible for a new kind of tax credit that lowers your monthly premium right away. Open enrollment for health insurance coverage through the Marketplace begins in October 2013 for coverage starting as early as January 1, Can I Save Money on my Health Insurance Premiums in the Marketplace? You may qualify to save money and lower your monthly premium, but only if your employer does not offer coverage, or offers coverage that doesn't meet certain standards. The savings on your premium that you're eligible for depends on your household income. Does Employer Health Coverage Affect Eligibility for Premium Savings through the Marketplace? Yes. If you have an offer of health coverage from your employer that meets certain standards, you will not be eligible for a tax credit through the Marketplace and may wish to enroll in your employer's health plan. However, you may be eligible for a tax credit that lowers your monthly premium, or a reduction in certain cost-sharing if your employer does not offer coverage to you at all or does not offer coverage that meets certain standards. If the cost of a plan from your employer that would cover you (and not any other members of your family) is more than 9.5% of your household income for the year, or if the coverage your employer provides does not meet the "minimum value" standard set by the Affordable Care Act, you may be eligible for a tax credit. 1 Note: If you purchase a health plan through the Marketplace instead of accepting health coverage offered by your employer, then you may lose the employer contribution (if any) to the employer-offered coverage. Also, this employer contribution -as well as your employee contribution to employer-offered coverage- is often excluded from income for Federal and State income tax purposes. Your payments for coverage through the Marketplace are made on an aftertax basis. How Can I Get More Information? For more information about your coverage offered by your employer, please check your summary plan description or contact Shannon Mehl, Benefits The Marketplace can help you evaluate your coverage options, including your eligibility for coverage through the Marketplace and its cost. Please visit HealthCare.gov for more information, including an online application for health insurance coverage and contact information for a Health Insurance Marketplace in your area. 1 An employer-sponsored health plan meets the "minimum value standard" if the plan's share of the total allowed benefit costs covered by the plan is no less than 60 percent of such costs.
30 PART B: Information About Health Coverage Offered by Your Employer This section contains information about any health coverage offered by your employer. If you decide to complete an application for coverage in the Marketplace, you will be asked to provide this information. This information is numbered to correspond to the Marketplace application. 3. Employer name 4. Employer Identification Number (EIN) \ Delta College Employer address 6. Employer phone number 1961 Delta Road City 8. State 9. ZIP code University Center Michigan Who can we contact about employee health coverage at this job? Shannon Mehl, Benefits Specialist 11. Phone number (if different from above) 12. address [email protected] Here is some basic information about health coverage offered by this employer: As your employer, we offer a health plan to: All employees. Eligible employees are: Some employees. Eligible employees are: With respect to dependents: We do offer coverage. Eligible dependents are: We do not offer coverage. If checked, this coverage meets the minimum value standard, and the cost of this coverage to you is intended to be affordable, based on employee wages. ** Even if your employer intends your coverage to be affordable, you may still be eligible for a premium discount through the Marketplace. The Marketplace will use your household income, along with other factors, to determine whether you may be eligible for a premium discount. If, for example, your wages vary from week to week (perhaps you are an hourly employee or you work on a commission basis), if you are newly employed mid-year, or if you have other income losses, you may still qualify for a premium discount. If you decide to shop for coverage in the Marketplace, HealthCare.gov will guide you through the process. Here's the employer information you'll enter when you visit HealthCare.gov to find out if you can get a tax credit to lower your monthly premiums.
31 The information below corresponds to the Marketplace Employer Coverage Tool. Completing this section is optional for employers, but will help ensure employees understand their coverage choices. 13. Is the employee currently eligible for coverage offered by this employer, or will the employee be eligible in the next 3 months? Yes (Continue) 13a. If the employee is not eligible today, including as a result of a waiting or probationary period, when is the employee eligible for coverage? (mm/dd/yyyy) (Continue) No (STOP and return this form to employee) 14. Does the employer offer a health plan that meets the minimum value standard*? Yes (Go to question 15) No (STOP and return form to employee) 15. For the lowest-cost plan that meets the minimum value standard* offered only to the employee (don't include family plans): If the employer has wellness programs, provide the premium that the employee would pay if he/ she received the maximum discount for any tobacco cessation programs, and didn't receive any other discounts based on wellness programs. a. How much would the employee have to pay in premiums for this plan? $ b. How often? Weekly Every 2 weeks Twice a month Monthly Quarterly Yearly If the plan year will end soon and you know that the health plans offered will change, go to question 16. If you don't know, STOP and return form to employee. 16. What change will the employer make for the new plan year? Employer won't offer health coverage Employer will start offering health coverage to employees or change the premium for the lowest-cost plan available only to the employee that meets the minimum value standard.* (Premium should reflect the discount for wellness programs. See question 15.) a. How much would the employee have to pay in premiums for this plan? $ b. How often? Weekly Every 2 weeks Twice a month Monthly Quarterly Yearly An employer-sponsored health plan meets the "minimum value standard" if the plan's share of the total allowed benefit costs covered by the plan is no less than 60 percent of such costs (Section 36B(c)(2)(C)(ii) of the Internal Revenue Code of 1986)
32 DELTA COLLEGE PPO #1 Coverage Period: Beginning on or after 07/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at or by calling the number on the back of your BCBSM ID card. Important Questions What is the overall? Are there other s for specific services? Is there an out-of-pocket limit on my expenses? (May include a co-insurance maximum) What is not included in the out-of-pocket limit? Is there an overall annual limit on what the plan pays? Does this plan use a network of providers? Do I need a referral to see a specialist? Are there services this plan doesn t cover? Answers In-Network Out-of-Network $250 Individual/ $500 Family No. $6,600 Individual/ $13,200 Family $250 Individual/ $500 Family $2,000 Individual/ $4,000 Family Premiums, balance-billed charges, any pharmacy penalty and health care this plan doesn t cover. No. Yes. For a list of in-network providers, see or call the number on the back of your BCBSM ID card. No. Yes. Why this Matters: You must pay all the costs up to the amount before this plan begins to pay for covered services you use. Check your policy or plan document to see when the starts over (usually, but not always, January 1st). See the chart starting on page 2 for how much you pay for covered services after you meet the. You don t have to meet s for specific services, but see the chart starting on page 2 for other costs for services this plan covers. The out-of-pocket limit is the most you could pay during a coverage period (usually one year) for your share of the cost of covered services. This limit helps you plan for health care expenses. Even though you pay these expenses, they don t count toward the out-of-pocket limit. The chart starting on page 2 describes any limits on what the plan will pay for specific covered services, such as office visits. If you use an in-network doctor or other health care provider, this plan will pay some or all of the costs of covered services. Be aware, your in-network doctor or hospital may use an out-of-network provider for some services. Plans use the term in-network, preferred, or participating for providers in their network. See the chart starting on page 2 for how this plan pays different kinds of providers. You can see the specialist you choose without permission from this plan. Some of the services this plan doesn t cover are listed on page 5. See your policy or plan document for additional information about excluded services. Group Number /0002/0003/0004/0005/0006/0007 Questions: Call the number on the back of your BCBSM ID card or visit us at If you aren t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at or call the number on the back of your BCBSM ID card to request a copy. SBC of 8
33 Co-payments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service. Co-insurance is your share of the costs of a covered service, calculated as a percent of the allowed amount for the service. For example, if the plan s allowed amount for an overnight hospital stay is $1,000, your co-insurance payment of 20% would be $200. This may change if you haven t met your. The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than the allowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay and the allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.) This plan may encourage you to use in-network providers by charging you lower s, co-payments and co-insurance amounts. Common Medical Event If you visit a health care provider s office or clinic If you have a test If you need drugs to treat your illness or condition Some plans may have a separate out of pocket maximum for prescription drug coverage, for more information please contact your plan administrator Services You May Need Primary care visit to treat an injury or illness Specialist visit Other practitioner office visit Your cost if you use a In-Network Provider Out-of-Network Provider Limitations & Exceptions $25 co-pay $25 co-pay $25 co-pay for chiropractic and osteopathic manipulative therapy for chiropractic and osteopathic manipulative therapy Preventive care/ No Charge Not Covered screening/immunization Diagnostic test (x-ray, blood work) Imaging (CT/PET scans, MRIs) Generic or select prescribed over-thecounter drugs Preferred brand-name drugs Nonpreferred brandname drugs No Charge after No Charge after $20 co-pay for retail 30-day supply; $40 co-pay for retail or mail order 90-day supply $40 co-pay for retail 30-day supply; $80 co-pay for retail or mail order 90-day supply $60 co-pay for retail 30-day supply; $120 co-pay for retail or mail order 90-day supply. In-Network co-pay plus an additional 25% of the approved amount In-Network co-pay plus an additional 25% of the approved amount In-Network co-pay plus an additional 25% of the approved amount Limited to a combined maximum of 24 visits per member per calendar year for chiropractic and osteopathic manipulative therapy. For information on women's contraceptive coverage, contact your plan administrator. 90-day supply not covered out-of-network. Specialty drugs limited to a 30-day supply per fill. 90-day supply not covered out-of-network. Specialty drugs limited to a 30-day supply per fill 90-day supply not covered out-of-network. Specialty drugs limited to a 30-day supply per fill 2 of 8
34 Common Medical Event If you have outpatient surgery If you need immediate medical attention If you have a hospital stay If you have mental health, behavioral health, or substance abuse needs If you are pregnant If you need help recovering or have other special health needs Services You May Need Facility fee (e.g., ambulatory surgery center) Your cost if you use a In-Network Provider Out-of-Network Provider No Charge after Physician/surgeon fees No Charge after Emergency room services Emergency medical transportation Urgent care Facility fee (e.g., hospital room) Physician/surgeon fee Mental/Behavioral health outpatient services Mental/Behavioral health inpatient services Substance use disorder outpatient services Substance use disorder inpatient services Prenatal and postnatal care Delivery and all inpatient services $150 co-pay $150 co-pay No Charge after No Charge after $40 co-pay No Charge after No Charge after No Charge after No Charge after 20% No Charge after No Charge after No Charge No Charge after co-insurance after Limitations & Exceptions Co-pay waived if admitted or for an accidental injury. Your cost share may be different for services performed in an office setting Home health care No Charge after No Charge after Rehabilitation services No Charge after Habilitation services Not Covered Not Covered Physical, Speech and Occupational Therapy is limited to a combined maximum of 60 visits per member, per calendar year. 3 of 8
35 Common Medical Event Services You May Need Your cost if you use a In-Network Provider Out-of-Network Provider Skilled nursing care No Charge after No Charge after Durable medical equipment No Charge after No Charge after Hospice service No Charge No Charge If your child needs Eye exam Not Covered Not Covered dental or eye care Glasses For more information on Not Covered Not Covered pediatric vision or dental, contact your plan administrator Dental check-up Not Covered Not Covered Limitations & Exceptions Limited to a maximum of 120 days per member per calendar year. 4 of 8
36 Excluded Services & Other Covered Services: Services Your Plan Does NOT Cover (This isn t a complete list. Check your policy or plan document for other excluded services.) Acupuncture Cosmetic surgery Dental care (Adult) Infertility treatment Long-term care Routine foot care Weight loss programs Other Covered Services (This isn t a complete list. Check your policy or plan document for other covered services and your costs for these services.) Bariatric surgery Chiropractic Care Coverage provided outside the United States. See If you are also covered by an account-type plan such as an integrated health flexible spending arrangement (FSA), health reimbursement arrangement (HRA), and/or a health savings account (HSA), then you may have access to additional funds to help cover certain out-of-pocket expenses like the, co-payments, or co-insurance, or benefits not otherwise covered Non-Emergency care when traveling outside the U.S. Private Duty Nursing Routine eye care (Adult) 5 of 8
37 Your Rights to Continue Coverage: If you lose coverage under the plan, then, depending upon the circumstances, Federal and State laws may provide protections that allow you to keep health coverage. Any such rights may be limited in duration and will require you to pay a premium, which may be significantly higher than the premium you pay while covered under the plan. Other limitations on your rights to continue coverage may also apply. For more information on your rights to continue coverage, contact the plan at the number on the back of your BCBSM ID card. You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at or or the U.S. Department of Health and Human Services at x61565 or Your Grievance and Appeals Rights: If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact Blue Cross and Blue Shield of Michigan by calling the number on the back of your BCBSM ID card. Or, you can contact Michigan Office of Financial and Insurance Regulation at or For group health coverage subject to ERISA, you may also contact Employee Benefits Security Administration at EBSA (3272). Does this Coverage Provide Minimum Essential Coverage? The Affordable Care Act requires most people to have health care coverage that qualifies as minimum essential coverage. This plan or policy does provide minimum essential coverage. Does this Coverage Meet the Minimum Value Standard? The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does meet the minimum value standard for the benefits it provides. (IMPORTANT: Blue Cross Blue Shield of Michigan is assuming that your coverage provides for all Essential Health Benefit (EHB) categories as defined by the State of Michigan. The minimum value of your plan may be affected if your plan does not cover certain EHB categories, such as prescription drugs, or if your plan provides coverage of specific EHB categories, for example prescription drugs, through another carrier.) Language Access Services For assistance in a language below please call the number on the back of your BCBSM ID card. SPANISH (Español): Para ayuda en español, llame al número de servicio al cliente que se encuentra en este aviso ó en el reverso de su tarjeta de identificación. TAGALOG (Tagalog): Para sa tulong sa wikang Tagalog, mangyaring tumawag sa numero ng serbisyo sa mamimili na nakalagay sa likod ng iyong pagkakakilanlan kard o sa paunawang ito. CHINESE ( 中 文 ): 要 获 取 中 文 帮 助, 请 致 电 您 的 身 份 识 别 卡 背 面 或 本 通 知 提 供 的 客 户 服 务 号 码 NAVAJO (Dine): Taa dineji keego shii kaa ahdool wool ninizin goo, beesh behane e naal tsoos bikii sin dahiigii binii deehgo eeh doodago di naaltsoo bikaiigii bichi hoodillnii. To see examples of how this plan might cover costs for a sample medical situation, see the next page. 6 of 8
38 About these Coverage Examples: These examples show how this plan might cover medical care in given situations. Use these examples to see, in general, how much financial protection a sample patient might get if they are covered under different plans. This is not a cost estimator. Don t use these examples to estimate your actual costs under this plan. The actual care you receive will be different from these examples, and the cost of that care will also be different. See the next page for important information about these examples. Having a baby (normal delivery) Amount owed to providers: $7,540 Plan pays $7,120 Patient pays $420 Sample care costs: Hospital charges (mother) $2,700 Routine obstetric care $2,100 Hospital charges (baby) $900 Anesthesia $900 Laboratory tests $500 Prescriptions $200 Radiology $200 Vaccines, other preventive $40 Total $7,540 Patient pays: Deductibles $250 Co-pays $20 Co-insurance $0 Limits or exclusions $150 Total $420 Managing type 2 diabetes (routine maintenance of a well-controlled condition) Amount owed to providers: $5,400 Plan pays $4,220 Patient pays $1,180 Sample care costs: Prescriptions $2,900 Medical Equipment and Supplies $1,300 Office Visits and Procedures $700 Education $300 Laboratory tests $100 Vaccines, other preventive $100 Total $5,400 Patient pays: Deductibles $250 Co-pays $850 Co-insurance $0 Limits or exclusions $80 Total $1,180 Please note: Coverage examples are calculated based on individual coverage and calculations may not include a coinsurance maximum. 7 of 8
39 Questions and answers about the Coverage Examples: What are some of the assumptions behind the Coverage Examples? Costs don t include premiums. Sample care costs are based on national averages supplied by the U.S. Department of Health and Human Services, and aren t specific to a particular geographic area or health plan. The patient s condition was not an excluded or preexisting condition. All services and treatments started and ended in the same coverage period. There are no other medical expenses for any member covered under this plan. Out-of-pocket expenses are based only on treating the condition in the example. The patient received all care from innetwork providers. If the patient had received care from out-of-network providers, costs would have been higher. What does a Coverage Example show? For each treatment situation, the Coverage Example helps you see how s, co-payments, and co-insurance can add up. It also helps you see what expenses might be left up to you to pay because the service or treatment isn t covered or payment is limited. Does the Coverage Example predict my own care needs? No. Treatments shown are just examples. The care you would receive for this condition could be different, based on your doctor s advice, your age, how serious your condition is, and many other factors. Does the Coverage Example predict my future expenses? No. Coverage Examples are not cost estimators. You can t use the examples to estimate costs for an actual condition. They are for comparative purposes only. Your own costs will be different depending on the care you receive, the prices your providers charge, and the reimbursement your health plan allows. Can I use Coverage Examples to compare plans? Yes. When you look at the Summary of Benefits and Coverage for other plans, you ll find the same Coverage Examples. When you compare plans, check the Patient Pays box in each example. The smaller that number, the more coverage the plan provides. Are there other costs I should consider when comparing plans? Yes. An important cost is the premium you pay. Generally, the lower your premium, the more you ll pay in out-of-pocket costs, such as co-payments, s, and co-insurance. You should also consider contributions to accounts such as health savings accounts (HSAs), flexible spending arrangements (FSAs) or health reimbursement accounts (HRAs) that help you pay out-of-pocket expenses. Questions: Call the number on the back of your BCBSM ID card or visit us at If you aren t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at or call the number on the back of your BCBSM ID card to request a copy. 8 of 8
40 DELTA COLLEGE PPO #15 Coverage Period: Beginning on or after 07/01/2015 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual/Family Plan Type: PPO This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at or by calling the number on the back of your BCBSM ID card. Important Questions What is the overall? Are there other s for specific services? Is there an out-of-pocket limit on my expenses? (May include a co-insurance maximum) What is not included in the out-of-pocket limit? Is there an overall annual limit on what the plan pays? Does this plan use a network of providers? Do I need a referral to see a specialist? Are there services this plan doesn t cover? Answers In-Network Out-of-Network $2,500 Individual/ $5,000 Family No. $6,600 Individual/ $13,200 Family $5,000 Individual/ $10,000 Family $10,000 Individual/ $20,000 Family Premiums, balance-billed charges, any pharmacy penalty and health care this plan doesn t cover. No. Yes. For a list of in-network providers, see or call the number on the back of your BCBSM ID card. No. Yes. Why this Matters: You must pay all the costs up to the amount before this plan begins to pay for covered services you use. Check your policy or plan document to see when the starts over (usually, but not always, January 1st). See the chart starting on page 2 for how much you pay for covered services after you meet the. You don t have to meet s for specific services, but see the chart starting on page 2 for other costs for services this plan covers. The out-of-pocket limit is the most you could pay during a coverage period (usually one year) for your share of the cost of covered services. This limit helps you plan for health care expenses. Even though you pay these expenses, they don t count toward the out-of-pocket limit. The chart starting on page 2 describes any limits on what the plan will pay for specific covered services, such as office visits. If you use an in-network doctor or other health care provider, this plan will pay some or all of the costs of covered services. Be aware, your in-network doctor or hospital may use an out-of-network provider for some services. Plans use the term in-network, preferred, or participating for providers in their network. See the chart starting on page 2 for how this plan pays different kinds of providers. You can see the specialist you choose without permission from this plan. Some of the services this plan doesn t cover are listed on page 5. See your policy or plan document for additional information about excluded services. Group Number /0002/0003/0004/0005/0006/0007 Questions: Call the number on the back of your BCBSM ID card or visit us at If you aren t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at or call the number on the back of your BCBSM ID card to request a copy. SBC of 8
41 Co-payments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service. Co-insurance is your share of the costs of a covered service, calculated as a percent of the allowed amount for the service. For example, if the plan s allowed amount for an overnight hospital stay is $1,000, your co-insurance payment of 20% would be $200. This may change if you haven t met your. The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than the allowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay and the allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.) This plan may encourage you to use in-network providers by charging you lower s, co-payments and co-insurance amounts. Common Medical Event If you visit a health care provider s office or clinic If you have a test If you need drugs to treat your illness or condition Some plans may have a separate out of pocket maximum for prescription drug coverage, for more information please contact your plan administrator Services You May Need Primary care visit to treat an injury or illness Specialist visit Other practitioner office visit Your cost if you use a In-Network Provider Out-of-Network Provider Limitations & Exceptions $40 co-pay 40% co-insurance after $40 co-pay 40% co-insurance after $40 co-pay for chiropractic and osteopathic manipulative therapy 40% co-insurance after for chiropractic and osteopathic manipulative therapy Preventive care/ No Charge Not Covered screening/immunization Diagnostic test (x-ray, blood work) Imaging (CT/PET scans, MRIs) Generic or select prescribed over-thecounter drugs Preferred brand-name drugs Nonpreferred brandname drugs $10 co-pay for retail 30-day supply; $20 co-pay for retail or mail order 90-day supply $40 co-pay for retail 30-day supply; $80 co-pay for retail or mail order 90-day supply 40% co-insurance after 40% co-insurance after In-Network co-pay plus an additional 25% of the approved amount In-Network co-pay plus an additional 25% of the approved amount Limited to 24 visits per member per calendar year. Not covered Not Covered For information on women's contraceptive coverage, contact your plan administrator. Mail order drugs are not covered out-of-network. Mail order drugs are not covered out-of-network. 2 of 8
42 Common Medical Event If you have outpatient surgery If you need immediate medical attention If you have a hospital stay If you have mental health, behavioral health, or substance abuse needs If you are pregnant If you need help recovering or have other special health needs Services You May Need Facility fee (e.g., ambulatory surgery center) Physician/surgeon fees Emergency room services Emergency medical transportation Urgent care Facility fee (e.g., hospital room) Physician/surgeon fee Mental/Behavioral health outpatient services Mental/Behavioral health inpatient services Substance use disorder outpatient services Substance use disorder inpatient services Prenatal and postnatal care Delivery and all inpatient services Home health care Rehabilitation services Your cost if you use a In-Network Provider Out-of-Network Provider 40% co-insurance after 40% co-insurance after $100 co-pay $100 co-pay $40 co-pay No Charge 40% co-insurance after 40% co-insurance after 40% co-insurance after 40% co-insurance after 40% co-insurance after 40% co-insurance after 40% co-insurance after 40% co-insurance after Limitations & Exceptions Co-pay waived if admitted or for an accidental injury. Your cost share may be different for services performed in an office setting Physical, Speech and Occupational Therapy is limited to a combined maximum of 60 visits per member, per calendar year. 3 of 8
43 Common Medical Event Services You May Need Your cost if you use a In-Network Provider Out-of-Network Provider Habilitation services Not Covered Not Covered Skilled nursing care Durable medical equipment Limitations & Exceptions Limited to a maximum of 120 days per member per calendar year. Hospice service No Charge No Charge If your child needs Eye exam Not Covered Not Covered dental or eye care Glasses For more information on Not Covered Not Covered pediatric vision or dental, contact your plan administrator Dental check-up Not Covered Not Covered 4 of 8
44 Excluded Services & Other Covered Services: Services Your Plan Does NOT Cover (This isn t a complete list. Check your policy or plan document for other excluded services.) Acupuncture Cosmetic surgery Dental care (Adult) Infertility treatment Long-term care Routine foot care Weight loss programs Other Covered Services (This isn t a complete list. Check your policy or plan document for other covered services and your costs for these services.) Bariatric surgery Chiropractic Care Coverage provided outside the United States. See If you are also covered by an account-type plan such as an integrated health flexible spending arrangement (FSA), health reimbursement arrangement (HRA), and/or a health savings account (HSA), then you may have access to additional funds to help cover certain out-of-pocket expenses like the, co-payments, or co-insurance, or benefits not otherwise covered Non-Emergency care when traveling outside the U.S. Private Duty Nursing Routine eye care (Adult) 5 of 8
45 Your Rights to Continue Coverage: If you lose coverage under the plan, then, depending upon the circumstances, Federal and State laws may provide protections that allow you to keep health coverage. Any such rights may be limited in duration and will require you to pay a premium, which may be significantly higher than the premium you pay while covered under the plan. Other limitations on your rights to continue coverage may also apply. For more information on your rights to continue coverage, contact the plan at the number on the back of your BCBSM ID card. You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at or or the U.S. Department of Health and Human Services at x61565 or Your Grievance and Appeals Rights: If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact Blue Cross and Blue Shield of Michigan by calling the number on the back of your BCBSM ID card. Or, you can contact Michigan Office of Financial and Insurance Regulation at or For group health coverage subject to ERISA, you may also contact Employee Benefits Security Administration at EBSA (3272). Does this Coverage Provide Minimum Essential Coverage? The Affordable Care Act requires most people to have health care coverage that qualifies as minimum essential coverage. This plan or policy does provide minimum essential coverage. Does this Coverage Meet the Minimum Value Standard? The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does meet the minimum value standard for the benefits it provides. (IMPORTANT: Blue Cross Blue Shield of Michigan is assuming that your coverage provides for all Essential Health Benefit (EHB) categories as defined by the State of Michigan. The minimum value of your plan may be affected if your plan does not cover certain EHB categories, such as prescription drugs, or if your plan provides coverage of specific EHB categories, for example prescription drugs, through another carrier.) Language Access Services For assistance in a language below please call the number on the back of your BCBSM ID card. SPANISH (Español): Para ayuda en español, llame al número de servicio al cliente que se encuentra en este aviso ó en el reverso de su tarjeta de identificación. TAGALOG (Tagalog): Para sa tulong sa wikang Tagalog, mangyaring tumawag sa numero ng serbisyo sa mamimili na nakalagay sa likod ng iyong pagkakakilanlan kard o sa paunawang ito. CHINESE ( 中 文 ): 要 获 取 中 文 帮 助, 请 致 电 您 的 身 份 识 别 卡 背 面 或 本 通 知 提 供 的 客 户 服 务 号 码 NAVAJO (Dine): Taa dineji keego shii kaa ahdool wool ninizin goo, beesh behane e naal tsoos bikii sin dahiigii binii deehgo eeh doodago di naaltsoo bikaiigii bichi hoodillnii. To see examples of how this plan might cover costs for a sample medical situation, see the next page. 6 of 8
46 About these Coverage Examples: These examples show how this plan might cover medical care in given situations. Use these examples to see, in general, how much financial protection a sample patient might get if they are covered under different plans. This is not a cost estimator. Don t use these examples to estimate your actual costs under this plan. The actual care you receive will be different from these examples, and the cost of that care will also be different. See the next page for important information about these examples. Having a baby (normal delivery) Amount owed to providers: $7,540 Plan pays $4,340 Patient pays $3,200 Sample care costs: Hospital charges (mother) $2,700 Routine obstetric care $2,100 Hospital charges (baby) $900 Anesthesia $900 Laboratory tests $500 Prescriptions $200 Radiology $200 Vaccines, other preventive $40 Total $7,540 Patient pays: Deductibles $2,500 Co-pays $20 Co-insurance $530 Limits or exclusions $150 Total $3,200 Managing type 2 diabetes (routine maintenance of a well-controlled condition) Amount owed to providers: $5,400 Plan pays $2,500 Patient pays $2,900 Sample care costs: Prescriptions $2,900 Medical Equipment and Supplies $1,300 Office Visits and Procedures $700 Education $300 Laboratory tests $100 Vaccines, other preventive $100 Total $5,400 Patient pays: Deductibles $2,420 Co-pays $400 Co-insurance $0 Limits or exclusions $80 Total $2,900 Please note: Coverage examples are calculated based on individual coverage and calculations may not include a coinsurance maximum. 7 of 8
47 Questions and answers about the Coverage Examples: What are some of the assumptions behind the Coverage Examples? Costs don t include premiums. Sample care costs are based on national averages supplied by the U.S. Department of Health and Human Services, and aren t specific to a particular geographic area or health plan. The patient s condition was not an excluded or preexisting condition. All services and treatments started and ended in the same coverage period. There are no other medical expenses for any member covered under this plan. Out-of-pocket expenses are based only on treating the condition in the example. The patient received all care from innetwork providers. If the patient had received care from out-of-network providers, costs would have been higher. What does a Coverage Example show? For each treatment situation, the Coverage Example helps you see how s, co-payments, and co-insurance can add up. It also helps you see what expenses might be left up to you to pay because the service or treatment isn t covered or payment is limited. Does the Coverage Example predict my own care needs? No. Treatments shown are just examples. The care you would receive for this condition could be different, based on your doctor s advice, your age, how serious your condition is, and many other factors. Does the Coverage Example predict my future expenses? No. Coverage Examples are not cost estimators. You can t use the examples to estimate costs for an actual condition. They are for comparative purposes only. Your own costs will be different depending on the care you receive, the prices your providers charge, and the reimbursement your health plan allows. Can I use Coverage Examples to compare plans? Yes. When you look at the Summary of Benefits and Coverage for other plans, you ll find the same Coverage Examples. When you compare plans, check the Patient Pays box in each example. The smaller that number, the more coverage the plan provides. Are there other costs I should consider when comparing plans? Yes. An important cost is the premium you pay. Generally, the lower your premium, the more you ll pay in out-of-pocket costs, such as co-payments, s, and co-insurance. You should also consider contributions to accounts such as health savings accounts (HSAs), flexible spending arrangements (FSAs) or health reimbursement accounts (HRAs) that help you pay out-of-pocket expenses. Questions: Call the number on the back of your BCBSM ID card or visit us at If you aren t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at or call the number on the back of your BCBSM ID card to request a copy. 8 of 8
PAYROLL CLIENT EMPLOYEE SETUP FORM
 EMPLOYEE INFORMATION EMPLOYEE DEMOGRAPHIC INFORMATION Employee ID EIN/SSN # First Name Middle Initial Last Name TAXING (HOME) ADDRESS: Address PAYROLL CLIENT EMPLOYEE SETUP FORM EMPLOYMENT/PERSONAL INFORMATION
EMPLOYEE INFORMATION EMPLOYEE DEMOGRAPHIC INFORMATION Employee ID EIN/SSN # First Name Middle Initial Last Name TAXING (HOME) ADDRESS: Address PAYROLL CLIENT EMPLOYEE SETUP FORM EMPLOYMENT/PERSONAL INFORMATION
Application for Part-Time Employment LSU Athletics Gameday Event Staff
 Application for Part-Time Employment LSU Athletics Gameday Event Staff Please follow the directions below, take your time and print neatly. Be sure to review all pages for accuracy. Incomplete packets
Application for Part-Time Employment LSU Athletics Gameday Event Staff Please follow the directions below, take your time and print neatly. Be sure to review all pages for accuracy. Incomplete packets
University of Northern Iowa
 University of Northern Iowa Direct Deposit of Payroll Authorization Form Name (Please Print) (Last, First, MI) UNI ID# I hereby authorize the University of Northern Iowa to initiate direct deposit credit
University of Northern Iowa Direct Deposit of Payroll Authorization Form Name (Please Print) (Last, First, MI) UNI ID# I hereby authorize the University of Northern Iowa to initiate direct deposit credit
Student Employee Onboarding Checklist
 Student Employee Onboarding Checklist US Ci zen The final component of the University of Pi sburgh s student hiring process is for you to complete this onboarding checklist along with the required documents.
Student Employee Onboarding Checklist US Ci zen The final component of the University of Pi sburgh s student hiring process is for you to complete this onboarding checklist along with the required documents.
FREQUENTLY ASKED QUESTIONS
 1/09 FREQUENTLY ASKED QUESTIONS 1. Which employees are eligible for an FMLA qualifying leave? An "eligible employee" is a State employee who: a) Has been employed by the State for at least 12 months, and
1/09 FREQUENTLY ASKED QUESTIONS 1. Which employees are eligible for an FMLA qualifying leave? An "eligible employee" is a State employee who: a) Has been employed by the State for at least 12 months, and
FAMILY CARE LEAVE OF ABSENCE REQUEST FORM
 FAMILY CARE LEAVE OF ABSENCE REQUEST FORM Section 1: For completion by the Employee The FMLA permits an employer to require that you submit a timely, complete, and sufficient medical certification to support
FAMILY CARE LEAVE OF ABSENCE REQUEST FORM Section 1: For completion by the Employee The FMLA permits an employer to require that you submit a timely, complete, and sufficient medical certification to support
FMLA: Certification of Health Care Provider for Employee s Serious Health Condition
 FMLA: Certification of Health Care Provider for Employee s Serious Health Condition Route this form to: Supervisor/responsible administrator U Wide Form: UM 1515 Rev: Mar 2009 NOTE: Failure to fully complete
FMLA: Certification of Health Care Provider for Employee s Serious Health Condition Route this form to: Supervisor/responsible administrator U Wide Form: UM 1515 Rev: Mar 2009 NOTE: Failure to fully complete
For additional information: 1-866-4US-WAGE (1-866-487-9243) TTY: 1-877-889-5627 WWW.WAGEHOUR.DOL.GOV
 TTY: 1-877-889-5627 WWW.WAGEHOUR.DOL.GOV") Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, jobprotected leave to eligible employees for the following reasons: For incapacity due to pregnancy, prenatal
Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, jobprotected leave to eligible employees for the following reasons: For incapacity due to pregnancy, prenatal
FAMILY AND MEDICAL LEAVE ACT (FMLA) POLICY
 POLICY") FAMILY AND MEDICAL LEAVE ACT (FMLA) POLICY Purpose To define policy pursuant to the federal Family and Medical Leave Act for employees of Olympus Corporation of the Americas ( OCA ), Olympus America Inc.
FAMILY AND MEDICAL LEAVE ACT (FMLA) POLICY Purpose To define policy pursuant to the federal Family and Medical Leave Act for employees of Olympus Corporation of the Americas ( OCA ), Olympus America Inc.
THE LAW. Equal Employment Opportunity is
 Equal Employment Opportunity is THE LAW Private Employers, State and Local Governments, Educational Institutions, Employment Agencies and Labor Organizations Applicants to and employees of most private
Equal Employment Opportunity is THE LAW Private Employers, State and Local Governments, Educational Institutions, Employment Agencies and Labor Organizations Applicants to and employees of most private
New Hire Booklet. Employee Name. Company Code 0104-0801. 2001 ADP TotalSource Services, Inc.
 New Hire Booklet Employee Name Company Code 2001 ADP TotalSource Services, Inc. 0104-0801 Welcome to ADP TotalSource The Basic Employment Policies included in this Booklet will explain your relationship
New Hire Booklet Employee Name Company Code 2001 ADP TotalSource Services, Inc. 0104-0801 Welcome to ADP TotalSource The Basic Employment Policies included in this Booklet will explain your relationship
EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT
 EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, jobprotected leave to eligible employees
EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, jobprotected leave to eligible employees
Employment Law Disclosures
 Employment Law Disclosures This document summarizes various federal and state employment law notifications that are required to be made to employees and/or applicants for employment. Federal Equal Employment
Employment Law Disclosures This document summarizes various federal and state employment law notifications that are required to be made to employees and/or applicants for employment. Federal Equal Employment
EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT
 EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, job-protected leave to eligible
EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, job-protected leave to eligible
How to Successfully Take Maternity Leave. Certified Employees
 WILSON COUNTY SCHOOLS Dr. Donna Wright Director of Schools 351 Stumpy Lane, Lebanon TN 37090 Tel : (615) 444-3282 Fax : (615) 449-3858 How to Successfully Take Maternity Leave Certified Employees For leave
WILSON COUNTY SCHOOLS Dr. Donna Wright Director of Schools 351 Stumpy Lane, Lebanon TN 37090 Tel : (615) 444-3282 Fax : (615) 449-3858 How to Successfully Take Maternity Leave Certified Employees For leave
Substitute W-4P Tax Withholding Certificate for Pension or Annuity Payments Wis. Stat. 40.08 (1)
") Substitute W-4P Tax Withholding Certificate for Pension or Annuity Payments Wis. Stat. 40.08 (1) Wisconsin Department of Employee Trust Funds 801 W Badger Road PO Box 7931 Madison WI 53707-7931 1-877-533-5020
Substitute W-4P Tax Withholding Certificate for Pension or Annuity Payments Wis. Stat. 40.08 (1) Wisconsin Department of Employee Trust Funds 801 W Badger Road PO Box 7931 Madison WI 53707-7931 1-877-533-5020
University of Massachusetts Amherst PSU/MTA Parental Leave
 University of Massachusetts Amherst PSU/MTA Parental Leave PSA/MTA members who become biological, adoptive or foster parents of a child less than five years of age receive, upon request, up to: 26 weeks
University of Massachusetts Amherst PSU/MTA Parental Leave PSA/MTA members who become biological, adoptive or foster parents of a child less than five years of age receive, upon request, up to: 26 weeks
FAMILY & MEDICAL LEAVE
 FAMILY & MEDICAL LEAVE Employees may be eligible for an unpaid leave of absence under the federal Family Medical Leave Act ("FMLA"), subject to its eligibility requirements and other terms, conditions
FAMILY & MEDICAL LEAVE Employees may be eligible for an unpaid leave of absence under the federal Family Medical Leave Act ("FMLA"), subject to its eligibility requirements and other terms, conditions
WINTHROP UNIVERSITY FAMILY AND MEDICAL LEAVE ACT
 WINTHROP UNIVERSITY FAMILY AND MEDICAL LEAVE ACT THIS DOCUMENT IS NOT A CONTRACT BETWEEN EMPLOYEES AND WINTHROP UNIVERSITY, EITHER EXPRESSED OR IMPLIED. THIS DOCUMENT DOES NOT CREATE ANY CONTRACTUAL RIGHTS
WINTHROP UNIVERSITY FAMILY AND MEDICAL LEAVE ACT THIS DOCUMENT IS NOT A CONTRACT BETWEEN EMPLOYEES AND WINTHROP UNIVERSITY, EITHER EXPRESSED OR IMPLIED. THIS DOCUMENT DOES NOT CREATE ANY CONTRACTUAL RIGHTS
EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT
 EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, jobprotected leave to eligible employees
EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, jobprotected leave to eligible employees
Family and Medical Leave Act/California Family Rights Act
 Family and Medical Leave Act/California Family Rights Act The Family and Medical Leave Act and California Family Rights Act ( FMLA / CFRA ) provide eligible employees the opportunity to take unpaid, job-protected
Family and Medical Leave Act/California Family Rights Act The Family and Medical Leave Act and California Family Rights Act ( FMLA / CFRA ) provide eligible employees the opportunity to take unpaid, job-protected
EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT
 EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, job-protected leave to eligible
EMPLOYEE RIGHTS AND RESPONSIBILITIES UNDER THE FAMILY AND MEDICAL LEAVE ACT Basic Leave Entitlement FMLA requires covered employers to provide up to 12 weeks of unpaid, job-protected leave to eligible
TAX FILING SERVICES AGREEMENT and LIMITED POWER OF ATTORNEY FORM
 Client Tax Filing Name TAX FILING SERVICES AGREEMENT and LIMITED POWER OF ATTORNEY FORM Federal Tax ID This is a Tax Filing Services Agreement with Limited Power of Attorney between PAYMEDIA, LLC. herein
Client Tax Filing Name TAX FILING SERVICES AGREEMENT and LIMITED POWER OF ATTORNEY FORM Federal Tax ID This is a Tax Filing Services Agreement with Limited Power of Attorney between PAYMEDIA, LLC. herein
Notice to Employees Sick, Parental and Family Care (SPF), Military Exigency and Military Caregiver Absences Family & Medical Leave Act AFSCME and PSSU
, Military Exigency and Military Caregiver Absences Family & Medical Leave Act AFSCME and PSSU") Notice to Employees Sick, Parental and Family Care (SPF), Military Exigency and s Family & Medical Leave Act AFSCME and PSSU FMLA Information The absence provisions described below are consistent with
Notice to Employees Sick, Parental and Family Care (SPF), Military Exigency and s Family & Medical Leave Act AFSCME and PSSU FMLA Information The absence provisions described below are consistent with
Notice to AFSCME and PSSU Employees Family and Medical Leave Act
 Notice to AFSCME and PSSU Employees Family and Medical Leave Act Sick, Parental, and Family Care (SPF), Military Exigency and Military Caregiver FMLA Information The absence provisions described below
Notice to AFSCME and PSSU Employees Family and Medical Leave Act Sick, Parental, and Family Care (SPF), Military Exigency and Military Caregiver FMLA Information The absence provisions described below
Important Information About. Tax Withholding and Railroad Retirement Payments
 Important Information About Tax Withholding and Railroad Retirement Payments For use with Form RRB W-4P U.S. Railroad Retirement Board 844 North Rush Street Chicago, IL 60611-2092 www.rrb.gov TXB-25 (01-15)
Important Information About Tax Withholding and Railroad Retirement Payments For use with Form RRB W-4P U.S. Railroad Retirement Board 844 North Rush Street Chicago, IL 60611-2092 www.rrb.gov TXB-25 (01-15)
UNIVERSITY OF HOUSTON SYSTEM ADMINISTRATIVE MEMORANDUM. SECTION: Human Resources NUMBER: 02.D.06
 UNIVERSITY OF HOUSTON SYSTEM ADMINISTRATIVE MEMORANDUM SECTION: Human Resources NUMBER: 02.D.06 AREA: SUBJECT: Leave Entitlement Family and Medical Leave 1. PURPOSE The University of Houston System provides
UNIVERSITY OF HOUSTON SYSTEM ADMINISTRATIVE MEMORANDUM SECTION: Human Resources NUMBER: 02.D.06 AREA: SUBJECT: Leave Entitlement Family and Medical Leave 1. PURPOSE The University of Houston System provides
Conditional Family Leave Notification
 Conditional Family Leave Notification Department of Administration It is State of Alaska policy to invoke family leave for all qualifying conditions. The supervisor or designee is responsible for initially
Conditional Family Leave Notification Department of Administration It is State of Alaska policy to invoke family leave for all qualifying conditions. The supervisor or designee is responsible for initially
OKLAHOMA CITY UNIVERSITY POLICY THE FAMILY AND MEDICAL LEAVE ACT (FMLA)
") OKLAHOMA CITY UNIVERSITY POLICY THE FAMILY AND MEDICAL LEAVE ACT (FMLA) Oklahoma City University provides leaves of absence under the Family and Medical Leave Act of 1993, as amended, to eligible regular
OKLAHOMA CITY UNIVERSITY POLICY THE FAMILY AND MEDICAL LEAVE ACT (FMLA) Oklahoma City University provides leaves of absence under the Family and Medical Leave Act of 1993, as amended, to eligible regular
Understanding Your Pay and Form W-2
 Understanding Your Pay and Form W-2 Table of Contents 3 Welcome to Understanding Your Pay 3 How is My Pay Calculated? 3 Gross Wages 4 Pre-Tax Deductions 4 Income Taxes 5 Employment Taxes 5 Post-Tax Deductions
Understanding Your Pay and Form W-2 Table of Contents 3 Welcome to Understanding Your Pay 3 How is My Pay Calculated? 3 Gross Wages 4 Pre-Tax Deductions 4 Income Taxes 5 Employment Taxes 5 Post-Tax Deductions
FREQUENTLY ASKED QUESTIONS CONCERNING FMLA FOR EXECUTIVE BRANCH EMPLOYEES
 FREQUENTLY ASKED QUESTIONS CONCERNING FMLA FOR EXECUTIVE BRANCH EMPLOYEES 1. What is the FMLA?... 2 2. Am I entitled to FMLA leave?... 2 3. When can FMLA leave be used?... 3 4. Who is considered a "family
FREQUENTLY ASKED QUESTIONS CONCERNING FMLA FOR EXECUTIVE BRANCH EMPLOYEES 1. What is the FMLA?... 2 2. Am I entitled to FMLA leave?... 2 3. When can FMLA leave be used?... 3 4. Who is considered a "family
Family and Medical Leave
 Family and Medical Leave Application: All positions covered under the Virginia Personnel Act to include full-time and part-time classified, restricted employees, and eligible wage employees. Background
Family and Medical Leave Application: All positions covered under the Virginia Personnel Act to include full-time and part-time classified, restricted employees, and eligible wage employees. Background
U. S. Department of Labor Employment Standards Administration Wage and Hour Division
 FMLA/CFRA MED-CERT Certification of Health Care Provider APPENDIX C U. S. Department of Labor Employment Standards Administration Wage and Hour Division (Family and Medical Leave Act of 1993) 1. Employee
FMLA/CFRA MED-CERT Certification of Health Care Provider APPENDIX C U. S. Department of Labor Employment Standards Administration Wage and Hour Division (Family and Medical Leave Act of 1993) 1. Employee
3. Duration of Leave A. Employees may take a maximum of twelve (12) workweeks of Family and Medical Leave
 workweeks of Family and Medical Leave") , Fair Employment and Housing Act (FEHA), Temporary Family Disability Insurance and Labor Code Section 233- Sick Leave to Attend Family 1. Policy Statement In accordance with employee MOUs and the District
, Fair Employment and Housing Act (FEHA), Temporary Family Disability Insurance and Labor Code Section 233- Sick Leave to Attend Family 1. Policy Statement In accordance with employee MOUs and the District
If you have any questions, concerns, or disputes with this policy, you must contact [insert name and contact info for appropriate person] in writing.
![If you have any questions, concerns, or disputes with this policy, you must contact [insert name and contact info for appropriate person] in writing.](/thumbs/37/17748318.jpg "If you have any questions, concerns, or disputes with this policy, you must contact [insert name and contact info for appropriate person] in writing.") EMPLOYMENT CONTRACT BETWEEN THE EMPLOYEE AND THE RIGHTS OR ENTITLEMENTS. THE AGENCY RESERVES THE RIGHT TO REVISE THE CONTENT OF THIS DOCUMENT, IN WHOLE OR IN ORAL, WHICH ARE CONTRARY TO OR INCONSISTENT
EMPLOYMENT CONTRACT BETWEEN THE EMPLOYEE AND THE RIGHTS OR ENTITLEMENTS. THE AGENCY RESERVES THE RIGHT TO REVISE THE CONTENT OF THIS DOCUMENT, IN WHOLE OR IN ORAL, WHICH ARE CONTRARY TO OR INCONSISTENT
FAMILY AND MEDICAL LEAVE (FMLA) POLICY AND PROCEDURE
 POLICY AND PROCEDURE") FAMILY AND MEDICAL LEAVE (FMLA) POLICY AND PROCEDURE PURPOSE: The Family and Medical Leave Act of 1993 (FMLA) allows an eligible employee up to 12 weeks of leave in a 12-month period for a qualifying reason(s).
FAMILY AND MEDICAL LEAVE (FMLA) POLICY AND PROCEDURE PURPOSE: The Family and Medical Leave Act of 1993 (FMLA) allows an eligible employee up to 12 weeks of leave in a 12-month period for a qualifying reason(s).
P E N N S Y L V A N I A
 P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
P E N N S Y L V A N I A Application for Payment of Medicare Premiums, Coinsurance and Deductibles If you have a disability and need this form in large print or another format, please call our helpline
Please read this statement before proceeding
 Family and Medical Leave FMLA Military Caregiver Leave A policy for administering the Federal Military Caregiver Leave for eligible employees at Portland State University This Policy Covers: The Federal
Family and Medical Leave FMLA Military Caregiver Leave A policy for administering the Federal Military Caregiver Leave for eligible employees at Portland State University This Policy Covers: The Federal
BUSINESS SERVICES FAMILY AND MEDICAL LEAVE CHAPTER 2 Board of Trustees Approval: 8/8/12 POLICY 4.13 Page 1 of 1
 CHAPTER 2 Board of Trustees Approval: 8/8/12 POLICY 4.13 Page 1 of 1 I. POLICY Salt Lake Community College will provide employee leave in accordance with the Family and Medical Leave Act of 1993. Provisions
CHAPTER 2 Board of Trustees Approval: 8/8/12 POLICY 4.13 Page 1 of 1 I. POLICY Salt Lake Community College will provide employee leave in accordance with the Family and Medical Leave Act of 1993. Provisions
PLEASE COMPLETE AND RETURN
 PLEASE COMPLETE AND RETURN Voluntary Care Network Application Name of Client (Last) (First) (Middle Initial) Street Address Telephone (home) City State Zip Telephone (alternate) Date of Birth US Citizen
PLEASE COMPLETE AND RETURN Voluntary Care Network Application Name of Client (Last) (First) (Middle Initial) Street Address Telephone (home) City State Zip Telephone (alternate) Date of Birth US Citizen
FAMILY AND MEDICAL LEAVE ACT OF 1993
 FAMILY AND MEDICAL LEAVE ACT OF 1993 Revised March 8, 2016 Department of HUMAN RESOURCES Division of Administrative Services HUMAN RESOURCES North End Center 300 Turner St. NW Suite 2300 (0318) Blacksburg,
FAMILY AND MEDICAL LEAVE ACT OF 1993 Revised March 8, 2016 Department of HUMAN RESOURCES Division of Administrative Services HUMAN RESOURCES North End Center 300 Turner St. NW Suite 2300 (0318) Blacksburg,
Policies and Procedures SECTION:
 Family and Medical Leave PAGE 1 OF 6 PURPOSE The Family and Medical Leave Act of 1993 (FMLA) requires employers with 50 or more employees to allow eligible employees to take up to 12 workweeks of unpaid,
Family and Medical Leave PAGE 1 OF 6 PURPOSE The Family and Medical Leave Act of 1993 (FMLA) requires employers with 50 or more employees to allow eligible employees to take up to 12 workweeks of unpaid,
INSTRUCTIONS FOR EMPLOYMENT APPLICATIONS
 INSTRUCTIONS FOR EMPLOYMENT APPLICATIONS In order to comply with Federal and State Government requirements, a complete file on all employees is required. The employee file must consist of a completed Employment
INSTRUCTIONS FOR EMPLOYMENT APPLICATIONS In order to comply with Federal and State Government requirements, a complete file on all employees is required. The employee file must consist of a completed Employment
Employee Name: Employee # Department (if applicable): Position Description:
: Position Description:") ADMIN: Rec d Dt Via Processed by Date Add/change done E-Verify done File Cabinet Employee Action Form ***See New Employee Checklist Below Employer Name: Employer Location (if applicable): Action (mark
ADMIN: Rec d Dt Via Processed by Date Add/change done E-Verify done File Cabinet Employee Action Form ***See New Employee Checklist Below Employer Name: Employer Location (if applicable): Action (mark
a) The employee s eligibility is determined from the date leave begins. b) Military time is credited as if the employee would have been working.
 The employee s eligibility is determined from the date leave begins. b) Military time is credited as if the employee would have been working.") I. Family Medical Leave Act (FMLA) A. Covered Employees 1. All employees, including seasonal, who have been employed for at least 52 weeks with the City and who have worked at least 1,250 hours in the
I. Family Medical Leave Act (FMLA) A. Covered Employees 1. All employees, including seasonal, who have been employed for at least 52 weeks with the City and who have worked at least 1,250 hours in the
- - If this claim is awarded, do you want a password to use SSA's Internet/phone service? Yes
 SOCIAL SECURITY ADMINISTRATION APPLICATION FOR RETIREMENT INSURANCE BENEFITS TEL TOE 120/145/155 Form Approved OMB. 0960-0618 (Do not write in this space) I apply for all insurance benefits for which I
SOCIAL SECURITY ADMINISTRATION APPLICATION FOR RETIREMENT INSURANCE BENEFITS TEL TOE 120/145/155 Form Approved OMB. 0960-0618 (Do not write in this space) I apply for all insurance benefits for which I
MEMBER S NAME (LAST, FIRST, M.I.) MEMBER ID OR SSN PHONE NUMBER ( ) PHYSICAL ADDRESS (CANNOT BE A PO BOX) COUNTY OF RESIDENCE EMAIL ADDRESS
 MEMBER ID OR SSN PHONE NUMBER ( ) PHYSICAL ADDRESS (CANNOT BE A PO BOX) COUNTY OF RESIDENCE EMAIL ADDRESS") Department of Technology, Management & Budget Office of Retirement Services www.michigan.gov/ors (800) 381-5111 P.O. Box 30171 Lansing, MI 48909-7671 Insurance Enrollment/Change Request MEMBER S NAME (LAST,
Department of Technology, Management & Budget Office of Retirement Services www.michigan.gov/ors (800) 381-5111 P.O. Box 30171 Lansing, MI 48909-7671 Insurance Enrollment/Change Request MEMBER S NAME (LAST,
APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS
 APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS 1. Please read the enclosed brochure for important information. 2. You may use this application to apply for Special Care for adults
APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS 1. Please read the enclosed brochure for important information. 2. You may use this application to apply for Special Care for adults
Family and Medical Leave Act 4510.6
 Human Resources Leaves of Absence Family and Medical Leave Act 4510.6 I. Entitlement to Unpaid Leave under the FMLA. A. Grounds for Family/Medical Leave. An eligible employee shall be entitled to a total
Human Resources Leaves of Absence Family and Medical Leave Act 4510.6 I. Entitlement to Unpaid Leave under the FMLA. A. Grounds for Family/Medical Leave. An eligible employee shall be entitled to a total
Employees may also be eligible to take up to 26 weeks of leave to care for a covered servicemember during a single 12-month period.
 State of Ohio Family and Medical Leave (FMLA) Policy BASIC LEAVE ENTITLEMENT The Family and Medical Leave Act (FMLA) allows an eligible state employee to take up to twelve workweeks of leave per rolling
State of Ohio Family and Medical Leave (FMLA) Policy BASIC LEAVE ENTITLEMENT The Family and Medical Leave Act (FMLA) allows an eligible state employee to take up to twelve workweeks of leave per rolling
Employee Enrollment Package WELCO ONE, LLC. dba Worksite Employee Leasing
 Employee Enrollment Package WELCO ONE, LLC. dba Worksite Employee Leasing An Equal Opportunity Employer We adhere to a policy of making employment decisions without regard to race, color, age, sex, religion,
Employee Enrollment Package WELCO ONE, LLC. dba Worksite Employee Leasing An Equal Opportunity Employer We adhere to a policy of making employment decisions without regard to race, color, age, sex, religion,
1.1 Work Services Corporation recognizes certain designated days throughout the year as paid holidays.
 Policy #300 Time, Attendance and Leaves of Absence Purpose Work Services Corporation provides various types of leave for employees covered by a collective bargaining agreement as well as those not covered
Policy #300 Time, Attendance and Leaves of Absence Purpose Work Services Corporation provides various types of leave for employees covered by a collective bargaining agreement as well as those not covered
HUMAN RESOURCES MANAGEMENT POLICY FAMILY AND MEDICAL LEAVE. Policy 30
 HUMAN RESOURCES MANAGEMENT POLICY FAMILY AND MEDICAL LEAVE Policy 30 NOTE: THE LANGUAGE USED IN THIS DOCUMENT DOES NOT CREATE AN EMPLOYMENT CONTRACT BETWEEN THE EMPLOYEE AND THE MEDICAL UNIVERSITY OF SOUTH
HUMAN RESOURCES MANAGEMENT POLICY FAMILY AND MEDICAL LEAVE Policy 30 NOTE: THE LANGUAGE USED IN THIS DOCUMENT DOES NOT CREATE AN EMPLOYMENT CONTRACT BETWEEN THE EMPLOYEE AND THE MEDICAL UNIVERSITY OF SOUTH
Dear State of Florida Retiree:
 P.O. Box 6830 Tallahassee, FL 32314 Tel: 866-663-4735 Fax: 800-422-3128 TTY: 866-221-0268 Dear State of Florida Retiree: Congratulations on your retirement! As a new retiree, you need to be aware of State
P.O. Box 6830 Tallahassee, FL 32314 Tel: 866-663-4735 Fax: 800-422-3128 TTY: 866-221-0268 Dear State of Florida Retiree: Congratulations on your retirement! As a new retiree, you need to be aware of State
Application & Renewal Form
 Section A: I want health insurance for: (Check ( ) the category or categories that match your situation.) Myself, my spouse (or other parent of my children) and our children under age 19 who live with
Section A: I want health insurance for: (Check ( ) the category or categories that match your situation.) Myself, my spouse (or other parent of my children) and our children under age 19 who live with
Your Health Care Benefit Program
 Your Health Care Benefit Program HMO ILLINOIS A Blue Cross HMO a product of Blue Cross and Blue Shield of Illinois HMO GROUP CERTIFICATE RIDER This Certificate, to which this Rider is attached to and becomes
Your Health Care Benefit Program HMO ILLINOIS A Blue Cross HMO a product of Blue Cross and Blue Shield of Illinois HMO GROUP CERTIFICATE RIDER This Certificate, to which this Rider is attached to and becomes
Q. Can I use my Short Term Disability (STD) policy concurrent with banked paid time during a FMLA leave?
 policy concurrent with banked paid time during a FMLA leave?") Changes to the FMLA Administration Process As of January 1, 2016, Milwaukee County is using a new vendor, FMLASource, to administer FMLA leaves for employees. FMLASource offers new resources and a user
Changes to the FMLA Administration Process As of January 1, 2016, Milwaukee County is using a new vendor, FMLASource, to administer FMLA leaves for employees. FMLASource offers new resources and a user
Dear Employee, 20-1923 (01-09)
") Dear Employee, 20-1923 (01-09) You may be eligible for leave under the Family and Medical Leave Act (FMLA) as described in the attachment, "Employee Rights and Responsibilities Under the Family and Medical
Dear Employee, 20-1923 (01-09) You may be eligible for leave under the Family and Medical Leave Act (FMLA) as described in the attachment, "Employee Rights and Responsibilities Under the Family and Medical
FAMILY MEDICAL LEAVE ACT FAQS Updated November 2013
 FAMILY MEDICAL LEAVE ACT FAQS Updated November 2013 Protections Q: What protections does the FMLA provide? A: Up to 12 weeks job protection in a 12 month period and maintains insurance. Q: Do I get to
FAMILY MEDICAL LEAVE ACT FAQS Updated November 2013 Protections Q: What protections does the FMLA provide? A: Up to 12 weeks job protection in a 12 month period and maintains insurance. Q: Do I get to
Family and Medical Leave Policy (FMLA) Updated May 2015
 Updated May 2015") Family and Medical Leave Policy (FMLA) Updated May 2015 Babson College complies with the Family and Medical Leave Act of 1993 (FMLA), as amended by the National Defense Authorization Act (NDAA) of 2008
Family and Medical Leave Policy (FMLA) Updated May 2015 Babson College complies with the Family and Medical Leave Act of 1993 (FMLA), as amended by the National Defense Authorization Act (NDAA) of 2008
Frequently Asked Questions and Answers About the Revisions to the Family and Medical Leave Act
 Frequently Asked Questions and Answers About the Revisions to the Family and Medical Leave Act The following are answers to commonly asked questions about the new Family and Medical Leave Act (FMLA) regulations.
Frequently Asked Questions and Answers About the Revisions to the Family and Medical Leave Act The following are answers to commonly asked questions about the new Family and Medical Leave Act (FMLA) regulations.
Family Medical Leave Act (FMLA) Employee Packet. FMLA Introduction and Qualifications. Employee Request Form. Medical Certification Form
 Employee Packet. FMLA Introduction and Qualifications. Employee Request Form. Medical Certification Form") Family Medical Leave Act (FMLA) Employee Packet FMLA Introduction and Qualifications Employee Request Form Medical Certification Form Employee Rights and Responsibilities Family Medical Leave Act (FMLA)
Family Medical Leave Act (FMLA) Employee Packet FMLA Introduction and Qualifications Employee Request Form Medical Certification Form Employee Rights and Responsibilities Family Medical Leave Act (FMLA)
Military Family Leave Provisions of the FMLA (Family and Medical Leave Act) Frequently Asked Questions and Answers
 Frequently Asked Questions and Answers") Military Family Leave Provisions of the FMLA (Family and Medical Leave Act) Frequently Asked Questions and Answers The following are answers to common questions about the military family leave provisions
Military Family Leave Provisions of the FMLA (Family and Medical Leave Act) Frequently Asked Questions and Answers The following are answers to common questions about the military family leave provisions
Frequently Asked Questions Family and Medical Leave Act (FMLA)
") Frequently Asked Questions Family and Medical Leave Act (FMLA) SECTION 1: THE BASICS OF FMLA 1. What is the FMLA? 2. Is there a similar state law in Iowa? 3. What sorts of situations are covered by the
Frequently Asked Questions Family and Medical Leave Act (FMLA) SECTION 1: THE BASICS OF FMLA 1. What is the FMLA? 2. Is there a similar state law in Iowa? 3. What sorts of situations are covered by the
SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee Email:
 SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee Email: Local Tax (IF APPLICABLE): SSN: City or County Township or Borough School District PA EMST:
SPORT CLIPS PAYROLL INFORMATION FORM CLIENT NAME: TO BE COMPLETED BY EMPLOYEE: Employee Name: Employee Email: Local Tax (IF APPLICABLE): SSN: City or County Township or Borough School District PA EMST:
The Board provides family and medical leave for eligible staff members under the following circumstances:
 3430.01 - FAMILY & MEDICAL LEAVE OF ABSENCE ("FMLA") Introduction In accordance with Federal and State law, the Board of Education will provide family and medical leave to professional staff. The Board's
3430.01 - FAMILY & MEDICAL LEAVE OF ABSENCE ("FMLA") Introduction In accordance with Federal and State law, the Board of Education will provide family and medical leave to professional staff. The Board's
UNDERSTANDING FAMILY AND MEDICAL LEAVE (A Primer for Connecticut State Employees) Revised July 2013
 Revised July 2013") UNDERSTANDING FAMILY AND MEDICAL LEAVE (A Primer for Connecticut State Employees) Revised July 2013 The Department of Administrative Services has prepared this brochure to help State of Connecticut employees
UNDERSTANDING FAMILY AND MEDICAL LEAVE (A Primer for Connecticut State Employees) Revised July 2013 The Department of Administrative Services has prepared this brochure to help State of Connecticut employees
New Hire Submission and Return Receipt PLEASE SUBMIT FORMS TO: [email protected] OR FAX 1-866-611-9598
 1933 E EDGEWOOD DR SUITE 102 LAKELAND, FL 33803 1-877-518-2881 WWW.ADVANCEDPEO.COM New Hire Submission and Return Receipt PLEASE SUBMIT FORMS TO: [email protected] OR FAX 1-866-611-9598 Notice to
1933 E EDGEWOOD DR SUITE 102 LAKELAND, FL 33803 1-877-518-2881 WWW.ADVANCEDPEO.COM New Hire Submission and Return Receipt PLEASE SUBMIT FORMS TO: [email protected] OR FAX 1-866-611-9598 Notice to
Purposes for Which the Plan May Use or Disclose PHI Without Your Authorization
 BOWDOIN COLLEGE HEALTH PLAN BOWDOIN COLLEGE DENTAL PLAN BOWDOIN COLLEGE VISION PLAN BOWDOIN COLLEGE HEALTH CARE REIMBURSEMENT PLAN NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION
BOWDOIN COLLEGE HEALTH PLAN BOWDOIN COLLEGE DENTAL PLAN BOWDOIN COLLEGE VISION PLAN BOWDOIN COLLEGE HEALTH CARE REIMBURSEMENT PLAN NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION
New Hire Packet. Human Resource Services Sam Ingram Building, Second Floor 2269 Middle Tennessee Blvd. Murfreesboro, TN 37132
 New Hire Packet A completed New Hire Packet and Form I-9 verification is a requirement of employment at Middle Tennessee State University. Please bring the completed signed, packet in person to Human Resource
New Hire Packet A completed New Hire Packet and Form I-9 verification is a requirement of employment at Middle Tennessee State University. Please bring the completed signed, packet in person to Human Resource
PROFESSIONAL-TECHNICAL EMPLOYEE BENEFITS SUMMARY Updated June 2015
 PROFESSIONAL-TECHNICAL EMPLOYEE BENEFITS SUMMARY Updated Pro-Tech employees receive a comprehensive benefits package consistent with the terms of their Collective Bargaining Agreement. The following summarizes
PROFESSIONAL-TECHNICAL EMPLOYEE BENEFITS SUMMARY Updated Pro-Tech employees receive a comprehensive benefits package consistent with the terms of their Collective Bargaining Agreement. The following summarizes
THE FEDERAL FAMILY & MEDICAL LEAVE ACT OF 1993 (AS REVISED)
") ENGLISH If you have any questions about this information, please contact us at the Office of Human Resources at (608) 265-2257 to communicate in English. If you would like to request translation or interpretation
ENGLISH If you have any questions about this information, please contact us at the Office of Human Resources at (608) 265-2257 to communicate in English. If you would like to request translation or interpretation
What is your racial origin? (check all that apply) White Black or African Descent
 White Black or African Descent") W-1QMB (Rev. 4/10) State of Connecticut Department of Social Services Medicare Savings Programs Application/Redetermination (QMB, SLMB, ALMB) Do you need a reasonable accommodation or special help to complete
W-1QMB (Rev. 4/10) State of Connecticut Department of Social Services Medicare Savings Programs Application/Redetermination (QMB, SLMB, ALMB) Do you need a reasonable accommodation or special help to complete
APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS
 Capital Advantage Insurance Company Commonwealth of Pennsylvania Edward G. Rendell, Governor APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS Application Information The information
Capital Advantage Insurance Company Commonwealth of Pennsylvania Edward G. Rendell, Governor APPLICATION FOR HEALTH CARE COVERAGE FOR UNINSURED CHILDREN AND ADULTS Application Information The information
HIPAA NOTICE OF PRIVACY PRACTICES
 HIPAA NOTICE OF PRIVACY PRACTICES Human Resources Department 16000 N. Civic Center Plaza Surprise, AZ 85374 Ph: 623-222-3532 // Fax: 623-222-3501 TTY: 623-222-1002 Purpose of This Notice This Notice describes
HIPAA NOTICE OF PRIVACY PRACTICES Human Resources Department 16000 N. Civic Center Plaza Surprise, AZ 85374 Ph: 623-222-3532 // Fax: 623-222-3501 TTY: 623-222-1002 Purpose of This Notice This Notice describes
Leave from Work to Care for A Family Member
 Leave from Work to Care for A Family Member YOUR LEGAL RIGHTS 1. What rights do family/medical leave laws provide? Federal and state law provide certain employees with the right to take an unpaid leave
Leave from Work to Care for A Family Member YOUR LEGAL RIGHTS 1. What rights do family/medical leave laws provide? Federal and state law provide certain employees with the right to take an unpaid leave
FMLA Eligibility Requirements
 FMLA Eligibility Requirements ELIGIBLE EMPLOYEES An employee who has been employed by the company for 12 months / 52 weeks as of the date the leave commences. During the preceding 12 months / 52 weeks
FMLA Eligibility Requirements ELIGIBLE EMPLOYEES An employee who has been employed by the company for 12 months / 52 weeks as of the date the leave commences. During the preceding 12 months / 52 weeks
RENTAL APPLICATION Caldwell Housing Authority 22730 Farmway Road Caldwell, Idaho 83607 (208) 459-2232
 459-2232") SECTION 1: APPLICANT INFORMATION RENTAL APPLICATION Accessible unit needed: Yes No (mm/dd/yyyy): Applicant Name (first, middle initial, last): Applicant (SSN): Sex: Male Female of Birth (mm/dd/yyyy): Age:
SECTION 1: APPLICANT INFORMATION RENTAL APPLICATION Accessible unit needed: Yes No (mm/dd/yyyy): Applicant Name (first, middle initial, last): Applicant (SSN): Sex: Male Female of Birth (mm/dd/yyyy): Age:
CITY OF NORWALK FAMILY AND MEDICAL LEAVE ACT POLICY
 CITY OF NORWALK FAMILY AND MEDICAL LEAVE ACT POLICY OVERVIEW The is a "covered" employer under the Federal Family and Medical Leave Act (FMLA or Act) and is subject to all rules and regulations under the
CITY OF NORWALK FAMILY AND MEDICAL LEAVE ACT POLICY OVERVIEW The is a "covered" employer under the Federal Family and Medical Leave Act (FMLA or Act) and is subject to all rules and regulations under the
Department of Employee Trust Funds Health Insurance Application/Change Form
 Department of Employee Trust Funds Health Insurance Application/Change Form 801 W. Badger Road PO Box 7931 Madison, WI 53707-7931 1-877-533-5020 (toll-free) Fax: 608-267-4549 etf.wi.gov Please complete
Department of Employee Trust Funds Health Insurance Application/Change Form 801 W. Badger Road PO Box 7931 Madison, WI 53707-7931 1-877-533-5020 (toll-free) Fax: 608-267-4549 etf.wi.gov Please complete
Disability Plan Claim Kit. Introduction
 Disability Plan Claim Kit Nonunion Employees and Jeppesen Sanderson, Inc., Employees Introduction If an illness or injury prevents you from working, this claim kit provides the materials and information
Disability Plan Claim Kit Nonunion Employees and Jeppesen Sanderson, Inc., Employees Introduction If an illness or injury prevents you from working, this claim kit provides the materials and information
Health Benefits Plans (Medical, Dental, and Vision) Summary Plan Description General Information Section
 Summary Plan Description General Information Section") Health Benefits Plans (Medical, Dental, and Vision) Summary Plan Description General Information Section (Effective: January 1, 2007) The Health Plan Summary Plan Description (SPD) includes three major
Health Benefits Plans (Medical, Dental, and Vision) Summary Plan Description General Information Section (Effective: January 1, 2007) The Health Plan Summary Plan Description (SPD) includes three major
Companion Life Insurance Company. Administrative Guide
 Companion Life Insurance Company Administrative Guide Contents Section.Title About Your Companion Life Administrative Guide I. Online Services II. New Enrollments Who is Eligible for insurance? Processing
Companion Life Insurance Company Administrative Guide Contents Section.Title About Your Companion Life Administrative Guide I. Online Services II. New Enrollments Who is Eligible for insurance? Processing
ATTENTION: NEW NC-4 WITHHOLDING FORMS ENCLOSED
 North Carolina Department of Revenue ATTENTION: NEW NC-4 WITHHOLDING FORMS ENCLOSED IMMEDIATE ACTION REQUIRED North Carolina Department of Revenue TO: IMPORTANT NOTICE: NEW NC-4 REQUIRED FOR PAYMENTS BEGINNING
North Carolina Department of Revenue ATTENTION: NEW NC-4 WITHHOLDING FORMS ENCLOSED IMMEDIATE ACTION REQUIRED North Carolina Department of Revenue TO: IMPORTANT NOTICE: NEW NC-4 REQUIRED FOR PAYMENTS BEGINNING
Brandeis University Office of Human Resources Benefits Section MS 118 781-736-4468
 Brandeis University Office of Human Resources Benefits Section MS 118 781-736-4468 Family and Medical Leave Policy for Faculty Brandeis University has adopted the following leave policy for faculty members
Brandeis University Office of Human Resources Benefits Section MS 118 781-736-4468 Family and Medical Leave Policy for Faculty Brandeis University has adopted the following leave policy for faculty members
FIRST NAME, MIDDLE INITIAL, LAST NAME
 SOCIAL SECURITY ADMINISTRATION TEL TOE 120/145 APPLICATION FOR DISABILITY INSURANCE BENEFITS Form Approved OMB. 0960-0060 (Do not write in this space) I apply for a period of disability and/or all insurance
SOCIAL SECURITY ADMINISTRATION TEL TOE 120/145 APPLICATION FOR DISABILITY INSURANCE BENEFITS Form Approved OMB. 0960-0060 (Do not write in this space) I apply for a period of disability and/or all insurance
2.3.2. Placement of a child with the employee for adoption or foster care,
 1. Purpose: The purpose of this policy is to outline an integrated approach for the efficient and effective management of sick leave in accordance with federal and state leave mandates, employee interests,
1. Purpose: The purpose of this policy is to outline an integrated approach for the efficient and effective management of sick leave in accordance with federal and state leave mandates, employee interests,
DRAKE UNIVERSITY SECTION 125 PRE-TAX SALARY REDUCTION PREMIUM PAYMENT PLAN
 SUMMARY PLAN DESCRIPTION under the DRAKE UNIVERSITY SECTION 125 PRE-TAX SALARY REDUCTION PREMIUM PAYMENT PLAN Dated August 2012 TABLE OF CONTENTS Q-1. What is the purpose of the Plan?.... Page 1 Q-2. What
SUMMARY PLAN DESCRIPTION under the DRAKE UNIVERSITY SECTION 125 PRE-TAX SALARY REDUCTION PREMIUM PAYMENT PLAN Dated August 2012 TABLE OF CONTENTS Q-1. What is the purpose of the Plan?.... Page 1 Q-2. What
HIPAA POLICIES & PROCEDURES AND ADMINISTRATIVE FORMS TABLE OF CONTENTS
 HIPAA POLICIES & PROCEDURES AND ADMINISTRATIVE FORMS TABLE OF CONTENTS 1. HIPAA Privacy Policies & Procedures Overview (Policy & Procedure) 2. HIPAA Privacy Officer (Policy & Procedure) 3. Notice of Privacy
HIPAA POLICIES & PROCEDURES AND ADMINISTRATIVE FORMS TABLE OF CONTENTS 1. HIPAA Privacy Policies & Procedures Overview (Policy & Procedure) 2. HIPAA Privacy Officer (Policy & Procedure) 3. Notice of Privacy
Section A Victim/Applicant Information (A separate application must be completed for each victim.)
") Application For Crime Victim Compensation Claim No. Arkansas Crime Victims Reparations Board 323 Center Street, Suite 200 Little Rock, Arkansas 72201 Office of the (501) 682-1020 or 1-800-448-3014 This
Application For Crime Victim Compensation Claim No. Arkansas Crime Victims Reparations Board 323 Center Street, Suite 200 Little Rock, Arkansas 72201 Office of the (501) 682-1020 or 1-800-448-3014 This
COUNTY OF KERN. HEALTH BENEFITS ELIGIBILITY POLICY for participants without Active Employee Medical Coverage. Rev 6/13
 COUNTY OF KERN HEALTH BENEFITS ELIGIBILITY POLICY for participants without Active Employee Medical Coverage Rev 6/13 Date: June 2013 To: From: Kern County Health Benefits Plan Participants Kern County
COUNTY OF KERN HEALTH BENEFITS ELIGIBILITY POLICY for participants without Active Employee Medical Coverage Rev 6/13 Date: June 2013 To: From: Kern County Health Benefits Plan Participants Kern County