NEURO NICU Concept. 1st unit in the country opened in the UCSF NICU, Summer of nd unit in the country: PCH NICU, Summer of 2009.
|
|
|
- Norma Pierce
- 8 years ago
- Views:
Transcription
1 Ice, Ice Baby: Treatment of Infants with Hypoxic Ischemic Encephalopathy Using Hypothermic Therapy Within a Successful Neuro NICU Program Cristina Carballo, M.D. Neuro NICU Medical Director Kim Allred, NNP-BC Neuro NICU Program Coordinator Christine Bure RN, Clinical Supervisor, NICU Phoenix Children s Hospital

2 NEURO NICU Concept 1st unit in the country opened in the UCSF NICU, Summer of nd unit in the country: PCH NICU, Summer of 2009.

3 Objectives Define HIE, identify HIE patients, and treatment modalities available Identify the necessity as well as the components of a successful Neuro NICU and the process for clinical education.

4 What is HIE? (Hypoxic Ischemic Encephalopathy)
5 HIE (Hypoxic Ischemic Encephalopathy)) Hypoxia = a decreased amount of oxygen Ischemia = a decreased amount of blood perfusing the brain Encephalopathy = any dysfunction of the brain HIE in general terms is a brain that has been deprived of oxygen just before and/or during delivery

6 Acute Brain Injury in Newborns Acute event Causes lack of oxygen to brain until oxygen is re-established Results in HIE (Hypoxic Ischemic Encephalopathy)

7 Causes of Acute Brain Injury in Newborns Acute event Causes lack of oxygen to brain until oxygen is reestablished Results in HIE (Hypoxic Ischemic Encephalopathy) Antepartum: Placental insufficiencies, umbilical cord accidents, viral infections, growth retardation, etc. Intrapartum: Placental abruption, cord prolapse, shoulder dystocia, abnormal cord insertion, etc. Postpartum: Infection, aspiration causing asphyxial event, brain blood vessel abnormality, etc.

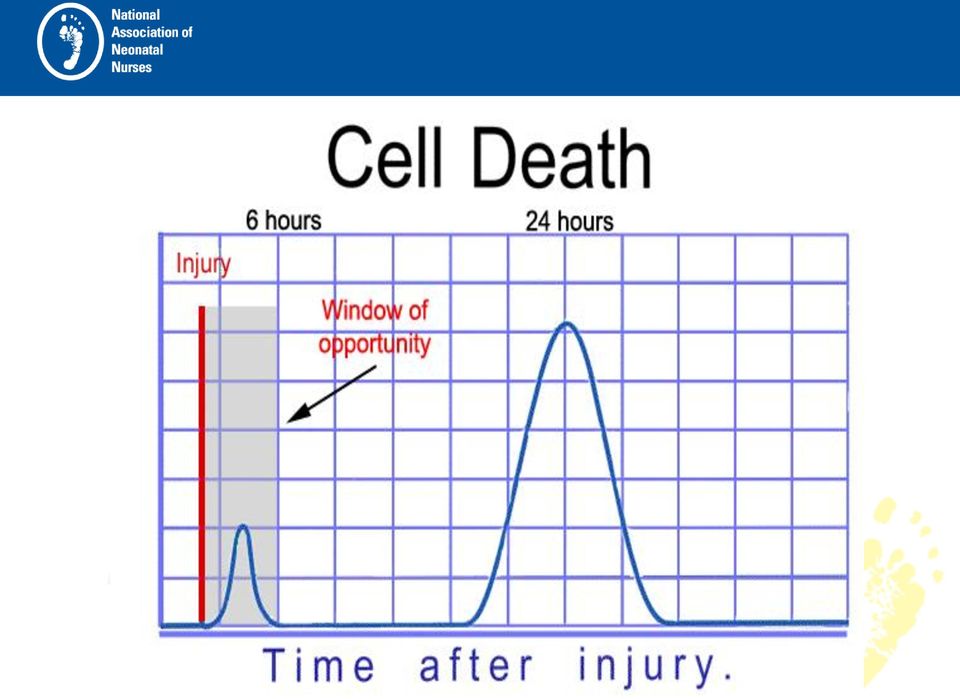
8 HIE Experimental studies have indicated that neuronal death occurs in 2 phases: Primary Neuronal death Delayed or Secondary Neuronal death

9 Primary neuronal death Cellular hypoxia with exhaustion of the cell s high energy stores also known as primary energy failure. It is the initial injury and is primarily necrotic cell death.


10 Secondary (or delayed) neuronal death Occurs 6 hours after the primary injury. Includes cytotoxic edema, mitochondrial failure, active cell death which leads to apoptotic death. Apoptosis, or programmed cell death, is a normal component of the development and health of multicellular organisms. Cells die in response to a variety of stimuli and during apoptosis they do so in a controlled, regulated fashion. Apoptosis is a process in which cells play an active role in their own death (apoptosis is often referred to as cell suicide).

11 Molecular Events Initiated in Brain Tissue by Acute Cerebral Ischemia Brott, NEJM 2000

12 Mechanisms of Brain Injury in the Term Neonate Oxidative stress and excitotoxicity, through downstream intracellular signaling, produce both inflammation and repair Cell death begins immediately and continues during a period of days to weeks. The cell-death phenotype changes from an early necrotic morphology to a pathology resembling apoptosis. This evolution is called the necrosis apoptosis continuum Donna Ferriero, NEJM, 2009


13 Electron microscopic images of dying neurons in neocortex from an infant rat 48 hours after hypoxia-ischemia Necrotic phase Apoptotic phase

14
15 Hypothermia therapy in neonates is now becoming more widely accepted and used in: Hypoxic Ischemic Encephalopathy (HIE) Hypoxic event post delivery, not related to delivery but within 6 hours of birth Prolonged hypoxic event prior to or during ECMO initiation

16 Impact of Brain Injury in Neonates Life-long disabilities include: Cerebral palsy: total cost in the US alone in 2007 was $4 Billion, with an individual cost $900 K/lifetime. (Access Economic Study, CP Foundation) Seizures Hydrocephaly Learning Disabilities and other cognitive dysfunction Speech and visual disturbances
 Seizures Hydrocephaly Learning")
17 HIE (Hypoxic Ischemic Encephalopathy) 1 to 2/1000 term live births are at risk for HIE (Gluckman, Lancet 2005) 25-30% who survive will be left with life-long disabilities: CP (dyskinetic and spastic tetraplegia being the most common), seizures and/or cognitive dysfunction. (Lin, J.Perin, 2006)
, seizures and/or cognitive dysfunction. (Lin, J.Perin, 2006)")
18 Impact of Early Identification and Treatment of Brain Injury/Pathology Decrease in CP severity Decrease in subclinical and clinical seizures resulting in improved brain function Decrease in cognitive deficits, visual and speech impairments

19 What can we do with this window of opportunity? Studies have found that HYPOTHERMIA provides a neuroprotective effect. Hypothermia may modify cells programmed for apoptosis potentially leading to their survival. Hypothermia may also protect neurons by reducing cerebral metabolic rate.

20 Newest Technology in the Treatment of a Birth Asphyxiated Neonate Hypothermic therapy: Head cooling Whole Body Cooling

21 Head Cooling VS Whole Body Cooling Both methods have similar outcomes Head Cooling PROS FDA Approved Whole Body Cooling PROS Easy MRI and EEG access Decreased scalp edema Decreased expense ($7,500) Increased access to infant CONS Limited MRI EEG access Scalp Edema Expense ($28,000) CONS Pending FDA approval Risk for subcutaneous fat necrosis Possible exacerbation of PPHN
22 Olympic Cool-Cap System Medi-Therm 7900
23 Inclusion Criteria Infant at to 36 weeks gestational age and at least ONE of the following: Apgar scores less than or equal to 5 at 10min after birth Continued need for resuscitation, including intubation or mask ventilation at 10min after birth Acidosis defined as either umbilical cord ph or any arterial ph within 60 minutes of birth less than 7.00 Base deficit greater than or equal to -16 mmol/l in any blood sample within 60min of birth (arterial or venous) Prolonged resuscitation while being placed on ECMO
24 Inclusion Criteria (cont) Infant with moderate to severe encephalopathy consisting of altered state of consciousness (as shown by lethargy, stupor, or coma) and at least one of the following: Hypotonia Abnormal reflexes, including oculomotor or pupillary abnormalities Absent or weak suck Clinical seizures
25 Exclusion Criteria infants expected to be >6 hours of age before therapy initiated Major congenital abnormalities excluding Trisomy 21 Evidence of head trauma or skull fracture Babies under 36wk of age Infants <1800 g birth weight
26 Sarnat Scoring A Neurologic evaluation including LOC, neuromuscular control, reflexes, autonomic function, evidence of seizures Three stages Stage 1 mild Good prognosis Stage 2 moderate Good prognosis if clinical and EEG recovery within 5 days Poor prognosis if periodic EEG with interburst intervals totally isoelectric, bursting frequency less than every 6 seconds, bursting pattern (every 3-6 seconds) lasting more than 7 days. Stage 3 severe Major neurologic sequelae, including microcephaly, mental retardation, CP, seizures (all cases).
27
28 Tips for sending facilities and transport teams Save and send placenta on ice for pathology studies Early identification of eligible patients Turn off all external heat sources Document time of heat source removal Monitor rectal temperature (goal ~34.5 C) Passively cool patients- not usually necessary to actively cool patients, but maybe necessary to use ice packs in the armpit and/or groin area during hot summer months of transport Be prepared to slowly warm if the patient falls below 34 C Obtain vascular access (becomes extremely difficult after coolvasoconstriction) Recommend treating with morphine and ativan if needed for comfort Treat only clinical seizures- phenobarbital 20mg/kg Support ventilation if necessary Hemodynamic support: May need volume replacement Expect a lower baseline HR with temperature decrease
29 Monitoring Neurological Status At present, the best technologies available include: the aeeg to monitor brain function Conventional EEGs are also done. INVOS to follow brain perfusion
30 Single EEG Lead (3 wires) What is aeeg?special Filtering Single EEG Lead (3 wires) Bi-parietal Monitor Global Electrocortical Activity Special Filtering Compression Very Slow, Trend Display PROS RN initiation, ease of use, STAT clinical data, early identification of seizure activities CONS Use of 29g needle electrode comes with minimal risk
31 aeeg tracings Normal Sleep/Wake Cycling Upper Margin > 10 µvolts Lower Margin > 5 µvolts Limited Variability Moderate suppression No Sleep/Wake Upper Margin > 10 µvolts Lower Margin < 5 µvolts Increased variability

32 aeeg tracings Severe suppression No Sleep/Wake Upper Margin < 10 µvolts Greatly reduced variability
33 Seizures cause sudden change in EEG amplitude usually a rise during seizure followed by reduced amplitude at the end of seizure aeeg tracings - seizures
34 Impedance Measure of quality of electrode contact Want it as low as possible Alarm if > 20 kohm Can be used to detect lead motion artifact
35
36 Use of NIRS (Near Infrared Spectroscopy). INVOS Brain Spectroscopy: demonstrates brain perfusion and uptake of O2. A high number indicates decreased O2 uptake by tissue Renal/Body Spectroscopy: demonstrates organ perfusion, specifically renal and intestinal. Correlates with changes in hemodynamic stability
37 Use of NIRS As new therapies are becoming available with potential for neuroprotection, NIRS could potentially discriminate between infants at high and low risk for poor outcome in the first few hours of life, and could be used to monitor the safety and efficacy of treatment interventions. NINDS (National institute of Neurological Disorders and Stroke) April 2011
38
39 Reflecting the Color of Life De-oxyhemoglobin and total hemoglobin are noninvasively assessed to generate a regional oxygen saturation (rso 2 ). This site-specific vital sign helps critical care teams detect and correct ischemia and oxygen imbalance to help prevent complications and poor outcomes Provides a continuous, quantitative signal of the physiologic variable most related to injury and most amenable to intervention Hoffman GM Ann Thorac Surg 2006
40 rso Day Day 2 Day 3 rewarming Day 4 Day 5 decannulated Day Cerebral Case History Data 5 days Series1 Version 3.2
41 MRI with Spectroscopy MRI with Spectroscopy done on Day 1 and Day 4 and repeated on either Day 14 or as outpatient. T1, T2 Diffusion Weighted Cerebral Perfusion
42 T1 imaging provides anatomic information as well as high contrast between gray and white matter
43 T2 imaging provides contrast resolution between gray matter, unmylinated and mylinated white matter.
44 Diffusion Weighted Imaging based on the microscopic movement of water molecules in brain tissue.
45 a T2-weighted image depicting normal term brain. b Diffusion-weighted MRI scan showing hypoxic ischemic injury to the deep gray nuclei (arrows). c Diffusion-weighted MRI scan with watershed pattern of hypoxic ischemic injury (top and bottom arrows point to anterior and posterior watershed regions of the cortex and white matter, central arrows show injury to white matter). d T1-weighted imaged depicting diffuse brain injury secondary to global hypoxic ischemic insult. e Diffusion-weighted image showing injury to the white matter and cortex (arrows) in an 11-day-old term infant with congenital heart disease. f Diffusion-weighted MRI scan showing focal stroke (arrow) in a term infant who presented with focal seizures on the second day of life.
46 Spectroscopy (MRS) Acute injury (such as HIE) can be detected by MRS when both diffusion imaging and conventional imaging is negative. MRS can detect elevated lactate in the cerebral cortex or basal ganglia depending on the pattern of injury within the first 24 hours of the injury Reduced NAA and elevated glutamate and glutamine is usually detected after 24 hours.
47 Spectroscopy (MRS) It is a measure of brain chemistry most commonly proton, sodium, phosphorus. Lipids products of brain destruction Lactate product of anaerobic glycolysis NAA neuronal marker Glutamine neurotransmitter Choline cell membrane marker
48 Spectroscopy (MRS) When there is ischemia in the brain it switches to anaerobic glycolysis and lactate accumulates. A markedly elevated lactate in spectroscopy is seen in cerebral hypoxia and ischemia. Choline is elevated, NAA is reduced. If there is cerebral infarction, lipids increase.
49
50 Protocol while utilizing hypothermia Minimize interventions Monitor 72 hours of therapy including q12hr scalp checks (head cooling) and OFC Hourly vital signs Keep rectal temperature C (head cooling). Keep esophageal temperature 33.5 C (whole body cooling) Morphine gtt Watch closely for seizures (aeeg) If seizures present Load with Phenobarbital and follow guidelines The heart rate will immediately fall, no intervention is necessary if BP and O2 sats are stable The infant may become edematous, reposition every four hours and massage skin closely watch urine output (indwelling uri-cath) Labs: ABG s, Electrolytes, CBC, DIC panel, Liver function Infuse as necessary for clotting insufficiencies HUS, MRI and EEG: goal of day one and after rewarm Rewarm after 72 hours- SLOWLY, between 4-6 hour time frame
51 Case Presentations
52 Implementation at PCH Our first Cool-Cap baby: Was born 4/21/08 at an out-lying hospital via primary C-section secondary to placental abruption (otherwise uncomplicated pregnancy) Apgars: 4 at 1min, 5 at 5min, and 6 at 10min Cord ph 6.8 Initial ABG ph 6.8 with a -19 base deficit Transported to PCH for further care arrived and was placed on Cool-Cap at approx 5 hr of age.
53 Post Cool-Cap MRI on 4/28 showed no acute intracranial abnormality and some focal abnormality in the frontal lobe. EEG 4/28 was abnormal, showing some activity over the midline left central region, which appeared depressed. EEG 5/19 continued to show some abnormality, but a normal background with continued depression over the left and central regions. Overall outcome is significantly improved with the use of the Cool-Cap
54 Hypothermia Therapy post delivery One patient: - Normal pregnancy and delivery - Mom given Ambien early in labor, sent home - Returned short time later while under the effects of Ambien and delivered vaginally - Baby given to mom to breastfeed within one hour after delivery, nurse left the room - Returned 5 minutes later to find mom having fallen asleep and baby blue and unresponsive at the breast with apparent suffocation - Code ensued and baby transferred to us for possible cooling - Baby demonstrated moderate encephalopathy on the aeeg and by SARNAT scoring - Baby cooled 72 hours, outcome was normal MRI, normal EEG and normal developmental outcome.
55 Hypothermia Experience with ECMO 5 patients placed on hypothermia therapy (one Cool Cap and four with whole body cooling) And within 24 hours then placed on ECMO (1 V-A 1 VV changed to VA, and 3 V-V ECMO).
56 Patients at Risk for HIE and PPHN MAS: Intrapartum hypoxic event increases meconium release prior to delivery. Chorio/Sepsis: increases risk for development of PPHN Malformations: CHD and CDH increase immediate postpartum hypoxia which increase risk for PPHN
57 Current Research First published trials were in the UK: babies were enrolled in a pilot study of mild hypothermia during ECMO. All of these babies did well, no complications noted using both therapies 2. Second study in 2007, also in the UK, studied aeeg s in infants on ECMO and receiving mild hypothermia. They showed that the aeeg reading was not affected by the mild hypothermia while on ECMO
58 Hypothermia Therapy experience in ECMO Centers in the US Children s National Medical Center (Billie Short): Protocol in place series of 10 patients, 6 MAS, 3 CDH, 1 tracheal stenosis. Results: 3 CDH patients died, tracheal stenosis patient died. Remaining 6 survivors includes 3 normal neurodevelopmental outcomes, 3 with abnormal tone
59 PCH Experience: Joaquin 1st Patient: DOB: 8/26/09 Gestational Age: 38 4/7 Maternal Hx: Unremarkable Birth Hx: Shoulder Dystocia 30 seconds APGARS: 1/3/4 at 1,5,10 minutes Resuscitated, intubated, NaHCO3 given X 2 Initial base deficit -21 ph 6.9 Pulmonary Hemorrhage Transported for hypothermia therapy
60 PCH Experience (cont) Neurological Evaluation upon arrival to PCH: Level of Consciousness: Lethargic Spontaneous Activity: Decreased Posture: Complete Extension Tone: Hypotonic Primitive Reflexes: Absent suck and Moro Autonomic System: Pupils poorly reactive, HR stable, Respiratory: Apnea (Pulmonary hemorrhage, requiring HFJOV) The above SARNAT SCORE is a 2 (Moderate)
61 PCH Experience (cont) INITIAL CLINICAL COURSE: Upon arrival, baby placed on Cool Cap Within less than 24 hrs, baby qualified for VA ECMO secondary to pulmonary hemorrhage and cardiovascular collapse despite Dopamine, Milrinone, and extensive support. ECHO that first day showed severely depressed bi-ventricular function, suprasystemic pressures, large PDA.
62 PCH Experience (cont) CONTINUED CLINICAL COURSE: Cool Cap continued for 72 hrs ECMO continued for total of 6 days, without any complications. Extubated on DOL #10 to CPAP, HHLF on DOL #12, RA on DOL #18 All pressor support d/c d on DOL #5 Feeds started on DOL # 12, full feeds DOL # 19 and all PO DOL #28. Home: DOL # 29
63 PCH Experience (cont) STUDIES: On cooling and ECMO: INVOS was continuously running. Showed good cerebral perfusion. aeeg was also running, showed no seizure activity. Tracing showed moderate to severe encephalopathy. HUS s remained normal
64 PCH Experience (cont) POST COOLING and ECMO STUDIES: EEG s: improved from the first one on DOL #14 showing abnormal, recurrent slow delta activity over L temporal lobe and overall mild to moderate diffuse disturbance of cerebral function to the second on DOL #20 showing mild diffuse abnormality with otherwise normal background
65 PCH Experience (cont) POST COOLING and ECMO STUDIES: MRI: done DOL #6 showed tiny foci of injury in the left posterior, parietal lobe, with otherwise normal parenchyma and spectroscopy, suggestive of NO hypoxic ischemic injury to the brain. MBS: DOL # 20, showed silent aspiration to all consistencies except honey consistency BAER passed bilaterally
66 PCH Experience (cont) POST-DISCHARGE NEURO NICU F/U 4 month Bayley Scales of Infant and Toddler Development III: appropriate for gestation age in all areas, cognitive, motor and language development INFINIB and Gesell done show him to be age appropriate in all areas, and slightly delayed in gross motor by about one month. Ongoing visits for the continued above assessments.
67 PCH Experience: Patient #2 2 nd Patient: DOB 8/6/10 Gestational age: 41 6/7 Maternal history: Lay Midwife care, +GBS, treated with chlorhexidine wipes and vaginal washes Birth history: Home delivery, Apgars 3 and 7. initially breathing then apneic and bradycardic at 15mins, required resuscitation. Initial baby gas: 6.8/89/ base deficit
68 PCH Experience (cont) Neurological Evaluation upon arrival to PCH: Level of Consciousness: Lethargic Spontaneous Activity: Depressed Posture: Complete Extension Tone: Flaccid Primitive Reflexes: Absent suck and Moro Autonomic System: Pupils poorly reactive, HR stable, Respiratory: Apnea The above SARNAT SCORE is a 3 (Severe)
69 PCH Experience (cont) Upon arrival, baby placed on whole body hypothermia blanket Within 6 hours, baby qualified for ECMO and was placed on V-V ECMO secondary to significant cardiovascular compromise (DOP, DOB and EPI drips with ino)
70 PCH Experience (cont) CONTINUED CLINICAL COURSE: - Hypothermia therapy continued for 72 hrs - ECMO continued for total of 8 days, without any complications. - Extubated on DOL #11 to HHLF, RA on DOL #18 - All pressor support d/c d on DOL #5 - Feeds started on DOL # 13, full feeds DOL # 24 - Back transported to continue learning po feeds: DOL # 25
71 PCH Experience (cont) STUDIES: On cooling and ECMO: INVOS was continuously running. Showed good cerebral perfusion. aeeg was also running, showed no seizure activity. Tracing showed moderate to severe encephalopathy. HUS s remained normal
72 PCH Experience (cont) Neurologic Studies: EEG: 1 st on DOL 1 is very abnormal, no sz 2 nd on DOL 10, improved, no sz 3 rd on DOL 14, vastly improved, almost normal MRI: 1 st on DOL 10 (2 nd to being on ECMO) was normal HUS: 5 studies during ECMO, all normal
73 PCH Experience (cont) MBS: Moderate to deep penetration 50% of time with ultrathin (breast milk) and thin consistency. BAER: passed bilaterally Follow-up post discharge: 1 st 4 month neurodevelopmental eval in December, parents report all milestones being met
74 PCH Experience: Patient #3 3 rd patient: DOB 10/19/10 -Gestational Age: 36 5/7 -Maternal HX: Previous two pregnancies with Gest DM, this pregnancy reportedly negative; +GBS received 3 doses of PenG prior to delivery -Birth HX: Attempted vaginal delivery, shoulder dystocia. Baby pushed back up the canal, cord prolapse and c-section. Apgars 0/4/5 at 1/5/10 mins. Cord ph 6.9
75 PCH Experience (cont) Neurological Evaluation upon arrival to PCH: Level of Consciousness: Lethargic Spontaneous Activity: None Posture: Complete Extension Tone: Flaccid Primitive Reflexes: Absent suck and Moro Autonomic System: Pupils reactive, HR stable, Respiratory: Apnea The above SARNAT SCORE is a 3 (Severe)
76 PCH Experience (cont) Upon arrival, baby placed on whole body hypothermia blanket Within 46 hours, baby qualified for ECMO and was placed on V-V ECMO. Prior to ECMO, baby on Dop, Dob and ino. Increasing pco2 despite HFJV.
77 PCH Experience (cont) CONTINUED CLINICAL COURSE: - Hypothermia therapy continued for 72 hrs - ECMO continued for total of 3 days (60 hrs), with prolonged PT despite FFP and development of IVH. - Extubated on DOL #6 to HHLF, RA on DOL #16 - All pressor support d/c d on DOL #5 - Feeds started on DOL # 7
78 PCH Experience (cont) STUDIES: On cooling and ECMO: INVOS was continuously running. Showed initial poor cerebral perfusion. aeeg was also running, continued to severe encephalopathy. Some seizure activity recognized post-ecmo HUS s showed R IVH with extension into septum pallucidum, but no intraparenchymal bleeds.
79 PCH Experience (cont) Neurologic Studies: EEG: 1 st on DOL 1 is very abnormal, no seizures 2 nd on DOL 6: worsening with seizure activity. 3 rd on DOL 8: improved but still abnormal, no seizures 4 th on DOL 14: continues to improve, still not completely normal HUS: first showed edema, repeat subsequently showed R IVH and septum pallucidum bleed. MRI: 1 st on DOL 1 showed mild diffuse white matter injury and R IVH with septum pallucidum bleed/cyst 2 nd : on DOL 6: shows stable ventricular size, no parenchymal bleeds, stable cyst size 3 rd : DOL 14: stable, continues to demonstrate white matter injury, normal gray matter
80 PCH Experience (cont) Brady continued to demonstrate significant emesis. UGI and pyloric U/S were normal. It was felt that the retching originated from pressure of the cyst sitting on the top of the brainstem. Neurosurgery became involved. A tapping reservoir was placed and the cyst drained. MBS soon after showed aspiration at all levels except honey so feeds were thickened.
81 PCH Experience Cooling and ECMO: CONCLUSION Limited evidenced-based results presently available Our five cases suggests that hypothermia therapy used with ECMO can be done safely University of Michigan has a protocol using whole body hypothermia and the ECMO circuit to cool, rather than the Cool Cap (which was cumbersome to use while on ECMO). We feel, that at PCH, consideration for the use of both therapies concomitantly should be done on a case-by-case basis Use of either therapy should not preclude consideration of using the other Need for ECMO secondary to PPHN, may suggest an etiology for CNS injury that may benefit from the use of hypothermia therapy We may want to consider using hypothermia therapy in those situations were there is cardiac arrest going on to ECMO, as this hypoxic state may benefit from hypothermia therapy.
82 NEURO NICU Statistics 4/08 7/11 TOTAL # 101 babies 13 deaths 1 Trisomy 21 2 other chromosomal anomaly
83 Statistics (cont) Maternal risk factor 15 Dec FHT 13 NR FHT 11 MAS 7 Abruption 4 Cord prolapse 4 Nuchal cord 3 True knot 3 Difficult delivery/shoulder/vac/forceps
84 Statistics (cont) Maternal risk factor 2 Maternal death 2 No FHT 1 Post delivery code 1 Pulmonary hemorrhage 1 H1N1 1 Uterine rupture 1 Failure to progress 1 Repeat
85 Statistics (cont) ph range avg=6.94 Base deficit -8 to -30 avg= Lactic Acid 1-24 avg=8.4 Sarnat mild 1 moderate 44 severe 21
86 Research Neuro NICU Data Registry: IRB approved. Allows entry of patient information into data base, tracks neurodevelopmental progress through 18 years of age and allows for ongoing studies concerning treatment modalities, early identification and interventions in relation to outcome measures.
87 Post Discharge Follow-up Neurodevelopmental Follow-up: to document neurodevelopmental assessments for research and recommend therapies for better patient care Rehab services: to document and implement therapy needs (OT/PT and Speech) to optimize neurodevelopmental outcomes
88 Neuro NICU Statistics (cont) 66 currently consented infants: 24 babies have normal neurodevelopmental follow-ups so far. The oldest is 3 1/2 yrs old 12 are delayed in motor 1 delayed cognitive 2 are delayed in speech 4 have documented CP 23 have not followed up
89 Neuro NICU Statistics (cont) In the past, at least 15 out of the 50 babies would have had some form of CP (30%) The numbers above show only 6% (4 out of 66 babies) have been affected by CP. If the 12 delayed motor babies are added to this the number becomes 24%. This indicates a significant improvement, translated as decreasing the rate of CP.
90 Components of a Neuro NICU Hypothermic Therapy Neonatal/Neurological Team Support/Rounds Neuroradiology Support NIDCAP Neurodevelopment Follow-up Research
91 Neuro NICU adjunct staff: Specially trained NICU nurses Pediatric Neurologists and Neonatologists Neurosurgery All NNP s Neuroradiology Genetics NIDCAP trained staff, Developmental Specialists Neurodevelopmental staff including OT/PT, Speech therapy Pathology
92 Guidelines for PT/OT evaluation for patients with HIE All patients who met criteria for hypothermia therapy Evaluation is completed within day one of rewarming to within 72 hours of rewarming Parent education is initiated at or soon after initial evaluation and is ongoing throughout inpatient stay Currently using the AIMS (Alberta Infant Motor Scale) Discharge recommendations are made including follow-up and referrals
93 Occupational therapists Assesses and supports neonate s: Sensory processing: visual, auditory, olfactory Self regulation Fine motor skill and development Midline / bilateral skill development Positioning/ developmental alignment Support family bonding in relation to development and sensory processing Fabricate hand splints as needed Educate family and staff
94 Physical Therapists Assesses and treats neonate s: Gross motor skill development Lower body anomalies Spinal and lower extremity alignment Head shape Developmental positioning Fabricate lower body splints as needed Support and educate family and staff
95 Speech Therapy Establish and support feeding guidelines in conjunction with nursing and medical team Evaluate readiness and coordinate Modified Barium Swallow (MBS)
96 Referral resources PCH NICU follow-up clinic DDD: division of Developmental Disabilities AZEIP: Arizona Early Intervention Program CRS: Children s Rehabilitation Services FBC: Foundation for Blind Children
97 Common Neuro NICU diagnoses HIE Seizures Neuromuscular diseases Metabolic/Genetic Disorders Meningomyelocoele Intraventricular hemmhorages (IVH)/Intracranial bleeds (ICH) CNS Malformations
98
99
100 Current Research MRI with Spectroscopy NIRS evaluation MBS (swallow study evaluation) Placental pathology Autologous cord blood stem cell therapy
101 MRI with Spectrocopy Can we determine outcomes based on spectroscopy evaluation? Can we correlate abnormal MBS findings in the spectroscopy?
102 NIRS Evaluation Trending the NIRS with clinical presentation, MRI, and outcome
103 Dysphagia in Neonates Treated with Hypothermic Therapy For HIE Cristina Carballo, MD, P. David Adelson, MD, Kimberlee Allred, RN NNP-BC, Pamela Clarke-Levens, MS, CCC-SLP Paula Kinnard, RN Neuro NICU, Phoenix Children s Hospital (PCH), Children s Neuroscience Institute, PCH, Phoenix, Arizona Neonatology Associates Ltd
104 Abstract Introduction:. Hypoxic Ischemic Encephalopathy (HIE) is a significant cause of brain injury in neonates. The impact of HIE has varying degrees of neurodevelopmental sequelae including dysphagia. Objectives: To document that infants with moderate to severe HIE, who have received hypothermia treatment as standard of care, are at risk for dysphagia. Methods: A retrospective chart review over a one year period of patients with HIE whom received hypothermia therapy was done. Modified Barium Swallow (MBS) studies were performed on this patient population. A comparison between abnormal and normal MBS study results were evaluated.
105 Abstract Continued Results: There were a total of 32 patients in this chart review. Of the 32 patients, 23 had MBS studies done. Eighteen of 23 MBS were abnormal. This demonstrates a 78% abnormal rate in MBS in infants post hypothermia therapy for treatment of HIE. Conclusions: At this point, in the HIE population, using a specific feeding protocol as well as the inclusion of a MBS with Speech Therapy involvement, would be beneficial for optimum management of these high-risk infants.
106 Introduction Hypoxic Ischemic Encephalopathy (HIE) Significant cause of brain injury in neonates ( 1-2/1000 term live births) Results in varying degrees of neurodevelopmental disabilities, including dysphagia Treatment with hypothermia Proven to be neuroprotective in moderate to severe HIE incidence of dysphagia in post-cooling therapy for HIE has not been studied
107 Objective To evaluate the MBS studies done on infants who had the diagnosis of HIE and also receive hypothermia therapy. To document that infants with moderate to severe HIE, who have been treated with hypothermia treatment, are at high risk for dysphagia's
108 Subjects and Methods Study Design - Retrospective chart review of neonatal cases of HIE evaluated at a pediatric stand-alone facility between Jan Jan Information gathered included MBS study results.
109 Subjects and Methods continued Inclusion Criteria Infants received hypothermia therapy who met the following criteria: > 36 weeks old and under 6 hrs of age -Plus one of the following: -Cord and or baby gas under 60 minutes with ph >7.0 or base deficit > -16 -Prolonged resuscitation, greater than ten minutes -Sarnat score 2-3 and/or seizures -Abnormal aeeg, indicating moderate to severe encephalopathy and/or seizures -infants cooled for the full 72hr Modified Barium Swallow study with speech therapist present
110 Subjects and Methods continued Exclusion Criteria -All congenital and or chromosomal anomalies including Trisomy 21 -Infants with HIE who were not given hypothermia therapy Statistical Analysis -Descriptive statistics to characterize the findings. Data was analyzed to evaluate the incidence of dysphagia -in infants with a diagnosis of HIE treated with hypothermia therapy.
111 Summary -Dysphagia was seen in the majority of HIE affected infants treated with hypothermia therapy. -The definition of dysphagia was an abnormal MBS study that showed laryngeal penetration and/or aspiration. -HIE patients, who were treated with hypothermia therapy, are at high risk for dysphagia. -Dysphagia was treated by thickening the feeds with rice cereal to the consistency deemed safe during the MBS study. All of the 18 infants with abnormal MBS were able to be nipple feed despite the severity of the dysphagia encountered on the MBS study.
112 Summary continued -Conclusions from these analyses must be interpreted cautiously since this was a one year review of charts of infants posthypothermia therapy for HIE. -Trending repeat MBS studies of these infants would provide further insight as to the evolution of the dysphagia.
113 Discussion -We started doing MBS studies on all our infants treated with hypothermia therapy for HIE after we began to notice soft clinical signs of feeding difficulties in some of these infants. -The implications of post-hypothermia treated infants for HIE, with apparently normal neurological exams, are that they are at an unexpected high risk for dysphagia. The dysphagia would not have not been identified except through MBS studies. Since this potential for dysphagia exists, not identifying it could lead to other morbidities, including long-term or late onset respiratory problems.
114 Discussion continued -Through this retrospective look of infants who had hypothermia therapy for HIE, we have realized that there exists an unexpectedly high risk for dysphagia in an otherwise neurologically normal appearing infant. -Based on these findings, we feel that in the post-hypothermia population diagnosed with HIE, using a specific feeding protocol as well as the inclusion of a MBS with Speech Therapy involvement, would be beneficial for optimum management of these high-risk infants.
115 Table 1. MBS Study Analysis MBS n % Normal 5/23 22% Abnormal 18/23 78%

116 Figure 1. Prevalence of Dysphagia

117 Table 2. Severity of Dysphagia
118 Figure 2. Severity of Dysphagia
119 Placental pathology Evaluation of the placenta can identify An acute injury VS chronic injury Sepsis, funicitis Hematological issues
120 Cord tissue vs Cord blood Cord tissue - a rich source of mesenchymal stem cells. These create structural and connective tissue, Cord blood - a rich source of hematopoietic stem cells. These create the blood and immune system. Since cord blood and cord tissue are rich sources of different types of stem cells, they may help repair the body in different ways.
121
122 Cord tissue is a rich source of mesenchymal stem cells, which create structural and connective tissue. These stem cells have unique properties that make them promising for cellular therapies. Stem cells from cord tissue have demonstrated the power to heal spinal cord, brain, and cartilage injuries in laboratory studies. This research is at an early stage and medical treatments are not available today.
123 Autologous cord blood: Baby s own cord blood Cord blood is collected because it contains stem cells, including hematopoietic cells, which can be used to treat hematopoietic and genetic disorders. Stem cells are the body s master cells because they are the building blocks of organ tissue, blood, and the immune system.
124 Cord Blood Cord blood, like bone marrow, is an invaluable source of a type of stem cell that can be used in a variety of medical treatments. To date, cord blood stem cells have been used to treat many life-threatening diseases, such as leukemia and other cancers. Cord blood is showing potential in research to treat conditions like brain injury.
125 Cord blood stem cells are biologically younger and have unique qualities and advantages compared to other stem cell sources like bone marrow: There is less risk of complications when used in transplants. They are immediately available, and early treatment can minimize disease progression. Freezing them "stops the clock" and protects them from environmental damage, age, and common viruses that will impact the stem cells in our bodies over time. Collection of cord blood is simple, safe, and painless. Cord blood stem cells are not embryonic stem cells and are not controversial.
126 In 2005, the National Academy of Sciences published an Institute of Medicine (IoM) report which recommended that expectant parents be given a balanced perspective on their options for cord blood banking. State legislatures around the country are introducing legislation intended to help inform physicians and expectant parents on the options for donating, discarding or banking lifesaving newborn stem cells. Currently 17 states, have enacted legislation recommended by the IoM guidelines.
127 There are 2 basic ways to store cord blood: Public less expensive, used in research Private - more expensive The company provides the kit to obtain the sample and send to them. It is frozen in a cryogenic storage tank until it needs to be used.
128 Clinical Trials
129 Duke University Autologous Cord Blood Cells for Hypoxic Ischemic Encephalopathy Study 1. Phase 1 Study of Feasibility and Safety. Initiated January 2008 Patient population <14 days meeting criteria for HIE Infusions: 4 infusions of own volume reduced cord blood cells. Infants will be have neurodevelopmental follow up at 4-6 and 9-12mos MRI s will be obtained between postnatal weeks 1 and 4, and, for study purposes at 4-6 postnatal months Results to date have shown the therapy to be safe and encouraging.
130 Medical College of Georgia Medical College of Georgia researchers are conducting the first FDA-approved clinical trial to determine whether an infusion of stem cells from umbilical cord blood can improve the quality of life for children with cerebral palsy. The trial Initiated February Evaluating 40 children ages 2-12 with the diagnosis of CP who have autogolous cord blood stored.
131 Phoenix Children s Implementation: (Awaiting IRB approval) 2 randomized groups. Treatment will be after second abnormal MRI (close to DOL 4) vs No treatment. A third MRI will be done at 6 months of age as well as a neurodevelopmental evaluation. If MRI remains abnormal a second injection will be given. Each infant will receive no more than 2 injections.
132 IN ANIMAL STUDIES, newborn stem cells from cord blood demonstrate an ability to cross the blood-brain barrier and migrate to damaged tissue to induce healing. The left-hand photo represents normal, healthy tissue in a rat s brain and shows no evidence of cord blood stem cell migration even after being infused with human cord blood stem cells. The right-hand photo represents diseased rat brain tissue with the green dots showing where the newborn stem cells from cord blood migrated in an effort to induce healing.
133 Seizure guidelines Currently there is a lack of evidence based guidelines for the treatment of neonatal seizures. Majority of NICU s use Phenobarbital as the first line (A 2009 retrospective analysis of 6099 neonates in 31 US hospitals were treated with Phenobarbital). There was more variability of further treatment. There are only 2 published RCT using the Phenobarbital as a first line agent. One study results showed that when used alone up to drug levels of 25mcg/ml, controlled seizures in less than half of the babies. The addition of Fosphenytoin increased the efficacy to 62%. The other study showed even less success with Phenobarbital, only 4/14 babies responding to Phenobarbital to doses of 40/kg.
134 There are only 2 published RCT using the Phenobarbital as a first line agent. One study results showed that when used alone up to drug levels of 25mcg/ml, controlled seizures in less than half of the babies. The addition of Fosphenytoin increased the efficacy to 62%. The other study showed even less success with Phenobarbital, only 4/14 babies responding to Phenobarbital to doses of 40/kg.
135 In fact, there is a landmark study published in 2002 that demonstrated the potential harm that high dose anticonvulsants can do in a neonatal brain. The rat brain is more susceptible to the neuroapoptotic affect of the Phenobarbital during the neonatal period than at any other time.
136 Suggested guidelines Seizures (clinical and/or electrographic) Load with 0.1mg/kg Bumex (blocks the NaK2Cl channel which has been proposed to be the etiology of the neonatal chloride gradient reversal phenomena; suppressing epileptiform activity). Load with 20mg/kg Phenobarbital and 30mg/kg Keppra (Phenobarbital at lower serum levels, not toxic. Keppra is a broad spectrum anticonvulsant with several case reports describing the efficacy in neonatal seizures.
137 Other adjunctive seizure treatment considerations: Magnesium at high end of normal Glucose and oxygen optimization Lidocaine drip
138 Goals for Seizure Treatment Minimize the time from seizure onset to treatment Minimize exposure to Phenobarbital Decrease duration of seizures Increase the efficacy of acute treatment Prophylaxis with non-apoptotic medication
139 Summary Hypothermic Therapy (head or whole body cooling) has shown an improvement in Neurodevelopmental outcomes. A Neuro NICU program implementation encourages a collaborative effort for patient follow up. Continued therapies and research could provide predictability of outcomes.
140 Conclusion Development of a Neuro NICU allows us to more effectively identify and treat brain injury/pathology. Earlier and more aggressive treatment of neonatal brain injury/pathology, whatever the etiology, will result in improved long term neurodevelopmental outcomes. We are a Center of Excellence in the treatment of neonatal brain pathology/injury in the Southwest and the USA
141 References Cochrane Database of Systematic Reviews, Issue 4, 2003 (Jacobs 2003) Hau S, Reich DM, Scholz M, et al. Evidence for neuroprotective properties of human umbilical cord blood cells after neuronal hypoxia in vitro. BMC Neurosci. 2008;9:30. Jacobs, Hunt, Tarnow-Mordi and Inder. Cooling for newborns with hypoxic ischaemic encephalopathy. 08/20/2007 Naqeeb, et al. Pediatrics 1999:103:1263 Natus Medical Cerebral Function Monitor Neuhoff S, Moers J, Rieks M, et al. Proliferation, differentiation, and cytokine secretion of human umbilical cord blood-derived mononuclear cells in vitro. Exp Hematol. 2007;35(7): Olympic Medical Cool-Cap System Phoenix Children s Hospital protocol on Cool-Cap Phoenix Children s Hospital protocol on Cooling Blanket Rocha V, Wagner JE, Jr., Sobocinski KA, et al. Graft-versus-host disease in children who have received a cord-blood or bone marrow transplant from an HLA-identical sibling. Eurocord and International Bone Marrow Transplant Registry Working Committee on Alternative Donor and Stem Cell Sources. N Engl J Med. 2000;342(25): Thorenson, Simmonds, Satas, Tooley and Silver. Effective head cooling during posthypoxic hypothermia in newborn piglets. Pedatri. Res. 49, (2001).
142 References Gunn AJ. Cerebral hypothermia for prevention of brain injury following perinatal asphyxia. Curr Opin. Pediatric 2000; 12: Thornberg E., Thirimyer K, Odebuck A, Milsom I. Birth asphyxia: incidence, clinical course and outcome in a Swedish population. Acta Paediatr 1995; 84: Dixon G, Badawi N, Kurinezvk JJ, Keogh JM, Stilborn Sr, Zubrick Sr, etal. Early developmental outcomes after newborn encephalopathy. Pediatrics 2002; 109: Wilkinson D, Trevor D, etal. Hypothermia: A Neuroprotective Therapy for Neonatal Hypoxic-Ischemic Encephalopathy. Pediatrics 2007; 119: Zanelli SA, Naylor M, Dobbins N, Yuigg M, Goodkin HP, Matsnoto SA, Fairchild KD. Implementation of a Hypothermia for HIE program: 2 year experience in a single NICU, Journal of Perinatology 2008; 28: Shankaran S, etal. Whole Body Hypothermia for Neonates with Hypoxic Ischemic Encephalopathy. NEJM 2005; 353: Gluckman P, Wyatt J, etal. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomized trial. The Lancet 2005; 365: Higgins R, Tonse NK, etal. Hypothermia and Perinatal Asphyxia: Executive Summary of the National Institute of Child Health and Human Development Workshop. Journal of Pediatrics 2006; 148: Kirplani H, Burks J, etal. Cooling for Neonatal Hypoxic Ischemic Encephalopathy: Do we have the answer? Pediatrics 2007; 120: Morgan A., Ward E., Murdoch B., etal Incidence, characteristics and predictive factors for dysphagia after pediatric traumatic brain injury. Journal of Head Trauma & Rehabilitation, 18 (3): Neurology of the Newborn. Joseph J. Volpe. Fifth edition 2008; pages
143 A special thank you to the families who gave permission for their stories to be shared and who shared their families with us.
144 THANK YOU!!!! QUESTIONS?????
145 Save the Date Oct 18-20, Palm Springs Convention Center and Renaissance Hotel - Palm Springs, CA
What do we mean by birth asphyxia
 Neonatal Medicine and brain injury in the Infant at term Andrew Whitelaw Professor of Neonatal Medicine University of Bristol What do we mean by birth asphyxia Interruption in oxygen delivery to the fetus
Neonatal Medicine and brain injury in the Infant at term Andrew Whitelaw Professor of Neonatal Medicine University of Bristol What do we mean by birth asphyxia Interruption in oxygen delivery to the fetus
Newborn Stem Cells from Cord Blood and the Brain: Repairing Injury and Improving Function
 BACKROUNDER: Newborn Stem Cells from Cord Blood and the Brain: Repairing Injury and Improving Function Introduction WITH ONGOING DEVELOPMENTS IN RESEARCH, it is estimated that 1 in every 3 people may benefit
BACKROUNDER: Newborn Stem Cells from Cord Blood and the Brain: Repairing Injury and Improving Function Introduction WITH ONGOING DEVELOPMENTS IN RESEARCH, it is estimated that 1 in every 3 people may benefit
A8b. Resuscitation of a Term Infant with Meconium Staining. Session Summary. Session Objectives. References
 A8b Resuscitation of a Term Infant with Meconium Staining Karen Wright, PhD, NNP-BC Assistant Professor and Coordinator, Neonatal Nurse Practitioner Program Dept. of Women, Children, and Family Nursing,
A8b Resuscitation of a Term Infant with Meconium Staining Karen Wright, PhD, NNP-BC Assistant Professor and Coordinator, Neonatal Nurse Practitioner Program Dept. of Women, Children, and Family Nursing,
Brain Injury during Fetal-Neonatal Transition
 Brain Injury during Fetal-Neonatal Transition Adre du Plessis, MBChB Fetal and Transitional Medicine Children s National Medical Center Washington, DC Brain injury during fetal-neonatal transition Injury
Brain Injury during Fetal-Neonatal Transition Adre du Plessis, MBChB Fetal and Transitional Medicine Children s National Medical Center Washington, DC Brain injury during fetal-neonatal transition Injury
UMBILICAL CORD BLOOD COLLECTION
 UMBILICAL CORD BLOOD COLLECTION by Frances Verter, PhD Founder & Director, Parent's Guide to Cord Blood Foundation info@parentsguidecordblood.org and Kim Petrella, RN Department of Obstetrics and Gynecology
UMBILICAL CORD BLOOD COLLECTION by Frances Verter, PhD Founder & Director, Parent's Guide to Cord Blood Foundation info@parentsguidecordblood.org and Kim Petrella, RN Department of Obstetrics and Gynecology
Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire
 Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire") Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire Date: RPICC Facility: CMS use only Include the following
Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire Date: RPICC Facility: CMS use only Include the following
Why is prematurity a concern?
 Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
Cerebral Palsy An Expensive Enigma
 Cerebral Palsy An Expensive Enigma Rhona Mahony National Maternity Hospital A group of permanent disorders of the development of movement and posture, causing activity limitation that are not attributed
Cerebral Palsy An Expensive Enigma Rhona Mahony National Maternity Hospital A group of permanent disorders of the development of movement and posture, causing activity limitation that are not attributed
Cerebral palsy can be classified according to the type of abnormal muscle tone or movement, and the distribution of these motor impairments.
 The Face of Cerebral Palsy Segment I Discovering Patterns What is Cerebral Palsy? Cerebral palsy (CP) is an umbrella term for a group of non-progressive but often changing motor impairment syndromes, which
The Face of Cerebral Palsy Segment I Discovering Patterns What is Cerebral Palsy? Cerebral palsy (CP) is an umbrella term for a group of non-progressive but often changing motor impairment syndromes, which
STEM CELLS FROM THE UMBLICAL CORD BLOOD AND UMBLICAL CORD TISSUE
 STEM CELLS FROM THE UMBLICAL CORD BLOOD AND UMBLICAL CORD TISSUE What are Stem Cells? Stem cells are the basic building blocks of all the cells, tissues and organs in the human body. The role of the stem
STEM CELLS FROM THE UMBLICAL CORD BLOOD AND UMBLICAL CORD TISSUE What are Stem Cells? Stem cells are the basic building blocks of all the cells, tissues and organs in the human body. The role of the stem
Fetal Acid Base Status and Umbilical Cord Sampling. David Acker, MD
 Fetal Acid Base Status and Umbilical Cord Sampling David Acker, MD Part I: Some Background Intra-uterine Event as Causative of CP Cord ph < 7.00 and base excess of > 12 Early onset neonatal encephalopathy
Fetal Acid Base Status and Umbilical Cord Sampling David Acker, MD Part I: Some Background Intra-uterine Event as Causative of CP Cord ph < 7.00 and base excess of > 12 Early onset neonatal encephalopathy
Standard of Care: Neonatal Intensive Care Unit (NICU) Physical and Occupational Therapy Management of the high risk infant.
 Physical and Occupational Therapy Management of the high risk infant.") BRIGHAM & WOMEN S HOSPITAL Department of Rehabilitation Services Standard of Care: Neonatal Intensive Care Unit (NICU) Case Type / Diagnosis: The high-risk infant is defined as the baby with any event
BRIGHAM & WOMEN S HOSPITAL Department of Rehabilitation Services Standard of Care: Neonatal Intensive Care Unit (NICU) Case Type / Diagnosis: The high-risk infant is defined as the baby with any event
Demystifying Stem Cells. Brent Bost M.D., CPA, MBA, FACOG
 Demystifying Stem Cells Brent Bost M.D., CPA, MBA, FACOG Disclaimers Author currently serves on Board of Directors of CordTrack Most applications discussed today are not currently FDA approved and are,
Demystifying Stem Cells Brent Bost M.D., CPA, MBA, FACOG Disclaimers Author currently serves on Board of Directors of CordTrack Most applications discussed today are not currently FDA approved and are,
Post - resuscitation management of an asphyxiated neonate
 Post - resuscitation management of an asphyxiated neonate Slide PA 1, 2 Introduction Perinatal asphyxia is a common neonatal problem and contributes significantly to neonatal morbidity and mortality. It
Post - resuscitation management of an asphyxiated neonate Slide PA 1, 2 Introduction Perinatal asphyxia is a common neonatal problem and contributes significantly to neonatal morbidity and mortality. It
Ischemia and Infarction
 Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Ischemia and Infarction HST.035 Spring 2003 In the US: ~50% of deaths are due to
Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Ischemia and Infarction HST.035 Spring 2003 In the US: ~50% of deaths are due to
A Cool Therapy for HIE. It s s Here! A Cool Therapy for Neonatal Brain Injury
 A Cool Therapy for HIE It s s Here! A Cool Therapy for Neonatal Brain Injury Corinne L. Leach, MD, PhD Women and Children s s Hospital of Buffalo Grand Rounds July 25, 2008 I. Case Report II. Extent of
A Cool Therapy for HIE It s s Here! A Cool Therapy for Neonatal Brain Injury Corinne L. Leach, MD, PhD Women and Children s s Hospital of Buffalo Grand Rounds July 25, 2008 I. Case Report II. Extent of
Discover the Possibilities Born With Your Baby
 Discover the Possibilities Born With Your Baby Your Simple Guide to Saving Cord Blood The Power and Promise The lifesaving power of cord blood and regenerative healing potential of cord blood and cord
Discover the Possibilities Born With Your Baby Your Simple Guide to Saving Cord Blood The Power and Promise The lifesaving power of cord blood and regenerative healing potential of cord blood and cord
the future in your hands imagine
 the future in your hands imagine The promise of hope Carrie and Wilf s story... Quinn weighed in at a healthy 4397g at birth. His parents, Carrie and Wilf, had decided to store the umbilical cord blood
the future in your hands imagine The promise of hope Carrie and Wilf s story... Quinn weighed in at a healthy 4397g at birth. His parents, Carrie and Wilf, had decided to store the umbilical cord blood
Developmental delay and Cerebral palsy. Present the differential diagnosis of developmental delay.
 Developmental delay and Cerebral palsy objectives 1. developmental delay Define developmental delay Etiologies of developmental delay Present the differential diagnosis of developmental delay. 2. cerebral
Developmental delay and Cerebral palsy objectives 1. developmental delay Define developmental delay Etiologies of developmental delay Present the differential diagnosis of developmental delay. 2. cerebral
Newborn Stem Cells from Cord Blood and the Brain: Repairing Injury and Improving Function
 BACKROUNDER: Newborn Stem Cells from Cord Blood and the Brain: Repairing Injury and Improving Function Introduction WITH ONGOING DEVELOPMENTS IN SCIENCE, researchers estimate that 1 in every 3 people may
BACKROUNDER: Newborn Stem Cells from Cord Blood and the Brain: Repairing Injury and Improving Function Introduction WITH ONGOING DEVELOPMENTS IN SCIENCE, researchers estimate that 1 in every 3 people may
House Resolution No. 37
 california legislature regular session House Resolution No. Introduced by Assembly Member Hill August, House Resolution No. Relative to umbilical cord blood banking. WHEREAS, Since the first umbilical
california legislature regular session House Resolution No. Introduced by Assembly Member Hill August, House Resolution No. Relative to umbilical cord blood banking. WHEREAS, Since the first umbilical
Newborn outcomes after cesarean section for fetal distress in BC
 Newborn outcomes after cesarean section for fetal distress in BC Patricia Janssen, PhD, UBC School of Population and Public Health Scientist, Child and Family Research Institute Kevin Jenniskens, MSc,
Newborn outcomes after cesarean section for fetal distress in BC Patricia Janssen, PhD, UBC School of Population and Public Health Scientist, Child and Family Research Institute Kevin Jenniskens, MSc,
Cerebral Palsy. In order to function, the brain needs a continuous supply of oxygen.
 Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Up to 5000 children in the United States are diagnosed with cerebral palsy every year. This reference
Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Up to 5000 children in the United States are diagnosed with cerebral palsy every year. This reference
C CS. California Children Services Alameda County
 C CS California Children Services Alameda County The California Children Services (CCS) Program strives to assure access to medical services essential to the health and well-being of children with catastrophic
C CS California Children Services Alameda County The California Children Services (CCS) Program strives to assure access to medical services essential to the health and well-being of children with catastrophic
Epilepsy 101: Getting Started
 American Epilepsy Society 1 Epilepsy 101 for nurses has been developed by the American Epilepsy Society to prepare professional nurses to understand the general issues, concerns and needs of people with
American Epilepsy Society 1 Epilepsy 101 for nurses has been developed by the American Epilepsy Society to prepare professional nurses to understand the general issues, concerns and needs of people with
Cerebral palsy, neonatal death and stillbirth rates Victoria, 1973-1999
 Cerebral Palsy: Aetiology, Associated Problems and Management Lecture for FRACP candidates July 2010 Definitions and prevalence Risk factors and aetiology Associated problems Management options Cerebral
Cerebral Palsy: Aetiology, Associated Problems and Management Lecture for FRACP candidates July 2010 Definitions and prevalence Risk factors and aetiology Associated problems Management options Cerebral
5 Frequently Asked Questions About Adult Stem Cell Research
 5 Frequently Asked Questions About Adult Stem Cell Research Stem cells are often referred to in the sociopolitical realm with some level of controversy and beyond that, some level of confusion. Many researchers
5 Frequently Asked Questions About Adult Stem Cell Research Stem cells are often referred to in the sociopolitical realm with some level of controversy and beyond that, some level of confusion. Many researchers
Careful collection, organization and review of medical information
 Preparing Birth Injury Case Prior To Expert Review of Causation Careful collection, organization and review of medical information essential to documentation of injury By RICHARD A. SILVER When analyzing
Preparing Birth Injury Case Prior To Expert Review of Causation Careful collection, organization and review of medical information essential to documentation of injury By RICHARD A. SILVER When analyzing
The Initial and 24 h (After the Patient Rehabilitation) Deficit of Arterial Blood Gases as Predictors of Patients Outcome
 Deficit of Arterial Blood Gases as Predictors of Patients Outcome") Biomedical & Pharmacology Journal Vol. 6(2), 259-264 (2013) The Initial and 24 h (After the Patient Rehabilitation) Deficit of Arterial Blood Gases as Predictors of Patients Outcome Vadod Norouzi 1, Ali
Biomedical & Pharmacology Journal Vol. 6(2), 259-264 (2013) The Initial and 24 h (After the Patient Rehabilitation) Deficit of Arterial Blood Gases as Predictors of Patients Outcome Vadod Norouzi 1, Ali
Not All Stem Cells are the Same
 Cord Blood Banking and Transplantation Jennifer Willert, M.D. Hematology/Oncology Blood and Marrow Transplant Rady Children s Hospital San Diego Clinical Professor UCSD Not All Stem Cells are the Same
Cord Blood Banking and Transplantation Jennifer Willert, M.D. Hematology/Oncology Blood and Marrow Transplant Rady Children s Hospital San Diego Clinical Professor UCSD Not All Stem Cells are the Same
PARAMEDIC TRAINING CLINICAL OBJECTIVES
 Page 1 of 21 GENERAL PATIENT UNIT When assigned to the General Patient unit paramedic student should gain knowledge and experience in the following: 1. Appropriate communication with patients and members
Page 1 of 21 GENERAL PATIENT UNIT When assigned to the General Patient unit paramedic student should gain knowledge and experience in the following: 1. Appropriate communication with patients and members
Promising Treatments for SCI: What s on The Horizon. SCI: A Devastating Injury. Case: Mr. MC 9/21/2015. Epidemiology: Costs:
 Promising Treatments for SCI: What s on The Horizon Shawn Song, MD SCI Fellow University of Washington/VA Puget Sound Healthcare System SCI: A Devastating Injury Epidemiology: Incidence of ~12,000 patients/year.
Promising Treatments for SCI: What s on The Horizon Shawn Song, MD SCI Fellow University of Washington/VA Puget Sound Healthcare System SCI: A Devastating Injury Epidemiology: Incidence of ~12,000 patients/year.
By Dr. Mindy Aisen CEO and Director United Cerebral Palsy Research and Educational Foundation www.ucpresearch.org CEREBRAL PALSY RESEARCH
 By Dr. Mindy Aisen CEO and Director United Cerebral Palsy Research and Educational Foundation www.ucpresearch.org CEREBRAL PALSY RESEARCH Main Sources of Federal Funding for Cerebral Palsy and Disability
By Dr. Mindy Aisen CEO and Director United Cerebral Palsy Research and Educational Foundation www.ucpresearch.org CEREBRAL PALSY RESEARCH Main Sources of Federal Funding for Cerebral Palsy and Disability
The importance of acidosis in asphyxia
 The importance of acidosis in asphyxia Janet M Rennie Senior Lecturer in Neonatal Medicine Institute for Women s Health, UCL, London Clinical negligence seminar, 1 Crown Office Row Objectives To review
The importance of acidosis in asphyxia Janet M Rennie Senior Lecturer in Neonatal Medicine Institute for Women s Health, UCL, London Clinical negligence seminar, 1 Crown Office Row Objectives To review
A look at continuing developments in the field, including history of fetal monitoring and causation issues
 Medical malpractice: Preparation and trial of birth injury cases A look at continuing developments in the field, including history of fetal monitoring and causation issues BY JAMES BOSTWICK Over the past
Medical malpractice: Preparation and trial of birth injury cases A look at continuing developments in the field, including history of fetal monitoring and causation issues BY JAMES BOSTWICK Over the past
Cerebral Palsy. 1995-2014, The Patient Education Institute, Inc. www.x-plain.com nr200105 Last reviewed: 06/17/2014 1
 Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Thousands of children are diagnosed with cerebral palsy every year. This reference summary explains
Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Thousands of children are diagnosed with cerebral palsy every year. This reference summary explains
Extracorporeal Life Support Organization (ELSO) Guidelines for Neonatal Respiratory Failure
 Guidelines for Neonatal Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Neonatal Respiratory Failure Introduction This neonatal respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Neonatal Respiratory Failure Introduction This neonatal respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas
 Billing and Coding in Neurology and Headache Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas CPT Codes vs. ICD Codes Category
Billing and Coding in Neurology and Headache Stuart B Black MD, FAAN Chief of Neurology Co-Medical Director: Neuroscience Center Baylor University Medical Center at Dallas CPT Codes vs. ICD Codes Category
Obstetrical Emergencies
 Date: July 18, 2014 Page 1 of 5 Obstetrical Emergencies Purpose: To provide the process for the assessment and management of the patient with an obstetrical related emergency. Pre-Medical Control 1. Follow
Date: July 18, 2014 Page 1 of 5 Obstetrical Emergencies Purpose: To provide the process for the assessment and management of the patient with an obstetrical related emergency. Pre-Medical Control 1. Follow
Jamie Peregrine, MD, PGY-4 KU-Wichita, OB/GYN Wesley Medical Center
 Jamie Peregrine, MD, PGY-4 KU-Wichita, OB/GYN Wesley Medical Center Uses for umbilical cord stem cells Describe the indications and uses for umbilical cord stem cells. Counsel patients on the advantages
Jamie Peregrine, MD, PGY-4 KU-Wichita, OB/GYN Wesley Medical Center Uses for umbilical cord stem cells Describe the indications and uses for umbilical cord stem cells. Counsel patients on the advantages
ELSO GUIDELINES FOR TRAINING AND CONTINUING EDUCATION OF ECMO SPECIALISTS
 ELSO GUIDELINES FOR TRAINING AND CONTINUING EDUCATION OF ECMO SPECIALISTS PURPOSE The "" is a document developed by the Extracorporeal Life Support Organization (ELSO) as a reference for current and future
ELSO GUIDELINES FOR TRAINING AND CONTINUING EDUCATION OF ECMO SPECIALISTS PURPOSE The "" is a document developed by the Extracorporeal Life Support Organization (ELSO) as a reference for current and future
CORD BLOOD COLLECTION / ANALYSIS- AT BIRTH
 WOMEN AND NEWBORN HEALTH SERVICE King Edward Memorial Hospital CLINICAL GUIDELINES OBSTETRICS AND MIDWIFERY King Edward Memorial Hospital WOMEN AND NEWBORN HEALTH SERVICE INTRAPARTUM CARE SPECIMEN COLLECTION
WOMEN AND NEWBORN HEALTH SERVICE King Edward Memorial Hospital CLINICAL GUIDELINES OBSTETRICS AND MIDWIFERY King Edward Memorial Hospital WOMEN AND NEWBORN HEALTH SERVICE INTRAPARTUM CARE SPECIMEN COLLECTION
TIMING OF ASPHYXIAL INJURY AND BIRTH TRAUMA
 TIMING OF ASPHYXIAL INJURY AND BIRTH TRAUMA Richard C. Halpern, Partner, Thomson Rogers Obstetric Malpractice cases involving asphyxiated newborns present unique challenges to Plaintiffs counsel. Standard
TIMING OF ASPHYXIAL INJURY AND BIRTH TRAUMA Richard C. Halpern, Partner, Thomson Rogers Obstetric Malpractice cases involving asphyxiated newborns present unique challenges to Plaintiffs counsel. Standard
REHABILITATION SERVICES
 REHABILITATION SERVICES Table of Contents GENERAL... 2 TERMS AND ABBREVIATIONS... 2 PRIOR AUTHORIZATION REQUIREMENTS FOR MEDICAID REIMBURSEMENT OF INPATIENT REHABILITATION SERVICES (Updated 4/1/11)...
REHABILITATION SERVICES Table of Contents GENERAL... 2 TERMS AND ABBREVIATIONS... 2 PRIOR AUTHORIZATION REQUIREMENTS FOR MEDICAID REIMBURSEMENT OF INPATIENT REHABILITATION SERVICES (Updated 4/1/11)...
It s not something you want to think about, but it s something you want to prepare for.
 It s not something you want to think about, but it s something you want to prepare for. StemCyte cord blood banking offers your family a new lifesaving treatment alternative Why Bank Take the once-in-alifetime
It s not something you want to think about, but it s something you want to prepare for. StemCyte cord blood banking offers your family a new lifesaving treatment alternative Why Bank Take the once-in-alifetime
Hyperbaric Oxygen Therapy (HBOT) as a treatment for Cerebral Palsy
 as a treatment for Cerebral Palsy") Hyperbaric Oxygen Therapy (HBOT) as a treatment for Cerebral Palsy What is Cerebral Palsy Cerebral palsy, or CP, refers to a group of developmental conditions that have several features in common (Rosenbaum,
Hyperbaric Oxygen Therapy (HBOT) as a treatment for Cerebral Palsy What is Cerebral Palsy Cerebral palsy, or CP, refers to a group of developmental conditions that have several features in common (Rosenbaum,
 GUIDELINES FOR HOSPITALS WITH NEONATAL INTENSIVE CARE SERVICE : REGULATION 4 OF THE PRIVATE HOSPITALS AND MEDICAL CLINICS REGULATIONS [CAP 248, Rg 1] I Introduction 1. These Guidelines serve as a guide
GUIDELINES FOR HOSPITALS WITH NEONATAL INTENSIVE CARE SERVICE : REGULATION 4 OF THE PRIVATE HOSPITALS AND MEDICAL CLINICS REGULATIONS [CAP 248, Rg 1] I Introduction 1. These Guidelines serve as a guide
Cerebral Palsy. www.teachinngei.org p. 1
 Cerebral Palsy What is cerebral palsy? Cerebral palsy (CP) is a motor disability caused by a static, non-progressive lesion (encephalopathy) in the brain that occurs in early childhood, usually before
Cerebral Palsy What is cerebral palsy? Cerebral palsy (CP) is a motor disability caused by a static, non-progressive lesion (encephalopathy) in the brain that occurs in early childhood, usually before
Guide to Pregnancy and Birth Injury Claims
 Being pregnant, especially for the first time can be a very daunting experience where you often have to put all of your faith in your midwife or doctor. The majority of pregnancies and births occur without
Being pregnant, especially for the first time can be a very daunting experience where you often have to put all of your faith in your midwife or doctor. The majority of pregnancies and births occur without
Hummi Micro Draw Blood Transfer Device. The Next Generation System for Closed Micro Blood Sampling in the Neonate
 Hummi Micro Draw Blood Transfer Device The Next Generation System for Closed Micro Blood Sampling in the Neonate Current Methods for Umbilical Blood Sampling Current Methods for Umbilical Blood Sampling
Hummi Micro Draw Blood Transfer Device The Next Generation System for Closed Micro Blood Sampling in the Neonate Current Methods for Umbilical Blood Sampling Current Methods for Umbilical Blood Sampling
Saving Your Baby s Cord Blood
 Saving Your Baby s Cord Blood An Important Pregnancy Decision 1-888-CORD BLOOD HEALTHY FUTURES ARE Born at CBR For every parent who wishes they could do more to protect their family s health, there s Cord
Saving Your Baby s Cord Blood An Important Pregnancy Decision 1-888-CORD BLOOD HEALTHY FUTURES ARE Born at CBR For every parent who wishes they could do more to protect their family s health, there s Cord
Request an information pack
 Request an information pack Please tear off completed form and place in mail box, alternatively please fax this page to 03 9551 2933 I would like to receive an information pack by (please tick one) Email
Request an information pack Please tear off completed form and place in mail box, alternatively please fax this page to 03 9551 2933 I would like to receive an information pack by (please tick one) Email
Chapter 10. Summary & Future perspectives
 Summary & Future perspectives 123 Multiple sclerosis is a chronic disorder of the central nervous system, characterized by inflammation and axonal degeneration. All current therapies modulate the peripheral
Summary & Future perspectives 123 Multiple sclerosis is a chronic disorder of the central nervous system, characterized by inflammation and axonal degeneration. All current therapies modulate the peripheral
Level III Stroke Center Data Collection Requirements
 Who? Level III Stroke Center Data Collection Requirements All LERN Level III Stroke Centers. LERN Level I and II Stroke Centers have reporting requirements to The Joint Commission or other Board approved
Who? Level III Stroke Center Data Collection Requirements All LERN Level III Stroke Centers. LERN Level I and II Stroke Centers have reporting requirements to The Joint Commission or other Board approved
Therapeutic Potential of Cells Derived from Gestational Tissues: A coming of age. Dr Roisin Deane Cell Care Australia Pty Ltd
 Therapeutic Potential of Cells Derived from Gestational Tissues: A coming of age Dr Roisin Deane Cell Care Australia Pty Ltd What are Gestational Stem Cells? Stem cells isolated from the gestational tissues
Therapeutic Potential of Cells Derived from Gestational Tissues: A coming of age Dr Roisin Deane Cell Care Australia Pty Ltd What are Gestational Stem Cells? Stem cells isolated from the gestational tissues
INTRAPARTUM PATHWAYS TO NEONATAL NEUROLOGIC INJURY - A LAWYER S VIEW OF THE MEDICINE
 INTRAPARTUM PATHWAYS TO NEONATAL NEUROLOGIC INJURY - A LAWYER S VIEW OF THE MEDICINE By Richard C. Halpern Partner Thomson Rogers rhalpern@thomsonrogers.com 416-868-3215 November 2013 INTRODUCTION Newborn
INTRAPARTUM PATHWAYS TO NEONATAL NEUROLOGIC INJURY - A LAWYER S VIEW OF THE MEDICINE By Richard C. Halpern Partner Thomson Rogers rhalpern@thomsonrogers.com 416-868-3215 November 2013 INTRODUCTION Newborn
Physiologic Basis for Fetal Heart Rate Monitoring
 Physiologic Basis for Fetal Heart Rate Monitoring Physiologic Basis for Fetal Heart Rate Monitoring The objective of intrapartum fetal heart rate (FHR) monitoring is to prevent fetal injury that might
Physiologic Basis for Fetal Heart Rate Monitoring Physiologic Basis for Fetal Heart Rate Monitoring The objective of intrapartum fetal heart rate (FHR) monitoring is to prevent fetal injury that might
Neonatal Emergencies. Care of the Neonate. Care of the Neonate. Care of the Neonate. Student Objectives. Student Objectives continued.
 Student Objectives Neonatal Emergencies After completing this section the student will be able to: 1. Identify three physiologic and/or anatomic features unique to the newborn 2. List three perinatal factors
Student Objectives Neonatal Emergencies After completing this section the student will be able to: 1. Identify three physiologic and/or anatomic features unique to the newborn 2. List three perinatal factors
Steps to getting a diagnosis: Finding out if it s Alzheimer s Disease.
 Steps to getting a diagnosis: Finding out if it s Alzheimer s Disease. Memory loss and changes in mood and behavior are some signs that you or a family member may have Alzheimer s disease. If you have
Steps to getting a diagnosis: Finding out if it s Alzheimer s Disease. Memory loss and changes in mood and behavior are some signs that you or a family member may have Alzheimer s disease. If you have
What percentage of term cerebral palsy cases have a normal head MRI? Cerebral Palsy: Definition. No financial conflicts of interest to report
 Cerebral Palsy: Risk Factors and Etiology No financial conflicts of interest to report William M. Gilbert, MD Regional Medical Director, Women s Services Sutter Health, Sac-Sierra Region What percentage
Cerebral Palsy: Risk Factors and Etiology No financial conflicts of interest to report William M. Gilbert, MD Regional Medical Director, Women s Services Sutter Health, Sac-Sierra Region What percentage
Pediatric Airway Management
 Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Cerebral Palsy Information
 Cerebral Palsy Information The following information was extracted from the Mayo Clinic s website Definition: "Cerebral palsy" is a general term for a group of disorders that appear during the first few
Cerebral Palsy Information The following information was extracted from the Mayo Clinic s website Definition: "Cerebral palsy" is a general term for a group of disorders that appear during the first few
Regions Hospital Delineation of Privileges Nurse Practitioner
 Regions Hospital Delineation of Privileges Nurse Practitioner Applicant s Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic
Regions Hospital Delineation of Privileges Nurse Practitioner Applicant s Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]
![SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]](/thumbs/27/9667060.jpg "SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D]") SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D] I. Definitions: Detoxification is the process of interrupting the momentum of compulsive drug and/or alcohol use in an individual
SUBSTANCE USE DISORDER SOCIAL DETOXIFICATION SERVICES [ASAM LEVEL III.2-D] I. Definitions: Detoxification is the process of interrupting the momentum of compulsive drug and/or alcohol use in an individual
CEREBRAL PALSY AND MENTAL RETARDATION DEFINITION
 CEREBRAL PALSY AND MENTAL RETARDATION DEFINITION It is a disorder of posture movement and tone due to a static encephalopathy acquired during brain growth in fetal life infancy or early childhood. Though
CEREBRAL PALSY AND MENTAL RETARDATION DEFINITION It is a disorder of posture movement and tone due to a static encephalopathy acquired during brain growth in fetal life infancy or early childhood. Though
The Facts about Cord Blood
 The Facts about Cord Blood Dear Future Mom and/or Dad, All of us at CorCell would like to give you a big CONGRATULATIONS on your new baby! Now that you are expecting, you have probably heard about saving
The Facts about Cord Blood Dear Future Mom and/or Dad, All of us at CorCell would like to give you a big CONGRATULATIONS on your new baby! Now that you are expecting, you have probably heard about saving
Safe Zone: CV PIP < 26; HFOV: MAP < 16; HFJV: MAP < 16 Dopamine infusion up to 20 mcg/kg/min Epinephrine infusion up to 0.1 mcg /kg/min.
 Congenital Diaphragmatic Hernia: Management Guidelines 5-2006 Issued By: Division of Neonatology Reviewed: Effective Date: Categories: Chronicity Document Congenital Diaphragmatic Hernia: Management Guidelines
Congenital Diaphragmatic Hernia: Management Guidelines 5-2006 Issued By: Division of Neonatology Reviewed: Effective Date: Categories: Chronicity Document Congenital Diaphragmatic Hernia: Management Guidelines
What You Should Know About Cerebral Aneurysms
 What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Interventions Committee of the American Heart Association Cardiovascular Radiology Council Randall T. Higashida, M.D.,
What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Interventions Committee of the American Heart Association Cardiovascular Radiology Council Randall T. Higashida, M.D.,
CORD BLOOD BANKING FAQ
 CORD BLOOD BANKING FAQ Cord Blood & Stem Cells Q: What is umbilical cord blood (UCB)? A: Bone marrow, peripheral blood and UCB constitute the three primary sources of stem cells. Cord blood, which, until
CORD BLOOD BANKING FAQ Cord Blood & Stem Cells Q: What is umbilical cord blood (UCB)? A: Bone marrow, peripheral blood and UCB constitute the three primary sources of stem cells. Cord blood, which, until
First Year. PT7040- Clinical Skills and Examination II
 First Year Summer PT7010 Anatomical Dissection for Physical Therapists This is a dissection-based, radiographic anatomical study of the spine, lower extremity, and upper extremity as related to physical
First Year Summer PT7010 Anatomical Dissection for Physical Therapists This is a dissection-based, radiographic anatomical study of the spine, lower extremity, and upper extremity as related to physical
Overview. Geriatric Overview. Chapter 26. Geriatrics 9/11/2012
 Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Neonatal Hypotonia. Clinical Approach to Floppy Baby
 Neonatal Hypotonia Clinical Approach to Floppy Baby Hypotonia in the newborn is a common presenting feature of systemic illness or neurologic dysfunction at any level of the central or peripheral nervous
Neonatal Hypotonia Clinical Approach to Floppy Baby Hypotonia in the newborn is a common presenting feature of systemic illness or neurologic dysfunction at any level of the central or peripheral nervous
Medicaid Disability Manual
 Part B The following sections apply to individuals under age 18. If the criteria in Part B do not apply, Part A criteria may be used when those criteria give appropriate consideration to the effects of
Part B The following sections apply to individuals under age 18. If the criteria in Part B do not apply, Part A criteria may be used when those criteria give appropriate consideration to the effects of
Why the INFANT Study
 The INFANT Study A multi-centre Randomised Controlled Trial (RCT) of an intelligent system to support decision making in the management of labour using the CTG Why the INFANT Study INFANT stands for INtelligent
The INFANT Study A multi-centre Randomised Controlled Trial (RCT) of an intelligent system to support decision making in the management of labour using the CTG Why the INFANT Study INFANT stands for INtelligent
Neonatal Outreach Education Program Course Catalog
 2012 Neonatal Outreach Education Program Course Catalog Photo by Brian Redden (559) 353-5615 (559) 353-6255 Table of Contents Program Overview... 2 General Course Information... 3 Save The Date Children
2012 Neonatal Outreach Education Program Course Catalog Photo by Brian Redden (559) 353-5615 (559) 353-6255 Table of Contents Program Overview... 2 General Course Information... 3 Save The Date Children
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
Head Injury. Dr Sally McCarthy Medical Director ECI
 Head Injury Dr Sally McCarthy Medical Director ECI Head injury in the emergency department A common presentation 80% Mild Head Injury = GCS 14 15 10% Moderate Head Injury = GCS 9 13 10% Severe Head Injury
Head Injury Dr Sally McCarthy Medical Director ECI Head injury in the emergency department A common presentation 80% Mild Head Injury = GCS 14 15 10% Moderate Head Injury = GCS 9 13 10% Severe Head Injury
ELSO GUIDELINES FOR ECMO CENTERS
 ELSO GUIDELINES FOR ECMO CENTERS PURPOSE These guidelines developed by the Extracorporeal Life Support Organization, outline the ideal institutional requirements needed for effective use of extracorporeal
ELSO GUIDELINES FOR ECMO CENTERS PURPOSE These guidelines developed by the Extracorporeal Life Support Organization, outline the ideal institutional requirements needed for effective use of extracorporeal
Cord Blood Erythropoietin and Markers of Fetal Hypoxia
 July 21, 2011 By NeedsFixing [1] To investigating the relationship between cord blood erythropoietin and clinical markers of fetal hypoxia. Abstract Objective: To investigating the relationship between
July 21, 2011 By NeedsFixing [1] To investigating the relationship between cord blood erythropoietin and clinical markers of fetal hypoxia. Abstract Objective: To investigating the relationship between
Functions of the Brain
 Objectives 0 Participants will be able to identify 4 characteristics of a healthy brain. 0 Participants will be able to state the functions of the brain. 0 Participants will be able to identify 3 types
Objectives 0 Participants will be able to identify 4 characteristics of a healthy brain. 0 Participants will be able to state the functions of the brain. 0 Participants will be able to identify 3 types
Delayed Cord Clamping
 ICEA Position Paper Delayed Cord Clamping Position The International Childbirth Education Association recognizes that the first minutes after birth are crucial to both mother and newborn. Optimal care
ICEA Position Paper Delayed Cord Clamping Position The International Childbirth Education Association recognizes that the first minutes after birth are crucial to both mother and newborn. Optimal care
Neonatal Intensive Care Unit (NICU)
") Neonatal Intensive Care Unit (NICU) Integrated Care for Newborns with Critical or Special Needs startstrongbaby.org A World Leader in Neonatal Research and Care Innovation As a birthplace of modern neonatology
Neonatal Intensive Care Unit (NICU) Integrated Care for Newborns with Critical or Special Needs startstrongbaby.org A World Leader in Neonatal Research and Care Innovation As a birthplace of modern neonatology
APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES
 APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES The critical care nurse practitioner orientation is an individualized process based on one s previous experiences and should
APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES The critical care nurse practitioner orientation is an individualized process based on one s previous experiences and should
ST. ROSE HOSPITAL EMERGENCY SERVICES THERAPEUTIC HYPOTHERMIA AFTER CARDIAC ARREST PROTOCOL PURPOSE
 PURPOSE To outline the management of therapeutic hypothermia for the patient following cardiac arrest. LEVEL SUPPORTIVE DATA EFFECTS OF THERAPEUTIC HYPOTHERMIA Interdependent. Requires MD order. Cardiac
PURPOSE To outline the management of therapeutic hypothermia for the patient following cardiac arrest. LEVEL SUPPORTIVE DATA EFFECTS OF THERAPEUTIC HYPOTHERMIA Interdependent. Requires MD order. Cardiac
GENERAL ADMISSION CRITERIA INPATIENT REHABILITATION PROGRAMS
 Originator: Case Management Original Date: 9/94 Review/Revision: 6/96, 2/98, 1/01, 4/02, 8/04, 3/06, 03/10, 3/11, 3/13 Stakeholders: Case Management, Medical Staff, Nursing, Inpatient Therapy GENERAL ADMISSION
Originator: Case Management Original Date: 9/94 Review/Revision: 6/96, 2/98, 1/01, 4/02, 8/04, 3/06, 03/10, 3/11, 3/13 Stakeholders: Case Management, Medical Staff, Nursing, Inpatient Therapy GENERAL ADMISSION
2016 CODING FOR FETAL ALCOHOL SPECTRUM DISORDERS
 2016 CODING FOR FETAL ALCOHOL SPECTRUM DISORDERS Listed below are the most commonly used codes applicable to FASD patient care. Code Description ICD-10-CM Primary Diagnosis P04.3 Newborn (suspected to
2016 CODING FOR FETAL ALCOHOL SPECTRUM DISORDERS Listed below are the most commonly used codes applicable to FASD patient care. Code Description ICD-10-CM Primary Diagnosis P04.3 Newborn (suspected to
Clinical Medical Policy Outpatient Rehab Therapies (PT & OT) for Members With Special Needs
 for Members With Special Needs") Benefit Coverage Rehabilitative services, (PT, OT,) are covered for members with neurodevelopmental disorders when recommended by a medical provider to address a specific condition, deficit, or dysfunction,
Benefit Coverage Rehabilitative services, (PT, OT,) are covered for members with neurodevelopmental disorders when recommended by a medical provider to address a specific condition, deficit, or dysfunction,
2014 Neurologic Physical Therapy Professional Education Consortium Webinar Course Descriptions and Objectives
 Descriptions and Neuroplasticity Health care providers are facing greater time restrictions to render services to the individual with neurological dysfunction. However, the scientific community has recognized
Descriptions and Neuroplasticity Health care providers are facing greater time restrictions to render services to the individual with neurological dysfunction. However, the scientific community has recognized
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Title: Routine Screening of Neonates Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 6
NEONATAL CLINICAL PRACTICE GUIDELINE Title: Routine Screening of Neonates Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 6
A Gift for life. HTA Licence No. 22653
 A Gift for life HTA Licence No. 22653 2 3 the best possible gift for your new born child. 4 6 8 9 10 12 14 16 19 what is cord blood current treatments services contents properties for treatment process
A Gift for life HTA Licence No. 22653 2 3 the best possible gift for your new born child. 4 6 8 9 10 12 14 16 19 what is cord blood current treatments services contents properties for treatment process
Transmittal 55 Date: MAY 5, 2006. SUBJECT: Changes Conforming to CR3648 for Therapy Services
 CMS Manual System Pub 100-03 Medicare National Coverage Determinations Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 55 Date: MAY 5, 2006 Change
CMS Manual System Pub 100-03 Medicare National Coverage Determinations Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 55 Date: MAY 5, 2006 Change
Corporate Medical Policy Cord Blood as a Source of Stem Cells
 Corporate Medical Policy Cord Blood as a Source of Stem Cells File Name: Origination: Last CAP Review: Next CAP Review: Last Review cord_blood_as_a_source_of_stem_cells 2/2001 3/2015 3/2016 3/2015 Description
Corporate Medical Policy Cord Blood as a Source of Stem Cells File Name: Origination: Last CAP Review: Next CAP Review: Last Review cord_blood_as_a_source_of_stem_cells 2/2001 3/2015 3/2016 3/2015 Description
5/30/2014 OBJECTIVES THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM. Disclosure
 THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM Ona Fofah, MD FAAP Assistant Professor of Pediatrics Director, Division of Neonatology Department of Pediatrics Rutgers- NJMS, Newark OBJECTIVES
THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM Ona Fofah, MD FAAP Assistant Professor of Pediatrics Director, Division of Neonatology Department of Pediatrics Rutgers- NJMS, Newark OBJECTIVES
Cerebral Palsy: Intervention Methods for Young Children. Emma Zercher. San Francisco State University
 RUNNING HEAD: Cerebral Palsy & Intervention Methods Cerebral Palsy & Intervention Methods, 1 Cerebral Palsy: Intervention Methods for Young Children Emma Zercher San Francisco State University May 21,
RUNNING HEAD: Cerebral Palsy & Intervention Methods Cerebral Palsy & Intervention Methods, 1 Cerebral Palsy: Intervention Methods for Young Children Emma Zercher San Francisco State University May 21,
KING FAISAL SPECIALIST HOSPITAL AND RESEARCH CENTRE (GEN. ORG.) NURSING AFFAIRS. Scope of Service PEDIATRIC INTENSIVE CARE UNIT (PICU)
 NURSING AFFAIRS. Scope of Service PEDIATRIC INTENSIVE CARE UNIT (PICU)") PICU-Jan.2012 Page 1 of 7 Number of Beds: 18 Nurse Patient Ratio: 1:1-2 : The Pediatric Intensive Care Unit (PICU) provides 24 hour intensive nursing care for patients aged neonate through adolescence.
PICU-Jan.2012 Page 1 of 7 Number of Beds: 18 Nurse Patient Ratio: 1:1-2 : The Pediatric Intensive Care Unit (PICU) provides 24 hour intensive nursing care for patients aged neonate through adolescence.
Screening for Critical Congenital Heart Disease in the Apparently Healthy Newborn
 Screening for Critical Congenital Heart Disease in the Apparently Healthy Newborn A presentation of Texas Pulse Oximetry Project: A Joint Educational Initiative of The University of Texas Health Science
Screening for Critical Congenital Heart Disease in the Apparently Healthy Newborn A presentation of Texas Pulse Oximetry Project: A Joint Educational Initiative of The University of Texas Health Science
acbis Chapter 1: Overview of Brain Injury
 acbis Academy for the Certification of Brain Injury Specialists Certification Exam Preparation Course Chapter 1: Overview of Brain Injury Module Objectives Describe the incidence, prevalence and epidemiology
acbis Academy for the Certification of Brain Injury Specialists Certification Exam Preparation Course Chapter 1: Overview of Brain Injury Module Objectives Describe the incidence, prevalence and epidemiology
6.0 Management of Head Injuries for Maxillofacial SHOs
 6.0 Management of Head Injuries for Maxillofacial SHOs As a Maxillofacial SHO you are not required to manage established head injury, however an awareness of the process is essential when dealing with
6.0 Management of Head Injuries for Maxillofacial SHOs As a Maxillofacial SHO you are not required to manage established head injury, however an awareness of the process is essential when dealing with
What Is an Arteriovenous Malformation (AVM)?
?") What Is an Arteriovenous Malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair 1 What
What Is an Arteriovenous Malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair 1 What