Nebraska Medicaid Annual Report
|
|
|
- Eleanore Bailey
- 10 years ago
- Views:
Transcription
1 Division of Medicaid & Long-Term Care Nebraska Medicaid Annual Report December 1, 2013 Prepared in Accordance with Neb. Rev. Stat (4) Vivianne M. Chaumont, Director Division of Medicaid & Long-Term Care Department of Health and Human Services

2 September 15, 2013 We are pleased to present the Medicaid Annual Report for State Fiscal Year The Children s Health Insurance Program, CHIP, which Nebraska administers as a Medicaid expansion and a separate standalone program, is included in the Report. In SFY 2013, Nebraska Medicaid s expenditures of $1.8 billion accounted for 18.3% of total state budget. While the number of average monthly eligible persons under Medicaid rose modestly in SFY 2013, 1.3% to 240,639, a multi-year cycle of increased numbers of eligible persons and the national economic downturn have posed significant challenges for management of the Medicaid program. These pressures underline the importance of ongoing efforts to control Medicaid costs, and emphasize the importance of the Medicaid Reform efforts begun under the Legislature s mandate in As outlined in this report, the Division of Medicaid and Long-Term Care has undertaken a number of projects and initiatives in the past year aimed at increasing efficiency and decreasing costs. Many of these efforts involve increasing the use of technology to support services provision, operations, and oversight. State legislation and new federal requirements have also resulted in numerous projects, most with the same target of better fiscal management and more efficient service provision. This report offers a window into the ongoing work of the Division, highlighting the year s major initiatives, describing the larger projects for the year ahead, and detailing the persons served and services provided through the program. The Medicaid Reform Council approved the Medicaid Annual Report for State Fiscal Year 2013 at its September 26, 2013 meeting. Sincerely, Vivianne M. Chaumont, Director Division of Medicaid & Long-Term Care Department of Health and Human Services

3 Helping People Live Better Lives An Equal Opportunity/Affirmative Action Employer printed with soy ink on recycled paper Nebraska Medicaid Annual Report Neb. Rev. Stat (4) I. Introduction.. 1 II. Discussion.1 A. Eligible Clients. 1 B. Covered Services.. 4 C. Provider Reimbursement 11 D. Program Trends and Projections 12 E. SFY 2013 Initiatives.. 15 F. SFY 2014 Projects. 22 III. Conclusion. 24

4 I. INTRODUCTION Medicaid is a public health insurance program that provides coverage for low-income individuals. Originally enacted in 1965 under Title XIX of the Social Security Act, Medicaid is an entitlement program (a program which guarantees benefits to anyone who meets the qualifications) which covers a low-income population including seniors, children and individuals with disabilities. State Medicaid programs are administered by the states with oversight from the Centers for Medicare and Medicaid Services (CMS) through the federal Department of Health and Human Services (HHS). Every state outlines the eligibility, benefits, provider payments, and service delivery systems of its specific Medicaid program within broad guidelines set by the federal government. Eligibility and benefit packages can vary widely from state to state. The Children s Health Insurance Program (CHIP) was created in 1997 under Title XXI of the Social Security Act, and was designed to offer insurance coverage for low-income children whose family income is above Medicaid limits. States administer their CHIP programs in a variety of different ways. In Nebraska, CHIP has been operated as a Medicaid expansion meaning that CHIP, with a few exceptions, operates using the same delivery system, benefit package and regulations as Medicaid. Effective July 19, 2012, Nebraska implanted a separate CHIP program which added prenatal and delivery services for the unborn children of certain women who do not meet Medicaid eligibility criteria. Medicaid and CHIP are financed jointly by the federal government and state governments, with the federal government matching state spending at a rate known as the Federal Match Assistance Percentage, or FMAP, which varies from state to state. FMAP is based on each state s per capita income relative to the national average and is highest in the poorest states, varying from 50% to 73%. Nebraska s FMAP in FFY 2013 was 55.76% for Medicaid and for CHIP, 69.03%. A. ELIGIBLE CLIENTS II. DISCUSSION Nebraska Medicaid provides coverage for individuals in the following eligibility categories: Children, Aged, Blind & Disabled and Aid to Dependent Children (ADC) Adults. Additional eligibility factors vary by group and include income, resources and employment status. Nebraska s CHIP, sometimes called Kids Connection, has operated as a Medicaid expansion program since May of 1998 and provides health coverage for eligible uninsured children if they have income at or below 200 percent of the federal poverty level (FPL) and are not eligible for Medicaid. On July 19, 2012, Nebraska implemented a separate CHIP program to provide coverage to the unborn children of women who are not otherwise eligible for Medicaid, have no creditable insurance and meet financial requirements. 1
 through the federal Department of Health and Human Services (HHS).")
5 ELIGIBLE POPULATIONS FIGURE 1 NEBRASKA MEDICAID AND CHIP AVERAGE MONTHLY ELIGIBLE PERSONS BY CATEGORY Fiscal Year 2012 Total: 237,543 ADC Adults 31, % NEBRASKA MEDICAID AND CHIP AVERAGE MONTHLY ELIGIBLE PERSONS BY CATEGORY Fiscal Year 2013 Total: 240,639 ADC Adults 31, % Children 152, % Aged 17, % Children 154, % Aged 17, % Blind & Disabled 35, % Blind & Disabled 36, % FIGURE 2 NEBRASKA MEDICAID AND CHIP VENDOR EXPENDITURES BY ELIGIBILITY Fiscal Year 2012 Total: $1,602,347,345 Children $378,940, % ADC Adults $170,704, % Aged $341,670, % NEBRASKA MEDICAID AND CHIP VENDOR EXPENDITURES BY ELIGIBILITY Fiscal Year 2013 Total: $1,799,457,166 Children $488,051, % ADC Adults $134,708, % Aged $372,963, % Blind & Disabled $711,031, % Blind & Disabled $803,733, % 2

6 Figure 1 compares eligibility categories for State Fiscal Years (SFY) 2012 and The total increase in average monthly eligibles from SFY 2012 to SFY 2013 was 1.3%. The largest percentage increase was in the Blind & Disabled category, which grew 2.9%. Average monthly eligibles in the Children category grew by 1.2%. ADC Adults grew 0.2% and the Aged category grew by 1.3%. Figure 2 compares vendor expenditures by eligibility category for SFYs 2012 and Viewing Figures 1 and 2 together provides insight into the cost differences of different eligibility categories. While the Aged and Blind & Disabled represent 22.8% of clients, they account for 65.4% of expenditures. This is almost the exact opposite with children who account for 64.0% of clients but only 27.1% of expenditures. Figure 2 does not account for all Medicaid/CHIP expenditures, in part because some payments and refunds are not specific to a recipient or eligibility category. Examples of transactions not shown are drug rebates, payments made outside the Medicaid Management Information Systems (MMIS), and premium payments paid on behalf of persons eligible for Medicare. Client demographic data are not available for these expenditures. This means that some expenditures, particularly in the Aged and Blind & Disabled categories, are understated. For example, Medicare Part B and Part D premium payments for clients who are eligible for both Medicaid and Medicare, i.e. duals. These premium payments totaled $94,088,563 in SFY Prorating these expenditures between the Blind & Disabled and the Aged categories increases total expenditures in SFY 2013 for Blind & Disabled to 45.1% and to 22.0% for the Aged. There are several reasons for the expenditure change when comparing SFY 2012 to SFY The recertification of the Beatrice State Developmental Center (BSDC) Center allowing it, once again, to bill as a Medicaid provider contributed to the increase. Rates were increased by 1.54% effective July 1, Physical health managed care expanded to the remaining 83 counties in July Because Medicaid providers could bill up to one year after the date the service, in SFY 13, Medicaid was still making payments for services provided prior to the expansion of Managed Care at the same time per member per month payments were made to the managed care companies. Additionally, the billing issues experienced by providers as well as the payment issues experienced by the Department as a result of the implementation of 5010 in SFY 2012 resulted in the delay of payments from SFY 2012 to SFY 2013, thereby possibly overstating SFY 2013 expenditures. Categories expected to decrease as a result of Managed Care decreased. These categories are Outpatient Health, Physicians Services and Inpatient Hospital. Additionally, Pharmacy decreased. Even though pharmacy benefits are not in managed care, managed care assignment of Primary Care Providers and care coordination can result in a decrease in pharmacy costs. The Disabled category also experienced a substantial increase in home and community-based services for persons with developmental disabilities. The Aged category was the third largest growing eligibility category with expenditures increasing 9.2% ($31,292,790) from $341,670,694 in SFY 2012 to $372,963,484 in SFY The largest increase was in Intermediate Care Facilities for the Developmentally Disabled (ICF/DD) 82.8% ($4,332,481) from SFY 2012 to SFY ADC Adults declined 21.1% ($40,487,442) in expenditures from $170,704,198 in SFY 2012 to $134,708,628 in SFY The largest decrease 3

7 in expenditures was Inpatient Hospital (53.9%) at a $14,484,179 decrease from SFY 2012 to SFY B. COVERED SERVICES Federal Medicaid statutes mandate states to provide certain services and allow states the option of providing a choice of others. The Nebraska Medical Assistance Act delineates the mandatory and optional services available to Medicaid and CHIP recipients in Nebraska. Figure 3 Federal Medicaid Mandatory and Optional Services Covered in Nebraska Neb. Rev. Stat Mandatory Services Inpatient and outpatient hospital services Laboratory and x-ray services Nursing facility services Home health services Nursing services Clinic services Physician services Medical and surgical services of a dentist Nurse practitioner services Nurse midwife services Pregnancy-related services Medical supplies Early and periodic screening and diagnosis treatment (EPSDT) services for children Nebraska Optional Services Prescribed drugs Intermediate care facilities for the Developmentally Disabled (ICF/DD) Home and community-based services for aged persons and persons with disabilities Dental services Rehabilitation services Personal care services Durable medical equipment Medical transportation services Vision-related services Speech therapy services Physical therapy services Chiropractic services Occupational therapy services Optometric services Podiatric services Hospice services Mental health and substance use disorder services Hearing screening services for newborn and infant children School-based administrative services 4

8 VENDOR EXPENDITURES Figure 4 shows how the $1.8 billion in Medicaid/CHIP expenditures to vendors are distributed by vendor type. Total vendor payments increased $197,109,823 or 12.3% from SFY 2012 to SFY However, implementation of new billing processes related to federal HIPAA 5010 requirements resulted in delays in billing and payment which caused SFY 2012 expenditures to be understated. SFY 2013 expenditures reflect the resolution of the billings issues resulting from the 5010 implementation. Additionally, with the move to statewide Managed Care, there were payments for services from SFY 2012 at the same time as capitation payments for SFY Figure 4 5

9 A significant shift in the management and administration of Medicaid services has taken place over the past several years with the growth of managed care. Full risk managed care is a health care delivery system where Managed Care Organizations (MCOs) are contracted to operate a health plan that authorizes, arranges, provides, and pays for the delivery of services to enrolled clients. Managed care offers an opportunity to assure access to a primary care provider, emphasizes preventive care, and encourages the appropriate utilization of services in the most costeffective setting. Nebraska Medicaid has utilized managed care in three urban counties since 1995, and added the seven surrounding counties in August As of July 1, 2012, Nebraska s managed care program was further expanded to statewide managed care for physical health services. This move is projected to result in additional savings in Medicaid and CHIP over time. On September 1, 2013, Nebraska shifted its behavioral health program to an at-risk model. Figure 5 shows vendor expenditures from SFY 2012 and SFY 2013 side by side. Expanding fullrisk capitated physical health managed care to cover the remaining 83 counties explains the decrease in these services and the corresponding increase in the Managed Care Capitations. In addition, implementation of new billing processes related to federal HIPAA 5010 requirements resulted in delays in billing and payment which caused SFY 2012 expenditures to be understated. SFY 2013 expenditures reflect the resolution of the billings issues resulting from the 5010 implementation. Even after taking into account billing issues related to the implementation of HIPAA 5010 transactions and the full provider revalidation process, which artificially increased SFY 2013 expenditures, it appears that the Managed Care program is controlling the costs of Medicaid and CHIP. 6

10 Figure 5 7

11 Figure 6 $1,799,457,166 Vendor Payments $42,013,107 Disproportionate Share Hospital/Rate Adjustments $43,056,973 Medicare Premiums $ 5,049,284 Intergovernmental Transfer (IGT) $49,924,887 Other Payments (Managed Care, Transportation, Federal Insurance Contributions Act taxes, AssistTech, Upper Limit Pmts) ($104,243,944) Rebates/Refunds ($137,078,926) General Funds Paid in Other Budget Programs $51,031,590 Phased Down Contribution $1,749,210,137 Net Medicaid and CHIP Expenditures Not all Medicaid/CHIP expenditures are captured in Figure 4. Medicaid/CHIP vendor expenditures totaled $1,799,457,166 in SFY The net program expenditures for this same time period totaled $1,749,210,137. Several of these manual transactions are highlighted below. Drug rebates refer to reimbursements made by pharmaceutical companies to Medicaid/CHIP that bring down individual drug cost to a more competitive or similar price that is being offered to other large drug payers, such as insurance companies. In SFY 2013, Medicaid received $93.2 million in Drug Rebates, an increase of 13.9% compared to the $81.8 million received in SFY Medicaid pays the Medicare Part B premium for clients that are dually eligible for Medicare and Medicaid. In SFY 2013, Medicaid paid $43,056,973 for Medicare Premiums, a 0.7% decrease from the $43,376,690 paid in SFY Part B premium amounts were $ in calendar year (CY) 2011, $99.90 in CY 2012, and $ in CY CY 2014 premium amounts are expected to remain the same as CY Disproportionate Share Hospital (DSH) payments are an add-on to hospitals that serve a high number of Medicaid and uninsured patients. In SFY 2013, Medicaid paid $42,013,107 through the DSH program, a 16.4% decrease compared to $50,240,316 paid in SFY Intergovernmental Transfers are payments made to public providers that have 40% or higher Medicaid utilization and whose direct nursing or direct support costs have exceeded the Medicaid maximum allowable rate. In SFY 2013, Medicaid paid $5,049,284 for Intergovernmental Transfers, an increase of 15.7% from the $4,363,355 paid in SFY Part D Clawback payments are made to CMS to cover the State s share of prescription drugs for persons dually eligible for both Medicare and Medicaid. In SFY 2013, Clawback payments totaled $51,031,590, a 9.3% increase from the $46,673,462 paid in SFY The Clawback payment 8

12 amount per person is based on a complex formula that takes into account the cost of drugs and the Federal Medical Assistance Percentage (FMAP). Nebraska s FMAP has been steadily decreasing since FFY LONG-TERM CARE SERVICES Long-Term Care Services support individuals with chronic or ongoing health needs related to age or disability. Services are geared to multiple levels of client need ranging from limited assistance with activities of daily living to complex nursing interventions. Assistance can be offered in a variety of settings from care in an individual s home, to care in small group settings with community supports, to care in a nursing facility or intermediate care facility for persons with mental retardation. In general, home and community based care is less expensive and offers greater independence for the consumer than facility based care. For these reasons, state and federal initiatives encourage the development of care options in the community as an alternative to institutional care. Efforts to encourage home and community based alternatives to facility based care are resulting in a gradual rebalancing of long-term care expenditures. 9

13 Figure 7 SFY2013 Medicaid Expenditures for Long-Term Care Services SFY2008 Medicaid Expenditures for Long-Term Care Services 10

14 C. PROVIDER REIMBURSEMENT Medicaid purchases health services for clients on a fee for service basis or, increasingly, by paying premiums to managed care plans which coordinate provider networks and provider reimbursements. The Nebraska Medicaid Program uses different methodologies to reimburse different Medicaid services. Practitioner, laboratory, and radiology services are reimbursed according to a fee schedule. Prescription drugs are reimbursed according to a discounted product cost calculation plus a pharmacy dispensing fee. Inpatient Hospital services are reimbursed based on a prospective system using either a diagnosis related group (DRG) or per diem rate. Critical Access Hospitals are reimbursed a per diem based on reasonable cost of providing the services. Federally Qualified Health Centers (FQHCs) are reimbursed on a prospective payment system. Rural Health Clinics (RHCs) are reimbursed cost or a prospective rate depending on whether they are independent or provider-based. Outpatient Hospital reimbursement is based on a percentage of the submitted charges. Nursing Facilities are reimbursed a daily rate based on facility cost and client level of care. Intermediate Care Facilities for the Developmentally Disabled (ICF/DDs) are reimbursed on a per diem rate based on a cost model. Home and Community Based Waiver services, including Assisted Living costs, are reimbursed at reasonable fees as determined by Medicaid. In many states, budget and enrollment pressures on Medicaid have led to cuts in provider rates. Nebraska Medicaid providers have received increased rates every year from 2005 through Effective July 1, 2011, rates for all provider types, excepting primary care services, were decreased by 2.5%. Effective July 1, 2012, the rates that were decreased were increased 1.54%. Effective July 1, 2013, Medicaid rates were increased by 2.25% except for primary care codes which were increased, as a result of implementation of the Affordable Care Act, to 100% of Medicare rates effective January 1,

15 D. PROGRAM TRENDS AND PROJECTIONS Figure Nebraska Medicaid and CHIP Average Monthly Eligibles SFY Actual and SFY Projected Based on Current Economic Predictions (includes Federal Healthcare Reform) , , , , , , FY10 FY11 FY12 FY13 FY14(Proj)* FY15(Proj) *ACA will be implemented Growth in Medicaid/CHIP eligibility was moderate from SFY 2006 through SFY Nebraska experienced a significant increase in eligibles the latter half of SFY 2009 that continued until through SFY 2011, with an increase from SFY 2010 to SFY 2011 of 4.9%. The increase from SFY 2011 to SFY 2012 was a modest 0.9% with the increase attributed in part to the statutory expansion of the Children s Health Insurance Program (CHIP) eligibility to 200% FPL and to the national economy. SFY 2013 had an increase of 1.3% from SFY Based on historical trends and on the findings from the Milliman Report regarding implementation of the Affordable Care Act (ACA) on January 1, 2014, average monthly eligibles in SFY 2014 are expected to increase by 7.7%. Average monthly eligibles in SFY 2015 are expected to increase 9.2% from SFY 2014 since SFY 2015 will have a full year of ACA implementation. 12

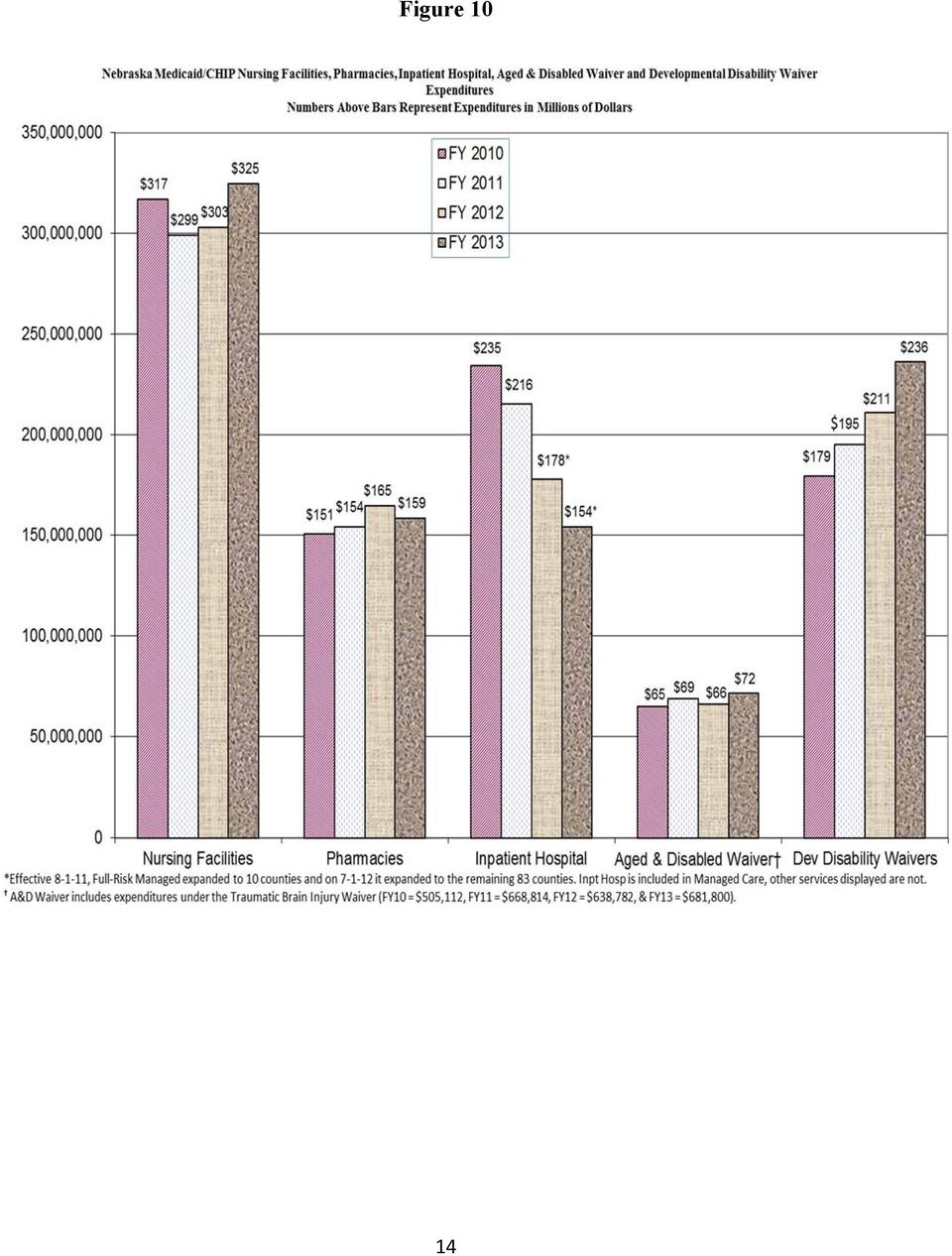
16 Figure 9 The average monthly cost per eligible (Figure 9) increased 6.4% overall from SFY 2012 to SFY The largest cost per eligible increase was in the Blind & Disabled category, which increased by 9.8%. The Aged category increased by 7.8%. The Children category increased by 27.3% and the ADC Adult category decreased by 27.3%. As noted previously, decreases in expenditures in the Adult categories appear to be related, in large part, to the increasing inclusion of those clients in managed care. The top four vendor expenditure categories in Medicaid/CHIP (excluding managed care capitation payments) are nursing facilities, pharmacies, inpatient hospital and home and community services. The home and community service category consists of home health, personal assistance services and waiver services, including assisted living. Figure 9 (previous page) reflects the trends in these categories from SFY 2010 through SFY The drop in Inpatient Hospitalization expenditures reflects inclusion under managed care. 13
 are nursing facilities, pharmacies, inpatient hospital and home and community services.")
17 Figure 10 14
18 E. SFY 2013 INITIATIVES Highlighted below are some of the major projects during SFY Efficiencies in Billing for Nursing Facility Providers Prior to 2013, the turnaround document was eliminated and nursing home providers began billing on a standard UB04 claim form. In April 2013, Medicaid eliminated the requirement for prior authorizations for nursing facility services. Currently providers are enrolling to test a web-based case-mix reporting system for nursing facilities. This enables them to see the status of their resident assessments in terms of timeliness, errors, reimbursement, accurate billing, resident data, and not having their claims rejected. It will also eliminate the monthly mailing of reports to facilities. Durable Medical Equipment and Supplies for Clients in Nursing Facilities and ICF/DDs In May of 2011, CMS made Nebraska Medicaid aware of the need to correct the payment of durable medical equipment and supplies for clients residing in nursing facilities and ICF/DDs. Medicaid established a transition plan whereby payments formerly made to Durable Medical Equipment (DME) suppliers will instead be made to the facilities. Medicaid developed new reimbursement methodology to comply with federal requirements and notified the DME providers and the facilities of these changes. The new reimbursement methodology was implemented on August 1, Electronic Health Record (EHR) Incentive Payment Program This program was established under the Federal Health Information Technology for Economic and Clinical Health (HITECH) Act which is a part of the American Reinvestment and Recovery Act (ARRA) of The Medicare EHR Incentive Program is administered by CMS and the Medicaid EHR Incentive Program is administered by the states. For providers, the payments can total a little over $63,000 over 6 years. Hospital payments, made over three years, are determined by a number of factors, beginning with a base rate of $2 million which can be increased or decreased by discharge numbers and growth rate trends. Incentive payments are 100% federally funded and administration of the program by Nebraska Medicaid is matched with 90% federal funding. Eligible professionals and hospitals must adopt, implement, upgrade or demonstrate meaningful use of a certified EHR system. Nebraska launched the EHR Incentive Program on May 7, As of June 30, 2013, there were 461 eligible professionals and 62 hospitals participating in the program and nearly $32 million has been paid to Nebraska providers. HITECH funds this program through Enhanced Provider Enrollment and Screening Requirement The ACA included enhanced provider screening and enrollment requirements for all Medicaid providers including those that order, refer, and prescribe services. Nebraska Medicaid has implemented many of these requirements and will be issuing a request for proposals to contract with a vendor for application and fee collection, database screening, and site visits. Additional 15

19 guidance about mandatory background checks is pending from the Centers for Medicare and Medicaid Services (CMS). Nebraska Medicaid will implement those requirements when available. Medicaid Patient-Centered Medical Home Pilot Medicaid implemented the Medicaid Patient-Centered Medical Home Pilot in February The pilot concluded in February 2013 and is currently being evaluated for improved health care access, improved health outcomes for patients, Medicaid cost containment, patient and provider satisfaction. Two practices participated in the pilot: Kearney Clinic, Kearney (20 providers) and Plum Creek Medical Group, Lexington (10 providers). Both practices received a per-memberper-month (PMPM) payment based on meeting Tier 1 or Tier 2 standards. The practices received funding for a Care Coordinator staff position and DHHS provided comprehensive technical assistance to work with the clinics as they transformed into medical homes. An evaluation of the pilot for improved health care access, improved health outcomes for patients, Medicaid cost containment, patient and provider satisfaction is currently being finalized and a report on the pilot is due in June Money Follows the Person (MFP) Money Follows the Person (MFP) is a rebalancing initiative that was made possible by a grant from the Centers for Medicare and Medicaid Services (CMS). This grant is designed to assist individuals who are institutionalized in in-patient facilities like nursing facilities, hospitals, and intermediate care facilities transition to their homes and communities. Transition assistance may consist of community resource development, applying for financial assistance, coordinating providers, and facilitating communication with the individual and their family in regard to transition options. Nebraska s MFP transitioned 97 individuals from institutional care to community-based living in SFY 2013, 297 since June Timely Filing Requirements Effective September 1, 2013, MLTC will be changing the timely filing requirements for Medicaid claims from the existing 12 months to six months (180 days). Data analysis revealed that in recent years nearly 85% of current providers have already been filing claims within 180 days of the date of services provided, so this change is not expected to adversely impact the normal course of business for providers. Ultimately, timelier filing will result in a faster rate of processing and payment for providers. Exceptions to the current timely filing requirements, for example, retroactive eligibility, Medicare denials, casualty insurance, and health insurance, remain unchanged. Full Risk Behavioral Health Managed Care An RFP for a Managed Care Organization to provide these services was released in the fall of Magellan was awarded the contract and implementation was effective September 1, This change will result in cost-savings and will address the compliance issues related to IMDs. 16
 and Plum Creek Medical Group, Lexington (10 providers).")
20 ICD-10 International Classification of Diseases Version 10 The federal Department of Health and Human Services mandated transition from the International Classification of Diseases version 9 (ICD-9) to ICD-10 for all Health Insurance Portability and Accountability Act of 1996 (HIPAA) covered entities (health care providers, clearinghouses and payers). Working in collaboration with the Division of Information & Technology (IS&T), Medicaid Management Information System (MMIS) requirements have been developed. Coding and remediation of policy, forms and contracts has begun. External interface testing with Trading Partners is planned to begin April, 2014, and continue through implementation on October 1, Communication and provider outreach activities continue. Primary Care Services at Medicare Rates Effective January 1, 2013, Medicaid payment rates for primary care services furnished by certain physicians in CYs 2013 and 2014 cannot be less than the Medicare rates. This minimum payment level applies to specified primary care services furnished by a physician with a specialty designation of family medicine, general internal medicine, or pediatric medicine. Methodology for Fee-For-Service (FFS) payments and for managed care capitation rates were approved by CMS. Effective September 23, 2013, the department will implement all program updates related to the enhanced rates for claims dates of service January 1, 2013 and after. Previously processed claims will be auto-adjusted to pay at the enhanced rates. Any new claims eligible for the enhanced rate, received September 23, 2013 and after will price correctly the first time. Diagnosis Related Group (DRG) Grouper Software Work on adoption of a new Diagnosis Related Group (DRG) grouper software for Medicaid use began in SFY 2012 and continued into SFY Medicaid contracted for the purpose of reviewing options and recommending and/or developing a DRG grouper software. Effective July 1, 2014, Nebraska will implement the All Patient Refined Diagnosis Related Grouper (APR- DRG) utilizing national relative weights and average length of stay (ALOS). Program of All-Inclusive Care for the Elderly (PACE) Programs of All-Inclusive Care for the Elderly provide comprehensive, coordinated health care services for voluntarily-enrolled individuals age 55 and older who meet nursing facility level of care criteria. Immanuel Pathways, located in north Omaha, became Nebraska s first PACE provider when its doors opened May 1, This new option offers another alternative along the continuum of available long-term care services. Services tailored to each individual s needs are provided where the participant lives, at the clinic-licensed center, or in another setting. The array of services is provided by Immanuel Pathways and their provider network using Medicaid, Medicare, and/or participant funds issued as a capitated monthly rate. As of September 1, 2013, Immanuel Pathways had enrolled 27 participants. Traumatic Brain Injury 1915(c) Waiver The Traumatic Brain Injury (TBI) Waiver provides specialized assisted living services to persons age who have a diagnosis of TBI and meet nursing facility level of care criteria. This waiver, implemented in 2000, has only one provider, Quality Living in Omaha, and serves a maximum of 17

21 40 persons. Periodic renewal of home and community-based waivers is required. The TBI Waiver renewal was approved for October 1, Recovery Audit Contractor (RAC) Nebraska Medicaid implemented the Nebraska Medicaid Recovery Audit Contractor program on November 30, 2012, by signing a contract with HMS. The Medicaid RAC objectives are to reduce erroneous payments, identify and recover overpayments, and identify underpayments in the Medicaid program. As allowed by state and federal law, the Nebraska Medicaid RAC contractor will be paid on a contingency basis from actual amounts recovered. The implementation has included establishing correspondence templates, reviewing steps, and data sharing. The vendor, HMS, will soon establish a Nebraska Medicaid specific website and will begin provider education. It is anticipated that the first record requests will be sent by the end of the year. Additional Program Integrity Initiatives Medicaid also participates in a variety of state and federal initiatives: The Medi-Medi Project CMS contracts with vendors to aggregate Medicare and Medicaid claims data to identify fraud, waste, or abuse by providers across both programs. Nebraska is participating in this project. Audits of New Initiatives Both the Electronic Health Record (EHR) Incentive Payment Program and the Medicaid Payment for Primary Care Services at Medicare Rates have specific auditing requirements that are completed by Program Integrity staff. Payment Suspensions Due to Credible Allegations of Fraud The ACA requires that Medicaid programs protect state and federal funds by suspending provider payments when there is a credible allegation of fraud against the provider. There are specific tracking and notifications that must be followed. Health Information Exchange (HIE) NeHII (Nebraska Health Information Initiative) is the lead Health Information Exchange (HIE) in Nebraska and has the capability to serve any health care provider. Another HIE, Electronic Behavioral Health Information Network (ebhin) focuses on the behavioral health care providers. These are the two health information exchanges in Nebraska which were established through the ehealth Council. The main purpose of an HIE is to exchange laboratory, radiology, medication history, clinical documentation, public health information and other medical data among Nebraska providers and hospitals. Nebraska Medicaid has recently submitted a funding request to CMS on behalf of NeHII and ebhin. If approved, this funding will allow the HIE organizations to assist Medicaid providers in achieving meaningful use of their Electronic Health Record (EHR) technology which is one of the qualifications for the EHR Incentive Program. Several of the meaningful use measures relate to the exchange of key medical information. The funding request is pending CMS approval at this time. The federal funding would be at 90% the total funds requested were just over $4 million. 18
22 MITA Medicaid IT Architecture The Medicaid IT Architecture (MITA) is a CMS initiative to establish national guidelines for technologies and processes that improve program administration for the State Medicaid Enterprise. All technology-related funding requests from Medicaid to CMS must now reference MITA status and explain how MITA maturity will be enhanced through the funded work. In SFY 2012, the Division completed a formal MITA 2.0 State Self-Assessment (SS-A) describing the extent to which the current Medicaid Management Information System (MMIS) aligns with the MITA framework and how requested changes will advance the transformation into the architecture. In March, 2012, CMS published the MITA 3.0 Framework which is an updated collection of principles, models, and guidelines. CMS requires each state to complete a MITA 3.0 SS-A in order to obtain enhanced federal funding for its Medicaid program. The Division is working on the MITA 3.0 SS-A. Administrative Simplification All HIPAA covered entities, including providers, clearinghouses and payers, are required to comply with the Affordable Care Act (ACA) requirements to implement the Council for Affordable Quality Healthcare (CAQH) Committee on Operating Rules for Information Exchange (CORE). The CORE Operating Rules are further standardization of the HIPAA Standard Electronic Transactions version 5010, implemented January 1, Planning and implementation of the first CORE Phases began in 2013 with Phase I and Phase II which impact the eligibility for a health plan (270/271) and the health care claim status (276/277) transactions. This project is known as Medicaid AS-ECS (Administrative Simplification Eligibility and Claim Status). A Request for Proposal to procure a solution to the real-time requirements was released in May Managed Care Waiver Nebraska Medicaid submitted to the Centers for Medicare and Medicaid (CMS) an amendment to the 1915(b) waiver in order to allow implementation of a full-risk behavioral health managed care program effective September 1, Health Insurance Premium Payment (HIPP) Program In SFY 2013, the Health Insurance Premium Payment Program underwent significant improvements. Efforts have been focused on ensuring strict compliance with 471 NAC 30, improvements in case management, and improvements in the gathering and retention of supporting documentation. As a result of the program s review of 100% of all current participants in the HIPP program, significant reductions in participation were made, ensuring that the program provides cost-savings for Medicaid. Additional controls were implemented to ensure the appropriateness of program expenditures, and to ensure the ongoing cost-effectiveness of program participants. Transition of Medicaid Eligibility Function In 2013, work began to move the eligibility determination for Medicaid and CHIP programs from the Division of Children and Family Services to the Division of Medicaid and Long-Term Care (MLTC). Based on the available data, 40% of the current workforce was transferred to MLTC on July 1,
23 In order to be accessible to the public, MLTC identified and secured additional office locations throughout the State of Nebraska. Additional MLTC staff was added to multiple offices statewide based on the space available. On July 1, 2103, the Lincoln and Lexington Customer Service Centers (CSC), as well as local office staff, were transitioned to MLTC for supervision. Effective October 1, Medicaid will have a separate phone numbers and processes to support Medicaid applicants and recipients. Implementation of ACA Eligibility Changes In July 2013, CMS released a final rule implementing several provisions of the ACA related to eligibility for Medicaid and the Children s Health Insurance Program (CHIP). In the process of updating Nebraska regulations to reflect applicable provisions of the ACA, Medicaid and CHIP eligibility regulations were reorganized and consolidated into Title 477. Process details were removed and placed in field process guides and an appendix to Title 477. The new Nebraska eligibility policy regulations will take effect January 1, The ACA requires the use of Modified Adjusted Gross Income (MAGI) as the income methodology for Medicaid and CHIP children, pregnant women and parents/caretaker relative groups. The Aged, Blind, and Disabled population will not be subject to MAGI or other eligibility changes under the ACA. States were required to convert their current financial eligibility income standards from net standards that incorporate current income disregards to an equivalent MAGI income standard. Throughout the year, Nebraska worked with an actuarial contractor to convert current income standards to the equivalent MAGI income standard. MLTC Quality Team The MLTC Quality Team was started in August 2012 with the core purpose of conducting surveys, analyzing data, developing and submitting reports based on CMS Core Quality Measures. The team has developed data reporting templates for use by Managed Care Organizations in reporting data and outcomes on quality measures and provided assistance to Managed Care Organizations in the implementation and measurement of Managed Care Quality Strategies. The team assists Managed Care Contract Managers in the monitoring and evaluation of Quality Performance Improvement Plans. In addition, the team is working on the implementation of the new version of T-MSIS federal reporting and the Health Information Exchange project. EQRO (External Quality Review Organization) Contract A Request for Proposal was issued for the purpose of selecting a qualified contractor to provide an annual external and independent review service. This is a component of the contract between Nebraska Medicaid and the Managed Care Organizations (MCOs) and Prepaid Inpatient Health Plan (PIHP) providing health care to Nebraska Medicaid clients enrolled in managed care. Enrollment Broker Contract 20
24 Enrollment Broker services, for clients eligible for enrollment in Nebraska Medicaid Managed Care and the Program of All-Inclusive Care for the Elderly (PACE), include client education of options for health plans, choice counseling, and all activities involved for a completed enrollment. The previous contract for enrollment broker services ended June 30, An RFP was issued to solicit proposals from qualified vendors. The contract was awarded to the incumbent, the Medicaid Enrollment Center Inc. Preferred Drug List An RFP was issued for the purpose of selecting a qualified contractor to provide services to support the Medicaid Pharmacy Program in maintaining a Preferred Drug List, participating in a multistate purchasing pool and obtaining supplemental drug rebates. The contract was awarded to the incumbent Magellan Medicaid Administration, Inc. Medicaid Upper Payment Limit Starting in 2013, CMS required states to submit upper payment limit (UPL) demonstrations on an annual basis. Previously, this information was collected or updated only when a state was proposing an amendment to a reimbursement methodology in its Medicaid state plan. CMS is now requiring that states submit UPL demonstrations for inpatient hospital services, outpatient hospital services, and nursing facilities. In 2014, and annually thereafter, states will be required to submit annual UPL demonstrations for the services listed above and clinics, physician services (for states that reimburse targeted physician supplemental payments), intermediate care facilities for the developmentally disabled (ICF/DD), private residential treatment facilities and institutes for mental disease (IMDs). This information must be submitted by the state prior to the start of the state fiscal year. An RFP has been issued to solicit proposals for qualified vendors to assist with these new requirements. National Correct Coding Initiative (NCCI) Nebraska Medicaid continues to implement all of the National Correct Coding Initiative (NCCI) edits as mandated as part of the Patient Protection & Affordable Care Act. CMS updates and adds to the edits quarterly. Recent additions to the edits address durable medical equipment, office visits and other physician services, and services only reimbursed by Medicaid. In fiscal year 2013, the edits led to a cost avoidance of $2,463,294. F. SFY2014 PROJECTS Many of the SFY 2013 projects detailed above will continue in SFY Managed Long-Term Services and Supports Work has begun on developing a statewide managed care program for the delivery of long-term care services and supports. Examples of long-term care services included in this initiative are nursing facility, personal assistance, home health, and those provided under Home & Community Based Services (HCBS) waivers such as home care/chore, respite, and assisted living. Goals of the program include the following: 21
25 Improve client health status and quality of life by better coordination of medical care, behavioral health care, and community-based services and supports. Promote client choice and use of the right services and supports at the right time in the right amount. Increase client access to responsive, quality services and supports. Use financial resources wisely to sustain Nebraska Medicaid. An advisory council is being formed to provide input into the design, planning, implementation and monitoring of the program. Town hall meetings are also being planned across the state to provide an opportunity for broader public input in the program design. The targeted implementation date is July Eligibility and Enrollment RFP and IV&V The Affordable Care Act (ACA) requires significant changes to state Medicaid eligibility and enrollment (E&E) systems. Nebraska's eligibility system could not meet the ACA requirements without significant investment and a complete rewrite. As a result, Nebraska is procuring a new Medicaid E&E system to meet ACA requirements. In FY 13, a major initiative was launched to plan for the Medicaid eligibility replacement system. Significant portions of the planning activities were to ensure the new system met requirements for enhanced 90/10 funding offered by CMS. The planning activities resulted in two RFPs. One is to procure an Enterprise Eligibility System (EES) and another for Independent Verification and Validation (IV&V) of the EES vendor. Awards are expected to be made for the IV&V and EES RFPs in the first half of FY 14 with implementation activities running through December Provider Eligibility and Enrollment An RFP is currently under internal and external review. Upon final approval, the RFP will be issued, and ultimately will result in the Medicaid contracting with an approved vendor for provider eligibility and enrollment services. Currently, a revision of the applicable Nebraska Medicaid rules is in process. American Dental Association (ADA) Claim Form 2012 Effective October 1, 2013, the Department will no longer accept the 1994, 1999, and 2002 versions of the American Dental Association (ADA) Claim Form. The 2006 ADA form will continue to be accepted only through December 31, Effective January 1, 2014, the 2012 ADA claim form will become the only hardcopy dental claim form accepted by the Department for prior authorizations and reimbursement of services. On or after January 1, 2014, any claims received utilizing the older versions of the ADA Claim Form will be returned to the provider. CMS 1500 Claim Form The National Uniform Claim Committee (NUCC) announced the final approval of the Version 02/ Health Insurance Claim Form (1500 Claim Form) that accommodates reporting needs 22
26 for ICD-10 and aligns with requirements in the Accredited Standards Committee X12 (ASC X12) Health Care Claim: Professional (837P) Version The NUCC is reviewing its initial proposed implementation timeline. The Department will announce its implementation timeline in the near future. Non-Emergency Medical Transportation RFP A Non-Emergency Medical Transportation RFP will be released in September The purpose of a new RFP is to enhance client transportation services and strengthen quality assurance measures for the provision of the services provided. An April 2014 implementation date is expected. Administrative Simplification All HIPAA covered entities, including providers, clearinghouses and payers, are required to comply with the Affordable Care Act (ACA) requirements to implement the Council for Affordable Quality Healthcare (CAQH) Committee on Operating Rules for Information Exchange (CORE). The CORE Operating Rules are further standardization of the HIPAA Standard Electronic Transactions version 5010, implemented January 1, Continuation of planning and implementing CORE Phase II and Phase III will continue in SFY 14. The CORE Phase III rules impact EFT (electronic fund transfers) and ERA (electronic remittance advice/835 transaction). Complete implementation of Phases I, II and III is expected in SFY 14. Utilization Review Contract Medicaid will be issuing an RFP to solicit bids for a contractor, certified as a Quality Improvement Organization (QIO), to manage a statewide quality and utilization control program for services provided to Nebraska Medicaid clients in Fee-For-Service (FFS) programs. The contractor will review and make determinations regarding prior authorization, continued service (clinical) reviews, and continued service (non-clinical) reviews for hospital, ambulatory surgical centers and home health and private-duty nursing services. Transformed-Medicaid Statistical Information System (T-MSIS) The T-MSIS project, started in January 2013, is the expansion of federal reporting measures from the States Medicaid Information Systems. The new report will be submitted monthly instead of the quarterly MSIS report. Report data has been expanded to include: eligibility information, health care quality measures, managed care measures in addition to medical services claims and frequency reporting. Medicaid will be utilizing the new reports by July MMIS Replacement Project Nebraska s Medicaid Management Information System (MMIS) was created in 1977 and is no longer able to meet the new demands of a rapidly changing Medicaid environment. The need for expedient programmatic changes and the ability to readily produce data are just two of the many enhancements necessary to efficiently manage today's Medicaid program. Nebraska Medicaid began an alternatives analysis process near the end of SFY 2012, examining the options for upgrading/replacing the MMIS. With technology improvements and increased federal 23
27 requirements over the past year, this analysis will be updated leveraging the work completed through the MITA 3.0 State Self-Assessment process. The alternatives analysis will assist the Division in decision making and lead to the next steps in the procurement process. III. CONCLUSION The Department of Health and Human Services, Division of Medicaid & Long-Term Care strives to operate a Medicaid program which addresses the health care needs of eligible low-income Nebraska residents in a cost-effective and deliberately planned manner. The number of Medicaid eligible recipients has increased in recent years due to economic conditions. Concurrently, the program and policies referenced in this Annual Report work to moderate the growth of Medicaid expenditures. These policies and initiatives slow the growth of the Medicaid program and further fiscal sustainability by making the program more efficient and more cost-effective through careful management of services, better delivery of care, more appropriate services, and improved administration of the program. The Department of Health and Human Services, Division of Medicaid & Long-Term Care looks forward to continuing to work with the Governor, the Legislature, the Medicaid Reform Council, and stakeholders to improve Medicaid for current and future generations. 24
DEPARTMENT OF HEALTH & HUMAN SERVICES MEDICAID PROGRAM OVERVIEW
 DEPARTMENT OF HEALTH & HUMAN SERVICES MEDICAID PROGRAM OVERVIEW North Carolina General Assembly Fiscal Research Division February 2005 Overview Purpose of Medicaid Impact of Medicaid - On the State Economy
DEPARTMENT OF HEALTH & HUMAN SERVICES MEDICAID PROGRAM OVERVIEW North Carolina General Assembly Fiscal Research Division February 2005 Overview Purpose of Medicaid Impact of Medicaid - On the State Economy
Nebraska Medicaid Managed Long-Term Services and Supports
 Background A significant shift in the management and administration of Medicaid services has taken place over the past several years with the growth of managed care. Full-risk managed care is a health
Background A significant shift in the management and administration of Medicaid services has taken place over the past several years with the growth of managed care. Full-risk managed care is a health
THE MEDICAID PROGRAM AT A GLANCE. Health Insurance Coverage
 on on medicaid and and the the uninsured March 2013 THE MEDICAID PROGRAM AT A GLANCE Medicaid, the nation s main public health insurance program for low-income people, covers over 62 million Americans,
on on medicaid and and the the uninsured March 2013 THE MEDICAID PROGRAM AT A GLANCE Medicaid, the nation s main public health insurance program for low-income people, covers over 62 million Americans,
Department of Social Services. South Dakota Medicaid Division of Medical Services (MS)
") Department of Social Services South Dakota Medicaid Division of Medical Services (MS) Overview What is Medicaid? Who We Serve Services Provided Medicaid Budget South Dakota Medicaid: Medicaid is the nation
Department of Social Services South Dakota Medicaid Division of Medical Services (MS) Overview What is Medicaid? Who We Serve Services Provided Medicaid Budget South Dakota Medicaid: Medicaid is the nation
Oregon Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Oregon
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Oregon As of July 2003, 398,874 people were covered under Oregon s Medicaid/SCHIP programs. There were 380,546 enrolled in the Medicaid
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Oregon As of July 2003, 398,874 people were covered under Oregon s Medicaid/SCHIP programs. There were 380,546 enrolled in the Medicaid
and the uninsured June 2005 Medicaid: An Overview of Spending on Mandatory vs. Optional Populations and Services
 I S S U E kaiser commission on medicaid and the uninsured June 2005 P A P E R Medicaid: An Overview of Spending on vs. Optional Populations and Services Medicaid is a federal-state program that provides
I S S U E kaiser commission on medicaid and the uninsured June 2005 P A P E R Medicaid: An Overview of Spending on vs. Optional Populations and Services Medicaid is a federal-state program that provides
Quarterly Medicaid Statement of Expenditures For the Medical Assistance Program
 Quarterly Medicaid Statement of Expenditures For the Medical Assistance Program CMS 64 Summary Sheet Net Expenditures Reported In This Period (Sum of Items 6, 7 and 8 Less 9 and 10) I certify that: Certification
Quarterly Medicaid Statement of Expenditures For the Medical Assistance Program CMS 64 Summary Sheet Net Expenditures Reported In This Period (Sum of Items 6, 7 and 8 Less 9 and 10) I certify that: Certification
Florida Medicaid and Implementation of SB 2654
 Florida Medicaid and Implementation of SB 2654 Shachi Mankodi Counsel to the Chief of Staff Florida Agency for Health Care Administration Autism Compact Presentation September 18, 2008 Overview What is
Florida Medicaid and Implementation of SB 2654 Shachi Mankodi Counsel to the Chief of Staff Florida Agency for Health Care Administration Autism Compact Presentation September 18, 2008 Overview What is
National Training Program
 National Training Program Module 12 Medicaid and the Children s Health Insurance Program Session Objectives This session will help you Describe eligibility, benefits, and administration of Medicaid Define
National Training Program Module 12 Medicaid and the Children s Health Insurance Program Session Objectives This session will help you Describe eligibility, benefits, and administration of Medicaid Define
History of Arkansas s Traditional Medicaid Program
 History of rkansas s Traditional Medicaid Program (1970-2013) Produced by 1401 W. Capitol venue, Suite 300 Little Rock, R 72201 (501) 526-2244, www.achi.net nonpartisan, independent, health policy center
History of rkansas s Traditional Medicaid Program (1970-2013) Produced by 1401 W. Capitol venue, Suite 300 Little Rock, R 72201 (501) 526-2244, www.achi.net nonpartisan, independent, health policy center
Maryland Medicaid Program. Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 15, 2012
 Maryland Medicaid Program Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 15, 2012 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance or MA. MA is a joint
Maryland Medicaid Program Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 15, 2012 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance or MA. MA is a joint
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Colorado
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Colorado As of July 2003, 377,123 people were covered under Colorado s Medicaid and SCHIP programs. There were 330,499 enrolled in the
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Colorado As of July 2003, 377,123 people were covered under Colorado s Medicaid and SCHIP programs. There were 330,499 enrolled in the
How To Get A Medicaid Card
 MEDICAID care is reasonable, necessary, and provided in the most appropriate setting. The PROs are composed of groups of practicing physicians. To receive Medicare payments, a hospital must have an agreement
MEDICAID care is reasonable, necessary, and provided in the most appropriate setting. The PROs are composed of groups of practicing physicians. To receive Medicare payments, a hospital must have an agreement
Managed Care in New York
 Managed Care in New York This profile reflects state managed care program information as of August 2014, and only includes information on active federal operating authorities, and as such, the program
Managed Care in New York This profile reflects state managed care program information as of August 2014, and only includes information on active federal operating authorities, and as such, the program
Vermont s Health Care System Overview: Payers & Players
 1 Vermont s Health Care System Overview: Payers & Players (as we currently know it) Updated January 2015 Nolan Langweil, Joint Fiscal Office 2 Parts of a Health Care System Patients Providers Payers (Insurance
1 Vermont s Health Care System Overview: Payers & Players (as we currently know it) Updated January 2015 Nolan Langweil, Joint Fiscal Office 2 Parts of a Health Care System Patients Providers Payers (Insurance
Appendix 4: SPA and Waiver Options to Enhance Concurrent Care Programs
 Appendix 4: SPA and Waiver Options to Enhance Concurrent Care Programs Medicaid State Plan Options Each state describes its Medicaid program in the Medicaid State Plan. The State Plan specifies how the
Appendix 4: SPA and Waiver Options to Enhance Concurrent Care Programs Medicaid State Plan Options Each state describes its Medicaid program in the Medicaid State Plan. The State Plan specifies how the
Maryland Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland As of July 2003, 638,662 people were covered under Maryland's Medicaid/SCHIP programs. There were 525,080 enrolled in the Medicaid
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland As of July 2003, 638,662 people were covered under Maryland's Medicaid/SCHIP programs. There were 525,080 enrolled in the Medicaid
Summary of Federal SCHIP Reauthorization, Economic Stimulus, and Health Care Reform Bills and Proposals
 Summary of Federal SCHIP Reauthorization, Economic Stimulus, and Health Care Reform Bills and Proposals I. Children s Health Insurance Program (CHIP) Reauthorization Act of 2009 A. Funding for CHIP. The
Summary of Federal SCHIP Reauthorization, Economic Stimulus, and Health Care Reform Bills and Proposals I. Children s Health Insurance Program (CHIP) Reauthorization Act of 2009 A. Funding for CHIP. The
New Hampshire Department of Health and Human Services. Medicaid Care Management Program Step 2 Design Concept
 New Hampshire Department of Health and Human Services Medicaid Care Management Program Step 2 Design Concept Redesign of New Hampshire s Long Term Services and Supports Delivery System: A Concept Paper
New Hampshire Department of Health and Human Services Medicaid Care Management Program Step 2 Design Concept Redesign of New Hampshire s Long Term Services and Supports Delivery System: A Concept Paper
Medicaid 101. The basics of publicly funded healthcare.
 Medicaid 101 The basics of publicly funded healthcare. Medicare Vs Medicaid Medicare: Over 65, or Disabled Federally Managed program Medicaid Resource & Need Based State Federal Partnership Social Security
Medicaid 101 The basics of publicly funded healthcare. Medicare Vs Medicaid Medicare: Over 65, or Disabled Federally Managed program Medicaid Resource & Need Based State Federal Partnership Social Security
An Overview of Wisconsin s Medical Assistance, BadgerCare, and SeniorCare Programs
 An Overview of Wisconsin s Medical Assistance, BadgerCare, and SeniorCare Programs Prepared by Marlia Moore and Charles Morgan Wisconsin Legislative Fiscal Bureau Medical Assistance W i sconsin s medical
An Overview of Wisconsin s Medical Assistance, BadgerCare, and SeniorCare Programs Prepared by Marlia Moore and Charles Morgan Wisconsin Legislative Fiscal Bureau Medical Assistance W i sconsin s medical
WHAT HEALTHCARE PROVIDERS SHOULD KNOW ABOUT THE PROPOSED MEDICAID MANAGED CARE REGULATIONS RELEASED LAST WEEK
 WHAT HEALTHCARE PROVIDERS SHOULD KNOW ABOUT THE PROPOSED MEDICAID MANAGED CARE REGULATIONS RELEASED LAST WEEK By Mark E. Reagan, Felicia Y Sze, Joseph R. LaMagna, Nina Adatia Marsden and Yanyan Zhou Basics:
WHAT HEALTHCARE PROVIDERS SHOULD KNOW ABOUT THE PROPOSED MEDICAID MANAGED CARE REGULATIONS RELEASED LAST WEEK By Mark E. Reagan, Felicia Y Sze, Joseph R. LaMagna, Nina Adatia Marsden and Yanyan Zhou Basics:
Chapter 7 Acute Care Inpatient/Outpatient Hospital Services
 Chapter 7: Acute Care Inpatient/ Outpatient Hospital Services Executive Summary Description Acute care hospitals are the largest group of enrolled hospital providers. Kansas Medicaid has 144 acute care
Chapter 7: Acute Care Inpatient/ Outpatient Hospital Services Executive Summary Description Acute care hospitals are the largest group of enrolled hospital providers. Kansas Medicaid has 144 acute care
Maryland Medicaid Program: An Overview. Stacey Davis Planning Administration Department of Health and Mental Hygiene May 22, 2007
 Maryland Medicaid Program: An Overview Stacey Davis Planning Administration Department of Health and Mental Hygiene May 22, 2007 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance
Maryland Medicaid Program: An Overview Stacey Davis Planning Administration Department of Health and Mental Hygiene May 22, 2007 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance
Maryland Medicaid Program
 Maryland Medicaid Program Maryland s Pharmacy Discount Waiver Tuesday, November 19, 2002 Debbie I. Chang Deputy Secretary for Health Care Financing Maryland Department of Health and Mental Hygiene Overview
Maryland Medicaid Program Maryland s Pharmacy Discount Waiver Tuesday, November 19, 2002 Debbie I. Chang Deputy Secretary for Health Care Financing Maryland Department of Health and Mental Hygiene Overview
Resources and Services Directory for Head Injury and Other Conditions
 Resources and Services Directory for Head Injury and Other Conditions Section 2: Accessing and Paying for TBI and Related Services 1000 NE 10 TH ST. OKC, OK 73117 TEL 405.271-3430 OR 800.522.0204 (OK only)
Resources and Services Directory for Head Injury and Other Conditions Section 2: Accessing and Paying for TBI and Related Services 1000 NE 10 TH ST. OKC, OK 73117 TEL 405.271-3430 OR 800.522.0204 (OK only)
COMPARISON OF THE FY 2015 HOUSE AND SENATE BUDGET PROPOSALS FOR MASSHEALTH AND HEALTH REFORM PROGRAMS
 COMPARISON OF THE HOUSE AND SENATE BUDGET PROPOSALS FOR MASSHEALTH AND HEALTH REFORM PROGRAMS BUDGET BRIEF JUNE 2014 The Fiscal Year (FY) 2015 Massachusetts state budget has moved into the final stages
COMPARISON OF THE HOUSE AND SENATE BUDGET PROPOSALS FOR MASSHEALTH AND HEALTH REFORM PROGRAMS BUDGET BRIEF JUNE 2014 The Fiscal Year (FY) 2015 Massachusetts state budget has moved into the final stages
Strengthening Community Health Centers. Provides funds to build new and expand existing community health centers. Effective Fiscal Year 2011.
 Implementation Timeline Reflecting the Affordable Care Act 2010 Access to Insurance for Uninsured Americans with a Pre-Existing Condition. Provides uninsured Americans with pre-existing conditions access
Implementation Timeline Reflecting the Affordable Care Act 2010 Access to Insurance for Uninsured Americans with a Pre-Existing Condition. Provides uninsured Americans with pre-existing conditions access
Statewide Medicaid Managed Care Managed Medical Assistance Program Update
 Statewide Medicaid Managed Care Managed Medical Assistance Program Update Beth Kidder Assistant Deputy Secretary for Medicaid Operations Agency for Health Care Administration Presented to the KidCare Coordinating
Statewide Medicaid Managed Care Managed Medical Assistance Program Update Beth Kidder Assistant Deputy Secretary for Medicaid Operations Agency for Health Care Administration Presented to the KidCare Coordinating
A Healthy Florida Works Program. Policy Proposal. The smart choice for individuals and businesses in Florida
 A Healthy Florida Works Program Policy Proposal The smart choice for individuals and businesses in Florida TABLE OF CONTENTS Introduction Executive Summary Program Description 3 5 6 Coverage Population
A Healthy Florida Works Program Policy Proposal The smart choice for individuals and businesses in Florida TABLE OF CONTENTS Introduction Executive Summary Program Description 3 5 6 Coverage Population
Health Information Technology (IT) Simplified
 Simplified") Health Information Technology (IT) Simplified A glossary of all things Health IT Accountable Care Organizations (ACO) - A group of health care providers who give coordinated care, chronic disease management,
Health Information Technology (IT) Simplified A glossary of all things Health IT Accountable Care Organizations (ACO) - A group of health care providers who give coordinated care, chronic disease management,
Florida Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Florida
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Florida As of July 2003 2,441,266 people were covered under Florida's Medicaid and SCHIP programs. There were 2,113,820 enrolled in the
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Florida As of July 2003 2,441,266 people were covered under Florida's Medicaid and SCHIP programs. There were 2,113,820 enrolled in the
HB 686-FN-A - AS INTRODUCED. establishing a single payer health care system and making an appropriation therefor.
 0 SESSION -0 0/0 HOUSE BILL AN ACT -FN-A establishing a single payer health care system and making an appropriation therefor. SPONSORS: Rep. McNamara, Hills ; Rep. Suzanne Smith, Graf ; Rep. Moody, Rock
0 SESSION -0 0/0 HOUSE BILL AN ACT -FN-A establishing a single payer health care system and making an appropriation therefor. SPONSORS: Rep. McNamara, Hills ; Rep. Suzanne Smith, Graf ; Rep. Moody, Rock
THE FISCAL YEAR 2015 BUDGET FOR MASSHEALTH AND HEALTH REFORM PROGRAMS
 THE FISCAL YEAR 2015 BUDGET FOR MASSHEALTH AND HEALTH REFORM PROGRAMS BUDGET BRIEF SEPTEMBER 2014 On July 10, 2014, Governor Deval Patrick signed the budget for fiscal year (FY) 2015, one week into the
THE FISCAL YEAR 2015 BUDGET FOR MASSHEALTH AND HEALTH REFORM PROGRAMS BUDGET BRIEF SEPTEMBER 2014 On July 10, 2014, Governor Deval Patrick signed the budget for fiscal year (FY) 2015, one week into the
Medicaid Home- and Community-Based Waiver Programs
 INFORMATION BRIEF Research Department Minnesota House of Representatives 600 State Office Building St. Paul, MN 55155 Danyell Punelli, Legislative Analyst 651-296-5058 Updated: November 2013 Medicaid Home-
INFORMATION BRIEF Research Department Minnesota House of Representatives 600 State Office Building St. Paul, MN 55155 Danyell Punelli, Legislative Analyst 651-296-5058 Updated: November 2013 Medicaid Home-
ENSURING STABLE AND CONTINUOUS HEALTH INSURANCE COVERAGE FOR CHILDREN WITH ASTHMA
 About This Series In February 2010, the George Washington University School of Public Health and Health Services, Department of Health Policy released Changing po 2 licy: The Elements for Improving Childhood
About This Series In February 2010, the George Washington University School of Public Health and Health Services, Department of Health Policy released Changing po 2 licy: The Elements for Improving Childhood
HOUSE OF REPRESENTATIVES
 HOUSE OF REPRESENTATIVES HB 2010 2013-2014; health; welfare; budget reconciliation. Sponsor: Representative Pratt DPA X Caucus and COW House Engrossed OVERVIEW HB 2010 includes provisions to health and
HOUSE OF REPRESENTATIVES HB 2010 2013-2014; health; welfare; budget reconciliation. Sponsor: Representative Pratt DPA X Caucus and COW House Engrossed OVERVIEW HB 2010 includes provisions to health and
Molina Healthcare of Ohio Nursing Facility Orientation Molina Dual Options MyCare Ohio 2014
 Molina Healthcare of Ohio Nursing Facility Orientation Molina Dual Options MyCare Ohio 2014 1 Eligibility Headline Goes Here Long Term Care (LTC) is the provision of medical, social, and personal care
Molina Healthcare of Ohio Nursing Facility Orientation Molina Dual Options MyCare Ohio 2014 1 Eligibility Headline Goes Here Long Term Care (LTC) is the provision of medical, social, and personal care
8.2000: HOSPITAL PROVIDER FEE COLLECTION AND DISBURSEMENT
 DEPARTMENT OF HEALTH CARE POLICY AND FINANCING MEDICAL ASSISTANCE SECTION 8.2000 [Editor s Notes follow the text of the rules at the end of this CCR Document.] 8.2000: HOSPITAL PROVIDER FEE COLLECTION
DEPARTMENT OF HEALTH CARE POLICY AND FINANCING MEDICAL ASSISTANCE SECTION 8.2000 [Editor s Notes follow the text of the rules at the end of this CCR Document.] 8.2000: HOSPITAL PROVIDER FEE COLLECTION
Affordable Care Act Opportunities for the Aging Network
 Affordable Care Act Opportunities for the Aging Network The Affordable Care Act (ACA) offers many opportunities for the Aging Network to be full partners in health system reform. These include demonstration
Affordable Care Act Opportunities for the Aging Network The Affordable Care Act (ACA) offers many opportunities for the Aging Network to be full partners in health system reform. These include demonstration
Molina Healthcare of Washington, Inc. Glossary GLOSSARY OF TERMS
 GLOSSARY OF TERMS Action The denial or limited Authorization of a requested service, including the type, level or provider of service; reduction, suspension, or termination of a previously authorized service;
GLOSSARY OF TERMS Action The denial or limited Authorization of a requested service, including the type, level or provider of service; reduction, suspension, or termination of a previously authorized service;
MANAGED LONG-TERM CARE AND NURSING HOMES
 MANAGED LONG-TERM CARE AND NURSING HOMES Frequently Asked Questions 12/13/2012 2 MANAGED LONG-TERM CARE AND NURSING HOMES This FAQ is divided into 4 sections: (1) The overview of Managed Long-Term Care
MANAGED LONG-TERM CARE AND NURSING HOMES Frequently Asked Questions 12/13/2012 2 MANAGED LONG-TERM CARE AND NURSING HOMES This FAQ is divided into 4 sections: (1) The overview of Managed Long-Term Care
Summary of the Major Provisions in the Patient Protection and Affordable Health Care Act
 Summary of the Major Provisions in the Patient Protection and Affordable Care Act Updated 10/22/10 On March 23, 2010, President Barack Obama signed into law comprehensive health care reform legislation,
Summary of the Major Provisions in the Patient Protection and Affordable Care Act Updated 10/22/10 On March 23, 2010, President Barack Obama signed into law comprehensive health care reform legislation,
Strengthening Medicare: Better Health, Better Care, Lower Costs Efforts Will Save Nearly $120 Billion for Medicare Over Five Years.
 Strengthening Medicare: Better Health, Better Care, Lower Costs Efforts Will Save Nearly $120 Billion for Medicare Over Five Years Introduction The Centers for Medicare and Medicaid Services (CMS) and
Strengthening Medicare: Better Health, Better Care, Lower Costs Efforts Will Save Nearly $120 Billion for Medicare Over Five Years Introduction The Centers for Medicare and Medicaid Services (CMS) and
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT
 Page 1 PROFESSIONAL MEDICAL PERSONNEL AND SUPPORTING STAFF USED IN THE ADMINISTRATION OF THE PROGRAM AND THEIR RESPONSIBILITIES Attached is a description of the kinds and number of the medical assistance
Page 1 PROFESSIONAL MEDICAL PERSONNEL AND SUPPORTING STAFF USED IN THE ADMINISTRATION OF THE PROGRAM AND THEIR RESPONSIBILITIES Attached is a description of the kinds and number of the medical assistance
Treatment Facilities Amended Date: October 1, 2015. Table of Contents
 Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1 General... 1 2.1.2 Specific... 1 2.2 Special
Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1 General... 1 2.1.2 Specific... 1 2.2 Special
Statewide Hospital Quality Care Assessment Frequently Asked Questions
 Statewide Hospital Quality Care Assessment 1. Q: Why are hospitals being assessed? A: Federal regulations, CFR 42 Part 433 - Fiscal Administration, allows states to assess 19 classes of providers under
Statewide Hospital Quality Care Assessment 1. Q: Why are hospitals being assessed? A: Federal regulations, CFR 42 Part 433 - Fiscal Administration, allows states to assess 19 classes of providers under
Maryland Medicaid s Partnership in Improving Behavioral Health Services. Susan Tucker Executive Director, Office of Health Services May 14, 2014
 Maryland Medicaid s Partnership in Improving Behavioral Health Services Susan Tucker Executive Director, Office of Health Services May 14, 2014 Began in 1966 Maryland Medicaid By FY 14, we provided full
Maryland Medicaid s Partnership in Improving Behavioral Health Services Susan Tucker Executive Director, Office of Health Services May 14, 2014 Began in 1966 Maryland Medicaid By FY 14, we provided full
Health Reform and the AAP: What the New Law Means for Children and Pediatricians
 Health Reform and the AAP: What the New Law Means for Children and Pediatricians Throughout the health reform process, the American Academy of Pediatrics has focused on three fundamental priorities for
Health Reform and the AAP: What the New Law Means for Children and Pediatricians Throughout the health reform process, the American Academy of Pediatrics has focused on three fundamental priorities for
Office of Health Transformation Extend Medicaid Coverage and Automate Enrollment
 Office of Health Transformation Extend Medicaid Coverage and Automate Enrollment Background: Eligibility determination for health and human services programs in Ohio are fragmented, overly complex, and
Office of Health Transformation Extend Medicaid Coverage and Automate Enrollment Background: Eligibility determination for health and human services programs in Ohio are fragmented, overly complex, and
Psychiatric Rehabilitation Clinical Coverage Policy No: 8D-1 Treatment Facilities Revised Date: August 1, 2012. Table of Contents
 Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 2.0 Eligible Recipients... 1 2.1 Provisions... 1 2.2 EPSDT Special Provision: Exception to Policy Limitations for Recipients
Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 2.0 Eligible Recipients... 1 2.1 Provisions... 1 2.2 EPSDT Special Provision: Exception to Policy Limitations for Recipients
1965-1969 1970-1974 1975-1979 1980-1984 1985-1989 1990-1994 1995-1999 2000-2004 2005-2009
 1965-1969 1970-1974 1975-1979 1980-1984 1985-1989 1990-1994 1995-1999 2000-2004 2005-2009 Intro Entire Timeline Displaying: 1965-2009 1965-2009 1965: Medicaid and Medicare passed by the U.S. House of Representatives
1965-1969 1970-1974 1975-1979 1980-1984 1985-1989 1990-1994 1995-1999 2000-2004 2005-2009 Intro Entire Timeline Displaying: 1965-2009 1965-2009 1965: Medicaid and Medicare passed by the U.S. House of Representatives
THE GOVERNOR S FY 2015 BUDGET PROPOSAL FOR MASSHEALTH (MEDICAID) AND HEALTH REFORM PROGRAMS
 AND HEALTH REFORM PROGRAMS") THE GOVERNOR S BUDGET PROPOSAL FOR MASSHEALTH (MEDICAID) AND HEALTH REFORM PROGRAMS BUDGET BRIEF MARCH 2014 On January 22, the Governor released his budget proposal for the upcoming fiscal year (FY) 2015,
THE GOVERNOR S BUDGET PROPOSAL FOR MASSHEALTH (MEDICAID) AND HEALTH REFORM PROGRAMS BUDGET BRIEF MARCH 2014 On January 22, the Governor released his budget proposal for the upcoming fiscal year (FY) 2015,
OVERVIEW OF KENTUCKY Outreach MEDICAID AND KCHIP
 OVERVIEW OF KENTUCKY Outreach MEDICAID AND KCHIP Lisa Lee Director, Medicaid Division of Provider Operations Program Director, Kentucky Children s Health Insurance Program (KCHIP) September 2011 Background
OVERVIEW OF KENTUCKY Outreach MEDICAID AND KCHIP Lisa Lee Director, Medicaid Division of Provider Operations Program Director, Kentucky Children s Health Insurance Program (KCHIP) September 2011 Background
Health Insurance Reform at a Glance Implementation Timeline
 Health Insurance Reform at a Glance Implementation Timeline 2010 Access to Insurance for Uninsured Americans with a Pre-Existing Condition. Provides uninsured Americans with pre-existing conditions access
Health Insurance Reform at a Glance Implementation Timeline 2010 Access to Insurance for Uninsured Americans with a Pre-Existing Condition. Provides uninsured Americans with pre-existing conditions access
Finally... maybe? The Long Awaited 340B Mega Guidance. Georgia Healthcare Financial Management Association. October 2015
 Finally... maybe? The Long Awaited 340B Mega Guidance Georgia Healthcare Financial Management Association October 2015 Disclaimer This webinar assumes the participant is familiar with the basic operations
Finally... maybe? The Long Awaited 340B Mega Guidance Georgia Healthcare Financial Management Association October 2015 Disclaimer This webinar assumes the participant is familiar with the basic operations
Kansas Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Kansas
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Kansas As of July 2003, 262,791 people were covered under Kansas's Medicaid and SCHIP programs. There were 233,481 enrolled in the Medicaid
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Kansas As of July 2003, 262,791 people were covered under Kansas's Medicaid and SCHIP programs. There were 233,481 enrolled in the Medicaid
Randall Chun, Legislative Analyst Updated: January 2016. MinnesotaCare
 INFORMATION BRIEF Research Department Minnesota House of Representatives 600 State Office Building St. Paul, MN 55155 Randall Chun, Legislative Analyst is administered by the Minnesota Department of Human
INFORMATION BRIEF Research Department Minnesota House of Representatives 600 State Office Building St. Paul, MN 55155 Randall Chun, Legislative Analyst is administered by the Minnesota Department of Human
Concept Paper: Texas Nursing Facility Transformation Program
 QAPI Version Concept Paper: Texas Nursing Facility Transformation Program Introduction This concept paper presents a proposal to establish a Nursing Facility (NF) Transformation Program beginning in DY
QAPI Version Concept Paper: Texas Nursing Facility Transformation Program Introduction This concept paper presents a proposal to establish a Nursing Facility (NF) Transformation Program beginning in DY
The Healthy Michigan Plan Handbook
 The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). The Healthy Michigan Plan provides health
The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). The Healthy Michigan Plan provides health
EXAMINING THE IMPACT OF THE PATIENT PROTECTION AND AFFORDABLE CARE ACT IN NORTH CAROLINA MEDICAID EXPANSION OPTION ISSUE BRIEF
 EXAMINING THE IMPACT OF THE PATIENT PROTECTION AND AFFORDABLE CARE ACT IN NORTH CAROLINA MEDICAID EXPANSION OPTION ISSUE BRIEF As originally passed, the Patient Protection and Affordable Care Act (ACA)
EXAMINING THE IMPACT OF THE PATIENT PROTECTION AND AFFORDABLE CARE ACT IN NORTH CAROLINA MEDICAID EXPANSION OPTION ISSUE BRIEF As originally passed, the Patient Protection and Affordable Care Act (ACA)
Appendix A. Glossary
 Glossary The following provides brief definitions and descriptions of terms, abbreviations, and acronyms often used in the conjunction with the Medicaid program. AI is an indicator in the CAP block on
Glossary The following provides brief definitions and descriptions of terms, abbreviations, and acronyms often used in the conjunction with the Medicaid program. AI is an indicator in the CAP block on
Medicaid Priorities in a Changing 21st Century Health Care Environment
 Medicaid Priorities in a Changing 21st Century Health Care Environment Michael J. Melendez, LMSW Associate Regional Administrator New York Regional Office Division of Medicaid and Children s Health Operations
Medicaid Priorities in a Changing 21st Century Health Care Environment Michael J. Melendez, LMSW Associate Regional Administrator New York Regional Office Division of Medicaid and Children s Health Operations
AGENCY FOR HEALTH CARE ADMINISTRATION MEDICAID OFFICE
 AGENCY FOR HEALTH CARE ADMINISTRATION MEDICAID OFFICE Attachment 1.2-8 Page 1 Director of Medicaid Pereonal Secretary I Sre Human Sarv. Program Administrator Eleven Area Of fices Program Analysis Third
AGENCY FOR HEALTH CARE ADMINISTRATION MEDICAID OFFICE Attachment 1.2-8 Page 1 Director of Medicaid Pereonal Secretary I Sre Human Sarv. Program Administrator Eleven Area Of fices Program Analysis Third
Application for CFSS Consultation and Financial Management Services. Section 1915(b) (4) Waiver Fee-for-Service Selective Contracting Program
 (4) Waiver Fee-for-Service Selective Contracting Program") Application for CFSS Consultation and Financial Management Services Section 1915(b) (4) Waiver Fee-for-Service Selective Contracting Program June 2014 Section A Waiver Program Description Part I: Program
Application for CFSS Consultation and Financial Management Services Section 1915(b) (4) Waiver Fee-for-Service Selective Contracting Program June 2014 Section A Waiver Program Description Part I: Program
Managed Care in Minnesota
 Managed Care in Minnesota This profile reflects state managed care program information as of August 2014, and only includes information on active federal operating authorities, and as such, the program
Managed Care in Minnesota This profile reflects state managed care program information as of August 2014, and only includes information on active federal operating authorities, and as such, the program
The Healthy Michigan Plan Handbook
 The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). Eligibility for this program will be determined
The Healthy Michigan Plan Handbook Introduction The Healthy Michigan Plan is a health care program through the Michigan Department of Community Health (MDCH). Eligibility for this program will be determined
COMMUNITY HEALTH CENTER GROWTH AND SUSTAINABILITY STATE PROFILES NEW HAMPSHIRE. Primary Care Transformation 10
 COMMUNITY HEALTH CENTER GROWTH AND STAINABILITY STATE PROFILES NEW HAMPSHIRE CONTENTS Overview 2 CHC Scale 3 CHC Financial Status 6 Primary Care Need 9 Primary Care Transformation 10 Medicaid and Health
COMMUNITY HEALTH CENTER GROWTH AND STAINABILITY STATE PROFILES NEW HAMPSHIRE CONTENTS Overview 2 CHC Scale 3 CHC Financial Status 6 Primary Care Need 9 Primary Care Transformation 10 Medicaid and Health
Health Care Eligibility and Access. Karen Gibson, Director
 Health Care Eligibility and Access Karen Gibson, Director Minnesota Health Care Programs Minnesota has a large and complex array of public health care programs funded either jointly with the federal government
Health Care Eligibility and Access Karen Gibson, Director Minnesota Health Care Programs Minnesota has a large and complex array of public health care programs funded either jointly with the federal government
Summary of the Final Medicaid Redesign Team (MRT) Report A Plan to Transform The Empire State s Medicaid Program
 Report A Plan to Transform The Empire State s Medicaid Program") Summary of the Final Medicaid Redesign Team (MRT) Report A Plan to Transform The Empire State s Medicaid Program May 2012 This document summarizes the key points contained in the MRT final report, A Plan
Summary of the Final Medicaid Redesign Team (MRT) Report A Plan to Transform The Empire State s Medicaid Program May 2012 This document summarizes the key points contained in the MRT final report, A Plan
CHAPTER 9 FRAUD, ABUSE, AND OVERUTILIZATION
 CHAPTER 9 FRAUD, ABUSE, AND OVERUTILIZATION OVERVIEW OF THE PROBLEM The ACA includes funding to support more aggressive efforts to eliminate fraud and abuse, and to recover overpayments in Medicare, Medicaid,
CHAPTER 9 FRAUD, ABUSE, AND OVERUTILIZATION OVERVIEW OF THE PROBLEM The ACA includes funding to support more aggressive efforts to eliminate fraud and abuse, and to recover overpayments in Medicare, Medicaid,