Combining Case and Care Management for Population Health
|
|
|
- Russell Summers
- 8 years ago
- Views:
Transcription
1 Combining Case and Care Management for Population Health Raena C. Akin-Deko, MHSA Assistant Vice President for Product Development, NCQA Karen Handmaker, MPP VP Population Health Strategies, Phytel August 28, 2013

2 About NCQA Our mission To improve the quality of health care Our method Measurement We can t improve what we don t measure Transparency We show how we measure so measurement will be accepted Accountability Once we measure, we can expect and track progress 2

3 Objectives Understanding Case and Care Management What s the difference? Why are both critical to population health management? How PCMH standards encourage both Lessons from NCQA s Recognized PCMHs Care management is harder to implement Funding is necessary for sustainability Health IT is a fundamental tool for care teams Strengthening Population Health Through the PCMH Model NCQA: Case Management 3

4 PCMH Transforms Practice Model for Population Health Current View 30 Patients Per Day 14 have Chronic Conditions Unknown Health Risks Visits Too Short for Coaching New Population View 2500 Patient Population 900 have Chronic Conditions have Mod-High Health Risk Care Teams Leveraged by HIT Volume-Based/Episodic Value-Based/Continuous

5 The Definition of Care Management 5
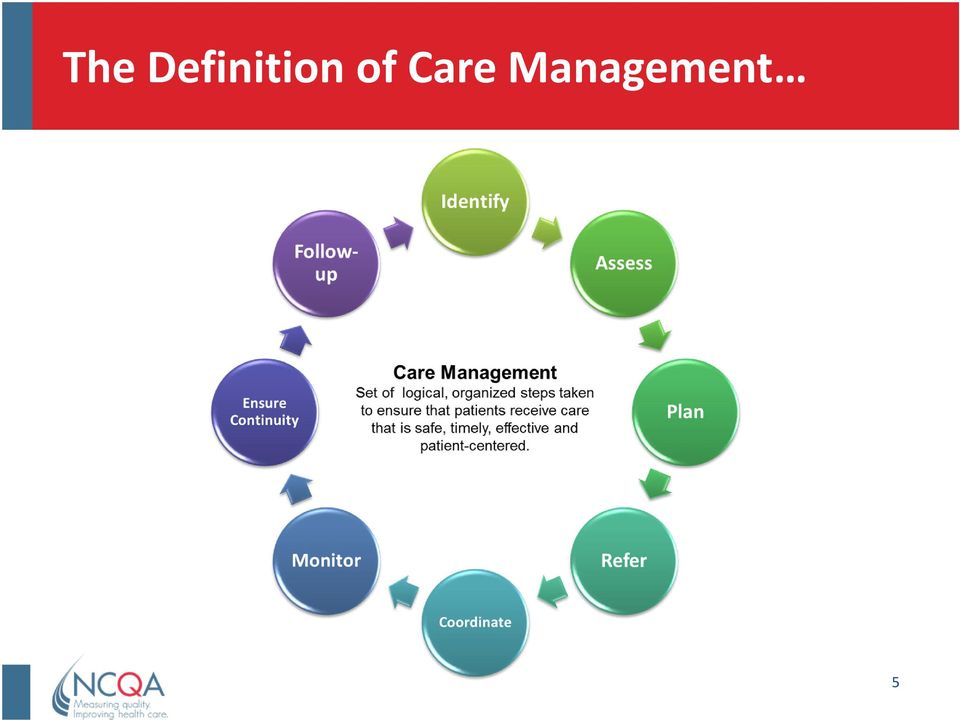
6 Looks a lot like the definition for Case Management NCQA: Case Management 6

7 Care Management vs. Case Management Care Management Case Management

8 What s Your Role? (Show of Hands!) CARE Manager Low-Moderate risk patients Risks & conditions have defined guidelines Increase monitoring & improve self-care to stabilize symptoms, prevent migration Caseload: Focus: Close care gaps Identify health risks early Preventive treatment Increase self-care capabilities Promote healthy lifestyle CASE Manager High-risk patients Complex, high cost treatment needs Significant barriers to self/care, services Post-acute risk spikes Caseload: Focus: Transition management Care coordination Stabilization at point of optimal recovery Cost containment Coordination of benefits 8

9 Costs of Uncoordinated Care Health care costs are expected to reached $4.4T in 2018 A 2010 IOM roundtable on Value and Science- Driven Healthcare 1 noted the following as drivers of health care costs: Unnecessary services Inefficiently delivered care Missed prevention opportunities Case management aims to coordinate care to mitigate these concerns 1. IOM. The Healthcare Imperative: Lowering Costs and Improving Outcomes: Workshop Series Summary. Roundtable on Value and Science-Driven Healthcare

10 Costs of Uncoordinated Care ""Health Policy Brief: Reducing Waste in Health Care," Health Affairs, December 13,

11 The Importance of CASE Management Case management helps patients navigate the health care system Allows for the coordination of care across the healthcare system Increases adherence to care plans and improves quality outcomes Reduces fragmentation of health care, which can occur when patients receive services from multiple settings Can reduce patient and system costs

12 Care Management: Look Below the Waterline Do you only focus the top 3%?

13 Evolution in Approach: Patient-Centered, Provider-Delivered Care Managemet Patient-Centered Medical Homes Care teams led by a clinician coordinate all aspects of a patient s care, including care planning and connections to community resources Accountable Care Organizations Provider-based organizations that are accountable for both quality and costs of care for a defined population Arrange for the total continuum of care Embedded Case Managers Geisinger ProvenHealth Navigator Community Care of North Carolina 13

14 NCQA PCMH Standards 14
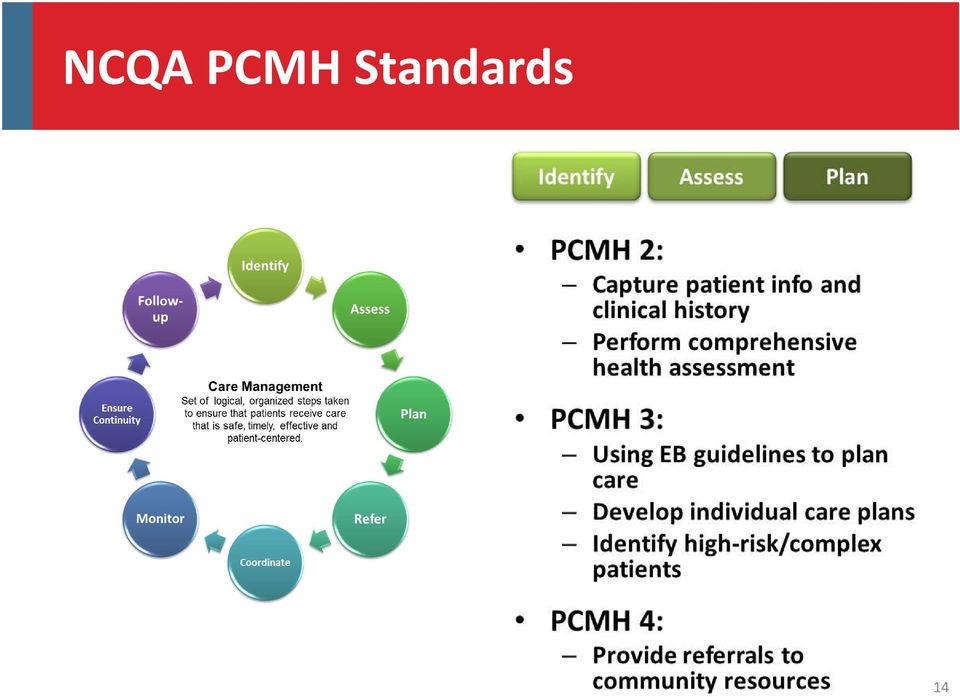
15 NCQA PCMH Standards (continued) 15

16 NCQA PCMH Standards (continued) 16

17 Research supporting comprehensive care and case management approaches In hospital settings: Comprehensive discharge planning plus post-discharge support for older patients with CHF significantly reduced readmission rates 1 Operationalization of case management in daily clinical routines for inpatients reduced hospital length of stay from 7.34 days to 5.79 days 2 In the medical home: A PCMH in integrated group practice showed significant improvements in patients and providers experiences in the quality of clinical care 3 Clinical systems are associated with decreased use of inpatient and emergency care but not ambulatory care utilization in diabetes 4 Higher quality of care, reduced cost of care on some measures 5 In community-based settings: A review of available RCTs and comparative observational studies showed that community-based case management for frail elderly individuals can improve client psychological health or well-being and unmet service needs 6 17

18 Key Findings from Recognized Medical Homes PCMH 2011 Analysis Demographics N=1039 practices with NCQA PCMH-Recognition 71% achieved Level 3 Practice Size 2-4 clinicians (42%) 5-9 clinicians (26%) 10+ clinicians (11%) Majority (78%) serve both children and adults Practice Ownership Hospital/health plan (40%) Physician-Owned (38%) FQHC (22%) Military clinics and FQHC/CHC more likely to be Level 3 and have higher average total scores
 FQHC (22%) Military clinics and FQHC/CHC more likely to be Level 3 and have higher")
19 Challenges Most challenging elements that practices must pass to become recognized: 1. Using data to support population health: Generating lists, proactively reminding patients about needed services (2D) 2. Care management: Carrying out functions such as pre-visit preparation, providing written care plans (3C) 3. Referral tracking and follow up: Giving the receiving site reason for the referral, providing electronic summaries of care, tracking referral status (5B)

20 Challenges (continued) Elements where less than half of practices achieved full credit: 1. Electronic access: Providing patients with electronic access to their health information; e.g., test results, medication lists (PCMH 1C) 2. Referrals: Providing referrals to community resources (PCMH 4B) 3. Agreements: Establishing and documenting agreements with specialists if co-management needed (PCMH 5B)

21 Areas of High Performance More than 80% of practices achieved full credit on the following: 1. Continuity: Ensuring the patients have a consistent care team (PCMH 1D) 2. Care Management: Implementing evidence-based guidelines through point of care reminders (PCMH 3A) 3. Care Management: Managing medications including (PCMH 3D): Reconciliation during care transitions Assessing patient response to medications and barriers to adherence Documenting over the counter medication and supplements
22 Key Findings from Survey of Recognized Medical Home Practices Surveyed practices that achieved different levels of recognition under NCQA s PCMH standards 7 N= 249 recognized practices from 23 states
23 Lessons from Level 3 Medical Homes: Motivation to Change Theleaders of our efforts to improve care quality are enthusiastic about their task. Our practice operations rely heavily on organized systems. Our resources (personnel, time, financial) are too tightly limited to improve care quality now.
24 Lessons from Level 3 Medical Homes: Health Information Technology We had already had an electronic medical record system for a couple years, and we were sort of doing internal improvements and tracking, but when we decided to do this it became really apparent that there were other functionalities of this program that we could really utilize care management functionality that was innate in the electronic medical records program that we had, but we just hadn t really branched out to do yet. - NCQA Recognized Patient-Centered Medical Home
25 Lessons from Level 3 Medical Homes: Team-Based Care Utilizing staff to the maximum potential of their license (e.g. standing orders) Gives physician more time to address patient concerns Empowers staff Improves relationships between physician and staff Information and skills training to clinicians and staff
26 Lessons from Level 3 Medical Homes: Resources Participation in a demonstration/pilot project Payment for being a PCMH Incentives allowed practices to hire dedicated population health staff: Medical home assistant Care coordinator Phone nurse
27 Lessons from Level 3 Medical Homes: Formal Approach to Quality Improvement Level 3 practices tended to use the following strategies: Piloting changes before implementing them practice-wide Performance feedback to physicians
28 Future Holds Promise: Medical Homes Showing Positive Results Outcomes Improving quality of care Systematic reviews (AHRQ 2012) Moderately strong evidence of improvement PCPCC2012 Most state-based PCMH initiatives show improvement in quality Improvingpatient experience Moderately strong evidence of improvement Improved patient experience Reducingcost and utilization Inconclusive, absenceof data Most state-based PCMH initiatives show reduction of cost, ED visits and hospital use
29 Future Holds Promise: NCQA s 2014 standards will continue to drive capabilities further The Practice Team (PCMH 1G) Defining staff leading change effort Regular team meetings to discuss individual patients Using a regular method to evaluate teamness within practices Care Management (PCMH 3) Decoupling 3 important conditions from review of files for care management activities (3C) Practices will define criteria and identify patients most appropriate for these service Referral Tracking and Follow-Up (PCMH 5B) Establishing formal agreements with specialists (including behavioral health) Triaging referrals Sharing care plans
30 Future Holds Promise: Emphasis on Care/Case Management Increasing Affordable Care Act (ACA) initiatives aimed at care coordination include provisions for: Requiring CMS to reduce payment to hospitals with high readmissions Requiring health plan reporting on structures such as case management that improve health outcomes (Section 2717) Supporting the development of ACOs and PCMHs to emphasize the need for care coordination Payment models moving towards value assume or reward care/case management: ACO and MSSP quality measures and shared savings model imply population health infrastructure Commercial payment models that subsidize care/case management ($ and/or staff)
31 Implications for Combining Care Management and Case Management Approaches for Population Health Think about work flows related to care/case management Define roles needed to carry out functions Use each team member to the top of their license Have the right tools in place to support care management functions (e.g. EHRs/registries) Make sure those tools can help you to: Proactively identify patients Track referrals Think about how you can use technology to capture patient experience and communicate provider performance Participate in collaborative/payer initiatives to get support for implementation (e.g. dedicated nurse care manager) 31
32 Framework for Automating Care/Case Management 32
33 Sample Care Team Roles in 2 MD Practice 5000 PATIENTS 2 Primary Care MDs, 2 Medical Assistants No Disease (60%) With Disease (40%) Risk Level Well At-Risk High Risk Low Risk Mod Risk High Risk Segment 30% 25% 5% 27% 10% 3% # Patients Care Team Role 0 0 Health Coach 250case load 2000 cases/yr LPN 1000 case load 5000 cases/yr RN 500 case load 5000 cases/yr Case Manager 150case load 1000 cases/yr FTE
34 Optimize Care Team Roles with Automation Patient Service Representative or Medical Assistant Schedule visits and tests indicated in Phytel Outreach interface and Pre-Visit reports Send out pre-visit communications and conduct follow up using Phytel Campaigns Care Manager Stratify patients by risk using Coordinate reports and filters Use Campaign functions to reach out to subgroups of patients with care gaps Reinforce importance of proper diabetes management through personal and automated patient education Physician Review Phytel Registry reports for attributed patients Assign high risk patients to Care Manager using Phytel reports and filters Address all diabetes care opportunities at every encounter, even for non-diabetes visits, using Phytel Patient Care Summary CMO/Quality Committee Review performance on each clinical goal overall and by location and provider Meet with MDs and Care Teams at least monthly to review progress 34
35 Track Performance to Target Improvement Monitor Quality Performance Presents an integrated quality dashboard using EMR and clinical data Enables oversight of chronic and preventive care conditions Allows you to gauge practice effectiveness and help resolve care gaps Accurately measure practice performance Monitor individual care providers performance Compare effectiveness of quality programs Compare your organization against national averages Enables your care team to track several different programs with a set of conditions and metrics related to that quality initiatives Helps your practice qualify for medical home and P4P programs 35
36 Engage Patients with HIT Assists 1) All >9 A1c and no office visit are sent a text message to call care manager 2) All >9 and BMI >35 are sent an automated invitation to a group visit with a diabetes dietician 3) All between A1c 7 and 9 are sent an automated message to encourage visit website to take diabetes selfmanagement course 4) All diabetics <7.0 are sent an message emphasizing the importance of nutrition and exercise to maintain low A1c levels with a link to a mobile app to track their progress 36
37 Questions 37
38 References 1 Phillips, C., et al., Comprehensive Discharge Planning With Post-discharge Support for Older Patients With Congestive Heart Failure: A Meta-analysis. JAMA. 291(11), Kainzinger, Florian, et al., Optimization of hospital stay through length-of-stay-oriented case management: an empirical study. J Public Health.17: Reid, R., P. Fishman, O. Yu, T. Ross, J.T. Tufano Patient-Centered Medical Home Demonstration: A prospective, quasi-experimental, before and after evaluation. American Journal of Managed Care. 15(9), e71-e87. 4 Flottemesch, T., S.H. Scholle, P.J. O Connor, L. Solberg, S. Asche, L.G. Pawlson Are Characteristics of the Medical Home Associated with Diabetes Care Costs? Under review. 5 Grumbach, K., P. Grundy. Outcomes of Implementing Patient Centered Medical Home Interventions: A Review of the Evidence from Prospective Evaluation Studies in the United States. November 16, (January 12, 2011) 6 Emily Chuanmei You, Emily C. et al., Effects of case management in community aged care on client and carer outcomes: a systematic review of randomized trials and comparative observational studies. BMC Health Services Research. 12: Scholle, Sarah Hudson "Support and Strategies for Change Among Small Patient-Centered Medical Home Practices." Annals Of Family Medicine 11(Supplement 1). 38
Population Health Management: Using Quality Metrics to Drive Improved Patient Outcomes
 Executive Webinar Series Population Health Management: Using Quality Metrics to Drive Improved Patient Outcomes Presenters: Richard Hodach, MD, PhD, MPH Chief Medical Officer and VP, Clinical Product Strategy
Executive Webinar Series Population Health Management: Using Quality Metrics to Drive Improved Patient Outcomes Presenters: Richard Hodach, MD, PhD, MPH Chief Medical Officer and VP, Clinical Product Strategy
Idaho Health Home State Plan Amendment Matrix: Summary Overview. Overview of Approved Health Home SPAs
 Idaho Health Home State Plan Amendment Matrix: Summary Overview This matrix outlines key program design features from health home State Plan Amendments (SPAs) approved by the Centers for Medicare & Medicaid
Idaho Health Home State Plan Amendment Matrix: Summary Overview This matrix outlines key program design features from health home State Plan Amendments (SPAs) approved by the Centers for Medicare & Medicaid
Proven Innovations in Primary Care Practice
 Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Designing the Role of the Embedded Care Manager
 Designing the Role of the Embedded By Patricia Hines, Ph.D., RN and Marge Mercury, RN, MS, CMCE The Embedded The use of an Embedded ( ECM ) to coordinate within the complex delivery system is sharply increasing.
Designing the Role of the Embedded By Patricia Hines, Ph.D., RN and Marge Mercury, RN, MS, CMCE The Embedded The use of an Embedded ( ECM ) to coordinate within the complex delivery system is sharply increasing.
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION)
") ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
Building an Accountable Care Organization. Jean Malouin, MD MPH University of Michigan Health System September 21, 2012
 Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Abundant research comparing nations, states
 The Outcomes of Implementing Patient-Centered Medical Home Interventions: A Review of the Evidence on Quality, Access and Costs from Recent Prospective Evaluation Studies, August 2009 Prepared by Kevin
The Outcomes of Implementing Patient-Centered Medical Home Interventions: A Review of the Evidence on Quality, Access and Costs from Recent Prospective Evaluation Studies, August 2009 Prepared by Kevin
Population Health Solutions for Employers MEDIA RESOURCES
 Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Columbus Regional Health. Diabetes Educators designing programs using Health Coach extenders in the PCMH.
 Columbus Regional Health Diabetes Educators designing programs using Health Coach extenders in the PCMH. Objectives: Define what generated the need for the project. Discuss the delivery design model in
Columbus Regional Health Diabetes Educators designing programs using Health Coach extenders in the PCMH. Objectives: Define what generated the need for the project. Discuss the delivery design model in
Delivery System Innovation
 Healthcare Transformation Concepts and Definitions Our healthcare transformation process is invigorated by many stakeholders with differing backgrounds. To help them with new terms and all of us to use
Healthcare Transformation Concepts and Definitions Our healthcare transformation process is invigorated by many stakeholders with differing backgrounds. To help them with new terms and all of us to use
Patient Centered Medical Homes
 Patient Centered Medical Homes Paul Kleeberg, MD, FAAFP, FHIMSS CMIO Stratis Health North Dakota e-health Summit November 20, 2013 REACH - Achieving - Achieving meaningful meaningful use of your use EHR
Patient Centered Medical Homes Paul Kleeberg, MD, FAAFP, FHIMSS CMIO Stratis Health North Dakota e-health Summit November 20, 2013 REACH - Achieving - Achieving meaningful meaningful use of your use EHR
The Value Quadrant of Healthcare Reform. 2008 Pharos Innovations, LLC. All Rights Reserved.
 The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
Our Patient-Centered Medical Home a Process, not a Click
 Our Patient-Centered Medical Home a Process, not a Click Richard Johnston, M.D. President, Medical Clinic of North Texas, P.A. Medical Clinic of North Texas, P.A. MCNT Physician Owned Primary Care Medical
Our Patient-Centered Medical Home a Process, not a Click Richard Johnston, M.D. President, Medical Clinic of North Texas, P.A. Medical Clinic of North Texas, P.A. MCNT Physician Owned Primary Care Medical
Analytic-Driven Quality Keys Success in Risk-Based Contracts. Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst
 Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
AGENCY-SPECIFIC PLAN FOR THE NATIONAL QUALITY STRATEGY
 AGENCY-SPECIFIC PLAN FOR THE NATIONAL QUALITY STRATEGY Adult Medicaid Quality Grants Program The Adult Medicaid Quality Grants Program is a 2-year funding opportunity designed to support grantee Medicaid
AGENCY-SPECIFIC PLAN FOR THE NATIONAL QUALITY STRATEGY Adult Medicaid Quality Grants Program The Adult Medicaid Quality Grants Program is a 2-year funding opportunity designed to support grantee Medicaid
Prevea Health. Prevea Health automates population health management and improves health outcomes. Overview
 Prevea Health Prevea Health automates population health management and improves health outcomes Overview The need Prevea Health needed an infrastructure to help its physician practices automate population
Prevea Health Prevea Health automates population health management and improves health outcomes Overview The need Prevea Health needed an infrastructure to help its physician practices automate population
Population Health Management: Advancing Your Position in the Journey to Value-Based Care
 Population Health Management: Advancing Your Position in the Journey to Value-Based Care Webcast Session One: An Integrated Approach to Population Health Management 11 August 2015 Welcome & Introductions
Population Health Management: Advancing Your Position in the Journey to Value-Based Care Webcast Session One: An Integrated Approach to Population Health Management 11 August 2015 Welcome & Introductions
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment
 Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY
 A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases
 Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Game Changer at the Primary Care Practice Embedded Care Management. Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012
 Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Continuity of Care Guide for Ambulatory Medical Practices
 Continuity of Care Guide for Ambulatory Medical Practices www.himss.org t ra n sf o r m i ng he a lth c a re th rou g h IT TM Table of Contents Introduction 3 Roles and Responsibilities 4 List of work/responsibilities
Continuity of Care Guide for Ambulatory Medical Practices www.himss.org t ra n sf o r m i ng he a lth c a re th rou g h IT TM Table of Contents Introduction 3 Roles and Responsibilities 4 List of work/responsibilities
Medical Homes- Understanding the Model Bob Perna, MBA, FACMPE WSMA Practice Resource Center
 Bob Perna, MBA, FACMPE WSMA Practice Resource Center Bob Perna, MBA, FACMPE Senior Director, WSMA Practice Resource Center E-mail: rjp@wsma.org Phone: 206.441.9762 1.800.552.0612 2 Program Objectives:
Bob Perna, MBA, FACMPE WSMA Practice Resource Center Bob Perna, MBA, FACMPE Senior Director, WSMA Practice Resource Center E-mail: rjp@wsma.org Phone: 206.441.9762 1.800.552.0612 2 Program Objectives:
A white paper. Collaborative Accountable Care. CIGNA s Approach to Accountable Care Organizations. 841282 a 11/11
 A white paper Collaborative Accountable Care CIGNA s Approach to Accountable Care Organizations 841282 a 11/11 Transforming the Health Care System Successfully transforming the U.S. health care system
A white paper Collaborative Accountable Care CIGNA s Approach to Accountable Care Organizations 841282 a 11/11 Transforming the Health Care System Successfully transforming the U.S. health care system
I n t e r S y S t e m S W h I t e P a P e r F O R H E A L T H C A R E IT E X E C U T I V E S. In accountable care
 I n t e r S y S t e m S W h I t e P a P e r F O R H E A L T H C A R E IT E X E C U T I V E S The Role of healthcare InfoRmaTIcs In accountable care I n t e r S y S t e m S W h I t e P a P e r F OR H E
I n t e r S y S t e m S W h I t e P a P e r F O R H E A L T H C A R E IT E X E C U T I V E S The Role of healthcare InfoRmaTIcs In accountable care I n t e r S y S t e m S W h I t e P a P e r F OR H E
HEDIS 2012 Results
 Capital District Physicians Health Plan, Inc. Nonprofit Health Plan Albany, New York Capital District Physicians Health Plan, Inc. (CDPHP ) is featured as a high performer in cardiovascular care, identified
Capital District Physicians Health Plan, Inc. Nonprofit Health Plan Albany, New York Capital District Physicians Health Plan, Inc. (CDPHP ) is featured as a high performer in cardiovascular care, identified
December 23, 2010. Dr. David Blumenthal National Coordinator for Health Information Technology Department of Health and Human Services
 December 23, 2010 Dr. David Blumenthal National Coordinator for Health Information Technology Department of Health and Human Services RE: Prioritized measurement concepts Dear Dr. Blumenthal: Thank you
December 23, 2010 Dr. David Blumenthal National Coordinator for Health Information Technology Department of Health and Human Services RE: Prioritized measurement concepts Dear Dr. Blumenthal: Thank you
Hitting a Home Run: The Patient Centered Medical Home and Home Care
 Hitting a Home Run: The Patient Centered Medical Home and Home Care This paper has been prepared by the Home Care Alliance of Massachusetts to support home health agencies seeking to align with community
Hitting a Home Run: The Patient Centered Medical Home and Home Care This paper has been prepared by the Home Care Alliance of Massachusetts to support home health agencies seeking to align with community
ACO s as Private Label Insurance Products
 ACO s as Private Label Insurance Products Creating Value for Plan Sponsors Continuing Education: November 19, 2013 Clarence Williams Vice President Client Strategy Accountable Care Solutions Today s discussion
ACO s as Private Label Insurance Products Creating Value for Plan Sponsors Continuing Education: November 19, 2013 Clarence Williams Vice President Client Strategy Accountable Care Solutions Today s discussion
Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD)
") Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD) DuPage Medical Group Case Study Organization Profile Established in 1999, DuPage Medical Group (DMG) is a multispecialty
Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD) DuPage Medical Group Case Study Organization Profile Established in 1999, DuPage Medical Group (DMG) is a multispecialty
DSRIP QUARTERLY REVIEW PROCESS: Project Requirement - Timeframe. Project Requirement - Unit Level Reporting
 DSRIP QUARTERLY REVIEW PROCESS: PPSs will submit a quarterly report to the Independent Assessor throughout the DSRIP program via the automated MAPP tool which includes Domain 1 DSRIP Requirement Milestone
DSRIP QUARTERLY REVIEW PROCESS: PPSs will submit a quarterly report to the Independent Assessor throughout the DSRIP program via the automated MAPP tool which includes Domain 1 DSRIP Requirement Milestone
POPULATION HEALTH MANAGEMENT The Lynchpin of Emerging Healthcare Delivery Improve Patient Outcomes, Engage Physicians, and Manage Risk
 POPULATION HEALTH MANAGEMENT The Lynchpin of Emerging Healthcare Delivery Improve Patient Outcomes, Engage Physicians, and Manage Risk Julia Andrieni, MD, FACP Vice President, Population Health and Primary
POPULATION HEALTH MANAGEMENT The Lynchpin of Emerging Healthcare Delivery Improve Patient Outcomes, Engage Physicians, and Manage Risk Julia Andrieni, MD, FACP Vice President, Population Health and Primary
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT
 ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
CHAPTER 535 HEALTH HOMES. Background... 2. Policy... 2. 535.1 Member Eligibility and Enrollment... 2. 535.2 Health Home Required Functions...
 TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
Disease Management Identifications and Stratification Health Risk Assessment Level 1: Level 2: Level 3: Stratification
 Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
The Next Shiny Object: Understanding Accountable Care Organizations in the PCMH and Meaningful Use Context
 The Next Shiny Object: Understanding Accountable Care Organizations in the PCMH and Meaningful Use Context 1 The Next Shiny Object: Understanding Accountable Care Organizations in the PCMH and Meaningful
The Next Shiny Object: Understanding Accountable Care Organizations in the PCMH and Meaningful Use Context 1 The Next Shiny Object: Understanding Accountable Care Organizations in the PCMH and Meaningful
COMPARISON: PPC-PCMH 2008 With PCMH 2011
 COMPARISON: PPC-PCMH 008 With PCMH 011 About This Crosswalk The following crosswalk compares Physician Practice Connections Patient-Centered Medical Home (PPC -PCMH ) 008 with NCQA s Patient-Centered Medical
COMPARISON: PPC-PCMH 008 With PCMH 011 About This Crosswalk The following crosswalk compares Physician Practice Connections Patient-Centered Medical Home (PPC -PCMH ) 008 with NCQA s Patient-Centered Medical
How Health Reform Will Affect Health Care Quality and the Delivery of Services
 Fact Sheet AARP Public Policy Institute How Health Reform Will Affect Health Care Quality and the Delivery of Services The recently enacted Affordable Care Act contains provisions to improve health care
Fact Sheet AARP Public Policy Institute How Health Reform Will Affect Health Care Quality and the Delivery of Services The recently enacted Affordable Care Act contains provisions to improve health care
Realizing ACO Success with ICW Solutions
 Realizing ACO Success with ICW Solutions A Pathway to Collaborative Care Coordination and Care Management Decrease Healthcare Costs Improve Population Health Enhance Care for the Individual connect. manage.
Realizing ACO Success with ICW Solutions A Pathway to Collaborative Care Coordination and Care Management Decrease Healthcare Costs Improve Population Health Enhance Care for the Individual connect. manage.
Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination of care for both services.
 Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Advancing Health Equity. Through national health care quality standards
 Advancing Health Equity Through national health care quality standards TABLE OF CONTENTS Stage 1 Requirements for Certified Electronic Health Records... 3 Proposed Stage 2 Requirements for Certified Electronic
Advancing Health Equity Through national health care quality standards TABLE OF CONTENTS Stage 1 Requirements for Certified Electronic Health Records... 3 Proposed Stage 2 Requirements for Certified Electronic
Low-Hanging Fruit: Analytic Best Practices for Physician-Led ACOs
 Low-Hanging Fruit: Analytic Best Practices for Physician-Led ACOs MY BACKGROUND Practicing General Internal Medicine Physician Hospitalist at Newton-Wellesley Hospital Researcher at Brigham and Women s
Low-Hanging Fruit: Analytic Best Practices for Physician-Led ACOs MY BACKGROUND Practicing General Internal Medicine Physician Hospitalist at Newton-Wellesley Hospital Researcher at Brigham and Women s
2015 ACO Survey Results Webinar. September 8, 2015 12:30 2:00 pm ET
 2015 ACO Survey Results Webinar September 8, 2015 12:30 2:00 pm ET **Audio for this webinar streams through the web. Please make sure the sound on your computer is turned on and you have speakers. If you
2015 ACO Survey Results Webinar September 8, 2015 12:30 2:00 pm ET **Audio for this webinar streams through the web. Please make sure the sound on your computer is turned on and you have speakers. If you
Subcommittee on PCCM improvement
 Subcommittee on PCCM improvement Principles of Care Coordination Comprehensive services linked by an "integrator." Payments reflect patient complexity Current PCCM PCP office serves as care coordinator
Subcommittee on PCCM improvement Principles of Care Coordination Comprehensive services linked by an "integrator." Payments reflect patient complexity Current PCCM PCP office serves as care coordinator
Population Health Management Primer
 Population Health Management Primer A White Paper October 2014 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800- 680-7570 Impact- Advisors.com Table of Contents What Is Population
Population Health Management Primer A White Paper October 2014 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800- 680-7570 Impact- Advisors.com Table of Contents What Is Population
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Colorado Permanente Medical Group Denver, Colo. Kaiser Permanente is an integrated care delivery organization that provides care for over 9 million members across
Strengthening Primary Care for Patients: Colorado Permanente Medical Group Denver, Colo. Kaiser Permanente is an integrated care delivery organization that provides care for over 9 million members across
Strategies and Considerations for Extending EHR Technology to Affiliated Practices/Community Physicians
 Strategies and Considerations for Extending EHR Technology to Affiliated Practices/Community Physicians Dr. Phil Oravetz, MD, MPH, MBA Medical Director, Accountable Care Ochsner Health System Brad Boyd
Strategies and Considerations for Extending EHR Technology to Affiliated Practices/Community Physicians Dr. Phil Oravetz, MD, MPH, MBA Medical Director, Accountable Care Ochsner Health System Brad Boyd
6/12/2015. Dignity Health Population Health Management and Compliance Programs. Moving Towards Accountable Care. Dignity Health Poised for Innovation
 Dignity Health Population Health Management and Compliance Programs Julie Bietsch, VP Population Health Management Dawnese Kindelt, Senior Compliance Director, Clinical Integration June 8, 2015 Moving
Dignity Health Population Health Management and Compliance Programs Julie Bietsch, VP Population Health Management Dawnese Kindelt, Senior Compliance Director, Clinical Integration June 8, 2015 Moving
Guide to Population Health Management
 Guide to Population Health Management presented by the Healthcare Intelligence Network Note: This is an authorized excerpt from the Guide to Population Health Management. To download the entire guide,
Guide to Population Health Management presented by the Healthcare Intelligence Network Note: This is an authorized excerpt from the Guide to Population Health Management. To download the entire guide,
Optum One. The Intelligent Health Platform
 Optum One The Intelligent Health Platform The Optum One intelligent health platform enables healthcare providers to manage patient populations. The platform combines the industry s most advanced integrated
Optum One The Intelligent Health Platform The Optum One intelligent health platform enables healthcare providers to manage patient populations. The platform combines the industry s most advanced integrated
Enterprise Analytics Strategic Planning
 Enterprise Analytics Strategic Planning June 5, 2013 1 "The first question a data driven organization needs to ask itself is not "what do we think?" but rather "what do we know? Big Data: The Management
Enterprise Analytics Strategic Planning June 5, 2013 1 "The first question a data driven organization needs to ask itself is not "what do we think?" but rather "what do we know? Big Data: The Management
Greater New York Hospital Association. Emerging Positions in Primary Care: Results from the 2014 Ambulatory Care Workforce Survey
 Greater New York Hospital Association Emerging Positions in Primary Care: Results from the 2014 Ambulatory Care Workforce Survey Introduction.......................................................... 1
Greater New York Hospital Association Emerging Positions in Primary Care: Results from the 2014 Ambulatory Care Workforce Survey Introduction.......................................................... 1
Care Transitions. Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model. Share This
 Care Transitions Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model Brought to you by Amedisys: Architects of a leading patient-centered Care Transitions network.
Care Transitions Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model Brought to you by Amedisys: Architects of a leading patient-centered Care Transitions network.
The most significant challenge of becoming accountable is not forming an organization, it is forging one. ~ Phillip I. Roning 1
 Physician Involvement in ACOs The Time is Now Julian D. ( Bo ) Bobbitt, Jr., Esq. Smith, Anderson, Blount, Dorsett, Mitchell & Jernigan, L.L.P. Raleigh, NC The most significant challenge of becoming accountable
Physician Involvement in ACOs The Time is Now Julian D. ( Bo ) Bobbitt, Jr., Esq. Smith, Anderson, Blount, Dorsett, Mitchell & Jernigan, L.L.P. Raleigh, NC The most significant challenge of becoming accountable
Population Health Management & the Medical Neighborhood. Patient Centered Primary Care Collaborative Monthly National Briefing September 26, 2013
 Population Health Management & the Medical Neighborhood Patient Centered Primary Care Collaborative Monthly National Briefing September 26, 2013 Outline What is Population Health Management? Registries
Population Health Management & the Medical Neighborhood Patient Centered Primary Care Collaborative Monthly National Briefing September 26, 2013 Outline What is Population Health Management? Registries
Affordable Care - The Real Deal?
 PREPARING FOR ACCOUNTABLE CARE: COORDINATED CARE PREPARING FOR ACCOUNTABLE CARE: COORDINATED CARE Global Institute for Emerging Healthcare Practices Accountable care is more than a new program for Medicare
PREPARING FOR ACCOUNTABLE CARE: COORDINATED CARE PREPARING FOR ACCOUNTABLE CARE: COORDINATED CARE Global Institute for Emerging Healthcare Practices Accountable care is more than a new program for Medicare
Population Health Management Helps Utica Park Clinic Ease the Transition to Value-Based Care
 CASE STUDY Utica Park Clinic Population Health Management Helps Utica Park Clinic Ease the Transition to Value-Based Care The transition from fee-for-service to value-based reimbursement has been a challenge
CASE STUDY Utica Park Clinic Population Health Management Helps Utica Park Clinic Ease the Transition to Value-Based Care The transition from fee-for-service to value-based reimbursement has been a challenge
Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home
 104 A LOOK TO THE FUTURE Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home Background Management of chronic diseases can be challenging in primary care,
104 A LOOK TO THE FUTURE Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home Background Management of chronic diseases can be challenging in primary care,
1900 K St. NW Washington, DC 20006 c/o McKenna Long
 1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
Solutions. Health Advocate Chronic Care Management Program
 Solutions Health Advocate Chronic Care Management Program Taking Control Immunizations, preventive screenings and managing chronic conditions are key to controlling costs. Yet physicians often have limited
Solutions Health Advocate Chronic Care Management Program Taking Control Immunizations, preventive screenings and managing chronic conditions are key to controlling costs. Yet physicians often have limited
Nuts and Bolts Accountable Care Organizations: A New Care Delivery Model for New Expectations
 Nuts and Bolts Accountable Care Organizations: A New Care Delivery Model for New Expectations Presented to The American College of Cardiology October 27, 2012 1 Franciscan Alliance Overview Franciscan
Nuts and Bolts Accountable Care Organizations: A New Care Delivery Model for New Expectations Presented to The American College of Cardiology October 27, 2012 1 Franciscan Alliance Overview Franciscan
PCMH and Care Management: Where do we start?
 PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
Care Coordination: Case managers connect the dots in new delivery models
 The Pathway to Certfication is CCMC IssueBrief VOLUME 1, ISSUE 2 Care Coordination: Case managers connect the dots in new delivery models Well before health reform was signed into law, new models for health
The Pathway to Certfication is CCMC IssueBrief VOLUME 1, ISSUE 2 Care Coordination: Case managers connect the dots in new delivery models Well before health reform was signed into law, new models for health
Pediatricians Implement Office-based Care Management Guided by Meaningful and Actionable Population Health Management
 Pediatricians Implement Office-based Care Management Guided by Meaningful and Actionable Population Health Management Changing needs of technology and data for successful coordinated care transformation
Pediatricians Implement Office-based Care Management Guided by Meaningful and Actionable Population Health Management Changing needs of technology and data for successful coordinated care transformation
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
WHITE PAPER. How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience
 WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
The Cornerstones of Accountable Care ACO
 The Cornerstones of Accountable Care Clinical Integration Care Coordination ACO Information Technology Financial Management The Accountable Care Organization is emerging as an important care delivery and
The Cornerstones of Accountable Care Clinical Integration Care Coordination ACO Information Technology Financial Management The Accountable Care Organization is emerging as an important care delivery and
Primary Care, ACOs, and Payment Reform
 Primary Care, ACOs, and Payment Reform Mark McClellan, MD, PhD Director, Initiatives on Value and Innovation in Health Care Engelberg Center for Healthcare Reform Senior Fellow, Economic Studies The Brookings
Primary Care, ACOs, and Payment Reform Mark McClellan, MD, PhD Director, Initiatives on Value and Innovation in Health Care Engelberg Center for Healthcare Reform Senior Fellow, Economic Studies The Brookings
CCNC Care Management
 CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
Accountable Care Organization Workgroup Glossary
 Accountable Care Organization Workgroup Glossary Accountable care organization (ACO) a group of coordinated health care providers that care for all or some of the health care needs of a defined population.
Accountable Care Organization Workgroup Glossary Accountable care organization (ACO) a group of coordinated health care providers that care for all or some of the health care needs of a defined population.
An Introduction to HealthInfoNet s HIE Reporting & Analytics. 6th Annual APS Healthcare Maine Conference May 14, 2015
 An Introduction to HealthInfoNet s HIE Reporting & Analytics 6th Annual APS Healthcare Maine Conference May 14, 2015 Presentation Outline HealthInfoNet Background Current Status of health information exchange
An Introduction to HealthInfoNet s HIE Reporting & Analytics 6th Annual APS Healthcare Maine Conference May 14, 2015 Presentation Outline HealthInfoNet Background Current Status of health information exchange
Accountable Care Organizations and Patient-Centered Medical Homes
 Emerging Topics in Healthcare Reform Accountable Care Organizations and Patient-Centered Medical Homes Janssen Pharmaceuticals, Inc. Accountable Care Organizations and Patient-Centered Medical Homes The
Emerging Topics in Healthcare Reform Accountable Care Organizations and Patient-Centered Medical Homes Janssen Pharmaceuticals, Inc. Accountable Care Organizations and Patient-Centered Medical Homes The
Transitional Care Management
 Transitional Care Management HE ALTH SOLUTIONS consulting technology innovation A DIVISION OF AVASTONE TECHNOLOGIES, LLC I avastonetech.com/healthsolutions transitional care management I Avastone Health
Transitional Care Management HE ALTH SOLUTIONS consulting technology innovation A DIVISION OF AVASTONE TECHNOLOGIES, LLC I avastonetech.com/healthsolutions transitional care management I Avastone Health
Patient-Centered Medical Home and Meaningful Use
 Health Home Series: Patient-Centered Medical Home and Meaningful Use Presenters: Christine Stroebel, MPH, PCIP/NYC REACH Natalie Fuentes, MPH, PCIP/NYC REACH Alan Silver, MD, MPH/IPRO March 27, 2012, 2:00
Health Home Series: Patient-Centered Medical Home and Meaningful Use Presenters: Christine Stroebel, MPH, PCIP/NYC REACH Natalie Fuentes, MPH, PCIP/NYC REACH Alan Silver, MD, MPH/IPRO March 27, 2012, 2:00
Medical Home in the Context of ACOs, Healthcare Reform and the New Payment Environment
 Medical Home in the Context of ACOs, Healthcare Reform and the New Payment Environment Six Simple Rules For Successful Organizations In The New Payment Environment Bruce Bagley, M.D. Session Objectives
Medical Home in the Context of ACOs, Healthcare Reform and the New Payment Environment Six Simple Rules For Successful Organizations In The New Payment Environment Bruce Bagley, M.D. Session Objectives
Accountable Care Organizations
 Accountable Care Organizations Myth, Reality, Facts Why =System Failure Low Quality - IOM report High Cost Quality Cost disconnect Low Value Problems Disconnect between Quality and Cost Care is fragmented
Accountable Care Organizations Myth, Reality, Facts Why =System Failure Low Quality - IOM report High Cost Quality Cost disconnect Low Value Problems Disconnect between Quality and Cost Care is fragmented
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services
 GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
How MissionPoint Health is Using Population Health Insights to Achieve ACO Success
 How MissionPoint Health is Using Population Health Insights to Achieve ACO Success Background The United States spends more per capita on healthcare than other country, yet is ranked last among industrialized
How MissionPoint Health is Using Population Health Insights to Achieve ACO Success Background The United States spends more per capita on healthcare than other country, yet is ranked last among industrialized
NCQA INCLUDES ODS PROGRAM IN NATIONAL QUALITY LEADERSHIP PUBLICATION
 NCQA INCLUDES ODS PROGRAM IN NATIONAL QUALITY LEADERSHIP PUBLICATION The National Committee for Quality Assurance (NCQA) invited ODS to submit a case study for publication in its Quality Profiles: The
NCQA INCLUDES ODS PROGRAM IN NATIONAL QUALITY LEADERSHIP PUBLICATION The National Committee for Quality Assurance (NCQA) invited ODS to submit a case study for publication in its Quality Profiles: The
Patient Centered Medical Home and ACO: Emerging US care models and what might Canada have in common?
 Patient Centered Medical Home and ACO: Emerging US care models and what might Canada have in common? M. Turner Billingsley MD FACEP Chief Medical Officer, InterSystems Topics Patient Centered Medical Home
Patient Centered Medical Home and ACO: Emerging US care models and what might Canada have in common? M. Turner Billingsley MD FACEP Chief Medical Officer, InterSystems Topics Patient Centered Medical Home
APPENDIX C CROSSWALK OF PPC-PCMH-CMS STANDARDS AND ELEMENTS TO MEDICAL HOME CAPABILITIES BY TIER
 APPENDIX C CROSSWALK OF PPC-PCMH-CMS STANDARDS AND ELEMENTS TO MEDICAL HOME CAPABILITIES BY TIER C.3 Table C.1. Crosswalk Between Tier Definitions (Table 2) and PPC-PCMH-CMS (Appendix B) PPC-PCMH-CMS
APPENDIX C CROSSWALK OF PPC-PCMH-CMS STANDARDS AND ELEMENTS TO MEDICAL HOME CAPABILITIES BY TIER C.3 Table C.1. Crosswalk Between Tier Definitions (Table 2) and PPC-PCMH-CMS (Appendix B) PPC-PCMH-CMS
THE ROLE OF HEALTH INFORMATION TECHNOLOGY IN PATIENT-CENTERED CARE COLLABORATION. 2012 Louisiana HIPAA & EHR Conference Presenter: Chris Williams
 THE ROLE OF HEALTH INFORMATION TECHNOLOGY IN PATIENT-CENTERED CARE COLLABORATION 2012 Louisiana HIPAA & EHR Conference Presenter: Chris Williams Agenda Overview Impact of HIT on Patient-Centered Care (PCC)
THE ROLE OF HEALTH INFORMATION TECHNOLOGY IN PATIENT-CENTERED CARE COLLABORATION 2012 Louisiana HIPAA & EHR Conference Presenter: Chris Williams Agenda Overview Impact of HIT on Patient-Centered Care (PCC)
Partnerships in Primary and Behavioral Health Care ACO Survival Integrated Care
 Partnerships in Primary and Behavioral Health Care ACO Survival Integrated Care Ensuring Success for ACOs September 22 23 Joyce Wale LCSW Vice President, Institute for Behavioral Healthcare Improvement
Partnerships in Primary and Behavioral Health Care ACO Survival Integrated Care Ensuring Success for ACOs September 22 23 Joyce Wale LCSW Vice President, Institute for Behavioral Healthcare Improvement
North Shore Physicians Group Primary Care Redesign
 North Shore Physicians Group Primary Care Redesign Christine Sinsky, MD 12.23.11 The physician cannot do this work alone, notes Lindsay Gainer, Director of Clinical Services and Innovations at North Shore
North Shore Physicians Group Primary Care Redesign Christine Sinsky, MD 12.23.11 The physician cannot do this work alone, notes Lindsay Gainer, Director of Clinical Services and Innovations at North Shore
A Roadmap for Population Health: Best Practices for Achieving Operational Alignment
 RESEARCH BRIEF A Roadmap for Population Health: Best Practices for Achieving Operational Alignment Larry Yuhasz February 2014 Reform under the Patient Protection and Affordable Care Act (PPACA) demands
RESEARCH BRIEF A Roadmap for Population Health: Best Practices for Achieving Operational Alignment Larry Yuhasz February 2014 Reform under the Patient Protection and Affordable Care Act (PPACA) demands
How To Prepare For A Patient Care System
 Preparing for Online Communication with Your Patients A Guide for Providers This easy-to-use, time-saving guide is designed to help medical practices and community clinics prepare for communicating with
Preparing for Online Communication with Your Patients A Guide for Providers This easy-to-use, time-saving guide is designed to help medical practices and community clinics prepare for communicating with
Modern care management
 The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
Advanced Clinical Social Work Practice in Integrated Healthcare Module 1. Marion Becker, PhD School of Social Work University of South Florida
 Advanced Clinical Social Work Practice in Integrated Healthcare Module 1 Marion Becker, PhD School of Social Work University of South Florida Introduction to Integrated Healthcare and the Culture of Health
Advanced Clinical Social Work Practice in Integrated Healthcare Module 1 Marion Becker, PhD School of Social Work University of South Florida Introduction to Integrated Healthcare and the Culture of Health
What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company?
 What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Lisa Harvey McPherson RN, MBA, MPPM EMHS Vice President Continuum of Care & Chief Advocacy Officer Disclosures
What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Lisa Harvey McPherson RN, MBA, MPPM EMHS Vice President Continuum of Care & Chief Advocacy Officer Disclosures
Identifying High-Risk Medicare Beneficiaries with Predictive Analytics
 Identifying High-Risk Medicare Beneficiaries with Predictive Analytics September 2014 Until recently, with the passage of the Affordable Care Act (ACA), Medicare Fee-for-Service (FFS) providers had little
Identifying High-Risk Medicare Beneficiaries with Predictive Analytics September 2014 Until recently, with the passage of the Affordable Care Act (ACA), Medicare Fee-for-Service (FFS) providers had little
Care Coordination among DSRIP Partners
 Care Coordination among DSRIP Partners John F. Skip Williams, Jr., MD, EdD, MPH Maureen Fahey, RN, MBA Thursday, June 25, 2015 3:00-3:30 pm OVERVIEW OF PRESENTATION New York State DSRIP Overview Brooklyn
Care Coordination among DSRIP Partners John F. Skip Williams, Jr., MD, EdD, MPH Maureen Fahey, RN, MBA Thursday, June 25, 2015 3:00-3:30 pm OVERVIEW OF PRESENTATION New York State DSRIP Overview Brooklyn
Cornerstone Health Care s ACO Playbook. Grace E. Terrell, MD January 17, 2012
 Cornerstone Health Care s ACO Playbook Grace E. Terrell, MD January 17, 2012 Mission: To be your medical home Vision: To be the model for physician-led health care in America Values: As a physician owned
Cornerstone Health Care s ACO Playbook Grace E. Terrell, MD January 17, 2012 Mission: To be your medical home Vision: To be the model for physician-led health care in America Values: As a physician owned
10 Key Concepts for Higher Sales into ACOs
 By Michelle O Connor President and CEO By Michelle O Connor President and CEO CMR Institute Healthcare providers are under significant pressure from government payers, commercial health plans, and patients
By Michelle O Connor President and CEO By Michelle O Connor President and CEO CMR Institute Healthcare providers are under significant pressure from government payers, commercial health plans, and patients
NCQA PCMH 2011 Standards, Elements and Factors Documentation Guideline/Data Sources
 NCQA PCMH 2011 Standards, Elements and Factors Documentation Guideline/Data Sources Key: DP = Documented Process N/D = Report numerator and denominator creating percent of use RPT = Report of data or information
NCQA PCMH 2011 Standards, Elements and Factors Documentation Guideline/Data Sources Key: DP = Documented Process N/D = Report numerator and denominator creating percent of use RPT = Report of data or information
Member Health Management Programs
 Independent Health s Member Health Management Programs Helping employees manage their health. Helping you manage your costs. Independent Health s Member Health Management Programs A Comprehensive Approach...
Independent Health s Member Health Management Programs Helping employees manage their health. Helping you manage your costs. Independent Health s Member Health Management Programs A Comprehensive Approach...
Moving Toward Accountable Care Organizations in the States
 Moving Toward Accountable Care Organizations in the States Delivering on the Promise Medicaid Health Plans of America 2012 Annual Meeting Presented by Joyce Dubow October 24, 2012 Presentation overview
Moving Toward Accountable Care Organizations in the States Delivering on the Promise Medicaid Health Plans of America 2012 Annual Meeting Presented by Joyce Dubow October 24, 2012 Presentation overview
Health Care Homes Certification Assessment Tool- With Examples
 Guidelines: Health Care Homes Certification Assessment Form Structure: This is the self-assessment form that HCH applicants should use to determine if they meet the requirements for HCH certification.
Guidelines: Health Care Homes Certification Assessment Form Structure: This is the self-assessment form that HCH applicants should use to determine if they meet the requirements for HCH certification.
Optum One Life Sciences
 Optum One Life Sciences April 15, 2015 Creating a profound and lasting impact on the health system Lower the cost trend > $100 billion 22 hours per day > 50% > $80 billion Unnecessary costs due to improper
Optum One Life Sciences April 15, 2015 Creating a profound and lasting impact on the health system Lower the cost trend > $100 billion 22 hours per day > 50% > $80 billion Unnecessary costs due to improper
Patient Centered Medical Home: An Approach for the Health Plan
 : An Approach for the Health Plan By Marissa A. Harper and JoAnn E. Balara Excellence in healthcare consulting The Medical Home Concept Works Recent Medicare demonstration projects on Patient Centered
: An Approach for the Health Plan By Marissa A. Harper and JoAnn E. Balara Excellence in healthcare consulting The Medical Home Concept Works Recent Medicare demonstration projects on Patient Centered