First-line Hormone Therapy
|
|
|
- Frederick Stanley
- 8 years ago
- Views:
Transcription
1 First-line Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK

2 MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA only recurrence Asymptomatic metastases Symptomatic metastases Castration resistant Post docetaxel Palliative care years

3 Hormone Therapies for Prostate Cancer LHRH agonists. Prostap LHRH antagonists Androgen Receptor targeted.. Flutamide, Enzalutamide Steroids.. Oestrogens Cyp 17 inhibitors. eg Zoladex, eg Degarelix eg Casodex, eg Prednisone, Dexamethasone eg Stilboestrol eg Abiraterone,

4 Androgen Deprivation in M1 Disease James et al Eur Urol men with M1 disease treated in the control arm (Androgen Deprivation) Median FFS 11.2 months (IQR months) Median overall survival 42.1 months (IQR months)
 Median overall survival 42.1 months (IQR 22.7-90.")
5 Androgen Ablation in Prostate Cancer Loss of libido Loss of muscle mass Erectile dysfunction Insulin resistance Hot flushes Fatigue Cardiovascular effects Decreased bone mineral density

6 Diabetes and cardiovascular disease during androgen deprivation for prostate cancer Keating JNCI 2010 VA Study N=37443 diagnosis ; 14,597 had ADT. Mean observation 2.6 yrs. Rate of event/1000 patient years and adjusted Hazard Ratio Diabetes Incident CHD MI Sudden Cardiac Death No ADT LHRHa Orchidectomy Antiandrogen

7 Efsathiou JCO No. = 945 FU 8.1 yrs CVD = 117 At 9 yrs CVD 8% vs 11% In favour of LHRHa group

8 Osteoporosis and duration of LHRHa therapy Stage I- II Ca Prostate with PSA control Morote Eur Urol Prostatectomy controls (57) Men treated with LHRHa (53) Femoral neck bone densitometry Duration of hormone therapy None 12-36m 36-60m >60m Incidence of osteoporosis 28% 35% 42% 50% Relative risk of hip fracture Loss of bone mineral density particularly in first 6 12m (Daniell 2000, Mittan 2002) Osteoporotic fracture rate increased. 4% 5yr, 20% 10yr (Oefelein 2001)
 Osteoporotic fracture rate increased.")
9 Issues for Hormone Therapy in Metastatic Prostate Cancer 1 Type of hormone therapy 2 Combined androgen blockade? 3 Immediate vs Deferred in asymptomatic patients? 4 Intermittent or continuous? 5 Combine with other treatment eg chemotherapy, bone targeting agents, newer AR targeted drugs, radiotherapy to the primary site? 6 Role with RT to the primary?

10 1. A randomised comparison of 'Casodex' (bicalutamide) 150 mg monotherapy versus castration in the treatment of metastatic and locally advanced prostate cancer patients with locally advanced or metastatic prostate cancer. Less hot flushes and improved physical activity and sexual health on bicalutamide. In M1 disease bicalutamide was less effective (HR for mortality 1.3) No difference in the 480 men with locally 2000 M1 patients Casodex less effective than androgen ablation Tyrrell et al 1998

11
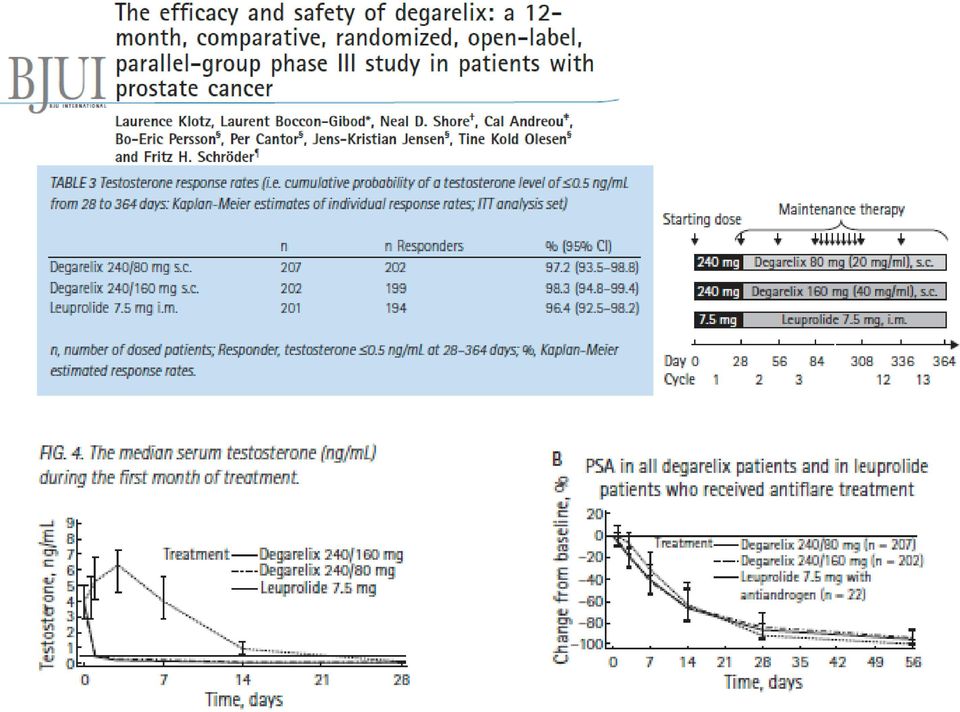
12 Degarelix CS21 and Extension Trial Crawford et al 2014 brfs Degarelix had better PSA-RFS at 12 months-no OS difference No overall difference? as crossover at 12 months Role in emergencies eg impending SCC? Role in intermittent therapy? More effective at PSA control (possible due to FSH suppression) BUT only monthly prep. And more injection site reactions

13 2. COMBINED ANDROGEN BLOCKADE Samson et al 2002 Modest benefit at 5 years probable outweighed by increased side-effects

14 3. Immediate versus deferred treatment for advanced prostatic cancer: initial results of the Medical Research Council Trial. The Medical Research Council Prostate Cancer Working Party Investigators Group. Br J Urol Feb;79(2): men with locally-advanced or metastatic prostate cancer Randomised to immediate or deferred treatment (orchx or LHRH) Deferred patients had more prostate cancer deaths (257 vs 203 (p=0.001) Also more TURPs, pathological fractures, spinal cord compressions. BUT 1. Pre PSA and 29 deferred patients died from prostate cancer without having started hormone treatment! Deferred treatment remains an option for selected indolent cases
 Also more TURPs, pathological fractures, spinal cord compressions. BUT 1.")
15 3. EARLY VERSUS DELAYED ENDOCRINE TREATMENT OF pn1-3 M0 PROSTATE CANCER---Schroeder et al 2004 for EORTC 234 node positive patients having no local prostate treatment were randomised to immediate or deferred hormones Median survivals: Early-7.8 yrs Delayed 6.2 yrs Underpowered. Trend to improved survival with early treatment-hr 1.23 (95%ci ) but Delayed Treatment remains an option.

16 3. Immediate vs deferred hormone therapy in 985 men with M0 prostate cancer who had refused or were unsuitable for radical treatment. RESULT HR 1.25 for OS favours immediate treatment. BUT Prostate cancer deaths deaths-no difference Other cause Time to hormone therapy in deferred patients EORTC Studer et al 2006 JCO 24;

17 4. Intermittent Androgen Suppression vs Continuous Androgen Deprivation PSA progression after local Rx; 2012 Crook et al NEJM Equivalent efficacy and Intermittent Hormones had improved Quality of Life

18 4. BUT Intermittent versus Continuous Androgen Deprivation in M1 Prostate Cancer. Hussain et al 2013 NEJM Randomised after 7 months combined androgen blockade IF PSA 4 Hazard Ratio 1.1 (95% CI ) As CI exceeded 20% detriment, it CANNOT be concluded that Intermittent therapy is not inferior. Therefore Intermittent Hormones NOT standard in M1 disease.
 As CI exceeded 20% detriment, it CANNOT be concluded that Intermittent therapy is not")
19 5. Adding treatments to androgen deprivation. STAMPEDE trial of celecoxib, Lancet Oncology 2012

20 Gravis G, Fizazi K et al Lancet Oncol 385 M1 hormone-naïve: randomised (median FU 50 months). No difference in overall survival (59 vs 54 months) PSA- PFS OS Median 23 v 13 months p=0.005

21 Docetaxel in hormone-naive metastatic prostate cancer. CHAARTED Trial: Sweeney et al ASCO 2014 Improved Overall Survival by 13 months!! Significant in High Volume subgroup. And improved time to develop CRPC by 6.7 months and TTP (imaging) by 13 months
22 OS by extent of metastatic disease at start of ADT High volume Low volume Probability p= HR=0.60 ( ) Median OS: ADT + D: 49.2 months ADT alone: 32.2 months Probability p= HR=0.63 ( ) Median OS: ADT + D: Not reached ADT alone: Not reached OS (Months) OS (Months) In patients with high volume metastatic disease, there is a 17 month improvement in median overall survival from 32.2 months to 49.2 months We projected 33 months in ADT alone arm with collaboration of SWOG9346 team Presented by: Christopher J. Sweeney, MBBS
23 OVERALL SURVIVAL HIGH VOLUME METASTASES GETUG-15 update MedSubgroup Analysis of «High Volume» ian follow-up: 84.0 months [ Median OS ADT alone: 35.1 [ ] ADT + D: 39 [ ] HR: 0.8 [ ] Median p=0.35 OS ADT alone: 35.1 [ ] ADT + D: 39 [ ] HR: 0.8 [ ] p=0.35 Fizazi GU ASCO 2015 median FU 83 months Subgroup analysis of those with High-Volume metastases.
24 5. CHAARTED and GETUG-15: differences Ack: David Dearnaley Presenting features CHAARTED GETUG-15 Geography N.America France/Belgium Recruitment period Number Follow-up 29 months 50 months Risk groups: High 66% 22% PSA at entry 53ng/ml 26ng/ml Outcomes OS ADT+D vs ADT 58m vs 44m 59m vs 54m ( median FFS 21m vs 15m 23m vs 13m ) Time from failure to death 37m vs 29m 36m vs 41m Surprising that in CHAARTED there was shorter survival after failure in the patients who had not yet had Docetaxel
25 5. Reasons why Overall Survival conclusion might differ in GETUG vs CHAARTED Trial populations? CHAARTED had a high proportion of poor risk patients. Chance? the OS hazard ratio in GETUG included within the 95%confidence intervals a possible 36% benefit Additional effective post-docetaxel therapies in CHAARTED trial? Possibility that more abiraterone, enzalutamide, cabazitaxel were given in the docetaxel arm? STAMPEDE result due ASCO 2015
26 6 Role of radiotherapy to the primary in patients with metastases? Mouse models of metastasis. Factors secreted by the primary tumors (e.g., VEGF-A, PlGF, PSAP) are thought to mobilize bone marrow derived cells that are subsequently attracted to premetastatic sites. The cells of this premetastatic niche then release factors that can attract disseminating tumor cells
27 PSA recurrence WIDMARK Lancet Death from CaP 24% vs 12% RR 0.44 p< % vs 26% RR 0.16 p< Result supported by Warde et al for NCIC/MRC 2011 Lancet. n=1205. Survival benefit in a similar trial. Also by STAMPEDE non-randomised result in either N0 or N1 patients (ESMO 2014)
28 6. STAMPEDE FROM 2014
29 PEACE-1: European Phase III Trial of Abiraterone Acetate in patients with newly diagnosed (hormonenaïve) metastatic prostate cancer Androgen deprivation therapy (ADT) Patients with newly diagnosed metastatic prostate cancer R A N D O M I Z E D ADT + Abiraterone 1000mg Prednisone 5mg BID ADT + Local radiotherapy Co-primary endpoints: OS and PFS (HR: 075) n= 916 planned patients ADT + Local radiotherapy + Abiraterone 1000 mg Prednisone 5mg BID 2x2 design Study sponsor: Unicancer Courtesy of K Fizazi
30 Conclusions Hormone therapy is a highly effective initial systemic treatment for prostate cancer. It is a low toxicity treatment but there are impacts on quality of life. Single modality androgen deprivation is the standard of care for initial Rx of M1 disease. Variations such as deferred or intermittent treatment or combination with Docetaxel are options to discuss with your patients.
Should we use Docetaxel in hormone- naïve prostate cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
 Should we use Docetaxel in hormone- naïve prostate cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards/honorarium from: Amgen, Astellas,
Should we use Docetaxel in hormone- naïve prostate cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards/honorarium from: Amgen, Astellas,
Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC)
") Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC) FDA Presentation ODAC Meeting September 14, 2011 1 Review Team Paul G. Kluetz,
Issues Concerning Development of Products for Treatment of Non-Metastatic Castration- Resistant Prostate Cancer (NM-CRPC) FDA Presentation ODAC Meeting September 14, 2011 1 Review Team Paul G. Kluetz,
Thomas de los Reyes PGY 1 Department of Urologic Sciences University of British Columbia. Meet Mr. S
 Thomas de los Reyes PGY 1 Department of Urologic Sciences University of British Columbia Meet Mr. S 74 M admitted for back pain X-ray: sclerotic lesions along spine PSA 800 Nuclear Medicine Bone Scan 1
Thomas de los Reyes PGY 1 Department of Urologic Sciences University of British Columbia Meet Mr. S 74 M admitted for back pain X-ray: sclerotic lesions along spine PSA 800 Nuclear Medicine Bone Scan 1
Kanıt: Klinik çalışmalarda ZYTIGA
 mkdpk de Sonunda Gerçek İlerleme! Kanıt: Klinik çalışmalarda ZYTIGA Dr. Sevil Bavbek 5. Türk Tıbbi Onkoloji Kongresi Mart 214, Antalya Endocrine therapies Adrenals Testis Abiraterone Orteronel Androgen
mkdpk de Sonunda Gerçek İlerleme! Kanıt: Klinik çalışmalarda ZYTIGA Dr. Sevil Bavbek 5. Türk Tıbbi Onkoloji Kongresi Mart 214, Antalya Endocrine therapies Adrenals Testis Abiraterone Orteronel Androgen
Advances In Chemotherapy For Hormone Refractory Prostate Cancer. TAX 327 study results & SWOG 99-16 study results presented at ASCO 2004
 Ronald de Wit Rotterdam Cancer Institute The Netherlands Advances In Chemotherapy For Hormone Refractory Prostate Cancer TAX 327 study results & SWOG 99-16 study results presented at Slide 1 Prostate Cancer
Ronald de Wit Rotterdam Cancer Institute The Netherlands Advances In Chemotherapy For Hormone Refractory Prostate Cancer TAX 327 study results & SWOG 99-16 study results presented at Slide 1 Prostate Cancer
Updates in Prostate Cancer Therapy Sequencing Strategies. Debates and Didactics in Hematology and Oncology. July 26, 2015.
 Updates in Prostate Cancer Therapy Sequencing Strategies Debates and Didactics in Hematology and Oncology July 26, 2015. Sea Island, GA Bradley C. Carthon, MD. Ph.D. Assistant Professor, Winship Cancer
Updates in Prostate Cancer Therapy Sequencing Strategies Debates and Didactics in Hematology and Oncology July 26, 2015. Sea Island, GA Bradley C. Carthon, MD. Ph.D. Assistant Professor, Winship Cancer
7. Prostate cancer in PSA relapse
 7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
Prostate cancer OLD PROBLEMS AND NEW DIRECTIONS. Liam Bourke PhD Mres BSc (Hons) FRSPH Queen Mary University of London l.bourke@qmul.ac.
 FRSPH Queen Mary University of London l.bourke@qmul.ac.") Prostate cancer OLD PROBLEMS AND NEW DIRECTIONS Liam Bourke PhD Mres BSc (Hons) FRSPH Queen Mary University of London l.bourke@qmul.ac.uk What s this talk about? OLD PROBLEMS: Advancing prostate cancer
Prostate cancer OLD PROBLEMS AND NEW DIRECTIONS Liam Bourke PhD Mres BSc (Hons) FRSPH Queen Mary University of London l.bourke@qmul.ac.uk What s this talk about? OLD PROBLEMS: Advancing prostate cancer
Prostate Cancer: Current Approach and Future Perspective in Castration-resistant Cancer Treatment
 Prostate Cancer: Current Approach and Future Perspective in Castration-resistant Cancer Treatment Abstract Prostate is one of the most commonly diagnosed solid tumours in males worldwide. Selection of
Prostate Cancer: Current Approach and Future Perspective in Castration-resistant Cancer Treatment Abstract Prostate is one of the most commonly diagnosed solid tumours in males worldwide. Selection of
Everolimus plus exemestane for second-line endocrine treatment of oestrogen receptor positive metastatic breast cancer
 LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW Everolimus plus exemestane for second-line endocrine treatment of oestrogen receptor positive metastatic breast cancer Everolimus plus exemestane for second-line
LONDON CANCER NEWS DRUGS GROUP RAPID REVIEW Everolimus plus exemestane for second-line endocrine treatment of oestrogen receptor positive metastatic breast cancer Everolimus plus exemestane for second-line
Evaluation of Treatment Pathways in Oncology: An Example in mcrpc
 Evaluation of Treatment Pathways in Oncology: An Example in mcrpc Sonja Sorensen, MPH United BioSource Corporation Bethesda, MD 1 Objectives Illustrate selection of modeling approach for evaluating pathways
Evaluation of Treatment Pathways in Oncology: An Example in mcrpc Sonja Sorensen, MPH United BioSource Corporation Bethesda, MD 1 Objectives Illustrate selection of modeling approach for evaluating pathways
What s new in prostate cancer research? Highlights of GU-ASCO 2014
 review What s new in prostate cancer research? Highlights of GU-ASCO 2014 Cite as: Can Urol Assoc J 2014;8(3-4Suppl2):S8-12. http://dx.doi.org/10.5489/cuaj.2013 Published online April 14, 2014. Abstract
review What s new in prostate cancer research? Highlights of GU-ASCO 2014 Cite as: Can Urol Assoc J 2014;8(3-4Suppl2):S8-12. http://dx.doi.org/10.5489/cuaj.2013 Published online April 14, 2014. Abstract
Establishing an Advanced Prostate Cancer Clinic: The Rationale
 The information, views and opinions expressed in this presentation and any accompanying materials are those of the speaker and do not necessarily reflect the views or position of Cardinal Health or VitalSource.
The information, views and opinions expressed in this presentation and any accompanying materials are those of the speaker and do not necessarily reflect the views or position of Cardinal Health or VitalSource.
SIOG Guidelines Update 2014 Prostate Cancer. Dr Helen Boyle Centre Léon Bérard SIOG meeting 25 October 2014,Lisbon
 SIOG Guidelines Update 2014 Prostate Cancer Dr Helen Boyle Centre Léon Bérard SIOG meeting 25 October 2014,Lisbon Droz JP, Aapro M, Balducci L, Boyle H, Van den Broeck T, Cathcart P, Dickinson L, Efstathiou
SIOG Guidelines Update 2014 Prostate Cancer Dr Helen Boyle Centre Léon Bérard SIOG meeting 25 October 2014,Lisbon Droz JP, Aapro M, Balducci L, Boyle H, Van den Broeck T, Cathcart P, Dickinson L, Efstathiou
2015 ASCO Conference Highlights for PCa Patients: May 29-June 2 Chicago, IL. Howard R. Soule, PhD
 2015 ASCO Conference Highlights for PCa Patients: May 29-June 2 Chicago, IL Howard R. Soule, PhD 1 May 29-June 2, 2015 Chicago, IL Theme: Illumination and Innovation Transforming Data Into Learning We
2015 ASCO Conference Highlights for PCa Patients: May 29-June 2 Chicago, IL Howard R. Soule, PhD 1 May 29-June 2, 2015 Chicago, IL Theme: Illumination and Innovation Transforming Data Into Learning We
Monitoring of Prostate Cancer Patients: Guidelines and Current Practice
 european urology supplements 6 (2007) 829 833 available at www.sciencedirect.com journal homepage: www.europeanurology.com Monitoring of Prostate Cancer Patients: Guidelines and Current Practice Laurent
european urology supplements 6 (2007) 829 833 available at www.sciencedirect.com journal homepage: www.europeanurology.com Monitoring of Prostate Cancer Patients: Guidelines and Current Practice Laurent
Advances in Prostate Cancer (Localized to Newly metastatic) Christopher Sweeney, MBBS Dana Farber Cancer Institute
 Christopher Sweeney, MBBS Dana Farber Cancer Institute") Advances in Prostate Cancer (Localized to Newly metastatic) Christopher Sweeney, MBBS Dana Farber Cancer Institute Prostate Cancer: A Diseases with Many States Organ Confined Low Risk Clinically Localized
Advances in Prostate Cancer (Localized to Newly metastatic) Christopher Sweeney, MBBS Dana Farber Cancer Institute Prostate Cancer: A Diseases with Many States Organ Confined Low Risk Clinically Localized
Prostate Cancer Treatment: What s Best for You?
 Prostate Cancer Treatment: What s Best for You? Prostate Cancer: Radiation Therapy Approaches I. Choices There is really a variety of options in prostate cancer management overall and in radiation therapy.
Prostate Cancer Treatment: What s Best for You? Prostate Cancer: Radiation Therapy Approaches I. Choices There is really a variety of options in prostate cancer management overall and in radiation therapy.
KELOWNA PROSTATE CANCER SUPPORT & AWARENESS GROUP NEWSLETTER
 KELOWNA PROSTATE CANCER SUPPORT & AWARENESS GROUP NEWSLETTER OKANAGAN PROSTATE RESOURCE CENTRE SOCIETY Okanagan Prostate Resource Centre To make an Appointment Call 250-712-2002 E-mail oprc@telus.net CCS
KELOWNA PROSTATE CANCER SUPPORT & AWARENESS GROUP NEWSLETTER OKANAGAN PROSTATE RESOURCE CENTRE SOCIETY Okanagan Prostate Resource Centre To make an Appointment Call 250-712-2002 E-mail oprc@telus.net CCS
Prostate Cancer. Screening and Diagnosis. Screening. Pardeep Kumar Consultant Urological Surgeon
 The Royal Marsden Prostate Cancer Screening and Diagnosis Pardeep Kumar Consultant Urological Surgeon Prostate Cancer Screening and Diagnosis 08 02 2013 2 Screening 1 3 Q1.Lots of men have prostate cancer
The Royal Marsden Prostate Cancer Screening and Diagnosis Pardeep Kumar Consultant Urological Surgeon Prostate Cancer Screening and Diagnosis 08 02 2013 2 Screening 1 3 Q1.Lots of men have prostate cancer
NHS England Reference: [B15/PS/a]
![NHS England Reference: [B15/PS/a]](/thumbs/37/17792575.jpg "NHS England Reference: [B15/PS/a]") Clinical Commissioning Policy Statement: Docetaxel in combination with androgen deprivation therapy for the treatment of hormone naïve metastatic prostate cancer NHS England Reference: [B15/PS/a] NHS England
Clinical Commissioning Policy Statement: Docetaxel in combination with androgen deprivation therapy for the treatment of hormone naïve metastatic prostate cancer NHS England Reference: [B15/PS/a] NHS England
Drug costs in the management of metastatic castration-resistant prostate cancer in Canada
 Dragomir et al. BMC Health Services Research 2014, 14:252 RESEARCH ARTICLE Drug costs in the management of metastatic castration-resistant prostate cancer in Canada Alice Dragomir 1,2*, Daniela Dinea 1,3,
Dragomir et al. BMC Health Services Research 2014, 14:252 RESEARCH ARTICLE Drug costs in the management of metastatic castration-resistant prostate cancer in Canada Alice Dragomir 1,2*, Daniela Dinea 1,3,
SRO Tutorial: Prostate Cancer Treatment Options
 SRO Tutorial: Prostate Cancer Treatment Options May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible,
SRO Tutorial: Prostate Cancer Treatment Options May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible,
Clinical Trials and Radiation Treatment. Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto
 Clinical Trials and Radiation Treatment Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto What I will cover.. A little about radiation treatment The clinical trials
Clinical Trials and Radiation Treatment Gerard Morton Odette Cancer Centre Sunnybrook Research Institute University of Toronto What I will cover.. A little about radiation treatment The clinical trials
Treatment of Metastatic Breast Cancer: Endocrine Therapies. Robert W. Carlson, M.D. Professor of Medicine Stanford University
 Treatment of Metastatic Breast Cancer: Endocrine Therapies Robert W. Carlson, M.D. Professor of Medicine Stanford University MDACC Experience with FAC in Chemotherapy-Naive MBC Greenberg et al, J Clin
Treatment of Metastatic Breast Cancer: Endocrine Therapies Robert W. Carlson, M.D. Professor of Medicine Stanford University MDACC Experience with FAC in Chemotherapy-Naive MBC Greenberg et al, J Clin
Prostate Cancer. Ravi A. Madan, MD Clinical Director Genitourinary Malignancies Branch National Cancer Institute
 Prostate Cancer Ravi A. Madan, MD Clinical Director Genitourinary Malignancies Branch National Cancer Institute 1 Educational Objectives By the end of this session, participants should be able to Understand
Prostate Cancer Ravi A. Madan, MD Clinical Director Genitourinary Malignancies Branch National Cancer Institute 1 Educational Objectives By the end of this session, participants should be able to Understand
Us TOO University Presents: Estrogen Deficiency Side Effects Due to Androgen Deprivation Therapy
 Us TOO University Presents: Estrogen Deficiency Side Effects Due to Androgen Deprivation Therapy Today s speaker is Samir Taneja, MD Program moderator is Pam Barrett, Us TOO International Made possible
Us TOO University Presents: Estrogen Deficiency Side Effects Due to Androgen Deprivation Therapy Today s speaker is Samir Taneja, MD Program moderator is Pam Barrett, Us TOO International Made possible
PROSTATE CANCER. Learning Objectives. Question 4/3/2014
 PROSTATE CANCER Lindsay Kaster, PharmD Clinical Oncology Pharmacist Boise VA Medical Center Learning Objectives Discuss the cancer diagnosis and screening, including the role of Prostate Specific Antigen
PROSTATE CANCER Lindsay Kaster, PharmD Clinical Oncology Pharmacist Boise VA Medical Center Learning Objectives Discuss the cancer diagnosis and screening, including the role of Prostate Specific Antigen
Hormone therapy and breast cancer: conflicting evidence. Cindy Farquhar Cochrane Menstrual Disorders and Subfertility Group
 Hormone therapy and breast cancer: conflicting evidence Cindy Farquhar Cochrane Menstrual Disorders and Subfertility Group The world of hormone therapy in the 1990 s Throughout the 1970s, 1980s and 1990s
Hormone therapy and breast cancer: conflicting evidence Cindy Farquhar Cochrane Menstrual Disorders and Subfertility Group The world of hormone therapy in the 1990 s Throughout the 1970s, 1980s and 1990s
People Living with Cancer
 Patient Guide ASCOInformation for People Living with Cancer HORMONE THERAPY FOR ADVANCED PROSTATE CANCER Recommendations of the American Society of Clinical Oncology Welcome The American Society of Clinical
Patient Guide ASCOInformation for People Living with Cancer HORMONE THERAPY FOR ADVANCED PROSTATE CANCER Recommendations of the American Society of Clinical Oncology Welcome The American Society of Clinical
Traitement médical du Cancer de la Prostate: du désert à la profusion. Prof. Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
 Traitement médical du Cancer de la Prostate: du désert à la profusion Prof. Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation in advisory boards or as a speaker for:
Traitement médical du Cancer de la Prostate: du désert à la profusion Prof. Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation in advisory boards or as a speaker for:
Neoadjuvant and Adjuvant Hormone Therapy: How and When?
 european urology supplements 7 (2008) 747 751 available at www.sciencedirect.com journal homepage: www.europeanurology.com Neoadjuvant and Adjuvant Hormone Therapy: How and When? Hein Van Poppel * Department
european urology supplements 7 (2008) 747 751 available at www.sciencedirect.com journal homepage: www.europeanurology.com Neoadjuvant and Adjuvant Hormone Therapy: How and When? Hein Van Poppel * Department
Before, Frank's immune cells could
 Before, Frank's immune cells could barely recognize a prostate cancer cell. Now, they are focused on it. Stimulate an immune response against advanced prostate cancer Extend median survival beyond 2 years
Before, Frank's immune cells could barely recognize a prostate cancer cell. Now, they are focused on it. Stimulate an immune response against advanced prostate cancer Extend median survival beyond 2 years
Cancer research in the Midland Region the prostate and bowel cancer projects
 Cancer research in the Midland Region the prostate and bowel cancer projects Ross Lawrenson Waikato Clinical School University of Auckland MoH/HRC Cancer Research agenda Lung cancer Palliative care Prostate
Cancer research in the Midland Region the prostate and bowel cancer projects Ross Lawrenson Waikato Clinical School University of Auckland MoH/HRC Cancer Research agenda Lung cancer Palliative care Prostate
Patient & Family Guide 2015 Hormone Therapy for Prostate Cancer
 Patient & Family Guide 2015 Hormone Therapy for Prostate Cancer www.nshealth.ca Hormone Therapy for Prostate Cancer What is the prostate? The prostate is one of the male sex glands. It makes seminal fluid
Patient & Family Guide 2015 Hormone Therapy for Prostate Cancer www.nshealth.ca Hormone Therapy for Prostate Cancer What is the prostate? The prostate is one of the male sex glands. It makes seminal fluid
NCCN Prostate Cancer Guidelines Update. James L. Mohler, MD Roswell Park Cancer Institute
 NCCN Prostate Cancer Guidelines Update James L. Mohler, MD Roswell Park Cancer Institute Every 2.5 Minutes an American is Diagnosed with Prostate Cancer Every 15 Minutes an American Dies of Prostate Cancer
NCCN Prostate Cancer Guidelines Update James L. Mohler, MD Roswell Park Cancer Institute Every 2.5 Minutes an American is Diagnosed with Prostate Cancer Every 15 Minutes an American Dies of Prostate Cancer
American Urological Association (AUA) Guideline
 Guideline") 1 Approved by the AUA Board of Directors April 2015 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2015 by the American Urological
1 Approved by the AUA Board of Directors April 2015 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2015 by the American Urological
Clinical guideline Published: 8 January 2014 nice.org.uk/guidance/cg175
 Prostate cancer: diagnosis and management Clinical guideline Published: 8 January 2014 nice.org.uk/guidance/cg175 NICE 2014. All rights reserved. Contents Introduction... 4 Drug recommendations... 5 Patient-centred
Prostate cancer: diagnosis and management Clinical guideline Published: 8 January 2014 nice.org.uk/guidance/cg175 NICE 2014. All rights reserved. Contents Introduction... 4 Drug recommendations... 5 Patient-centred
Therapy in Prostate Cancer: Cure or Regression
 Therapy in Prostate Cancer: Cure or Regression F. Di Silverio Department of Urologia U Bracci University La Sapienza Rome Objectives and classification of the results obtained from therapies in oncology
Therapy in Prostate Cancer: Cure or Regression F. Di Silverio Department of Urologia U Bracci University La Sapienza Rome Objectives and classification of the results obtained from therapies in oncology
What is the goal after hormone therapy: PSA or testosterone? 삼성서울병원 서성일
 What is the goal after hormone therapy: PSA or testosterone? 삼성서울병원 서성일 Huggins & Hodges s study in the 1940s. Testosterone (T) became as a key therapeutic target, and ADT to lower serum T remains standard
What is the goal after hormone therapy: PSA or testosterone? 삼성서울병원 서성일 Huggins & Hodges s study in the 1940s. Testosterone (T) became as a key therapeutic target, and ADT to lower serum T remains standard
Hormone Therapy and Prostate Cancer
 Drug therapy Hormone Therapy and Prostate Cancer Hormone Therapy and Prostate Cancer This factsheet will help you to understand more about hormone therapy for prostate cancer. It describes the types of
Drug therapy Hormone Therapy and Prostate Cancer Hormone Therapy and Prostate Cancer This factsheet will help you to understand more about hormone therapy for prostate cancer. It describes the types of
DECISION AND SUMMARY OF RATIONALE
 DECISION AND SUMMARY OF RATIONALE Indication under consideration Clinical evidence Everolimus in combination with exemestane hormone therapy for oestrogen receptor positive locally advanced or metastatic
DECISION AND SUMMARY OF RATIONALE Indication under consideration Clinical evidence Everolimus in combination with exemestane hormone therapy for oestrogen receptor positive locally advanced or metastatic
Hormonal therapy for advanced prostate cancer
 Hormonal therapy for advanced prostate cancer This information is an extract from the booklet Understanding advanced (metastatic) prostate cancer. You may find the full booklet helpful. We can send you
Hormonal therapy for advanced prostate cancer This information is an extract from the booklet Understanding advanced (metastatic) prostate cancer. You may find the full booklet helpful. We can send you
Treating Patients with Hormone Receptor Positive, HER2 Positive Operable or Locally Advanced Breast Cancer
 Breast Studies Adjuvant therapy after surgery Her 2 positive Breast Cancer B 52 Docetaxel, Carboplatin, Trastuzumab, and Pertuzumab With or Without Estrogen Deprivation in Treating Patients with Hormone
Breast Studies Adjuvant therapy after surgery Her 2 positive Breast Cancer B 52 Docetaxel, Carboplatin, Trastuzumab, and Pertuzumab With or Without Estrogen Deprivation in Treating Patients with Hormone
Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
 Annals of Oncology Advance Access published June 27, 2013 Annals of Oncology 00: 1 9, 2013 doi:10.1093/annonc/mdt208 Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
Annals of Oncology Advance Access published June 27, 2013 Annals of Oncology 00: 1 9, 2013 doi:10.1093/annonc/mdt208 Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
Incorporating Xofigo (radium Ra 223 dichloride) into Clinical Practice
 into Clinical Practice") Incorporating Xofigo (radium Ra 223 dichloride) into Clinical Practice Please see Important Safety Information throughout this presentation and full Prescribing Information available at this 2014 Bayer
Incorporating Xofigo (radium Ra 223 dichloride) into Clinical Practice Please see Important Safety Information throughout this presentation and full Prescribing Information available at this 2014 Bayer
La personalizzazione terapeutica: quanto influisce l età
 La personalizzazione terapeutica: quanto influisce l età PierFranco Conte University of Padova Department of Surgery, Oncology and Gastroenterology IOV Istituto Oncologico Veneto I.R.C.C.S. Breast Cancer
La personalizzazione terapeutica: quanto influisce l età PierFranco Conte University of Padova Department of Surgery, Oncology and Gastroenterology IOV Istituto Oncologico Veneto I.R.C.C.S. Breast Cancer
Prostatectomy, pelvic lymphadenect. Med age 63 years Mean followup 53 months No other cancer related therapy before recurrence. Negative.
 Adjuvante und Salvage Radiotherapie Ludwig Plasswilm Klinik für Radio-Onkologie, KSSG CANCER CONTROL WITH RADICAL PROSTATECTOMY ALONE IN 1,000 CONSECUTIVE PATIENTS 1983 1998 Clinical stage T1 and T2 Mean
Adjuvante und Salvage Radiotherapie Ludwig Plasswilm Klinik für Radio-Onkologie, KSSG CANCER CONTROL WITH RADICAL PROSTATECTOMY ALONE IN 1,000 CONSECUTIVE PATIENTS 1983 1998 Clinical stage T1 and T2 Mean
Treatment of metastatic prostate cancer CLARE GILSON, THUBEENA MANICKAVASAGAR AND SIMON CHOWDHURY
 7 Treatment of metastatic prostate cancer CLE GILSON, THUBEENA MANICKAVASAG AND SIMON CHOWDHURY The authors review the current therapeutic approaches and consider the many remaining questions and challenges
7 Treatment of metastatic prostate cancer CLE GILSON, THUBEENA MANICKAVASAG AND SIMON CHOWDHURY The authors review the current therapeutic approaches and consider the many remaining questions and challenges
Maintenance therapy in in Metastatic NSCLC. Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai
 Maintenance therapy in in Metastatic NSCLC Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai Definition of Maintenance therapy The U.S. National Cancer Institute s
Maintenance therapy in in Metastatic NSCLC Dr Amit Joshi Associate Professor Dept. Of Medical Oncology Tata Memorial Centre Mumbai Definition of Maintenance therapy The U.S. National Cancer Institute s
Understanding the. Controversies of. testosterone replacement. therapy in hypogonadal men with prostate cancer. controversies surrounding
 Controversies of testosterone replacement therapy in hypogonadal men with prostate cancer Samuel Deem, DO CULTURA CREATIVE (RF) / ALAMY Understanding the controversies surrounding testosterone replacement
Controversies of testosterone replacement therapy in hypogonadal men with prostate cancer Samuel Deem, DO CULTURA CREATIVE (RF) / ALAMY Understanding the controversies surrounding testosterone replacement
CMScript. Member of a medical scheme? Know your guaranteed benefits! Issue 7 of 2014
 Background CMScript Member of a medical scheme? Know your guaranteed benefits! Issue 7 of 2014 Prostate cancer is second only to lung cancer as the leading cause of cancer-related deaths in men. It is
Background CMScript Member of a medical scheme? Know your guaranteed benefits! Issue 7 of 2014 Prostate cancer is second only to lung cancer as the leading cause of cancer-related deaths in men. It is
TRANSPARENCY COMMITTEE OPINION. 18 July 2007
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 July 2007 ENANTONE SR 3.75 mg, sustained-release powder and solvent for suspension for injection (SC or IM ) (CIP:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 July 2007 ENANTONE SR 3.75 mg, sustained-release powder and solvent for suspension for injection (SC or IM ) (CIP:
National Horizon Scanning Centre. Vandetanib (Zactima) for advanced or metastatic non-small cell lung cancer. December 2007
 for advanced or metastatic non-small cell lung cancer. December 2007") Vandetanib (Zactima) for advanced or metastatic non-small cell lung cancer December 2007 This technology summary is based on information available at the time of research and a limited literature search.
Vandetanib (Zactima) for advanced or metastatic non-small cell lung cancer December 2007 This technology summary is based on information available at the time of research and a limited literature search.
Clinical Practice Guidelines for the management of locally advanced and metastatic prostate cancer
 Clinical Practice Guidelines for the management of locally advanced and metastatic prostate cancer www.cancer.org.au Clinical Practice Guidelines for the management of locally advanced and metastatic prostate
Clinical Practice Guidelines for the management of locally advanced and metastatic prostate cancer www.cancer.org.au Clinical Practice Guidelines for the management of locally advanced and metastatic prostate
Trials in Elderly Melanoma Patients (with a focus on immunotherapy)
") Trials in Elderly Melanoma Patients (with a focus on immunotherapy) Where we were Immunotherapy Trials: past and present Relevance for real world practice Where we are SIOG October 2012 James Larkin FRCP
Trials in Elderly Melanoma Patients (with a focus on immunotherapy) Where we were Immunotherapy Trials: past and present Relevance for real world practice Where we are SIOG October 2012 James Larkin FRCP
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
PCa Commentary. Volume 73 January-February 2012 PSA AND TREATMENT DECISIONS:
 1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 73 January-February 2012 CONTENTS PSA SCREENING & BASIC SCIENCE PSA AND TREATMENT 1 DECISIONS
1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 73 January-February 2012 CONTENTS PSA SCREENING & BASIC SCIENCE PSA AND TREATMENT 1 DECISIONS
TO SCREEN OR NOT TO SCREEN: THE PROSTATE CANCER
 TO SCREEN OR NOT TO SCREEN: THE PROSTATE CANCER DILEMMA Thomas J Stormont MD January 2012 http://www.youtube.com/watch?v=8jd 7bAHVp0A&feature=related related INTRODUCTION A government health panel (the
TO SCREEN OR NOT TO SCREEN: THE PROSTATE CANCER DILEMMA Thomas J Stormont MD January 2012 http://www.youtube.com/watch?v=8jd 7bAHVp0A&feature=related related INTRODUCTION A government health panel (the
Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group
 Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group Lotte Holm Land MD, ph.d. Onkologisk Afd. R. OUH Kræft og komorbiditet - alle skal
Komorbide brystkræftpatienter kan de tåle behandling? Et registerstudie baseret på Danish Breast Cancer Cooperative Group Lotte Holm Land MD, ph.d. Onkologisk Afd. R. OUH Kræft og komorbiditet - alle skal
Urology Nurse Practitioner Urology Research Nurse Australian Prostate Cancer Research Centre Epworth November 18, 2011
 Urology Nurse Practitioner Helen Crowe Urology Nurse Practitioner Urology Research Nurse Australian Prostate Cancer Research Centre Epworth November 18, 2011 Nurse Practitioner Registered nurse who has
Urology Nurse Practitioner Helen Crowe Urology Nurse Practitioner Urology Research Nurse Australian Prostate Cancer Research Centre Epworth November 18, 2011 Nurse Practitioner Registered nurse who has
Prostate Cancer Studies
 Prostate Cancer Studies STUDIES CURRENTLY RECRUITING MDV3100-14 A multinational, Phase 3, Randomized, Double- Blind, Placebo-Controlled, Efficacy and Safety Study of Enzalutamide in Patients With Nonmetastic
Prostate Cancer Studies STUDIES CURRENTLY RECRUITING MDV3100-14 A multinational, Phase 3, Randomized, Double- Blind, Placebo-Controlled, Efficacy and Safety Study of Enzalutamide in Patients With Nonmetastic
Hormone therapy. In this fact sheet: How does hormone therapy treat prostate cancer? What happens next?
 1 Hormone therapy In this fact sheet: How does hormone therapy treat prostate cancer? Who can have hormone therapy? What types of hormone therapy are there? What are the advantages and disadvantages of
1 Hormone therapy In this fact sheet: How does hormone therapy treat prostate cancer? Who can have hormone therapy? What types of hormone therapy are there? What are the advantages and disadvantages of
PROSTATE CANCER. Effective Date: March, 2015
 PROSTATE CANCER Effective Date: March, 2015 The recommendations contained in this guideline are a consensus of the Alberta Provincial Genitourinary Tumour Team and are a synthesis of currently accepted
PROSTATE CANCER Effective Date: March, 2015 The recommendations contained in this guideline are a consensus of the Alberta Provincial Genitourinary Tumour Team and are a synthesis of currently accepted
Department of Clinical Effectiveness V10 Approved by the Executive Committee of the Medical Staff 10/28/2014
 te: Consider Clinical Trials as treatment options for eligible patients. This Prostate Cancer treatment consensus algorithm is used as a framework for the application of individualized therapy for patients
te: Consider Clinical Trials as treatment options for eligible patients. This Prostate Cancer treatment consensus algorithm is used as a framework for the application of individualized therapy for patients
THE MANY FACES OF MCRPC: ASSESSING PATIENT PROFILES AND TAILORING TREATMENT IN A CHANGING THERAPEUTIC LANDSCAPE
 THE MANY FACES OF MCRPC: ASSESSING PATIENT PROFILES AND TAILORING TREATMENT IN A CHANGING THERAPEUTIC LANDSCAPE Summary of Presentations from the Bayer Healthcare Symposium, held at the 29 th Annual EAU
THE MANY FACES OF MCRPC: ASSESSING PATIENT PROFILES AND TAILORING TREATMENT IN A CHANGING THERAPEUTIC LANDSCAPE Summary of Presentations from the Bayer Healthcare Symposium, held at the 29 th Annual EAU
馬 偕 紀 念 醫 院 新 竹 分 院 前 列 腺 癌 放 射 治 療 指 引
 馬 偕 紀 念 醫 院 新 竹 分 院 前 列 腺 癌 放 射 治 療 指 引 2009.12.02 修 訂 2013.05.13 四 版 前 言 新 竹 馬 偕 醫 院 放 射 腫 瘤 科 藉 由 跨 院 聯 合 會 議 機 制 進 行 討 論, 以 制 定 符 合 現 狀 之 前 列 腺 癌 放 射 治 療 指 引 本 院 前 列 腺 癌 放 射 治 療 指 引 的 建 立, 係 參 考 國 內
馬 偕 紀 念 醫 院 新 竹 分 院 前 列 腺 癌 放 射 治 療 指 引 2009.12.02 修 訂 2013.05.13 四 版 前 言 新 竹 馬 偕 醫 院 放 射 腫 瘤 科 藉 由 跨 院 聯 合 會 議 機 制 進 行 討 論, 以 制 定 符 合 現 狀 之 前 列 腺 癌 放 射 治 療 指 引 本 院 前 列 腺 癌 放 射 治 療 指 引 的 建 立, 係 參 考 國 內
Prostate Cancer. Dr Paula Wells Consultant Clinical Oncologist
 Prostate Cancer Dr Paula Wells Consultant Clinical Oncologist The Facts In UK: Prostate cancer most common cancer in men Second commonest cause of cancer death in men Prostate cancer rates have tripled
Prostate Cancer Dr Paula Wells Consultant Clinical Oncologist The Facts In UK: Prostate cancer most common cancer in men Second commonest cause of cancer death in men Prostate cancer rates have tripled
Historical Basis for Concern
 Androgens After : Are We Ready? Mohit Khera, MD, MBA Assistant Professor of Urology Division of Male Reproductive Medicine and Surgery Scott Department of Urology Baylor College of Medicine Historical
Androgens After : Are We Ready? Mohit Khera, MD, MBA Assistant Professor of Urology Division of Male Reproductive Medicine and Surgery Scott Department of Urology Baylor College of Medicine Historical
Chemotherapy in Ovarian Cancer. Dr R Jones Consultant Medical Oncologist South Wales Gynaecological Oncology Group
 Chemotherapy in Ovarian Cancer Dr R Jones Consultant Medical Oncologist South Wales Gynaecological Oncology Group Adjuvant chemotherapy for early stage EOC Fewer than 30% women present with FIGO stage
Chemotherapy in Ovarian Cancer Dr R Jones Consultant Medical Oncologist South Wales Gynaecological Oncology Group Adjuvant chemotherapy for early stage EOC Fewer than 30% women present with FIGO stage
The PSA Controversy: Defining It, Discussing It, and Coping With It
 The PSA Controversy: Defining It, Discussing It, and Coping With It 11 TH ANNUAL SYMPOSIUM ON MEN S HEALTH June 12, 2013 The PSA Controversy Defining It, Discussing It and Coping With It As of May 2012,
The PSA Controversy: Defining It, Discussing It, and Coping With It 11 TH ANNUAL SYMPOSIUM ON MEN S HEALTH June 12, 2013 The PSA Controversy Defining It, Discussing It and Coping With It As of May 2012,
January 2013 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW. Summary. Contents
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/paclitaxel for cancer Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/ paclitaxel for
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/paclitaxel for cancer Paclitaxel albumin (Abraxane ) as a substitute for docetaxel/ paclitaxel for
Understanding Locally-Advanced Prostate Cancer
 Understanding Locally-Advanced Prostate Cancer This booklet is to help you and your family understand what it means if you have been diagnosed as having locally-advanced prostate cancer. It gives an outline
Understanding Locally-Advanced Prostate Cancer This booklet is to help you and your family understand what it means if you have been diagnosed as having locally-advanced prostate cancer. It gives an outline
Current management of advanced and castration resistant prostate cancer Leonard G. Gomella, MD, 1 Daniel P. Petrylak, MD, 2 Bobby Shayegan, MD 3 1
 INTRODUCTION Current management of advanced and castration resistant prostate cancer Leonard G. Gomella, MD, 1 Daniel P. Petrylak, MD, 2 Bobby Shayegan, MD 3 1 Department of Urology Kimmel Cancer Center,
INTRODUCTION Current management of advanced and castration resistant prostate cancer Leonard G. Gomella, MD, 1 Daniel P. Petrylak, MD, 2 Bobby Shayegan, MD 3 1 Department of Urology Kimmel Cancer Center,
Advanced prostate cancer
 1 Advanced prostate cancer In this fact sheet: What is advanced (metastatic) prostate cancer? What tests are used to diagnose advanced prostate cancer? What do my test results mean? What are my treatment
1 Advanced prostate cancer In this fact sheet: What is advanced (metastatic) prostate cancer? What tests are used to diagnose advanced prostate cancer? What do my test results mean? What are my treatment
Advances in the Management of Prostate Cancer: Highlights from the 2014 ASCO Annual Meeting
 An Interactive PDF Newsletter Advances in the Management of Prostate Cancer: Highlights from the 2014 ASCO Annual Meeting Editors Robert Dreicer, MD, MS, FACP, FASCO Chairman, Department of Solid Tumor
An Interactive PDF Newsletter Advances in the Management of Prostate Cancer: Highlights from the 2014 ASCO Annual Meeting Editors Robert Dreicer, MD, MS, FACP, FASCO Chairman, Department of Solid Tumor
Advanced prostate cancer
 Diagnosis Helpline 0800 074 8383 prostatecanceruk.org 1 Advanced prostate cancer In this fact sheet: What is advanced (metastatic) prostate cancer? What tests are used to diagnose advanced prostate cancer?
Diagnosis Helpline 0800 074 8383 prostatecanceruk.org 1 Advanced prostate cancer In this fact sheet: What is advanced (metastatic) prostate cancer? What tests are used to diagnose advanced prostate cancer?
Robert Bristow MD PhD FRCPC
 Robert Bristow MD PhD FRCPC Clinician-Scientist and Professor, Radiation Oncology and Medical Biophysics, University of Toronto and Ontario Cancer Institute/ (UHN) Head, PMH-CFCRI Prostate Cancer Research
Robert Bristow MD PhD FRCPC Clinician-Scientist and Professor, Radiation Oncology and Medical Biophysics, University of Toronto and Ontario Cancer Institute/ (UHN) Head, PMH-CFCRI Prostate Cancer Research
What is prostate cancer?
 Prostate Cancer What is prostate cancer? Let us explain it to you. www.anticancerfund.org www.esmo.org ESMO/ACF Patient Guide Series based on the ESMO Clinical Practice Guidelines PROSTATE CANCER: A GUIDE
Prostate Cancer What is prostate cancer? Let us explain it to you. www.anticancerfund.org www.esmo.org ESMO/ACF Patient Guide Series based on the ESMO Clinical Practice Guidelines PROSTATE CANCER: A GUIDE
the standard of care 2009 5/1/2009 Mesothelioma: The standard of care take home messages PILC 2006 Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009
 Mesothelioma: The standard of care Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009 take home messages PILC 2006 All patients should receive adequate palliation of dyspnea and pain before starting chemotherapy
Mesothelioma: The standard of care Jan.vanmeerbeeck@ugent.be Brussels, March 7, 2009 take home messages PILC 2006 All patients should receive adequate palliation of dyspnea and pain before starting chemotherapy
Management of low grade glioma s: update on recent trials
 Management of low grade glioma s: update on recent trials M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Low grades Female, born 1976 1 st seizure 2005,
Management of low grade glioma s: update on recent trials M.J. van den Bent The Brain Tumor Center at Erasmus MC Cancer Center Rotterdam, the Netherlands Low grades Female, born 1976 1 st seizure 2005,
EAU Guidelines on Prostate Cancer. Part II: Treatment of Advanced, Relapsing, and Castration-Resistant Prostate Cancer
 EUROPEAN UROLOGY 59 (2011) 572 583 available at www.sciencedirect.com journal homepage: www.europeanurology.com Guidelines EAU Guidelines on Prostate Cancer. Part II: Treatment of Advanced, Relapsing,
EUROPEAN UROLOGY 59 (2011) 572 583 available at www.sciencedirect.com journal homepage: www.europeanurology.com Guidelines EAU Guidelines on Prostate Cancer. Part II: Treatment of Advanced, Relapsing,
GUIDELINES ADJUVANT SYSTEMIC BREAST CANCER
 GUIDELINES ADJUVANT SYSTEMIC BREAST CANCER Author: Dr Susan O Reilly On behalf of the Breast CNG Written: December 2008 Agreed at CNG: June 2009 & June 2010 Review due: June 2011 Guidelines Adjuvant Systemic
GUIDELINES ADJUVANT SYSTEMIC BREAST CANCER Author: Dr Susan O Reilly On behalf of the Breast CNG Written: December 2008 Agreed at CNG: June 2009 & June 2010 Review due: June 2011 Guidelines Adjuvant Systemic
Metastatic Prostate Cancer
 CANCERCARE CONNECT BOOKLET SERIES Treatment Update Metastatic Prostate Cancer www.cancercare.org The CancerCare Connect Booklet Series offers up-to-date, easy-to-read information on the latest treatments,
CANCERCARE CONNECT BOOKLET SERIES Treatment Update Metastatic Prostate Cancer www.cancercare.org The CancerCare Connect Booklet Series offers up-to-date, easy-to-read information on the latest treatments,
Living with hormone therapy A guide for men with prostate cancer
 Living with hormone therapy A guide for men with prostate cancer 2 Living with hormone therapy About this booklet This booklet is for you if you are about to start, or are already having, hormone therapy
Living with hormone therapy A guide for men with prostate cancer 2 Living with hormone therapy About this booklet This booklet is for you if you are about to start, or are already having, hormone therapy
Living with hormone therapy A guide for men with prostate cancer
 Living with hormone therapy A guide for men with prostate cancer 2 Living with hormone therapy A guide for men with prostate cancer About this booklet This booklet is for you if you are about to start,
Living with hormone therapy A guide for men with prostate cancer 2 Living with hormone therapy A guide for men with prostate cancer About this booklet This booklet is for you if you are about to start,
Prostate Cancer: National Collaborating Centre for Cancer. diagnosis and treatment. Clinical Guideline. January 2014. Prostate Cancer.
 National Collaborating Centre for Cancer Prostate Cancer Prostate Cancer: diagnosis and treatment Clinical Guideline Full Guideline January 2014 Final version Commissioned by the National Institute for
National Collaborating Centre for Cancer Prostate Cancer Prostate Cancer: diagnosis and treatment Clinical Guideline Full Guideline January 2014 Final version Commissioned by the National Institute for
Metastatic Prostate Cancer
 Patient Information English 35 Metastatic Prostate Cancer The underlined terms are listed in the glossary. Prostate cancer can spread to other organs or lymph nodes outside the pelvic area. This is called
Patient Information English 35 Metastatic Prostate Cancer The underlined terms are listed in the glossary. Prostate cancer can spread to other organs or lymph nodes outside the pelvic area. This is called
4/8/13. Pre-test Audience Response. Prostate Cancer 2012. Screening and Treatment of Prostate Cancer: The 2013 Perspective
 Pre-test Audience Response Screening and Treatment of Prostate Cancer: The 2013 Perspective 1. I do not offer routine PSA screening, and the USPSTF D recommendation will not change my practice. 2. In light
Pre-test Audience Response Screening and Treatment of Prostate Cancer: The 2013 Perspective 1. I do not offer routine PSA screening, and the USPSTF D recommendation will not change my practice. 2. In light
NATIONAL CANCER DRUG FUND PRIORITISATION SCORES
 NATIONAL CANCER DRUG FUND PRIORITISATION SCORES Drug Indication Regimen (where appropriate) BORTEZOMIB In combination with dexamethasone (VD), or with dexamethasone and thalidomide (VTD), is indicated
NATIONAL CANCER DRUG FUND PRIORITISATION SCORES Drug Indication Regimen (where appropriate) BORTEZOMIB In combination with dexamethasone (VD), or with dexamethasone and thalidomide (VTD), is indicated
PSA Testing 101. Stanley H. Weiss, MD. Professor, UMDNJ-New Jersey Medical School. Director & PI, Essex County Cancer Coalition. weiss@umdnj.
 PSA Testing 101 Stanley H. Weiss, MD Professor, UMDNJ-New Jersey Medical School Director & PI, Essex County Cancer Coalition weiss@umdnj.edu September 23, 2010 Screening: 3 tests for PCa A good screening
PSA Testing 101 Stanley H. Weiss, MD Professor, UMDNJ-New Jersey Medical School Director & PI, Essex County Cancer Coalition weiss@umdnj.edu September 23, 2010 Screening: 3 tests for PCa A good screening
Highlights in Advanced Prostate Cancer From the 2014 AUA and ASCO Meetings
 Highlights in Advanced Prostate Cancer From the 2014 AUA and ASCO Meetings A Review of Selected Presentations From the 2014 American Urological Association Meeting, May 16-21, 2014, Orlando, Florida and
Highlights in Advanced Prostate Cancer From the 2014 AUA and ASCO Meetings A Review of Selected Presentations From the 2014 American Urological Association Meeting, May 16-21, 2014, Orlando, Florida and
Technology appraisal guidance Published: 27 January 2016 nice.org.uk/guidance/ta376
 Radium-223 dichloride for treating hormone-relapsed prostate cancer with bone metastases Technology appraisal guidance Published: 27 January 2016 nice.org.uk/guidance/ta376 NICE 2016. All rights reserved.
Radium-223 dichloride for treating hormone-relapsed prostate cancer with bone metastases Technology appraisal guidance Published: 27 January 2016 nice.org.uk/guidance/ta376 NICE 2016. All rights reserved.
Second line. Elena Verzoni Oncologia Medica Fondazione IRCCS Istituto Nazionale Tumori Milano
 mcrpc: First and Second line Elena Verzoni Oncologia Medica Fondazione IRCCS Istituto Nazionale Tumori Milano Landmarks of disease progression in CRPC 2-10 years 30 months Failed localized therapy Hormonal
mcrpc: First and Second line Elena Verzoni Oncologia Medica Fondazione IRCCS Istituto Nazionale Tumori Milano Landmarks of disease progression in CRPC 2-10 years 30 months Failed localized therapy Hormonal
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT
 MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
Drug/Drug Combination: Bevacizumab in combination with chemotherapy
 AHFS Final Determination of Medical Acceptance: Off-label Use of Bevacizumab in Combination with Chemotherapy for the Treatment of Metastatic Breast Cancer Previously Treated with Cytotoxic Chemotherapy
AHFS Final Determination of Medical Acceptance: Off-label Use of Bevacizumab in Combination with Chemotherapy for the Treatment of Metastatic Breast Cancer Previously Treated with Cytotoxic Chemotherapy
New Treatment Options for Breast Cancer
 New Treatment Options for Breast Cancer Brandon Vakiner, PharmD., BCOP Clinical Pharmacy Specialist - Oncology The University of Iowa Hospitals and Clinics Assistant Professor (Clinical) University of
New Treatment Options for Breast Cancer Brandon Vakiner, PharmD., BCOP Clinical Pharmacy Specialist - Oncology The University of Iowa Hospitals and Clinics Assistant Professor (Clinical) University of
REVIEW. Introduction. Key Words: prostatic cancer, biochemical recurrence, salvage radiotherapy, androgen deprivation therapy, systemic therapy
 REVIEW Therapeutic options for a rising PSA after radical prostatectomy Bradley C. Carthon, MD, 1,2 David M. Marcus, MD, 2,3 Lindsey A. Herrel, MD, 4 Ashesh B. Jani, MD, 2,3,4 Peter J. Rossi, MD, 2,3,4
REVIEW Therapeutic options for a rising PSA after radical prostatectomy Bradley C. Carthon, MD, 1,2 David M. Marcus, MD, 2,3 Lindsey A. Herrel, MD, 4 Ashesh B. Jani, MD, 2,3,4 Peter J. Rossi, MD, 2,3,4
Hormone Therapy for Prostate Cancer A Patient Guide
 Your Health Matters Hormone Therapy for Prostate Cancer A Patient Guide Urologic Oncology Program UCSF Helen Diller Family Comprehensive Cancer Center University of California, San Francisco Phone number:
Your Health Matters Hormone Therapy for Prostate Cancer A Patient Guide Urologic Oncology Program UCSF Helen Diller Family Comprehensive Cancer Center University of California, San Francisco Phone number:
American Urological Association (AUA) Guideline
 Guideline") 1 (AUA) Guideline Approved by the AUA Board of Directors April 2013 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2013 by the American
1 (AUA) Guideline Approved by the AUA Board of Directors April 2013 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2013 by the American