HUMAN ANATOMY ILLUSTRATIVE GUIDE & MEDICAL TERMINOLOGY
|
|
|
- Piers Cox
- 8 years ago
- Views:
Transcription
1 HUMAN ANATOMY ILLUSTRATIVE GUIDE & MEDICAL TERMINOLOGY ENGLISH/SPANISH VERSION 1 Developed by: Cultural and Linguistic Services Department Copyright 2004 L.A. Care Health Plan Permission granted to adapt by LA Care Health Plan

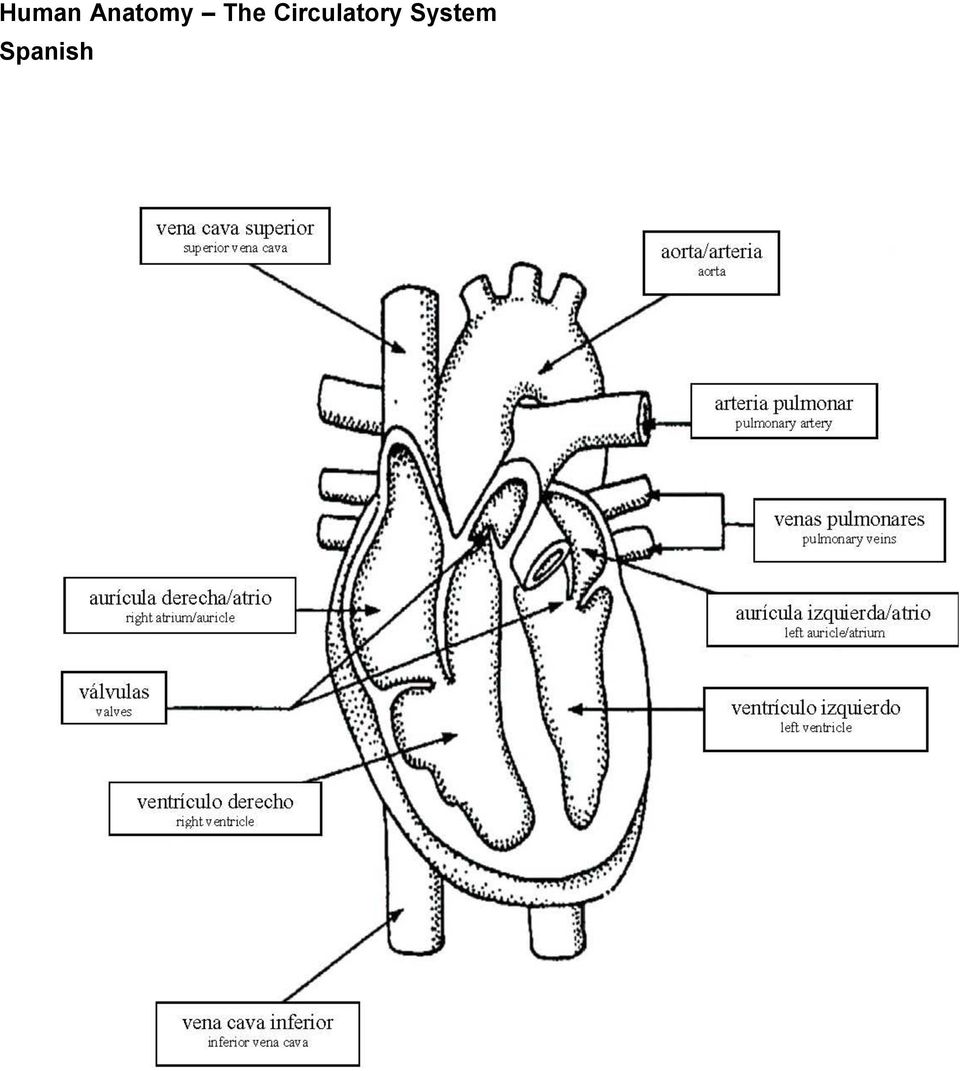
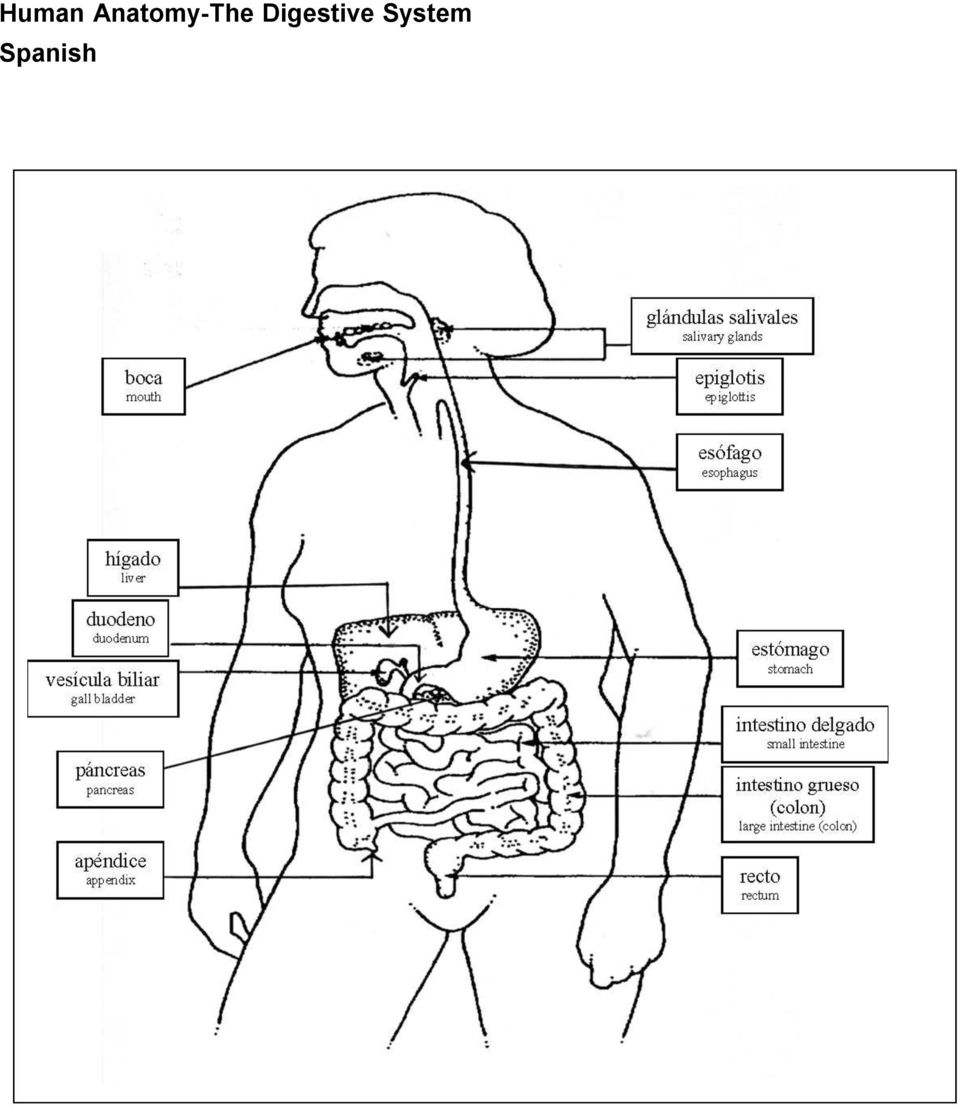
2 Introduction The Human Anatomy Illustrative Guide and Medical Terminology was developed out of a need that was identified through our training programs on health care interpreting and instructing clinical staff on how to work with an interpreter. We heard from bilingual/multilingual staff that they needed tools that would help them communicate with limited English proficient (LEP) patients. From our evaluative work, we also understood that some bilingual/multilingual staff also needed to know human anatomy terms in English as well as the target language. In our mission to close the language gap, we developed the bilingual anatomy chart that includes human anatomical charts, medical terms, and frequently asked questions by doctors during their interactions with patients, in Los Angeles County s ten threshold languages (Armenian, Chinese, English, Farsi, Khmer, Korean, Russian, Spanish, Tagalog, and Vietnamese). Communication is a critical link to patient safety, quality of care, access to needed health care services, and patient satisfaction. The rapid changes that occur in health care settings create many challenges and opportunities to develop innovative ways of communicating with patients, particularly with linguistically diverse patient population. This resource is in alignment with L.A. Care s over arching mission which is: To ensure the provision of culturally sensitive and linguistically competent quality health care services to the Med- Cal population in Los Angeles County through the Safety Net Providers and our health partners, to promote health and disease prevention, to continuously improve the knowledge and effectiveness of our provider community, and to assist in the provision of the same quality of services for the vulnerable populations. L.A. Care wishes to acknowledge all those that have contributed to the development of this guide. First and foremost, we must thank The Cross Cultural Health Care Program for allowing us to use the illustrations from the Bridging the Gap interpreter s handbook. Sarkis Semerdjyan, Fatima Rodriguez and Elizabeth Nguyen were key staff members of the Cultural and Linguistic Services Department at L.A. Care, who put much energy and effort to ensure the quality of this guide. We also would like to thank the Marketing Department, Young Chi in particular, for her assistance with the layout of the guide. Together in Health, Beatriz M. Solís Director of Cultural and Linguistic Services

3 Human Anatomy The Circulatory System Spanish
4 Human Anatomy-The Digestive System Spanish
5 Human Anatomy - The Endocrine (Ductless Gland) System Spanish
 System")
6 Human Anatomy - The Optical System Spanish

7 Human Anatomy - The Male Reproductive/Urinary System Spanish

8 Human Anatomy - The Female Reproductive System Spanish

9 Human anatomy - The Respiratory System Spanish

10 Medical Terminology & Frequently Asked Questions by Providers During Encounters with Patients 1. Abdominal pain dolor abdominal 2. Acquired Immunodeficiency Syndrome (AIDS) síndrome de inmunodeficiencia adquirida (SIDA) 3. Allergies alergias 4. Appendicitis apendicitis 5. Arthritis artritis 6. Asthma asma 7. Bronchitis bronquitis 8. Cervical cancer cáncer cervical, cáncer del cervix 9. Chest pain dolor en el pecho 10. Chicken pox varicela (viruelas) 11. Chlamydia clamidia 12. Constipation estreñimiento 13. Contraceptive anticonceptivo (contraceptivo) 14. Cyst quiste 15. Diabetes diabetes 16. Diet dieta, régimen alimenticio 17. Difficulty breathing dificultad al respirar 18. Diphtheria difteria 19. Discharge (e.g. a discharge from the vagina) 20. Dizziness mareo flujo, desecho, secreción 21. Drugs (illegal drugs) drogas ilicitas 22. Earache dolor de oído 23. Ectopic pregnancy embarazo ectópico, gestación fuera 24. Fever fiebre 25. Human Immunodeficiency Virus (HIV) Virus de inmunodeficiencia (VIH) 26. Hemorrhoids hemorroides
 14. Cyst quiste 15. Diabetes diabetes 16. Diet dieta, régimen alimenticio 17.")
11 27. Hepatitis hepatitis 28. Hypertension hypertension, alta presión 29. Ulcer ulcera, llaga, lesión 30. Measles sarampión 31. Mumps paperas, parotiditis 32. Pap smear prueba de papanicolaou 33. Pneumonia neumonía, pulmonía 34. Sexually transmitted diseases (STDs) enfermedades trasmitidas sexualmente 35. Shortness of breath falta de respiración 36. Sore throat dolor de garganta 37. Stomach ache dolor de estómago 38. Tetanus shot vacuna contra el tétano 39. Toothache dolor de muela 40. Tuberculosis tuberculosis 41. Urinary infection infección renal, infección urinaria 42. Urine analysis análisis de orina 43. Vaccination vacunación, inoculación de una vacuna 44. Varicose vein várices, venas varicosas 45. Whooping cough tos ferina 46. Yeast infection hongo vaginal, infección vaginal 47. Are you in pain? Siente dolor? 48. Are you taking any medications? Está tomando algún medicamento? 49. Are your stools normal? Su excremento es normal? 50. Do you feel dizzy? Se siente mariado? 51. Do you have a fever? Tiene fiebre? 52. Do you have a runny nose? Le gotea la nariz? 53. Do you have numbness or tingling? Está entumecido o siente hormigueo? 54. Hold your breath Mantenga la respiración

12 55. Is the pain a sharp pain or dull pain? El dolor es agudo o sordo? 56. May I help you? Le puedo ayudar? 57. How did you hurt yourself? Cómo se lastimo? 58. Have you ever had this problem before? Ha tenido este problema anteriormente? 59. Does anyone in your family have asthma? Hay alguien en su familia que tiene asma? 60. Has anyone in your family been treated for diabetes? Ha recibido algún miembro de su familia tratamiento por la diabetes? 61. Has your child been vaccinated? Ha sido vacunado su niño(a)? 62. Have you ever had any operations? Le han hecho alguna cirugía anteriormente? 63. Do you have any allergy to any food or drug? Tiene alguna alergia a ciertas comidas o medicamentos? 64. Do you have any trouble with your throat? Tiene algún problema en su garganta? 65. Have you been going to the bathroom regularly? 66. Has your baby been tugging at his ear a lot? Ha estado yendo al baño regularmente? Se ha estado jalando la oreja mucho su bebé? 67. Which tooth is bothering you? Cuál diente le está molestando? 68. When was the last time you saw a dentist? Cuándo fue la última vez que vio el dentista? 69. When was your last menstrual period? Cuándo tuvo su última regla menstrual? 70. Is this your first pregnancy? Este es su primer embarazo? 71. Have you ever had a miscarriage? Ha tenido malpartos (abortos espontáneos) en el pasado? 72. Did you have any complications with your Tuvo alguna complicación con sus otros embarazos? other pregnancies? 73. Were any of your children born by C- section? Ha tenido partos por cesaria?

13 74. How many months pregnant are you now? Cuántos meses de embarazo tiene? 75. How much weigh have you gained? Cuánto peso ha aumentado? 76. Have you received prenatal care? Ha recibido cuidado prenatal? 77. When did you start having contractions? Cuándo empezó a tener contracciones? 78. Will you be breastfeeding your baby? Le dará pecho a su bebé? 79. What seems to be the problem with your child? Cuál parece ser el problema con su niño(a)? 80. Was he unconscious after he fell? Estuvo inconsciente después de haberse caído? 81. Did he appear to be in pain? Le pareció que él tenía dolor? 82. Has he been vomiting? Se ha estado vomitando? 83. How did you cut yourself? Cómo se cortó? 84. Is there any swelling? Hay alguna hinchazón? 85. Has the baby had any diarrhea? Ha tenido diarrea el bebé? 86. Was there any blood in the stool? Hubo sangre en el excremento? 87. Do you ever vomit when you have this stomach pain? Se vomita cuándo le da dolor de estómago? 88. Do you often have stomach cramps or fever? Sufre usted de calambres estomacales o fiebre a menudo? Permission to use granted by LA Care Health Plan

14

Project J-FIT TEMPLATE
 Project J-FIT TEMPLATE!" # $ %&'(), -. * ++*+) Please complete all information requested. 1) Toolkit name: 2) Project manager contact information Name: Address: Phone number: Email address: 3) Team member
Project J-FIT TEMPLATE!" # $ %&'(), -. * ++*+) Please complete all information requested. 1) Toolkit name: 2) Project manager contact information Name: Address: Phone number: Email address: 3) Team member
Application For Admission To The Non-Surgical Spinal Decompression Program At The Spinal Decompression Center of Long Beach
 Application For Admission To The Non-Surgical Spinal Decompression Program At The Spinal Decompression Center of Long Beach If you are reading this form, you have qualified for a consultation with Dr.
Application For Admission To The Non-Surgical Spinal Decompression Program At The Spinal Decompression Center of Long Beach If you are reading this form, you have qualified for a consultation with Dr.
SOUTH FLORIDA RADIATION ONCOLOGY HISTORY GENERAL - HISTORIA GENERAL PRELIMINARY PATIENT INFORMATION / INFORMACION PRELIMINARIA DEL PACIENTE
 SOUTH FLORIDA RADIATION ONCOLOGY HISTORY GENERAL - HISTORIA GENERAL PRELIMINARY PATIENT INFORMATION / INFORMACION PRELIMINARIA DEL PACIENTE Patient Name/Nombre delpaciente: Referring Doctor/Doctor que
SOUTH FLORIDA RADIATION ONCOLOGY HISTORY GENERAL - HISTORIA GENERAL PRELIMINARY PATIENT INFORMATION / INFORMACION PRELIMINARIA DEL PACIENTE Patient Name/Nombre delpaciente: Referring Doctor/Doctor que
MEDICAL HISTORY AND SCREENING FORM
 MEDICAL HISTORY AND SCREENING FORM The purpose of preventive exams is to screen for potential health problems and provide education to promote optimal health. It is best practice for chronic health problems
MEDICAL HISTORY AND SCREENING FORM The purpose of preventive exams is to screen for potential health problems and provide education to promote optimal health. It is best practice for chronic health problems
POINCIANA INTERNAL MEDICINE PA. Patient Name: Social Security Number: Date of Birth: / / Sex: M/F (Circle One) Married/Single/Divorced/Widow Address:
 Married/Single/Divorced/Widow Address:") Patient Name: Social Security Number: Date of Birth: / / Sex: M/F (Circle One) Married/Single/Divorced/Widow Address: (Street) (City/State/Zip) Home Phone: ( ) E Mail Address: Would you be interested in
Patient Name: Social Security Number: Date of Birth: / / Sex: M/F (Circle One) Married/Single/Divorced/Widow Address: (Street) (City/State/Zip) Home Phone: ( ) E Mail Address: Would you be interested in
CLINIC APPLICATION. Client Information
 ICNA Relief USA Shifa Free Medical Clinic 1092 Johnnie Dodds Boulevard, Suite 108 Mount Pleasant, SC 29464 Tel: (843) 352-4580 Fax: (843) 375-9063 Last Name Street Address City, State, Zip Code Home Phone
ICNA Relief USA Shifa Free Medical Clinic 1092 Johnnie Dodds Boulevard, Suite 108 Mount Pleasant, SC 29464 Tel: (843) 352-4580 Fax: (843) 375-9063 Last Name Street Address City, State, Zip Code Home Phone
Horn Family Chiropractic Non-Surgical Spinal Decompression Application For Admission
 Horn Family Chiropractic Non-Surgical Spinal Decompression Application For Admission Non surgical Spinal Care for Severe Neck, Shoulder, Low Back & Leg Pain If you are reading this you have been fortunate
Horn Family Chiropractic Non-Surgical Spinal Decompression Application For Admission Non surgical Spinal Care for Severe Neck, Shoulder, Low Back & Leg Pain If you are reading this you have been fortunate
Health Information Form for Adults
 A. Identification B. Emergency Contacts Name (Last) (First) (Middle) Maiden Name In Case of Emergency, Notify: Primary Contact Name (Last) (First) (Middle) Primary Alternate Relationship Home Work Home
A. Identification B. Emergency Contacts Name (Last) (First) (Middle) Maiden Name In Case of Emergency, Notify: Primary Contact Name (Last) (First) (Middle) Primary Alternate Relationship Home Work Home
General Internal Medicine Clinic New Patient Questionnaire
 General Internal Medicine Clinic New Patient Questionnaire Date: Name: What would you like to be called by the doctor? Marital Status: Please list how you would like to be contacted, for test results:
General Internal Medicine Clinic New Patient Questionnaire Date: Name: What would you like to be called by the doctor? Marital Status: Please list how you would like to be contacted, for test results:
Shelby Foot & Ankle 1. PATIENT INFORMATION 2. INSURANCE. 50505 Schoenherr Road, Suite 230 Shelby Township, MI 48315 (586) 580-3728 www.shelbyfoot.
 580-3728 www.shelbyfoot.") : 1. PATIENT INFORMATION 2. INSURANCE SS/H/C/Patient ID#: Patient Last Name: Who is responsible for this account? Relationship to Patient: Insurance Co.: Patient First Name: Middle Int: Group #: Address:
: 1. PATIENT INFORMATION 2. INSURANCE SS/H/C/Patient ID#: Patient Last Name: Who is responsible for this account? Relationship to Patient: Insurance Co.: Patient First Name: Middle Int: Group #: Address:
Health Information Form for Adults
 A. IDENTIFICATION B. EMERGENCY CONTACTS Name (Last) (First) (Middle) Maiden Name Primary Alternate In Case of Emergency, Notify: Primary Contact Name (Last) (First) (Middle) Relationship Home Work Home
A. IDENTIFICATION B. EMERGENCY CONTACTS Name (Last) (First) (Middle) Maiden Name Primary Alternate In Case of Emergency, Notify: Primary Contact Name (Last) (First) (Middle) Relationship Home Work Home
Please fill out forms, sign where needed and bring with you to your first visit. If you have any questions please call the office at 212-751-8300.
 Welcome to Manhattan Sports Medicine and the office of Dr. Kyle Worell. Before we get started please see all forms below: Personal History (Intake) Informed Consent Payments HIPPA Please fill out forms,
Welcome to Manhattan Sports Medicine and the office of Dr. Kyle Worell. Before we get started please see all forms below: Personal History (Intake) Informed Consent Payments HIPPA Please fill out forms,
Neurological Surgery and Spine Surgery, S.C. Suite 800 1 Westbrook Corporate Center Westchester, Illinois 60154
 Neurological Surgery and Spine Surgery, S.C. Suite 800 1 Westbrook Corporate Center Westchester, Illinois 60154 BACK AND NECK PAIN QUESTIONNAIRE Please PRINT all information CLEARLY. Note that there are
Neurological Surgery and Spine Surgery, S.C. Suite 800 1 Westbrook Corporate Center Westchester, Illinois 60154 BACK AND NECK PAIN QUESTIONNAIRE Please PRINT all information CLEARLY. Note that there are
NEW PATIENT HISTORY QUESTIONNAIRE. Physician Initials Date PATIENT INFORMATION
 NEW PATIENT HISTORY QUESTIONNAIRE Physician Initials Date PATIENT INFORMATION JHH# DOB# AGE HOME PH CELL PH DAY PH EMAIL Who is your REFERRING PHYSICIAN? (The doctor who referred you to Johns Hopkins Neurology.)
NEW PATIENT HISTORY QUESTIONNAIRE Physician Initials Date PATIENT INFORMATION JHH# DOB# AGE HOME PH CELL PH DAY PH EMAIL Who is your REFERRING PHYSICIAN? (The doctor who referred you to Johns Hopkins Neurology.)
Diseases that can be spread during sex
 Diseases that can be spread during sex Did you know... over 65 million people in the United States have a chronic, incurable sexually transmitted disease (STD)? and that every year another 19 million persons
Diseases that can be spread during sex Did you know... over 65 million people in the United States have a chronic, incurable sexually transmitted disease (STD)? and that every year another 19 million persons
PATIENT INFORMATION INSURANCE INFORMATION
 (mm/dd/yyyy): Have you been to Physicians Urgent Care before? Yes No Arrival Time: If yes, when? Is this a follow-up to a previous visit: Yes No PATIENT INFORMATION Patient s First Name: Middle Name: Last
(mm/dd/yyyy): Have you been to Physicians Urgent Care before? Yes No Arrival Time: If yes, when? Is this a follow-up to a previous visit: Yes No PATIENT INFORMATION Patient s First Name: Middle Name: Last
Cornerstone Family Practice REGISTRATION FORM (Please Print)
") Cornerstone Family Practice REGISTRATION FORM (Please Print) Today s Date: PCP: PATIENT INFORMATION Patient s last name: First: Middle: Mr. Mrs. Miss Ms. Marital status: Single Mar Div Sep Wid Language
Cornerstone Family Practice REGISTRATION FORM (Please Print) Today s Date: PCP: PATIENT INFORMATION Patient s last name: First: Middle: Mr. Mrs. Miss Ms. Marital status: Single Mar Div Sep Wid Language
Lesson 29. Notes. Necesita tomar estos comprimidos. Lesson 29. CoffeeBreakSpanish.com. Recap. A little more pain... May 28th, 2007
 May 28th, 2007 In this edition: more aches and pains, illnesses and useful language for a visit to the pharmacy Lesson 29 Notes CoffeeBreakSpanish.com Necesita tomar estos comprimidos Lesson 29 Programme
May 28th, 2007 In this edition: more aches and pains, illnesses and useful language for a visit to the pharmacy Lesson 29 Notes CoffeeBreakSpanish.com Necesita tomar estos comprimidos Lesson 29 Programme
2 P age. Babies from Birth to Age 2
 Contents Babies from Birth to Age 2... 2 Vaccines give parents the power... 2 Vaccines are recommended throughout our lives... 3 Talk to your doctor... 3 Vaccines are very safe... 3 Whooping Cough (Pertussis)...
Contents Babies from Birth to Age 2... 2 Vaccines give parents the power... 2 Vaccines are recommended throughout our lives... 3 Talk to your doctor... 3 Vaccines are very safe... 3 Whooping Cough (Pertussis)...
Women s Continence and Pelvic Health Center
 Women s Continence and Pelvic Health Center Committed to Caring 580-590 Court Street Keene, New Hampshire 03431 (603) 354-5454 Ext. 6643 URINARY INCONTINENCE QUESTIONNAIRE The purpose of this questionnaire
Women s Continence and Pelvic Health Center Committed to Caring 580-590 Court Street Keene, New Hampshire 03431 (603) 354-5454 Ext. 6643 URINARY INCONTINENCE QUESTIONNAIRE The purpose of this questionnaire
Workman s Compensation
 Workman s Compensation Name: Sex: Phone Number: Age: Address (Street/City/State/Zip) Name of Employer: Phone: Address of Employer (Street/City/State/Zip) Date and time of accident?: Where were you taken
Workman s Compensation Name: Sex: Phone Number: Age: Address (Street/City/State/Zip) Name of Employer: Phone: Address of Employer (Street/City/State/Zip) Date and time of accident?: Where were you taken
1584 Wesleyan Drive FORM A Norfolk, VA 23504 Phone: (757) 455-3108 Health History immunization & Physical Form
 455-3108 Health History immunization & Physical Form") Mail completed form to: Marlin Health Services 1584 Wesleyan Drive FORM A Norfolk, VA 23504 Phone: (757) 455-3108 Health History immunization & Physical Form Virginia State law (code 23-7.5) requires all
Mail completed form to: Marlin Health Services 1584 Wesleyan Drive FORM A Norfolk, VA 23504 Phone: (757) 455-3108 Health History immunization & Physical Form Virginia State law (code 23-7.5) requires all
Board Certified Endocrinology, Diabetes & Metabolism Palm Harbor, FL 34684 Phone (727) 784-3366 FAX (727) 784-3527
 784-3366 FAX (727) 784-3527") Jerry Drucker, MD, FACE The Endocrine Center of Florida, LLC Board Certified Internal Medicine 34041 US Highway 19 North, Suite C Board Certified Endocrinology, Diabetes & Metabolism Palm Harbor, FL 34684
Jerry Drucker, MD, FACE The Endocrine Center of Florida, LLC Board Certified Internal Medicine 34041 US Highway 19 North, Suite C Board Certified Endocrinology, Diabetes & Metabolism Palm Harbor, FL 34684
IF THIS IS RELATED TO A WORKMAN S COMPENSATION CLAIM OR AN AUTOMOBILE ACCIDENT, PLEASE FILL OUT ADDITIONAL SHEET IN THE BACK OF THIS PACKET (PIP FORM)
") PATIENT INFORMATION Last Name: First: MI: of Birth: Social Security #: - - Address: City State Zip Home#: ( ) - Cell#: ( ) - Employer: Employer#: ( ) - Occupation: Retired Unemployed Student Self-Employed
PATIENT INFORMATION Last Name: First: MI: of Birth: Social Security #: - - Address: City State Zip Home#: ( ) - Cell#: ( ) - Employer: Employer#: ( ) - Occupation: Retired Unemployed Student Self-Employed
Surgery Health Survey
 Surgery Health Survey Name: Social Security Number: Date of Birth: Please tell us which physician(s) we should contact regarding your visit: REFERRING PHYSICIAN Name: Address: PRIMARY CARE PHSYICIAN Name:
Surgery Health Survey Name: Social Security Number: Date of Birth: Please tell us which physician(s) we should contact regarding your visit: REFERRING PHYSICIAN Name: Address: PRIMARY CARE PHSYICIAN Name:
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology (Patient Label)
") REVIEWED DATE / INITIALS SAFETY: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? ALLERGIES: Do you have any allergies to medications? If, please
REVIEWED DATE / INITIALS SAFETY: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? ALLERGIES: Do you have any allergies to medications? If, please
PLEASE PRINT LEGIBLY
 Patient Information PLEASE PRINT LEGIBLY Patients Name: Date of Birth: Sex: Patients Address: City: State: Zip: Home Phone: Cell: Work: Email: SSN: Employer: Occupation: Marital Status: Employed: Full
Patient Information PLEASE PRINT LEGIBLY Patients Name: Date of Birth: Sex: Patients Address: City: State: Zip: Home Phone: Cell: Work: Email: SSN: Employer: Occupation: Marital Status: Employed: Full
Dear Patient, Sincerely, Gastroenterology Associates of North Jersey
 GASTROENTEROLOGY ASSOCIATES OF NORTH JERSEY, P.A. Doctors Park 369 West Blackwell Street, Dover, NJ 07801 16 Pocono Road, Suite 210, Denville, NJ 07834 Tel (973) 361-7660 Fax (973) 361-0455 Tel (973) 627-7600
GASTROENTEROLOGY ASSOCIATES OF NORTH JERSEY, P.A. Doctors Park 369 West Blackwell Street, Dover, NJ 07801 16 Pocono Road, Suite 210, Denville, NJ 07834 Tel (973) 361-7660 Fax (973) 361-0455 Tel (973) 627-7600
Patient Medical History Form
 Patient Medical History Form Patient Name: To help the doctor serve you better, please complete the information below. Thank you! Allergies: No known Allergies (If yes, please list all Drug, Food, and
Patient Medical History Form Patient Name: To help the doctor serve you better, please complete the information below. Thank you! Allergies: No known Allergies (If yes, please list all Drug, Food, and
PATIENT INFORMATION / / OTHER CONTACT NUMERS: (CIRCLE ONE) CELL, HOME OR OTHER. ENTER NUMBER BELOW. ( ) EMPLOYER ( )
 CELL, HOME OR OTHER. ENTER NUMBER BELOW. ( ) EMPLOYER ( )") PATIENT INFORMATION PATIENT S LEGAL NAME DATE OF BIRTH AGE DATE / / / / HEIGHT AND WEIGHT SEX REASON FOR VISIT: MARITAL STATUS FT IN LBS MALE FEMALE S M D W ADDRESS CITY STATE ZIP CODE THE BEST NUMBER
PATIENT INFORMATION PATIENT S LEGAL NAME DATE OF BIRTH AGE DATE / / / / HEIGHT AND WEIGHT SEX REASON FOR VISIT: MARITAL STATUS FT IN LBS MALE FEMALE S M D W ADDRESS CITY STATE ZIP CODE THE BEST NUMBER
Disclosure Form. Memberships: National Certification Commission for Acupuncture and Oriental Medicine (Dipl. Acup.)
") Consent Form By signing below, I do hereby voluntarily consent to be treated with acupuncture and/or substances from the Oriental materia medica Matt Hillman, L.Ac. I understand that acupuncturists practicing
Consent Form By signing below, I do hereby voluntarily consent to be treated with acupuncture and/or substances from the Oriental materia medica Matt Hillman, L.Ac. I understand that acupuncturists practicing
PATIENT INITIAL FORM
 Cocoa Accident & Injury Center, Inc. Titusville Chiropractic & Injury Center, Inc. PATIENT INITIAL FORM Patient Name: DOB: Age: Phone: Social Security #: Address: City: Zip Code: of Accident: Marital Status:
Cocoa Accident & Injury Center, Inc. Titusville Chiropractic & Injury Center, Inc. PATIENT INITIAL FORM Patient Name: DOB: Age: Phone: Social Security #: Address: City: Zip Code: of Accident: Marital Status:
Name Last First Middle. (Complete Mailing) Address ** Street Apt# City State Zip. Work Phone # ( ) ** Emergency Contact Relationship Phone# ( )
 Address ** Street Apt# City State Zip. Work Phone # ( ) ** Emergency Contact Relationship Phone# ( )") Today s Date NEW PATIENT REGISTRATION Name Last First Middle (Complete Mailing) Address ** Street Apt# City State Zip Social Security # Home Phone # ( ) ** Date of Birth Work Phone # ( ) ** Cell Phone
Today s Date NEW PATIENT REGISTRATION Name Last First Middle (Complete Mailing) Address ** Street Apt# City State Zip Social Security # Home Phone # ( ) ** Date of Birth Work Phone # ( ) ** Cell Phone
Beach Family Doctors Medical Group
 Beach Family Doctors Medical Group Welcome to our practice! Office Hours / After Hours 8:30am-5:00pm Monday through Friday; Closed for lunch; Closed all major holidays. For urgent medical issues after
Beach Family Doctors Medical Group Welcome to our practice! Office Hours / After Hours 8:30am-5:00pm Monday through Friday; Closed for lunch; Closed all major holidays. For urgent medical issues after
BRENTWOOD EAST FAMILY MEDICINE Patient Registration Form (ecw)
") BRENTWOOD EAST FAMILY MEDICINE Patient Registration Form (ecw) PATIENT INFORMATION Dr. Miss Mr. Mrs. Ms. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Pharmacy Pharmacy
BRENTWOOD EAST FAMILY MEDICINE Patient Registration Form (ecw) PATIENT INFORMATION Dr. Miss Mr. Mrs. Ms. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Pharmacy Pharmacy
1MFBTF GJMM PVU GPSNT BOE GBY 'PSNT XJMM CF TJHOFE BU ZPVS BQQPJOUNFOU
 CELL PHONE: PATIENT HISTORY FORM - CONFIDENTIAL DATE: PATIENT: (LAST NAME) (FIRST NAME) (Ml) (NICKNAME) DOB: Primary Physician/ Family Doctor: Phone: Past Medical History (Click all that apply) High blood
CELL PHONE: PATIENT HISTORY FORM - CONFIDENTIAL DATE: PATIENT: (LAST NAME) (FIRST NAME) (Ml) (NICKNAME) DOB: Primary Physician/ Family Doctor: Phone: Past Medical History (Click all that apply) High blood
412 Holistic Health, LLC Maura Schuster, L.OM 412.841.2065 Practitioner of Oriental Medicine NEW PATIENT INTAKE
 412 Holistic Health, LLC Maura Schuster, L.OM 412.841.2065 Practitioner of Oriental Medicine NEW PATIENT INTAKE PATIENT INFORMATION Date Name Address City State Zip Age Birthdate Occupation Company name
412 Holistic Health, LLC Maura Schuster, L.OM 412.841.2065 Practitioner of Oriental Medicine NEW PATIENT INTAKE PATIENT INFORMATION Date Name Address City State Zip Age Birthdate Occupation Company name
Relation Address City State Zip Code
 To enable us to provide you with the best possible care, please complete the following: Date: Name Social Security # First Full Middle Last Address City Zip Code_ Telephone (home) (work) Date of Birth
To enable us to provide you with the best possible care, please complete the following: Date: Name Social Security # First Full Middle Last Address City Zip Code_ Telephone (home) (work) Date of Birth
Prevents future health problems. You receive these services without having any specific symptoms.
 Preventive Care To help you live the healthiest life possible, we offer free preventive services for most Network Health members. Please refer to your member materials, which you received when you enrolled
Preventive Care To help you live the healthiest life possible, we offer free preventive services for most Network Health members. Please refer to your member materials, which you received when you enrolled
PATIENT HEALTH QUESTIONNAIRE: Urology
 PATIENT HEALTH QUESTIONNAIRE: Urology Patient Name: Sex: M F Last, First, Middle Initial Email: Date of Birth: \ \ Age: Social Sec #: - - Type of visit: Consultation requested by another Physician Self-referred
PATIENT HEALTH QUESTIONNAIRE: Urology Patient Name: Sex: M F Last, First, Middle Initial Email: Date of Birth: \ \ Age: Social Sec #: - - Type of visit: Consultation requested by another Physician Self-referred
319 Airport Road Hackettstown, NJ 07840 Ph: 908-850-0888 / FAX: 908-850-1005
 319 Airport Road Hackettstown, NJ 07840 Ph: 908-850-0888 / FAX: 908-850-1005 Dear New Patient: Thank you for choosing Holistic Family Healthcare as your holistic healthcare provider. Our goal is to help
319 Airport Road Hackettstown, NJ 07840 Ph: 908-850-0888 / FAX: 908-850-1005 Dear New Patient: Thank you for choosing Holistic Family Healthcare as your holistic healthcare provider. Our goal is to help
Emory Eye Center New Patient Questionnaire
 Patient Name: Date: Current Address: Current Phone: Date of Birth: Primary Care Physician: Referring Physician: (First & Last Name) (First & Last Name) Pharmacy Name: Phone #: ( ) Please answer all questions
Patient Name: Date: Current Address: Current Phone: Date of Birth: Primary Care Physician: Referring Physician: (First & Last Name) (First & Last Name) Pharmacy Name: Phone #: ( ) Please answer all questions
FATHER Present Health MOTHER Present Health Spouse Present Health
 PATIENT INFORMATION : SS/HIC/Patient ID#: Patient Name: Last Name First Name Middle Initial Address: City: State: Zip Home Phone: Cell Phone: E-mail: Sex: Age: Birthday: Race: American Indian Asia Pacific
PATIENT INFORMATION : SS/HIC/Patient ID#: Patient Name: Last Name First Name Middle Initial Address: City: State: Zip Home Phone: Cell Phone: E-mail: Sex: Age: Birthday: Race: American Indian Asia Pacific
Full name DOB Age Address Email Phone numbers (H) (W) (C) Emergency contact Phone
 (W) (C) Emergency contact Phone") DEMOGRAPHIC INFORMATION Full name DOB Age Address Email Phone numbers (H) (W) (C) Emergency contact Phone CARE INFORMATION Primary care physician: Address Phone Fax Referring physician: Specialty Address
DEMOGRAPHIC INFORMATION Full name DOB Age Address Email Phone numbers (H) (W) (C) Emergency contact Phone CARE INFORMATION Primary care physician: Address Phone Fax Referring physician: Specialty Address
Leader's Resource. Note: Both men and women can have an STD without physical symptoms.
 Leader's Resource Information on Sexually Transmitted Diseases (STDs) Signs and Symptoms of STDs Note: Both men and women can have an STD without physical symptoms. Any of the following can indicate to
Leader's Resource Information on Sexually Transmitted Diseases (STDs) Signs and Symptoms of STDs Note: Both men and women can have an STD without physical symptoms. Any of the following can indicate to
BE SURE. BE SAFE. VACCINATE.
 DON T GET OR GIVE THE FLU THIS YEAR THANK YOU Vaccination is the only protection. www.immunisation.ie BE SURE. BE SAFE. VACCINATE. FLU VACCINE 2013-2014 Healthcare workers prevent the spread of flu and
DON T GET OR GIVE THE FLU THIS YEAR THANK YOU Vaccination is the only protection. www.immunisation.ie BE SURE. BE SAFE. VACCINATE. FLU VACCINE 2013-2014 Healthcare workers prevent the spread of flu and
Chlamydia THE FACTS. How do people get Chlamydia?
 What is Chlamydia? Chlamydia is a common bacterial infection that is sexually transmitted and often causes no symptoms. If not treated, chlamydia can damage reproductive organs and make it difficult for
What is Chlamydia? Chlamydia is a common bacterial infection that is sexually transmitted and often causes no symptoms. If not treated, chlamydia can damage reproductive organs and make it difficult for
New Patient Intake Form
 New Patient Intake Form Title: (Circle one) Mr. Mrs. Ms. Miss Dr. Other First Name Middle Initial Last Name Address City State Zip Code Leave Messages on: (Circle one) Home Cell Work Don t leave messages
New Patient Intake Form Title: (Circle one) Mr. Mrs. Ms. Miss Dr. Other First Name Middle Initial Last Name Address City State Zip Code Leave Messages on: (Circle one) Home Cell Work Don t leave messages
What is cervical cancer?
 What is cervical cancer? Cervical cancer is a term used for a tumour that starts in the cervix where the uterus (womb) meets the vagina (birth canal). The cells of the cervix don t suddenly turn into cancer;
What is cervical cancer? Cervical cancer is a term used for a tumour that starts in the cervix where the uterus (womb) meets the vagina (birth canal). The cells of the cervix don t suddenly turn into cancer;
PATIENT INFORMATION. Patient Name/Nombre
 Patient Information Cont d PATIENT INFORMATION Patient Name/Nombre Birth date/fecha de Nacimeinto Age/Edad Sex/Sexo How do you prefer to be addressed by our physicians and staff? Como prefiere que le llamen
Patient Information Cont d PATIENT INFORMATION Patient Name/Nombre Birth date/fecha de Nacimeinto Age/Edad Sex/Sexo How do you prefer to be addressed by our physicians and staff? Como prefiere que le llamen
Other Healthcare Providers Medical Doctor: Location: Permission to contact? (Y/N) Specialist: Location: Permission to contact?
 Specialist: Location: Permission to contact?") Other Healthcare Providers Medical Doctor: Location: Permission to contact? (Y/N) Dr. James Yoon, ND Date of last visit: Specialist: Location: Permission to contact? (Y/N) Specialist: Location: Permission
Other Healthcare Providers Medical Doctor: Location: Permission to contact? (Y/N) Dr. James Yoon, ND Date of last visit: Specialist: Location: Permission to contact? (Y/N) Specialist: Location: Permission
Western Center Eye Care 2720 Western Center Blvd Ste 316 Fort Worth, TX 76131
 Today s Date Western Center Eye Care WELCOME TO OUR OFFICE Patient s Name (First, Middle, Last): Address: City: State: Zip Code: Email: Main Contact #: Alternate#: Date of Birth: / / Sex: Male Female Primary
Today s Date Western Center Eye Care WELCOME TO OUR OFFICE Patient s Name (First, Middle, Last): Address: City: State: Zip Code: Email: Main Contact #: Alternate#: Date of Birth: / / Sex: Male Female Primary
WORKERS COMPENSATION INFORMATION
 WORKERS COMPENSATION INFORMATION PATIENT REGISTRATION INFORMATION 15215 Shady Grove Rd. # 100 Patient Name: Last First MI Address: Street City State Zip Home Phone: Cell Phone: Work Phone: Primary Doctor:
WORKERS COMPENSATION INFORMATION PATIENT REGISTRATION INFORMATION 15215 Shady Grove Rd. # 100 Patient Name: Last First MI Address: Street City State Zip Home Phone: Cell Phone: Work Phone: Primary Doctor:
MEDICATION GUIDE STELARA
 MEDICATION GUIDE STELARA (stel ar a) (ustekinumab) Injection What is the most important information I should know about STELARA? STELARA is a medicine that affects your immune system. STELARA can increase
MEDICATION GUIDE STELARA (stel ar a) (ustekinumab) Injection What is the most important information I should know about STELARA? STELARA is a medicine that affects your immune system. STELARA can increase
NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only)
") PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
IMPORTANT: PLEASE READ
 PART III: CONSUMER INFORMATION combined hepatitis A (inactivated) and hepatitis B (recombinant) vaccine This leaflet is part III of a three-part "Product Monograph" published when was approved for sale
PART III: CONSUMER INFORMATION combined hepatitis A (inactivated) and hepatitis B (recombinant) vaccine This leaflet is part III of a three-part "Product Monograph" published when was approved for sale
Riverwalk Physical Therapy, L.L.C. ACUPUNCTURE HEALTH HISTORY QUESTIONNAIRE
 Riverwalk Physical Therapy, L.L.C. ACUPUNCTURE HEALTH HISTORY QUESTIONNAIRE Name: Date: Street: City: State: Zip: Cell Phone: Home Phone: Occupation: Marital Status: Date of Birth: Age: Gender: M F Height:
Riverwalk Physical Therapy, L.L.C. ACUPUNCTURE HEALTH HISTORY QUESTIONNAIRE Name: Date: Street: City: State: Zip: Cell Phone: Home Phone: Occupation: Marital Status: Date of Birth: Age: Gender: M F Height:
Las Vegas Neuroscience and Pain medicine Institute
 ****************************************************************************************** ****************************************************************************************** IMPORTANT INFORMATION
****************************************************************************************** ****************************************************************************************** IMPORTANT INFORMATION
SOUTH TAMPA MULTIPLE SCLEROSIS CENTER
 SOUTH TAMPA MULTIPLE SCLEROSIS CENTER PATIENT/CARE GIVER QUESTIONNAIRE DEMOGRAPHIC INFORMATION Patient's Name: City: State: Zip Code: Phone: Marital Status: Spouse/Care Giver Name: Phone (H) (W) Occupation:
SOUTH TAMPA MULTIPLE SCLEROSIS CENTER PATIENT/CARE GIVER QUESTIONNAIRE DEMOGRAPHIC INFORMATION Patient's Name: City: State: Zip Code: Phone: Marital Status: Spouse/Care Giver Name: Phone (H) (W) Occupation:
State of Illinois Department of Healthcare and Family Services Healthcare Programs for Families
 State of Illinois Department of Healthcare and Family Services Healthcare Programs for Families Member Handbook Table of Contents Healthcare programs for families...1 Welcome to your health insurance program!...1
State of Illinois Department of Healthcare and Family Services Healthcare Programs for Families Member Handbook Table of Contents Healthcare programs for families...1 Welcome to your health insurance program!...1
Southwestern Foot & Ankle Associates, P.C. 3880 Parkwood Blvd, Suite 602 Frisco, TX 75034 Phone: 972-335-9071 Fax: 972-335-8920 Dr. Thomas H.
 Phone: 972-335-9071 Fax: 972-335-8920 Date: Home Phone ( ) Patient Information (Please Print) Email: Name: SS/Patient ID # Last Name First Name Middle Initial Address Cell Phone ( ) City State Zip Sex
Phone: 972-335-9071 Fax: 972-335-8920 Date: Home Phone ( ) Patient Information (Please Print) Email: Name: SS/Patient ID # Last Name First Name Middle Initial Address Cell Phone ( ) City State Zip Sex
Preventive Care Services Health Care Reform The following benefits are effective beginning the first plan year on or after Sept.
 Coding Summary for Providers NOTE THE FOLLOWING: The purpose of this document is to provide a quick reference of the applicable codes for UnitedHealthcare plans that cover preventive care services in accordance
Coding Summary for Providers NOTE THE FOLLOWING: The purpose of this document is to provide a quick reference of the applicable codes for UnitedHealthcare plans that cover preventive care services in accordance
Life Insurance Application Form
 Life Insurance Application Form INSTRUCTION To be completed by all applicants PERSONAL DETAILS Surname First name Middle name Sex Female Male Marital status (please tick) Single Married Other Current residential
Life Insurance Application Form INSTRUCTION To be completed by all applicants PERSONAL DETAILS Surname First name Middle name Sex Female Male Marital status (please tick) Single Married Other Current residential
Plan your health.live your life. A Guide To Making A Reproductive Life Plan That Is Right For YOU!!
 Plan your health.live your life A Guide To Making A Reproductive Life Plan That Is Right For YOU!! What is a Reproductive Plan and Why is it important for me?? A Reproductive Life Plan( RLP) is a set of
Plan your health.live your life A Guide To Making A Reproductive Life Plan That Is Right For YOU!! What is a Reproductive Plan and Why is it important for me?? A Reproductive Life Plan( RLP) is a set of
Borland-Groover Clinic PATIENT GENERATED MEDICAL HISTORY Name: DOB: Email: Primary Care Physician: Pharmacy: Pharmacy Phone #:
 PATIENT GENERATED MEDICAL HISTORY Name: DOB: Email: Primary Care Physician: Referring: Pharmacy: Pharmacy Phone #: Place Sticker Here Directions: Please circle any of the following you have personally
PATIENT GENERATED MEDICAL HISTORY Name: DOB: Email: Primary Care Physician: Referring: Pharmacy: Pharmacy Phone #: Place Sticker Here Directions: Please circle any of the following you have personally
For the Patient: Paclitaxel injection Other names: TAXOL
 For the Patient: Paclitaxel injection Other names: TAXOL Paclitaxel (pak'' li tax' el) is a drug that is used to treat many types of cancer. It is a clear liquid that is injected into a vein. Tell your
For the Patient: Paclitaxel injection Other names: TAXOL Paclitaxel (pak'' li tax' el) is a drug that is used to treat many types of cancer. It is a clear liquid that is injected into a vein. Tell your
Pulmonary Associates of Richmond
 Pulmonary Associates of Richmond Name: Address One: City: Home Phone#: Work Phone#: Cell Phone#: State: Zip: Sex: Social Security Number: Referring Doctor: of Birth: Employer: Primary Care Doctor: Employment
Pulmonary Associates of Richmond Name: Address One: City: Home Phone#: Work Phone#: Cell Phone#: State: Zip: Sex: Social Security Number: Referring Doctor: of Birth: Employer: Primary Care Doctor: Employment
School Board of Broward County
 School Board of Broward County Open Enrollment 2013 Table of Contents Preventive Care Coverage...1 Knowing where to go can help you save on health care costs...2 Coventry WellBeing...3 WellBeing has its
School Board of Broward County Open Enrollment 2013 Table of Contents Preventive Care Coverage...1 Knowing where to go can help you save on health care costs...2 Coventry WellBeing...3 WellBeing has its
PATIENT DEMOGRAPHICS
 PATIENT DEMOGRAPHICS Prefix: Patient's First Name: Preferred Name: M.I.: Last Name: Mailing Address: Apt: City: State: Zip Code: Social Security No. (necessary for billing): Guardian's Last Name (if patient
PATIENT DEMOGRAPHICS Prefix: Patient's First Name: Preferred Name: M.I.: Last Name: Mailing Address: Apt: City: State: Zip Code: Social Security No. (necessary for billing): Guardian's Last Name (if patient
71 Spit Brook Road, Suite 407 Nashua, NH 03060
 71 Spit Brook Road, Suite 407 Nashua, NH 03060 Welcome! I look forward to helping you to meet your health goals. Please take a few minutes to fill out this questionnaire to help me to serve you better.
71 Spit Brook Road, Suite 407 Nashua, NH 03060 Welcome! I look forward to helping you to meet your health goals. Please take a few minutes to fill out this questionnaire to help me to serve you better.
St. Luke s MS Center New Patient Questionnaire. Name: Date: Birth date: Right or Left handed? Who is your Primary Doctor?
 St. Luke s MS Center New Patient Questionnaire Name: Date: Birth date: Right or Left handed? Who is your Primary Doctor? Who referred you to the MS Center? List any other doctors you see: Reason you have
St. Luke s MS Center New Patient Questionnaire Name: Date: Birth date: Right or Left handed? Who is your Primary Doctor? Who referred you to the MS Center? List any other doctors you see: Reason you have
PATIENT HISTORY FORM
 PATIENT HISTORY FORM If you are new to the office, have not been seen in over one (1) year, or are returning for a new problem, please complete this form in full. If there have been any changes since your
PATIENT HISTORY FORM If you are new to the office, have not been seen in over one (1) year, or are returning for a new problem, please complete this form in full. If there have been any changes since your
How To Fill Out A Health Declaration
 The English translation has no legal force and is provided to the customer for convenience only. The Dutch health declaration should be filled in. Health declaration for occupational disability insurance
The English translation has no legal force and is provided to the customer for convenience only. The Dutch health declaration should be filled in. Health declaration for occupational disability insurance
LOEWENBERG SCHOOL OF NURSING LOEWENBERG SCHOOL OF NURSING HEALTH EXAMINATION FORM (FORM 003)
") SECTION I: To be completed by STUDENT: Name: DOB: Address: Phone (H): Phone (C): Health History: Please complete the following information: Recent weight loss or gain Fatigue, fever, sweats Difficulty
SECTION I: To be completed by STUDENT: Name: DOB: Address: Phone (H): Phone (C): Health History: Please complete the following information: Recent weight loss or gain Fatigue, fever, sweats Difficulty
Pregnancy True Not True Can't Say
 Child's Name Date of Birth Date form filled out The information obtained from the following checklists will assist us in our evaluations of your child. Please try to answer all the questions, even though
Child's Name Date of Birth Date form filled out The information obtained from the following checklists will assist us in our evaluations of your child. Please try to answer all the questions, even though
COURSE: Workplace Spanish for HOSPITALS & NURSES ISBN# 1-930134-18-5 WHO WILL BENEFIT FROM THIS COURSE:
 Workplace Spanish, Inc. HOSPITAS & NURSES The rapid growth of the Hispanic population & workforce has created critical communication challenges for business, government and education. These language barriers
Workplace Spanish, Inc. HOSPITAS & NURSES The rapid growth of the Hispanic population & workforce has created critical communication challenges for business, government and education. These language barriers
Dallas Neurosurgical and Spine Associates, P.A Patient Health History
 Dallas Neurosurgical and Spine Associates, P.A Patient Health History DOB: Date: Reason for your visit (Chief complaint): Past Medical History Please check corresponding box if you have ever had any of
Dallas Neurosurgical and Spine Associates, P.A Patient Health History DOB: Date: Reason for your visit (Chief complaint): Past Medical History Please check corresponding box if you have ever had any of
NEW YORK SPINE & PAIN PHYSICIANS NEW PATIENT QUESTIONNAIRE
 NEW YORK SPINE & PAIN PHYSICIANS NEW PATIENT QUESTIONNAIRE DEMOGRAPHICS- To be completed by all patients Patient Name: Today s Date: / / Patient Address: _ City: State: Zip: Home Phone #: ( ) - Work #:
NEW YORK SPINE & PAIN PHYSICIANS NEW PATIENT QUESTIONNAIRE DEMOGRAPHICS- To be completed by all patients Patient Name: Today s Date: / / Patient Address: _ City: State: Zip: Home Phone #: ( ) - Work #:
NEW PATIENT CONSULTATION FORM. Social Security Number - - Date of Birth Age. Home Address. Home phone Cell phone. Work phone Email address
 NEW PATIENT CONSULTATION FORM Welcome to our office. Please fill out the first four pages. Date Name Social Security Number - - Date of Birth Age Home Address Home phone Cell phone Work phone Email address
NEW PATIENT CONSULTATION FORM Welcome to our office. Please fill out the first four pages. Date Name Social Security Number - - Date of Birth Age Home Address Home phone Cell phone Work phone Email address
PEDIATRIC HEALTH, P.A. PLEASE PRINT AND COMPLETE ALL ENTRIES Patient Name (Last, First, MI) Date of Birth Sex Today's Date
 Date of Birth Sex Today's Date") PEDIATRIC HEALTH, P.A. PLEASE PRINT AND COMPLETE ALL ENTRIES Patient Name (Last, First, MI) Date of Birth Sex Today's Date M F Address (Street, City, State, Zip) Home Phone Pt Social Security # () -_ Mother's
PEDIATRIC HEALTH, P.A. PLEASE PRINT AND COMPLETE ALL ENTRIES Patient Name (Last, First, MI) Date of Birth Sex Today's Date M F Address (Street, City, State, Zip) Home Phone Pt Social Security # () -_ Mother's
 Additional details >>> HERE
Additional details >>> HERE PODIATRIC ASSOCIATES OF NW OHIO, INC. PATIENT HISTORY INSURANCE INFORMATION
 PODIATRIC ASSOCIATES OF NW OHIO, INC. DATE PATIENT HISTORY PATIENT S LAST NAME FIRST NAME MIDDLE SOCIAL SECURITY NUMBER ADDRESS STREET APT. NO. CITY STATE ZIP DATE OF BIRTH AGE SEX MARITAL STATUS HOME/CELL
PODIATRIC ASSOCIATES OF NW OHIO, INC. DATE PATIENT HISTORY PATIENT S LAST NAME FIRST NAME MIDDLE SOCIAL SECURITY NUMBER ADDRESS STREET APT. NO. CITY STATE ZIP DATE OF BIRTH AGE SEX MARITAL STATUS HOME/CELL
*3451 BARIATRIC SERVICE HEALTH QUESTIONNAIRE
 BARIATRIC SERVICE HEALTH QUESTIONNAIRE Name: Male Female Address: City: State: Zip: Home Phone: ( ) E-Mail: Mobile Phone: ( ) Primary Language: Religious Preference : Education Level: Date of Birth: Social
BARIATRIC SERVICE HEALTH QUESTIONNAIRE Name: Male Female Address: City: State: Zip: Home Phone: ( ) E-Mail: Mobile Phone: ( ) Primary Language: Religious Preference : Education Level: Date of Birth: Social
Preterm Labour. Signs & Symptoms. Learn about the signs of preterm labour and what to do if it happens.
 An important message for pregnant women, their partners and families Preterm Labour Signs & Symptoms Learn about the signs of preterm labour and what to do if it happens. What is preterm labour? A normal,
An important message for pregnant women, their partners and families Preterm Labour Signs & Symptoms Learn about the signs of preterm labour and what to do if it happens. What is preterm labour? A normal,
MEDICAL HISTORY INFORMATION
 MEDICAL HISTORY INFORMATION Name: Birthdate: Age: Address: Home Telephone: Cell Telephone: Work Telephone: Social Security Number: Marital Status: Single Married Divorced Widowed Spouse s Name: Birthdate:
MEDICAL HISTORY INFORMATION Name: Birthdate: Age: Address: Home Telephone: Cell Telephone: Work Telephone: Social Security Number: Marital Status: Single Married Divorced Widowed Spouse s Name: Birthdate:
Patient Information. Today s date: Your Name: Social Security Number: Date of Birth: Age: Height: Weight: lbs. Street Address: City/State/Zip:
 Welcome to Avenstar Pain Specialists! Your completed intake paperwork helps our providers get to know you and your medical history. We rely on its accuracy and completeness to provide you with the best
Welcome to Avenstar Pain Specialists! Your completed intake paperwork helps our providers get to know you and your medical history. We rely on its accuracy and completeness to provide you with the best
Infant / Child New Patient Information Package Dr. Anne M. Desneiges - Chiropractor
 Dr. Anne Desneiges Inner Waves Centre for Well~Being Infant / Child New Patient Information Package Dr. Anne M. Desneiges - Chiropractor Name: Address: Postal code: street city Telephone: home: ( ) work:
Dr. Anne Desneiges Inner Waves Centre for Well~Being Infant / Child New Patient Information Package Dr. Anne M. Desneiges - Chiropractor Name: Address: Postal code: street city Telephone: home: ( ) work:
Sore Throat. Definition. Causes. (Pharyngitis; Tonsillopharyngitis; Throat Infection) Pronounced: Fare-en-JY-tis /TAHN-sill-oh-fare-en-JY-tis
 Pronounced: Fare-en-JY-tis /TAHN-sill-oh-fare-en-JY-tis") Sore Throat (Pharyngitis; Tonsillopharyngitis; Throat Infection) Pronounced: Fare-en-JY-tis /TAHN-sill-oh-fare-en-JY-tis by Jennifer Lewy, MSW En Español (Spanish Version) Definition A sore throat is the
Sore Throat (Pharyngitis; Tonsillopharyngitis; Throat Infection) Pronounced: Fare-en-JY-tis /TAHN-sill-oh-fare-en-JY-tis by Jennifer Lewy, MSW En Español (Spanish Version) Definition A sore throat is the
INFLUENZA (FLU) Flu and You
 Flu and You") Influenza (Flu) What is the flu? The flu is an illness caused by flu viruses. The flu may make people cough and have a sore throat and fever. They may also have a runny or stuffy nose, feel tired, have
Influenza (Flu) What is the flu? The flu is an illness caused by flu viruses. The flu may make people cough and have a sore throat and fever. They may also have a runny or stuffy nose, feel tired, have
THE AYURVEDIC CENTER OF VERMONT, LLC Health Information and History
 THE AYURVEDIC CENTER OF VERMONT, LLC Health Information and History Name DOB Date Age Occupation Email Address Home address City State Zip Home phone Cell Phone Referred By Physician Physician Phone Please
THE AYURVEDIC CENTER OF VERMONT, LLC Health Information and History Name DOB Date Age Occupation Email Address Home address City State Zip Home phone Cell Phone Referred By Physician Physician Phone Please
The NeuroCenter Swedish Covenant Medical Group 6225 W. Touhy Ave, Chicago, Il 60646 Tel: 773-775-7540 Fax: 773-763-9792
 The NeuroCenter Swedish Covenant Medical Group 6225 W. Touhy Ave, Chicago, Il 60646 Tel: 773-775-7540 Fax: 773-763-9792 1 PAIN MANAGEMENT SERVICES New Patient Questionnaire Date: Primary MD: Referring
The NeuroCenter Swedish Covenant Medical Group 6225 W. Touhy Ave, Chicago, Il 60646 Tel: 773-775-7540 Fax: 773-763-9792 1 PAIN MANAGEMENT SERVICES New Patient Questionnaire Date: Primary MD: Referring
HPSM Medi-Cal Benefits
 HPSM Medi-Cal Benefits A Guide on How to Get Your Health Care Health care and insurance benefits can be difficult to understand. This guide introduces you to your basic Medi-Cal benefits, to the Health
HPSM Medi-Cal Benefits A Guide on How to Get Your Health Care Health care and insurance benefits can be difficult to understand. This guide introduces you to your basic Medi-Cal benefits, to the Health
State of Illinois Department of Healthcare and Family Services Healthcare Programs for Families
 State of Illinois Department of Healthcare and Family Services Healthcare Programs for Families Member Handbook Table of Contents Healthcare programs for families...1 Welcome to your health insurance program!...1
State of Illinois Department of Healthcare and Family Services Healthcare Programs for Families Member Handbook Table of Contents Healthcare programs for families...1 Welcome to your health insurance program!...1
Dear Incoming Student:
 FOR THE ADVANCEMENT OF SCIENCE AND ART Dear Incoming Student: It is mandatory that you complete and return the enclosed Cooper Union health forms and the New York State required response forms for Meningitis,
FOR THE ADVANCEMENT OF SCIENCE AND ART Dear Incoming Student: It is mandatory that you complete and return the enclosed Cooper Union health forms and the New York State required response forms for Meningitis,
PATIENT INFORMATION INSURANCE PHONE NUMBERS ACCIDENT INFORMATION GENERAL INFORMATION. Sex: M F Age Birthdate. Date. Name. Relationship to Patient
 PATIENT INFORMATION Name Address City State Zip Sex: M F Age Birthdate Single Married Significant Other Widowed Separated Divorced Patient SS# Occupation Employer Emp. Address Emp. Phone Spouse/Partner
PATIENT INFORMATION Name Address City State Zip Sex: M F Age Birthdate Single Married Significant Other Widowed Separated Divorced Patient SS# Occupation Employer Emp. Address Emp. Phone Spouse/Partner
Tuberculosis and You A Guide to Tuberculosis Treatment and Services
 Tuberculosis and You A Guide to Tuberculosis Treatment and Services Tuberculosis (TB) is a serious disease that can damage the lungs or other parts of the body like the brain, kidneys or spine. There are
Tuberculosis and You A Guide to Tuberculosis Treatment and Services Tuberculosis (TB) is a serious disease that can damage the lungs or other parts of the body like the brain, kidneys or spine. There are
FREQUENTLY ASKED QUESTIONS ABOUT PERTUSSIS (WHOOPING COUGH)
") FREQUENTLY ASKED QUESTIONS ABOUT PERTUSSIS (WHOOPING COUGH) What is pertussis? General Questions About Pertussis Pertussis, or whooping cough, is a contagious illness that is spread when an infected person
FREQUENTLY ASKED QUESTIONS ABOUT PERTUSSIS (WHOOPING COUGH) What is pertussis? General Questions About Pertussis Pertussis, or whooping cough, is a contagious illness that is spread when an infected person
MEDICATION GUIDE. ACTEMRA (AC-TEM-RA) (tocilizumab) Solution for Intravenous Infusion
 (tocilizumab) Solution for Intravenous Infusion") MEDICATION GUIDE ACTEMRA (AC-TEM-RA) (tocilizumab) Solution for Intravenous Infusion ACTEMRA (AC-TEM-RA) (tocilizumab) Injection, Solution for Subcutaneous Administration Read this Medication Guide before
MEDICATION GUIDE ACTEMRA (AC-TEM-RA) (tocilizumab) Solution for Intravenous Infusion ACTEMRA (AC-TEM-RA) (tocilizumab) Injection, Solution for Subcutaneous Administration Read this Medication Guide before
Like cocaine, heroin is a drug that is illegal in some areas of the world. Heroin is highly addictive.
 Heroin Introduction Heroin is a powerful drug that affects the brain. People who use it can form a strong addiction. Addiction is when a drug user can t stop taking a drug, even when he or she wants to.
Heroin Introduction Heroin is a powerful drug that affects the brain. People who use it can form a strong addiction. Addiction is when a drug user can t stop taking a drug, even when he or she wants to.
Emergency Care for Patients of The James
 PATIENT EDUCATION patienteducation.osumc.edu Emergency Care for Patients of The James Emergency Care During and After Treatment Here are guidelines about when and how to report problems that you may have
PATIENT EDUCATION patienteducation.osumc.edu Emergency Care for Patients of The James Emergency Care During and After Treatment Here are guidelines about when and how to report problems that you may have