AGENCY OF HUMAN SERVICES PROGRAMS AND SUBSTANCE ABUSE CONTINUUM OF SERVICES; REVIEW AND RECOMMENDATION
|
|
|
- Alban Nash
- 8 years ago
- Views:
Transcription
1 Report to The Vermont Legislature AGENCY OF HUMAN SERVICES PROGRAMS AND SUBSTANCE ABUSE CONTINUUM OF SERVICES; REVIEW AND RECOMMENDATION In Accordance with Act 50, Sec. E An Act relating to making appropriations for the support of government. Submitted to: Submitted by: Prepared by: House Committee on Appropriations Senate Committee on Appropriations Douglas A. Racine Secretary, Agency of Human Services Barbara Cimaglio Deputy Commissioner, Vermont Department of Health Report date: January 15, 2014 AHS Central Office Suite Hurricane Lane Williston, VT 05495

2 Act 50. Sec. E Legislative Report AGENCY OF HUMAN SERVICES PROGRAMS AND SUBSTANCE ABUSE CONTINUUM OF SERVICES; Legislative Charge REVIEW AND RECOMMENDATION (a) To ensure Agency programs serve persons with substance abuse and persons with co-occurring substance abuse, medical, and mental health conditions, the Secretary of Human Services shall report on the capacity of the system, including outpatient, inpatient, residential treatment, and recovery substance abuse, medical, and mental health services to address these needs. In addition to the resources of the Agency, the Secretary may seek the advice and consultation of independent persons with clinical case management and public policy expertise to assess current policies and resources available within the Agency and make recommendations to change current policies, change the allocations of resources, restructure payment systems, and prioritize future additional resources. The Secretary of Education, the Commissioner of Labor, the Administrative Judge in the Judiciary, and leaders in the State s law enforcement agencies are expected to be available as needed for consultation in this effort as well as the report on opioid addiction required in H.522 of the 2013 legislative session. The Secretary of Human Services shall report to the General Assembly with this assessment and recommendations by January 15 INTRODUCTION Historically, substance abuse treatment services have been funded through Federal grants and limited allocations of Medicaid and other state funds. As Vermont implements the Affordable Care Act our vision is to treat substance abuse disorders and co-occurring mental health disorders in the same way we treat other chronic diseases. This implies developing provider networks that include a basic range of services from prevention through recovery supports that are available statewide. We have started on this path with the development of a system for delivering Medication-Assisted Treatment through a partnership with the Blueprint for Health (hub and spoke system). These partnerships will be enhanced to include links to other levels of care, outpatient through residential. Patient need for specialty services will be determined through the use of evidence-based screening protocols. The concept is to link primary care medical homes to specialty addiction and co-occurring mental health services. It is with this vision in mind that the current system components are reviewed. 1

3 Context of Substance Abuse and Mental Health Disorders Mental health and substance use disorders are common, recurrent, and often serious, but treatable. Importantly, different disorders have different ages at which symptoms tend to occur, get worse, or get better. Thus, understanding the onset, course, and prevalence of these disorders across the life span is an essential step in preventing and treating addiction, and assisting in recovery. 1 Almost one in five young people has one or more mental, behavioral, or emotional disorder, including substance abuse. 2 About 11 percent of 13- to 18-year-olds have met the criteria for a lifetime alcohol or illicit drug use disorder. For adolescents, these disorders are most likely to appear around age 15. For adults, substance use disorder onset is about 20 years of age. 3 Prevalence of substance use disorders increases during adolescence. Between the ages of 13 and 14, approximately 4 percent of youth meet the criteria for a substance use disorder. The rate increases to 12 percent for those aged 15 and 16 and then to 22 percent for those aged 17 and Until adults reach the age of 60, the prevalence of substance use disorders remains relatively constant; approximately 17 percent of adults aged 18 to 29, 18 percent of adults aged 30 to 44, and 15 percent of adults aged 45 to 59 meet the criteria. However, the prevalence of substance use disorder drops to about 6 percent for adults aged 60 or older. Research has shown that early initiation of substance use increases the risk for subsequent substance use disorder. 5 For mental health, certain disorders or classes of disorders are more likely to begin during particular times in life and are thus more prevalent in certain age groups. Among adolescents between the ages of 13 and 18, lifetime anxiety disorders (e.g., generalized anxiety disorder, specific phobia) are the most prevalent (31 percent) and have the earliest median age of first onset, usually around age 6. Behavior disorders (e.g., attention-deficit/hyperactivity disorder [ADHD], conduct disorder, oppositional defiant disorder) are present in approximately 19 percent of adolescents and are most likely to first appear around age 11. Mood disorders (e.g., bipolar disorder, major depressive disorder) are experienced by approximately 14 percent of adolescents and are most likely to first appear around age Preventing Mental, Emotional and Behavioral Disorders Among Young People: Progress and Possibilities, National Research Council and Institute of Medicine, Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., & Swendsen, J. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication Adolescent Supplement (NCS- A). Journal of the American Academy of Child and Adolescent Psychiatry, 49(10), doi: /j.jaac Behrendt, S., Wittchen, H.-U., Höfler, M., Lieb, R., & Beesdo, K. (2009). Transitions from first substance use to substance use disorders in adolescence: Is early onset associated with a rapid escalation? Alcohol and drug Dependence, 99(1-3), doi: /j.drugalcdep boyle 6 Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., & Swendsen, J. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication Adolescent Supplement (NCS- A). Journal of the American Academy of Child and Adolescent Psychiatry, 49(10), doi: /j.jaac

4 Co-occurring mental health and substance use disorders can be quite complex to address. People with co-occurring disorders are more difficult to treat, more likely to have treatment adherence problems, and more likely to have poorer outcomes than those with only a mental health or substance use disorder. 7, 8 The functional impairment associated with co-occurring mental health and substance use disorders is often more pronounced than impairment associated with either a mental health disorder or a substance use disorder alone. Substance abuse and co-occurring mental health and substance use disorders are common in Vermont and significantly impact the health care system. It is estimated that: Approximately 10% of the Vermont population age 12 and older can be diagnosed with alcohol or drug dependence or abuse. 9 Approximately 20% of adult Vermonters had any mental illness in the last year. 10 Among those with a past year substance use disorder, 42.8 percent had a co-occurring mental illness. 11 Of mental health patients treated in Vermont s Designated Agencies, 19% also have a substance use diagnosis 12 The majority of people nationwide with co-occurring disorders receive no treatment but those that do receive care are significantly more likely to receive mental health care than substance abuse treatment Kelly, T. M., Daley, D. C., & Douaihy, A. B. (2012). Treatment of substance abusing patients with comorbid psychiatric disorders. Addictive Behavior, 37(1), doi: /j.addbeh Herbeck, D. M., Fitek, D. J., Svikis, D. S., Montoya, I. D., Marcus, S. C., & West, J. C. (2005). Treatment compliance in patients with comorbid psychiatric and substance use disorders. The American Journal on Addictions, 14(3), doi: / National Survey on Drug Use and Health, 2010 and

5 Past Year Mental Health and Substance Abuse Care for Adults with Co-Occurring Disorders 2011 Both Mental Health and and Substance Abuse Care 7% Substance Abuse Only 4% Mental Health Care Only 32% No Treatment 57% Challenges within the Current Service System Despite the number of people with substance use disorders, this condition is significantly under -treated for many reasons. More people access the health care system though primary care than any other access point but physicians receive very limited training to identify and treat substance use disorders, often less than 12 hours 14, which may be compounded by negative attitudes about treating substance abusers. People are also unlikely to seek help due a belief that their substance use is not an issue. Nationally, 94.6% of those who needed but did not seek treatment for alcohol or illicit drug didn t seek treatment because they did not believe they needed it. 15 In addition, when a physician does identify and refer a person to specialty treatment, there are constraints on sharing mental health and substance use treatment information imposed by Federal medical records privacy laws, specifically the consent and confidentiality requirements in 42 CFR Part 2, that make communications around substance abuse treatment complex and different than referrals for other types of care 16. For instance, Vermont Information Technology Leaders (VITL) has chosen to delay the inclusion of substance abuse specialty treatment providers from VITL because they could not easily resolve issues around consent and confidentiality. An additional challenge in providing and managing co-occurring care is related to the Federal funding sources that pay for care. There are different Federal funding standards and reporting requirements for each mental health and substance abuse and both are separate from typical payment and reporting 14 Isaacson JH, Fleming M, Kraus M, et al. A national survey of training in substance use disorders in residency programs. J Stud Alcohol. 2000;61: [PubMed]

6 structures for physical health care. This can make new initiatives challenging to implement. While parity is required per the Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA), there are still significant challenges to overcome in making care more accessible to clients. In Vermont, there are additional systems challenges. The majority of the Vermont Division of Alcohol and Drug Abuse Program s (ADAP) resources are allocated to the highest levels of care, residential treatment and Medication -Assisted Therapy (MAT). This means that there are fewer resources for prevention and early intervention which means that people do not receive services until the problem is severe. Resources are currently allocated based on demand for services, but demand which does not necessarily conform to evidence-based treatment guidelines. Research shows that outcomes for outpatient and residential treatment are similar 17 but residential care costs are nearly five times as much as outpatient care. There are also challenges associated with attracting and retaining qualified individuals to the field of substance abuse treatment and prevention. There are insufficient training opportunities, no opportunities for private practitioner Licensed Alcohol and Drug Counselors (LADC) to receive payment for providing services to Medicaid eligible patients and low wages for LADCs working in community provider settings. It is difficult to coordinate substance abuse care, such as between a physician and a substance abuse treatment provider, between providers of different levels of care such as between outpatient and residential care, and between the formal treatment system and the support services such as housing and employment. This often causes patients to leave care before they have completed their course of treatment. SUBSTANCE ABUSE AND CO-OCCURRING TREATMENT CAPACITY BY LEVELS OF CARE According to the National Coordination Replication Survey (NCS-R), adults with mental health disorders who receive treatment average about four visits to treatment per year. Those who receive treatment in specialized mental health care settings (e.g., from a psychologist) generally have more visits than those treated in general medical settings (e.g., from a primary care doctor) 18. People treated for substance use disorders average six visits per year, with those receiving care in a specialty setting (e.g., substance abuse treatment center) averaging more visits per year than those receiving care in a general medical setting (e.g., primary care practice). The national data suggest that most mental health or substance abuse treatment does not meet guidelines to be minimally adequate. 19 Adequate treatment in the NCS-R is defined as receiving certain 17 Hayashida M, Alterman AI, et al. Comparative Effectiveness and Costs of Inpatient and Outpatient Detoxification of Patients with Mild-to-Moderate Alcohol Withdrawal Syndrome. NE J of Medicine. 1989; Vol 320 Number 6: Wang et al., 2005b 19 The NCS-R defined minimally adequate treatment as receiving either pharmacotherapy ( 2 months of an appropriate medication for the mental health disorder plus >4 visits to any type of physician) or psychotherapy ( 8 visits with any health care or human services professional lasting an average of 30 minutes), based on available evidence-based guidelines from organizations such as the American Psychiatric Association (1998, 2000, 2002, 2004), the Agency for Healthcare Research and 5
 resources are allocated to the highest levels of care, residential treatment and Medication -Assisted Therapy (MAT).")
7 amounts of medication or treatment according to accepted guidelines. Rates of minimally adequate treatment are highest in the specialty mental health sector and lowest in the general medical care sector. While all ADAP Preferred Providers are required to have the expertise to treat people with co-occurring disorders, the level of expertise varies by provider and level of care. See Appendix I for a description of the Preferred Provider system and locations. Outpatient/Intensive Outpatient Outpatient services are the backbone of the treatment system, the equivalent of primary care in the physical health arena. All ADAP Preferred Providers are required to have the capability to identify and treat co-occurring disorders using evidence-based screening and assessment tools. Patients are assessed within the outpatient system to determine the care necessary to address substance abuse and mental health issues; the majority of substance abuse treatment patients may be helped with outpatient behavioral health care alone if he or she has a stable living situation. Outpatient treatment consists of group, individual, family treatment and case management services (up to eight hours of service). Patients with higher needs may receive intensive outpatient services, which is nine to 19 hours of outpatient services per week until the patient can decrease treatment intensity to regular outpatient care. When needed, outpatient providers refer to higher levels of care such as residential or medication assisted therapy (MAT). All client service needs are determined by using the American Society for Addiction Medicine Patient Placement Criteria (ASAM PPC-2R). This is a framework for determining the most appropriate clinical treatment setting based upon an assessment of the patient s functioning in key life areas. Behavioral health counseling is a component of all levels of care. In SFY12, 7193 people received outpatient care in Vermont s Preferred Provider system. The average SFY2013 Medicaid cost/client for outpatient/intensive outpatient care was $1,028, which reflects the cost of an assessment and approximately eight hours of outpatient care Residential The purpose of residential treatment is to stabilize patients though the detoxification process, begin the behavior modification process, and prepare patients to step down to outpatient care. Clients may receive up to 15 days of residential care; for those needing extended residential care, ADAP/DVHA has implemented a Utilization Review Process to approve additional medically necessary services. There are three providers of this service: Maple Leaf Farm, Serenity House, and Valley Vista. Valley Vista provides medically managed detoxification and has extensive co-occurring capabilities to serve very complex patients; Serenity House and Maple Leaf Farm provide social detoxification services and co-occurring care to moderately complex patients. Quality (formerly known as the Agency for Health Care Policy and Research) (1993), and the National Committee for Quality Assurance (1997). 6

8 There is one long term residential treatment program run by Phoenix House in Dublin N.H. This program provides up to six months of treatment. While in this program clients have access to psychiatric care. In addition, there is one short term social detoxification program, Howard s Act One/Bridge program. This program provides non-medical detoxification services in five or fewer days then refers the patient to an appropriate level of outpatient, residential, or medication assisted treatment. In SFY2012, 2084 people received residential care in the Preferred Provider system. Statewide SFY13 Medicaid average cost/client accessing residential care is $5,000 for approximately 20 days of care Medication Assisted Therapy or Opiod Care Alliance(Hub and Spoke) Medication Assisted Therapy (MAT) is an effective treatment for opioid addiction that involves prescribing medication methadone or buprenorphine in combination with counseling. MAT in Vermont is delivered through an integrated treatment model, called the Care Alliance for Opioid Treatment (Hub and Spoke), which was co-developed with DVHA, and relies on the strengths of the specialty methadone addiction treatment clinics, the physicians who prescribe buprenorphine in officebased settings, and the local Blueprint Community Health Teams and Medical Home infrastructure. This model consists of Hubs and Spokes described below. A Hub is a regional opioid treatment center responsible for coordinating the care and support services for patients who have complex addictions and co-occurring substance abuse and mental health conditions. Patients who need methadone must be treated here. Patients who need buprenorphine may or may not be treated here. Hubs serve as the regional consultants and subject matter experts on opioid dependence and treatment. Hubs are Health Home providers that integrate and coordinate all primary, acute behavioral health, and long-term services and supports to treat the whole person. By the end of SFY14, there will be five regional hubs. A Spoke is a medical home responsible for coordinating the care and support services for patients with opioid addictions who have less complex medical needs, such as in a primary care practice or health center. Only patients who are treated with buprenorphine receive treatment in the spokes. Spokes are supported in providing individuals with substance abuse issues with Health Home services through the Blueprint Community Health Teams. DMH, VDH, and the Blueprint are in active conversations about the expansion of Health Homes beyond Hub and Spoke. Analysis shows that a majority of Vermonters who suffer from one or more chronic health condition also have some form of co-occurring Mental Health condition. DMH, ADAP, and the Blueprint recognize the complexity of serving this population and have been coordinating to plan the expansion of Health Homes in Vermont. 7

9 Average cost/patient for Hub services: $5,920 (This rate includes methadone but excludes the cost of Suboxone. Annual Suboxone costs are $5,220 per patient for those using Suboxone.) It is anticipated that approximately 1800 individuals will receive Hub services in SFY14. Additional Types of Services Funded Through ADAP s Budget In addition to the formal levels of treatment listed above, ADAP funds Public Inebriate Program (PIP) services (see Public Inebriate Report to the Legislature submitted January 2008), as well as Halfway and Transitional Housing services. PIP is designed to keep inebriated individuals out of protective custody and provide screening and referral to treatment when needed. Halfway and transitional housing programs support patients who may be homeless or who may benefit from a sober living environment. These programs provide shelter and recovery support services; they do not provide formal treatment. Patients needing behavioral or health treatment are referred to other providers for these services. These services are not accessible statewide and would not be considered essential components of health services. Unless additional funds become available there would not be a way to expand these community services. It is also not feasible to envision these services being available in all communities because they are only cost effective where there are larger populations. Recovery Services There are eleven state funded Recovery Centers in Vermont. These are community based support programs and do not provide treatment but do collaborate with the Preferred Provider system. Recovery Centers are available to all individuals seeking support on a drop in basis regardless of treatment involvement. People with substance use disorders may participate only in activities at the Recovery Centers, such as Alcoholics Anonymous or Narcotics Anonymous, rather than accessing formal treatment elsewhere. This makes the Recovery Centers a very important component of the continuum of care. The Recovery Center hours of operation are limited by funding, the vast majority of which is state funding. Without state funding, Recovery Centers would not exist. Recovery centers are a participant along with DVHA, DMH, and ADAP in a pilot initiative that has sought to increase referrals between primary care providers and recovery supports. There are over 150,000 visits per year and 76% of visitors report current or past participation in outpatient/inpatient mental health services. Please see Appendix I for maps showing ADAP treatment, and recovery center locations. Community and School Based Prevention Services Prevention and health promotion strategies are designed to prevent disorders before they occur. Evidenced-based prevention strategies are most effective when they are targeted at certain developmental windows, such as early childhood and early adolescence and are multidisciplinary, requiring coordination of multiple human services and education programs. ADAP funds communitywide and school based prevention strategies. A combination of such strategies has demonstrated reductions in substance abuse in Vermont. Currently 21 supervisory unions and 28 prevention programs and coalitions receive grants. However, there has been a variety of funding reductions between 2011 and the present. Currently, prevention resources vary greatly from AHS region 8
, as well as Halfway and Transitional Housing services.")
10 to AHS region so capacity to carry out evidence based interventions is limited and inconsistent around the state. Examples of supported strategies include community education campaigns, support of education on responsible beverage service, school curricula, training for school staff, educational support groups for youth and parents, and screening and referral services. ENHANCING CAPACITY TO ADDRESS SUBSTANCE ABUSE AND CO-OCCURRING DISORDERS Current data suggests that Vermont can do better at identifying those at high risk for substance use and mental disorders. When a physician identifies substance use as an issue, the likelihood that the patient initiates treatment is less than 40% and the likelihood that the person continues treatment for 30 days, or treatment engagement, is under 23%. 20 There are both new and existing efforts to improve screening. One of the existing initiatives is a collaboration between VDH Maternal Child Health and ADAP to encourage pediatricians to screen for substance abuse. The Blueprint has also identified substance abuse and mental health as some of the chronic conditions for which expertise is necessary to be considered a National Committee for Quality Assurance (NCQA) Designated Medical Home. There are several new initiatives designed to address the connection between primary care and behavioral health care that may help improve rates of initiation and engagement in treatment. Screening, Brief Intervention, and Referral to Treatment (SBIRT) In August 2013, ADAP received a SAMHSA grant of $10M over five years for a Screening, Brief Intervention, and Referral to Treatment project. Grant funding will train health care professionals in medical settings to screen for abuse of alcohol and illicit substances, depression, and tobacco use as well as the use of intervention tools to employ for those screening positive. These health care professionals will provide services to 95,000 Vermonters over the grant period. The overlapping coordination between DMH and ADAP will occur once the referral is made. This grant extends Vermont s progress under the Blueprint for Health initiatives by further integrating behavioral health and physical health to focus on substance use risk for all Vermonters. Since the prevalence of co-occurring mental health and substance use disorders is so common it is essential to build strong referrals to both DMH and ADAP supported services. This will increase awareness of substance use and mental health issues throughout primary care on an ongoing basis. Funding will also be focused on the Vermont Health Information Exchange (VHIE). Medical providers will be able to effectively deliver and share integrated electronic health records decreasing provider and patient burden through new health information technology, policies, and procedures. Building this infrastructure will streamline services, improve the standard of coordinated care, and standardize evidence based substance use screenings as part of a visit to the doctor

11 Initiation and Engagement in Treatment Performance Indicator Project (IET) The Department of Vermont Health Access (DVHA) has received performance improvement funds from the Center for Medicare and Medicaid Services (CMS) and has selected the initiation and engagement of treatment for adults with alcohol diagnoses in Rutland County and surrounding area. This project will provide three interventions: 1) add treatment resources by allowing private practitioner Licensed Alcohol and Drug Counselors (LADC) to bill for services to Medicaid recipients, 2) notify physicians of the additional capacity, and 3) pay LADCs based on performance. Agency of Human Services Efforts to Address Substance Abuse and Co-Occurring Disorders Department of Mental Health/Department for Children and Families The Department of Mental Health has been addressing co-occurring disorders for several years. First, funded by a five year infrastructure planning grant from SAMHSA, the Vermont Integrated Services Initiative (VISI) provided training and technical assistance to a wide group of service providers to increase their programmatic and clinical capacity to effectively treat clients with co-occurring disorders. Twenty-six different service provider agencies participated in the project including community mental health centers, federally qualified health centers, housing and homeless service providers, and specialty residential providers. This grant ended in DVHA, DMH and ADAP have been working to improve the capacity of patient-centered medical homes statewide to provide mental health and substance abuse care to both individuals with mental health and substance abuse needs who are served by primary care practices, and individuals who live with varying substance abuse conditions. DMH, VDH and the Blueprint are collaborating to examine a state wide expansion of bi-directional care delivery. This means that primary care, mental health, and substance abuse supports will be provided in both primary care and Community Mental Health Center settings. The model will work to foster an environment where individuals can receive access to high-level evidence-based care wherever they feel most comfortable accessing both primary and mental health care. While most Primary Care Medical Home (PCMH) providers offer some existing level of mental health and substance abuse support inhouse or as a referral to the Community Health Team, clients of Community Mental Health Centers often do not have a meaningful relationship with a primary care provider and often do not seek out primary care for various reasons. Bringing primary care to Community Mental Health Centers will improve access and unitization of primary care services by historically underserved individuals including the Community Rehabilitation Treatment and Adult Outpatient Populations. This model is currently being piloted by Clara Martin Center and Northwestern Counseling and Support Services. 10
 pay LADCs based on performance.")
12 Department for Children and Families/Economic Services Division Reach Up Substance abuse and mental health conditions are leading barriers to employment for families on Reach Up. To address this issue, three Agency of Human Services departments have partnered to provide services to Reach Up participants with mental health or substance abuse conditions: the Department of Mental Health (DMH), the Department for Children and Families Economic Services Division (ESD) and ADAP. Funding provides systems improvements at Designated Agencies in four areas of the state: Rutland Mental Health, Washington County Mental Health, and HowardCenter (serving both Chittenden and Franklin Counties). The services provided under this contract integrate substance abuse and mental health service planning and coordination, specialized support services, and clinical treatment services to enhance access to care, increase duration of treatment and recovery services, increase family wellness and stability, and contribute to participant s transition to employment. The services being provided include emergency services, individual, family, and group therapy, intensive outpatient treatment, medication management, residential substance abuse treatment, and medication assisted therapy. Integrated Family Services DMH and VDH actively participate in the (AHS) Integrated Family Services (IFS) initiative, which includes representatives from each of the AHS departments that serve children (0-22) and the Agency of Education (AOE). This group is identifying and undertaking changes in policy and internal operations (services, service design, grants, payment structures, etc.) that are needed to improve outcomes and achieve integrated child and family-centered responses from the various AHS and AOE programs. Currently there is one operational IFS pilot in Addison County with Franklin County coming online within the next three months. Rapid Arraignment and Early Referral The Rapid Referral Program is a partnership between Spectrum Youth & Family Services and the Chittenden County District Court to increase access to mental health and substance abuse assessment services for individuals involved in the criminal justice system whose charge(s) are related to substance use. The main objective of the program is to provide judges with a mechanism to rapidly refer defendants for substance abuse screening and treatment rather than delaying services until the case is disposed by the court. An evaluation has documented significant decreases in recidivism for participants completing the program fewer than 20% of participants had subsequent convictions compared to nearly 85% of a control group. Treatment Courts Treatment Courts are available in Rutland, Chittenden and Washington Counties and are a coordinated effort of the judiciary, prosecution, defense bar, probation, law enforcement, mental health and substance abuse treatment to actively intervene and the break the cycle of substance abuse addiction and crime. 11

13 Eligible offenders are offered treatment in exchange for reduced or dismissed charges when they successfully complete the program. Treatment Courts provide an intense regimen of substance abuse and mental health treatment, links to health services, wrap around case management, drug testing, regularly scheduled status hearings before a judge, links with job skills training and employment, educational services, housing and other needed support. Treatment Courts promote positive community trends, increase public safety, reduce recidivism rates, and are a less expensive alternative to prisons. Recidivism rates for treatment court completers are lower than rates for those who do not participate or complete the program. Treatment court graduates who do commit additional crimes have significantly fewer felony convictions than those who do not complete the program. Department of Corrections System Capacity to Address Substance Abuse and Co-Occurring Disorders Many inmates have substance abuse and mental health issues. In 2012, Vermont s Department of Corrections screened 7,779 individuals and transferred an additional 5,245 for external screening, for a total of 13,024 screenings for substance abuse. Of these, 1560 individuals (12%) were subject to detoxification protocols. Some inmates are opioid addicted and others are receiving medication-assisted treatment (MAT) immediately prior to incarceration. To address issues associated with these inmates, ADAP and the Department of Corrections (DOC) convened a workgroup to assess current practices, review research materials, and develop guidelines and procedures. Details of the recommendations are included in legislative response to Act No. 67 (H.523), Sec. 11. This group has developed recommendations for providing care when an inmate is in protective custody as well as how to coordinate care with Hubs and Spokes in the community upon release. They propose a one year demonstration project to validate the recommendations. A recent initiative for the criminal justice population is the offender re-entry program. This supports care coordination between treatment providers, DOC facilities, and probation officers for offenders with moderate to high risk of recidivism. Prior to this initiative, there was no systematic coordination of care between the treatment providers, correctional facilities, and community supervision officers. This funding and technical assistance has increased the frequency of communication to between weekly and monthly depending on the needs of the offender. Early review of data indicates that those with care coordination appear to have decreased recidivism rates. Presently ADAP funds offender re-entry initiatives in Chittenden and Franklin/Grand Isle counties via the HowardCenter; in Washington and Windsor counties via Clara Martin Center; the Northeast Kingdom via Northeast Kingdom Human Services, and Rutland county via Rutland Mental Health. Funds for these services were reallocated from DOC to ADAP in the 2008 Justice Reinvestment Initiative. While not funded by VDH/ADAP, ADAP maintains membership on the State Interagency Team (SIT) for individuals labeled with Severe Functional Impairment (SFI) in the correctional facilities. The role of the SIT is to provide resource knowledge and case conceptualization assistance to local communities supporting individuals labeled SFI, who present complexities that may require supports or consultation not currently available within all geographic regions of the state. Additionally the SIT has reviewed 12

14 funding requests for individual budget requests to assist in triaging those SFI labeled individuals who may be exhibiting the most clinical need or criminogenic risk. Agency of Human Services Recommendations for Addressing Substance Abuse and Co-occurring Disorders - Substance Abuse Treatment Coordination (SATC) Initiative While substance abuse has a significant impact on the health care system, it clearly impacts all areas of the Agency of Human Services (AHS). In order to address this circumstance in a more organized way, the Secretary of the AHS convened a working group of leaders from each Department to develop of a set of actionable policies around the coordination of substance abuse treatment services within the Agency. This initiative is known as Substance Abuse Treatment Coordination (SATC). Participation includes members from AHS central office, DMH, DOC, DAIL, DCF, DVHA, and VDH. SATC reviewed each Department s involvement and funding of substance abuse treatment, and developed the recommendations below. Timelines and implementation tasks associated with these recommendations are being developed. Recommended Policies Screening: AHS will develop a policy for participants in identified AHS direct services and health programs upon program entry and exit and when a client s needs are assessed. Screening will not impact access to AHS services; rather it will allow AHS to better serve clients. Referral: Adopt a standardized mechanism for referring clients whose evidence-based screen indicates a need for further assessment to the appropriate treatment services. Case Management: AHS will adopt a standardized working definition of case management. ADAP will develop Substance Abuse 101 training sessions for staff on the implementation of evidence-based screening tools, including motivational interviewing. This will allow state staff to provide screening and early intervention services to those with risky substance use. Recommended Regional Approach Community Needs Assessment: ADAP will conduct regional/local community needs assessments around substance abuse problems and resources. This process would involve bringing in all those working with substance abuse issues, or with individuals who struggle with substance abuse to discuss the strengths and gaps in each given community setting, including working with schools and criminal justice partners. The Partnership for Success (PFS) grant awarded to VDH by the Substance Abuse and Mental Health Services Administration Center for Substance Abuse Prevention provided a model for substance abuse prevention and strong guidance for a regional approach for services. ADAP plans to use the PFS model to incorporate the full continuum of care, and begin with one initial community to systematically evaluate use of all resources, from prevention through intervention, treatment, and recovery in FY15. 13

15 Through this approach access to evidence based prevention services could be expanded. The AHS regional structure and district offices would serve as centers of local assessment and prevention planning. Recommended Restructured Payment Systems Health Reform Based Funding Method Changes -- Investigate funding methodology changes, in combination with DVHA payment reform efforts associated with Vermont Health Care Innovation Project (VHCIP), to better serve substance abuse and co-occurring patients. For instance, it may be possible to move from the current fee for service funding mechanism to a bundled rate. ADAP has discussed this concept with the Green Mountain Care board and will be making an application for a payment reform pilot project related to the funding of the Hub and Spoke Initiative. It is necessary for health insurers to use similar funding approaches to Medicaid in order to achieve parity for addiction treatment services. Capacity Funding -- Restructure grant funds to eliminate the concept of paying for the uninsured patient. Current Federal Substance Abuse Prevention & Treatment Block Grant funding could be used for capacity, uninsured patients, or additional services. This would incentivize providers to collect insurance from a greater portion of patients to increase overall revenues and flexibility in the use of funding. Recommended Priorities for Supportive Resources Housing: AHS, through the AHS Housing Task Force, is convening an interdepartmental Housing Initiative committee to identify housing options and develop plans for more accessible housing for persons in recovery, particularly those being released from residential treatment or DOC. Workforce Development: Assess workforce needs, and increase training opportunities to make it easier for the existing and entering workforce to obtain and maintain the necessary training and education for licensure. Explore strategies to encourage and incentivize redistribution of Licensed Alcohol and Drug Counselors to underserved areas. Conclusion Many Vermonters face challenges around substance use and mental health and people with cooccurring disorders are likely to intersect with AHS in many areas. As evidenced by the summary of activities and initiatives listed above, AHS is supporting a number of activities to promote the coordination and integration of Vermont s mental health, health, and substance abuse services. 14
, to better serve substance abuse and co-occurring patients.")
16 Over the past two years, the number of projects, initiatives, activities, and planning focused on health/mental health/substance abuse integration has continued to grow, and the number of public and private stakeholders involved in that work has also expanded greatly. These developments represent a significant improvement in the degree to which Vermont is focused on integration, and Vermont may soon reach a point where integration and coordination of health, mental health and substance abuse services is the norm. However, as the number of initiatives, activities and stakeholders increase, there is an increased need for coordination to avoid fragmentation or duplication of efforts. As the Vermont Blueprint for Health continues to expand, DMH and VDH will continue to use this initiative to provide an organizing structure and vision for Vermont s integration and coordination efforts. Going forward, it will be imperative that the executive and legislative branches continue to support the inclusion of mental health and substance abuse integration as a prime feature of health care reform both in Vermont and at a national level. In addition, the focus of improvements in care across all of health care must be based on a patient/consumer-driven philosophy, and the concepts of resiliency and recovery should be cornerstones of all health care efforts. 15

17 Appendix I ADAP Preferred Provider System VDH/ADAP maintains a network of providers who meet the ADAP Treatment Program Approval Standards rds.pdf and are designated as Preferred Providers. Preferred Providers deliver outpatient, intensive outpatient, Medication Assisted Treatment, residential, and halfway services. In addition to direct treatment, ADAP funds emergency services through the public inebriate system, school health services, and programs for special populations, such as the court population. Recovery services, through a network of recovery centers, are also provided through the system of care. Outpatient and intensive outpatient (OP/IOP) services are the most commonly used and lowest level of care in the addictions treatment continuum. It is the most appropriate level of care for the majority of people accessing the system. The OP/IOP service capacity is regional and often limited by workforce shortages. For those requiring more intensive services, there are three residential facilities that serve clients statewide. Methadone has been provided through the Preferred Provider system and the methadone treatment facilities are being enhanced to provide more comprehensive services. Ideally, individuals in each area of the state have access to a full continuum of care such as the one shown below. A list of substance abuse treatment providers by county is located on the ADAP website at 16

18 17
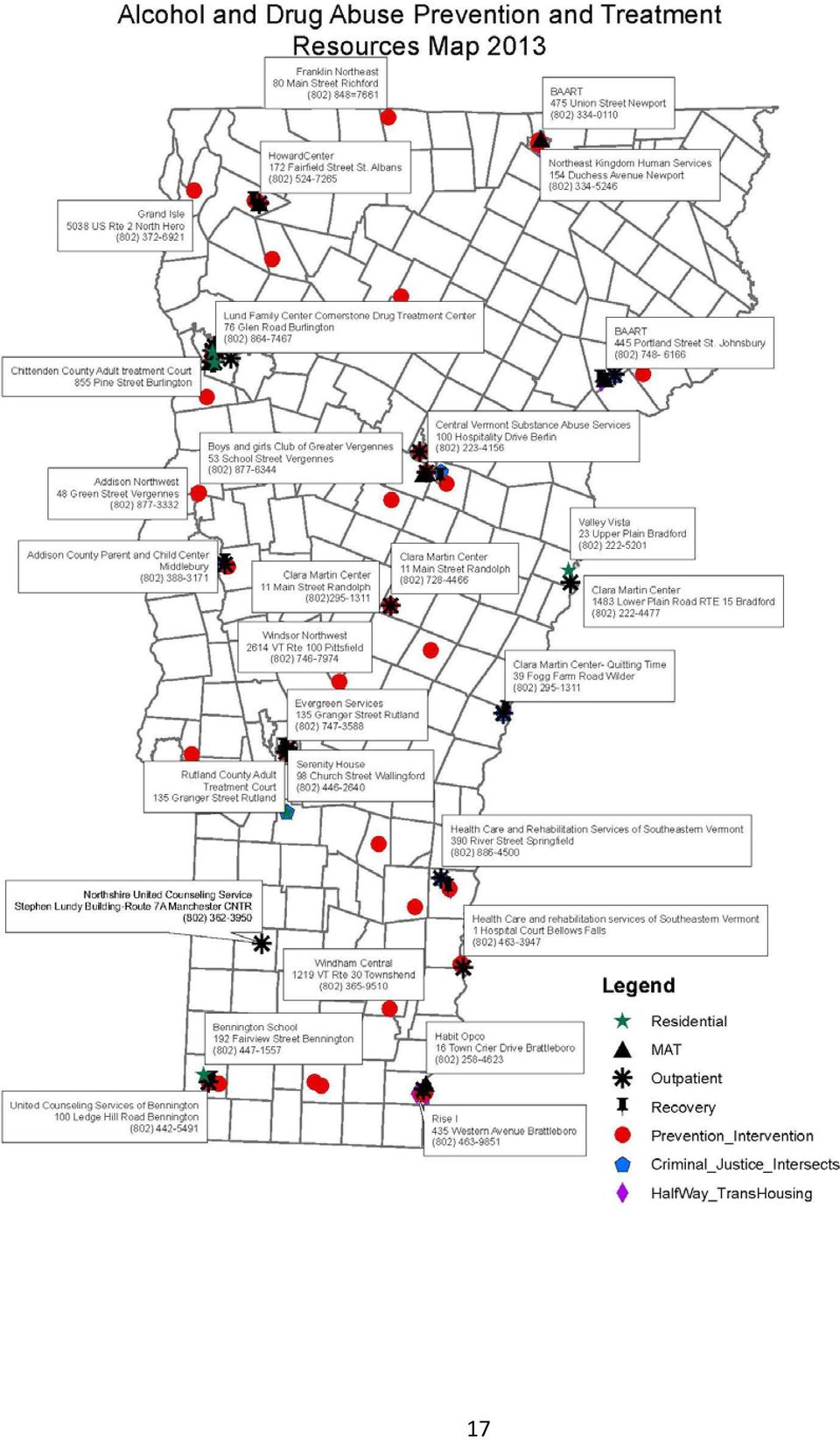
19 Care Alliance for Opioid Treatment Locations 18

Opioid Addiction Treatment Programs
 Report to The Vermont Legislature Opioid Addiction Treatment Programs In Accordance with Act 75, 2013, Section 15a Submitted to: Submitted by: Prepared by: House Committees on Human Services, Health and
Report to The Vermont Legislature Opioid Addiction Treatment Programs In Accordance with Act 75, 2013, Section 15a Submitted to: Submitted by: Prepared by: House Committees on Human Services, Health and
Alcohol and Drug Abuse Program Division Overview
 Alcohol and Drug Abuse Program Division Overview Presented to House Human Services Committee Barbara Cimaglio, Deputy Commissioner, Alcohol and Drug Abuse Programs January 9, 2015 ADAP Organizational Chart
Alcohol and Drug Abuse Program Division Overview Presented to House Human Services Committee Barbara Cimaglio, Deputy Commissioner, Alcohol and Drug Abuse Programs January 9, 2015 ADAP Organizational Chart
Residential Substance Abuse Treatment: Impact of Concurrent Utilization Review
 Report to The Vermont Legislature Residential Substance Abuse Treatment: Impact of Concurrent Utilization Review In Accordance with Act 179 (2014), Section E.300.2, An Act Relating to Making Appropriations
Report to The Vermont Legislature Residential Substance Abuse Treatment: Impact of Concurrent Utilization Review In Accordance with Act 179 (2014), Section E.300.2, An Act Relating to Making Appropriations
Substance Abuse Treatment Services Objective and Performance Measures
 Report to The Vermont Legislature Substance Abuse Treatment Services Objective and Performance Measures In Accordance with Act 179 (2014) Sec. E.306.2 Submitted to: Submitted by: Prepared by: Joint Fiscal
Report to The Vermont Legislature Substance Abuse Treatment Services Objective and Performance Measures In Accordance with Act 179 (2014) Sec. E.306.2 Submitted to: Submitted by: Prepared by: Joint Fiscal
Substance Abuse Treatment Services Objectives and Performance Measures Progress: First Annual Report
 Report to The Vermont Legislature Substance Abuse Treatment Services Objectives and Performance Measures Progress: First Annual Report In Accordance with Act 179 (2014) Sec. E.306.2 (a)(1) Submitted to:
Report to The Vermont Legislature Substance Abuse Treatment Services Objectives and Performance Measures Progress: First Annual Report In Accordance with Act 179 (2014) Sec. E.306.2 (a)(1) Submitted to:
Increasing Access to Opioid Addiction Treatment
 Report to The Vermont Legislature Increasing Access to Opioid Addiction Treatment In Accordance with Act 75, 2013, Section 14b An Act Relating to Strengthening Vermont s Response to Opioid Addiction and
Report to The Vermont Legislature Increasing Access to Opioid Addiction Treatment In Accordance with Act 75, 2013, Section 14b An Act Relating to Strengthening Vermont s Response to Opioid Addiction and
TESTIMONY. March 17, 2014. Rutland, VT
 Community Solutions to Breaking the Cycle of Heroin & Opioid Addiction TESTIMONY Harry Chen, MD, Commissioner of Health March 17, 2014 Senate Committee on the Judiciary Franklin Conference Center at the
Community Solutions to Breaking the Cycle of Heroin & Opioid Addiction TESTIMONY Harry Chen, MD, Commissioner of Health March 17, 2014 Senate Committee on the Judiciary Franklin Conference Center at the
TREATMENT MODALITIES. May, 2013
 TREATMENT MODALITIES May, 2013 Treatment Modalities New York State Office of Alcoholism and Substance Abuse Services (NYS OASAS) regulates the addiction treatment modalities offered in New York State.
TREATMENT MODALITIES May, 2013 Treatment Modalities New York State Office of Alcoholism and Substance Abuse Services (NYS OASAS) regulates the addiction treatment modalities offered in New York State.
The Effectiveness of Vermont s System of Opioid Addiction Treatment
 Report to The Vermont Legislature The Effectiveness of Vermont s System of Opioid Addiction Treatment In Accordance with Act 135 (2012), An Act Relating To the Treatment of Opioid Addiction, Section 1
Report to The Vermont Legislature The Effectiveness of Vermont s System of Opioid Addiction Treatment In Accordance with Act 135 (2012), An Act Relating To the Treatment of Opioid Addiction, Section 1
Addressing Substance Abuse in the Child Welfare Population: Lessons Learned in Vermont
 Agency of Human Services Alcohol and Drug Abuse Programs Blueprint for Health Addressing Substance Abuse in the Child Welfare Population: Lessons Learned in Vermont Tri-Branch Institute on Child Social
Agency of Human Services Alcohol and Drug Abuse Programs Blueprint for Health Addressing Substance Abuse in the Child Welfare Population: Lessons Learned in Vermont Tri-Branch Institute on Child Social
Mental Health & Addiction Forensics Treatment
 Mental Health & Addiction Forensics Treatment Sheriffs: Help needed to cope with September 15, 2014 mentally ill INDIANAPOLIS - A sheriff says county jails have become the "insane asylums" for Indiana
Mental Health & Addiction Forensics Treatment Sheriffs: Help needed to cope with September 15, 2014 mentally ill INDIANAPOLIS - A sheriff says county jails have become the "insane asylums" for Indiana
Many public agencies provide services aimed at preventing, reducing, or
 Publicly-Funded Substance Abuse Services Chapter 3 Developmental Disabilities, and Substance Abuse Services Many public agencies provide services aimed at preventing, reducing, or treating people with
Publicly-Funded Substance Abuse Services Chapter 3 Developmental Disabilities, and Substance Abuse Services Many public agencies provide services aimed at preventing, reducing, or treating people with
American Society of Addiction Medicine
 American Society of Addiction Medicine Public Policy Statement on Treatment for Alcohol and Other Drug Addiction 1 I. General Definitions of Addiction Treatment Addiction Treatment is the use of any planned,
American Society of Addiction Medicine Public Policy Statement on Treatment for Alcohol and Other Drug Addiction 1 I. General Definitions of Addiction Treatment Addiction Treatment is the use of any planned,
Vermont s Experience A Systematic Approach to Health Care Integration Barbara Cimaglio, Deputy Commissioner. NASADAD 2015 Annual Meeting
 Vermont s Experience A Systematic Approach to Health Care Integration Barbara Cimaglio, Deputy Commissioner NASADAD 2015 Annual Meeting Background Goal of Health Care Reform Triple Aim: Better Population
Vermont s Experience A Systematic Approach to Health Care Integration Barbara Cimaglio, Deputy Commissioner NASADAD 2015 Annual Meeting Background Goal of Health Care Reform Triple Aim: Better Population
Redesigning the Publicly-Funded Mental Health System in Texas
 Redesigning the Publicly-Funded Mental Health System in Texas Access to care when services are needed Choice in health plans for consumers and providers Integration of care at the plan and provider level
Redesigning the Publicly-Funded Mental Health System in Texas Access to care when services are needed Choice in health plans for consumers and providers Integration of care at the plan and provider level
Written statement of the American Psychological Association. Hearing before the United States Senate Committee on the Judiciary
 Written statement of the American Psychological Association Hearing before the United States Senate Committee on the Judiciary Breaking the Cycle: Mental Health and the Justice System February 10, 2016
Written statement of the American Psychological Association Hearing before the United States Senate Committee on the Judiciary Breaking the Cycle: Mental Health and the Justice System February 10, 2016
NEW HAMPSHIRE CODE OF ADMINISTRATIVE RULES. PART He-W 513 SUBSTANCE USE DISORDER (SUD) TREATMENT AND RECOVERY SUPPORT SERVICES
 TREATMENT AND RECOVERY SUPPORT SERVICES") CHAPTER He-W 500 MEDICAL ASSISTANCE PART He-W 513 SUBSTANCE USE DISORDER (SUD) TREATMENT AND RECOVERY SUPPORT SERVICES He-W 513.01 Purpose. The purpose of this part is to establish the procedures and requirements
CHAPTER He-W 500 MEDICAL ASSISTANCE PART He-W 513 SUBSTANCE USE DISORDER (SUD) TREATMENT AND RECOVERY SUPPORT SERVICES He-W 513.01 Purpose. The purpose of this part is to establish the procedures and requirements
A Plan to Include Detoxification Services as a Covered Medical Assistance Benefit
 A Plan to Include Detoxification Services as a Covered Medical Assistance Benefit Alcohol and Drug Abuse Division Minnesota Department of Human Services December 2014 For more information contact: Minnesota
A Plan to Include Detoxification Services as a Covered Medical Assistance Benefit Alcohol and Drug Abuse Division Minnesota Department of Human Services December 2014 For more information contact: Minnesota
UTAH DIVISION OF SUBSTANCE ABUSE AND MENTAL HEALTH SUBSTANCE USE DISORDER SERVICES MONITORING CHECKLIST (FY 2014) GENERAL PROGRAM REQUIREMENTS
 GENERAL PROGRAM REQUIREMENTS") UTAH DIVISION OF SUBSTANCE ABUSE AND MENTAL HEALTH SUBSTANCE USE DISORDER SERVICES MONITORING CHECKLIST (FY 2014) Program Name Reviewer Name Date(s) of Review GENERAL PROGRAM REQUIREMENTS 2014 Division
UTAH DIVISION OF SUBSTANCE ABUSE AND MENTAL HEALTH SUBSTANCE USE DISORDER SERVICES MONITORING CHECKLIST (FY 2014) Program Name Reviewer Name Date(s) of Review GENERAL PROGRAM REQUIREMENTS 2014 Division
Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas
 Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas David Lakey, MD Commissioner, Department of State Health Services Lauren Lacefield Lewis Assistant Commissioner,
Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas David Lakey, MD Commissioner, Department of State Health Services Lauren Lacefield Lewis Assistant Commissioner,
Behavioral Health Policy in Illinois: Major Policy Initiatives in 2013 and Beyond
 : Major Policy Initiatives in 2013 and Beyond P R E S E N T A T I O N T O T H E M E D I C A I D A D V I S O R Y C O M M I T T E E N O V E M B E R 7, 2 0 1 3 L O R R I E R I C K M A N J O N E S, P H. D.
: Major Policy Initiatives in 2013 and Beyond P R E S E N T A T I O N T O T H E M E D I C A I D A D V I S O R Y C O M M I T T E E N O V E M B E R 7, 2 0 1 3 L O R R I E R I C K M A N J O N E S, P H. D.
Affordable Care Act: Health Coverage for Criminal Justice Populations. Colorado Center on Law and Policy Colorado Criminal Justice Reform Coalition
 Affordable Care Act: Health Coverage for Criminal Justice Populations Colorado Center on Law and Policy Colorado Criminal Justice Reform Coalition Who we are CCJRC and CCLP have partnered to help Colorado
Affordable Care Act: Health Coverage for Criminal Justice Populations Colorado Center on Law and Policy Colorado Criminal Justice Reform Coalition Who we are CCJRC and CCLP have partnered to help Colorado
SUBSTANCE USE DISORDER (SUD)BENEFIT UNDER MEDICAID EXPANSION
BENEFIT UNDER MEDICAID EXPANSION") A statewide coalition of consumers, providers, educators, and advocates representing the voice for alcohol and drug abuse services SUBSTANCE USE DISORDER (SUD)BENEFIT UNDER MEDICAID EXPANSION The Coalition
A statewide coalition of consumers, providers, educators, and advocates representing the voice for alcohol and drug abuse services SUBSTANCE USE DISORDER (SUD)BENEFIT UNDER MEDICAID EXPANSION The Coalition
How Health Reform Will Help Children with Mental Health Needs
 How Health Reform Will Help Children with Mental Health Needs The new health care reform law, called the Affordable Care Act (or ACA), will give children who have mental health needs better access to the
How Health Reform Will Help Children with Mental Health Needs The new health care reform law, called the Affordable Care Act (or ACA), will give children who have mental health needs better access to the
Best Principles for Integration of Child Psychiatry into the Pediatric Health Home
 Best Principles for Integration of Child Psychiatry into the Pediatric Health Home Approved by AACAP Council June 2012 These guidelines were developed by: Richard Martini, M.D., co-chair, Committee on
Best Principles for Integration of Child Psychiatry into the Pediatric Health Home Approved by AACAP Council June 2012 These guidelines were developed by: Richard Martini, M.D., co-chair, Committee on
Mental Health Fact Sheet
 Mental Health Fact Sheet Substance Abuse and Treatment Branch (SATB), Community Supervision Services Re-Entry and Sanctions Center (RSC), Office of Community Justice Programs Adult Probationers / Parolees
Mental Health Fact Sheet Substance Abuse and Treatment Branch (SATB), Community Supervision Services Re-Entry and Sanctions Center (RSC), Office of Community Justice Programs Adult Probationers / Parolees
Alabama Autism Task Force Preliminary Recommendations
 Alabama Autism Task Force Preliminary Recommendations Having reviewed the findings to date from the Alabama Autism Collaborative Group (AACG), The Alabama Autism Task Force proposes the following changes
Alabama Autism Task Force Preliminary Recommendations Having reviewed the findings to date from the Alabama Autism Collaborative Group (AACG), The Alabama Autism Task Force proposes the following changes
Keep Your Mind and Body Healthy: Understanding Mental Health Providers, Care and Coverage
 Keep Your Mind and Body Healthy: Understanding Mental Health Providers, Care and Coverage Our mental health is a vital part of our overall well-being. It affects how we think, how we feel, and how we act.
Keep Your Mind and Body Healthy: Understanding Mental Health Providers, Care and Coverage Our mental health is a vital part of our overall well-being. It affects how we think, how we feel, and how we act.
Testimony on Addressing Heroin and Opioid Addiction. Theodore Dallas. Secretary, Department of Human Services. Center for Rural Pennsylvania
 Testimony on Addressing Heroin and Opioid Addiction Theodore Dallas Secretary, Department of Human Services Center for Rural Pennsylvania July 29, 2015 1 P a g e Introduction Good morning Senator Yaw,
Testimony on Addressing Heroin and Opioid Addiction Theodore Dallas Secretary, Department of Human Services Center for Rural Pennsylvania July 29, 2015 1 P a g e Introduction Good morning Senator Yaw,
American Society of Addiction Medicine
 American Society Medicine Public Policy Statement on Parity in Publicly Funded Health Insurance Benefits for Treatment 1 Background The American Society Medicine has well-established policy affirming that
American Society Medicine Public Policy Statement on Parity in Publicly Funded Health Insurance Benefits for Treatment 1 Background The American Society Medicine has well-established policy affirming that
Structure and Function
 Structure and Function OKLAHOMA State SSA Director Mr. Ben Brown, Deputy Commissioner Oklahoma Department of Mental Health and Substance Abuse Services P.O. Box 53277 Oklahoma City, OK 73152-3277 Phone:
Structure and Function OKLAHOMA State SSA Director Mr. Ben Brown, Deputy Commissioner Oklahoma Department of Mental Health and Substance Abuse Services P.O. Box 53277 Oklahoma City, OK 73152-3277 Phone:
2015 OPIOID TREATMENT PROGRAM DESCRIPTIONS
 2015 OPIOID TREATMENT PROGRAM PROGRAM DESCRIPTIONS Contents Opioid T reatment Program Core Program Standards... 2 Court Treatment (CT)... 2 Detoxification... 2 Day Treatment... 3 Health Home (HH)... 3
2015 OPIOID TREATMENT PROGRAM PROGRAM DESCRIPTIONS Contents Opioid T reatment Program Core Program Standards... 2 Court Treatment (CT)... 2 Detoxification... 2 Day Treatment... 3 Health Home (HH)... 3
Summary: There are four major initiatives underway that address integration of substance abuse care with physical and mental health.
 Summary: Section E.306.2(b)(1) requires the Secretary of Administration and the Chief of Health Care Reform to submit a report on current and additional strategies to achieve a more comprehensive health
Summary: Section E.306.2(b)(1) requires the Secretary of Administration and the Chief of Health Care Reform to submit a report on current and additional strategies to achieve a more comprehensive health
Appendix D. Behavioral Health Partnership. Adolescent/Adult Substance Abuse Guidelines
 Appendix D Behavioral Health Partnership Adolescent/Adult Substance Abuse Guidelines Handbook for Providers 92 ASAM CRITERIA The CT BHP utilizes the ASAM PPC-2R criteria for rendering decisions regarding
Appendix D Behavioral Health Partnership Adolescent/Adult Substance Abuse Guidelines Handbook for Providers 92 ASAM CRITERIA The CT BHP utilizes the ASAM PPC-2R criteria for rendering decisions regarding
Behavioral Health Management of Substance Use Disorder Services
 Behavioral Health Management of Substance Use Disorder Services Arlene González-Sánchez, Commissioner Robert Kent, General Counsel SAMSHA: New York State should remain consistent with SAMSHA policy philosophy
Behavioral Health Management of Substance Use Disorder Services Arlene González-Sánchez, Commissioner Robert Kent, General Counsel SAMSHA: New York State should remain consistent with SAMSHA policy philosophy
P a g e 1. Ken Cuccinelli Mental Health Forum Responses
 P a g e 1 Ken Cuccinelli Mental Health Forum Responses 1) Virginians of all ages and situations in life can experience mental health problems. Almost a quarter million adults in Virginia live with co-occurring
P a g e 1 Ken Cuccinelli Mental Health Forum Responses 1) Virginians of all ages and situations in life can experience mental health problems. Almost a quarter million adults in Virginia live with co-occurring
CRIMINAL JUSTICE ADVISORY COUNCIL ALTERNATIVES TO INCARCERATION REPORT September 8, 2005
 CRIMINAL JUSTICE ADVISORY COUNCIL ALTERNATIVES TO INCARCERATION REPORT September 8, 2005 The Criminal Justice Advisory Council ( CJAC ) established a Subcommittee to address recommendations regarding alternatives
CRIMINAL JUSTICE ADVISORY COUNCIL ALTERNATIVES TO INCARCERATION REPORT September 8, 2005 The Criminal Justice Advisory Council ( CJAC ) established a Subcommittee to address recommendations regarding alternatives
The Opiod Addiction Treatment System
 Report to The Vermont Legislature The Opiod Addiction Treatment System In Accordance with Act 135 (2012, Adj.), Section 1(c) An Act Relating to an Opiod Addiction Treatment System Submitted to: Submitted
Report to The Vermont Legislature The Opiod Addiction Treatment System In Accordance with Act 135 (2012, Adj.), Section 1(c) An Act Relating to an Opiod Addiction Treatment System Submitted to: Submitted
(1) Sex offenders who have been convicted of: * * * an attempt to commit any offense listed in this subdivision. (a)(1). * * *
 Sex offenders who have been convicted of: * * * an attempt to commit any offense listed in this subdivision. (a)(1). * * *") House Proposal of Amendment S. 292 An act relating to term probation, the right to bail, medical care of inmates, and a reduction in the number of nonviolent prisoners, probationers, and detainees. The
House Proposal of Amendment S. 292 An act relating to term probation, the right to bail, medical care of inmates, and a reduction in the number of nonviolent prisoners, probationers, and detainees. The
Performance Standards
 Performance Standards Co-Occurring Disorder Competency Performance Standards are intended to provide a foundation and serve as a tool to promote continuous quality improvement and progression toward best
Performance Standards Co-Occurring Disorder Competency Performance Standards are intended to provide a foundation and serve as a tool to promote continuous quality improvement and progression toward best
VI. Substance Use Disorder Services
 VI. Substance Use Disorder Services Background In Pennsylvania, administration of services for persons with substance use disorders (SUD) is shared by the Bureau of Drug and Alcohol Programs (BDAP) in
VI. Substance Use Disorder Services Background In Pennsylvania, administration of services for persons with substance use disorders (SUD) is shared by the Bureau of Drug and Alcohol Programs (BDAP) in
MENTAL HEALTH AND SUBSTANCE ABUSE
 MENTAL HEALTH AND SUBSTANCE ABUSE Perhaps no state government function has experienced such a profound change in its mission over the past 40 years than the mental health system. As late as the 1960s,
MENTAL HEALTH AND SUBSTANCE ABUSE Perhaps no state government function has experienced such a profound change in its mission over the past 40 years than the mental health system. As late as the 1960s,
Contents Opioid Treatment Program Core Program Standards... 2
 2016 OPIOID TREATMENT PROGRAM PROGRAM DESCRIPTIONS Contents Opioid Treatment Program Core Program Standards... 2 Court Treatment (CT)... 2 Detoxification... 2 Day Treatment... 3 Health Home (HH)... 3 Integrated
2016 OPIOID TREATMENT PROGRAM PROGRAM DESCRIPTIONS Contents Opioid Treatment Program Core Program Standards... 2 Court Treatment (CT)... 2 Detoxification... 2 Day Treatment... 3 Health Home (HH)... 3 Integrated
How To Fund A Mental Health Court
 Mental Health Courts: A New Tool By Stephanie Yu, Fiscal Analyst For fiscal year (FY) 2008-09, appropriations for the Judiciary and the Department of Community Health (DCH) include funding for a mental
Mental Health Courts: A New Tool By Stephanie Yu, Fiscal Analyst For fiscal year (FY) 2008-09, appropriations for the Judiciary and the Department of Community Health (DCH) include funding for a mental
Outpatient and Intensive Outpatient Narrative
 Los Angeles County Department of Public Health Substance Abuse Prevention and Control (SAPC) will implement an initial benefit package of Substance Use Disorder (SUD) services within the initial twelve
Los Angeles County Department of Public Health Substance Abuse Prevention and Control (SAPC) will implement an initial benefit package of Substance Use Disorder (SUD) services within the initial twelve
Behavioral Health Provider Implementation of Whole Health Integrative Treatment Services
 Behavioral Health Provider Implementation of Whole Health Integrative Treatment Services Maryland Integrative Learning Community Lynn H Albizo, Director of Public Affairs Maryland Addictions Directors
Behavioral Health Provider Implementation of Whole Health Integrative Treatment Services Maryland Integrative Learning Community Lynn H Albizo, Director of Public Affairs Maryland Addictions Directors
SENATE BILL No. 614 AMENDED IN ASSEMBLY JULY 16, 2015 AMENDED IN ASSEMBLY JULY 6, 2015 AMENDED IN SENATE APRIL 6, 2015
 AMENDED IN ASSEMBLY JULY 16, 2015 AMENDED IN ASSEMBLY JULY 6, 2015 AMENDED IN SENATE APRIL 6, 2015 SENATE BILL No. 614 Introduced by Senator Leno (Coauthor: Senator Anderson) February 27, 2015 An act to
AMENDED IN ASSEMBLY JULY 16, 2015 AMENDED IN ASSEMBLY JULY 6, 2015 AMENDED IN SENATE APRIL 6, 2015 SENATE BILL No. 614 Introduced by Senator Leno (Coauthor: Senator Anderson) February 27, 2015 An act to
Florida s Approach to Mental Illnesses and Substance Abuse: Penny-Wise and Pound-Foolish? A White Paper Proposal. Prepared by
 Florida s Approach to Mental Illnesses and Substance Abuse: Penny-Wise and Pound-Foolish? A White Paper Proposal Prepared by The Key Clubhouse of South Florida 260 NE 17 th Terrace, Suite 202 Miami, FL
Florida s Approach to Mental Illnesses and Substance Abuse: Penny-Wise and Pound-Foolish? A White Paper Proposal Prepared by The Key Clubhouse of South Florida 260 NE 17 th Terrace, Suite 202 Miami, FL
Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio
 Governor s Cabinet Opiate Action Team Promoting Wellness and Recovery John R. Kasich, Governor Tracy J. Plouck, Director Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio November 14,
Governor s Cabinet Opiate Action Team Promoting Wellness and Recovery John R. Kasich, Governor Tracy J. Plouck, Director Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio November 14,
CHAPTER 1223. OUTPATIENT DRUG AND ALCOHOL CLINIC SERVICES
 CHAPTER 1223. OUTPATIENT DRUG AND ALCOHOL CLINIC SERVICES GENERAL PROVISIONS Sec. 1223.1. Policy. 1223.2. Definitions. 1223.11. Types of services covered. 1223.12. Outpatient services. 1223.13. Inpatient
CHAPTER 1223. OUTPATIENT DRUG AND ALCOHOL CLINIC SERVICES GENERAL PROVISIONS Sec. 1223.1. Policy. 1223.2. Definitions. 1223.11. Types of services covered. 1223.12. Outpatient services. 1223.13. Inpatient
Title: Opening Plenary Session Challenges and Opportunities to Impact the Opioid Dependence Crisis
 The American Association for the Treatment of Opioid Dependence, provider #1044, is approved as a provider for social work continuing education by the Association of Social Work Boards (ASWB) www.aswb.org,
The American Association for the Treatment of Opioid Dependence, provider #1044, is approved as a provider for social work continuing education by the Association of Social Work Boards (ASWB) www.aswb.org,
John R. Kasich, Governor Orman Hall, Director
 John R. Kasich, Governor Orman Hall, Director 2 3 Epidemics of unintentional drug overdoses in Ohio, 1979-2011 1,2,3 1800 1600 1400 1200 1000 800 Prescription drugs are causing a larger overdose epidemic
John R. Kasich, Governor Orman Hall, Director 2 3 Epidemics of unintentional drug overdoses in Ohio, 1979-2011 1,2,3 1800 1600 1400 1200 1000 800 Prescription drugs are causing a larger overdose epidemic
Report on the Repurposing of the Woodside Juvenile Rehabilitation Center
 Report to The Vermont Legislature Report on the Repurposing of the Woodside Juvenile Rehabilitation Center In Accordance with Act 146 Sec. C 10: Woodside Juvenile Rehabilitation Center Submitted to: Submitted
Report to The Vermont Legislature Report on the Repurposing of the Woodside Juvenile Rehabilitation Center In Accordance with Act 146 Sec. C 10: Woodside Juvenile Rehabilitation Center Submitted to: Submitted
Mental Health Needs of Juvenile Offenders. Mental Health Needs of Juvenile Offenders. Juvenile Justice Guide Book for Legislators
 Mental Health Needs of Juvenile Offenders Mental Health Needs of Juvenile Offenders Juvenile Justice Guide Book for Legislators Mental Health Needs of Juvenile Offenders Introduction Children with mental
Mental Health Needs of Juvenile Offenders Mental Health Needs of Juvenile Offenders Juvenile Justice Guide Book for Legislators Mental Health Needs of Juvenile Offenders Introduction Children with mental
Status of Legislation Impacting Community Mental Health in the 2015 Indiana General Assembly
 Status of Legislation Impacting Community Mental Health in the 2015 Indiana General Assembly Matt Brooks, CEO Indiana Council of Community Mental Health Centers 2015 Webinar Series March 9 th, 2015 Current
Status of Legislation Impacting Community Mental Health in the 2015 Indiana General Assembly Matt Brooks, CEO Indiana Council of Community Mental Health Centers 2015 Webinar Series March 9 th, 2015 Current
Department of Health Services. Alcohol and Other Drug Services Division
 Department of Health Services Alcohol and Other Drug Services Division Summary of Programs and Services Rita Scardaci, MPH, Health Services Director Gino Giannavola, AODS Division Director Alcohol and
Department of Health Services Alcohol and Other Drug Services Division Summary of Programs and Services Rita Scardaci, MPH, Health Services Director Gino Giannavola, AODS Division Director Alcohol and
Mental Health. Health Equity Highlight: Women
 Mental Health Background A person s ability to carry on productive activities and live a rewarding life is affected not only by physical health but by mental health. In addition, mental well-being can
Mental Health Background A person s ability to carry on productive activities and live a rewarding life is affected not only by physical health but by mental health. In addition, mental well-being can
H.R 2646 Summary and S. 1945 Comparison
 H.R 2646 Summary and S. 1945 Comparison TITLE I ASSISTANT SECRETARY FOR MENTAL HEALTH AND SUBSTANCE USE DISORDERS It establishes an Office of the Assistant Secretary for Mental Health and Substance Use
H.R 2646 Summary and S. 1945 Comparison TITLE I ASSISTANT SECRETARY FOR MENTAL HEALTH AND SUBSTANCE USE DISORDERS It establishes an Office of the Assistant Secretary for Mental Health and Substance Use
COMPARISON OF KEY PROVISIONS House and Senate Comprehensive Mental Health Reform Legislation
 COMPARISON OF KEY PROVISIONS House and Senate Comprehensive Mental Health Reform Legislation Note: A full title-by-title summary of H.R. 2646, the Helping Families in Mental Health Crisis Act of 2015 (Murphy/Johnson)
COMPARISON OF KEY PROVISIONS House and Senate Comprehensive Mental Health Reform Legislation Note: A full title-by-title summary of H.R. 2646, the Helping Families in Mental Health Crisis Act of 2015 (Murphy/Johnson)
IN THE GENERAL ASSEMBLY STATE OF. Ensuring Access to Medication Assisted Treatment Act
 IN THE GENERAL ASSEMBLY STATE OF Ensuring Access to Medication Assisted Treatment Act 1 Be it enacted by the People of the State of Assembly:, represented in the General 1 1 1 1 Section 1. Title. This
IN THE GENERAL ASSEMBLY STATE OF Ensuring Access to Medication Assisted Treatment Act 1 Be it enacted by the People of the State of Assembly:, represented in the General 1 1 1 1 Section 1. Title. This
How To Know If You Can Get Help For An Addiction
 2014 FLORIDA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA Overview Psychcare strives to provide quality care in the least restrictive environment. An
2014 FLORIDA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA SUBSTANCE ABUSE LEVEL OF CARE CLINICAL CRITERIA Overview Psychcare strives to provide quality care in the least restrictive environment. An
OUTPATIENT SUBSTANCE USE DISORDER SERVICES FEE-FOR-SERVICE
 OUTPATIENT SUBSTANCE USE DISORDER SERVICES FEE-FOR-SERVICE Brief Coverage Statement Outpatient Substance Use Disorder (SUD) Fee-For-Service (FFS) Treatment Services are available for the treatment of substance
OUTPATIENT SUBSTANCE USE DISORDER SERVICES FEE-FOR-SERVICE Brief Coverage Statement Outpatient Substance Use Disorder (SUD) Fee-For-Service (FFS) Treatment Services are available for the treatment of substance
RECOVERY HOUSING POLICY BRIEF
 I. Introduction and Intent As communities implement strategies to end homelessness, they need to be able to provide effective housing and services options for people experiencing homelessness who have
I. Introduction and Intent As communities implement strategies to end homelessness, they need to be able to provide effective housing and services options for people experiencing homelessness who have
Department of Mental Health and Addiction Services 17a-453a-1 2
 17a-453a-1 2 DEPARTMENT OF MENTAL HEALTH AND ADDICTION SERVICES General Assistance Behavioral Health Program The Regulations of Connecticut State Agencies are amended by adding sections 17a-453a-1 to 17a-453a-19,
17a-453a-1 2 DEPARTMENT OF MENTAL HEALTH AND ADDICTION SERVICES General Assistance Behavioral Health Program The Regulations of Connecticut State Agencies are amended by adding sections 17a-453a-1 to 17a-453a-19,
PSYCHIATRY IN HEALTHCARE REFORM SUMMARY REPORT A REPORT BY AMERICAN PSYCHIATRIC ASSOCIATION BOARD OF TRUSTEES WORK GROUP ON THE ROLE OF
 ROLE OF PSYCHIATRY IN HEALTHCARE REFORM SUMMARY REPORT A REPORT BY AMERICAN PSYCHIATRIC ASSOCIATION BOARD OF TRUSTEES WORK GROUP ON THE ROLE OF PSYCHIATRY IN HEALTHCARE REFORM 2014 Role of Psychiatry in
ROLE OF PSYCHIATRY IN HEALTHCARE REFORM SUMMARY REPORT A REPORT BY AMERICAN PSYCHIATRIC ASSOCIATION BOARD OF TRUSTEES WORK GROUP ON THE ROLE OF PSYCHIATRY IN HEALTHCARE REFORM 2014 Role of Psychiatry in
Chapter 18 Behavioral Health Services
 18 Behavioral Health Services INTRODUCTION The State of Arizona has contracted the administration of the AHCCCS mental health and substance abuse services program to the Arizona Department of Health Services
18 Behavioral Health Services INTRODUCTION The State of Arizona has contracted the administration of the AHCCCS mental health and substance abuse services program to the Arizona Department of Health Services
Maryland Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland As of July 2003, 638,662 people were covered under Maryland's Medicaid/SCHIP programs. There were 525,080 enrolled in the Medicaid
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland As of July 2003, 638,662 people were covered under Maryland's Medicaid/SCHIP programs. There were 525,080 enrolled in the Medicaid
How To Get A Mental Health Care Plan In Vermont
 Agency of Human Services STANDARD OPERATING PROCEDURES MANUAL FOR VERMONT MEDICAID INPATIENT PSYCHIATRIC AND DETOXIFICATION AUTHORIZATIONS Department of Vermont Health Access Department of Mental Health
Agency of Human Services STANDARD OPERATING PROCEDURES MANUAL FOR VERMONT MEDICAID INPATIENT PSYCHIATRIC AND DETOXIFICATION AUTHORIZATIONS Department of Vermont Health Access Department of Mental Health
Strategic Plan for Vermont Health Reform
 Strategic Plan for Vermont Health Reform 2012 2014 Released January, 2012; Revised July 2012 by Robin J. Lunge, J.D., Director of Health Care Reform, Agency of Administration, State of Vermont Developed
Strategic Plan for Vermont Health Reform 2012 2014 Released January, 2012; Revised July 2012 by Robin J. Lunge, J.D., Director of Health Care Reform, Agency of Administration, State of Vermont Developed
NARRATIVE INFORMATION DA
 DIVISION OVERVIEW Disability and Behavioral Health Services MISSION: Disability and Behavioral Health Services (DBHS) vision for the persons it supports and serves is to ensure they live healthy, successful,
DIVISION OVERVIEW Disability and Behavioral Health Services MISSION: Disability and Behavioral Health Services (DBHS) vision for the persons it supports and serves is to ensure they live healthy, successful,
Chapter 4 STRATEGIC GOALS AND OBJECTIVES
 Chapter 4 STRATEGIC GOALS AND OBJECTIVES PRINCIPLES OF A COMPREHENSIVE, BALANCED STRATEGY This urban-based Substance Abuse Strategy (the Strategy) is built on the premise that no single approach can end
Chapter 4 STRATEGIC GOALS AND OBJECTIVES PRINCIPLES OF A COMPREHENSIVE, BALANCED STRATEGY This urban-based Substance Abuse Strategy (the Strategy) is built on the premise that no single approach can end
LOCAL NEEDS LOCAL DECISI NS LOCAL BOARDS
 ALCOHOL, DRUG ADDICTION, AND MENTAL HEALTH BOARDS OF OHIO The Value of Ohio s Alcohol, Drug Addiction, and Mental Health Boards Providing hope and helping local communities thrive ++--------- LOCAL NEEDS
ALCOHOL, DRUG ADDICTION, AND MENTAL HEALTH BOARDS OF OHIO The Value of Ohio s Alcohol, Drug Addiction, and Mental Health Boards Providing hope and helping local communities thrive ++--------- LOCAL NEEDS
Overview of Federal Health Care Reform and NYS Medicaid Redesign
 Overview of Federal Health Care Reform and NYS Medicaid Redesign Issues and opportunities for Criminal Justice organizations and their clients Paul N. Samuels, Director and President, Legal Action Center
Overview of Federal Health Care Reform and NYS Medicaid Redesign Issues and opportunities for Criminal Justice organizations and their clients Paul N. Samuels, Director and President, Legal Action Center
Oklahoma Department of Mental Health & Substance Abuse Services Oklahoma Department of Rehabilitation Services Oklahoma Health Care Authority
 Oklahoma Department of Mental Health & Substance Abuse Services Oklahoma Department of Rehabilitation Services Oklahoma Health Care Authority Improving the System of Care for Individuals with Mental Health
Oklahoma Department of Mental Health & Substance Abuse Services Oklahoma Department of Rehabilitation Services Oklahoma Health Care Authority Improving the System of Care for Individuals with Mental Health
Smoky Mountain Center LME-MCO Care Coordination
 Smoky Mountain Center LME-MCO Care Coordination Care Coordination activities include the identification, coordination and monitoring of, linkage to behavioral health treatment services and/or habilitative
Smoky Mountain Center LME-MCO Care Coordination Care Coordination activities include the identification, coordination and monitoring of, linkage to behavioral health treatment services and/or habilitative
Fairfax-Falls Church Community Services Board
 LOB #267: ADULT RESIDENTIAL TREATMENT SERVICES Purpose Adult Residential Treatment Services provides residential treatment programs for adults with severe substance use disorders and/or co occurring mental
LOB #267: ADULT RESIDENTIAL TREATMENT SERVICES Purpose Adult Residential Treatment Services provides residential treatment programs for adults with severe substance use disorders and/or co occurring mental
QUEEN ANNE S COUNTY STRATEGIC PLAN ALCOHOL AND DRUG ABUSE SERVICES
 QUEEN ANNE S COUNTY STRATEGIC PLAN ALCOHOL AND DRUG ABUSE SERVICES 2016 2018 INTRODUCTION Local councils are established under Chapters 237 and 238 of the Acts of the General Assembly of Maryland of 2004,
QUEEN ANNE S COUNTY STRATEGIC PLAN ALCOHOL AND DRUG ABUSE SERVICES 2016 2018 INTRODUCTION Local councils are established under Chapters 237 and 238 of the Acts of the General Assembly of Maryland of 2004,
1) What would it take to get four or five FQHCs to implement ECHO, and how many patients can we serve?
 What would it take to get four or five FQHCs to implement ECHO, and how many patients can we serve?") RI Mental Health Summit Lightning Round Q&A s June 8, 2015 Opiate Addiction Epidemic 1) What would it take to get four or five FQHCs to implement ECHO, and how many patients can we serve? 2) What would
RI Mental Health Summit Lightning Round Q&A s June 8, 2015 Opiate Addiction Epidemic 1) What would it take to get four or five FQHCs to implement ECHO, and how many patients can we serve? 2) What would
Vermont s Approach Treating the Opiate Epidemic Barbara Cimaglio Deputy Commissioner, Vermont Department of Health
 Vermont s Approach Treating the Opiate Epidemic Barbara Cimaglio Deputy Commissioner, Vermont Department of Health State Experiences with Health Care Reform Grand America Hotel Salt Lake City, Utah October
Vermont s Approach Treating the Opiate Epidemic Barbara Cimaglio Deputy Commissioner, Vermont Department of Health State Experiences with Health Care Reform Grand America Hotel Salt Lake City, Utah October
Illinois Mental Health and Substance Abuse Services in Crisis
 May 2011 Illinois Mental Health and Substance Abuse Services in Crisis Each year, hospitals in Illinois are encountering a steadily increasing number of persons with mental and substance use illnesses
May 2011 Illinois Mental Health and Substance Abuse Services in Crisis Each year, hospitals in Illinois are encountering a steadily increasing number of persons with mental and substance use illnesses
LEVEL III.5 SA: SHORT TERM RESIDENTIAL - Adult (DUAL DIAGNOSIS CAPABLE)
") LEVEL III.5 SA: SHT TERM RESIDENTIAL - Adult (DUAL DIAGNOSIS CAPABLE) Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders
LEVEL III.5 SA: SHT TERM RESIDENTIAL - Adult (DUAL DIAGNOSIS CAPABLE) Definition The following is based on the Adult Criteria of the Patient Placement Criteria for the Treatment of Substance-Related Disorders
Optum By United Behavioral Health. 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines
 Level of Care Guidelines") Optum By United Behavioral Health 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines Statewide Inpatient Psychiatric Program Services (SIPP) Statewide Inpatient Psychiatric
Optum By United Behavioral Health 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines Statewide Inpatient Psychiatric Program Services (SIPP) Statewide Inpatient Psychiatric
Mental Illness, Addiction and the Whatcom County Jail
 March 1, 015 Mental Illness, Addiction and the Whatcom County Jail Bill Elfo, Sheriff Whatcom County America is experiencing a disturbing and increasing trend in the number of offenders housed in its county
March 1, 015 Mental Illness, Addiction and the Whatcom County Jail Bill Elfo, Sheriff Whatcom County America is experiencing a disturbing and increasing trend in the number of offenders housed in its county
1. Increase Access to Effective Mental Health Care. 3. Maximize Federal Financial Support for Mental Health Care
 NAMI Illinois Action Agenda 2015 NAMI Illinois is the state organization affiliated with the National Alliance on Mental Illness, the nation s largest grassroots organization for people with mental illness
NAMI Illinois Action Agenda 2015 NAMI Illinois is the state organization affiliated with the National Alliance on Mental Illness, the nation s largest grassroots organization for people with mental illness
OAHP Key Adolescent Health Issue. Behavioral Health. (Mental Health & Substance Abuse)
") OAHP Key Adolescent Health Issue Area 1 Behavioral Health (Mental Health & Substance Abuse) Introduction In Ohio, the promotion of positive mental health and the prevention of substance abuse and mental
OAHP Key Adolescent Health Issue Area 1 Behavioral Health (Mental Health & Substance Abuse) Introduction In Ohio, the promotion of positive mental health and the prevention of substance abuse and mental
Evidence Based Approaches to Addiction and Mental Illness Treatment for Adults
 Evidence Based Practice Continuum Guidelines The Division of Behavioral Health strongly encourages behavioral health providers in Alaska to implement evidence based practices and effective program models.
Evidence Based Practice Continuum Guidelines The Division of Behavioral Health strongly encourages behavioral health providers in Alaska to implement evidence based practices and effective program models.
Massachusetts Council on Compulsive Gambling
 Massachusetts Council on Compulsive Gambling We understand the problem. We can help. Gambling Problems and Corrections Solutions for the Future Scott Melissa, Massachusetts Council on Compulsive Gambling
Massachusetts Council on Compulsive Gambling We understand the problem. We can help. Gambling Problems and Corrections Solutions for the Future Scott Melissa, Massachusetts Council on Compulsive Gambling
Illinois Insurance Facts Illinois Department of Insurance Mental Health and Substance Use Disorder Coverage
 Illinois Insurance Facts Illinois Department of Insurance Mental Health and Substance Use Disorder Coverage Revised October 2012 Note: This information was developed to provide consumers with general information
Illinois Insurance Facts Illinois Department of Insurance Mental Health and Substance Use Disorder Coverage Revised October 2012 Note: This information was developed to provide consumers with general information
External Advisory Group Meeting June 2, 2015
 External Advisory Group Meeting June 2, 2015 1. There seems to be an extended wait from disposition to sentence where defendants are in jail awaiting the completion of the pre-sentence report. How many
External Advisory Group Meeting June 2, 2015 1. There seems to be an extended wait from disposition to sentence where defendants are in jail awaiting the completion of the pre-sentence report. How many
Quality Management. Substance Abuse Outpatient Care Services Service Delivery Model. Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA)
") Quality Management Substance Abuse Outpatient Care Services Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal Ryan White
Quality Management Substance Abuse Outpatient Care Services Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal Ryan White
Alcoholism and Substance Abuse
 State of Illinois Department of Human Services Division of Alcoholism and Substance Abuse OVERVIEW The Illinois Department of Human Services, Division of Alcoholism and Substance Abuse (IDHS/DASA) is the
State of Illinois Department of Human Services Division of Alcoholism and Substance Abuse OVERVIEW The Illinois Department of Human Services, Division of Alcoholism and Substance Abuse (IDHS/DASA) is the
July 15, 2015. Dear April Leonhard:
 July 15, 2015 April Leonhard Department of Human Services Office of Long Term Living, Bureau of Policy and Regulatory Management P.O. Box 8025 Harrisburg, PA 17105-8025 Dear April Leonhard: Thank you for
July 15, 2015 April Leonhard Department of Human Services Office of Long Term Living, Bureau of Policy and Regulatory Management P.O. Box 8025 Harrisburg, PA 17105-8025 Dear April Leonhard: Thank you for
LOI Cover Page. Organization Name: Willamette Family, Inc. Mailing Address: 687 Cheshire Avenue. City/State: Eugene, OR Zip: 97402
 26 Attachment - Willamette Family A LOI Cover Page Contact Information Organization Name: Willamette Family, Inc. Mailing Address: 687 Cheshire Avenue City/State: Eugene, OR Zip: 97402 Contact Name: Susie
26 Attachment - Willamette Family A LOI Cover Page Contact Information Organization Name: Willamette Family, Inc. Mailing Address: 687 Cheshire Avenue City/State: Eugene, OR Zip: 97402 Contact Name: Susie
Children, youth and families with co-occurring mental health and substance abuse issues are welcomed in every contact, and in every setting.
 Practice Guidelines for the Identification and Treatment of Co-occurring Mental Health and Substance Abuse Issues In Children, Youth and Families June, 2008 This document is adapted from The Vermont Practice
Practice Guidelines for the Identification and Treatment of Co-occurring Mental Health and Substance Abuse Issues In Children, Youth and Families June, 2008 This document is adapted from The Vermont Practice
Agency of Human Services
 Agency of Human Services Practice Guidelines for the Identification and Treatment of Co-occurring Mental Health and Substance Abuse Issues In Children, Youth and Families The Vermont Practice Guidelines
Agency of Human Services Practice Guidelines for the Identification and Treatment of Co-occurring Mental Health and Substance Abuse Issues In Children, Youth and Families The Vermont Practice Guidelines
DIVISION OF BEHAVIORAL HEALTH SERVICES SUBSTANCE ABUSE TREATMENT SERVICES PLAN
 DIVISION OF BEHAVIORAL HEALTH SERVICES SUBSTANCE ABUSE TREATMENT SERVICES PLAN NOVEMBER 2009 SUBSTANCE ABUSE TREATMENT SERVICES PLAN November 2009 Salt Lake County Department of Human Services Division
DIVISION OF BEHAVIORAL HEALTH SERVICES SUBSTANCE ABUSE TREATMENT SERVICES PLAN NOVEMBER 2009 SUBSTANCE ABUSE TREATMENT SERVICES PLAN November 2009 Salt Lake County Department of Human Services Division
Adult Mental Health Court Certification Application
 As required by O.C.G.A. 15-1-16, to receive state appropriated funds adult mental health courts must be certified by the Judicial Council of Georgia (Council). The certification process is part of an effort
As required by O.C.G.A. 15-1-16, to receive state appropriated funds adult mental health courts must be certified by the Judicial Council of Georgia (Council). The certification process is part of an effort
Alcohol and Drug Abuse Treatment Centers
 Division of State Operated Healthcare Facilities Alcohol and Drug Abuse Treatment Centers Jenny Wood Interim ADATC Team Leader HHS LOC Mental Health Subcommittee February 24, 2014 ADATC Locations R.J.
Division of State Operated Healthcare Facilities Alcohol and Drug Abuse Treatment Centers Jenny Wood Interim ADATC Team Leader HHS LOC Mental Health Subcommittee February 24, 2014 ADATC Locations R.J.
TN No: 09-024 Supersedes Approval Date:01-27-10 Effective Date: 10/01/09 TN No: 08-011
 Page 15a.2 (iii) Community Support - (adults) (CS) North Carolina is revising the State Plan to facilitate phase out of the Community Support - Adults service, which will end effective July 1, 2010. Beginning
Page 15a.2 (iii) Community Support - (adults) (CS) North Carolina is revising the State Plan to facilitate phase out of the Community Support - Adults service, which will end effective July 1, 2010. Beginning
ADDRESSING COLORADO S SUBSTANCE USE DISORDER MEDICAID BENEFIT
 ADDRESSING COLORADO S SUBSTANCE USE DISORDER MEDICAID BENEFIT Recommendations for a Community-Based Approach PRESENTED TO: Colorado Department of Health Care Policy and Financing July 31, 2012 EXECUTIVE
ADDRESSING COLORADO S SUBSTANCE USE DISORDER MEDICAID BENEFIT Recommendations for a Community-Based Approach PRESENTED TO: Colorado Department of Health Care Policy and Financing July 31, 2012 EXECUTIVE