DR. RAJENDRAN S INSTITUTE OF MEDICAL EDUCATION
|
|
|
- Owen Carter
- 8 years ago
- Views:
Transcription
1 Page 1 of 17 DR. RAJENDRAN S INSTITUTE OF MEDICAL EDUCATION SPINAL CORD DISEASES PART 2 1) Match presentation with site of lesion a. Lesion near foramen magnum A b. Conus medullaris (sacral cord) B [ No anal reflex.] c. Cauda equina C [ Radicular pain is typical.] d. Cervical cord D [ Ipsilateral Horner s syndrome may develop with cervical cord lesion at any level.] A Weakness of ipsilateral shoulder and arm, followed by weakness of ipsilateral leg, then contralateral leg, then contralateral arm, with respiratory paralysis B Saddle anesthesia, early bladder/bowel/sexual dysfunction. C Flaccid, areflexic, asymmetric paraparesis, bladder/bowel dysfunction, sensory loss below L1, pain in perineum D Horner s syndrome

2 Page 2 of 17 C3, C4 - Extensive lesions near the junction of the cervical cord and medulla are fatal due to involvement of adjacent medullary vasomotor and respiratory centers. - Upper cervical cord lesions produce quadriplegia and weakness of the diaphragm. Phrenic nerve supply is C3 to C5. Breathing is possible only by use of accessory muscles of respiration. C4, C5 - Quadriplegia with preserved respiratory function. C5, C6 - Loss of biceps and brachioradialis reflex {LMN signs at the level of lesion and UMN signs (i.e., quadriparesis) below the level of lesion}. Shoulder muscles are spared. - Triceps reflex (C6-8) is exaggerated. - Inversion of the brachioradialis reflex is typical of a lesion at C5 level. The normal components of brachioradialis reflex are flexion of the forearm, supination of the forearm and flexion of the fingers. In inversion of the brachioradialis reflex, tapping the radius to elicit the brachioradialis reflex causes exaggerated finger and hand flexion without flexion and supination of the forearm. C7 - Biceps are spared. Biceps and brachioradialis reflexes (C5, 6 segments) are preserved. - There is weakness of finger and wrist extensors. - There is loss of triceps reflex. C8 - There is paralysis of finger and wrist flexion and spastic paraparesis. - Triceps reflex is reduced or absent. - Horner s syndrome may be present. T1 to T12 - Thoracic cord lesion is best localized by sensory level. See figures below. L2 to L4 - There is paralysis of flexion and adduction of the thigh. Leg extension becomes weak at the knee, and the knee jerk is absent. S1 - Paralysis of movements of the foot and ankle, flexion at the knee, and extension of the thigh, and abolish the ankle jerk (S1).
 is exaggerated. - Inversion of the brachioradialis reflex is typical of a lesion at C5 level.")

3 Page 3 of 17 A dermatome is a portion of the skin supplied by each spinal nerve There is no C1 dermatome in many persons. When a C1 dermatome is present, it covers a small area in the central part of the neck, close to the occiput C5 dermatome is over the deltoid muscle T1 is confined to the medial side of arm The thumb, middle finger, and fifth digit are within the C6, C7, and C8 dermatomes, respectively. The nipple is at the level of T4 The umbilicus is at the level of T10

4 Page 4 of 17 2) Which is/are seen in lesions of the foramen magnum? a. "Around the clock" pattern of weakness [ Compressive lesions near the foramen magnum may produce weakness of the ipsilateral shoulder and arm followed by weakness of the ipsilateral leg, then the contralateral leg, and finally the contralateral arm ("around the clock" pattern). This may begin in any of the four limbs.] b. Suboccipital pain [ Occipital or neck pain, often increased by neck movement, is a common initial manifestation. The second cervical root innervates the posterior aspect of the scalp, which explains the pattern of radicular pain. If the compression is at the third or fourth cervical level, radicular pain may be projected to the neck or the top of the shoulder.] c. Dissociated sensory loss [ Pain and numbness affecting the same upper extremity first involved by spastic weakness is an early finding. The sensory disturbances are often of the dissociated type (i.e., loss of pain and temperature sensation with preserved tactile sensation).] d. Downbeating nystagmus [ Cranial nerve symptoms and signs may include nystagmus, often downbeating; impaired sensation over the upper face (caused by involvement of the descending tract of cranial nerve V); and dysarthria, dysphonia, and dysphagia.] e. All of the above T [ Foramen magnum and upper cervical spine tumors may cause signs of LMN weakness, atrophy, and depressed reflexes in the arms and hands. The mechanism of this LMN disturbance is uncertain but may be due to ischemia as a result of involvement of the anterior spinal artery. Magnetic resonance imaging (MRI) is the test of choice for imaging the craniocervical junction.] 3) What is/are the cause(s) of Lhermitte s sign? a. Cervical cord lesion [ Lhermitte's symptom is an electrical sensation radiating down the spine from the neck elicited by neck flexion. It usually indicates involvement of the cervical or upper thoracic (T1-T2) spine. Lhermitte's sign may be an early sign of cord compression.]
![contralateral leg, and finally the contralateral arm ("around the clock" pattern). This may begin in any of the four limbs.] b.](/docs-images/45/10120968/images/page_4.jpg "Suboccipital pain [ Occipital or neck pain, often increased by neck movement, is a common initial manifestation.")
5 Page 5 of 17 b. Multiple sclerosis c. Cervical spondylosis d. Reaction to radiation treatment [ Lhermitte's sign is due to transient demyelination of the spinal cord following significant radiation exposure.] e. All of the above T CAUSES OF CERVICAL CORD DISEASE Cervical spondylosis Trauma Congenital disturbances of the craniocervical junction Chiari malformation Foramen magnum tumors Metastasis Meningiomas Neurofibroma Glioma Teratoma Atlantoaxial subluxation (e.g., rheumatoid arthritis) Multiple sclerosis Syrinomyelia
![radiation exposure.] e.](/docs-images/45/10120968/images/page_5.jpg "All of the above T CAUSES OF CERVICAL CORD DISEASE Cervical spondylosis Trauma Congenital disturbances of the craniocervical")
6 Page 6 of 17 4) Whiplash injury - False statement a. Usually due to automobile accidents [ Whiplash injury is due to trauma (usually automobile accidents) causing strain of muscles and ligaments of the cervical vertebrae. Rearend collisions are responsible for about 85% of all whiplash injuries. When an occupant of a motor vehicle is hit from behind by another vehicle, there occurs hyperextension of neck followed by flexion.] b. Due to hyperextension of neck c. Due to hyper flexion of neck [ Some clinicians use the term to also describe other types of collisions wherein the neck is subjected to different combinations of flexion, extension, and lateral motion.] d. Usually associated with fractures or disk herniation F [ False statement. This diagnosis should not be applied to patients with fractures, disk herniation, head injury, or altered consciousness.] e. Neck pain is common [ Following a whiplash injury, patients present with neck pain within 24 hours. The most common cause of the neck pain is myofascial injury. Eighty percent of patients with whiplash-type injuries also complain of headaches during the first 4 weeks after the accident.] 5) Spurling's sign a. Parkinson s disease b. Wilson disease c. Cervical disk disease [ Herniation of a lower cervical disk is a common cause of neck pain radiating to shoulder or arm. Neck movement aggravates this radicular pain. Extension and lateral rotation of the neck narrows the intervertebral foramen (see figure below) and may reproduce radicular pain (Spurling's sign). In young individuals, acute radiculopathy and ruptured cervical disk is usually due to trauma. Subacute radiculopathy is usually due to a combination of disk disease and spondylosis.]


7 Page 7 of 17 d. Down syndrome e. Prion disease

8 Page 8 of 17 6) Cervical spondylosis - True statement a. Due to osteoarthritis of the cervical spine [ It may produce neck pain that radiates into the back of the head, shoulders, or arms. It may also cause headaches in the posterior occipital region (supplied by the C2-C4 nerve roots).] b. May compress the cervical spinal cord [ Narrowing of the spinal canal by osteophytes, ossification of the posterior longitudinal ligament, or a large central disk may compress the cervical spinal cord. Combinations of radiculopathy and myelopathy also occur.] c. Lhermitte's symptom may develop [ Lhermitte's symptom indicates involvement of the cervical or upper thoracic (T1-T2) spine.] d. MRI is diagnostic [ MRI or CT myelography can show the anatomic abnormalities. EMG and nerve conduction studies can localize and assess the severity of the nerve root injury.] e. All of the above T [ Differential diagnosis include amyotrophic lateral sclerosis, multiple sclerosis, spinal cord tumors, and syringomyelia. ] 7) Not typical of spondylitic myelopathy is a. C5 nerve root compression [ Cervical spondylosis tends to affect particularly the C5 and C6 nerve roots. Early symptoms are neck and shoulder pain with stiffness. This is due compression of C5 or C6 nerve roots by bone and soft tissue overgrowth. Biceps reflex (C5-C6) is commonly reduced. Suggestive of cervical spondylosis is a depressed brachioradialis (C6) reflex with hyperactive finger flexors (C8-T1), indicating a C6 radiculoneuropathy with myelopathy. Neoplasms or other diseases at the C6 level may cause a similar clinical presentation.] b. Slowly progressive spastic paraparesis [ If there is an associated myelopathy, upper motor neuron weakness develops in one or both legs. Spastic paraparesis is due to compression of the cervical cord. Cervical spondylosis is one of the most common causes of gait difficulty in the elderly.]
 spine.] d.")
9 Page 9 of 17 c. Atrophy of intrinsic hand muscles [ Dermatomal sensory loss in the arms, atrophy of intrinsic hand muscles, increased deep tendon reflexes in the legs, and extensor plantar responses are common.] d. Diminished vibration sense [ Vibratory sense is diminished in the legs. Romberg sign may be present.] e. Urinary incontinence T [ Urinary urgency or incontinence occurs in advanced cases. Diagnosis is best made by MRI. Definitive therapy consists of surgical relief of the compression. A cervical collar may be very helpful in milder cases.] DIAGNOSIS OF CERVICAL RADICULOPATHY Pain Weakness Sensory Loss Reflex Loss C5 Neck, shoulder, and Deltoid Lateral border of the Biceps interscapular region; lateral aspect of the arm Spinati Rhomboids shoulder and upper part of the arm (brachioradialis) C6 Shoulder; lateral aspect of Biceps Lateral aspect of the Brachioradialis the forearm, and the first two digits Brachioradialis Extensor carpi radialis forearm and the first two digits (biceps) C7 Interscapular region, posterior of the arm, midforearm Triceps Midforearm and middle digit Triceps Extensor carpi and digitorum Flexor carpi radialis
![Diminished vibration sense [ Vibratory sense is diminished in the legs. Romberg sign may be present.] e. Urinary incontinence T [ Urinary urgency or incontinence occurs in advanced cases.](/docs-images/45/10120968/images/page_9.jpg "Diagnosis is best made by MRI. Definitive therapy consists of surgical relief of the compression. A cervical collar may be very helpful in milder cases.")
10 Page 10 of 17 C8 Medial aspect of the forearm Extensor carpi and Medial aspect of the Finger flexors and hand digitorum forearm and hand and the (triceps) Flexor digitorum fourth and fifth digits (sublimis and profundus) Flexor carpi ulnaris T1 Medial aspect of the arm to Intrinsic hand muscles Medial aspect of the arm to the elbow the elbow 8) Bilateral Hoffmann's signs a. UMN disease b. Anxiety c. Hyperthyroidism d. All of the above T [ Hoffmann's sign is performed by dorsiflexing the patient's wrist and then flicking the distal phalanx of the middle finger with the examiner's thumb. The patient's middle finger is thereby flexed and suddenly extended. Hoffmann's sign is present when there is reflex flexion of the patient's thumb and other fingers. Bilateral Hoffmann's sign usually is an indication of hyperactive deep tendon reflexes. Although disease of the pyramidal pathways may be responsible, healthy persons with hyperactive reflexes may have bilateral Hoffmann's signs (e.g., anxiety, hyperthyroidism, and stimulatory drugs). When Hoffmann's sign is present unilaterally, it usually signifies disease of the nervous system.]

11 Page 11 of 17 9) What is the most common site of lesion in a patient with paraparesis? a. Spinal cord T [ Most lesions of the spinal cord produce quadriparesis or paraparesis. A spinal cord lesion should be suspected in a patient with bilateral weakness, bowel or bladder control deficits, and back pain. Common causes of spinal cord compression are disk protrusion, spondylosis and acute trauma, but neoplastic and infectious causes should always be considered. Spinal cord compression resulting in paralysis should be evaluated as quickly as possible with MRI.] b. Parasagittal lesions [ An intraspinal lesion at or below the upper thoracic spinal cord level is most commonly responsible for paraparesis. Paraparesis may also result from parasagittal intracranial lesions, anterior horn cell disorders, cauda equina syndromes and peripheral neuropathies.] c. Anterior horn cell disorders [ E.g., poliovirus.] d. Cauda equina syndrome [ Cauda equina syndrome result from trauma to the low back, midline disk herniation, or intraspinal tumor.] e. Guillain-Barre syndrome [ Paraparesis may be due to a peripheral neuropathy such as Guillain-Barre syndrome.] ACUTE PARAPARESIS (Spinal cord compression resulting in paralysis should be evaluated as quickly as possible with MRI) Compressive spinal cord lesions - Disc prolapse - Vertebral involvement by malignancy or infection - Epidural tumor, abscess, or hematoma Guillain-Barre syndrome This is the most common LMN weakness that progresses over days to several weeks Spinal cord infarction {Anterior spinal artery infarction usually causes paraparesis and spinothalamic sensory loss below the level of the lesion; dorsal column function (proprioception) is preserved.} Spinal cord vascular anomaly Transverse myelitis (Postinfectious, viral infections, SLE, Sarcoidosis, Multiple sclerosis) Diseases of the cerebral hemispheres ( Parasagittal meningiomas, anterior cerebral artery ischemia, superior sagittal sinus or cortical venous thrombosis, and acute hydrocephalus)

12 Page 12 of 17 CHRONIC PARAPARESIS (OVER WEEKS OR MONTHS) Degenerative disease of the spine Hereditary degenerative diseases Intraparenchymal spinal cord tumor Multiple sclerosis Subacute combined degeneration Motor system disease Syringomyelia Tropical spastic paraparesis Paraneoplastic syndromes Parasagittal meningiomas Chronic hydrocephalus CAUDA EQUINA SYNDROME Trauma to the low back Midline disk herniation Intraspinal tumor; although sphincters are affected, hip flexion is often spared, as is sensation over the anterolateral thighs. Rarely, paraparesis is caused by a rapidly evolving anterior horn cell disease (such as poliovirus or West Nile virus infection), peripheral neuropathy (such as Guillain-Barré syndrome; Chap. 380) or myopathy (Chap. 382). In such cases, electrophysiologic studies are diagnostically helpful and refocus the subsequent evaluation. RECURRENT EPISODES OF PARAPARESIS Multiple sclerosis Vascular malformations of the spinal cord
, peripheral neuropathy (such as Guillain-Barré syndrome; Chap.")
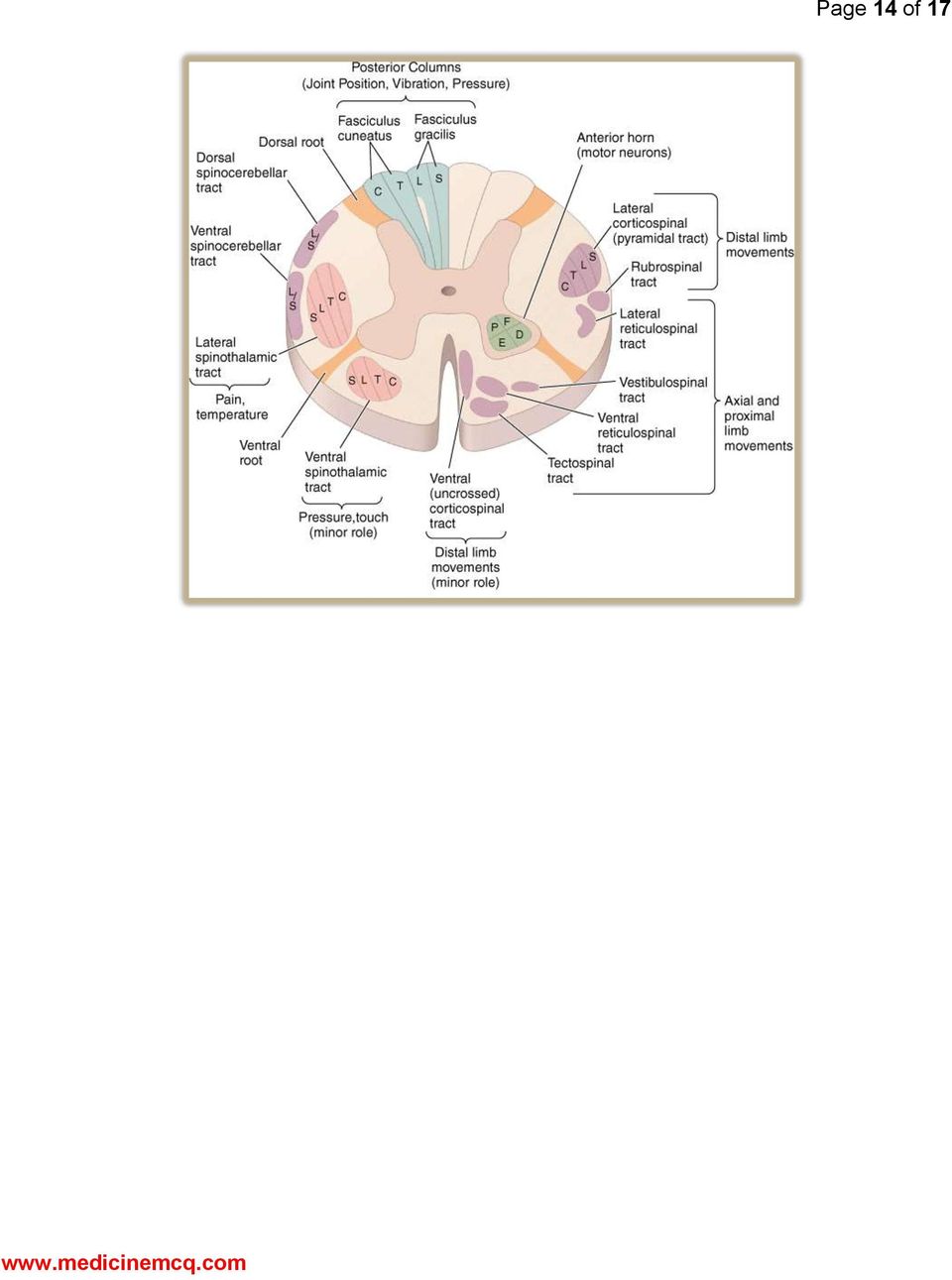
13 Page 13 of 17 ACUTE QUADRIPARESIS Guillain-Barre syndrome This is the most common LMN weakness that progresses over days to several weeks Cerebral anoxia Hypotension Brainstem or cervical cord ischemia Trauma Systemic metabolic abnormalities and electrolyte disturbances Toxins Periodic paralyses 10) Early sacral sensory loss is typical of a. Extramedullary lesions T [ In extramedullary lesions (90%), radicular pain is usually prominent. There is early sacral sensory loss (damage to lateral spinothalamic tract). This is due to lamination of the spinothalamic tract with the sacral fibers being outermost. Spastic weakness in the legs (damage to corticospinal tract) also appears early. See 2 figures below.] b. Intramedullary lesions [ Intramedullary lesions (10%) usually produce poorly localized burning pain rather than radicular pain. Sensation in the perineal and sacral areas ( sacral sparing ) is usually present normally in the early stages. Corticospinal tract signs appear later. Intramedullary diseases presents with tract dysfunction (not with nerve root pain). Extramedullary compression presents with nerve root pain (radicular pain).] c. Both d. None
 also appears early. See 2 figures below.] b.")

14 Page 14 of 17


15 Page 15 of 17 ACUTE AND SUBACUTE SPINAL CORD DISEASES Compressive myelopathies Neoplastic Spinal cord compression Spinal epidural abscess Epidural hematoma Hematomyelia

16 Page 16 of 17 Noncompressive myelopathies (Acute transverse myelopathies) Spinal cord infarction Acute transverse myelopathies Infectious myelitis (Herpes zoster is the most common viral cause of acute myelitis) Postinfectious myelitis or postvaccinial myelitis Multiple sclerosis CHRONIC SPINAL CORD DISEASES Spondylitic myelopathy Vascular malformations Retrovirus-associated myelopathies Syringomyelia Multiple sclerosis Subacute combined degeneration (vitamin b12 deficiency) Tabes dorsalis Familial spastic paraplegia Primary lateral sclerosis Lathyrism
 Tabes dorsalis Familial spastic paraplegia Primary lateral")
17 Page 17 of 17 Chronic paraneoplastic myelopathy Radiation injury For rest of the 37 questions with explanatory answers, click premium content > Neurology.

III./8.4.2: Spinal trauma. III./8.4.2.1 Injury of the spinal cord
 III./8.4.2: Spinal trauma Introduction Causes: motor vehicle accidents, falls, sport injuries, industrial accidents The prevalence of spinal column trauma is 64/100,000, associated with neurological dysfunction
III./8.4.2: Spinal trauma Introduction Causes: motor vehicle accidents, falls, sport injuries, industrial accidents The prevalence of spinal column trauma is 64/100,000, associated with neurological dysfunction
Weakness More diffuse More focal Atrophy Mild, general Severe, focal Atrophy versus weakness
 Spinal Cord Disorders (Dr. Merchut) Clinical signs and symptoms in spinal cord lesions 1. Motor signs and symptoms Lower motor neuron (LMN) signs (Table 1) are found in a limb if some of its muscles are
Spinal Cord Disorders (Dr. Merchut) Clinical signs and symptoms in spinal cord lesions 1. Motor signs and symptoms Lower motor neuron (LMN) signs (Table 1) are found in a limb if some of its muscles are
CERVICAL DISC HERNIATION
 CERVICAL DISC HERNIATION Most frequent at C 5/6 level but also occur at C 6 7 & to a lesser extent at C4 5 & other levels In relatively younger persons soft disk protrusion is more common than hard disk
CERVICAL DISC HERNIATION Most frequent at C 5/6 level but also occur at C 6 7 & to a lesser extent at C4 5 & other levels In relatively younger persons soft disk protrusion is more common than hard disk
Chapter 15. Spinal conditions. Spinal cord disease (myelopathy) Clinical neuroanatomy. Symptoms and signs. Sensory. Motor.
 Clinical neuroanatomy. Symptoms and signs. Sensory. Motor.") GIN15 8/27/04 12:42 PM Page 121 Chapter 15 Spinal conditions Spinal cord disease (myelopathy) Clinical neuroanatomy Figure 15.1 is a transverse section of the spinal cord, showing the location of the major
GIN15 8/27/04 12:42 PM Page 121 Chapter 15 Spinal conditions Spinal cord disease (myelopathy) Clinical neuroanatomy Figure 15.1 is a transverse section of the spinal cord, showing the location of the major
CERVICAL SPONDYLOSIS
 CERVICAL SPONDYLOSIS Dr. Sahni B.S Dy. Chief Medical Officer, ONGC Hospital Panvel-410221,Navi Mumbai,India Introduction The cervical spine consists of the top 7 vertebrae of the spine. These are referred
CERVICAL SPONDYLOSIS Dr. Sahni B.S Dy. Chief Medical Officer, ONGC Hospital Panvel-410221,Navi Mumbai,India Introduction The cervical spine consists of the top 7 vertebrae of the spine. These are referred
Spine and Spinal Cord Injuries. William Schecter, MD
 Spine and Spinal Cord Injuries William Schecter, MD Anatomy of the Spine http://education.yahoo.com/reference/gray/fig/387.html Anatomy of the spine 7 cervical vertebrae 12 thoracic vertebrae 5 lumbar
Spine and Spinal Cord Injuries William Schecter, MD Anatomy of the Spine http://education.yahoo.com/reference/gray/fig/387.html Anatomy of the spine 7 cervical vertebrae 12 thoracic vertebrae 5 lumbar
ICD-9-CM coding for patients with Spinal Cord Injury*
 ICD-9-CM coding for patients with Spinal Cord Injury* indicates intervening codes have been left out of this list. OTHER DISORDERS OF THE CENTRAL NERVOUS SYSTEM (340-349) 344 Other paralytic syndromes
ICD-9-CM coding for patients with Spinal Cord Injury* indicates intervening codes have been left out of this list. OTHER DISORDERS OF THE CENTRAL NERVOUS SYSTEM (340-349) 344 Other paralytic syndromes
Temple Physical Therapy
 Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
The Anatomy of Spinal Cord Injury (SCI)
") The Anatomy of Spinal Cord Injury (SCI) What is the Spinal Cord? The spinal cord is that part of your central nervous system that transmits messages between your brain and your body. The spinal cord has
The Anatomy of Spinal Cord Injury (SCI) What is the Spinal Cord? The spinal cord is that part of your central nervous system that transmits messages between your brain and your body. The spinal cord has
Differentiating Cervical Radiculopathy and Peripheral Neuropathy. Adam P. Smith, MD
 Differentiating Cervical Radiculopathy and Peripheral Neuropathy Adam P. Smith, MD I have no financial, personal, or professional conflicts of interest to report Radiculopathy versus Neuropathy Radiculopathy
Differentiating Cervical Radiculopathy and Peripheral Neuropathy Adam P. Smith, MD I have no financial, personal, or professional conflicts of interest to report Radiculopathy versus Neuropathy Radiculopathy
Advanced Practice Provider Academy
 (+)Dean T. Harrison, MPAS,PA C,DFAAPA Director of Mid Level Practitioners; Assistant Medical Director Clinical Evaluation Unit, Division of Emergency Medicine, Department of Surgery, Duke University Medical
(+)Dean T. Harrison, MPAS,PA C,DFAAPA Director of Mid Level Practitioners; Assistant Medical Director Clinical Evaluation Unit, Division of Emergency Medicine, Department of Surgery, Duke University Medical
ICD-10 Cheat Sheet Frequently Used ICD-10 Codes for Musculoskeletal Conditions *
 ICD-10 Cheat Sheet Frequently Used ICD-10 Codes for Musculoskeletal Conditions * Finding the ICD-10 equivalent for an ICD-9 code can be a challenge. This resource of frequently used codes can help when
ICD-10 Cheat Sheet Frequently Used ICD-10 Codes for Musculoskeletal Conditions * Finding the ICD-10 equivalent for an ICD-9 code can be a challenge. This resource of frequently used codes can help when
OVERVIEW. NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. WHAT IS THE MOST IMPORTANT PART OF THE PHYSICAL EXAM?
 NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. Neurological Surgery Bluegrass Orthopaedics and Hand Care OVERVIEW SCOPE OF THE PROBLEM PREVALENCE PATHOLOGY ANATOMIC CONSIDERATIONS ASSESSMENT
NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. Neurological Surgery Bluegrass Orthopaedics and Hand Care OVERVIEW SCOPE OF THE PROBLEM PREVALENCE PATHOLOGY ANATOMIC CONSIDERATIONS ASSESSMENT
Pain Management Top Diagnosis Codes (Crosswalk)
") Pain Management Top s (Crosswalk) 274.00 Gout arthropathy, M1000 Idiopathic gout, unspecified site unspecified M10011 Idiopathic gout, right shoulder M10012 Idiopathic gout, left shoulder M10019 Idiopathic
Pain Management Top s (Crosswalk) 274.00 Gout arthropathy, M1000 Idiopathic gout, unspecified site unspecified M10011 Idiopathic gout, right shoulder M10012 Idiopathic gout, left shoulder M10019 Idiopathic
Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario
 Page 1 Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario Injury Descriptions Developed from Newfoundland claim study injury definitions No injury Death Psychological
Page 1 Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario Injury Descriptions Developed from Newfoundland claim study injury definitions No injury Death Psychological
Cervicogenic Headache: A Review of Diagnostic and Treatment Strategies
 Cervicogenic Headache: A Review of Diagnostic and Treatment Strategies 1 Journal of the American Osteopathic Association April 2005, Vol. 105, No. 4 supplement, pp. 16-22 David M. Biondi, DO FROM ABSTRACT:
Cervicogenic Headache: A Review of Diagnostic and Treatment Strategies 1 Journal of the American Osteopathic Association April 2005, Vol. 105, No. 4 supplement, pp. 16-22 David M. Biondi, DO FROM ABSTRACT:
BACK PAIN PATHWAY DEFINTIONS
 BACK PAIN PATHWAY DEFINTIONS Cauda Equina Syndrome (CES) Current or imminent compression of the sacral nerve roots resulting in neurogenic bladder and bowel dysfunction. Symptoms typically include: severe
BACK PAIN PATHWAY DEFINTIONS Cauda Equina Syndrome (CES) Current or imminent compression of the sacral nerve roots resulting in neurogenic bladder and bowel dysfunction. Symptoms typically include: severe
Low Back Injury in the Industrial Athlete: An Anatomic Approach
 Low Back Injury in the Industrial Athlete: An Anatomic Approach Earl J. Craig, M.D. Assistant Professor Indiana University School of Medicine Department of Physical Medicine and Rehabilitation Epidemiology
Low Back Injury in the Industrial Athlete: An Anatomic Approach Earl J. Craig, M.D. Assistant Professor Indiana University School of Medicine Department of Physical Medicine and Rehabilitation Epidemiology
Spinal Cord Injury Education. An Overview for Patients, Families, and Caregivers
 Spinal Cord Injury Education An Overview for Patients, Families, and Caregivers Spinal Cord Anatomy A major component of the Central Nervous System (CNS) It is 15 to 16 inches long, and weighs 1 to 2 ounces
Spinal Cord Injury Education An Overview for Patients, Families, and Caregivers Spinal Cord Anatomy A major component of the Central Nervous System (CNS) It is 15 to 16 inches long, and weighs 1 to 2 ounces
Traumatic injuries SPINAL CORD. Causes of Traumatic SCI SYMPTOMS. Spinal Cord trauma can be caused by:
 Traumatic injuries SPINAL CORD Jennie Trkulja RN, BScN, ENC (c) Causes of Traumatic SCI Spinal Cord trauma can be caused by: MVC (most injuries) Gunshots Falls Stabbings Assaults Industrial accidents Sports
Traumatic injuries SPINAL CORD Jennie Trkulja RN, BScN, ENC (c) Causes of Traumatic SCI Spinal Cord trauma can be caused by: MVC (most injuries) Gunshots Falls Stabbings Assaults Industrial accidents Sports
.org. Cervical Spondylosis (Arthritis of the Neck) Anatomy. Cause
 Anatomy. Cause") Cervical Spondylosis (Arthritis of the Neck) Page ( 1 ) Neck pain can be caused by many things but is most often related to getting older. Like the rest of the body, the disks and joints in the neck (cervical
Cervical Spondylosis (Arthritis of the Neck) Page ( 1 ) Neck pain can be caused by many things but is most often related to getting older. Like the rest of the body, the disks and joints in the neck (cervical
Neck Injuries and Disorders
 Neck Injuries and Disorders Introduction Any part of your neck can be affected by neck problems. These affect the muscles, bones, joints, tendons, ligaments or nerves in the neck. There are many common
Neck Injuries and Disorders Introduction Any part of your neck can be affected by neck problems. These affect the muscles, bones, joints, tendons, ligaments or nerves in the neck. There are many common
IMPAIRMENT RATING 5 TH EDITION MODULE II
 IMPAIRMENT RATING 5 TH EDITION MODULE II THE SPINE AND ALTERATION OF MOTION SEGMENT INTEGRITY (AOMSI) PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with: The chapter on the spine includes
IMPAIRMENT RATING 5 TH EDITION MODULE II THE SPINE AND ALTERATION OF MOTION SEGMENT INTEGRITY (AOMSI) PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with: The chapter on the spine includes
Contact your Doctor or Nurse for more information.
 A spinal cord injury is damage to your spinal cord that affects your movement, feeling, or the way your organs work. The injury can happen by cutting, stretching, or swelling of the spinal cord. Injury
A spinal cord injury is damage to your spinal cord that affects your movement, feeling, or the way your organs work. The injury can happen by cutting, stretching, or swelling of the spinal cord. Injury
Clinical guidance for MRI referral
 MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
Spine Anatomy and Spine General The purpose of the spine is to help us stand and sit straight, move, and provide protection to the spinal cord.
 Spine Anatomy and Spine General The purpose of the spine is to help us stand and sit straight, move, and provide protection to the spinal cord. Normal List Kyphosis The human spine has 7 Cervical vertebra
Spine Anatomy and Spine General The purpose of the spine is to help us stand and sit straight, move, and provide protection to the spinal cord. Normal List Kyphosis The human spine has 7 Cervical vertebra
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
Colossus Important Diagnoses. Instructions for How to List Diagnoses
 1 Colossus Important Diagnoses Instructions for How to List Diagnoses 1. Only list diagnoses on HCFA-1500 or CMS-1500 billing forms 2. Use as many billing forms/pages as necessary (4 diagnoses per billing
1 Colossus Important Diagnoses Instructions for How to List Diagnoses 1. Only list diagnoses on HCFA-1500 or CMS-1500 billing forms 2. Use as many billing forms/pages as necessary (4 diagnoses per billing
THE LUMBAR SPINE (BACK)
") THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
Cervical Spondylosis (Arthritis of the Neck)
") Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Copyright 2009 American Academy of Orthopaedic Surgeons Cervical Spondylosis (Arthritis of the Neck) Neck pain is extremely common. It can be caused by many things, and is most often related to getting
Neck Pain Overview Causes, Diagnosis and Treatment Options
 Neck Pain Overview Causes, Diagnosis and Treatment Options Neck pain is one of the most common forms of pain for which people seek treatment. Most individuals experience neck pain at some point during
Neck Pain Overview Causes, Diagnosis and Treatment Options Neck pain is one of the most common forms of pain for which people seek treatment. Most individuals experience neck pain at some point during
AMA Guides & California Code of Regulations P&S Report Checklist
 http://www.pdratings.com/ AMA Guides & California Code of Regulations P&S Report Checklist [L.C. 139.2 (J)-(2)&(3), (k)-(5), 4060(b)(1), 4062 (d)(2), 4068, 4620, 8 CCR WCAB 10606 & 8 CCR 9785] AMA Brachial
http://www.pdratings.com/ AMA Guides & California Code of Regulations P&S Report Checklist [L.C. 139.2 (J)-(2)&(3), (k)-(5), 4060(b)(1), 4062 (d)(2), 4068, 4620, 8 CCR WCAB 10606 & 8 CCR 9785] AMA Brachial
Human Anatomy & Physiology Spinal Cord, Spinal Nerves and Somatic Reflexes 13-1
 Human Anatomy & Physiology Spinal Cord, Spinal Nerves and Somatic Reflexes 13-1 Spinal Cord, Spinal Nerves and Somatic Reflexes Spinal cord Spinal nerves Somatic reflexes 13-2 Overview of Spinal Cord Information
Human Anatomy & Physiology Spinal Cord, Spinal Nerves and Somatic Reflexes 13-1 Spinal Cord, Spinal Nerves and Somatic Reflexes Spinal cord Spinal nerves Somatic reflexes 13-2 Overview of Spinal Cord Information
LOW BACK PAIN EXAMINATION
 LOW BACK PAIN EXAMINATION John Petty, M.D. Medical Director Department of Physical Medicine & Rehabilitation Kettering Medical Center February 8, 2014 PRE-TEST QUESTION What part of the low back physical
LOW BACK PAIN EXAMINATION John Petty, M.D. Medical Director Department of Physical Medicine & Rehabilitation Kettering Medical Center February 8, 2014 PRE-TEST QUESTION What part of the low back physical
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College
 Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College") Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Primary Sources for figures and content: Eastern Campus Marieb,
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Primary Sources for figures and content: Eastern Campus Marieb,
Objectives. Spinal Fractures: Classification Diagnosis and Treatment. Level of Fracture. Neuro exam Muscle Grading
 Objectives Spinal Fractures: Classification Diagnosis and Treatment Johannes Bernbeck,, MD Review and apply the understanding of incidence and etiology of VCF. Examine conservative and operative management
Objectives Spinal Fractures: Classification Diagnosis and Treatment Johannes Bernbeck,, MD Review and apply the understanding of incidence and etiology of VCF. Examine conservative and operative management
Return to same game if sx s resolve within 15 minutes. Return to next game if sx s resolve within one week Return to Competition
 Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Spine University s Guide to Cauda Equina Syndrome
 Spine University s Guide to Cauda Equina Syndrome 2 Introduction Your spine is a very complicated part of your body. It s made up of the bones (vertebrae) that keep it aligned, nerves that channel down
Spine University s Guide to Cauda Equina Syndrome 2 Introduction Your spine is a very complicated part of your body. It s made up of the bones (vertebrae) that keep it aligned, nerves that channel down
Pathoanatomical Changes of the Brachial Plexus and of C5-C6 Following Whiplash-Type Injury: A Case Report
 Pathoanatomical Changes of the Brachial Plexus and of C5-C6 Following Whiplash-Type Injury: A Case Report 1 Journal Of Whiplash & Related Disorders Vol. 1, No, 1, 2002 Gunilla Bring, Halldor Jonsson Jr.,
Pathoanatomical Changes of the Brachial Plexus and of C5-C6 Following Whiplash-Type Injury: A Case Report 1 Journal Of Whiplash & Related Disorders Vol. 1, No, 1, 2002 Gunilla Bring, Halldor Jonsson Jr.,
Disorders of the Spine & Peripheral Nerves
 Disorders of the Spine & Peripheral Nerves An Introduction The LSU-Shreveport Department of Neurosurgery Presenting Authors: Neurosurgery Residents & Faculty Spine Disorders & Neurosurgery Neurosurgery
Disorders of the Spine & Peripheral Nerves An Introduction The LSU-Shreveport Department of Neurosurgery Presenting Authors: Neurosurgery Residents & Faculty Spine Disorders & Neurosurgery Neurosurgery
Aetna Nerve Conduction Study Policy
 Aetna Nerve Conduction Study Policy Policy Aetna considers nerve conduction velocity (NCV) studies medically necessary when both of the following criteria are met: 1. Member has any of the following indications:
Aetna Nerve Conduction Study Policy Policy Aetna considers nerve conduction velocity (NCV) studies medically necessary when both of the following criteria are met: 1. Member has any of the following indications:
Spine & Nervous System Trauma
 Spine & Nervous System Trauma Andrea L. Williams PhD, RN Emergency Education Specialist Clinical Associate Professor University of Wisconsin School of Nursing http://www.youtube.com/watch?v=g2tdp_7q3n4
Spine & Nervous System Trauma Andrea L. Williams PhD, RN Emergency Education Specialist Clinical Associate Professor University of Wisconsin School of Nursing http://www.youtube.com/watch?v=g2tdp_7q3n4
.org. Herniated Disk in the Lower Back. Anatomy. Description
 Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN
 CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
CLINICAL PRACTICE GUIDELINES FOR MANAGEMENT OF LOW BACK PAIN Low back pain is very common, up to 90+% of people are affected by back pain at some time in their lives. Most often back pain is benign and
1 REVISOR 5223.0070. (4) Pain associated with rigidity (loss of motion or postural abnormality) or
 Pain associated with rigidity (loss of motion or postural abnormality) or") 1 REVISOR 5223.0070 5223.0070 MUSCULOSKELETAL SCHEDULE; BACK. Subpart 1. Lumbar spine. The spine rating is inclusive of leg symptoms except for gross motor weakness, bladder or bowel dysfunction, or sexual
1 REVISOR 5223.0070 5223.0070 MUSCULOSKELETAL SCHEDULE; BACK. Subpart 1. Lumbar spine. The spine rating is inclusive of leg symptoms except for gross motor weakness, bladder or bowel dysfunction, or sexual
Spine Trauma: When to Transfer. Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU
 Spine Trauma: When to Transfer Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU Disclosures Depuy Spine Consultant (teaching and courses) Department education and research funds Atlas Spine
Spine Trauma: When to Transfer Alexander Ching, MD Director, Orthopaedic Spine Trauma OHSU Disclosures Depuy Spine Consultant (teaching and courses) Department education and research funds Atlas Spine
Pathophysiology of Acute and Chronic Low Back Pain
 Pathophysiology of Acute and Chronic Low Back Pain Mary Beth Partyka MSN APN Adult Nurse Practitioner Adult Pain Service Advocate Christ Medical Center Presentation Objectives Review the incidence of acute
Pathophysiology of Acute and Chronic Low Back Pain Mary Beth Partyka MSN APN Adult Nurse Practitioner Adult Pain Service Advocate Christ Medical Center Presentation Objectives Review the incidence of acute
Cervical Conditions: Diagnosis and Treatments
 Cervical Conditions: Diagnosis and Treatments Mark R Mikles, M.D. Cervical Conditions: Diagnosis and Treatment Cervical conditions Neck Pain Radiculopathy Myelopathy 1 Cervical Conditions: Diagnosis and
Cervical Conditions: Diagnosis and Treatments Mark R Mikles, M.D. Cervical Conditions: Diagnosis and Treatment Cervical conditions Neck Pain Radiculopathy Myelopathy 1 Cervical Conditions: Diagnosis and
NEUROLOCALIZATION MADE EASY
 NEUROLOCALIZATION MADE EASY Jared B. Galle, DVM, Diplomate ACVIM (Neurology) Dogwood Veterinary Referral Center 4920 Ann Arbor-Saline Road Ann Arbor, MI 48103 Localizing a neurologic problem to an anatomical
NEUROLOCALIZATION MADE EASY Jared B. Galle, DVM, Diplomate ACVIM (Neurology) Dogwood Veterinary Referral Center 4920 Ann Arbor-Saline Road Ann Arbor, MI 48103 Localizing a neurologic problem to an anatomical
If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time.
 If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time. You may be worried about your future, both in respect of finances and
If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time. You may be worried about your future, both in respect of finances and
Emergency Neurological Life Support. Spinal Cord Compression. Version: 1.0 Last Updated: 8/3/2014. Checklist & Communication
 Emergency Neurological Life Support 18 Spinal Cord Compression Version: 1.0 Last Updated: 8/3/2014 17 5 10 12 9 7 13 6 15 4 Checklist & Communication Spinal Cord Compression Page 2 Checklist Quadriplegia?
Emergency Neurological Life Support 18 Spinal Cord Compression Version: 1.0 Last Updated: 8/3/2014 17 5 10 12 9 7 13 6 15 4 Checklist & Communication Spinal Cord Compression Page 2 Checklist Quadriplegia?
Cervical Spine Surgery. Orthopaedic Nursing Seminar. Dr Michelle Atkinson. Friday October 21 st 2011. Cervical Disc Herniation
 Cervical Spine Surgery Dr Michelle Atkinson The Sydney and Dalcross Adventist Hospitals Orthopaedic Nursing Seminar Friday October 21 st 2011 Cervical disc herniation The most frequently treated surgical
Cervical Spine Surgery Dr Michelle Atkinson The Sydney and Dalcross Adventist Hospitals Orthopaedic Nursing Seminar Friday October 21 st 2011 Cervical disc herniation The most frequently treated surgical
The Spine Center at Beth Israel Deaconess
 Spinal Pain The Spine Center at Beth Israel Deaconess Medical Center developed the following detailed eplanation of our care pathways for primary care providers to help support your interactions with patients
Spinal Pain The Spine Center at Beth Israel Deaconess Medical Center developed the following detailed eplanation of our care pathways for primary care providers to help support your interactions with patients
Standard of Care: Cervical Radiculopathy
 Department of Rehabilitation Services Physical Therapy Diagnosis: Cervical radiculopathy, injury to one or more nerve roots, has multiple presentations. Symptoms may include pain in the cervical spine
Department of Rehabilitation Services Physical Therapy Diagnosis: Cervical radiculopathy, injury to one or more nerve roots, has multiple presentations. Symptoms may include pain in the cervical spine
Medical Drug Monitoring ICD-10-CM Sign and Symptom Codes
 Medical Drug Monitoring ICD-10-CM Sign and Symptom s The ICD-10-CM codes listed below are commonly associated with LabCorp and MedTox Laboratories for medical drug monitoring and were selected based on
Medical Drug Monitoring ICD-10-CM Sign and Symptom s The ICD-10-CM codes listed below are commonly associated with LabCorp and MedTox Laboratories for medical drug monitoring and were selected based on
UBC Pain Medicine Residency Program: CanMEDS Goals and Objectives of the Neurology Rotation
 UBC Pain Medicine Residency Program: CanMEDS Goals and Objectives of the Neurology Rotation Goals of the Program To acquire the knowledge and skills necessary to assess and provide a management plan for
UBC Pain Medicine Residency Program: CanMEDS Goals and Objectives of the Neurology Rotation Goals of the Program To acquire the knowledge and skills necessary to assess and provide a management plan for
Cervical Spondylosis. Understanding the neck
 Page 1 of 5 Cervical Spondylosis This leaflet is aimed at people who have been told they have cervical spondylosis as a cause of their neck symptoms. Cervical spondylosis is a 'wear and tear' of the vertebrae
Page 1 of 5 Cervical Spondylosis This leaflet is aimed at people who have been told they have cervical spondylosis as a cause of their neck symptoms. Cervical spondylosis is a 'wear and tear' of the vertebrae
Multiple Sclerosis Jeffrey M. Gelfand, MD
 Multiple Sclerosis Jeffrey M. Gelfand, MD UCSF Multiple Sclerosis Center SFGH Neuroimmunology Clinic UCSF and SFGH Departments of Neurology Goals To review the fundamentals of neurological localization
Multiple Sclerosis Jeffrey M. Gelfand, MD UCSF Multiple Sclerosis Center SFGH Neuroimmunology Clinic UCSF and SFGH Departments of Neurology Goals To review the fundamentals of neurological localization
Spinal Cord Diseases in Bernese Mountain Dogs
 Spinal Cord Diseases in Bernese Mountain Dogs 0 A N O V E R V I E W F O R BERNER O W N E R S O R G A N I Z E D B Y N A N C Y M E L O N E, P H. D. Based on materials obtained from the Berner Garde Foundation
Spinal Cord Diseases in Bernese Mountain Dogs 0 A N O V E R V I E W F O R BERNER O W N E R S O R G A N I Z E D B Y N A N C Y M E L O N E, P H. D. Based on materials obtained from the Berner Garde Foundation
6/3/2011. High Prevalence and Incidence. Low back pain is 5 th most common reason for all physician office visits in the U.S.
 High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
Surgery for cervical disc prolapse or cervical osteophyte
 Mr Paul S. D Urso MBBS(Hons), PhD, FRACS Neurosurgeon Provider Nº: 081161DY Epworth Centre Suite 6.1 32 Erin Street Richmond 3121 Tel: 03 9421 5844 Fax: 03 9421 4186 AH: 03 9483 4040 email: paul@pauldurso.com
Mr Paul S. D Urso MBBS(Hons), PhD, FRACS Neurosurgeon Provider Nº: 081161DY Epworth Centre Suite 6.1 32 Erin Street Richmond 3121 Tel: 03 9421 5844 Fax: 03 9421 4186 AH: 03 9483 4040 email: paul@pauldurso.com
Herniated Disk. This reference summary explains herniated disks. It discusses symptoms and causes of the condition, as well as treatment options.
 Herniated Disk Introduction Your backbone, or spine, has 24 moveable vertebrae made of bone. Between the bones are soft disks filled with a jelly-like substance. These disks cushion the vertebrae and keep
Herniated Disk Introduction Your backbone, or spine, has 24 moveable vertebrae made of bone. Between the bones are soft disks filled with a jelly-like substance. These disks cushion the vertebrae and keep
Reflex Physiology. Dr. Ali Ebneshahidi. 2009 Ebneshahidi
 Reflex Physiology Dr. Ali Ebneshahidi Reflex Physiology Reflexes are automatic, subconscious response to changes within or outside the body. a. Reflexes maintain homeostasis (autonomic reflexes) heart
Reflex Physiology Dr. Ali Ebneshahidi Reflex Physiology Reflexes are automatic, subconscious response to changes within or outside the body. a. Reflexes maintain homeostasis (autonomic reflexes) heart
.org. Cervical Radiculopathy (Pinched Nerve) Anatomy. Cause
 Anatomy. Cause") Cervical Radiculopathy (Pinched Nerve) Page ( 1 ) Cervical radiculopathy, commonly called a pinched nerve occurs when a nerve in the neck is compressed or irritated where it branches away from the spinal
Cervical Radiculopathy (Pinched Nerve) Page ( 1 ) Cervical radiculopathy, commonly called a pinched nerve occurs when a nerve in the neck is compressed or irritated where it branches away from the spinal
Brown-Sequard Syndrome Caused by Cervical Disc Herniation
 62 CASE REPORT Brown-Sequard Syndrome Caused by Cervical Disc Herniation Chih-Hsiu Wang, Chun-Chung Chen, Der-Yang Cho Department of Neurosurgery, China Medical University Hospital, Taichung, Taiwan, R.O.C.
62 CASE REPORT Brown-Sequard Syndrome Caused by Cervical Disc Herniation Chih-Hsiu Wang, Chun-Chung Chen, Der-Yang Cho Department of Neurosurgery, China Medical University Hospital, Taichung, Taiwan, R.O.C.
Spinal Cord Injury Rehabilitation Functional Expectations and Ambulation Potential. Diane Johnston, MSPT
 Spinal Cord Injury Rehabilitation Functional Expectations and Ambulation Potential Diane Johnston, MSPT Objectives for the course Participants will have a general understanding of the epidemiology of Spinal
Spinal Cord Injury Rehabilitation Functional Expectations and Ambulation Potential Diane Johnston, MSPT Objectives for the course Participants will have a general understanding of the epidemiology of Spinal
CONCOMITANT COMBINED DEGENERATIVE COMPRESSION OF THE SPINAL CORD AND CAUDA EQUINA: A REPORT ON THREE CASES
 CASE REPORT CONCOMITANT COMBINED DEGENERATIVE COMPRESSION OF THE SPINAL CORD AND CAUDA EQUINA: A REPORT ON THREE CASES Atanas Davarski 1, Ivo Kehayov 1, Tanya Kitova 2, Christo Zhelyazkov 1, Borislav Kitov
CASE REPORT CONCOMITANT COMBINED DEGENERATIVE COMPRESSION OF THE SPINAL CORD AND CAUDA EQUINA: A REPORT ON THREE CASES Atanas Davarski 1, Ivo Kehayov 1, Tanya Kitova 2, Christo Zhelyazkov 1, Borislav Kitov
Module 1: The Somato-Motor System: Tendon Tap reflex
 Module 1: The Somato-Motor System: Tendon Tap reflex Module Objectives: 1. Describe the anatomic pathway of a tendon tap reflex. 2. Explain how a tendon tap reflex assessment assists in diagnosis of a
Module 1: The Somato-Motor System: Tendon Tap reflex Module Objectives: 1. Describe the anatomic pathway of a tendon tap reflex. 2. Explain how a tendon tap reflex assessment assists in diagnosis of a
Spinal Surgery 2. Teaching Aims. Common Spinal Pathologies. Disc Degeneration. Disc Degeneration. Causes of LBP 8/2/13. Common Spinal Conditions
 Teaching Aims Spinal Surgery 2 Mr Mushtaque A. Ishaque BSc(Hons) BChir(Cantab) DM FRCS FRCS(Ed) FRCS(Orth) Hunterian Professor at The Royal College of Surgeons of England Consultant Orthopaedic Spinal
Teaching Aims Spinal Surgery 2 Mr Mushtaque A. Ishaque BSc(Hons) BChir(Cantab) DM FRCS FRCS(Ed) FRCS(Orth) Hunterian Professor at The Royal College of Surgeons of England Consultant Orthopaedic Spinal
Myelopathy Paresis and Paralysis in Cats
 Myelopathy Paresis and Paralysis in Cats (Disorder of the Spinal Cord Leading to Weakness and Paralysis in Cats) Basics OVERVIEW Myelopathy any disorder or disease affecting the spinal cord; a myelopathy
Myelopathy Paresis and Paralysis in Cats (Disorder of the Spinal Cord Leading to Weakness and Paralysis in Cats) Basics OVERVIEW Myelopathy any disorder or disease affecting the spinal cord; a myelopathy
Diagnostic Imaging Exams
 Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
A Patient s Guide to Artificial Cervical Disc Replacement
 A Patient s Guide to Artificial Cervical Disc Replacement Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness
A Patient s Guide to Artificial Cervical Disc Replacement Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness
Neurology Clerkship Learning Objectives
 Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Management of spinal cord compression
 Management of spinal cord compression (SUMMARY) Main points a) On diagnosis, all patients should receive dexamethasone 10mg IV one dose, then 4mg every 6h. then switched to oral dose and tapered as tolerated
Management of spinal cord compression (SUMMARY) Main points a) On diagnosis, all patients should receive dexamethasone 10mg IV one dose, then 4mg every 6h. then switched to oral dose and tapered as tolerated
Clinical Signs of Low Back Pain
 Review of Clinical Signs Series Editor: Bernard Karnath, MD Clinical Signs of Low Back Pain Bernard Karnath, MD Back pain has been cited as the fifth most common reason that patients visit a physician.
Review of Clinical Signs Series Editor: Bernard Karnath, MD Clinical Signs of Low Back Pain Bernard Karnath, MD Back pain has been cited as the fifth most common reason that patients visit a physician.
Cervical-Spine Injuries: Catastrophic Injury to Neck Sprain. Seth Cheatham, MD
 Cervical-Spine Injuries: Catastrophic Injury to Neck Sprain Seth Cheatham, MD 236 Seth A. Cheatham, MD VCU Sports Medicine I have no financial disclosures Contact sports, specifically football, places
Cervical-Spine Injuries: Catastrophic Injury to Neck Sprain Seth Cheatham, MD 236 Seth A. Cheatham, MD VCU Sports Medicine I have no financial disclosures Contact sports, specifically football, places
Clinical Guideline. Low Back Pain Orthopaedics. Princess Alexandra Hospital Emergency Department. 1 Purpose. 2 Background
 Princess Alexandra Hospital Emergency Department Clinical Guideline Orthopaedics Review Officer: Katherine Isoardi Version no: 1 Approval date: 18/03/2015 Review date: 18/03/2017 Approving Officer Dr James
Princess Alexandra Hospital Emergency Department Clinical Guideline Orthopaedics Review Officer: Katherine Isoardi Version no: 1 Approval date: 18/03/2015 Review date: 18/03/2017 Approving Officer Dr James
Medical Report Checklist: Upper Extremities Peripheral Nerve Disorders Impairments (PND)
") http://www.pdratings.com/ Craig Andrew Lange craig@pdratings.com California Workers Compensation Certified AMA Guides Impairment & Disability Rating Specialists Voice: (415) 861-4040 / Fax: (415) 276-3741
http://www.pdratings.com/ Craig Andrew Lange craig@pdratings.com California Workers Compensation Certified AMA Guides Impairment & Disability Rating Specialists Voice: (415) 861-4040 / Fax: (415) 276-3741
EPIDURAL STEROID AND FACET INJECTIONS FOR SPINAL PAIN
 CLINICAL POLICY EPIDURAL STEROID AND FACET INJECTIONS FOR SPINAL PAIN Policy Number: PAIN 019.16 T2 Effective Date: December 1, 2015 Table of Contents CONDITIONS OF COVERAGE... BENEFIT CONSIDERATIONS..
CLINICAL POLICY EPIDURAL STEROID AND FACET INJECTIONS FOR SPINAL PAIN Policy Number: PAIN 019.16 T2 Effective Date: December 1, 2015 Table of Contents CONDITIONS OF COVERAGE... BENEFIT CONSIDERATIONS..
Anatomy of the Spine. Figure 1. (left) The spine has three natural curves that form an S-shape; strong muscles keep our spine in alignment.
 The spine has three natural curves that form an S-shape; strong muscles keep our spine in alignment.") 1 2 Anatomy of the Spine Overview The spine is made of 33 individual bony vertebrae stacked one on top of the other. This spinal column provides the main support for your body, allowing you to stand upright,
1 2 Anatomy of the Spine Overview The spine is made of 33 individual bony vertebrae stacked one on top of the other. This spinal column provides the main support for your body, allowing you to stand upright,
DISORDERS OF THE CERVICAL SPINE
 DISORDERS OF THE CERVICAL SPINE Kathleen A. Geier, DNP, NP, ONC kgeier@jacksonortho.org (510)238-4851 Jackson Orthopaedic Foundation CONFLICT OF INTEREST I hereby certify that, to the best of my knowledge,
DISORDERS OF THE CERVICAL SPINE Kathleen A. Geier, DNP, NP, ONC kgeier@jacksonortho.org (510)238-4851 Jackson Orthopaedic Foundation CONFLICT OF INTEREST I hereby certify that, to the best of my knowledge,
THE SPINAL CORD AND THE INFLUENCE OF ITS DAMAGE ON THE HUMAN BODY
 THE SPINAL CORD AND THE INFLUENCE OF ITS DAMAGE ON THE HUMAN BODY THE SPINAL CORD. A part of the Central Nervous System The nervous system is a vast network of cells, which carry information in the form
THE SPINAL CORD AND THE INFLUENCE OF ITS DAMAGE ON THE HUMAN BODY THE SPINAL CORD. A part of the Central Nervous System The nervous system is a vast network of cells, which carry information in the form
International Standards for the Classification of Spinal Cord Injury Motor Exam Guide
 C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
Options for Cervical Disc Degeneration A Guide to the Fusion Arm of the M6 -C Artificial Disc Study
 Options for Cervical Disc Degeneration A Guide to the Fusion Arm of the M6 -C Artificial Disc Study Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine
Options for Cervical Disc Degeneration A Guide to the Fusion Arm of the M6 -C Artificial Disc Study Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine
REFERRAL GUIDELINES: NEUROSURGERY
 Outpatient Referral Guidelines Page 1 1 REFERRAL GUIDELINES: NEUROSURGERY Essential Referral Content Date of birth Demographic Contact details (including mobile phone) Referring GP details Interpreter
Outpatient Referral Guidelines Page 1 1 REFERRAL GUIDELINES: NEUROSURGERY Essential Referral Content Date of birth Demographic Contact details (including mobile phone) Referring GP details Interpreter
Whiplash and Whiplash- Associated Disorders
 Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
Transverse Sections of the Spinal Cord
 Transverse Sections of the Spinal Cord The spinal cord is perhaps the most simply arranged part of the CNS. Its basic structure, indicated in a schematic drawing of the eighth cervical segment (Figure
Transverse Sections of the Spinal Cord The spinal cord is perhaps the most simply arranged part of the CNS. Its basic structure, indicated in a schematic drawing of the eighth cervical segment (Figure
EPIDURAL STEROID AND FACET INJECTIONS FOR SPINAL PAIN
 MEDICAL POLICY EPIDURAL STEROID AND FACET INJECTIONS FOR SPINAL PAIN Policy Number: 2015T0004W Effective Date: December 1, 2015 Table of Contents BENEFIT CONSIDERATIONS COVERAGE RATIONALE APPLICABLE CODES..
MEDICAL POLICY EPIDURAL STEROID AND FACET INJECTIONS FOR SPINAL PAIN Policy Number: 2015T0004W Effective Date: December 1, 2015 Table of Contents BENEFIT CONSIDERATIONS COVERAGE RATIONALE APPLICABLE CODES..
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN. Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA
 DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
Herniated Disk in the Lower Back
 Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological Institute Al Maryah Island
Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological Institute Al Maryah Island
Sample Treatment Protocol
 Sample Treatment Protocol 1 Adults with acute episode of LBP Definition: Acute episode Back pain lasting
Sample Treatment Protocol 1 Adults with acute episode of LBP Definition: Acute episode Back pain lasting
Radiculopathy vs. Peripheral Neuropathy. What to do with arm pain? Defining Arm Pain. Arm Pain
 Radiculopathy vs. Peripheral Neuropathy What to do with arm pain? Miriana G. Popadich RN, MSN Clinical Care Coordinator Brachial Plexus Program Department of Neurosurgery University of Michigan Timing
Radiculopathy vs. Peripheral Neuropathy What to do with arm pain? Miriana G. Popadich RN, MSN Clinical Care Coordinator Brachial Plexus Program Department of Neurosurgery University of Michigan Timing
Thoracolumbar Fratures R1: 胡 家 瑞 指 导 老 师 : 吴 轲 主 任
 Thoracolumbar Fratures R1: 胡 家 瑞 指 导 老 师 : 吴 轲 主 任 Patient Data Name: 苏 XX Gender: Female Age:47 years old Admission date: 2010.06.09 Chief complaint Fell down from 4-54 5 meter tree and lead to lumbosacral
Thoracolumbar Fratures R1: 胡 家 瑞 指 导 老 师 : 吴 轲 主 任 Patient Data Name: 苏 XX Gender: Female Age:47 years old Admission date: 2010.06.09 Chief complaint Fell down from 4-54 5 meter tree and lead to lumbosacral
Whiplash Associated Disorder
 Whiplash Associated Disorder The pathology Whiplash is a mechanism of injury, consisting of acceleration-deceleration forces to the neck. Mechanism: Hyperflexion/extension injury Stationary vehicle hit
Whiplash Associated Disorder The pathology Whiplash is a mechanism of injury, consisting of acceleration-deceleration forces to the neck. Mechanism: Hyperflexion/extension injury Stationary vehicle hit
o Understand the anatomy of the covered areas. This includes bony, muscular and ligamentous anatomy.
 COURSE TITLE Kin 505 Activities, Injuries Disease in the Larger Society On-Line offering Instructor Dr. John Miller John.Miller@unh.edu Course Description. Sports and exercise are a part of American society
COURSE TITLE Kin 505 Activities, Injuries Disease in the Larger Society On-Line offering Instructor Dr. John Miller John.Miller@unh.edu Course Description. Sports and exercise are a part of American society
Sciatica Yuliya Mutsa PTA 236
 Sciatica Yuliya Mutsa PTA 236 Sciatica is a common type of pain affecting the sciatic nerve, which extends from the lower back all the way through the back of the thigh and down through the leg. Depending
Sciatica Yuliya Mutsa PTA 236 Sciatica is a common type of pain affecting the sciatic nerve, which extends from the lower back all the way through the back of the thigh and down through the leg. Depending
MALIGNANT SPINAL CORD COMPRESSION. Kate Hamilton Head of Medical Oncology Ballarat Health Services
 MALIGNANT SPINAL CORD COMPRESSION Kate Hamilton Head of Medical Oncology Ballarat Health Services OVERVIEW Background Epidemiology Pathophysiology Diagnosis Investigation Differential Diagnosis Management
MALIGNANT SPINAL CORD COMPRESSION Kate Hamilton Head of Medical Oncology Ballarat Health Services OVERVIEW Background Epidemiology Pathophysiology Diagnosis Investigation Differential Diagnosis Management
Diagnosis and Treatment of Lumbar Spinal Canal Stenosis
 Low Back Pains Diagnosis and Treatment of Lumbar Spinal Canal Stenosis JMAJ 46(10): 439 444, 2003 Katsuro TOMITA Department of Orthopedic Surgery, Kanazawa University Abstract: Lumbar spinal canal stenosis
Low Back Pains Diagnosis and Treatment of Lumbar Spinal Canal Stenosis JMAJ 46(10): 439 444, 2003 Katsuro TOMITA Department of Orthopedic Surgery, Kanazawa University Abstract: Lumbar spinal canal stenosis
Musculoskeletal: Acute Lower Back Pain
 Musculoskeletal: Acute Lower Back Pain Acute Lower Back Pain Back Pain only Sciatica / Radiculopathy Possible Cord or Cauda Equina Compression Possible Spinal Canal Stenosis Red Flags Initial conservative
Musculoskeletal: Acute Lower Back Pain Acute Lower Back Pain Back Pain only Sciatica / Radiculopathy Possible Cord or Cauda Equina Compression Possible Spinal Canal Stenosis Red Flags Initial conservative
SPINE. Postural Malalignments 4/9/2015. Cervical Spine Evaluation. Thoracic Spine Evaluation. Observations. Assess position of head and neck
 SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural